Embed Size (px)
Citation preview

4th Quarter MSHO/MSC+ Care
Coordination Training
December 11th and 12th

Agenda
• Welcome
• STARS-Cindy Radke
• HEDIS-Chelsey Doepner
• Behavioral Health-Jennifer Andersen/Elena Hawj
• 2020 MSHO/MSC+ Benefits-Robert Burkhardt
• PCA-Esther Versalles-Hester
• Model of Care-Bobbi Jo Glood
• Care Coordination Survey-Dawn Sulland/Bobbi Jo Glood
• Member Satisfaction Survey-Bobbi Jo Glood
• Care Coordination Updates-Bobbi Jo Glood
• Q & A
2

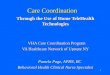
UCare Stars Update-December, 2019

5 Year Overall Rate Trending
3.442
3.268
3.578
3.778
3.949
3
3.1
3.2
3.3
3.4
3.5
3.6
3.7
3.8
3.9
4
2016 2017 2018 2019 2020
MSHO
Presentation title 4

MSHO– Clinical Strengths
Weight2019 CUT POINTS 2020 CUT POINTS
2-Star 3-Star 4-Star 5-Star 2-Star 3-Star 4-Star 5-Star
Diabetes Care- A1c Control 1 39 68 78 87 37 61 72 85
Diabetes Care- Eye Exam 1 56 64 73 80 63 69 73 78
Care Management (SNP-only) 1 46 63 73 89 45 58 75 88
78% 78%81%
77%81% 81%81% 81%
84%83% 81%84%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Diabetes Care- A1c Control Diabetes Eye Exam Care Management (SNP-only)
’17 ’18 ’19 ’20
’17 ‘18 ’19 ‘20
’17 ‘18 ’19 ‘20

MSHO– Clinical Opportunities for Improvement
Weight2019 CUT POINTS 2020 CUT POINTS
2-Star 3-Star 4-Star 5-Star 2-Star 3-Star 4-Star 5-Star
Breast Cancer Screening 1 47 68 76 82 50 66 76 83
Diabetes Care - Kidney Disease Monitoring
1 NA 87 95 97 NA 80 95 97
Plan All-Cause Readmissions (Reversed) 3 12 10 8 5 10 8 7 3
65%
96%
12%
63%
91%
11%
64%
93%
11%
64%
94%
10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Breast Cancer Screening Diabetes Care - Kidney Disease Monitoring Plan All-Cause Readmissions (Reversed)
‘17 ‘18 ’19 ‘20
‘17 ‘18 ’19 ‘20
‘17 ‘18 ’ 19 ‘20

What is UCare doing?
• Reminder calls to members for Breast Cancer, Colon Cancer, Diabetes care. Calls recorded in Hmong and Somali.
• Colon Cancer kits provided in September to all MSHO members who have a gap.
• Live agent calls to MSHO members completed in November. Education and assistance to members to schedule appointments. Reminder calls also will happen for members where an appointment was scheduled.
• Partnerships with community agencies, clinics.

What is coming in 2020?
• Will continue automated calls in 2020.
• Live agent calls will happen in 3rd Quarter to assist members to close gaps.
• In-home kits for members for A1c, Nephropathy, and colon cancer kits.
• Looking at innovative ways to help members with fall prevention.
• Ways to improve assessment reporting.
• Continued partnerships with clinics and community agencies.

Upcoming Requests
• Assessment Reporting clarifications coming in January.
• Turn in December reporting as soon as you can in January!
• Around April, CMS data validation –requests for assessment clarifications may come in.

Log Change • Streamlining choices:
– Assessment
– Refusal
– Unable to reach


HEDIS 2020 Care Coordinator Request
December 11th, 2019
Chelsey Doepner, UCare HEDIS Manager

What is HEDIS• Healthcare Effectiveness Data and Information Set
• American Health plans use HEDIS data to benchmark health plan performance against national and state quality levels
• All populations report HEDIS: Medicare, Medicaid and Commercial
• UCare uses HEDIS internally to focus improvement efforts
• Annual data collection is January to May for the year that just ended
• HEDIS 2020 is measuring 2019 patient care.

