Embed Size (px)
Citation preview

192
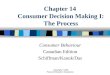
The recent regulatory approval in the UnitedStates and Europe of imatinib mesylate(Gleevec®) for patients with bcr/abl transloca-tion positive chronic myelogenous leukemia(FIG. 14.1) and the subsequent approval forgastrointestinal stromal tumors featuring anactivating c-kit growth factor receptor muta-tion infused the oncology drug developmentcommunity with enthusiasm for anticancertargeted therapy.1,2 Recent major news maga-zines have headlined the considerable publicinterest in new anticancer drugs that exploitdisease-specific genetic defects as the target oftheir mechanism of action.3,4 Many scientists,clinicians, and pharmaceutical company execu-tives now believe that in the next 5 to 10 years,the integration of molecular oncology and mo-lecular diagnostics will further revolutionizeoncology drug discovery and development; cus-tomize the selection, dosing, and route of
administration of both previously approvedtraditional agents and new therapeutics inclinical trials; and truly personalize medicalcare for the cancer patient.5–8
Targeted Therapies for Cancer: Definitions
During the last several years, multiple defini-tions for the term “targeted therapy” haveemerged. From the regulatory perspective,targeted therapy has been defined as a drug inwhose approval label there is a specific refer-ence to a simultaneously or previously ap-proved diagnostic test that must be performedbefore the patient can be considered eligibleto receive the drug. The classic example ofthis definition for targeted therapy is thecoapprovals of the anti-breast cancer an-tibody trastuzumab (Herceptin®) and the eli-gibility tests (Herceptest®, Pathway®, andPathvysion®) (see Chapter 16 and below). Formany scientists and oncologists, targeted ther-apy is defined as a drug with a focused mecha-nism that specifically acts on a well-definedtarget or biologic pathway that, when inacti-vated, causes regression or destruction of themalignant process. Examples of this type oftargeted therapy include hormonal-basedtherapies (see Chapter 15), inhibitors of theepidermal growth factor receptor (EGFR)pathway (see Chapter 17), blockers of inva-sion and metastasis enabling proteins andenzymes (see Chapter 18), antiangiogene-sis agents (see Chapter 19), proapoptoticdrugs (see Chapter 21), and proteasome in-hibitors (see Chapter 24). In addition, mostscientists and oncologists consider anticancerantibody therapeutics that seek out and killmalignant cells bearing the target antigen asanother type of targeted therapy.
Jeffrey S. Ross, MD
Albany Medical College, Albany, New Yorkand Millennium Pharmaceuticals, Inc.,Cambridge, Massachusetts
Targeted Therapy forCancer: IntegratingDiagnostics andTherapeutics
C H A P T E R
14
FIGURE 14.1 Chronic myelogenous leukemia and imatinib(Gleevec®) therapy. Photomicrograph demonstrates a bcr/abltranslocation detected by FISH in a patient with a packed bonemarrow biopsy diagnostic of chronic myelogenous leukemia(inset). Note the yellow “fusion” gene product, indicating the ap-position of one green (chromosome 22) and one red (chromo-some 9) resulting from the translocation.This patient was treatedwith single agent imatinib (Gleevec®) and achieved completeremission of bone marrow histology and absence of bcr/abl byroutine cytogenetics and FISH assessment. See Plate 30 forcolor image.

Chapter 14 Targeted Therapy for Cancer 193
creating enough fresh tissue to perform theassay.10 The drug tamoxifen (Nolvadex®), whichhas both hormonal and nonhormonal mecha-nisms of action, has been the most widely pre-scribed antiestrogen for the treatment ofmetastatic breast cancer and chemopreventionof the disease in high risk women.11,12 Although,ER and progesterone receptor testing is thefront line for predicting tamoxifen response, ad-ditional biomarkers, including HER-2/neu(HER-2) and cathepsin D testing, have beenused to further refine therapy selection.13 Theintroductions of specific estrogen response mod-ulators and aromatase inhibitors such as anas-trozole (Arimidex®), letrozole (Femara®), andthe combination chemotherapeutic, estramus-tine (Emcyt®)14–18 have added new strategies forevaluating tumors for hormonal therapy.
