-
5/17/2013
1
Myelodysplastic Syndrome: a pathologist’s perspective
Kajal Sitwala, MD, PhD
MYELODYSPLASTIC SYNDROMES: Part 1 – Example MDS cases coming
into our practice over the last several weeks Part 2 – Review of
MDS definition, features, morphology, and biology
Case 1: -64 y.o. man with longstanding low back pain (unrelated)
-MRI showed abnormal bone marrow signal referred to Hematology -Had
normocytic anemia dating back 15 years -Bone marrow biopsy showed
fairly normal overall cellularity, but relative expansion in
erythropoiesis. Iron stain showed many ring sideroblasts -Diagnosis
of RARS (low-grade MDS) -Refractory Anemia with Ring Sideroblasts
-Interval treatment supportive (erythropoietin to boost RBC
production) -Follow-up bone marrow
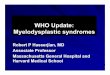
Dyserythropoiesis in aspirate smear
Ring sideroblasts (special stain of aspirate smear)
Hypercellularity; odd megakaryocytes, but not typical for MDS
-
5/17/2013
2
Diagnosis:
Persistent RARS -No increase in blasts -Frank dysplasia still
limited to the erythroid lineage -Cytogenetic analysis showed same
abnormality as before (+8) -Trisomy 8 can be seen in myeloid
disorders including MDS and AML -For RARS, it’s worse prognosis to
see it (versus normal karyotype) -Flow cytometry: main contribution
is confirming no increase in blasts -Mild aberrancy of CD56
co-expression on maturing granulocytes and monocytes -(supportive
finding, not enough to definitively diagnose MDS) -Recently,
MDS-RARS shown to have strong association with gene mutation:
-Haploinsufficiency of SF3B1
Case 2: -62 y.o. man with anemia and thrombocytopenia -Bone
marrow showed RAEB-1 (high-grade MDS) -Refractory Anemia with
Excess Blasts -Treatment/management course complicated by cold
agglutinin disease and transfusion refractoriness -Recently,
transfusion requirements became too severe to manage supportively,
hospitalized for aggressive chemotherapy -Bone marrow performed to
assess response
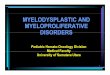
Peripheral blood: Granulocyte with mature, clumped chromatin but
lack of granulation or nuclear lobation (Pseudo-Pelger-Huet)
Increased blasts in aspirate smear
Hypercellular but loose marrow (fibrosis), Dysplastic
megakaryocytes
Diagnosis:
Persistent MDS, now best classified as RAEB-2 -In subsequent
bone marrows, I only reclassify MDS if worse -improvements are
described, but disease isn’t “downgraded” as a new MDS subtype -14%
blasts in differential count of aspirate smear -Reticulin stain
confirmed the presence of fibrosis -Historically normal karyotype
in leukemia cells; not repeated with this specimen -Flow cytometry
with 15% blasts, similar phenotype as prior cells -Patient given
even more aggressive treatment (AML induction), however, disease is
persisting
-
5/17/2013
3
Case 3: -83 y.o. woman with history of MDS dating back to 2008
-When seen here in 2010, classified as RCMD -Refractory Cytopenia
with Multilineage Dysplasia -2010 bone marrow with similar
cytogenetic abnormalities, still low-grade (no increase in blasts
-Since then, CBC counts have held pretty steady with lenolidamide
treatment -uniquely efficacious in cases involving chromosomal
deletions on 5q -Some concern with low hemoglobin values, so bone
marrow reassessed
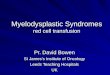
Basophilic stippling in peripheral blood
Dyserythropoiesis in aspirate smear Small and hypolobated
megakaryocytes in aspirate smear
Ring sideroblasts in aspirate smear
Diagnosis:
Persistent RCMD -Cytogenetics unchanged over past 5 years
-46,XX,del(5)(q13q33),add(11)(q23)[19]/46,XX[1] -doesn’t fit for
isolated 5q deletion (‘’5q-minus syndrome’’) but some features
overlap -often, dramatic worsening (e.g. increase in blasts)
corresponds with clonal evolution -Flow cytometry: increased
basophils, light scatter changes (but no aberrant phenotype) -No
increase in blasts -Later: discuss role of lenolidamide in 5q
deleted cases
-
5/17/2013
4
A group of clonal hematopoietic stem cell
diseases characterized by cytopenias,
dysplasia, ineffective hematopoiesis, and
increased risk of developing acute
myeloid leukemia.