HEDIS Measures from Care Coordination –MSHO Only
14
1. Advanced Care Planning Evidence of a document or discussions in the measurement year (2019). Obtained from the Comprehensive Care Plan.
2. Evidence of a Pain Assessment in the measure year (2019). Obtained from the Comprehensive Care Plan.
3. Evidence of a Functional Status Assessment in the measure year (2019). Obtained from the Health Risk Assessment.
4. A Physician, Nurse Practitioner, or PharmD signed Medication List from any time during the measure year (2019.)

How can you help?
• Requests will be sent to counties/delegates for information that supporting measures in early February.
• Provide the following information:
– LTCC/HRA completed during 2019
– Care plans including completed signature page and date summary sent to PCP.
– Provide all documents in separate document format.
– Refusal Care Plans
– If institutional member provide:
• ICCD
• MDS Assessment (If you are able to get it)
• MD Signed Medication review (list)
• LTCC or POC as above if resided in community at any point during the year.
15

Timeline for Request
• Initial Request Letter will be sent approximately:
February 5th , 2020
• We need complete documentation by:
February 21st , 2020
• We know it’s a tight turnaround , but your support is critical to scoring well on this Stars HEDIS measure! Every piece of information can help!
• How many members? Some may have none, some may have 2 and some may have 20. The sampling is random and UCare will not know until late January, early February.
16

Commonly Asked Questions
• Do you need the refusal care plan? NO
• Do you need to replace refused members with another member? No
• What if I get a member who is not mine? Please just let the HEDIS Manager (Chelsey) know. If you do have 2019 data though, please send it even if the member is not yours.
• What if my member is institutional? If you receive a request for an institutional member and can provide us any of the document please do. **Otherwise, please inform us of the facility name and contact.
17

Questions?
Chelsey Doepner, HEDIS Manager
[email protected] or [email protected]
Phone and Secure Voicemail: 612-294-5674
Secure Fax: 612-884-2275
18

Behavioral Health Services101

Agenda
• Department Overview
• Care Management
• Triage Line
20

The birth of the Behavioral Health Department
21

Behavioral Health Department Plan Build case management: develop model and its key components, including assessment, triage, care
coordination; develop training model; recruit and hire; evaluate model through ongoing metric review
Stronger partnerships with providers: establish partnerships and agree upon key initiatives for focus;
develop contracts specific to support implementation on these key areas; explore development of preferred
partnerships/ centers of excellence
Improve UCare member access: develop a single point of entry, hire/train staff to improve member
referral to treatment services, establish and promote single contact number for members and providers
Robust response to 2019 Family and Children’s and MSHO/MSC+ RFPs, including readiness for
response to 2020 RFP: Stronger partnerships with providers: regional specific examples; focus on SUD
reform responses; coordinate with other departments; identify key initiatives to highlight BH value add’s
Leadership Team Meeting 22

BH Care Management Program

BH Care Management
• Started with PMAP/MNCare members in 2018
– Many lessons learned and we improved our model in 2019
• Expanded to MSHO/MSC+ members 11/1/19
• Plan to expand to additional UCare products in 2020
• Your role as a CC will remain critical to your members. We are there to help!!!
24QIACC

Care ManagementEmphasis on assessment, triage, and care
coordination of behavioral and social services
– Shaping the care of our members
– Advocacy
– Improving quality of life
– Positively impacting our members lives
25Future of BHS Care Management Program

Referral Criteria
Member must meet one or more of the criteria listed below to be eligible for Behavioral Health Case Management.
Members may have a combination of the items below to meet our criteria
Triage Coordinators will receive the referral and screen if member meets criteria using an claims report.
If criteria not met, will send back to referral source with option for consult with a case manager.
Criteria:
• 2 admissions in the past 12 months of the following:
– Inpatient mental health, eating disorder, detox or substance use disorder
– Residential treatment for mental health, substance use disorder, IRTS or eating disorder
• 3 admissions in 6 months for crisis residential-
• 2 episodes in the past 12 months for partial hospitalization program
• 2 ER visits in the past 6 months for behavioral health conditions.
26

Questions

BEHAVIORAL HEALTH TRIAGE
Elena Hawj, BH Operations Manager

Triage DefinitionThe assignment of degrees of urgency to wounds
or illnesses to decide the order of treatment of a
larger number of patients or casualties.

