Embed Size (px)
Citation preview
Objectives
Colorindex
Extra informationandfurtherexplanation
Important
Doctors’notes
Drugsnames
Mnemonics
Kindlychecktheeditingfilebeforestudyingthisdocument
5: Pharmacology of corticosteroids
1. Defineandclassifycorticosteroids
2. ToCompareVariousCorticosteroids
3. Conceptofmechanismofactionandpharmacological
effectsofcorticosteroids
4. Explaintheclinicalusesofcorticosteroids
5. Todiscusstheadverseeffectprofileofcorticosteroids
To Understand
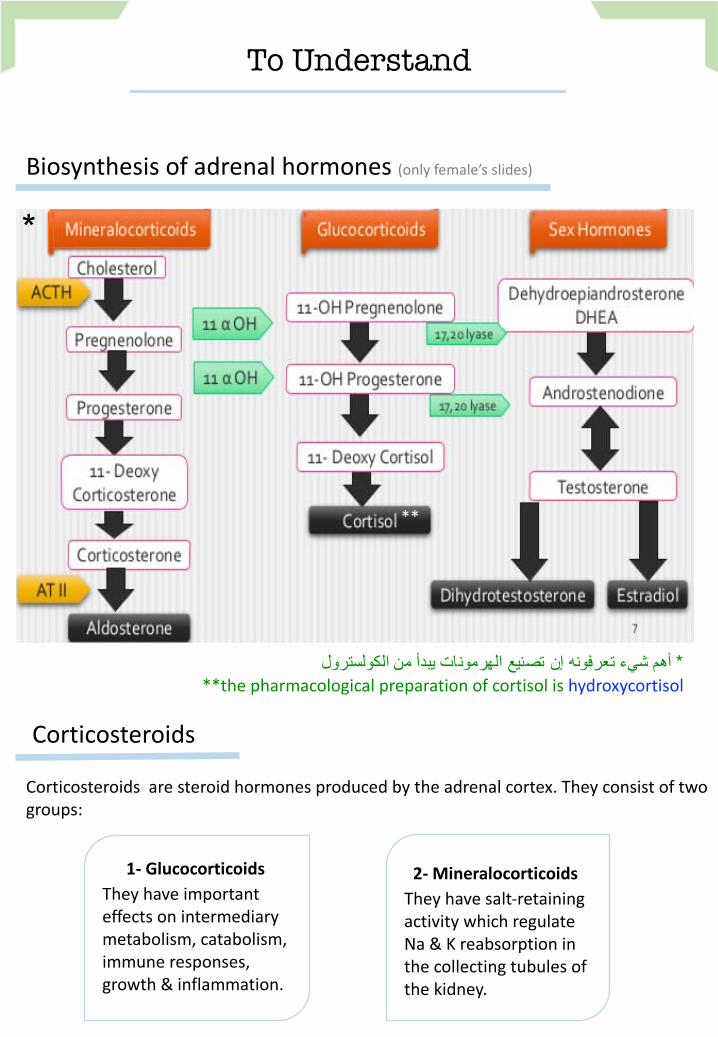
Biosynthesisofadrenalhormones(onlyfemale’sslides)
أھم شيء تعرفونھ إن تصنیع الھرمونات یبدأ من الكولسترول* **thepharmacologicalpreparationofcortisolishydroxycortisol
*
Corticosteroids
Corticosteroidsaresteroidhormonesproducedbytheadrenalcortex.Theyconsistoftwo
groups:
1- GlucocorticoidsTheyhaveimportant
effectsonintermediary
metabolism, catabolism,
immuneresponses,
growth&inflammation.
2- MineralocorticoidsTheyhavesalt-retaining
activitywhichregulate
Na&Kreabsorptionin
thecollectingtubulesof
thekidney.
**
Introduction to corticosteroids
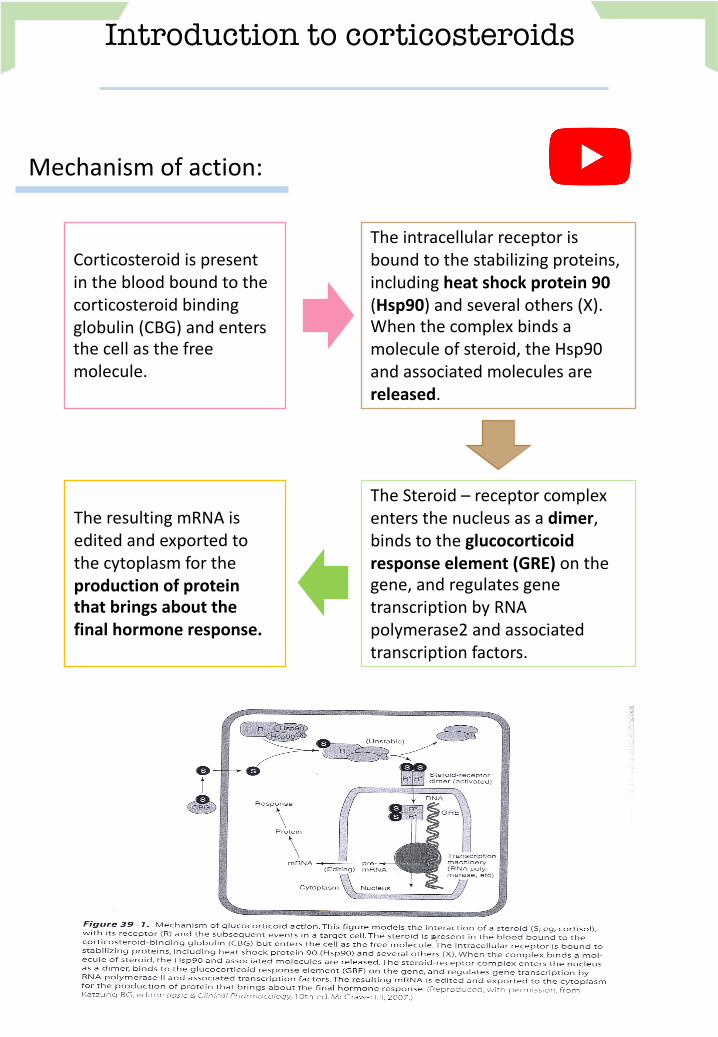
Mechanismofaction:
Corticosteroidispresent
inthebloodboundtothe
corticosteroidbinding
globulin(CBG)andenters
thecellasthefree
molecule.
