Embed Size (px)
Citation preview

by Rastogi et al. to differentiate between adenoma and hyperplastic polyps(Gastrointest. Endosc. 2008;67:280). These criteria are highly suited to practice inthe United states as they are based on non-magnification colonoscopy. Aim: Toprospectively validate modified NBI criteria to distinguish between adenomatousand hyperplastic polyps. Methods: We enrolled seven endoscopists without priorexperience with NBI to participate in our study. In the white-light phase,endoscopists were asked to predict polyp histology during colonoscopy usingstandard features observed under white light. After completion of white-lightphase, three educational sessions were conducted with each endoscopist tofamiliarize them with the modified NBI criteria. In the NBI phase, endoscopistswere asked to predict polyp histology using the modified NBI criteria. A posterwith modified NBI criteria and representative polyp images was available toendoscopists at the time of colonoscopy as reference. Polyp histology served asthe criteria standard. All data were prospectively collected. A priori sample sizecalculation showed that 400 polyps were needed for the study. Results: Duringthe white-light phase, 142 patients underwent colonoscopies and 206 polypswere removed. The average age of study subjects was 59 years and 58% weremales. During the NBI phase, 147 patients underwent colonoscopies and 232polyps were removed. The average age of study subjects was 59 years and 44%were males. The accuracy of white light and NBI in predicting polyp histologyfor any type of polyp was equivalent for white light and NBI (66% versus 57%;p �0.362) (Table 1). The accuracy of predicting adenomas for white light andNBI was equivalent (73% versus 65%; p�0.426). The accuracy of predictinghyperplastic polyps for white light and NBI was also equivalent (75% versus64%; p�0.27). During the NBI phase, 20 sessile serrated adenomas (SSA) werenoted in the study, 15 of which were classified as hyperplastic polyps based onNBI criteria (sensitivity�25%) Conclusion: The modified NBI criteria cannot berecommended in clinical practice to select polyps for polypectomy. Further, mostSSA were mis-classified as hyperplastic polyps by these criteria.
Table 1. Comparison of white light and NBI in predicting polyp histology
Polyp type ParameterWhite light
(95% CI) NBI (95% CI)�2 Pearson
uncorrectedP
value
Adenoma Sensitivity 0.867 (0.811–0.912) 0.673 (0.623–0.72) 1.848 0.174Specificity 0.558 (0.481–0.622) 0.622 (0.53–0.707) 0.182 0.669Accuracy 0.738 (0.673–0.791) 0.655 (0.59–0.715) 0.633 0.426
Hyperplastic Sensitivity 0.632 (0.518–0.732) 0.68 (0.543–0.797) 0.058 0.810Specificity 0.805 (0.762–0.844) 0.632 (0.598 0.662) 2.018 0.155Accuracy 0.757 (0.694–0.813) 0.642 (0.587–0.689) 1.219 0.27
Overall Accuracy 0.66 (0.651–0.669) 0.573 (0.565–0.581) 0.829 0.362
572A Standardized Learning Module Improves the Accuracy of Ex-Vivo Endoscopic Diagnosis of Polyp Histology With NarrowBand Imaging (NBI) by Community-Based EndoscopistsUri Ladabaum*1, Ann Fioritto3, Jane Paik2, Aya Mitani2, Manisha Desai2,Douglas K. Rex4, Thomas F. Imperiale4, Naresh T. Gunaratnam3
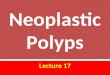
1Gastroenterology, Medicine, Stanford University, Redwood City, CA;2Quantitative Research Unit, Stanford University, Palo Alto, CA;3Huron Gastroenterology, Ann Arbor, MI; 4Gastroenterology, Medicine,Indiana University, Indianapolis, INIntroduction: High accuracy in real-time endoscopic diagnosis of polyp histologycould justify a resect-and-discard practice for polyps ��5mm in size. Theacquisition of novel skills by community endoscopists has received little study.We report on the ex-vivo Phase I of a study of practice-based learning ofendoscopic diagnosis of polyp histology using NBI in community practice. PhaseII, an in-vivo real-time program, is still ongoing. Methods: Fourteen endoscopistsin a large community