What’s our purpose? To promote and provide a telephonic response to members
and providers who are seeking UCare behavioral health
services or guidance.
• Centralized or direct access to intake/behavioral health dept.
• Provide specific assistance and triaging needs to members, their responsible parties, or providers.
• Overall, improve member and provider experiences as it relates to behavioral health inquires.

How may we help?• Crisis Intervention
• BH Referrals
• BH Case Management & Consultations
• BH Provider In-Network and Specialty Search• BH Service Authorization and Notifications• Identification and Connection to Community Resources

Benefits/Eligibility• Pharmacy• Dental• Chiro Care
PremiumsClaimsMaterials/MailingsTransportationAppeals/Grievances
Customer Service BH TriageCrisis InterventionBH Significant Needs/ComplexBH ReferralsBH Provider NetworkBH Case ManagementBH Auth/NotificationsCommunity Resources

Launch of Phone Line3 phase pilot approach in preparation for go-live on 01/01/2020.
Phase 2: 10/01/2019 BH Triage phone number published in member materialsAdd additional UCare Customer Service Reps
Phase 3: Until 12/31/2019Add remaining UCare Customer Service Reps (up to 150 agents)Phase in BH CM consultations
Go Live: 01/01/2020BH Triage phone number published on the back of member’s ID cards.Members, providers, counties and care coordinators will have full access to the UCare Behavioral Health Triage Line.
Phase 1: 09/01/2019 Small set of UCare Customer Service Reps

Hours of OperationMonday thru Friday
8:00am – 5:00pm
Afterhours support for members is available through
UCare’s 24 hour nurse’s line.

QUESTIONS?

Proprietary & Confidential 36
2020 MSHO & MSC+Benefit Changes
MSHO / MSC+ Care Coordinator Training 12/11 and 12/12

2020 MSHO / MSC+ Extra Benefits
Annual Readiness: Proprietary & Confidential 37
Fitness / Social Isolation support MSHO MSC+
Silver Sneakers fitness membership, fitness kits, up to 3 round-trip rides to gym / week
Y -
$15 Community Education class discount Y Y
Independent Living Skills (ILS) training - 2 hours/month up to 6 months for EW members with Instrumental Activities of Daily Living dependencies in their EW care plan – (requires auth) NEW
Y -
Mobility related MSHO MSC+
Anti-glare eyewear lens coating – once / 2 years NEW Y -
Routine foot care visit per month not related to a specific diagnosis already covered by Medicare.
Y -

2020 MSHO / MSC+ Extra Benefits
Annual Readiness: Proprietary & Confidential 38
Preventive Care Incentives MSHO MSC+
$25 Annual exam incentive with primary care physician (all ages)
Y -
$25 Dental visit incentive (all ages) Y Y
Mammogram, colon cancer, diabetes testing incentives (see Health & Wellness for qualifying details, amounts)
Y -
Healthy eating / Nutrition MSHO MSC+
Nutrition counseling – up to 5 visits / year not related to specific diagnosis
Y -
Healthy Savings – up to $200 savings on healthy foods each month
Y Y

2020 MSHO / MSC+ Extra Benefits
Annual Readiness: Proprietary & Confidential 39
Readmission prevention MSHO MSC+
Post-discharge medication review in pharmacy Y -
Post-discharge meals (non-EW only) – up to 2 meals/day for 4 weeks following discharge (requires auth)Mom’s Meals only – (see later slides for details)
Y
Coveredunder Elderly Waiver
Personal Emergency Response System (PERS) (non-EW) (requires auth)
Y
$450 annual allowance for bath safety devices (non-EW) risk or history of falls (device examples: grab bars, handheld showers, toilet frames, support poles, permanent bath seat, handheld shower) - (requires auth) NEW
Y
Strong & Stable Kit (theraband strength kit, bath/shower grips, nightlight, pill box)
Y Y
Behavioral Health MSHO MSC+
Transportation to AA/NA meetings – up to 1 ride / day NEW (requires auth)
Y -