Theintracellularreceptoris
boundtothestabilizingproteins,
includingheatshockprotein90(Hsp90)andseveralothers(X).Whenthecomplexbindsa
moleculeofsteroid,theHsp90
andassociatedmoleculesare
released.
TheSteroid– receptorcomplex
entersthenucleusasadimer,bindstotheglucocorticoidresponseelement(GRE)onthegene,andregulatesgene
transcriptionbyRNA
polymerase2andassociated
transcriptionfactors.
TheresultingmRNAis
editedandexportedto
thecytoplasmforthe
productionofproteinthatbringsaboutthefinalhormoneresponse.
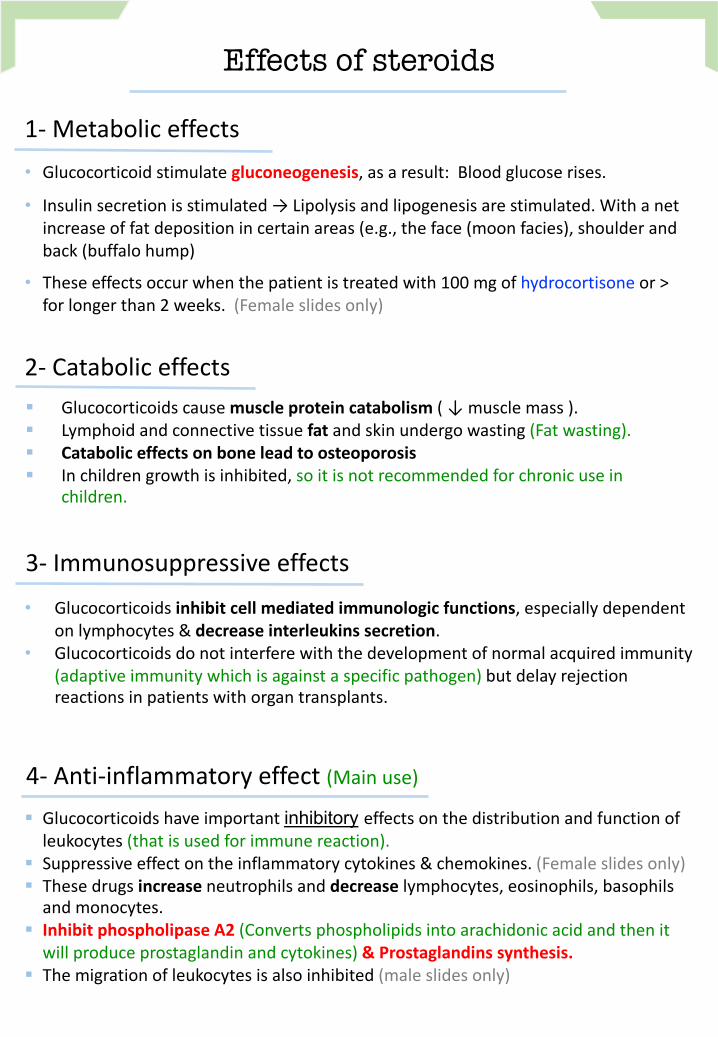
• Glucocorticoidstimulategluconeogenesis,asaresult:Bloodglucoserises.
• Insulinsecretionisstimulated→Lipolysisandlipogenesisarestimulated.Withanet
increaseoffatdepositionincertainareas(e.g.,theface(moonfacies),shoulderand
back(buffalohump)
• Theseeffectsoccurwhenthepatientistreatedwith100mgofhydrocortisone or>
forlongerthan2weeks.(Femaleslidesonly)
Effects of steroids
1- Metaboliceffects
§ Glucocorticoidscausemuscleproteincatabolism(↓musclemass).
§ Lymphoidandconnectivetissuefatandskinundergowasting(Fatwasting).§ Cataboliceffectsonboneleadtoosteoporosis§ Inchildrengrowthisinhibited,soitisnotrecommendedforchronicusein
children.
2- Cataboliceffects
3- Immunosuppressiveeffects
• Glucocorticoidsinhibitcellmediatedimmunologicfunctions,especiallydependentonlymphocytes&decreaseinterleukinssecretion.
