Embed Size (px)
Citation preview

A. Nursing Health Historya. Biographic Datab. Chief Complaintc. History of Present Illnessd. Past Health History of Illnesse. FUNCTIONAL HEALTH PATTERNS
(11 by Gordon)
B. Physical Examination

Best done when?
Techniques:
Head – toe (cephalo-caudal) examination
Special Considerations: Positioning:
a. Neck: nurse behind the client
b. Thorax/Lungs: sitting position
c. Abdomen: Position sequence of examination (technique and quadrants)

Skills of Physical AssessmentPalpation:
SENSITIVITY OF PARTS OF THE HAND
Hand Part Used Type of Sensation Felt
Fingertips Fine discriminations
Palmar / Ulnar surface
Vibratory sensations(e.g. thrills, fremitus)
Dorsal Surface Temperature
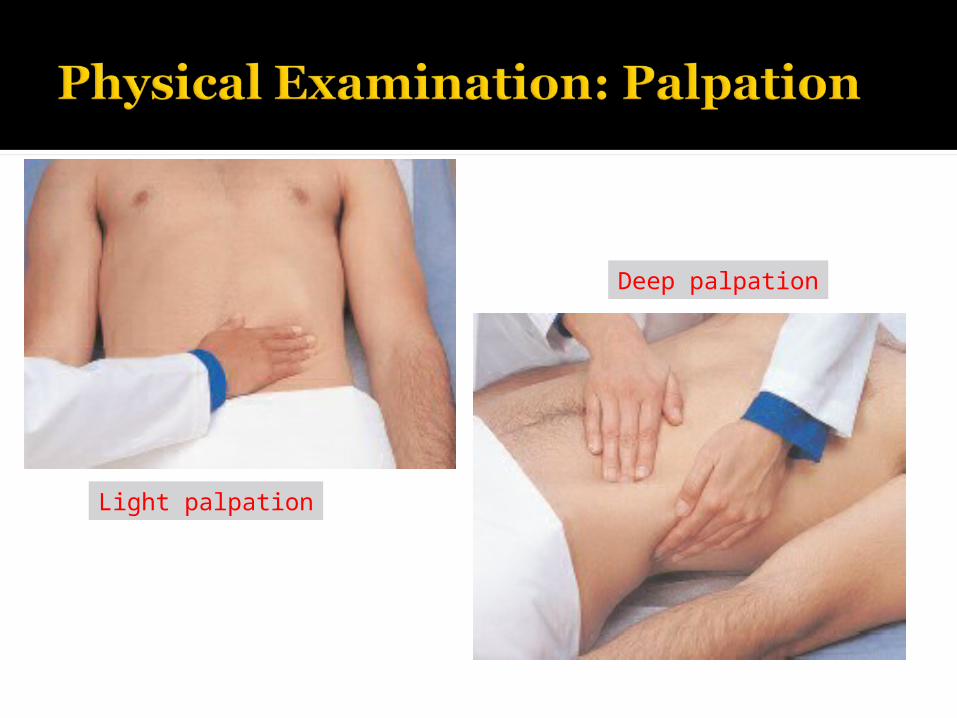
Light palpation
Deep palpation

2 TYPES OF PALPATION:1. Light palpation - 1 cm
dominant hand’s fingers parallel to skin surface
skin is slightly depressed; 2. Deep palpation – 4 cm
done with one or two hands (bimanually)
a. deep bimanualb. deep palpation using one hand

Direct percussion
Indirect percussion

Skills of Physical Assessment3. Percussion
sense of touch and hearing tapping a part of body with fingertips to
elicit character and density of underlying tissue
determine whether underlying tissue a. AIR – FILLEDb. FLUID FILLED C. SOLID

Skills of Physical Assessment3. PercussionTwo types:a. Direct – to elicit tenderness or pain
(differentiate)b. Indirect Pleximeter: middle finger of non-
dominant hand Plexor: dominant hand* Plexor strikes the distal interphalengeal
joint
Skills for Physical Assessment4. Auscultation process of listening to various sounds
(breath, heart, bowel) produced within the body using stethoscope- stethoscope: bell and diaphragm: types of sounds

General Color: a. Normal: pinkish
b. Pallor Dark – skinned? Ashen gray Brown – skinned? Yellowish
brown tinge Light skin?
* Face, conjunctiva, nails

General Color:
c. Jaundice – yellowish tinge Evident where?
* Sclera, mucous membranes, skin
Dark skinned: normal yellow pigmentation of sclera:
Where to assess for jaundice? * Hard palate