2020 MSHO / MSC+ Extra Benefits
Annual Readiness: Proprietary & Confidential 40
Dental Benefits MSHO MSC+
Additional dental exam (1/year) Y Y
Full mouth series x-ray (1/five years) Y -
Endodontic - Root canal (1/tooth/lifetime) Y -
Root canal re-treatment (1/tooth/lifetime) Y -
Periodontal maintenance (up to four visits/year) Y -
Scaling and root planing (1/two years in office) Y -
One electric toothbrush /three years, two replacement heads/year (comes w/ adult Dental Kit)
Y -
Restorative - two crowns / year NEW Y -
Tissue conditioning for dentures - (1/year in addition to Medicaid coverage) NEW
Y -

MSHO Post Discharge Meals - 2020
• Mom’s Meals will be exclusive meal provider for UCare’s MSHO post-discharge meals for non-EW members effective 1/1/2020
• This change does not impact EW home delivered meals (Mom’s Meals is a provider option for those meals, but all DHS participating providers can provide)
• Post-discharge meal request form will be faxed to UCare Clinical Intake, using the Mom’s Meals order form. UCare will send request form to Mom’s Meals
41

MSHO Post Discharge Meals - 2020
• Process:
–UCare receives discharge notification from facility
–UCare forwards discharge information in dailty report to care coordinators
–Care coordinator discusses benefit with member
–If member is interested / willing / able:
• Care coordinator completes meal request form
• ucare.org>provider information>care managers>msho>forms
• Fax to UCare CLS Intake
–UCare validates member non-EW, discharge status
–UCare forwards approval, meal request to Mom’s Meals
–UCare issues approval letter to member
42

43

Mom’s Meals Order elements:
• Member receiving meals, address, contact
• Do not need to provide diagnosis
• Authorization start date
• Meal plan selection (options listed)
–General wellness (w/ low sodium, heart friendly or vegetarian options)
–Diabetes-friendly
–Renal-friendly
–Glute-free (not dedicated kitchen)
–Pureed meals
• Any special comments
44

Mom’s Meals process
• Post-discharge meal deliveries are prioritized to ensure timeliness – sometimes meal arrives before Welcome Call
• Mom’s Meals phone outreach to member after first delivery
• Member can select from menu (English, Spanish)
• 14 meals (1 week) are delivered at a time
• Meals should be refrigerated, but can stay cool overnight in their shipping container
• Refrigerated rather than frozen (higher quality) - but can freeze without impact
• Located in Iowa – can ship within 24 - 48 hours of request
45

Medicaid benefit changes of note:
–Housing Stabilization Services (7/1/2020)
–For seniors who are homeless / at risk of becoming homeless
– living in institutions / segregated settings or at risk of living in those settings
–Goal:
• support a person’s transition to safe, sustained housing
• avoid future periods of homelessness
• increase long-term stability in community-based housing
–Transition services: housing plan, support obtaining, preparing housing, lease support, moving resource identification, not rent or payment
–Housing Sustaining services: help with behaviors, recertification help, tenancy training / support, income maintenance training, not room & board
46

More information? ucare.org
Annual Readiness: Proprietary & Confidential 47

PCA Assessments
Presented by: Esther Versalles-Hester

Reminders and Tips
Conducting the Assessment:
• Individual PCA can not participate in the PCA assessment
• The PCA can not also act as the Responsible Party ( RP)
• Requiring a RP for the sole purpose of an interpreter during the assessment process alone does not constitute a need for a RP.
Diagnosis:
• Document all diagnosis that are relative to the members ADL, Complex Health Related Needs and Behavioral Dependency needs for PCA.
• If a member has experienced an acute episode ( fracture, surgical procedure, etc..) consider recommending a 6 month or less authorization to allow health status improvement.