• Glucocorticoidsdonotinterferewiththedevelopmentofnormalacquiredimmunity
(adaptiveimmunitywhichisagainstaspecificpathogen) butdelayrejection
reactionsinpatientswithorgantransplants.
4- Anti-inflammatoryeffect(Mainuse)
§ Glucocorticoidshaveimportantinhibitory effectsonthedistributionandfunctionof
leukocytes(thatisusedforimmunereaction).
§ Suppressiveeffectontheinflammatorycytokines&chemokines.(Femaleslidesonly)
§ Thesedrugsincreaseneutrophilsanddecreaselymphocytes,eosinophils,basophils
andmonocytes.
§ InhibitphospholipaseA2(Convertsphospholipidsintoarachidonicacidandthenitwillproduceprostaglandinandcytokines)&Prostaglandinssynthesis.
§ Themigrationofleukocytesisalsoinhibited(maleslidesonly)
Overview
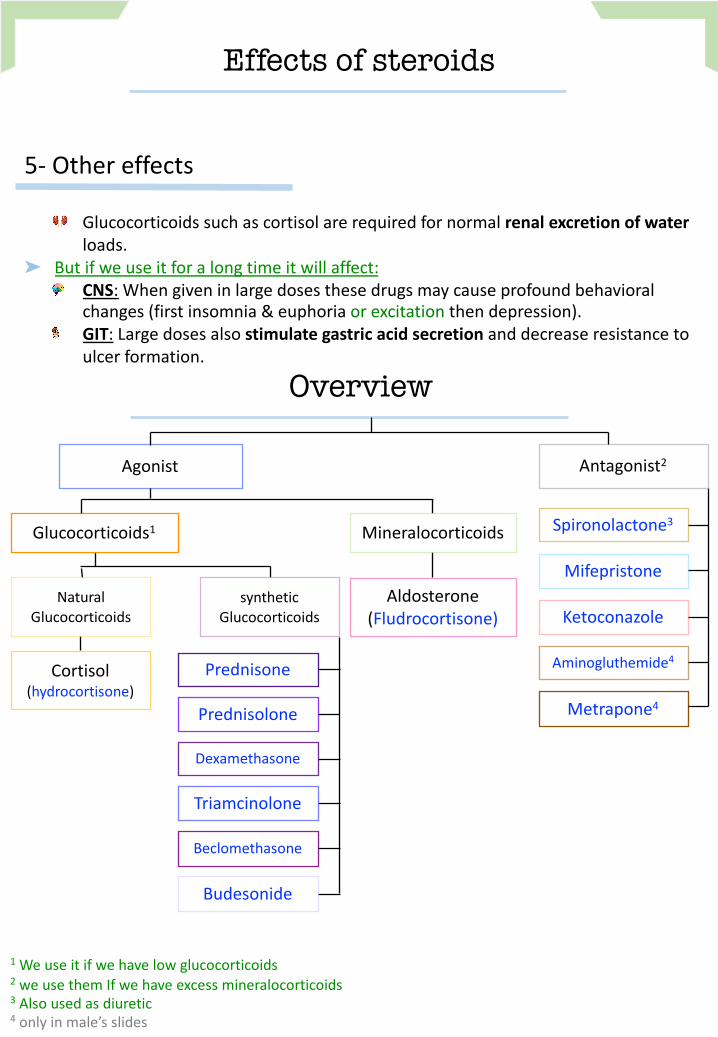
5- Othereffects
Glucocorticoidssuchascortisolarerequiredfornormalrenalexcretionofwaterloads.
➤ Butifweuseitforalongtimeitwillaffect:
CNS: Whengiveninlargedosesthesedrugsmaycauseprofoundbehavioral
changes(firstinsomnia&euphoriaorexcitationthendepression).
GIT: Largedosesalsostimulategastricacidsecretionanddecreaseresistancetoulcerformation.