Leukemia and Lymphoma Lead the Way
The introduction of immunophenotyping forleukemia and lymphoma was followed by thefirst applications of DNA based assays, thepolymerase chain reaction, and RNA basedmolecular technologies in these diseases thatcomplemented continuing advances in tumorcytogenetics.19,20 In addition to the imatinib(Gleevec®) targeted therapy for chronic mye-logenous leukemia, other molecular targetedtherapy in hematologic malignancies includesthe use of all-trans-retinoic acid (ATRA) for thetreatment of acute promyelocytic leukemia21;anti-CD20 antibody therapeutics targetingnon-Hodgkin lymphomas, including rituximab(Rituxan®)22; and the emerging Flt-3 target fora subset of acute myelogenous leukemia pa-tients (see below).23
Thirty Years Later: HER-2 and Trastuzumab(Herceptin®)
After the introduction of hormone receptor test-ing, some 30 years then elapsed before the nextmajor targeted cancer chemotherapy programfor a solid tumor was developed. In the mid-1980s, the discovery of the HER-2 (c-erbB2)gene and protein and subsequent associa-tion with an adverse outcome in breast cancerprovided clinicians with a new biomarkerthat could be used to guide adjuvant chemo-therapy.24 The development of trastuzu-mab (Herceptin®), a humanized monoclonal
The Ideal Target
The ideal cancer target (Table 14.1) can be de-fined as a macromolecule that is crucial to themalignant phenotype and is not significantlyexpressed in vital organs and tissues; that hasbiologic relevance that can be reproduciblymeasured in readily obtained clinical samples;that is definably correlated with clinical out-come; and that interruption, interference, orinhibition of such a macromolecule yields aclinical response in a significant proportion ofpatients whose tumors express the target withminimal to absent responses in patients whosetumors do not express the target. For antibodytherapeutics, additional important criteria in-clude the use of cell surface targets that whencomplexed with the therapeutic naked or con-jugated antibody, internalize the antigen–antibody complex by reverse pinocytosis, thusfacilitating tumor cell killing.
The Original Targeted Therapy:Antiestrogens for Breast Cancer
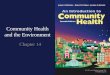
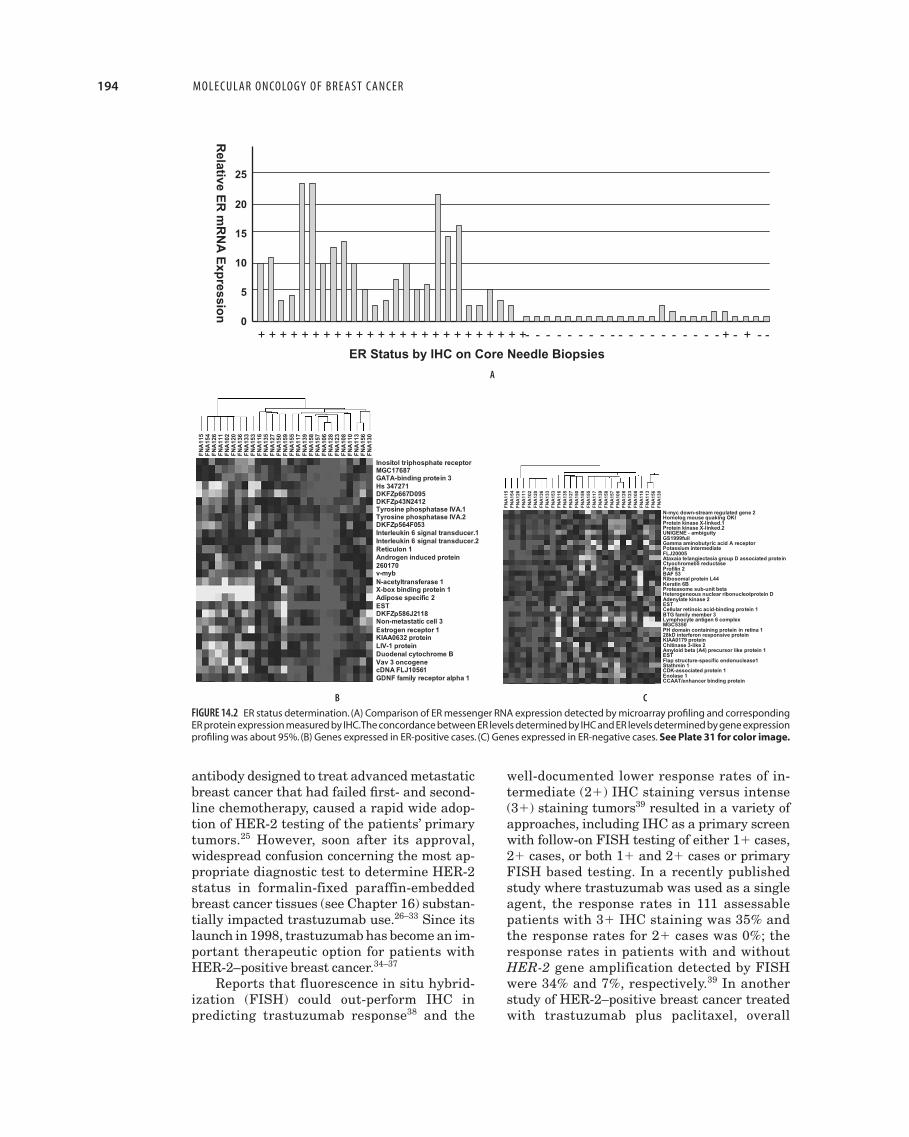
Arguably the first type of targeted therapyin oncology was the development of antiestro-gen therapies for patients with breast cancerthat expressed the estrogen receptor (ER) pro-tein (see Chapter 15) (FIG. 14.2).9 Originallydeveloped as a competitive binding bioassayperformed on fresh tumor protein extracts andused to select for hormone production ablationby surgery (oophorectomy, adrenalectomy, andhypophysectomy), the ER and progesterone re-ceptor test format converted to an immunohis-tochemistry (IHC) platform when the decreasedsize of primary tumors enabled by mass screen-ing programs produced insufficient material for
Table 14.1 Features of the Ideal Anticancer Target
• Crucial to the malignant phenotype
• Not significantly expressed in vital organs and tissues
• A biologically relevant molecular feature
• Reproducibly measurable in readily obtained clinicalsamples
• Correlated with clinical outcome
• When interrupted, interfered with, or inhibited, the result isa clinical response in a significant proportion of patientswhose tumors express the target
• Responses in patients whose tumors do not express thetarget are minimal
194 MOLECULAR ONCOLOGY OF BREAST C ANCER