Section 6. Complex Health-Related NeedsDefinition: A complex health-related need is an intervention that is ordered by a physician and specified in a care plan. A PCA may or may not be able to assist with the health-related need.
Categories include: • Tube Feeding• Parenteral/IV Therapy• Wounds• Respiratory Interventions• Catheter Insertion and Maintenance• Bowel Program• Neurological Intervention • Other Congenital or Acquired Disease.
Other Congenital or Acquired Disease:• Due to a Congenital or Acquired Disease, the members condition creates a need for significantly increased direct hands on assistance and
interventions in 6-8 ADLS.– Please note that although a member may have been assessed for 6-8 ADL’s they do not necessarily meet this dependency unless
they have a Congenital or Acquired Disease.
DHS provides the following examples of complex health related diagnosis:• Spinal Stenosis, Muscular Dystrophy, Multiple Sclerosis, Cerebral Palsy, CVA/Stroke, Brain Injury, End stages of cancer and ALS. Due to
this types of diagnosis, a member may require extensive or considerable hands-on assistance with ADL’s to name a few.
The ADL section of the PCA assessment allots 30 minutes per ADL, therefore when considering this category, the members condition would warrant more than 30 minutes to complete the task. • For example: Does member Jane Doe’s condition rise to the level of requiring more than 30 minutes to bath, dress or groom etc…?

Section 7. BehaviorsA PCA worker may observe and provide redirection to the recipient for episodes of behavior needing redirection as identified in the care plan
Reminder: when completing this section of the assessment, describe the recipients behavior including the description, frequency, interventions needed and how the behavior affects the persons day.
Level 1 behaviors Definition:
• Physical aggression to self, others or destruction of property. A recipient meets this category if, it requires the IMMEDIATE response of another party to prevent injury to self, others or property.
• Increase vulnerability due to cognitive deficits or social inappropriate behavior:
• Age alone or occasional forgetfulness does not constitute a dependency in this category.
• Resistant to Care, verbal aggression
• A recipient may choose not to bath on a specific day or change their clothes. This does not necessarily constitute a dependency in this area. Remember that a recipient still have the right to choose. Ask additional questions that may provide some rationale. Please note page 16 on DHS 3428D guidelines in regards to behaviors policy.
Additional Time: Do any of the behaviors documented require assistance at least 4 times/week in the last 7 days and if so, an additional 30 mins per description is added to the based time.

Section 8. Activities of Daily Living
Dependency in ADL means a person requires assistance to begin and complete the activity and has a need on a daily basis or needs on the day during the week the activity is completed for.
Cuing AND constant supervision to complete the task or, Hands on assistance to complete the task
Reminders: Provide detailed description of your observations and reported information.
If during a reassessment the member no longer meets a specific dependency, document the rationale.
• Please do not copy and paste the PCA assessment documentation from the previous year into the new PCA assessment.

ADL Dependency’s and Definitions
• Dressing– Assistance with choosing, application and changing of clothing and special appliances, wraps or clothing.
• Grooming– Assistance with basic hair care, oral care, shaving applying cosmetics, deodorant and basic nail care.
• Bathing– Assistance with basic personal hygiene and skin care including starting and completing the steps of bath or shower. This includes
transferring in and out of shower.
• Eating– Assistance to complete the task of eating. Includes assistance with hand washing, and application of orthotics required for eating.
Includes supervision related to a chewing/swallowing issue, choking and monitoring intake. – Cutting food and meal prep is not considered a eating dependency.
• Transfers– Assistance transferring the recipient from one seating or reclining area to another – Assistance in transferring for bathing is a bathing dependency not a transferring dependency.
• Mobility– Assistance needed with ambulation, including use of wheelchair. – If member can safely and independently use cane, walker or wheelchair, member does not meet this dependency.
• Positioning– Assistance with positioning or turning a person for necessary care and comfort.
• Toileting– Assistance with bowel or bladder elimination and care including transfers, mobility, position, feminine hygiene, use of toileting
equipment an supplies, cleansing the perineal area, infection of the skin and adjusting clothing. – Indicates Critical ADL – Additional 30 minutes ( 2 units) per ADL. Only applies if recipient has 2 or ore ADLs

PCA Recipient's Open to CADI Waiver
• The CADI case manager/care coordinator is responsible for conducting the PCA assessment.
• UCare will accept the MnCHOICES assessment tool as well as the Legacy 3428D Format.
• Determination will appear on daily care system auth report.

Assessment Discrepancies
When a discrepancy is identified on the PCA assessment:
• UCare will reach out the assigned care coordinator/assessor via e-mail or phone to discuss.
• Gather additional information, share DHS guidelines and may ask that corrections be made to the assessment.
• To ensure regulatory determination requirements are met as well as avoid delays in service delivery, corrections to an assessment are asked to be completed within 72hrs of UCare outreach.