Effects of steroids
1
Weuseitifwehavelowglucocorticoids
2
weusethemIfwehaveexcessmineralocorticoids
3
Alsousedasdiuretic
4
onlyinmale’sslides
Aldosterone
(Fludrocortisone)
synthetic
Glucocorticoids
Antagonist2
Agonist
MineralocorticoidsGlucocorticoids1
Spironolactone3
Ketoconazole
Mifepristone
Prednisone
Triamcinolone
Dexamethasone
Beclomethasone
Budesonide
Prednisolone
Cortisol
(hydrocortisone)
Aminogluthemide4
Metrapone4
Natural
Glucocorticoids
Glucocorticoids
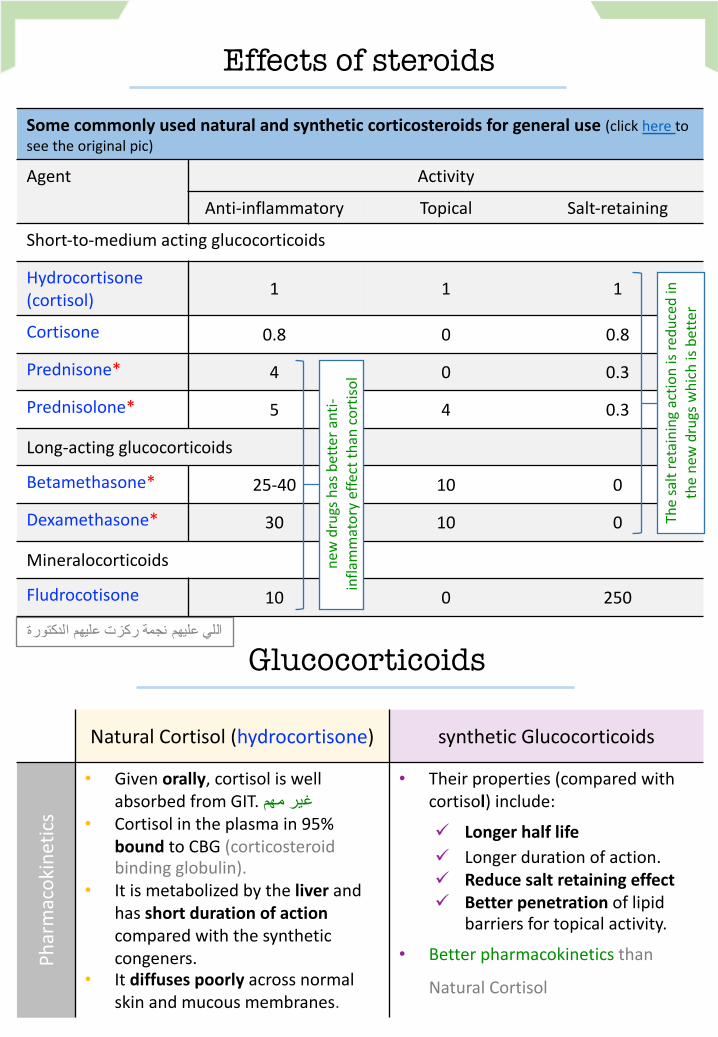
NaturalCortisol (hydrocortisone) syntheticGlucocorticoids
Pharmacokinetics
• Givenorally,cortisoliswellabsorbedfromGIT.غیر مھم
• Cortisolintheplasmain95%
boundtoCBG(corticosteroidbindingglobulin).
• Itismetabolizedbytheliverandhas shortdurationofactioncomparedwiththesynthetic
congeners.
• Itdiffusespoorlyacrossnormal
skinandmucousmembranes.
• Theirproperties(comparedwith
cortisol)include:
ü Longerhalflifeü Longerdurationofaction.
ü Reducesaltretainingeffectü Betterpenetrationoflipid
barriersfortopicalactivity.
• Betterpharmacokinetics than
NaturalCortisol
Somecommonlyusednaturalandsyntheticcorticosteroidsforgeneraluse(clickheretoseetheoriginalpic)
Agent Activity
Anti-inflammatory Topical Salt-retaining
Short-to-mediumactingglucocorticoids
Hydrocortisone
(cortisol)
1 1 1
Cortisone 0.8 0 0.8
Prednisone* 4 0 0.3
Prednisolone* 5 4 0.3
Long-actingglucocorticoids
Betamethasone* 25-40 10 0
Dexamethasone* 30 10 0
Mineralocorticoids
Fludrocotisone 10 0 250
Effects of steroids
newdrugshasbetteranti-
inflammatoryeffectthancortisol
Thesaltretainingactionisreducedin
thenewdrugswhichisbetter
اللي علیھم نجمة ركزت علیھم الدكتورة
Glucocorticoids
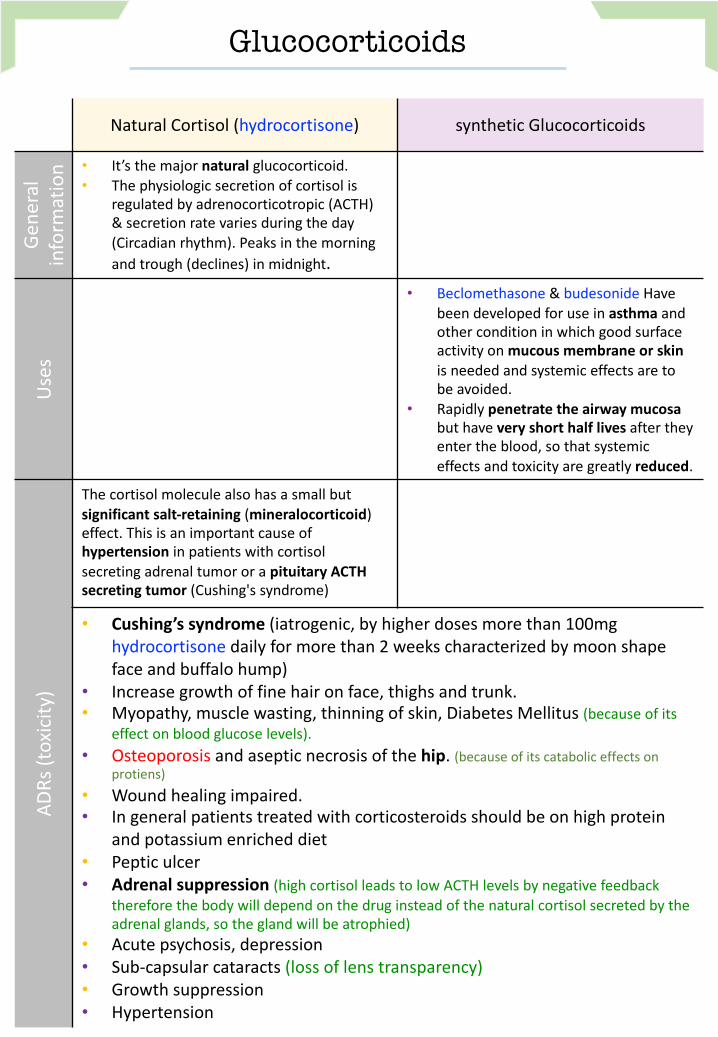
NaturalCortisol (hydrocortisone) syntheticGlucocorticoids
General
information
• It’sthemajornaturalglucocorticoid.• Thephysiologicsecretionofcortisolis
regulatedbyadrenocorticotropic(ACTH)
&secretionratevariesduringtheday
(Circadianrhythm).Peaksinthemorning
andtrough(declines)inmidnight.
