Embed Size (px)
Citation preview

The International Journal of Periodontics & Restorative Dentistry
McGuire.qxd 5/30/06 4:07 PM Page 222

Recombinant human platelet-derivedgrowth factor-BB (rhPDGF-BB) is a well-characterized tissue growth factor thathas been shown, in animals andhumans, to be mitogenic and chemo-tactic for periodontal ligament andbone cells, with the additional effect ofpromoting regeneration of bone, lig-ament, and cementum.1–16 An initialhuman clinical trial showed that appli-cation of 0.15 mg/mL of rhPDGF-BBand 0.15 mg/mL recombinant humaninsulin-like growth factor I resulted in asignificant improvement in bone fill inperiodontal defects compared to con-ventional surgery plus a vehicle con-trol.17 Additionally, results of a pilothuman trial indicated that applicationof 0.5 to 1.0 mg/mL rhPDGF-BB inallograft resulted in regeneration ofbone, ligament, and cementum, asdemonstrated by blinded histologicevaluation.2,18
A new therapeutic system usingpurified rhPDGF-BB in combinationwith a biocompatible, osteoconduc-tive, synthetic scaffold (beta-tricalciumphosphate [�-TCP]) has recently beenevaluated in a large-scale, prospective,blinded, randomized clinical trial for itsability to safely and effectively treat
rhPDGF-BB Promotes Healing ofPeriodontal Defects: 24-Month Clinicaland Radiographic Observations
Michael K. McGuire, DDS*/Richard T. Kao, DDS, PhD**Myron Nevins, DDS***/Samuel E. Lynch, DMD, DMSc****
A new therapeutic system using purified recombinant human platelet-derived growthfactor-BB (rhPDGF-BB) in combination with a biocompatible, osteoconductive, syntheticscaffold beta-tricalcium phosphate (�-TCP) has recently been shown in a large-scale,prospective, blinded, randomized clinical trial to safely and effectively treat advancedperiodontal osseous defects. A significant gain in clinical attachment level was observed3 months postsurgery for sites treated with 0.3 mg/mL rhPDGF-BB + �-TCP versus �-TCP + buffer (active control), with this trend continuing at 6 months postsurgery.Additionally, sites treated with 0.3 mg/mL rhPDGF-BB + �-TCP also had significantlygreater radiographic linear bone gain and percent defect fill at 6 months postsurgerythan sites that received bone substitute with buffer. Representative cases from the clini-cal trial were followed to assess their ability to maintain the initial effect of treatmentobserved at 6 months. At 18 or 24 months postsurgery, with the same clinical and radio-graphic measurement techniques used as were performed at the 6-month time point forthe clinical trial, these cases demonstrated maintenance of the clinical attachment levelfor all but one case, with all cases demonstrating substantial increases in linear bonegain and percent bone fill versus measurements obtained at 6 months postsurgery.Substantial radiographic changes in the appearance of the defect fill were observed forboth rhPDGF-BB treatment groups, consisting of increased radiopacity and bone tra-beculation, indicative of increased mineralization and maturation of the bone observed6 months postsurgery. (Int J Periodontics Restorative Dent 2006;26:223–231.)
*Private Practice, Houston, Texas.**Private Practice, Cupertino, California.
***Clinical Associate Professor of Periodontology, Harvard School of Dental Medicine,Boston, Massachusetts; Private Practice, Swampscott, Massachusetts.
****Clinical Professor, Vanderbilt University, Nashville, Tennessee; President, BioMimeticTherapeutics, Franklin, Tennessee.
Correspondence to: Dr Michael McGuire, 3400 S. Gessner, #102, Houston, Texas 77063;e-mail: [email protected].
223
Volume 26, Number 3, 2006
McGuire.qxd 5/30/06 4:07 PM Page 223

advanced periodontal osseousdefects.19 The purpose of this report isto present representative cases fromthe clinical trial for this new therapeu-tic system, for the period of enrollmentthrough 24 months posttreatment.Extensive clinical and radiographic doc-umentation, including clinical attach-ment level (CAL) measurements andradiographic percent bone fill (%BF) aswell as linear bone gain (LBG), are pre-sented for each case beyond the initialstudy period of 6 months to providelonger follow-up information relatedto maintenance of the initial results.
