Embed Size (px)
Citation preview
1
Unit 3 ©2014 Barkley & Associates
Advanced PharmacologyCardiovascular Agents Part 2
Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANPPresident, Barkley & Associates
www.NPcourses.comand
Professor of NursingDirector of Nurse Practitioner ProgramsCalifornia State University, Los Angeles
Robert Fellin, PharmD, BCPSFaculty, Barkley & Associates
Pharmacist, Cedars‐Sinai Medical CenterLos Angeles, CA
Unit 3 ©2014 Barkley & Associates
Heart Failure Affects approximately 6 million Americans
6-10% of individuals aged > 65 years have heart failure
500,000 new cases diagnosed each year
Direct and indirect health care costs of HF in 2010 were estimated to be $39.2 billion
300,000 deaths per year in the United States
$500 million annually is spent on pharmacologic therapy
2
Unit 3 ©2014 Barkley & Associates
Clinical syndrome caused by the inability of the heart to pump sufficient blood to meet the metabolic demands of the body
Can result from reduced ventricular filling (diastolic dysfunction) and/or reduced myocardial contractility (systolic dysfunction)
Heart Failure
Unit 3 ©2014 Barkley & Associates
Compensatory Mechanisms in HF Cardiac “remodeling”
ventricular dilation
cardiac hypertrophy
SNS activation:
vasoconstriction
tachycardia
increased contractility
RAAS activation
Na & H2O retention
3
Unit 3 ©2014 Barkley & Associates
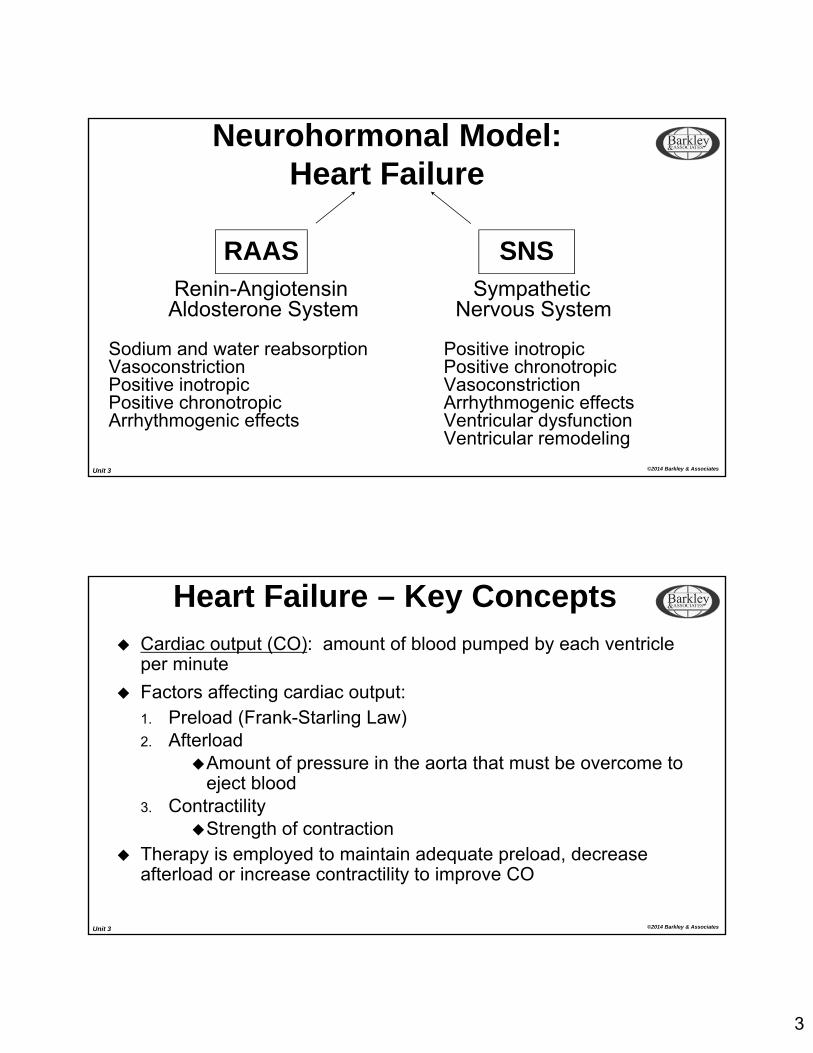
Neurohormonal Model:Heart Failure
Renin-Angiotensin SympatheticAldosterone System Nervous System
Sodium and water reabsorption Positive inotropicVasoconstriction Positive chronotropicPositive inotropic VasoconstrictionPositive chronotropic Arrhythmogenic effectsArrhythmogenic effects Ventricular dysfunction
Ventricular remodeling
RAAS SNS
Unit 3 ©2014 Barkley & Associates
Heart Failure – Key Concepts Cardiac output (CO): amount of blood pumped by each ventricle
per minute
Factors affecting cardiac output:1. Preload (Frank-Starling Law)2. Afterload
Amount of pressure in the aorta that must be overcome to eject blood
3. ContractilityStrength of contraction
Therapy is employed to maintain adequate preload, decreaseafterload or increase contractility to improve CO
4
Unit 3 ©2014 Barkley & Associates
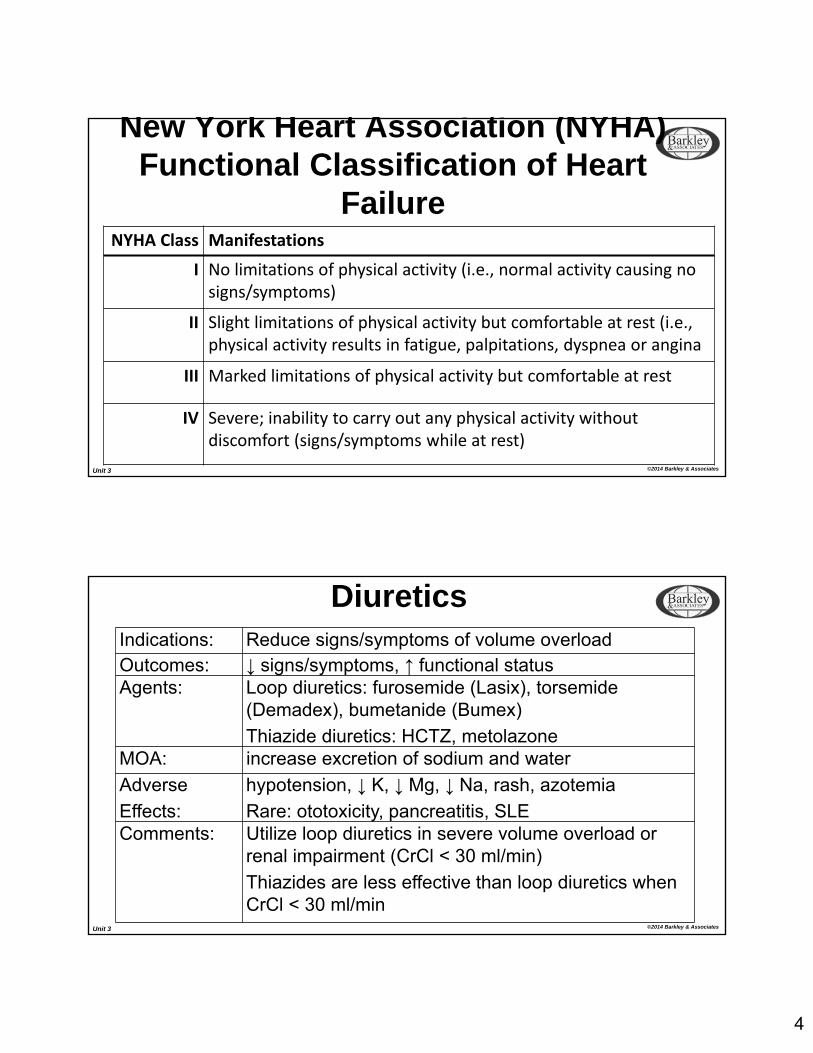
New York Heart Association (NYHA) Functional Classification of Heart
FailureNYHA Class Manifestations
I No limitations of physical activity (i.e., normal activity causing no signs/symptoms)
II Slight limitations of physical activity but comfortable at rest (i.e., physical activity results in fatigue, palpitations, dyspnea or angina
III Marked limitations of physical activity but comfortable at rest
IV Severe; inability to carry out any physical activity without discomfort (signs/symptoms while at rest)
Unit 3 ©2014 Barkley & Associates
DiureticsIndications: Reduce signs/symptoms of volume overloadOutcomes: ↓ signs/symptoms, ↑ functional statusAgents: Loop diuretics: furosemide (Lasix), torsemide
(Demadex), bumetanide (Bumex)
Thiazide diuretics: HCTZ, metolazoneMOA: increase excretion of sodium and water
Adverse
Effects:
hypotension, ↓ K, ↓ Mg, ↓ Na, rash, azotemia
Rare: ototoxicity, pancreatitis, SLEComments: Utilize loop diuretics in severe volume overload or
renal impairment (CrCl < 30 ml/min)