Uses
• Beclomethasone& budesonide Have
beendevelopedforuseinasthmaandotherconditioninwhichgoodsurface
activityonmucousmembraneorskinisneededandsystemiceffectsareto
beavoided.
• Rapidlypenetratetheairwaymucosabut haveveryshorthalflivesaftertheyentertheblood,sothatsystemic
effectsandtoxicityaregreatlyreduced.
ADRs(toxicity)
Thecortisolmoleculealsohasasmallbut
significantsalt-retaining(mineralocorticoid)effect.Thisisanimportantcauseof
hypertensioninpatientswithcortisolsecretingadrenaltumororapituitaryACTHsecretingtumor(Cushing'ssyndrome)
• Cushing’ssyndrome(iatrogenic,byhigherdosesmorethan100mg
hydrocortisone dailyformorethan2weekscharacterizedbymoonshape
faceandbuffalohump)
• Increasegrowthoffinehaironface,thighsandtrunk.
• Myopathy,musclewasting,thinningofskin,DiabetesMellitus (becauseofits
effectonbloodglucoselevels).
• Osteoporosis andasepticnecrosisofthehip.(because ofitscataboliceffectsonprotiens)
• Woundhealingimpaired.
• Ingeneralpatientstreatedwithcorticosteroidsshouldbeonhighprotein
andpotassium enricheddiet
• Pepticulcer
• Adrenalsuppression(highcortisolleadstolowACTHlevelsbynegativefeedbackthereforethebodywilldependonthedruginsteadofthenaturalcortisolsecretedbythe
adrenalglands,sotheglandwillbeatrophied)
• Acutepsychosis,depression
• Sub-capsularcataracts(lossoflenstransparency)
• Growthsuppression
• Hypertension
§ Addison’sdisease(chronicadrenalcorticalinsufficiency)
§ Acuteadrenalinsufficiency associatedwithlifethreateningshock,infectionsortrauma.
§ Congenitaladrenalhyperplasia(inwhichsynthesisofabnormalformsofcorticosteroidsarestimulatedbyACTH).
Clinical uses of glucocorticoids
Adrenaldisorders
Non-adrenaldisorders5
• Allergicreactions(e.g;bronchialasthma,angioneuroticedema-swellinginlarynx
andrespiratorysystem-,drugsreactions,urticaria,allergicrhinitis)
• Collagen vascular disorders:Auto-immunediseasesagainstconnectivetissues
(e.g;rheumatoidarthritis,systemiclupuserythematous,giantcellarteritis,poly
myositis,mixedconnectivetissuesyndrome)
• Organtransplant:preventionandtreatmentofrejection- immunosuppression.
• GIT disorders: inflammatoryboweldisease,non-tropicalsprue.
• Hematologicdisorders:leukemia,multiplemyeloma,acquiredhemolyticanemia,
acuteallergicpurpura‘auto-immunediseasecausedestructionintheRBCs’.
• Infections: acuterespiratorydistresssyndrome,sepsis-highimmunecellsrelease-
• Neurologicdisorders:tominimizecerebraledemaafterbrainsurgery,multiple
sclerosis
• Pulmonarydisease:e.g;aspirationpneumonia,bronchialasthma,sarcoidosis
accumulationofinflammatorycellsinsidethelungsandlymph
• Thyroid diseases:malignantexophthalmos,subacutethyroiditis
• Renal disorders:nephroticsyndrome
• Miscellaneous: hypercalcemiatosecreteCafromthebody,mountainsickness
5
allofthesediseasesareautoimmunediseases,andhereweuseglucocorticoids asanti-
inflammatorydrug
1
•Localapplication(e.g;aerosolforasthma)
2
•Alternatedaytherapy(toreducepituitarysuppression)toinduce
feedbackmechanismsیوم نستخدمھ ویوم ال
3
•Taperingthedosesoonafterachievingatherapeuticresponse.
4
•Toavoidadrenalinsufficiencyinpatientwhohavehadlongterm
therapy,additionalstressdoses(high dose)mayneedtobegiven
duringseriousillnessorbeforemajorsurgery(toavoidwithdrawal
symptoms)
Methods for minimizing corticosteroid toxicity
Mineralocorticoids
Aldosterone(e.g.Fludrocortisone)
Notes
§ Themajornaturalmineralocorticoidinhuman.
§ Aldosteroneisthemainsalt-retaininghormone,promotesNareabsorption
andthereforewaterreabsorption,Kexcretion,inthedistalconvoluted
tubule&thusitisveryimportantintheregulationofbloodvolume&
bloodpressure.ItssecretionisregulatedbyACTH&bytherenin-
angiotensinsystem.