antibody designed to treat advanced metastaticbreast cancer that had failed first- and second-line chemotherapy, caused a rapid wide adop-tion of HER-2 testing of the patients’ primarytumors.25 However, soon after its approval,widespread confusion concerning the most ap-propriate diagnostic test to determine HER-2status in formalin-fixed paraffin-embeddedbreast cancer tissues (see Chapter 16) substan-tially impacted trastuzumab use.26–33 Since itslaunch in 1998, trastuzumab has become an im-portant therapeutic option for patients withHER-2–positive breast cancer.34–37
Reports that fluorescence in situ hybrid-ization (FISH) could out-perform IHC inpredicting trastuzumab response38 and the
well-documented lower response rates of in-termediate (2�) IHC staining versus intense(3�) staining tumors39 resulted in a variety ofapproaches, including IHC as a primary screenwith follow-on FISH testing of either 1� cases,2� cases, or both 1� and 2� cases or primaryFISH based testing. In a recently publishedstudy where trastuzumab was used as a singleagent, the response rates in 111 assessablepatients with 3� IHC staining was 35% andthe response rates for 2� cases was 0%; theresponse rates in patients with and withoutHER-2 gene amplification detected by FISHwere 34% and 7%, respectively.39 In anotherstudy of HER-2–positive breast cancer treatedwith trastuzumab plus paclitaxel, overall
Relative E
R m
RN
A E
xpressio
n
ER Status by IHC on Core Needle Biopsies
+ + + + + + + + + + + + + + + + + + + + + + + + + - - - - - - - - - - - - - - - - - - - + - + - -
25
20
15
10
5
0
Inositol triphosphate receptorMGC17687GATA-binding protein 3Hs 347271DKFZp667D095DKFZp43N2412Tyrosine phosphatase IVA.1Tyrosine phosphatase IVA.2DKFZp564F053Interleukin 6 signal transducer.1Interleukin 6 signal transducer.2Reticulon 1Androgen induced protein260170v-mybN-acetyltransferase 1X-box binding protein 1Adipose specific 2ESTDKFZp586J2118Non-metastatic cell 3Estrogen receptor 1KIAA0632 proteinLIV-1 proteinDuodenal cytochrome BVav 3 oncogenecDNA FLJ10561GDNF family receptor alpha 1
FN
A11
5F
NA
154
FN
A12
6F
NA
111
FN
A10
2F
NA
120
FN
A13
6F
NA
133
FN
A15
3F
NA
116
FN
A13
5F
NA
127
FN
A15
0F
NA
159
FN
A15
5F
NA
117
FN
A13
9F
NA
158
FN
A15
7F
NA
106
FN
A12
8F
NA
123
FN
A10
8F
NA
110
FN
A11
3F
NA
156
FN
A13
0
FN
A11
5F
NA
154
FN
A12
6F
NA
111
FN
A10
2F
NA
120
FN
A13
6F
NA
133
FN
A15
3F
NA
116
FN
A13
5F
NA
127
FN
A15
0F
NA
159
FN
A15
5F
NA
117
FN
A13
9F
NA
158
FN
A15
7F
NA
106
FN
A12
8F
NA
123
FN
A10
8F
NA
110
FN
A11
3F
NA
156
FN
A13
0
N-myc down-stream regulated gene 2Homolog mouse quaking OKIProtein kinase X-linked.1Protein kinase X-linked.2UNIGENE - ambiguityGS1999fullGamma aminobutyric acid A receptorPotassium intermediateFLJ20005Ataxaia telangiectasia group D associated proteinCtyochromeb5 reductaseProfilin 2BAF 53Ribosomal protein L44Keratin 6BProteasome sub-unit betaHeterogeneous nuclear ribonucleotprotein DAdenylate kinase 2ESTCellular retinoic acid-binding protein 1BTG family member 3Lymphocyte antigen 6 complexMGC5350PH domain containing protein in retina 128kD interferon responsive proteinKIAA0179 proteinChitinase 3-like 2Amyloid beta (A4) precursor like protein 1ESTFlap structure-specific endonuclease1Stathmin 1CDK-associated protein 1Enolase 1CCAAT/enhancer binding protein
FIGURE 14.2 ER status determination. (A) Comparison of ER messenger RNA expression detected by microarray profiling and correspondingER protein expression measured by IHC.The concordance between ER levels determined by IHC and ER levels determined by gene expressionprofiling was about 95%. (B) Genes expressed in ER-positive cases. (C) Genes expressed in ER-negative cases. See Plate 31 for color image.