General Color:
d. Cyanotic – bluish tinge/discoloration Best assess where? * Nail beds, lips, buccal mucosa1. Central cyanosis lips, buccal mucosa, tongue2. Peripheral cyanosis nails and skin of extremities

Skin Turgor: fullness or elasticity How:
* lifting and pinching the skina. Normal: Good: springs back to previous stateb. Poor
For elderly: For children:

Scale for describing edema:Grade 1+ : 2 mmGrade 2+ : 4 mmGrade 3+ : 6 mmGrade 4+ : 8 mm
* BRAWNY EDEMA

SKIN LESIONS:PRIMARY = APPEARS INITIALLY
Macule – small flat Patch – bigger macule
Papule – elevated Plaque – bigger papule
Vesicle – with fluid Bulla– bigger vesiclePustule – with pus Wheal – mosquito
bites

SECONDARY :TRAUMATIZED PRIMARY LESION
C = Crust – dried blood, pus or serumU = Ulcer – deep, irregular wearing
awayE = Erosion – wearing away of
epidermis S = Scales – shedding flakes

NAIL PLATE SHAPE : curvature and angle▪ convex curvature▪ angle between nail and nail bed: 160 degrees
b. Spoon – shaped nail: Koilonychia: (IDA)

NAIL PLATE SHAPE : curvature and angle
c. ClubbingEarly clubbing: flattened angle (180)Late Clubbing > 180

BLANCH TEST (CAPILLARY REFILL)a. Normal:
b. Delayed return of pink

EYES AND VISIONVisual Acuity Tests:
a. Distance Vision Testb. Near Vision Test
PERRLA Pupil size
Abnormalities: Unequal pupil: Dilated pupil? Constricted pupil?

II. EYES AND VISION Abnormalities:
a. Myopiab. Hyperopiac. Presbyopia: loss of elasticity of lensd. Astigmatism: uneven curvature of cornea
Tests for glaucoma:a. Tonometry – measures IOP: Normal: 8- 21 mmHgb. Perimetry – loss of peripheral visionc. Opthalmoscopy – cupping of the discd. Gonioscopy – measures the angle to differentiate closed and open angle glaucoma

Question:
What type of lens should be used to correct myopia?
Type of lens to be used to correct hyperopia?

EARS AND HEARING To visualize ear canal:
a. AdUltb. ChilD
Tests:a. Rinne Test Normal: AC is greater than BC Conductive problems: BC > ACc. Schwabach Test

b. Weber test bone conduction by testing lateralization of
sounds: N:(-)
Conductive hearing loss,Bad ear hears better
Sensorineural hearing loss,Good ear hears better
Interpretations:BAD-CONDUCTION, GOOD-SENSATION

Mouth and Pharynx
Question:
PART WHERE CENTRAL CYANOSIS IS BEST ASSESSED?

THORAX AND LUNGS
a. APL ratiob. Percussion:
Normal: ResonantDullness:
with solid tissue (PNEUMONIA) or fluid (Pleural effusion)
Hyperresonance: hyper-inflated lungs (asthma, emphysema)

Thorax and LungsChest deformities:
1. Pigeon chest : pectus carinatum Narrow, transverse diameter, increased
AP and protruding sternum
2. Funnel chest : pectus excavatum Sternum depressed, narrow AP
diameter,

Thorax and LungsChest deformities:
3. Barrel chest : APL is 1:1
4. Kyphosis Excessive convex curvature
5. Scoliosis

NORMAL BREATH SOUNDS:
a. Bronchial air passing thru trachea in front of trachea. 1:2 ratio (inspiration: expiration)

NORMAL BREATH SOUNDS:
b. Bronchovesicular air moving thru larger bronchi between scapulae, 2nd ICS. 1:1 ratio

NORMAL BREATH SOUNDS:
c. Vesicular air moving through smaller
bronchioles and alveoli peripheral, base of lungs 5:2 ratio

ADVENTITIOUS BREATH SOUNDS:
1. CRACKLES – RALES: R = Roll hairA = Air pass mucusL = Low lungsE = Exaged by inspirationS = Styles: fine, med, course
ADVENTITIOUS BREATH SOUNDS:
2. FRICTION RUB rubbing, inflamed pleural surfaces. grating sound lower anterior chest audible: both inspiration and expiration.