§ Aldosteronehasshorthalflife&littleglucocorticoidactivity
M.O.A
§ Sameasthatofglucocorticoids.
§ Fludrocortisone: itisamineralocorticoidhasalongdurationofactionand
significantglucocorticoidactivitycomparedtoaldosterone(only maleslides)
Uses
Fludrocortisone isfavoredforreplacementtherapyafteradrenalectomy&in
otherconditionsinwhichmineralocorticoidtherapyisneeded.Andcanbe
givento hypotensivepeopletomaintainnormalNaandwaterlevels.
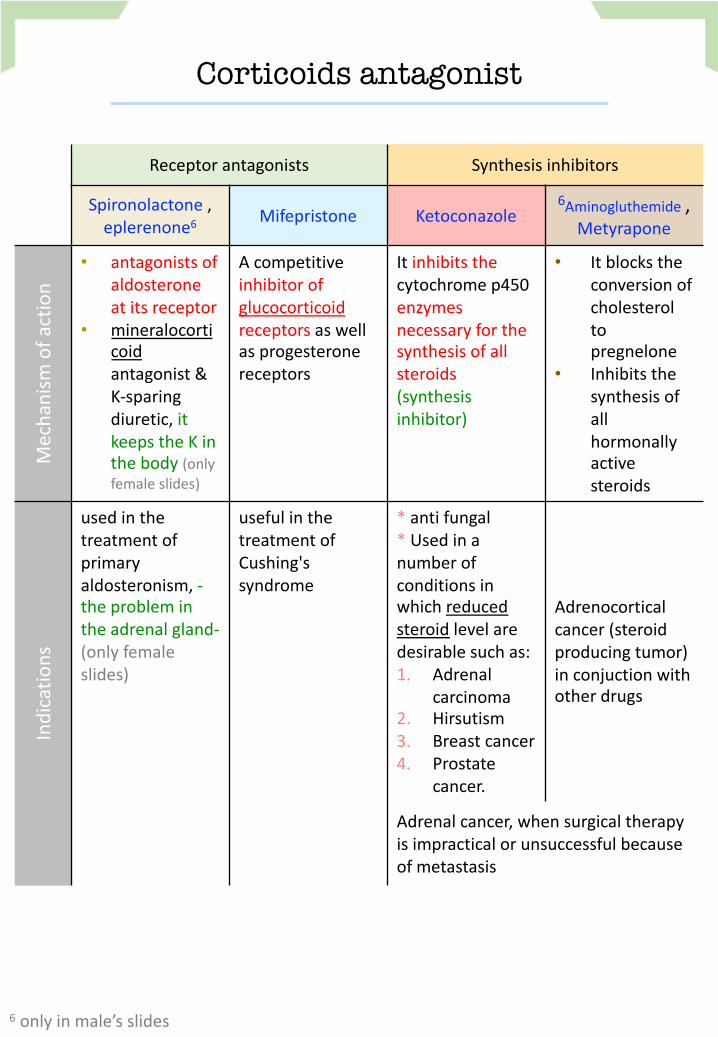
Corticoids antagonist
Receptorantagonists Synthesisinhibitors
Spironolactone,
eplerenone6
Mifepristone Ketoconazole
6
Aminogluthemide,
Metyrapone
Mechanism
ofaction
• antagonistsof
aldosterone
atitsreceptor
• mineralocorti
coid
antagonist&
K-sparing
diuretic, it
keepstheKin
thebody (only
femaleslides)
Acompetitive
inhibitorof
glucocorticoid
receptorsaswell
asprogesterone
receptors
Itinhibitsthe
cytochromep450
enzymes
necessaryforthe
synthesisofall
steroids
(synthesis
inhibitor)
• Itblocksthe
conversionof
cholesterol
to
pregnelone
• Inhibitsthe
synthesisof
all
hormonally
active
steroids
Indications
usedinthe
treatmentof
primary
aldosteronism, -
theproblemin
theadrenalgland-
(onlyfemale
slides)
usefulinthe
treatmentof
Cushing's
syndrome
* antifungal
* Usedina
numberof
conditionsin
whichreduced
steroid levelare
desirablesuchas:
1. Adrenal
carcinoma
2. Hirsutism
3. Breastcancer
4. Prostate
cancer.