Elderly Waiver Services• EW Change of Agency:
– When switching services from one provider to another, please submit a new WSAF.
• Case Coordinator notifies previous/current agency when services will end.
• UCare will issue written notification to both the previously approved provider and new provider.
• Budget Exception ( request to exceed case mix cap) Requests.
– Please use the “Request To Exceed Case Mix Cap” form
– Include:
• Rationale: Justification for request and options that have been considered to stay under cap
• Plan of Care/Budget Worksheet
• LTCC
• CL Tool if applicable

Resources
Who to Contact ?
EW
• General Inquires
– Clinical Liaison: [email protected]
• Authorization Inquires
– 612 676-6705 option 2, option 5
– E-mail: [email protected]
– Fax:612 884-2185
PCA
• General and Authorization Inquires
– 612 676-6705 option 2, option 4
– E-mail: [email protected]
– Fax: 612 884-2094
57

Resources
Policy/Guides and Training Resources:
• Supplemental Guide
– https://edocs.dhs.state.mn.us/lfserver/Public/DHS-3428D-ENG
• MCHP Provider Manual – PCA
– https://www.dhs.state.mn.us/main/idcplg?IdcService=GET_DYNAMIC_CONVERSION&RevisionSelectionMethod=LatestReleased&dDocName=id_000094
• PCA Training
– https://www.youtube.com/playlist?list=PL6_zMEWPk7PlgpWE9tewalGuWSEo0WJCw
58

Questions?

UCare Model of Care
Minnesota Health Options (MSHO) & UCare Connect + Medicare
2019

UCare’s Model of Care (MOC)
Overall goal of the MOC:
Drive improvements in health outcomes and quality of life for members.
UCare’s MOC is designed to:
Increase access to affordable, cost-effective health care.
Improve coordination of care.
Ensure seamless transitions of care.
Manage costs.
61

UCare Special Needs Plans (SNP)
Minnesota Senior Health Options (MSHO):
The MSHO program serves elderly members who are dually eligible for Medicare and Medical Assistance and are 65 years or older.
Special Needs Basic Care (UCare Connect + Medicare):
The UCare Connect + Medicare Program serves members with disabilities who are dually eligible for Medicare and Medical Assistance under the age of 65.
62

UCare Special Needs Plans
Integrated products combining Medicaid & Medicare:
Parts A, B, and D (pharmacy)
Members have 1 ID card
One phone number to call for health plan questions
63
Over 15,000 members:
13,000 MSHO
2,400 UCare Connect + Medicare

Why does UCare have a MOC?
Required by CMS & DHS & has four components:
Population description & characteristics
Care Coordination details
Provider Network to ensure adequate access
Quality Measures & Process Improvement goals
64
It helps provide:
Appropriate access to primary & specialty care providers
Integrates care coordination based upon a member’s Health Risk Assessment
Ensures members receive individualized care plans
Encourages and provides care transitions support to members and families

Care Coordination
The care coordinator (CC) coordinates care and services for the member which includes:
Face-to-face Health Risk Assessment (HRA) annually which is used to evaluate members’ health risks, gaps in care and quality of life.
An individualized, person centered care plan.
Facilitating access to affordable care such as: medical, preventive, mental health and social services.
Communicating with the Interdisciplinary Care Team (ICT), a team of professionals involved with the member to coordinate and provide health care services.
Care Coordinators are Qualified Professionals:
Registered Nurses, Nurse Practitioners and Social Workers
65

Care Transition Protocols
The care coordinator assists members, families, facilities, providers, or others with planned and unplanned transitions from one care setting to another.
Examples include: Transition from hospital to home or nursing facility
Goal is improved transitions to reduce fragmented care and avoid re-hospitalizations.
66

Provider Network
UCare’s provider network meets a wide range of needs.
The network includes, but is not limited to:
Primary care providers
Specialists
Primary and specialty clinics
Dental providers
The member may have care from any contracted provider without referral.
Model of Care training is offered annually to all providers, delegates and UCare employees.
67

Clinical Practice Guidelines (CPGs)
UCare adopts clinical practice guidelines to support good decision-making by patients and clinicians to improve health care outcomes, and meet state and federal regulatory requirements.
CPGs are available on our provider website.
68