Method and materials
As reported earlier,19 in the 180-patientclinical trial designed to evaluate thisnew therapeutic system for the treat-ment of intrabony periodontal defects(≥ 4 mm) patients were randomlyplaced into one of three treatmentgroups: (1) �-TCP + 0.3 mg/mLrhPDGF-BB in buffer; (2) �-TCP + 1.0mg/mL rhPDGF-BB in buffer; and (3) �-TCP + buffer (active control). Safetydata were assessed by the frequencyand severity of adverse events.Effectiveness measurements includedCAL and gingival recession (GR), mea-sured clinically, as well as LBG and %BF,as assessed radiographically by an inde-pendent centralized radiology reviewcenter. All participants were maskedwith respect to treatment group.
Briefly, the results demonstrated asignificant gain in CAL at 3 months forgroup 1 compared to group 3 (3.8 ver-sus 3.3 mm; P = .032), with this trendcontinuing at 6 months, although thedifference was not statistically signifi-
cant (P = .11). Group 1 sites also hadsignificantly greater LBG (2.6 versus 0.9mm, respectively; P < .001) and %BF(57% versus 18% respectively; P < .001) than group 3 sites at 6 months.No serious adverse events were attrib-utable to any of the treatments.
This study demonstrated that theuse of rhPDGF-BB was safe and effec-tive in the treatment of osseous peri-odontal defects and that treatmentwith rhPDGF-BB stimulated a signifi-cant increase in the rate of CAL gain,reduced GR at 3 months postsurgery,and improved bone fill as compared toa TCP bone substitute at 6 months.
The ability to maintain the initialeffect of treatment observed at 6months was evaluated at 12 and 24months posttreatment using the sameclinical and radiographic measurementtechniques that were performed at the6-month time point. Representativepatients from the study are presented.
Results
Patient 1
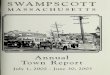
The patient, a 61-year-old nonsmokingHispanic woman, presented with radio-graphic evidence of bone loss on thedistal surface, as well as in the area ofthe furcation, of the mandibular leftfirst molar (Fig 1a). Clinical probingdepth (PD) and attachment levels of 8and 11 mm, respectively, wereobserved at baseline. The associatedbone defect measured 5 mm deepdistobuccally, 8 mm deep on the directdistal side, and 3 mm mesiodistally (Fig1b). Surgery was performed followingthe study protocol; this case was ran-
224
The International Journal of Periodontics & Restorative Dentistry
McGuire.qxd 5/30/06 4:07 PM Page 224

domized to receive 0.3 mg/mLrhPDGF-BB + �-TCP (Fig 1c).
At 6 months postsurgery, PD andCAL measurements were 3 and 6 mm,respectively, representing a 5-mmimprovement from baseline measure-ments. Increased radiopacity wasobserved on the distal surface of thetooth (Fig 1d), although the area ofthe furcation had not changed signifi-cantly from baseline. %BF on the dis-tal surface of the tooth was calculatedto be 81%, with an LBG of 5.11 mm.
At 12 months postsurgery, PDand CAL remained unchanged from
bone maturation (Fig 1f). These clinicaland radiographic observations werefurther supported by the calculated%BF of 89% and an LBG of 5.62 mm.
Patient 2
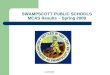
The patient, a 55-year-old Caucasianwoman and smoker for 40 years, pre-sented with radiographic evidence ofbone loss on the mesial surface of themandibular right first molar extendinginto the area of the furcation (Fig 2a).A clinical PD of 9 mm and CAL of 11
6 months postsurgery. Increasedradiopacity, with a distinct patternof trabeculation, was observed inthe area of the original defect onboth the distal surface of the root aswell as in the area of the furcation.The %BF was 94.3%, with an LBG of5.97 mm (Fig 1e).
At 24 months postsurgery, PD andCAL remained unchanged from 6months postsurgery. Radiographicbone fill continued to progress fromobservations made at 12 months, withincreased crestal cortication and a pat-tern of bony trabeculation, indicative of
225
Volume 26, Number 3, 2006
Fig 1a (left) Baseline periapical radi-ograph of patient #1 showing bone loss onthe distal surface of the mandibular left firstmolar (arrow) that extends into the area ofthe furcation.