ADVENTITIOUS BREATH SOUNDS:
3. GURGLES air thru narrowed spaces coarse, with snoring quality predominate: bronchi and trachea. best heard on expiration.

ADVENTITIOUS BREATH SOUNDS:
4. WHEEZE air thru constricted bronchus high pitched, squeaky musical
sound. over all lung fields best heard on expiration.


JUGULAR VEIN:semi-fowler’s: 30-45° during
assessment.veins not visible: normalveins distended: possible right sided
heart disease.Measure JV highest distention from
angle of Louisuntil 4cm only.above 4cm: vein distention.

a. Point of Maximal Impulse
a. Semilunar and Attrioventricular (AV) valves
P: 2nd ICS left sternal border
A: 2nd ICS right sternal border
M: 5th ICS left MCL
T: 5th ICS left sternal border


BREASTa. Upper outer quadrant
common site of breast cancerb. BSE 5-7 after the first
menstruation day MONTHLYc. 20-40 y/o: Clinical breast exam
yearlyD. Mammography at 40 yearly


a. Sequence:
By quadrant: RLQ, RUQ, LUQ, LLQ
b. Position:
c. Bowel Sounds: Normoactive Hypoactive Hyperactive Absent:

Abdominal Test:
Shifting Dullness


COMPONENTS OFNEUROLOGICAL ASSESSMENT
1. Mental Status 2. Level of Consciousness3. Reflexes4. Motor Functions5. Sensory Functions 6. Cranial Nerves

I. Mental Status: Reveals cerebral function (intellectual
and affective) Major areas of assessment:a. Languageb. Orientationc. Memoryd. Attention span e. Calculation

A. LanguageAphasia – inability to express oneself
by speech, writing or comprehend spoken or written language due to disease of cerebral cortex
Two Categories:1. Sensory or receptive aphasia2. Motor or expressive aphasia

1. Sensory/receptive aphasia- loss of ability to comprehend written or spoken words
Two types:a. Auditory aphasia – unable to understand
symbolic content associated with soundsb. Visual aphasia – unable to understand
printed or written figures

2. Motor/ expressive aphasia- loss of power to express oneself by writing, making signs or speaking
How to assess language deficits: Point to common objects and name them Read some words and match printed and
written words with pictures Respond to verbal/written commands

Speech Patterns: - pace, clarity, spontaneity
Abnormalities:a. Perseveration
- repeating the same response as different questions are asked
b. Paraphasia- speech appropriately expressed but contains incorrect words

B. Orientation – 3 spheresC. Memory- Listen for lapses of memory- If problems are present:Three categories of memory:1. Immediate recallN: can repeat series of 5 – 8 digits in
sequence and 4 – 6 digits in reverse order

C. Memory2. Recent memory- Ask to recall the events of the day- Recall information given early in the
interview- Provide 3 facts to recall (color,
object, address), then ask later

C. Memory3. Remote memory- Previous illness or surgery (years ago),
birthday, anniversaryD. Attention Span- Tests the ability to concentrate
(alphabet, count backward from 100)

E. Calculation- Serial seven or serial three testN: can complete serial seven in 90
seconds with 3 or less errors

II. Level of Consciousness Conscious, L O S C Glasgow Coma Scale (GCS)a. Eye opening 4b. Verbal response 5c. Motor response 6
Perfect score: 15(fully alert and oriented)
* Score of 7 or less- comatose

III. REFLEXES- Automatic response of the body to
stimulus- Not voluntary learned or conscious- Deep tendon reflex (DTR) is activated
when tendon is stimulated (tapped) and its associated muscle contracts
- Reflex response varies among individuals and by age


Equipment: reflex hammerScale for Grading Reflex Responses 0: No reflex response+1: minimal activity (hypoactive)+2: normal response+3: more active than normal+4: maximum activity (hyperactive)

REFLEXES:1. Biceps Reflex
- tests the spinal cord C5 & C62. Triceps Reflex
- spinal cord C7 and C8- triceps tendon 1-2 in above elbow

REFLEXES3. Brachioradialis reflex
- spinal cord C3 and C6- tap directly on the radius (1-2 in) above the wrist or the styloid process (bony prominence on the thumb side of the wrist)

REFLEXES4. Patellar reflex
- spinal cord L2, L3, L45. Achilles reflex
- spinal cord level S1 and S2- dorsiflex the ankle
6. Plantar (Babinski) reflex

CEREBELLAR FUNCTIONa. Posture and gaitb. Smooth and coordinated
movementsc. Equilibrium