A
B C

Chapter 14 Targeted Therapy for Cancer 195
overall potency of naked mouse antibodies asanticancer drugs, (3) antibodies penetratedtumor cells poorly, (4) there was limitedsuccess in producing radioisotope and toxinconjugates, and (5) the development of humanantimouse antibodies (HAMA) prevented theuse of multiple dosing schedules.48
The next advance in antibody therapeuticsbegan in the early 1980s when recombinantDNAtechnology was applied to antibody designto reduce the antigenicity of murine andother rodent-derived monoclonal antibodies.Chimeric antibodies were developed where theconstant domains of the human IgG moleculewere combined with the murine variable re-gions by transgenic fusion of the immunoglobu-lin genes; the chimeric monoclonal antibodieswere produced from engineered hybridomasand CHO cells.49,50 The use of chimeric antibod-ies significantly reduced the HAMA responsesbut did not completely eliminate them.51,52 Al-though several chimeric antibodies achievedregulatory approval, certain targets requiredhumanized antibodies to achieve appropriatedosing. Partially humanized antibodies werethen developed where the six complementaritydetermining regions of the heavy and lightchains and a limited number of structuralamino acids of the murine monoclonal antibodywere grafted by recombinant technology to thecomplementarity determining region depletedhuman IgG scaffold.53 Although this processfurther reduced or eliminated the HAMAresponses, in many cases significant furtherantibody design procedures were needed toreestablish the required specificity and affinityof the original murine antibody.54,55
A second approach to reducing the im-munogenicity of monoclonal antibodies hasbeen to replace immunogenic epitopes in themurine variable domains with benign aminoacid sequences, resulting in a deimmunizedvariable domain. The deimmunized variabledomains are genetically linked to human IgGconstant domains to yield a deimmunizedantibody (Biovation, Aberdeen, Scotland). Ad-ditionally, primatized antibodies were subse-quently developed that featured a chimericantibody structure of human and monkeythat, as a near exact copy of a human antibody,further reduced immunogenicity and enabledthe capability for continuous repeat dosingand chronic therapy.56 Finally, fully humanantibodies have now been developed usingmurine sources and transgenic techniques.56
response rates ranged from 67% to 81% com-pared with 41% to 46% in patients with normalexpression of HER-2.40 Interestingly, althoughFISH based testing is more expensive to per-form and is not as widely available as IHC, arecent published review from New York andItaly suggested that FISH was actually themost cost-effective option.41 With trastuzumabachieving excellent results in the treatment ofHER-2–positive advanced metastatic diseaseand under extensive evaluation in major clini-cal trials for its potential efficacy when used inearlier stages, the potential role(s) for HER-2testing as a predictor(s) of responses to othertherapies being resolved by large prospectiveclinical outcome studies and the more conve-nient gene-based chromogenic in situ hy-bridization technique “waiting in the wings,”the story of HER-2 testing in breast cancer willcontinue to unfold over the next several years.
Targeted Anticancer Therapies Using Antibodies
An unprecedented number and variety of tar-geted small molecule and antibody basedtherapeutics are currently in early develop-ment and clinical trials for the treatment ofcancer. Therapeutic antibodies have become amajor strategy in clinical oncology because oftheir ability to specifically bind to primaryand metastatic cancer cells with high affinityand create antitumor effects by complement-mediated cytolysis and antibody-dependentcell-mediated cytotoxicity (naked antibodies) orby the focused delivery of radiation or cellulartoxins (conjugated antibodies).42–47 Currently,there are six anticancer therapeutic antibodiesapproved by the US Food and Drug Adminis-tration (FDA) for sale in the United States(Table 14.2). Therapeutic monoclonal antibod-ies are typically of the IgG class containing twoheavy and two light chains. The heavy chainsform a fused “Y” structure with two light chainsrunning in parallel to the open portion of theheavy chain. The tips of the heavy–light chainpairs form the antigen binding sites, with theprimary antigen recognition regions known asthe complementarity determining regions.