Thiazides are less effective than loop diuretics when CrCl < 30 ml/min
5
Unit 3 ©2014 Barkley & Associates
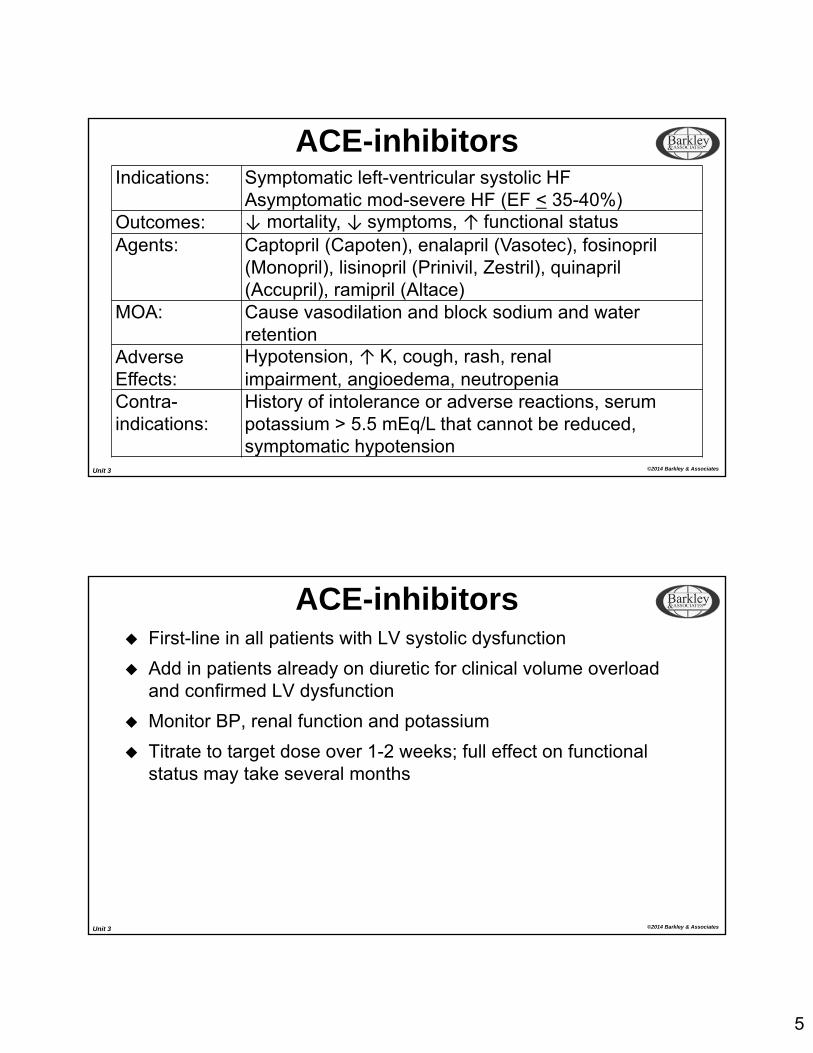
ACE-inhibitorsIndications: Symptomatic left-ventricular systolic HF
Asymptomatic mod-severe HF (EF < 35-40%)Outcomes: ↓ mortality, ↓ symptoms, ↑ functional statusAgents: Captopril (Capoten), enalapril (Vasotec), fosinopril
(Monopril), lisinopril (Prinivil, Zestril), quinapril (Accupril), ramipril (Altace)
MOA: Cause vasodilation and block sodium and water retention
AdverseEffects:
Hypotension, ↑ K, cough, rash, renal impairment, angioedema, neutropenia
Contra-indications:
History of intolerance or adverse reactions, serum potassium > 5.5 mEq/L that cannot be reduced, symptomatic hypotension
Unit 3 ©2014 Barkley & Associates
First-line in all patients with LV systolic dysfunction
Add in patients already on diuretic for clinical volume overload and confirmed LV dysfunction
Monitor BP, renal function and potassium
Titrate to target dose over 1-2 weeks; full effect on functional status may take several months
ACE-inhibitors
6
Unit 3 ©2014 Barkley & Associates
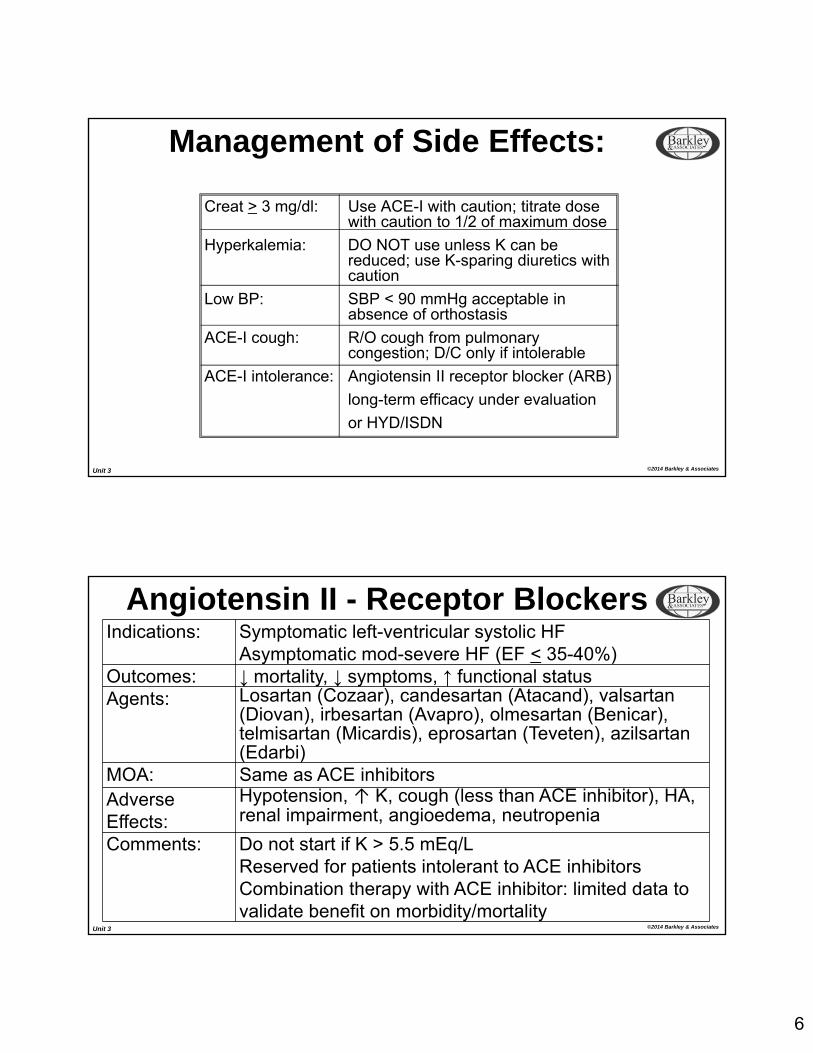
Management of Side Effects:
Creat > 3 mg/dl: Use ACE-I with caution; titrate dosewith caution to 1/2 of maximum dose
Hyperkalemia: DO NOT use unless K can bereduced; use K-sparing diuretics with caution
Low BP: SBP < 90 mmHg acceptable in absence of orthostasis
ACE-I cough: R/O cough from pulmonary congestion; D/C only if intolerable
ACE-I intolerance: Angiotensin II receptor blocker (ARB)
long-term efficacy under evaluation
or HYD/ISDN
Unit 3 ©2014 Barkley & Associates
Angiotensin II - Receptor BlockersIndications: Symptomatic left-ventricular systolic HF
Asymptomatic mod-severe HF (EF < 35-40%)Outcomes: ↓ mortality, ↓ symptoms, ↑ functional statusAgents: Losartan (Cozaar), candesartan (Atacand), valsartan
(Diovan), irbesartan (Avapro), olmesartan (Benicar), telmisartan (Micardis), eprosartan (Teveten), azilsartan(Edarbi)
MOA: Same as ACE inhibitorsAdverseEffects:
Hypotension, ↑ K, cough (less than ACE inhibitor), HA, renal impairment, angioedema, neutropenia
Comments: Do not start if K > 5.5 mEq/LReserved for patients intolerant to ACE inhibitorsCombination therapy with ACE inhibitor: limited data to validate benefit on morbidity/mortality
7
Unit 3 ©2014 Barkley & Associates
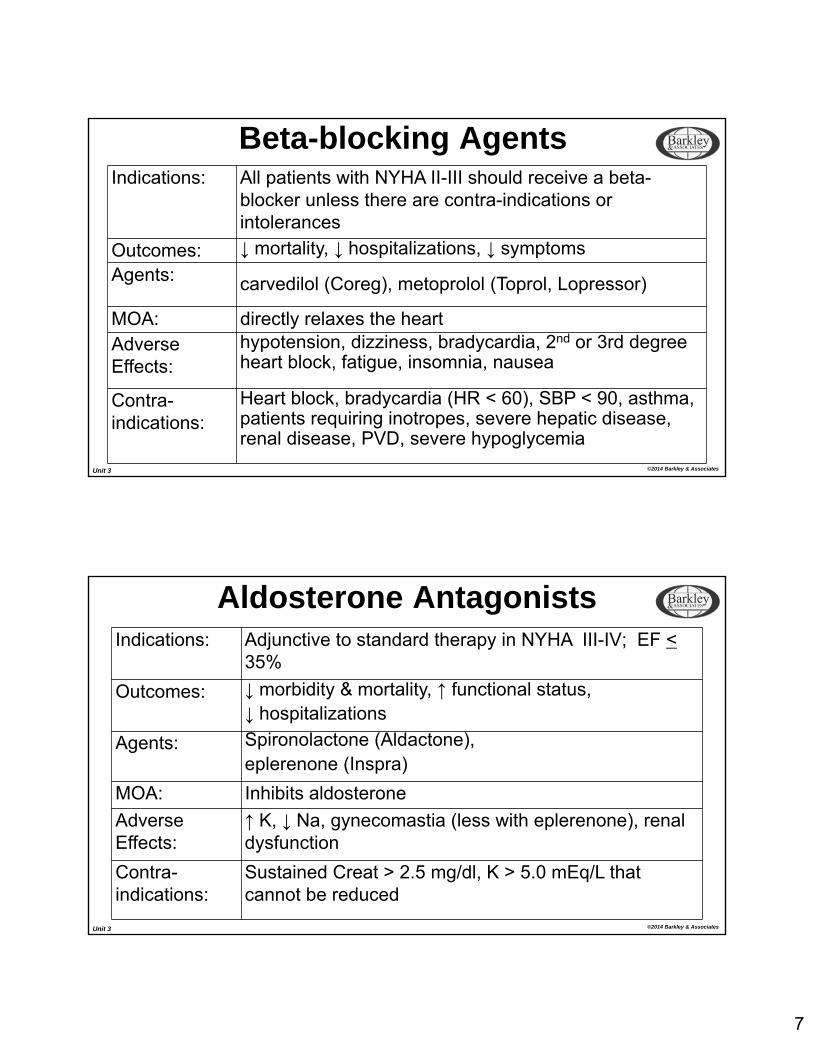
Indications: All patients with NYHA II-III should receive a beta-blocker unless there are contra-indications or intolerances
Outcomes: ↓ mortality, ↓ hospitalizations, ↓ symptoms
Agents: carvedilol (Coreg), metoprolol (Toprol, Lopressor)
MOA: directly relaxes the heartAdverseEffects:
hypotension, dizziness, bradycardia, 2nd or 3rd degree heart block, fatigue, insomnia, nausea
Contra-indications:
Heart block, bradycardia (HR < 60), SBP < 90, asthma, patients requiring inotropes, severe hepatic disease, renal disease, PVD, severe hypoglycemia
Beta-blocking Agents
Unit 3 ©2014 Barkley & Associates
Aldosterone AntagonistsIndications: Adjunctive to standard therapy in NYHA III-IV; EF <
35%
Outcomes: ↓ morbidity & mortality, ↑ functional status,↓ hospitalizations
Agents: Spironolactone (Aldactone),eplerenone (Inspra)
MOA: Inhibits aldosterone
AdverseEffects:
↑ K, ↓ Na, gynecomastia (less with eplerenone), renal dysfunction