-Principally a disease of older adults -Disorder of HSCs and
their microenvironment
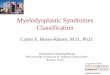
MDS 1953 – Knudson hypothesis: cancer results from accumulated
DNA mutations 1990’s – 2-hit model of leukemia
Adapted from WHO 2008
Class I mutations Class II mutations
FLT3-ITD FLT3-TKD
JAK2-V617F KIT mutations RAS mutations
PML-RARA AML1-ETO
CBF -MYH11 CEBPA mutations NPM1 mutations?
Proliferation advantage Survival advantage
Differentiation arrest clonogenicity
AML
General (simplified) model of myeloid malignancies
Proliferation advantage Survival advantage
Differentiation arrest clonogenicity
AML
Myeloproliferative disorders Myelodysplastic syndromes
CLASS I CLASS II
So MDS is a stem cell neoplasm: but what does “immortalization”
look like? Clonogenic, but not rapid, proliferation of stem cells
(There is also increased apoptosis) Inability to complete
differentiation and leave marrow Hallmark of MDS – peripheral blood
cytopenias PLUS bone marrow hypercellularity In contrast to MPDs…
Rapid proliferation but complete differentiation – cells accumulate
in both places (clinical presentation from tumor burden rather than
loss of function) Or acute leukemia… Proliferation and lack of
differentiation: blasts in bone marrow and blood
Programs of self-renewal and differentiation use some of the
same molecules (transcription factors)
-Clonogenicity: (Can’t see whether a cell will keep dividing or
not) -Hypercellularity
-Maturation arrest: (Marrow is full of precursors anyhow) -Skew
toward immaturity As Hematopathologists, what we SEE is morphologic
abnormalities that result From these molecular processes
Normal Erythroid Maturation (ASH image Bank)
-
5/17/2013
5
Normal Megakaryocyte making platelets (ASH image Bank)
Pictures of normal hematopoietic elements
A blood smear and a marrow, or just a single marrow picture
Normal Leukocytes in peripheral blood (ASH image Bank)
Predictions about dysplasia, based on concept of “maturation
arrest” – 1. immaturity of any kind a. cells that are more like a
precursor form b. failure to develop characteristics of final state
2. dyssynchrony between different elements/split personality as far
as further cell division 3. just plain weird
1a. Immaturity
Excess blasts Erythroid immaturity (increase in early forms)
Small megakaryocytes that have not divided the nucleus yet
Patient with RCMD (including 5q minus but with additional
abnormalities) Patient with RCMD (including 5q minus but with
additional abnormalities)
-
5/17/2013
6
Patient with RCMD (including 5q minus but with additional
abnormalities) Patient with RCMD (including 5q minus but with
additional abnormalities)
Patient with RAEB-1)
1b. Failure to finalize -lack of granulation in circulating
neutrophils -lack of nuclear lobation in circulating neutrophils
*mimic of harmless genetic state (Pelger-Huet anomaly)
Pseudo-Pelger Huet neutrophils with hypogranulation (ASH image
Bank)
2. Dyssynchrony, or confusion about further division
-Hemoglobinized cytoplasm with still immature nucleus -Nuclear
budding in erythroid precursors -Megakaryocytes with completely
separated nuclear lobes
-
5/17/2013
7
Patient with RAEB-1 Dysplastic erythroid precursor with
hemoglobinization and large nucleus (ASH image Bank)
Dysplastic megakaryocytes with separation of nuclear lobes (ASH
image Bank) Nuclear budding in erythroid precursor (ASH image
Bank)
Patient with RCMD (core biopsy touch imprints)
3. Just plain weird -Ring sideroblasts -Megaloblastoid chromatin
in erythroid precursors -Basophilic stippling in red blood cells
-Dimorphic circulating red cell population -Vacuoles (especially
erythroid precursors) *beware of MDS mimic – copper deficiency
(sometimes caused by zinc toxicity)
-
5/17/2013
8
Patient with RCMD (including 5q minus but with additional
abnormalities) Megaloblastoid chromatin (ASH image Bank)
Ring sideroblasts (ASH image Bank)
That “classification” was purely speculative, a tool to mentally
account for dysplasia Are there any cases where we have pinpointed
the connection between genes and dysplasia?