Adrenocortical
cancer(steroid
producingtumor)
inconjuction with
otherdrugs
Adrenalcancer,whensurgicaltherapy
isimpracticalor unsuccessfulbecause
ofmetastasis
6
onlyinmale’sslides
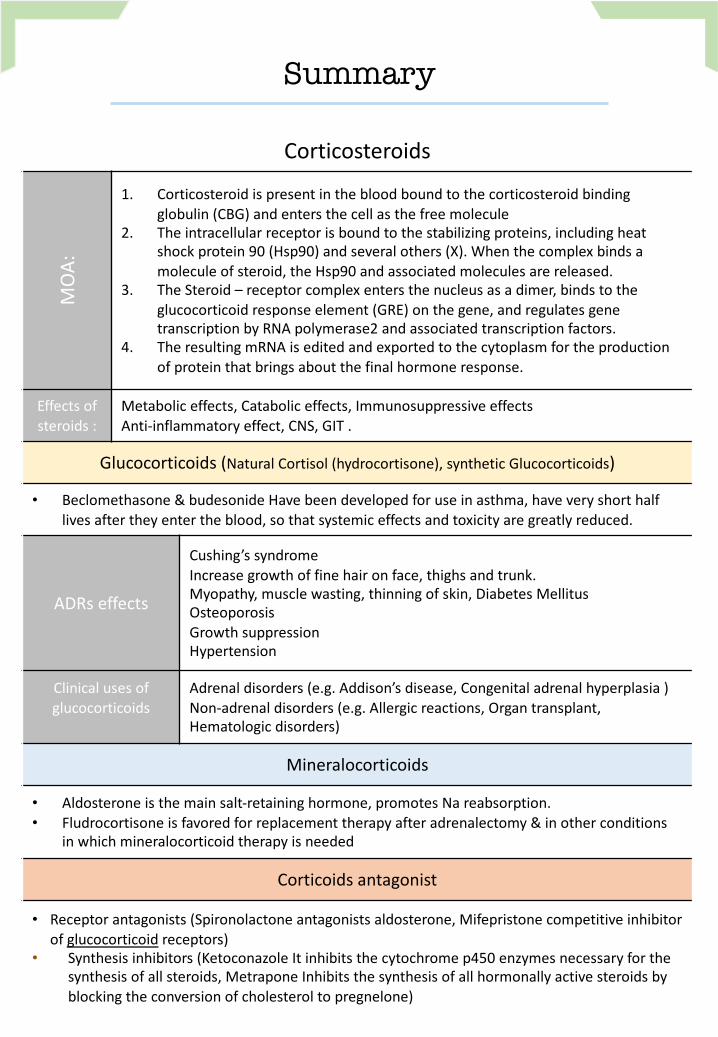
Summary
Corticosteroids
MOA:
1. Corticosteroidispresentinthebloodboundtothecorticosteroidbinding
globulin(CBG)andentersthecellasthefreemolecule
2. Theintracellularreceptorisboundtothestabilizingproteins,includingheat
shockprotein90(Hsp90)andseveralothers(X).Whenthecomplexbindsa
moleculeofsteroid,theHsp90andassociatedmoleculesarereleased.
3. TheSteroid– receptorcomplexentersthenucleusasadimer,bindstothe
glucocorticoidresponseelement(GRE)onthegene,andregulatesgene
transcriptionbyRNApolymerase2andassociatedtranscriptionfactors.
4. TheresultingmRNAiseditedandexportedtothecytoplasmfortheproduction
ofproteinthatbringsaboutthefinalhormoneresponse.
Effectsof
steroids:
Metaboliceffects, Cataboliceffects, Immunosuppressiveeffects
Anti-inflammatoryeffect, CNS,GIT.
Glucocorticoids (NaturalCortisol(hydrocortisone),syntheticGlucocorticoids)
• Beclomethasone&budesonide Havebeendevelopedforuseinasthma, haveveryshorthalf
livesaftertheyentertheblood,sothatsystemiceffectsandtoxicityaregreatlyreduced.
ADRs effects
Cushing’ssyndrome
Increasegrowthoffinehaironface,thighsandtrunk.
Myopathy,musclewasting,thinningofskin,DiabetesMellitus
Osteoporosis
Growthsuppression
Hypertension
Clinicalusesof
glucocorticoids
Adrenaldisorders (e.g.Addison’sdisease,Congenitaladrenalhyperplasia)
Non-adrenaldisorders (e.g.Allergicreactions, Organtransplant,
Hematologicdisorders)
Mineralocorticoids
• Aldosteroneisthemainsalt-retaininghormone,promotesNareabsorption.
• Fludrocortisoneisfavoredforreplacementtherapyafteradrenalectomy&inotherconditions
inwhichmineralocorticoidtherapyisneeded
Corticoidsantagonist
• Receptorantagonists (Spironolactoneantagonistsaldosterone,Mifepristonecompetitiveinhibitor
ofglucocorticoid receptors)
• Synthesisinhibitors(KetoconazoleItinhibitsthecytochromep450enzymesnecessaryforthe
synthesisofallsteroids, Metrapone Inhibitsthesynthesisofallhormonallyactivesteroidsby
blockingtheconversionofcholesteroltopregnelone)
MCQs
Q1:Whichoneofthefollowingisthemostimportanttherapeuticpropertyofglucocorticoidsinclinicalpractice?A.Metaboliceffect.B.Immunosuppressant.C.Anti-inflammatory.
Q2;Whichoneofthefollowingisthemainmechanisminwhichglucocorticoidsactasanti-inflammatorydrugs?A.Blocktheactionofcytokinesandchemokines.
B.InhibitphospholipaseA2andprostaglandinsynthesis.
C.Inhibitthemigrationofneutrophilsandleukocytes.
Q3:Whichcorticosteroidspossessthehighestmineralocorticoidfunction?A.Hydrocortisone.B.Fluprednisolone.C.Fludrocortisone.
Q4:Corticosteroidsareusefulinthetreatmentofallofthefollowingdisordersexcept:A. Addisondisease.B.Allergicrhinitis.C.Cushingsyndrome.D.Inflammatoryboweldisease.
Q5:Allofthefollowingadverseeffectscommonlyoccurwithglucocorticoidtherapyexcept:A. Glaucoma.B.Increasedriskofinfection.C.Hypotension.D.Peripheraledema.