Contra-indications:
Sustained Creat > 2.5 mg/dl, K > 5.0 mEq/L that cannot be reduced
8
Unit 3 ©2014 Barkley & Associates
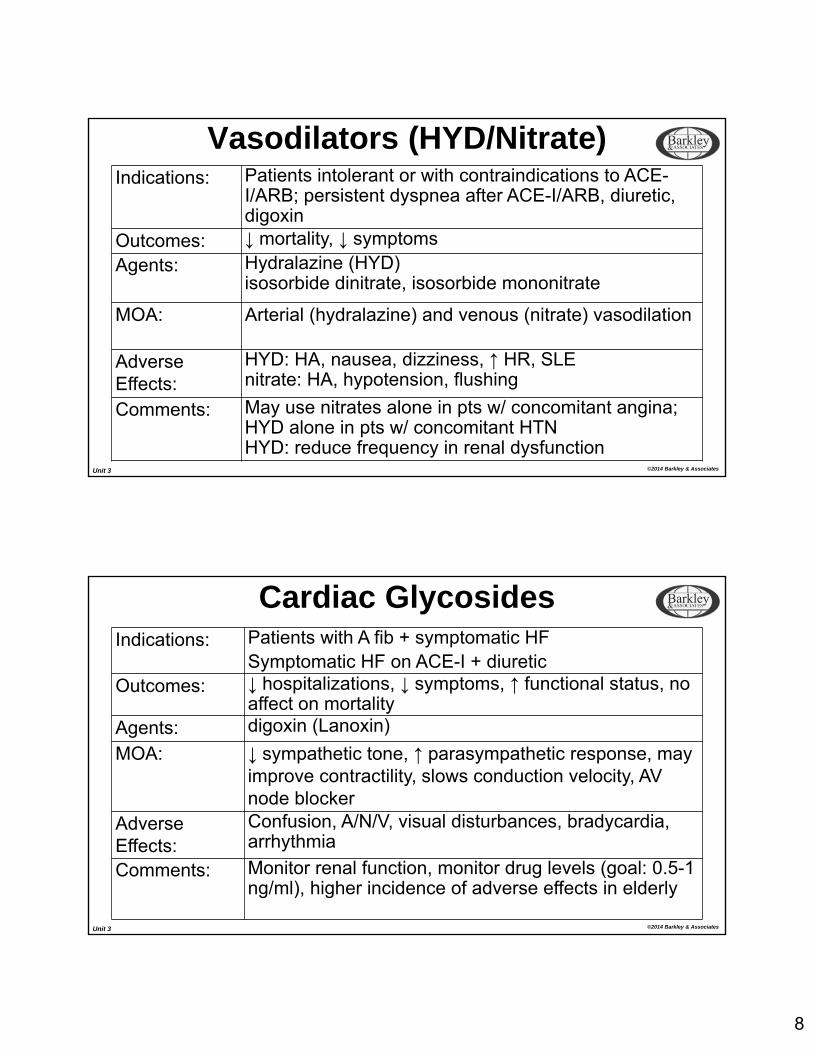
Vasodilators (HYD/Nitrate)Indications: Patients intolerant or with contraindications to ACE-
I/ARB; persistent dyspnea after ACE-I/ARB, diuretic, digoxin
Outcomes: ↓ mortality, ↓ symptoms
Agents: Hydralazine (HYD)isosorbide dinitrate, isosorbide mononitrate
MOA: Arterial (hydralazine) and venous (nitrate) vasodilation
AdverseEffects:
HYD: HA, nausea, dizziness, ↑ HR, SLEnitrate: HA, hypotension, flushing
Comments: May use nitrates alone in pts w/ concomitant angina; HYD alone in pts w/ concomitant HTNHYD: reduce frequency in renal dysfunction
Unit 3 ©2014 Barkley & Associates
Cardiac GlycosidesIndications: Patients with A fib + symptomatic HF
Symptomatic HF on ACE-I + diureticOutcomes: ↓ hospitalizations, ↓ symptoms, ↑ functional status, no
affect on mortalityAgents: digoxin (Lanoxin)
MOA: ↓ sympathetic tone, ↑ parasympathetic response, mayimprove contractility, slows conduction velocity, AV node blocker
AdverseEffects:
Confusion, A/N/V, visual disturbances, bradycardia, arrhythmia
Comments: Monitor renal function, monitor drug levels (goal: 0.5-1 ng/ml), higher incidence of adverse effects in elderly
9
Unit 3 ©2014 Barkley & Associates
Digoxin (Lanoxin)Interactions:
Many drug/drug interactions…
Dig + diuretics = hypokalemia & increased risk of dysrhythmias
Dig + ACEIs, spironolactone or K+ supplements = hyperkalemia
Dig + beta blockers = additive bradycardia
Dig + Ca intravenously = ↑ of dysrhythmias
Dig may ↓ the absorption of antacids and anti-lipid meds
Dig + quinidine, verapamil, amiodarone or alprazolam will decrease distribution and excretion of digoxin resulting in toxicity
Erythromycin and tetracyclines may ↑ plasma digoxin concentrations
Dig + ginseng = increased risk for digoxin toxicity
Unit 3 ©2014 Barkley & Associates
Dihydropyridine CCB
Indications: HTN in the setting of CHF
Outcomes: ↓ symptoms, mortalityAgents: Amlodipine, felodipine
Dosage: Amlodipine: 2.5-5 dailyfelodipine: 5 mg daily
AdverseEffects:
Hypotension, peripheral edema, HA, dizziness, nausea, abdominal, pain palpitations
Comments: Do not appear to increase mortalityFew studies of CCB in HF show either no difference or an increase in mortality (non-dihydropyridines)
10
Unit 3 ©2014 Barkley & Associates
Inotropic Agents MOA: increase intracellular cAMP thereby increasing the rate and
extent of calcium influx during systole and enhancing contractility
Dobutamine and milrinone have emerged as the two most commonly administered inotropes
Dopamine should generally be avoided except in instances of severe hypotension and cardiogenic shock
“Renal dose” dopamine (1-3 mcg/kg/min) may not be safe or effective
Unit 3 ©2014 Barkley & Associates
Dobutamine b1, b2 and a1 activity
Initial dose: 2.5-5 mcg/kg/min
Higher doses may be required for patients on b-blockers
Adverse effects: arrhythmogenic, may potentiate hypokalemia, myocardial ischemia
Tolerance to hemodynamic effects has been reported after 72 hours of continuous infusion
Increased mortality
11
Unit 3 ©2014 Barkley & Associates
Milrinone Potent inotropic and vasodilating effects
Loading dose: 50 mcg/kg over 10 minutes f/b a continuous infusion of 0.125-0.75 mcg/kg/min