The early promise of mouse monoclonalantibodies for the treatment of human cancerswas not realized because (1) unfocused targetselection led to the identification of targetantigens that were not critical for cancer cellsurvival and progression, (2) there was a low
196 MOLECULAR ONCOLOGY OF BREAST C ANCER
Using modern antibody design and deim-munization technologies, scientists and clini-cians have attempted to improve the efficacyand reduce the toxicity of anticancer antibodytherapeutics.42,48,57–59 The bacteriophage an-tibody design system has facilitated thedevelopment of high affinity antibodies by in-creasing antigen binding rates and reducingcorresponding detachment rates.59 Increasedantigen binding is also achieved in bivalent an-
tibodies with multiple attachment sites, a fea-ture known as avidity. Modern antibody designhas endeavored to create small antibodies thatcan penetrate to cancerous sites but maintaintheir affinity and avidity. A variety of ap-proaches has been used to increase antibody ef-ficacy.42 Clinical trials have recently combinedanticancer antibodies with conventional cyto-toxic drugs, yielding promising results.42–45 Theapplication of radioisotope, a small molecule
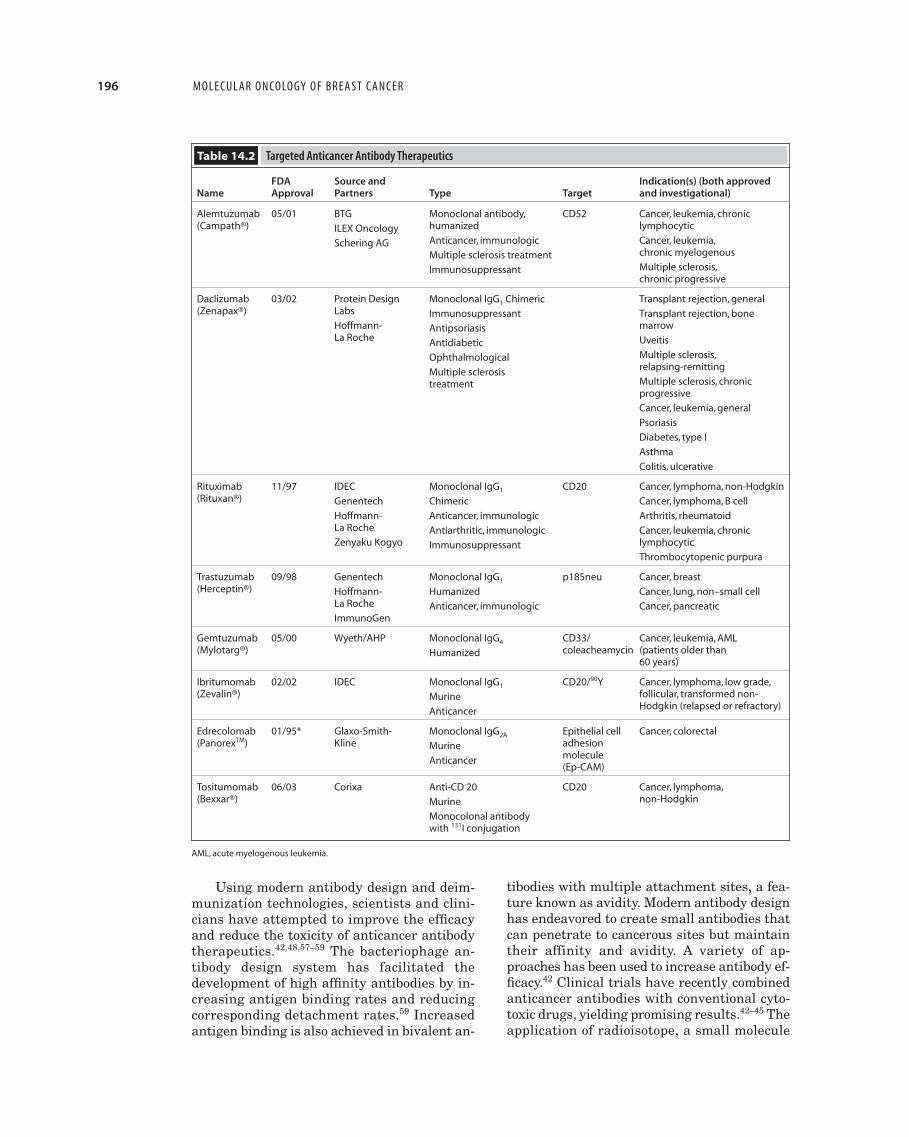
Table 14.2 Targeted Anticancer Antibody Therapeutics
FDA Source and Indication(s) (both approvedName Approval Partners Type Target and investigational)
Alemtuzumab 05/01 BTG Monoclonal antibody, CD52 Cancer, leukemia, chronic(Campath®) ILEX Oncology humanized lymphocytic
Schering AG Anticancer, immunologic Cancer, leukemia,
Multiple sclerosis treatment chronic myelogenous
Immunosuppressant Multiple sclerosis,chronic progressive
Daclizumab 03/02 Protein Design Monoclonal IgG1 Chimeric Transplant rejection, general(Zenapax®) Labs Immunosuppressant Transplant rejection, bone
Hoffmann- Antipsoriasis marrowLa Roche Antidiabetic Uveitis
Ophthalmological Multiple sclerosis,
Multiple sclerosis relapsing-remitting
treatment Multiple sclerosis, chronic progressive
Cancer, leukemia, general
Psoriasis
Diabetes, type I
Asthma
Colitis, ulcerative
Rituximab 11/97 IDEC Monoclonal IgG1 CD20 Cancer, lymphoma, non-Hodgkin(Rituxan®) Genentech Chimeric Cancer, lymphoma, B cell
Hoffmann- Anticancer, immunologic Arthritis, rheumatoid La Roche Antiarthritic, immunologic Cancer, leukemia, chronic Zenyaku Kogyo Immunosuppressant lymphocytic
Thrombocytopenic purpura
Trastuzumab 09/98 Genentech Monoclonal IgG1 p185neu Cancer, breast (Herceptin®) Hoffmann- Humanized Cancer, lung, non–small cell
La Roche Anticancer, immunologic Cancer, pancreatic ImmunoGen
Gemtuzumab 05/00 Wyeth/AHP Monoclonal IgG4 CD33/ Cancer, leukemia, AML(Mylotarg®) Humanized coleacheamycin (patients older than
60 years)
Ibritumomab 02/02 IDEC Monoclonal IgG1 CD20/90Y Cancer, lymphoma, low grade,(Zevalin®) Murine follicular, transformed non-
Anticancer Hodgkin (relapsed or refractory)
Edrecolomab 01/95* Glaxo-Smith- Monoclonal IgG2A Epithelial cell Cancer, colorectal (PanorexTM) Kline Murine adhesion
Anticancer molecule(Ep-CAM)
Tositumomab 06/03 Corixa Anti-CD 20 CD20 Cancer, lymphoma,(Bexxar®) Murine non-Hodgkin
Monocolonal antibodywith 131I conjugation
AML, acute myelogenous leukemia.