5q minus syndrome
Anemia – can be quite severe Normal to elevated platelet count;
characteristic megakaryocytes Hypercellular marrow, variable
erythroid dysplasia Female predominance – middle to older age
5q minus syndrome
1974 – Nature – clinical syndrome with chr 5 long arm deletion
reported 2001 – WHO classification recognizes 5q- as distinct
subtype of MDS 2002 – Blood – commonly deleted region narrowed to
40 genes by FISH/Southern 2007 – ASH plenary abstract –
identification of candidate gene no biallelic deletions or point
mutations in 40 genes – likely haploinsufficiency therefore
reduction in gene expression could be exploited: RNA interference
findings published: Ebert et al., Nature, January 2008 (Golub
laboratory – Harvard)
-
5/17/2013
9
Ebert et al., Nature, January 2008
Megakaryocyte:erythroid ratio using markers CD41, glycophorin
A
RPS14 participates in ribosomal synthesis RPS19 mutations found
in 25% Diamond-Blackfan Anemia cases
Haploinsufficiency of ribosomal proteins: Phenotype of
macrocytic anemia shows p53 dependence -Cell cycle arrest, failure
to complete erythroid differentiation -Interestingly, 5q minus
syndrome differs from other MDS by exhibiting erythroid hypoplasia
Studies in mice prove the genotype:phenotype correlation for anemia
Further research showed increased RPS14 levels after lenolidamide
therapy But, doesn’t answer the whole question…megs are normal in
those mice Also, DBA patients (RPS19) don’t have platelet or
megakaryocyte problems
From Identification of miR-145 and miR-146a as mediators of the
5q– syndrome phenotype; Daniel T Starczynowski, et al Nature
Medicine 16, 49–58 (2010) (obtained with permission)
microRNA: from non-coding parts of genome -regulate mRNA (coding
parts of genome) However, another gene on 5q-, in fact the genes
for two microRNAs, have
recently been shown to recapitulate the phenotype of small
megs….
From Identification of miR-145 and miR-146a as mediators of the
5q– syndrome phenotype; Daniel T Starczynowski, et al Nature
Medicine 16, 49–58 (2010) (obtained with permission)
Targets of these microRNAs are transcription factors (TiRAP,
TRAF6), and these in turn Regulate level of interleukin-6 Increased
IL-6 can recapitulate megakaryocyte phenotype Lenolidamide* reduces
IL-6 levels But wait…didn’t they think lenolidamide worked by
increasing RPS14 expression? But wait…there’s also the SPARC gene
on 5q-, necessary for mouse hematopoiesis, lenolidamide increases
its expression as well! *Thalidomide analog with many anti-cancer
mechanisms in vitro and in vivo Genotype:phenotype correlations are
real, but messy and redundant Hard to untangle, because of
complexity of hematologic pathway, evolved in parallel to general
embryogenic cascade
The genes used to regulate hematopoiesis are the same set of
genes that determine body patterning during embryogenesis!
Fro
m W
ikip
edia
http://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/fig_tab/nm.2054_F2.htmlhttp://www.nature.com/nm/journal/v16/n1/fig_tab/nm.2054_F2.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/full/nm.2054.htmlhttp://www.nature.com/nm/journal/v16/n1/fig_tab/nm.2054_F2.htmlhttp://www.nature.com/nm/journal/v16/n1/fig_tab/nm.2054_F2.html
-
5/17/2013
10
The genes used to regulate hematopoiesis are the same set of
genes that determine body patterning during embryogenesis! Human
genes: -Used once to make our body (in utero), then over and over
for the rest of our lives to make blood cells -HOXA9 is most
upregulated gene in AML -Potent mediator of leukemia
cluster chromosome genes
HOXA chromosome 7 HOXA1, HOXA2, HOXA3, HOXA4, HOXA5, HOXA6,
HOXA7, HOXA9, HOXA10, HOXA11, HOXA13
HOXB chromosome 17 HOXB1, HOXB2, HOXB3, HOXB4, HOXB5, HOXB6,
HOXB7, HOXB8, HOXB9, HOXB13
HOXC chromosome 12 HOXC4, HOXC5, HOXC6, HOXC8, HOXC9, HOXC10,
HOXC11, HOXC12, HOXC13
HOXD chromosome 2 HOXD1, HOXD3, HOXD4, HOXD8, HOXD9, HOXD10,