Adverse effects: arrhythmogenic, thrombocytopenia, myocardial ischemia
Reduce dose for significant renal impairment
Physiologic effects not antagonized by
b-blockade
Increased mortality
Unit 3 ©2014 Barkley & Associates
Intravenous Vasodilators Hydralazine
arterial vasodilator that acts as an impedance reducing agent and typically increases cardiac output
Nitroglycerin venodilator that acts as preload reducer by increasing venous
capacitance
Nitroprusside mixed vasodilators act on both resistance and capacitance
vessels
12
Unit 3 ©2014 Barkley & Associates
Nitroglycerin
Preferred agent for pre-load reduction
Little or no effect on after-load (SVR)
Initial dose: 5-10 mcg/min
Tolerance to hemodynamic effects may develop over 12-72 hours
Adverse effects: hypotension, tachycardia
Used in combination with inotropic agent
Agent of choice for heart failure patients with ischemic component
Unit 3 ©2014 Barkley & Associates
Nitroprusside Primarily utilized in patients with significantly elevated SVR
Initial dose: 0.1-0.25 mcg/kg/min
Tolerance to hemodynamic effects may develop
Adverse effects: hypotension, reflex tachycardia
Rebound phenomenon occurs if discontinued abruptly; taper slowly
Can cause cyanide/thiocyanate toxicity with doses > 3 mcg/kg/min for > 3 days and in patients with renal impairment
13
Unit 3 ©2014 Barkley & Associates
Nesiritide Restricted to patients with acute, symptomatic, decompensated
heart failure (NYHA Stage IV) with evidence of fluid overload
Dose: 2 mcg/kg f/b continuous infusion of 0.01mcg/kg/min
Adverse effects: hypotension
Use with caution when SBP < 90 mm Hg
No dosage adjustment necessary for renal dysfunction
Limited data on outcomes and use > 48 hours
Unit 3 ©2014 Barkley & Associates
Mechanical Circulatory Support Intra-aortic balloon pump (IABP)
Impella
Tandem Heart
Ventricular assist device (VAD)
LVAD
BiVAD
Total Artificial Heart (TAH)
14
Unit 3 ©2014 Barkley & Associates
Anginal Syndromes Although difficult to fully assess, the AHA estimated the prevalence
of angina is
9.8 million annually
CHD is the leading cause of death in the US
Direct and indirect costs associated with CHD are estimated to be $286 billion per year
Outcome (survival) is determined by the number of vessels obstructed
Unit 3 ©2014 Barkley & Associates
Anginal Syndromes
Presentation is variable
Physical Exam Findings
Elevated BP
Levine’s sign = “clinched fist” sign
Transient S4 and apical systolic murmur not uncommon
Classifications:
Chronic stable angina
Unstable angina
Vasospastic angina (Prinzmetal’s angina)
15
Unit 3 ©2014 Barkley & Associates
Angina: Labs/Diagnostics ECG may be normal
Down sloping ST segment
T wave peak or inversion
Exercise ECG
Pharmacologic stress
test
Serum lipid levels
Cardiac catheterization
Coronary angiography –definitive but not necessary to make the diagnosis
Unit 3 ©2014 Barkley & Associates
Angina: Management Risk factor modification
Pharmacologic Therapy
Nitrates
Beta-blockers
Calcium channel blockers
Adjunct therapy
ACE Inhibitors
Antiplatelet therapy
Anticoagulant therapy
16
Unit 3 ©2014 Barkley & Associates
Major Goals in Treating Angina
1. Slow heart rate
2. Dilate veins (decrease preload)
3. Decrease contractility
4. Decrease BP = Decrease afterload