practice participated. The median years in practice were 16[range 2-36], median annual colonoscopy volume was 922 [range 443-1176], andmedian adenoma detection rate (ADR) in 2009-2010 with high definitioncolonoscopes was 34 [range 24-40] %. Subjects completed a standardizedlearning module with a pre-test, teaching section, and post-test. The teachingsection provided training in the NBI International Colorectal Endoscopic (NICE)classification. Each test consisted of 25 different images of polyps which subjectscategorized as “hyperplastic,” “adenomatous” or “I don’t know,” with each worth4 points out of a 100 maximum. Complete pre-test and post-test data wereavailable for 11 subjects. Post-test data were missing for 1 and pre-test data for 2subjects. The primary outcome was the change in test score. We assessedassociations between the change in test score and endoscopist characteristicsusing linear regression models and chi-square tests at alpha�0.05. Results: Testscores improved in 10/11 subjects (Figure). The mean change in test score was�16 points (p �0.006) (Table). In the pre-test, 4 (33%) participants answered “Idon’t know” at least once, and 6.5% of answers were “I don’t know.” Inconstrast, no answers were “I don’t know” in the post-test. All but 1 subjectscored �90 on the post-test. An endoscopist’s ADR, but not years in practice orcolonoscopy volume, was marginally associated with change in test score(p�0.06). Six out 7 (86%) subjects with ADR �30% scored 80 or higher on thepre-test (mean score 80, SD 14, for the 7 subjects), while 3 out of 5 (60%)
subjects with ADR �30% scored lower than 80 (mean score 67, SD 15, for the 5subjects). However, the subjects with adenoma detection rates �30% showed thegreatest gains in test score, with a mean increase of 26 points (SD 12), whilesubjects with adenoma detection rates �30% showed a mean increase in testscores of 8 points (SD 13). Analogous non-parametric techniques yieldedcomparable results. Discussion: Community endoscopists’ test scores forphotograph-based endoscopic diagnosis of polyp histology improved after studyof a computerized learning module that teaches the NICE classification. Itremains to be determined whether proficiency in ex-vivo endoscopic diagnosistranslates into accurate in-vivo endoscopic diagnosis of polyp histology that isdurable over time in community practice.
Table. Results of Pre-Test, Post-Test and Score Change
Pre-Test Post-TestChange from pre-test
to post-test
Subject number, n 12 13 11% Questions Answered “I Don’t
Know”6.5% 0% �0.07%
Score with “I Don’t Know” countedas incorrect, mean (SD)
79 (15) 94 (5) 16 (15)
Score excluding “I Don’t Know” fromthe count, mean (SD)
85 (9) 94 (5) 10 (8)
573Impact of a Computer Based Teaching Module onCharacterization of Diminutive Colon Polyps Using NarrowBand Imaging (NBI) by Non-Experts in Academics andCommunity Practice: A Video Based StudyAmit Rastogi*1,2, Deepthi S. Rao1, Neil Gupta3, Scott W. Grisolano2,Daniel C. Buckles2, Elena Sidorenko2, John Bonino2,Takahisa Matsuda4, Evelien Dekker5, Tonya Kaltenbach6,Rajvinder Singh7, Sachin Wani8, Prateek Sharma1,2, Mojtaba S. Olyaee2,Ajay Bansal1,2, James E. East91Gastroenterology, Veterans Affairs Medical Center, Kansas City, MO;2Gastroenterology, University of Kansas School of Medicine, KansasCity, KS; 3Gastroenterology, Washington University in St. Louis, St.Louis, MO; 4Gastroenterology, National Cancer Center Hospital, Tokyo,Japan; 5Gastroenterology, Academic Medical Center, Amsterdam,Netherlands; 6Gastroenterology, VA Palo Alto, Stanford UniversitySchool of Medicine, Palo Alto, CA; 7Gastroenterology, Lyell McEwinHospital, Elizabeth Vale, SA, Australia; 8Gastroenterology, University ofColorado, Denver, CO; 9Gastroenterology, John Radcliffe Hospital,Oxford, United KingdomBackground: Real time prediction of polyp histology with NBI has the potential
Score change from pre-test to post-test.