Quality Measurement & Performance Management
UCare collects and analyzes data and reports from a variety of sources to:
Annually evaluate the Model of Care.
Identify improvements to be made for our members.
69

Summary
Care Coordination is one component of our care model.
UCare has two products with care coordination services – MSHO & Connect + Medicare which currently serves around 15,000 members.
Care coordinators work with members, families and providers on transitions of care with a goal of reducing re-admissions.
UCare uses data and reports to evaluate the Model of Care annually.
70

Questions?
71

2019 MSHO/MSC+ Care Coordination
Survey Results
December 2019

73
We had nearly a 50% response rate!
Thank you to everyone for taking the time to respond to the survey!

PCC/Care Coordination Change Process
76

UCare Website
78

Care Coordination Survey Results• Continued concerns with care coordination enrollment rosters:
– Process improvement work continues to address these issues.
– Timeline currently focused on Q1 2020.
• PCC Change Process:
– Outlined on the 2020 Care Coordination Requirement Grids.
• Concerns with Clinical Liaison responses:
– Efforts will be placed on reviewing responses thoroughly prior to responding.
– Focus will be placed on individual responses pertinent to your situation.
– UCare’s goal will be first email resolution
• UCare Website:
– Working through current limitations i.e. provider search tool.
– Developing a WebEx that will guide you through aspects of the website as well as the provider search tool.
79

80

MSHO/MSC+ MemberSatisfaction Survey
December 2019

Survey Overview
Objective:
Assess member satisfaction with care coordination
Improve care coordination based on member feedback
Topic Areas:
Satisfaction with care coordinator
Satisfaction with care plan
Input into care plan
82

Methodology
Random distribution of surveys
Community members surveyed in June 2019
Members surveyed were in care coordination at least a year
27% response rate for MSHO
13% response rate for MSC+
83

Summary of Results
84
MSHO MSC+
I know who my care coordinator is 90% 80%
My care coordinator is respectful 91% 78%
Overall satisfaction with care coordinator 92% 87%
CC makes it easier to stay in home – yes or sometimes
76% 72%
My care coordinator asks for input into care plan
85% 78%
My satisfaction with the care plan developed
91% 87%

Summary of Results (cont.)
• Survey response rates consistent with those of 2018
• Most members satisfied with care coordinator and care plan
development
• Most members indicate CC works with them to improve
health
• Member comments indicated satisfaction – some CC’s
mentioned by name
85

Opportunities for Improvement
• Efforts to help members know/remember health plan care coordinator
– Use term care coordinator to differentiate between other case managers member may have
• Continue to encourage member involvement in care plan development
Thank you for all you do for our members!
86

Questions?

Care Coordination Updates
88

Account Validation Services (AVS)
• It is important that enrollees complete and return this form along with the cover letter to maintain their MA eligibility. They may lose their MA coverage if they do not.
• Please encourage these enrollees to return both the cover letter and the completed authorization form to the county indicated on the cover letter as soon as possible.
• DHS has asked that AVS forms are not handed out to members who have not received a DHS letter, as AVS forms are being submitted by people for whom the requirement does not apply.
89

MnCHOICES Updates & Reminders
• DHS has indicated they will continue to have trainings and informational meetings for MnCHOICES where MCO MnCHOICES Mentors are expected to attend through the launch of MnCHOICES.
• As we currently understand it all MCO care coordinators, MSHO/MSC+ and Connect, will begin to use MnCHOICES at the same time
• The expectation is that every UCare delegate will have at least one MnCHOICES Mentor who works with UCare members
• We will continue to keep you in the loop through emails and/or articles in the UCare Clinical Services Newsletter
90

2020 UCare MSHO/MSC+ Care Coordination Requirements Grids
• The MSHO/MSC+ requirement grids will be updated and effective 1.1.20.
• All changes will be highlighted in yellow.
• The requirement grids will be sent out in December to provide you time to review and ask clarification questions.
91

Contacts:
• Clinical Liaisons at 612-294-5045 or [email protected] any care coordination questions.
• Please reach out to [email protected] with any enrollment questions.
92

Questions?
93

Thank you!