Fig 1b (right) Intraoperative buccal viewof the circumferential intrabony defect.
Fig 1c (left) Intraoperative view of surgicalsite following placement of 0.3 mg/mLrhPDGF-BB + �-TCP.
Fig 1d (right) Bone fill distally and in thearea of the furcation at 6 months post-surgery. Arrow marks base of originaldefect.
Fig 1e (left) At 12 months, demonstrationof extensive bone fill distally and in the fur-cation of the mandibular left first molar.Bone trabeculation and a well-defined lami-na dura are evident. Arrow marks base oforiginal defect.
Fig 1f (right) Bone fill of the distal and fur-cal components of the original defect at 24months. Crestal cortication is evident, alongwith a distinct lamina dura along the distalroot surface. Arrow marks base of originaldefect.
McGuire.qxd 5/30/06 4:07 PM Page 225

mm were observed at baseline (Fig2b). During surgery, a 7-mm-deep by3-mm-wide (mesiodistally) two- andthree-walled intrabony defect on themesiolingual surface of the tooth wasrevealed. Surgery was performed fol-lowing the study protocol, with thiscase receiving 0.3 mg/mL rhPDGF-BB+ �-TCP.
At 3 months postsurgery, therewas increased radiopacity in the area ofthe original defect, although it was uni-form in appearance without any dis-cernible pattern of bony trabeculation(Fig 2c). At 6 months, PD and CAL were
3 and 5 mm, respectively. Increasedradiopacity was apparent in the area ofthe furcation as well as on the mesialsurface of the root, with isolated areasexhibiting a pattern of bony trabecu-lation not observed at 3 months (Fig2d). %BF on the mesial was calculatedto be 65%, with an LBG of 4.11 mm.
At 12 months, PD and CALremained unchanged from 6 months.Radiographic examination revealedincreased radiopacity in the area ofthe original defect, which was calcu-lated to be 75% BF with an LBG of 4.79mm (Fig 2e).
At 24 months, PD and CALremained unchanged. The 6-mmimprovement in CAL from baselinemeasurements was further supportedby radiographic findings, whichdemonstrated increased bone fill anda pattern of trabeculation indicative ofmature bone (Fig 2f). The area of thefurcation was totally radiopaque inappearance, indicating the presenceof mineralized tissue throughout thefurcation. These clinical and radio-graphic improvements were sup-ported by the calculated %BF of 99%and an LBG of 6.29 mm.
226
The International Journal of Periodontics & Restorative Dentistry
Fig 2a (left) Baseline periapical radio-graph of patient #2 showing bone loss onthe mesial root surface of the mandibularright first molar (arrow) that extends into thearea of the furcation.
Fig 2b (right) Baseline clinical measure-ment on the mesial surface of the mandibu-lar right first molar.
Fig 2c (left) Treated site at 3 months post-surgery showing diffuse, slightly radiopaquefill of the original mesial defect (arrow marksbase of original defect) and small residualradiolucency at the fornix of the furcation.
Fig 2d (right) At 6 months postsurgery,mesial bone fill has increased both in heightand density, with discrete areas of trabecu-lation present. Arrow marks base of originaldefect.
Fig 2e (left) Further bone fill of the origi-nal mesial defect at 12 months, with furthermaturation (trabeculation). Arrow marksbase of original defect.
Fig 2f (right) At 24 months, complete fillof the furcation and the area of the originalmesial defect. The bone fill is contiguouswith the surrounding bone. Arrow marksbase of original defect.
McGuire.qxd 5/30/06 4:07 PM Page 226

Patient 3
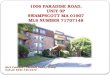
The patient, a 38-year-old nonsmokingCaucasian man, presented with radio-graphic evidence of bone loss on thedistal root surface of the mandibularright first molar that extended into thefurcation (Fig 3a). Baseline PD and CALof 13 mm were observed. Upon surgi-cal exposure, a 7-mm-deep by 4-mm-wide (mesiodistally) two- and three-walled intrabony defect was revealedon the distobuccal surface of the tooth.Surgery was performed following thestudy protocol, with this case receiving1.0 mg/mL rhPDGF-BB + �-TCP.
to be 64.2% with an LBG of 7.0 mm(Fig 3c).