Abstracts
www.giejournal.org Volume 75, No. 4S : 2012 GASTROINTESTINAL ENDOSCOPY AB152

to be utilized for “resect and discard” strategy for diminutive (� 5mm) polypswith significant cost savings. For this strategy to be widely implemented by non-experts, teaching tools have to be developed. Aim: To assess whether acomputer based training tool could improve non-expert NBI performance usinga novel video based approach to simulate clinical practice. Methods: A 20 minaudiovisual (Power Point) teaching module was developed demonstratingpreviously described criteria to differentiate adenomas from hyperplastic polypswith NBI. 80 short video clips of � 5mm polyps with NBI without magnificationwere randomly allocated to pre and post test sets in a blinded fashion using acomputer generated random sequence stratified by polyp histology. Each setconsisted of 40 videos (26 adenomas and 14 hyperplastic). We recruited 3groups of reviewers - experts in NBI (Gp A), non-experts in academics (Gp B)and non-experts in community practice (Gp C). All participants (5 in each group)reviewed pre test videos and reported their diagnosis and confidence level - high(� 90%) or low (�90%). They then viewed the teaching module followed by thepost test videos. A sample size of 200 (40 videos x 5 reviewers) observationswould allow detection of a change in non-expert accuracy from 60% to 75% with80% power and alpha of 0.05. The sensitivity, specificity and accuracy werecalculated by comparing predicted and actual histology for each group, both forpre and post test. Fisher’s exact test was used for statistical analysis. Results: Preand post test results are shown in Table 1. For non-experts (Gp B and C) theaccuracy improved significantly in post test compared to pre test (81% vs 64%; p� 0.001). Accuracy of non experts was significantly lower than that of experts(Gp A) in both pretest ( 64% vs 87%; p �0.001) and post test ( 81% vs 93%; p�0.001). Performance characteristics in post test when diagnosis was made withhigh confidence vs low confidence are shown in Table 2. In all 3 gps, accuracywas significantly higher when participants had high confidence in theirdiagnosis. Non-experts made a greater proportion of high confidence diagnosesfollowing the teaching module - Gp B: 69% vs 49%; p �0.001 and Gp C: 72% vs49%; p �0.001. Conclusions: In a novel video based assessment, practicingacademic and community gastroenterologists can achieve significantimprovements in both accuracy for polyp histology characterization andproportion of high confidence diagnosis following a brief computer basedtraining. Performance post training approached that of experts but further clinicalexperience may be required to surmount the final part of the learning curvebefore widespread implementation can be contemplated.
Table 1.
Pre Test Post Test P value
Gp A SensitivitySpecificity Accuracy
83% 99% 89% 89% 100% 93% 0.2 1.0 0.17
Gp B Sensitivity SpecificityAccuracy
54% 83% 64% 79% 84% 81% �0.001 1.0 �0.001
Gp C Sensitivity SpecificityAccuracy
58% 76% 64% 75% 90% 81% 0.004 0.042 �0.001
Table 2.
Post Test
Diagnosismade with
Lowconfidence
Diagnosismade with
Highconfidence P value
Gp A SensitivitySpecificity Accuracy
60% 100% 66% 96% 100% 98% �0.001 NS �0.001
Gp B Sensitivity SpecificityAccuracy
76% 60% 70% 79% 98% 85% 0.81 �0.001 0.013
Gp C Sensitivity SpecificityAccuracy
61% 86% 67% 83% 91% 86% 0.009 0.62 0.003
574A Comparison of Technical Success and Complications ofOvertube-Assisted ERCP vs. Laparoscopy-Assisted ERCP in Roux-en-Y Gastric Bypass Patients With Pancreaticobiliary DiseasesMaximiliano J. Smolkin*1, Roy D. Yen1, Leonard W. Faulk2,Jonathan A. Schoen2, Brian C. Brauer1, Brett E. Fortune1, Raj J. Shah1
1Gastroenterology, University of Colorado Hospital, Aurora, CO;2Surgery, University of Colorado Hospital, Aurora, COBackground: Limited comparative data exists for overtube-assisted small bowelenteroscopy ERCP (SBE-ERCP) with laparoscopy-assisted ERCP (LA-ERCP) inRoux-en-Y Gastric Bypass patients (RYGBP). Although technical success ishigher with the LA-ERCP approach, it is mostly unknown which algorithm ofindex SBE-ERCP or LA-ERCP is more cost-effective or associated with fewercomplications. The disadvantages of LA-ERCP are the logistics of a surgeon andendoscopist, use of post-op G-tubes susceptible to infection, and conversion toopen gastric remnant access. Aim: Compare the technical success andcomplications of SBE-ERCP vs. LA-ERCP. Methods: Consecutive patients wereretrospectively identified from prospectively maintained GI and surgerydatabases. Definitions: Technical Success -Completion of the intended
intervention by SBE-ERCP or LA-ERCP; Clinical Improvement: abdominal pain,LFT’s, or bilirubin decline � 50%. Comparison between SBE-ERCP and LA-ERCPwas done for Technical Success and Clinical Improvement. Cost analysesincluded provider/facility average medicare reimbursement for: ERCP, Lap- oropen G-tube, office/hospital days. To determine a cost-effective strategy, patientswere divided into index SBE-ERCP vs. LA-ERCP. SPSS Stats. Results: From 11/06 -10/11, 33 RYGBP (31F, median age 44) underwent SBE-ERCP (N�23) or LA-ERCP (N�10). Prior non SBE-ERCP attempts in 11/33 (33%). Indications:Presumed SOD Type 1 (N�14) or Type 2 (N�11); jaundice (N�3); other (5).Technical Success: 14/23 (61%) in the SBE-ERCP group and 10/10 (100%) in theLA-ERCP group (p�0.007). SBE-ERCP complications (N�4, 17%): Pancreatitis(N�1), Bleeding (N�2), perforation (N�1). LA-ERCP complications (N�3, 30%):gastric outlet obstruction (N�1), enterotomy of Roux limb (N�1), and bleeding(N�1). Follow-up obtained 21/23 (91%) for a median of 5 months (1-30). Threefailed SBE-ERCP went on to successful LA-ERCP. Clinical improvement in thosewith evaluable data was 48% (10/21) of the SBE-ERCP group and 46% (6/13) inthe LA-ERCP group (p�0.93). Hospitalization days in SBE-ERCP vs. LA-ERCP wasmedian 0 (0-42) and 3 (2-9) days, respectively (p� 0.0003); office visits postprocedure were median 0 (0-1) and 3 (0-5), respectively (p�.0001). Surgery:biliary bypass in the SBE-ERCP (N�2) and LA-ERCP (N�2), sphincteroplasty inLA-ERCP group (N�1). Median costs were lower for an index SBE-ERCP ($5174)vs LA-ERCP ($15,310) approach (p�0.002). Conclusion: 1) In our experience,technical success rate of LA-ERCP is 100%, however, hospitalization and officevisits are higher compared to SBE-ERCP. 2) An approach of index attempt atSBE-ERCP may be more cost-effective than index LA-ERCP. 3) Clinicalimprovement following either technique is low and case selection remainscritical.