Q6:Osteoporosisisamajoradverseeffectcausedbytheglucocorticoids.Itisduetotheirabilityto:A.Increasetheexcretionofcalcium.B.Inhibitabsorptionofcalcium.C.Decreasecollagensynthesis.
Q7:Achildwithsevereasthmaisbeingtreatedwithhighdosesofinhaledcorticosteroids.Whichofthefollowingadverseeffectsisofparticularconcern?A. Hypoglycemia.B.Hirsutism.C.Growthsuppression.
Q8:Thediagnosisofcongenitaladrenalhyperplasia(CAH)isconfirmedinachild.ThisconditioncanbeeffectivelytreatedbyAdministering:A.Glucocorticoid.B.Androgenantagonist.C.ketoconazoletodecreasecortisolsynthesis.
Q9:ApatientwithAddisondiseaseisbeingtreatedwithhydrocortisonebutisstillhavingproblemswithdehydrationandhyponatremia.Whichofthefollowingdrugswouldbebesttoaddtothepatient’stherapy?A. Dexamethasone.B.Fludrocortisone.C.Prednisone.
Q10:Amalepatientisplacedonanewmedicationandnotesthathisbreastshavebecomeenlargedandtendertothetouch.Whichmedicationishemostlikelytaking?**A. Hydrocortisone.B.Spironolactone.C.Eplerenone.
** An adverse drug reaction to spironolactone is gynecomastia due to its effects on androgens and progesterone in the body. Eplerenone may be a suitable alternative if the patient is in need of an aldosterone antagonist but has a history of gynecomastia.
1)
C
2)
B
3)
C
4)
C
5)
C
6)
B
7)
C
8)
A
9)
B
10)
B
MCQs
Q11:Whichcorticosteroidspossessthelowestsaltretainingeffect?A. Hydrocortisone.B.Prednisone.C.Dexamethasone.
Q12:ComparingtoCortisol/Hydrocortisone,thesyntheticglucocorticoidsarepreferredtobeuseddueto:A. Rapidonsetofaction.B.Mineralocorticoideffect.C.Betterpenetrationoflipidbarrier.
Q13:PatientswhoaretreatedbyHydrocortisone,theirdietshouldberichin:A. Carbohydrates&Na.B.Proteins&K.C.Fats&Cl.
Q14:49yearsoldpatientwhoisoncortisoltherebyfor2years.Heisgoingtomajorsurgeryaftersystemicinfection.Howcanhisdoctoradjustthedoseofcortisolbeforesurgery?A. Taperingthedosebeforethesurgerytothehalf.
B. Givehimthedrugdailyinsteadofalternatedaythereby.
C. Givehimadditionalstressdosebeforethesurgery.
Q15:Whichiscontraindicatedinapatientwithhyperkalemia?A. Aldosterone.B.Ketoconazole.C.Spironolactone.
Q16:Whichoneofthefollowingsyntheticsteroidshowspredominantlyanti-inflammatoryeffect?A. Hydrocortisone.B.Prednisone.C.Dexamethasone.
Q17:Whichoneofthefollowingdrugsactbyinhibitingthesynthesisofcorticosteroids?A.Aldosterone.B.Ketoconazole.C.Spironolactone.
Q18:AllofthefollowingarestrategiestominimizethedevelopmentofHPAaxissuppressionwithcorticosteroidtherapyexcept***:A. Alternate-dayadministrationoftherapy.
B. Usingthelowestdoseofcorticosteroidthatadequatelycontrolssymptoms.
C. Administrationoftwo-thirdsofthedailydoseinthemorningandone-thirdintheafternoon.
Q19:WhichofthefollowingpatientswouldmostlikelyhavesuppressionoftheHPAaxisandrequireaslowtaperofcorticosteroidtherapy****?A. Apatienttaking40mgorallyofprednisonedailyfor7daystotreatanasthmaexacerbation.
B. Apatienttaking10mgorallyofprednisonedailyfor3monthsforrheumatoidarthritis.
C. Apatientusingbeclomethasonenasalspraydailyfor6monthsforallergicrhinitis.
D. Apatientreceivinganintra-articularinjectionofmethylprednisoloneforosteoarthritis.
*** Administration of two-thirds of the dose in the morning and one-third in the afternoon is a strategy to mimic the normal diurnal variation of cortisol secretion. However, it is not a strategy to prevent suppression of the HPA axis. All of the other methods will help prevent the likelihood of suppression of the HPA axis.
**** Correct answer = B. Suppression of the HPA axis usually occurs with higher doses of corticosteroids when used for a duration of 2 weeks or more. Although the dose of prednisone is higher in the asthma patient, the duration of therapy is short, so the risk of HPA axis suppression is lower. The risk of HPA axis suppression is low with topical therapies like intranasal beclomethasone and with one-time joint injections.
11)
C
12)
C
13)
B
14)
C
15)
C
16)
C
17)
B
18)
C
19)
B
:قادة فريق علم األدوية
اللولو الصليهم - جومانا القحطاني - فارس النفيسة -
: الشكر موصول ألعضاء الفريق املتميزين
References:
1- 436doctorsslidesandnotes
2- 435pharmacologyteamwork
@[email protected] Yourfeedback
روان سعد القحطانيحني باشيخري الشثريرميا البراك