At 24 months, radiographic evi-dence of bone fill continued toincrease from observations made at12 months, with increased radiopacityin the area of the original defect and apattern of bony trabeculation indica-tive of further bone maturation (Fig3d). PD and CAL remained unchangedfrom the 6- and 12-month measure-ments, with a significant improvementfrom baseline (Figs 3e and 3f). Theseclinical and radiographic improve-ments are supported by the calculated%BF of 77% and the LBG of 8.44 mm.
At 6 months postsurgery, PD andCAL were 4 mm, representing a 9-mmgain in CAL from baseline. Increasedradiopacity was demonstrated in thearea of the furcation as well as on thedistal surface of the tooth (Fig 3b). %BFwas calculated to be 46.2%, with anLBG of 4.98 mm.
At 12 months, progression andmaturation of bone fill continued inboth the furcation and the distaldefect, as evidenced by increasedradiopacity within the defect and apattern of bone trabeculation notpreviously observed. %BF on the dis-tal surface of the tooth was calculated
227
Volume 26, Number 3, 2006
Fig 3a (left) Baseline periapical radio-graph of patient #3 showing distal boneloss (arrow) on the mandibular right firstmolar extending into the area of the furca-tion.
Fig 3b (right) Six-month postsurgicalbone fill of the distal and furcal componentsof the original defect. Arrow marks base oforiginal defect.
Fig 3c (left) Further bone fill andincreased radiopacity (bone density) at 12months. Arrow marks base of originaldefect.
Fig 3d (right) At 24 months, the bone fillheight observed at 12 months has beenmaintained, with further increases in densityand maturity (trabeculation). The furcationappears to be completely filled with bone.Arrow marks base of original defect.
Figs 3e and 3f Clinical measurements(buccal view) (e, left) at baseline and (f,right) at 24 months postsurgery.
McGuire.qxd 5/30/06 4:07 PM Page 227

Patient 4
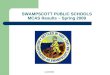
The patient, a 31-year-old nonsmokingAfrican American man, presented withradiographic evidence of bone loss onthe mesial surface of the mandibularright first molar, with incipient boneloss in the area of the furcation (Fig 4a).PD and CAL of 11 mm were observedat baseline. Upon surgical exposure, abone defect was revealed that mea-sured 10 mm deep mesiobuccally, 12mm deep on the direct mesial side,and 4 mm mesiodistally (Fig 4b).
Surgery was performed following thestudy protocol, with this case ran-domized to receive 0.3 mg/mLrhPDGF-BB + �-TCP (Fig 4c).
At 6 months postsurgery, PD andCAL were 4 mm, a 7-mm improve-ment from baseline. Increasedradiopacity was seen on the mesialsurface of the tooth, although theradiopacity lacked an organized, tra-becular bone pattern (Fig 4d). %BF inthe area of the original mesial defectwas calculated to be 93%, with an LBGof 5.36 mm.
At 18 months, PD and CAL mea-sured 3 and 6 mm, respectively, rep-resenting 8- and 5-mm improvementsfrom baseline measurements. Radio-graphic evidence of bone fill continuedto increase from observations madeat 6 months, with increased radiopac-ity in the area of the original defectand a pattern of bony trabeculationindicative of mature bone (Fig 4e).Radiographic LBG was 5.43 mm, for acalculated %BF of 88%.
228
The International Journal of Periodontics & Restorative Dentistry
Fig 4a (left) Baseline periapical radi-ograph of patient #4 demonstrating boneloss (arrow) on the mesial root surface of themandibular right first molar with incipientbone loss in the area of the furcation.
Fig 4b (right) Intraoperative lingual viewof the affected tooth showing a deep, wideintrabony defect on the mesial root surface.
Fig 4c (left) Intraoperative lingual view ofthe tooth following placement of 0.3mg/mL rhPDGF-BB + �-TCP.
Fig 4d (right) Diffuse, slightly radiopaquefill of the mesial defect at 6 months post-surgery. Arrow marks base of originaldefect.