Cerebellar disorders:Ataxia lack of muscle coordination tremors disturbance of equilibrium, timing
of movements and gait

MOTOR FUNCTIONGross Motor and Balance Testsa. Gaitb. Romberg testc. Standing on one foot with eyes
closed (5 seconds)d. Heel to toe walking

MOTOR FUNCTIONFine Motor Tests for Upper Extremitiesa. Finger to Nose Testb. Alternating Supination and Pronation of
Hands on Kneesc. Finger to Nose and nurse’s finger ( 18
in)d. Finger to thumb

V. SENSORY FUNCTION include touch, pain, temperature,
position and tactile discrimination face, arms, legs, hands, feet are
tested

Three types of tactile discrimination:a. One and two point discrimination ability to sense whether one or two areas of
skin are being stimulated by pressureb. Stereognosis act of recognizing objects by touching and
manipulating themc. Extinction failure to perceive touch on one side of the
body when two symmetrical areas of the body touched simultaneously
AGNOSIA - Inability to recognize objects by use of senses

THE CRANIAL NERVES CN I: OlfactoryCN II: OpticCN III: OculomotorCN IV: TrochlearCN V: TrigeminalCN VI: AbducensCN VII: FacialCN VIII: Vestibulocochlear/AcousticCN IX: GlossopharyngealCN X: VagusCN XI: Spinal AccessoryCN XII: Hypoglossal


The intervention that should be included in the assessment of a patient’s orientation would be:A. asking the patient to state the time of day
B. inquiring if the patient remembers the nurse’s name
C. ascertaining if the patient can follow simple
directions D. determining if the patient follows
movement with the eyes

Which of the following indicates a normal finding on percussion of the lungs?
1. Tympany over the right upper lobe2. Resonance over the left upper lobe3. Hyperresonance over the left lower
lobe4. Dullness above the left 10th
intercostal space

1. Tympany would be heard over the stomach (air filled).
2. Correct. Resonance is a normal sound over the lung.
3. Hyperresonance is never a normal finding
4. Dullness would be heard below (not above) the 10th intercostal space.

After auscultating the abdomen, the nurse should report which of the following to the primary care provider?
1. Bruit over the aorta2. Absence of bowel sounds for 60
seconds3. Continuous bowel sounds over the
ileocecal valve4. A completely irregular pattern of
bowel sounds

1. Correct. A bruit suggests abnormal turbulence in the aorta, and the primary care provider must be notified.
2. In order for absence of bowel sounds to be considered abnormal, they must be silent for 3 to 5 minutes.
3. Continuous bowel sounds are normally heard over the ileocecal valve following meals.
4. Bowel sounds are more commonly irregular than they are regular.

If unable to locate the client’s popliteal pulse during a routine examination, the nurse should perform which of the following next?
1. Check for a pedal pulse.2. Check for a femoral pulse.3. Take the client’s blood pressure on
that thigh.4. Ask another nurse to try to locate
the pulse.

1. Correct. If a pedal pulse, which is more distal than the popliteal, is present, then adequate arterial circulation to the leg is present even though the popliteal artery has not been located.
2. Presence of a femoral pulse would not provide confirmation that arterial flow exists below that point.
3. Taking a thigh BP requires locating the popliteal pulse.
4. Since the purpose of finding the popliteal pulse is to provide information about arterial circulation to the leg, checking the distal pulse before requesting assistance from another nurse is appropriate.

Which of the following is an expected finding during assessment of the older adult?
1. Facial hair becomes finer and softer.
2. Decreased peripheral, color, and night vision.
3. Increased sensitivity to odors.4. Respiratory rate and rhythm are
irregular at rest.

1. Facial hair is likely to become coarser, not finer.
2. Correct. Visual acuity often lessens with age.
3. The sense of smell becomes less, rather than more acute.
4. The respiratory rate and rhythm is regular at rest. However, both may change quickly with activity and be slow to return to the resting level.

If the client reports loss of short-term memory, the nurse would assess this using which one of the following?
1. Have the client repeat a series of three numbers, increasing to eight if possible.
2. Have the client describe his or her childhood illnesses.
3. Ask the client to describe how he or she arrived at this location.
4. Ask the client to count backwards from 100 subtracting seven each time.

1. Recalling a series of numbers tests immediate recall.
2. Recalling childhood events tests remote (long-term) memory.
3. Correct. Recent memory includes events of the current day.
4. Subtracting backwards from 100 tests attention span and calculation skills.





