Unit 3 ©2014 Barkley & Associates
NitratesAgents: Isosorbide dinitrate, isosorbide mononitrate,
nitroglycerinMOA: Reduces myocardial oxygen demand due to
venodilation of coronary vasculatureIndications: Acute attacks, unstable and chronic angina
Dosage: Isosorbide mononitrate: 30 mg PO dailySL NTG 0.4 mg q5minutes prn chest pain x3
AdverseEffects:
Postural hypotension, headache, flushing, tachycardia, nausea
Comments: Utilize intermittent dosing that allows a drug-free interval to avoid toleranceVarious formulations (IV, PO, SL, topical)
17
Unit 3 ©2014 Barkley & Associates
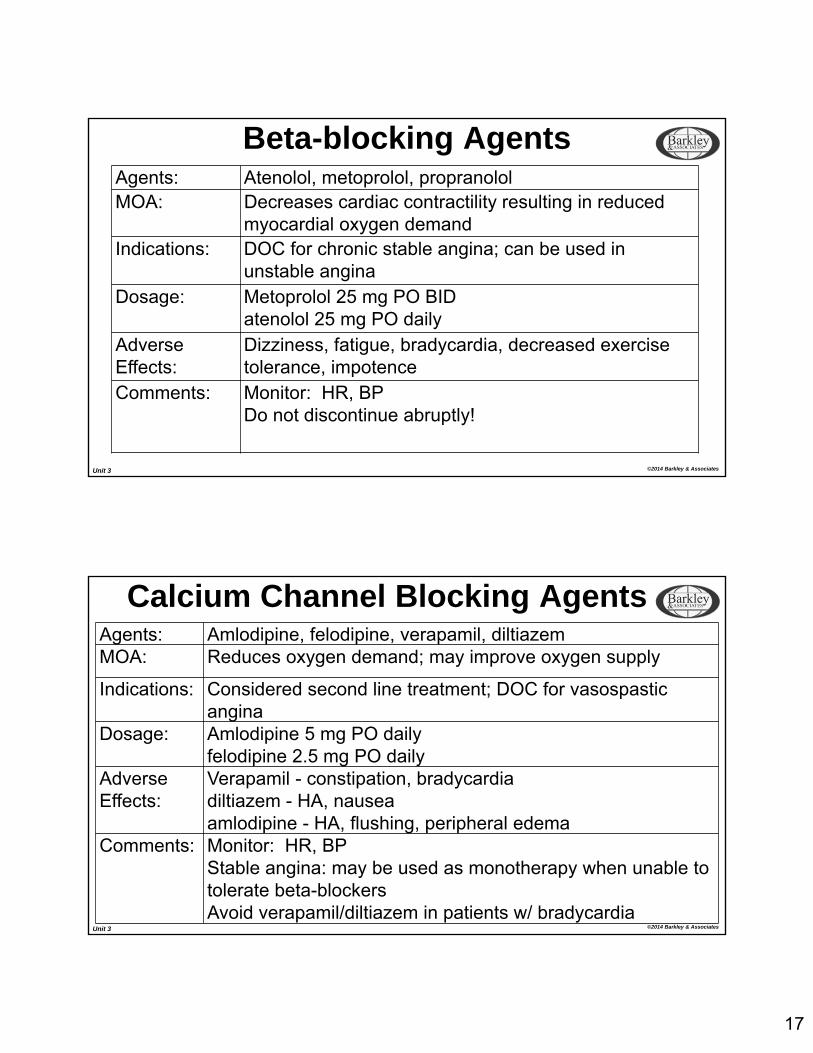
Beta-blocking AgentsAgents: Atenolol, metoprolol, propranololMOA: Decreases cardiac contractility resulting in reduced
myocardial oxygen demandIndications: DOC for chronic stable angina; can be used in
unstable anginaDosage: Metoprolol 25 mg PO BID
atenolol 25 mg PO dailyAdverseEffects:
Dizziness, fatigue, bradycardia, decreased exercise tolerance, impotence
Comments: Monitor: HR, BPDo not discontinue abruptly!
Unit 3 ©2014 Barkley & Associates
Calcium Channel Blocking AgentsAgents: Amlodipine, felodipine, verapamil, diltiazemMOA: Reduces oxygen demand; may improve oxygen supply
Indications: Considered second line treatment; DOC for vasospastic angina
Dosage: Amlodipine 5 mg PO dailyfelodipine 2.5 mg PO daily
AdverseEffects:
Verapamil - constipation, bradycardiadiltiazem - HA, nauseaamlodipine - HA, flushing, peripheral edema
Comments: Monitor: HR, BPStable angina: may be used as monotherapy when unable to tolerate beta-blockersAvoid verapamil/diltiazem in patients w/ bradycardia
18
Unit 3 ©2014 Barkley & Associates
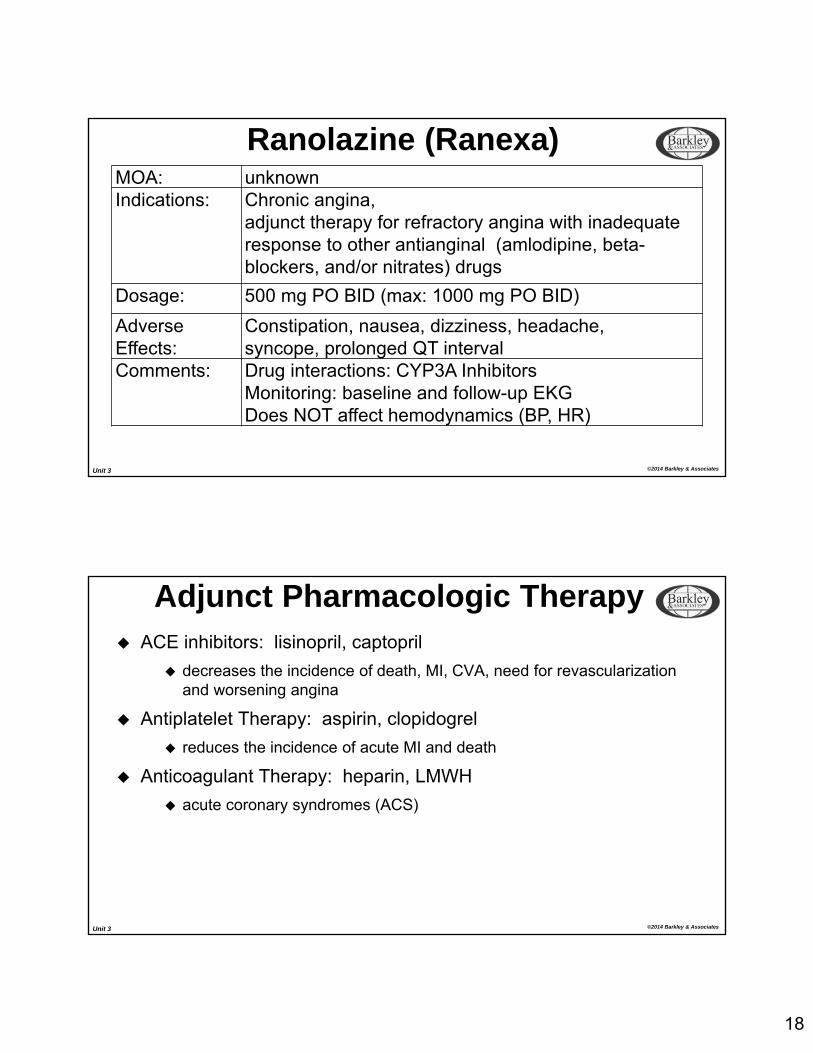
Ranolazine (Ranexa)MOA: unknownIndications: Chronic angina,
adjunct therapy for refractory angina with inadequate response to other antianginal (amlodipine, beta-blockers, and/or nitrates) drugs
Dosage: 500 mg PO BID (max: 1000 mg PO BID)
AdverseEffects:
Constipation, nausea, dizziness, headache,syncope, prolonged QT interval
Comments: Drug interactions: CYP3A InhibitorsMonitoring: baseline and follow-up EKGDoes NOT affect hemodynamics (BP, HR)
Unit 3 ©2014 Barkley & Associates
Adjunct Pharmacologic Therapy ACE inhibitors: lisinopril, captopril
decreases the incidence of death, MI, CVA, need for revascularization and worsening angina
Antiplatelet Therapy: aspirin, clopidogrel
reduces the incidence of acute MI and death
Anticoagulant Therapy: heparin, LMWH
acute coronary syndromes (ACS)
19
Unit 3 ©2014 Barkley & Associates
Drugs for Dysrhythmias
Unit 3 ©2014 Barkley & Associates
Drugs for Dysrhythmias Act by altering specific electrophysiological properties of the heart
Two basic mechanisms: Blocking flow through ion channels (conduction) Altering autonomic activity (automaticity)
Use has declined in recent years: use for prophylaxis may actually increase mortality Narrow therapeutic index May also worsen or create new dysrhythmias Less use of Class I agents, more use of classes II and III
(amiodarone) More use of catheter ablation and implantable defibrillators
20
Unit 3 ©2014 Barkley & Associates
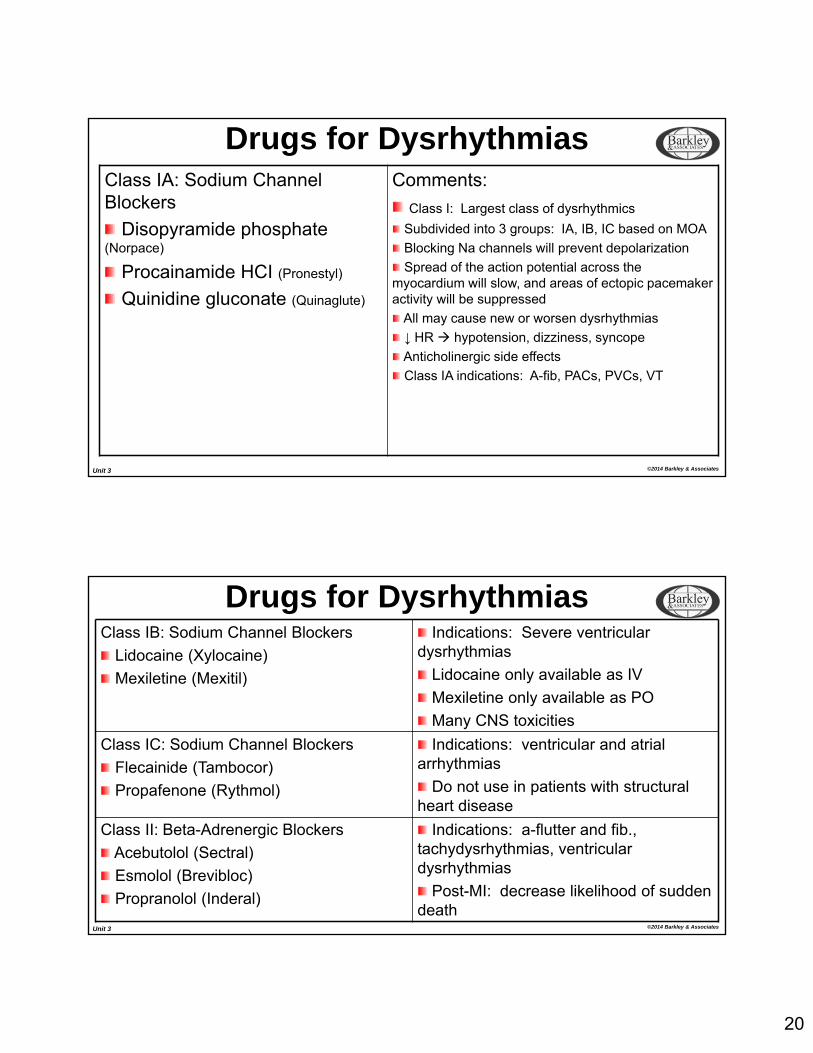
Class IA: Sodium Channel Blockers
Disopyramide phosphate (Norpace)
Procainamide HCI (Pronestyl)
Quinidine gluconate (Quinaglute)
Comments:
Class I: Largest class of dysrhythmics
Subdivided into 3 groups: IA, IB, IC based on MOA
Blocking Na channels will prevent depolarization
Spread of the action potential across the myocardium will slow, and areas of ectopic pacemaker activity will be suppressed
All may cause new or worsen dysrhythmias
↓ HR hypotension, dizziness, syncope
Anticholinergic side effects
Class IA indications: A-fib, PACs, PVCs, VT
Drugs for Dysrhythmias
Unit 3 ©2014 Barkley & Associates
Class IB: Sodium Channel Blockers
Lidocaine (Xylocaine)
Mexiletine (Mexitil)
Indications: Severe ventricular dysrhythmias
Lidocaine only available as IV
Mexiletine only available as PO
Many CNS toxicities
Class IC: Sodium Channel Blockers
Flecainide (Tambocor)
Propafenone (Rythmol)
Indications: ventricular and atrial arrhythmias
Do not use in patients with structural heart disease
Class II: Beta-Adrenergic Blockers
Acebutolol (Sectral)
Esmolol (Brevibloc)
Propranolol (Inderal)
Indications: a-flutter and fib., tachydysrhythmias, ventricular dysrhythmias
Post-MI: decrease likelihood of sudden death
Drugs for Dysrhythmias
21
Unit 3 ©2014 Barkley & Associates
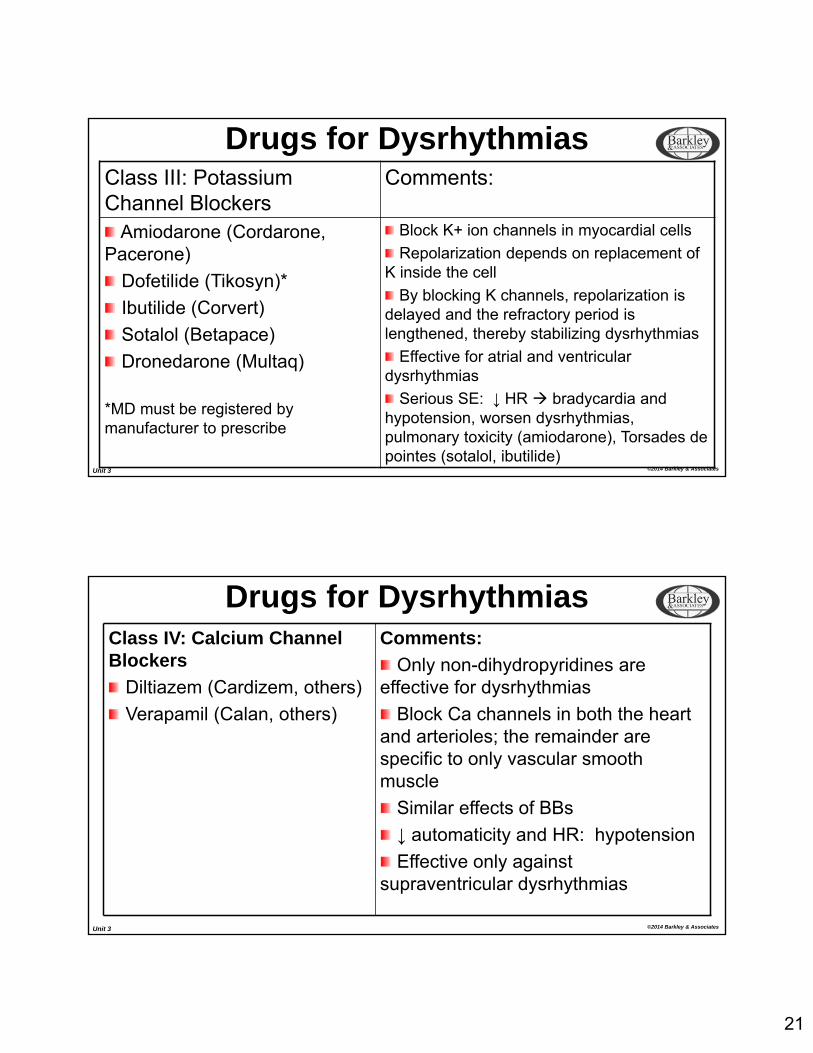
Class III: Potassium Channel Blockers
Comments:
Amiodarone (Cordarone, Pacerone)
Dofetilide (Tikosyn)*
Ibutilide (Corvert)
Sotalol (Betapace)
Dronedarone (Multaq)
*MD must be registered by manufacturer to prescribe
Block K+ ion channels in myocardial cells
Repolarization depends on replacement of K inside the cell
By blocking K channels, repolarization is delayed and the refractory period is lengthened, thereby stabilizing dysrhythmias
Effective for atrial and ventricular dysrhythmias
Serious SE: ↓ HR bradycardia and hypotension, worsen dysrhythmias, pulmonary toxicity (amiodarone), Torsades de pointes (sotalol, ibutilide)
Drugs for Dysrhythmias
Unit 3 ©2014 Barkley & Associates
Class IV: Calcium Channel Blockers
Diltiazem (Cardizem, others)
Verapamil (Calan, others)
Comments:
Only non-dihydropyridines are effective for dysrhythmias
Block Ca channels in both the heart and arterioles; the remainder are specific to only vascular smooth muscle
Similar effects of BBs
↓ automaticity and HR: hypotension
Effective only against supraventricular dysrhythmias
Drugs for Dysrhythmias
22
Unit 3 ©2014 Barkley & Associates
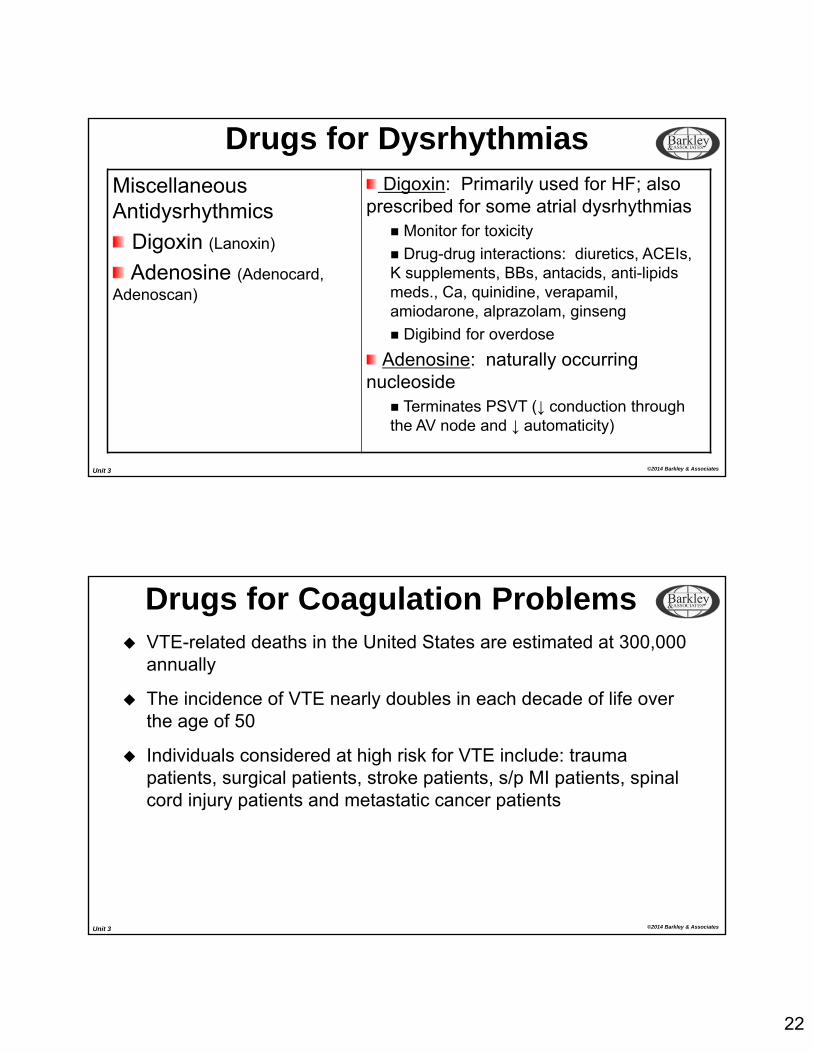
Miscellaneous Antidysrhythmics
Digoxin (Lanoxin)
Adenosine (Adenocard, Adenoscan)
Digoxin: Primarily used for HF; also prescribed for some atrial dysrhythmias
Monitor for toxicity
Drug-drug interactions: diuretics, ACEIs, K supplements, BBs, antacids, anti-lipids meds., Ca, quinidine, verapamil, amiodarone, alprazolam, ginseng
Digibind for overdose
Adenosine: naturally occurring nucleoside
Terminates PSVT (↓ conduction through the AV node and ↓ automaticity)
Drugs for Dysrhythmias
Unit 3 ©2014 Barkley & Associates
Drugs for Coagulation Problems VTE-related deaths in the United States are estimated at 300,000
annually
The incidence of VTE nearly doubles in each decade of life over the age of 50
Individuals considered at high risk for VTE include: trauma patients, surgical patients, stroke patients, s/p MI patients, spinal cord injury patients and metastatic cancer patients
23
Unit 3 ©2014 Barkley & Associates
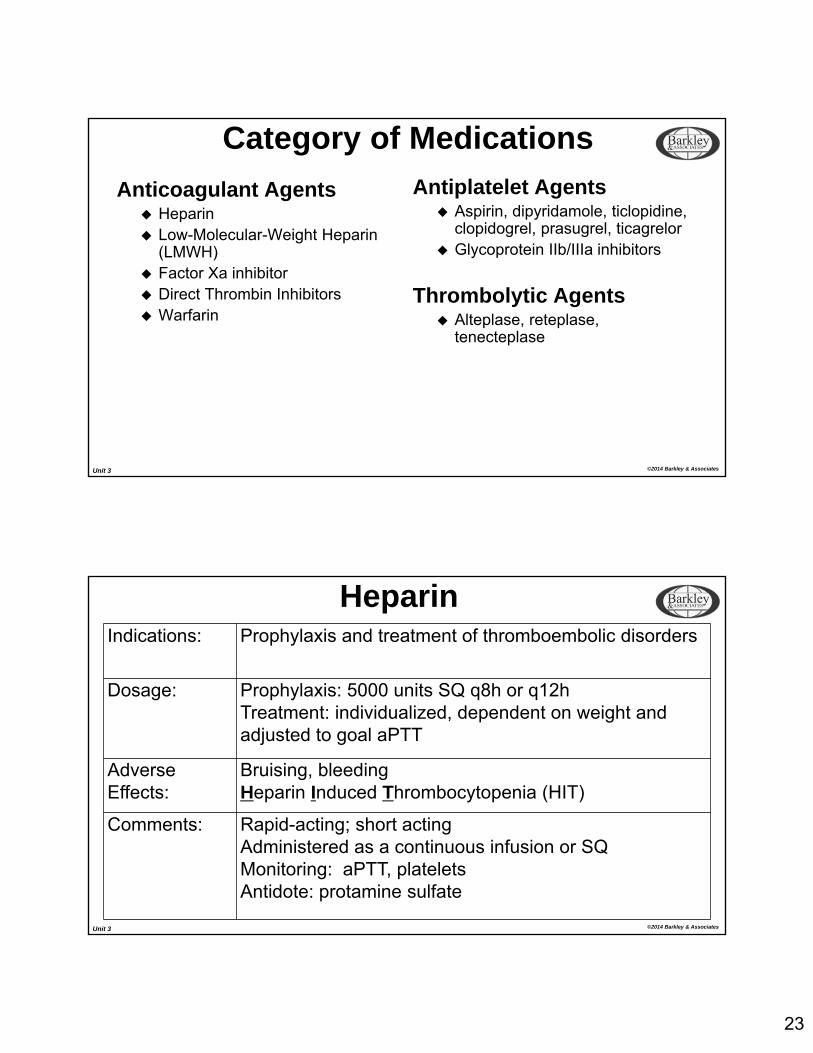