Fig 4e At 18 months, the area of the fur-cation is completely filled, and the mesialdefect fill has increased both in height anddensity compared with 6-month measure-ments. Arrow marks base of original defect.
McGuire.qxd 5/30/06 4:07 PM Page 228

Table 1 Results of four cases treated with rhPDGF-BB + �-TCP
Time of evaluation
Baseline 6 months 12 months 24 months
Case/ PD CAL PD CAL LBG PD CAL LBG PD CAL LBGtreatment group (mm) (mm) (mm) (mm) (mm) %BF (mm) (mm) (mm) %BF (mm) (mm) (mm) %BF
1 (1.0 mg/mL 13 13 4 4 4.98 46 6 5 7.0 64 4 4 5.62 89rhPDGF-BB + �-TCP)2 (0.3 mg/mL 9 11 3 5 4.11 65 3 5 4.79 75 3 5 6.29 99rhPDGF-BB + �-TCP)3 (0.3 mg/mL 8 11 3 6 5.11 81 3 6 5.97 94 3 6 8.44 77rhPDGF-BB + �-TCP)4 (0.3 mg/mL 11 11 4 4 5.36 93 NA NA NA NA 3* 6* 6.72* 88*rhPDGF-BB + �-TCP)
*Measurements are from 21 months postsurgery, not 24 months.PD = probing depth; CAL = clinical attachment level; LBG = linear bone gain; %BF = % bone fill; NA = not available.
Discussion
This article presents the long-termresults of four representative casesfrom a large-scale, prospective,blinded, randomized clinical trialdesigned to evaluate a new therapeu-tic system using rhPDGF-BB in combi-nation with �-TCP for the treatment ofintrabony periodontal defects.
The initial report of results fromthe trial19 demonstrated that the use ofrhPDGF-BB was safe and effective inthe treatment of intrabony periodontaldefects and that rhPDGF-BB stimu-lated a significant increase in the rate
of CAL gain, reduced GR at 3 monthspostsurgery, and improved bone fill ascompared to the �-TCP bone substi-tute at 6 months.
The long-term results (12 and 21 or24 months postsurgery) of representa-tive cases from the trial illustrate main-tenance of the initial 6-month clinicalresults and substantial improvementof the 6-month radiographic results.
In both rhPDGF-BB treatmentgroups, the CAL measurements weremaintained in most cases, and all casesdemonstrated an increase in radio-graphic %BF and LBG measurements(Table 1).
229
Volume 26, Number 3, 2006
McGuire.qxd 5/30/06 4:07 PM Page 229

Important observations related tothe radiographic results for all rhPDGF-BB cases were also noted. For theperiod between 6 and 12 months (or21 months for patient #4), there werenotable changes in the appearance ofthe defect fill. In addition to increasedradiopacity of the defect fill, a bony tra-becular pattern became more evident,indicative of the bone maturationprocess during which host bone con-tinues to be deposited and mineralizedand the synthetic bone matrix isreplaced. This pattern continuedthroughout the remaining 9- to 12-month observation period, with a“blending” of the defect fill and bonesurrounding the original defect. Thisfinding is important because it pro-vides surgeons with important infor-mation related to expectations at var-ious time points following surgicaltreatment using the new therapeuticsystem.
The current case series illustratesthat gains in CAL following treatmentwith rhPDGF-BB + �-TCP are stable,and radiographic %BF and LBG maybe expected to increase substantiallyfollowing the initial 6-month postsur-gical observation.
References
1. Nevins ML, Camelo M, Nevins M, SchenkRK, Lynch SE. Periodontal regeneration inhumans using recombinant humanplatelet-derived growth factor-BB(rhPDGF-BB) and allogeneic bone. JPeriodontol 2003;74:1282–1292.
2. Camelo M, Nevins, ML, Schenk RK, et al.Periodontal regeneration can be achievedin human class II furcations using purifiedrecombinant human platelet-derivedgrowth factor BB (rhPDGF-BB) with boneallograft. Int J Periodontics RestorativeDent 2003;23:213–225.
3. Howell TH, Fiorellini JP, Paquette DW, etal. A phase I/II clinical trial to evaluate acombination of recombinant humanplatelet-derived growth factor-BB andrecombinant human insulin-like growth fac-tor-I in subjects with periodontal disease.J Periodontol 1997;68:1186–1193.