575ERCP via Gastrostomy vs. Double Balloon Enteroscopy AssistedERCP in Patients With Prior Bariatric Roux-en-Y Gastric BypassSurgery: Single Center ExperienceEun Kwang Choi*, Glen A. Lehman, Michael V. Chiorean,Suzette E. Schmidt, Ihab I. El Hajj, Darren D. Ballard, Gregory A. Cote,Evan L. Fogel, James L. Watkins, Lee Mchenry, Stuart ShermanMedicine-GI, Indiana University Medical Center, Indianapolis, INBackground: The performance of ERCP in bariatric Roux-en-Y gastric bypass(RYGB) is challenging due to long roux limb. We herein describe indicationsand outcomes of gastrostomy-assisted ERCP (GERCP) and double balloonenteroscopy-assisted ERCP (DBERCP) for the patients with prior bariatric RYGBanatomy. Methods: Between Dec. 2005 and Nov. 2011, consecutive ERCPpatients who had undergone RYGB were identified using a prospectivelymaintained electronic ERCP database. Medical records were abstracted for ERCPindications and outcomes. The gastrostomy was done by either laparoscopic oropen surgery. In most cases, gastrostomy tract had been allowed to maturebefore performing ERCP. Results: Forty four patients (F�42) with GERCP and 28patients (F�26) with DBERCP were identified. The mean age was younger inGERCP than DBERCP (44.8 y vs. 56.1 y, p�0.001). The indications for GERCPwere suspected sphincter of Oddi dysfunction (SOD) in 34 (77%), recurrentpancreatitis in 8 (18%) and suspected common bile duct stone (CBDS) in 2 (5%).In DBERCP, the indications were suspected CBDS (16, 57%), suspected SOD (6,21%), suspected pancreatobiliary cancer (4, 15%) and post-cholecystectomy bileleak (2, 7%). The mean total number of sessions/patient in GERCP and DBERCPwas 1.7 and 1.1, respectively (p�0.002). The median time delay betweensurgical gastrostomy and ERCP was 42 days (range, 0-240). In all GERCP,endoscopic access to the major papilla, cannulation and therapeutic interventionswere successful (100%). Among all GERCP, 37 (84%) patients underwent biliaryand/or pancreatic manometry successfully and 41 (93%) patients had biliary and/or pancreatic sphincterotomy. Four patients with recurrent pancreatitis had minorpapilla sphincterotomy. In DBERCP, the success rate of accessing major papilla,cannulation (among successful papilla access), and therapeutic intervention(among successful cannulation) was 82%, 78%, 89%, respectively. The mostcommon treatment was biliary sphincterotomy (17 cases). There were no short-term complications in DBERCP cases. Complications occurred in 9 (21%) patientsin GERCP, and all were associated with gastrostomy or G-tube problems asfollows: infection (4), spontaneous dislodgement (2), gastrostomy track leak (1),gastrostomy site bleeding (1), persisting gastrocutaneous fistula (1). A secondoperation (G-tube replacement, gastric remnant closure, fistula repair) wasrequired in 3 patients. Conclusions: GERCP is a more effective route thanDBERCP to gain access to the pancreatobiliary tree in patients with RYGB, but ishindered by the gastrostomy maturation delay and a higher morbidity. DBERCPhad a reasonable success rate for managing biliary stone disease, but does notadequately address SOD and pancreatic diseases. Refinements in gastrostomycreation and maintenance are needed.
Abstracts
AB153 GASTROINTESTINAL ENDOSCOPY Volume 75, No. 4S : 2012 www.giejournal.org