Chapter 14 Targeted Therapy for Cancer 197
Unconjugated or naked antibodies includea variety of targeting molecules both on themarket and in early and late clinical develop-ment.Avariety of mechanisms has been cited toexplain the therapeutic benefit of these drugs,including enhanced immune effector functionsand direct inactivation of the targeted path-ways as seen in the antibodies directed atsurface receptors such as HER-1 (EGFR) andHER-2.2–5 Surface receptor targeting can re-duce intracellular signaling, resulting in de-creased cell growth and increased apoptosis.56
As seen in Table 14.2, of the seven anti-cancer antibodies on the market, one is conju-gated with a radioisotope Y90-ibritumomabtiuxetan (Zevalin®) and one is conjugated to acomplex natural product toxin gemtuzumabozogamicin (Mylotarg®). Conjugation proce-dures have been designed to improve antibodytherapy efficacy and have used a variety ofmethods to complex the isotope, toxin, or cyto-toxic agent to the antibody.42,43 Cytotoxic smallmolecule drug conjugates have been widelytested, but enthusiasm for this approach hasbeen limited by the relatively low potency ofthese compounds.42 Fungal derived potent tox-ins have yielded greater success with thecalicheamicin conjugated anti-CD33 antibodygemtuzumab ozogamicin approved for thetreatment of acute myelogenous leukemia anda variety of antibodies conjugated with thefungal toxin maytansanoid (DM-1) in preclini-cal development and early clinical trials. Theinterest in radioimmunotherapy increased sig-nificantly in 2001 with the FDA approvals ofthe 90Y-conjugated anti-CD20 antibody Y90-ibritumomab tiuxetan and the 131I-conjugatedanti-CD20 antibody I131-tositumomab. Avariety of isotopes is under investigation inaddition to 90Y as potential conjugates for an-ticancer antibodies.43 Radioimmunotherapyfeatures the phenomenon of the bystandereffect, in which if antigen expression is hetero-geneous, extensive tumor cell killing can stilltake place, even on nonexpressing cells, butcan also lead to significant toxicity when theneighboring cells are vital non-neoplastic tis-sues such as the bone marrow and liver.
Antibody Therapeutics for HematologicMalignancies
The earliest and most successful clinical use ofantibodies in oncology has been for the treat-ment of hematologic malignancies.42–45,56,60–63
cytotoxic drug, and protein toxin conjugationhas resulted in promising results in clinicaltrials and achieved regulatory approval for sev-eral drugs now on the market (see below). Anti-bodies have also been designed to increase theirenhancement of effector functions of antibody-dependent cellular cytotoxicity. Another causeof toxicity of conjugated antibodies has been thelimitations of the conjugation technology,which can restrict the ratio of the number oftoxin molecules per antibody molecule.42,43,55
Methods designed to overcome the toxicity ofconjugated antibodies include the use of anti-body targeted liposomal small molecule drugconjugates and the use of antibody conjugateswith drugs in nanoparticle formats to enhancebonding strength that enable controlled releaseof the cytotoxic agent. Another technique thatuses site selective prodrug activation to reducebystander tissue toxicity is the antibody di-rected enzyme prodrug therapy. An antibodybound enzyme is targeted to tumor cells. Thisallows for selective activation of a nontoxic pro-drug to a cytotoxic agent at the tumor site forcancer therapy.