4. Wang HL, Pappert T, Castelli W, et al. Theeffect of platelet-derived growth factor onthe cellular response of the periodontium:An autoradiographic study in dogs. JPeriodontol 1994;65:429–436.
5. Lynch SE, Williams RC, Polson AM, et al. Acombination of platelet-derived growthfactor and insulin-like growth factorenhances periodontal regeneration. J ClinPeriodontol 1989;16:545–554.
6. Lynch SE, Castilla GR, Williams RC, et al.The effect of short term application of acombination of platelet-derived andinsulin-like growth factors on periodontalwound healing. J Periodontol 1991;62:458–467.
7. Lynch SE. The role of growth factors inperiodontal repair and regeneration. In:Polson A (ed). Periodontal Regeneration:Current Status and Directions. Chicago:Quintessence, 1994:179–198.
8. Lynch SE. Introduction. In: Lynch SE,Genco RJ, Marx RE (eds). TissueEngineering: Applications in MaxillofacialSurgery and Periodontics. Chicago:Quintessence, 1999:xi–xviii.
230
The International Journal of Periodontics & Restorative Dentistry
McGuire.qxd 5/30/06 4:07 PM Page 230

9. Giannobile WV, Hernandez RA, FinkelmanRD, et al. Comparative effects of platelet-derived growth factor, insulin-like growthfactor, individually and in combination onperiodontal regeneration in Macaca fasci-cularis. J Periodontal Res 1996;31:301–312.
10. Park JB, Matsuura M, Han K-Y, et al.Periodontal regeneration in class III furca-tion defects of beagle dogs using guidedtissue regeneration therapy with platelet-derived growth factor. J Periodontol1995;66:462–477.
11. Cho MI, Lin WL, Genco RJ. Platelet-derived growth factor-modulated guidedtissue regeneration therapy. J Periodontol1995;66:522–530.
12. Rutherford RB, Niekrash CE, Kennedy JE,Charette MF. Platelet-derived and insulin-like growth factors stimulate regenerationof periodontal attachment in monkeys. JPeriodontal Res 1992;27:285–290.
13. Hsieh SC, Graves DT. Pulse application ofplatelet-derived growth factor enhancesformation of a mineralizing matrix whilecontinuous application is inhibitory. J CellBiochem 1998;69:169–180.
14. Yu X, Hsieh SC, Bao W, Graves DT.Temporal expression of PDGF receptorsand PDGF regulatory effects on osteoblas-tic cells in mineralizing cultures. Am JPhysiol 1997;272:C1709–C1716.
15. Matsuda N, Lin W, Kumar M, et al. Mito-genic, chemotactic and synthetic respons-es of rat periodontal ligament fibroblasticcells to polypeptide growth factors in vitro.J Periodontol 1992;63:515–525.
16. Anusaksathien O, Jin Q, Zhao M, Somer-man MJ, Giannobile WV. Effect of sus-tained delivery of PDGF or its antagonist(PDGF-1308) on tissue-engineered cemen-tum. J Periodontol 2004;75:429–440.
17. Howell TH, Fiorellini JP, Paquette DW,Offenbacher S, Giannobile WV, Lynch SE.A phase I/II clinical trial to evaluate a com-bination of recombinant human platelet-derived growth factor-BB and recombi-nant human insulin-I like growth factor-I inpatients with periodontal disease. JPeriodontol 1997;68:1186–1193.
18. Nevins ML, Camelo M, Nevins M, SchenkRK, Lynch SE. Periodontal regeneration inhumans using recombinant humanplatelet-derived growth factor-BB(rhPDGF-BB) and allogeneic bone. JPeriodontol 2003;74:1282–1292.
19. Nevins ML, Giannobile WV, McGuire MK,et al. Platelet-derived growth factor(rhPDGF-BB) stimulates bone fill and rateof attachment level gain: Results of a largemulticenter randomized controlled trial. JPeriodontol 2005 Dec;76:2205–2215.
231
Volume 26, Number 3, 2006
McGuire.qxd 5/30/06 4:07 PM Page 231