HOXD11, HOXD12, HOXD13
Control
Hoxa9
Meis1
0
2000
4000
6000
8000
10000
12000
0 2 4 6 8day
ce
lls x
10
00
0
- 4-OHT
+ 4-OHT+ -
>-8-fold no change >8-fold
Slc18a1 Sox4
Auts2 Flt3
Dnajc10 A930001M12
Cd34 Pctk2 Amot Tgm3 Cradd
Rora Foxp1
B4galt4 Man1a
Lmo2 5830405N20
Pcnx Pdcd4 Pde7a
Fut8 Tox
Tcf4 Fndc3b
4931406I20 Map4k5
Bmp2k 9330182L06
Aff3 Camk2d
Il10rb 1110028C15
Pdk1 Usp12
Csf2ra Lhfpl2
Myo1e Ier3
4631426J05 Per2
Vcl Ctsc
Cpne2 Ifngr1 Dach1
Dfna5h Bpil2
Klf5 Crem
2900024C23 A130090K04
Hist1h1c Niban
Ebi2 Plxnd1 P2ry1 Trps1 Bcar3 Msr1
Frmd4b Ccl4
Osbpl3 Mrvi1 Gpr84 Ch25h
Rgs1 Gca
Mgll Zfp36l1
Hgf Id2
Thbs1
Cd34 Flt3
Gpr56
Csf2ra B2Galt6
Tgfbr3 Tlr4
72 96 120 h 72 96 120 h
Me
an+/
- 2
SD C
on
serv
atio
n S
core
Peak-widths from center of peak 0 1 2 3 4 5 6
Inpp5a gene exon
Meis1
Hoxa9
Vertebrate conservation
Hox Loci
MLL Polycomb
TALE factors
Common developmental genes (direct targets)
Body patterning/ Hematopoiesis/ Embryonic development
Leukemogenesis
Context-specific downstream targets
WHO 2008 Myelodysplastic Syndromes:
Refractory cytopenia with unilineage dysplasia: Refractory
anemia Refractory neutropenia Refractory thrombocytopenia
Refractory anemia with ring sideroblasts
Refractory anemia with multilineage dysplasia
Refractory anemia with excess blasts
Myelodysplastic syndrome associated with isolated del(5q)
Myelodysplastic syndrome, unclassifiable
Childhood myelodysplastic syndrome provisional category:
Refractory cytopenia of childhood
In the separate category of AML and Related Precursor
Neoplasms:
Therapy-related myeloid neoplasms (includes cases meeting
morphologic MDS criteria)
Transformation from MDS: AML with myelodysplasia-related
changes
Also a separate category: Myelodysplastic/Myeloproliferative
Neoplasms
Summary – A pathologist’s perspective on MDS -WHO classification
is our guide to approaching the diagnosis -Threshold is key -CBC
information is the predictor -This is how patients come to
attention of hematology, then to us -Morphology and cytogenetics
make up our toolset -Flow cytometry can sometimes contribute -FISH
plays a more minor role than conventional karyotype -New studies
support possible role for point mutations -The biology guides our
understanding, and contextualizes morphology -And genetics holds
(some of) the answers
http://en.wikipedia.org/wiki/Chromosomehttp://en.wikipedia.org/wiki/Chromosome_7http://en.wikipedia.org/wiki/HOXA1http://en.wikipedia.org/wiki/HOXA2http://en.wikipedia.org/wiki/HOXA3http://en.wikipedia.org/wiki/HOXA4http://en.wikipedia.org/wiki/HOXA5http://en.wikipedia.org/wiki/HOXA6http://en.wikipedia.org/wiki/HOXA7http://en.wikipedia.org/wiki/HOXA9http://en.wikipedia.org/wiki/HOXA10http://en.wikipedia.org/wiki/HOXA11http://en.wikipedia.org/wiki/HOXA13http://en.wikipedia.org/wiki/Chromosome_17http://en.wikipedia.org/wiki/HOXB1http://en.wikipedia.org/wiki/HOXB2http://en.wikipedia.org/wiki/HOXB3http://en.wikipedia.org/wiki/HOXB4http://en.wikipedia.org/wiki/HOXB5http://en.wikipedia.org/wiki/HOXB6http://en.wikipedia.org/wiki/HOXB7http://en.wikipedia.org/wiki/HOXB8http://en.wikipedia.org/wiki/HOXB9http://en.wikipedia.org/wiki/HOXB13http://en.wikipedia.org/wiki/Chromosome_12http://en.wikipedia.org/wiki/HOXC4http://en.wikipedia.org/wiki/HOXC5http://en.wikipedia.org/wiki/HOXC6http://en.wikipedia.org/wiki/HOXC8http://en.wikipedia.org/wiki/HOXC9http://en.wikipedia.org/wiki/HOXC10http://en.wikipedia.org/wiki/HOXC11http://en.wikipedia.org/wiki/HOXC12http://en.wikipedia.org/wiki/HOXC13http://en.wikipedia.org/wiki/Chromosome_2http://en.wikipedia.org/wiki/HOXD1http://en.wikipedia.org/wiki/HOXD3http://en.wikipedia.org/wiki/HOXD4http://en.wikipedia.org/wiki/HOXD8http://en.wikipedia.org/wiki/HOXD9http://en.wikipedia.org/wiki/HOXD10http://en.wikipedia.org/wiki/HOXD11http://en.wikipedia.org/wiki/HOXD12http://en.wikipedia.org/wiki/HOXD13