A variety of factors can reduce antibody ef-ficacy48: (1) limited penetration of the antibodyinto a large solid tumor or into vital regionssuch as the brain, (2) reduced extravasationsof antibodies into target sites due to decreasedvascular permeability, (3) cross-reactivity andnonspecific binding of antibody to normal tis-sues reduces targeting effect, (4) heteroge-neous tumor uptake results in untreatedzones, (5) increased metabolism of injectedantibodies reduces therapeutic effects, and(6) HAMA and human antihuman antibodiesform rapidly and inactivate the therapeuticantibody.
Toxicity has been a major obstacle in thedevelopment of therapeutic antibodies for can-cer.42–45 Cross-reactivity with normal tissuescan cause significant side effects for unconju-gated (naked) antibodies, which can be en-hanced when the antibodies are conjugatedwith toxins or radioisotopes. Immune mediatedcomplications can include dyspnea from pul-monary toxicity, occasional central and pe-ripheral nervous system complications, anddecreased liver and renal function. On occasion,unexpected toxic complications can be seen,such as the cardiotoxicity associated with theHER-2/neu targeting antibody trastuzumab.Radioimmunotherapy with isotopic-conjugatedantibodies can also cause bone marrow suppres-sion (see below).

198 MOLECULAR ONCOLOGY OF BREAST C ANCER
By taking advantage of improved recombinanttechnologies generating more specific andhigher affinity monoclonal antibodies with re-duced immunogenicity after humanization ordeimmunization and the emerging conjuga-tion capabilities, antibody therapeutics havebecome a major weapon in the treatment ofleukemias and lymphomas.60–63
Approved in 1997, rituximab (Rituxan®) isarguably the most commercially successful an-ticancer drug of any type since the introductionof taxanes. Rituximab sales exceeded $700 mil-lion in sales in the United States in 2001.44
Targeting the CD20 surface receptor commonto many B cell non-Hodgkin lymphoma sub-types, rituximab is a chimeric monoclonal IgG1antibody that induces apoptosis, antibody-dependent cell cytotoxicity, and complement-mediated cytotoxicity56 and has achievedsignificantly improved disease-free survivalrates compared with patients receiving cyto-toxic agents alone.64–67
Y90-ibritumomab tiuxetan (Zevalin®) con-sists of the murine version of the anti-CD20chimeric monoclonal antibody, rituximab,which has been covalently linked to the metalchelator, MD-DTPA, permitting stable bind-ing of 111In when used for radionucleotidetumor imaging and 90Y when used to produceenhanced targeted cytotoxicity.68–71 In early2002, Y90-ibritumomab tiuxetan became thefirst radioconjugated antibody therapeutic forcancer approved by the FDA. Since its FDAapproval, numerous patients who have re-ceived Y90-ibritumomab tiuxetan after becom-ing refractory to a rituximab-based regimenhave achieved significant responses.69,70
The approval of gemtuzumab ozogamicin(Mylotarg®) by the FDA in 2000 marked thefirst introduction of a plant toxin conjugatedantibody therapeutic.72–76 Gemtuzumab ozo-gamicin is targeted against CD33, a surfacemarker expressed by 90% of myeloid leukemicblasts but absent from stem cells, armedwith calicheamicin, a potent cytotoxic antibi-otic that inhibits DNA synthesis and inducesapoptosis.72 The current indication for use ofgemtuzumab ozogamicin is in acute myeloge-nous leukemia patients older than 60 yearswith the recommendation that before the initi-ation of therapy, the leukemic blast count isbelow 30,000/mL.73–75
Alemtuzumab (Campath®), a humanizedmonoclonal antibody, was approved in mid-2001for the treatment of B-cell chronic lymphocytic
leukemia in patients who have been treatedwith alkylating agents and who have failed flu-darabine therapy.77,78 Daclizumab (Zenapax®)is a chimeric monoclonal antibody that targetsthe interleukin-2 receptor. This antibody is pri-marily used to prevent and treat patients withorgan transplant rejection but has also beenused in a wide variety of chronic inflammatoryconditions, including psoriasis, multiple sclero-sis, ulcerative colitis, asthma, type I diabetesmellitus, uveitis, and also in a variety ofleukemias.79,80 I131-tositumomab (Bexxar®) is aradiolabeled anti-CD20 murine monoclonal an-tibody approved in 2003 for the treatment of re-lapsed and refractory follicular/ low grade andtransformed non-Hodgkin lymphoma.81,82
Antibody Therapeutics for Solid Tumors
Interest in the development of antibody thera-peutics for solid tumors among many commer-cial organizations and universities has beensignificantly impacted by the technologicadvances in antibody engineering and theapproval and recent clinical and commercialsuccess of trastuzumab, the only therapeuticantibody approved by the FDA for the treat-ment of solid tumors (edrecolomab is approvedin Germany, but not in the United States).Trastuzumab has been described extensivelyabove.
During the 4 years since the FDA approvalof trastuzumab, there have been no additionalantibodies approved for the treatment of solidtumors. Nonetheless, significant progress hasbeen made in this field, and a number of bothlate stage and early stage products show sub-stantial promise.