Category of Medications
Anticoagulant Agents Heparin Low-Molecular-Weight Heparin
(LMWH) Factor Xa inhibitor Direct Thrombin Inhibitors Warfarin
Antiplatelet Agents Aspirin, dipyridamole, ticlopidine,
clopidogrel, prasugrel, ticagrelor Glycoprotein IIb/IIIa inhibitors
Thrombolytic Agents Alteplase, reteplase,
tenecteplase
Unit 3 ©2014 Barkley & Associates
HeparinIndications: Prophylaxis and treatment of thromboembolic disorders
Dosage: Prophylaxis: 5000 units SQ q8h or q12hTreatment: individualized, dependent on weight and adjusted to goal aPTT
AdverseEffects:
Bruising, bleedingHeparin Induced Thrombocytopenia (HIT)
Comments: Rapid-acting; short actingAdministered as a continuous infusion or SQMonitoring: aPTT, plateletsAntidote: protamine sulfate
24
Unit 3 ©2014 Barkley & Associates
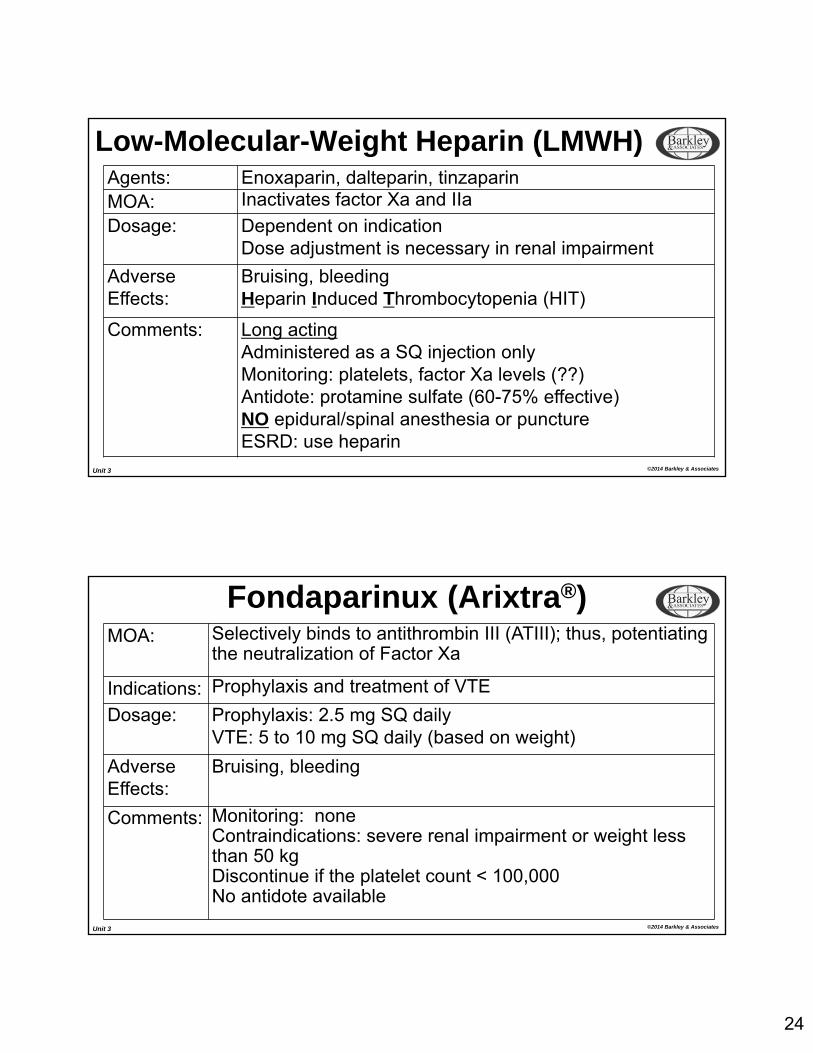
Low-Molecular-Weight Heparin (LMWH)Agents: Enoxaparin, dalteparin, tinzaparinMOA: Inactivates factor Xa and IIa
Dosage: Dependent on indicationDose adjustment is necessary in renal impairment
AdverseEffects:
Bruising, bleedingHeparin Induced Thrombocytopenia (HIT)
Comments: Long actingAdministered as a SQ injection onlyMonitoring: platelets, factor Xa levels (??)Antidote: protamine sulfate (60-75% effective)NO epidural/spinal anesthesia or punctureESRD: use heparin
Unit 3 ©2014 Barkley & Associates
Fondaparinux (Arixtra®)MOA: Selectively binds to antithrombin III (ATIII); thus, potentiating
the neutralization of Factor Xa
Indications: Prophylaxis and treatment of VTE
Dosage: Prophylaxis: 2.5 mg SQ dailyVTE: 5 to 10 mg SQ daily (based on weight)
AdverseEffects:
Bruising, bleeding
Comments: Monitoring: noneContraindications: severe renal impairment or weight less than 50 kgDiscontinue if the platelet count < 100,000No antidote available
25
Unit 3 ©2014 Barkley & Associates
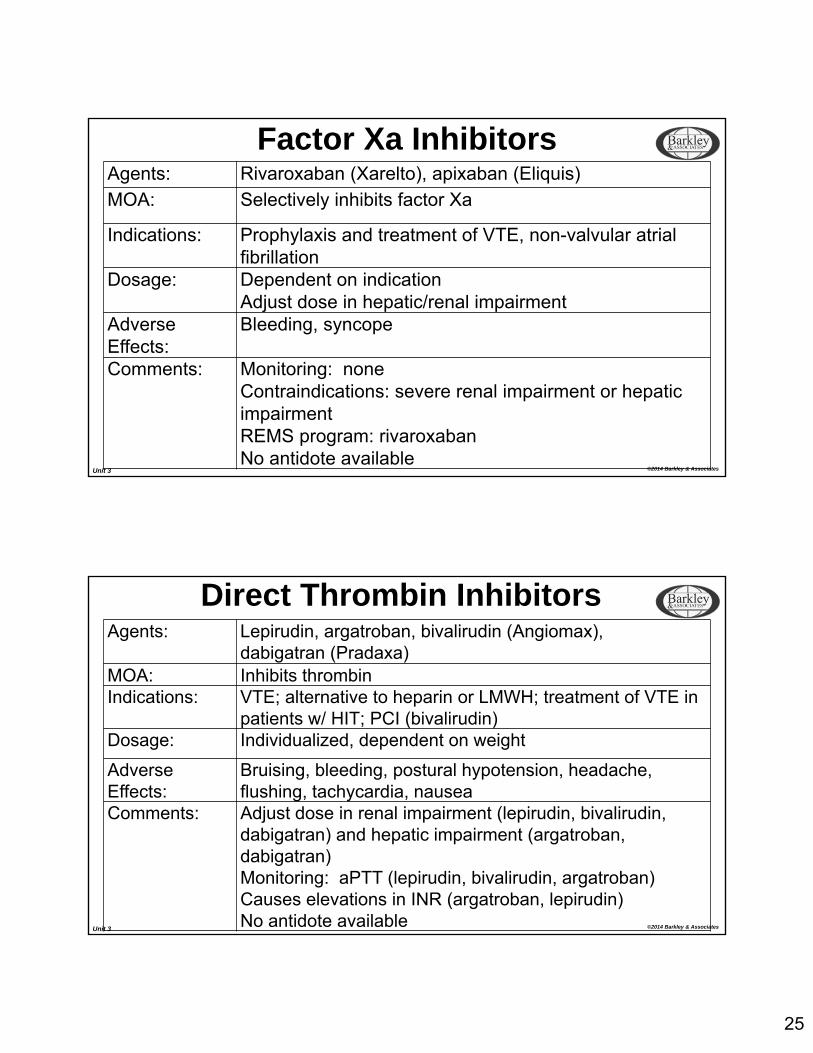
Factor Xa InhibitorsAgents: Rivaroxaban (Xarelto), apixaban (Eliquis)
MOA: Selectively inhibits factor Xa
Indications: Prophylaxis and treatment of VTE, non-valvular atrial fibrillation
Dosage: Dependent on indicationAdjust dose in hepatic/renal impairment
AdverseEffects:
Bleeding, syncope
Comments: Monitoring: noneContraindications: severe renal impairment or hepatic impairmentREMS program: rivaroxabanNo antidote available
Unit 3 ©2014 Barkley & Associates
Direct Thrombin InhibitorsAgents: Lepirudin, argatroban, bivalirudin (Angiomax),
dabigatran (Pradaxa)MOA: Inhibits thrombinIndications: VTE; alternative to heparin or LMWH; treatment of VTE in
patients w/ HIT; PCI (bivalirudin)Dosage: Individualized, dependent on weight
AdverseEffects:
Bruising, bleeding, postural hypotension, headache, flushing, tachycardia, nausea
Comments: Adjust dose in renal impairment (lepirudin, bivalirudin, dabigatran) and hepatic impairment (argatroban, dabigatran)Monitoring: aPTT (lepirudin, bivalirudin, argatroban)Causes elevations in INR (argatroban, lepirudin)No antidote available
26
Unit 3 ©2014 Barkley & Associates
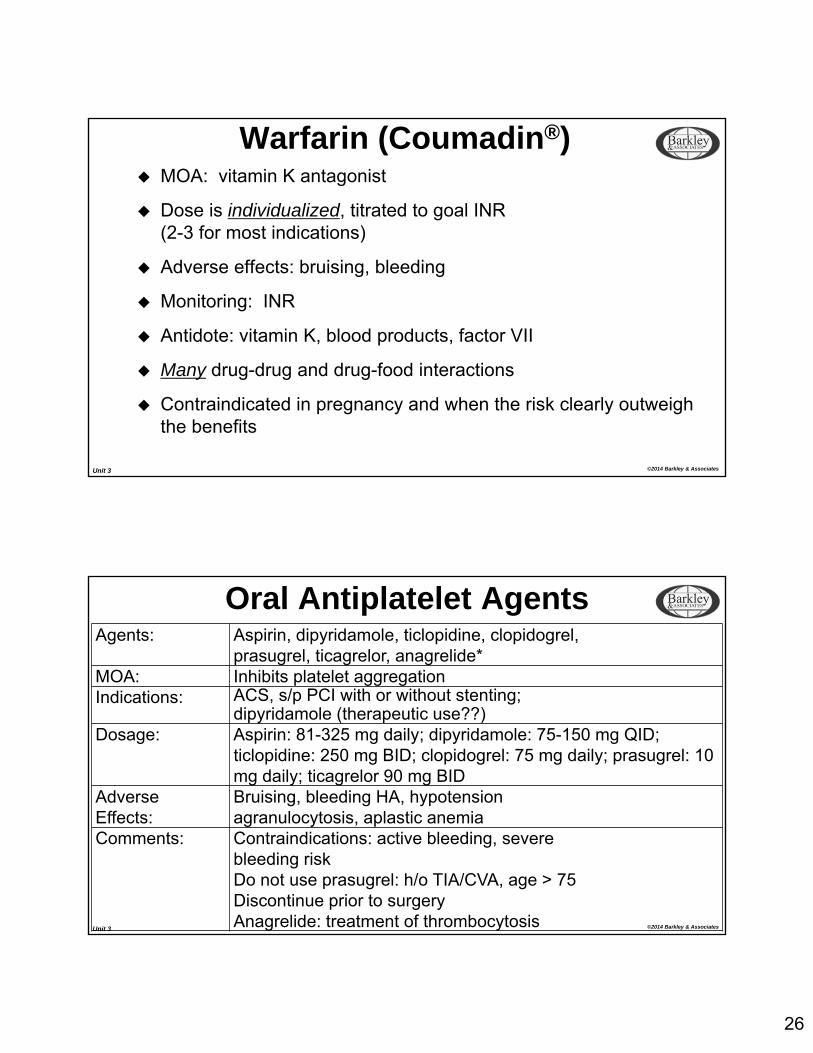
Warfarin (Coumadin®) MOA: vitamin K antagonist
Dose is individualized, titrated to goal INR(2-3 for most indications)
Adverse effects: bruising, bleeding
Monitoring: INR
Antidote: vitamin K, blood products, factor VII
Many drug-drug and drug-food interactions
Contraindicated in pregnancy and when the risk clearly outweigh the benefits
Unit 3 ©2014 Barkley & Associates
Oral Antiplatelet AgentsAgents: Aspirin, dipyridamole, ticlopidine, clopidogrel,
prasugrel, ticagrelor, anagrelide*MOA: Inhibits platelet aggregationIndications: ACS, s/p PCI with or without stenting;
dipyridamole (therapeutic use??)Dosage: Aspirin: 81-325 mg daily; dipyridamole: 75-150 mg QID;
ticlopidine: 250 mg BID; clopidogrel: 75 mg daily; prasugrel: 10 mg daily; ticagrelor 90 mg BID
AdverseEffects:
Bruising, bleeding HA, hypotensionagranulocytosis, aplastic anemia
Comments: Contraindications: active bleeding, severebleeding riskDo not use prasugrel: h/o TIA/CVA, age > 75Discontinue prior to surgeryAnagrelide: treatment of thrombocytosis
27
Unit 3 ©2014 Barkley & Associates
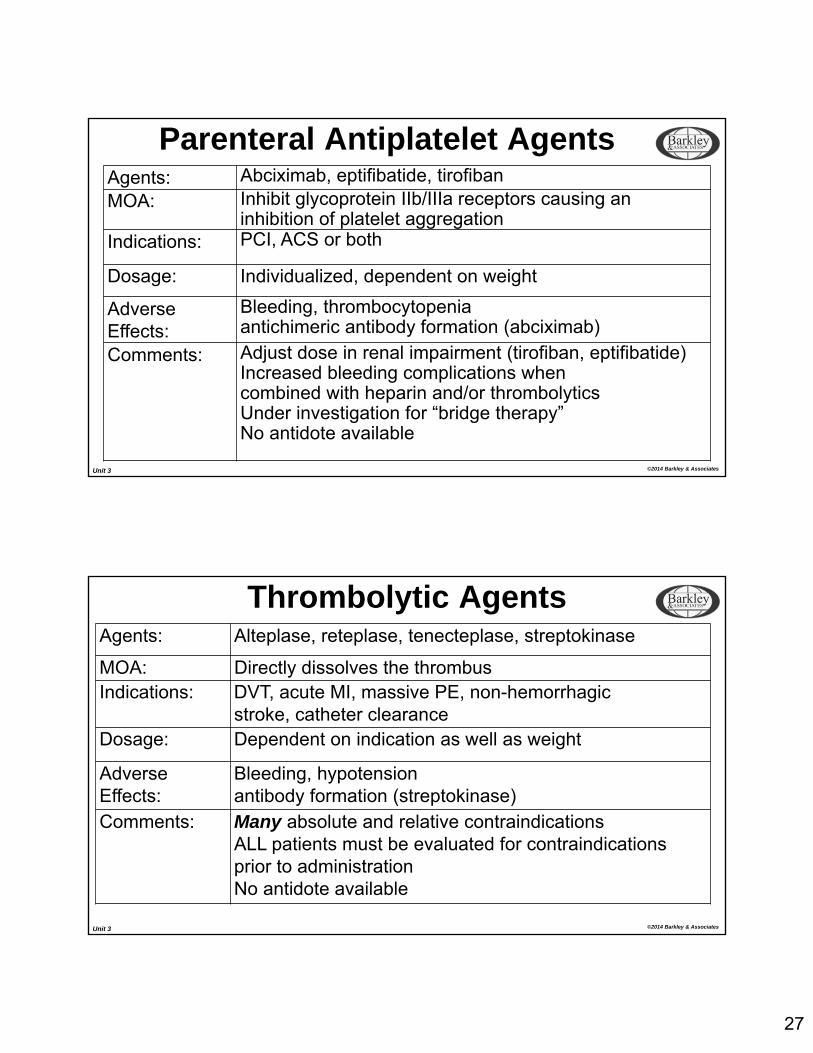
Parenteral Antiplatelet AgentsAgents: Abciximab, eptifibatide, tirofibanMOA: Inhibit glycoprotein IIb/IIIa receptors causing an
inhibition of platelet aggregationIndications: PCI, ACS or both
Dosage: Individualized, dependent on weight
AdverseEffects:
Bleeding, thrombocytopeniaantichimeric antibody formation (abciximab)
Comments: Adjust dose in renal impairment (tirofiban, eptifibatide)Increased bleeding complications whencombined with heparin and/or thrombolyticsUnder investigation for “bridge therapy”No antidote available
Unit 3 ©2014 Barkley & Associates
Thrombolytic AgentsAgents: Alteplase, reteplase, tenecteplase, streptokinase
MOA: Directly dissolves the thrombusIndications: DVT, acute MI, massive PE, non-hemorrhagic
stroke, catheter clearanceDosage: Dependent on indication as well as weight
AdverseEffects:
Bleeding, hypotensionantibody formation (streptokinase)
Comments: Many absolute and relative contraindicationsALL patients must be evaluated for contraindications prior to administrationNo antidote available
28
Unit 3 ©2014 Barkley & Associates
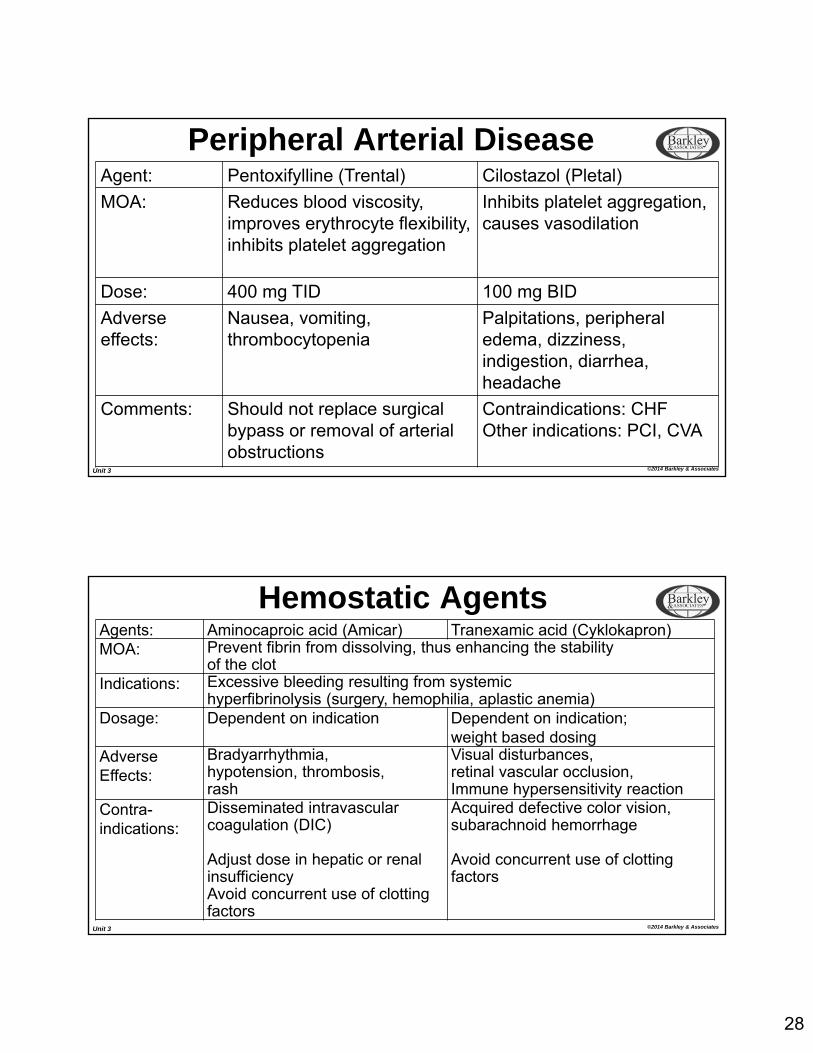
Peripheral Arterial DiseaseAgent: Pentoxifylline (Trental) Cilostazol (Pletal)
MOA: Reduces blood viscosity, improves erythrocyte flexibility, inhibits platelet aggregation
Inhibits platelet aggregation, causes vasodilation
Dose: 400 mg TID 100 mg BID
Adverse effects:
Nausea, vomiting, thrombocytopenia
Palpitations, peripheral edema, dizziness, indigestion, diarrhea, headache
Comments: Should not replace surgical bypass or removal of arterial obstructions
Contraindications: CHFOther indications: PCI, CVA
Unit 3 ©2014 Barkley & Associates
Hemostatic AgentsAgents: Aminocaproic acid (Amicar) Tranexamic acid (Cyklokapron)MOA: Prevent fibrin from dissolving, thus enhancing the stability
of the clotIndications: Excessive bleeding resulting from systemic
hyperfibrinolysis (surgery, hemophilia, aplastic anemia)Dosage: Dependent on indication Dependent on indication;
weight based dosingAdverseEffects:
Bradyarrhythmia,hypotension, thrombosis,rash
Visual disturbances,retinal vascular occlusion,Immune hypersensitivity reaction
Contra-indications:
Disseminated intravascular coagulation (DIC)
Adjust dose in hepatic or renal insufficiencyAvoid concurrent use of clotting factors
Acquired defective color vision, subarachnoid hemorrhage
Avoid concurrent use of clotting factors
29
Unit 3 ©2014 Barkley & Associates
The End

