Cetuximab (Erbitux®)The EGFR (HER-1) is the target of a variety ofsmall molecule drugs and the late stage anti-body cetuximab.83 Cetuximab, a chimeric mono-clonal antibody, binds to the EGFR with highaffinity, blocking growth factor binding, recep-tor activation, and subsequent signal transduc-tion events and leading to cell proliferation.84
Cetuximab enhanced the antitumor effects ofchemotherapy and radiotherapy in preclinicalmodels by inhibiting cell proliferation, angio-genesis, and metastasis and by promotingapoptosis.84 Cetuximab has been evaluatedboth alone and in combination with radiother-apy and various cytotoxic chemotherapeutic

Chapter 14 Targeted Therapy for Cancer 199
an approval by the FDA of bevacizumab forthe treatment of metastatic colorectal cancerin February 2004.
Unlike cetuximab, the development of be-vacizumab has not included a diagnostic eligi-bility test. Neither direct measurement ofVEGF expression or assessment of tumor mi-crovessel density has been incorporated into theclinical trials or linked to the response rates tothe antibody. Thus, bevacizumab cannot be con-sidered a true targeted therapy, and further fo-cusing of this agent for colorectal, breast, lung,and other cancers will likely be inhibited by theinability to individually select patients with adiagnostic test who will be more likely to benefitfrom its use, either alone or in combination withother known and novel drugs.
Edrecolomab (Panorex®)Edrecolomab is a murine IgG2A monoclonalantibody that targets the human tumor-associated antigen Ep-CAM (17-1A). Edre-colomab has been approved in Europe(Germany) since 1995, but to date has not beenapproved by the FDA. In a study of 189 pa-tients with resected stage III colorectal can-cer, treatment with edrecolomab resultedin a 32% increase in overall survival com-pared with no treatment (P � 0.01).96 Edre-colomab’s antitumor effects are mediatedthrough antibody-dependent cellular cytotoxi-city, complement-mediated cytolysis, and theinduction of an anti-idiotypic network.97 Edre-colomab is also currently being tested in largemulticenter adjuvant phase III studies instage II/III rectal cancer and stage II coloncancer. Edrecolomab was well tolerated whenused as monotherapy and added little tochemotherapy-related side effects when usedin combination. Sequential treatment of pa-tients with metastatic breast cancer with edre-colomab after adjuvant chemotherapy reducedlevels of disseminated tumor cells in the bonemarrow and eliminated Ep-CAM–positivemicrometastases.98
huJ-591 (Anti-PSMAEXT)Prostate-specific membrane antigen (PSMA)is a membrane-bound glycoprotein restrictedto normal prostatic epithelial cells, prostatecancer, and the endothelium of the neovascu-lature of a wide variety of nonprostatic carci-nomas and other solid tumors.99–101 PSMAexpression per cell progressively increases inprimary prostate cancer, metastatic hormone
agents in a series of phase II/III studies thatprimarily treated patients with either headand neck or colorectal cancer.84,85 Breast cancertrials are also underway.86 Although the FDAapproval process for cetuximab was initiallyslowed because of concerns over clinical trialdesign and outcome data management,87 theantibody was approved for use in the treat-ment of advanced metastatic colorectal cancerin February 2004. Similar to trastuzumab, thedevelopment of cetuximab also included an im-munohistochemical test for determining EGFRoverexpression to define patient eligibility toreceive the antibody. Thus, cetuximab hasjoined trastuzumab as an FDA-approved tar-geted therapy featuring an unconjugated anti-body. Although anti-EGFR small moleculedrugs (see below) are under continuing clinicaltrial evaluation in breast cancer,88 cetuximab isnot currently projected as a potential therapeu-tic for this disease.
Bevacizumab (Avastin®)Bevacizumab (rhuMAb-VEGF) is a human-ized murine monoclonal antibody target-ing the vascular endothelial growth factor(VEGF) ligand. VEGF regulates both vascularproliferation and permeability and functionsas an antiapoptotic factor for newly formedblood vessels.89,91 Patients treated with beva-cizumab alone have shown significant tumorresponses. Patients treated with bevacizumabin combination with conventional chemother-apy have had greater responses.89,91 In clinicaltrials for advanced metastatic breast cancer,the initial results of the combination treat-ment of bevacizumab and paclitaxel showedantitumor activity,92 but follow-on studieswere not convincing that the targeting ofVEGF in this clinical setting would be effec-tive. Bevacizumab has also been combinedwith trastuzumab in a two antibody therapeu-tic strategy for HER-2 overexpressing breastcancer.93 The phase II study evaluating beva-cizumab in metastatic renal cell carcinomareached its prespecified efficacy end point ear-lier than expected. Finally, late-stage clinicaltrials using bevacizumab with 5-fluorouracil,leucovorin, and CPT-11 (Irinotecan®) in ad-vanced colorectal cancer are currently un-derway,94 with recently released resultsindicating a major prolongation in the time todisease progression and overall survival in pa-tients who received the angiogenesis inhibitorversus those who did not.95 These data led to

200 MOLECULAR ONCOLOGY OF BREAST C ANCER
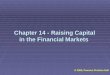
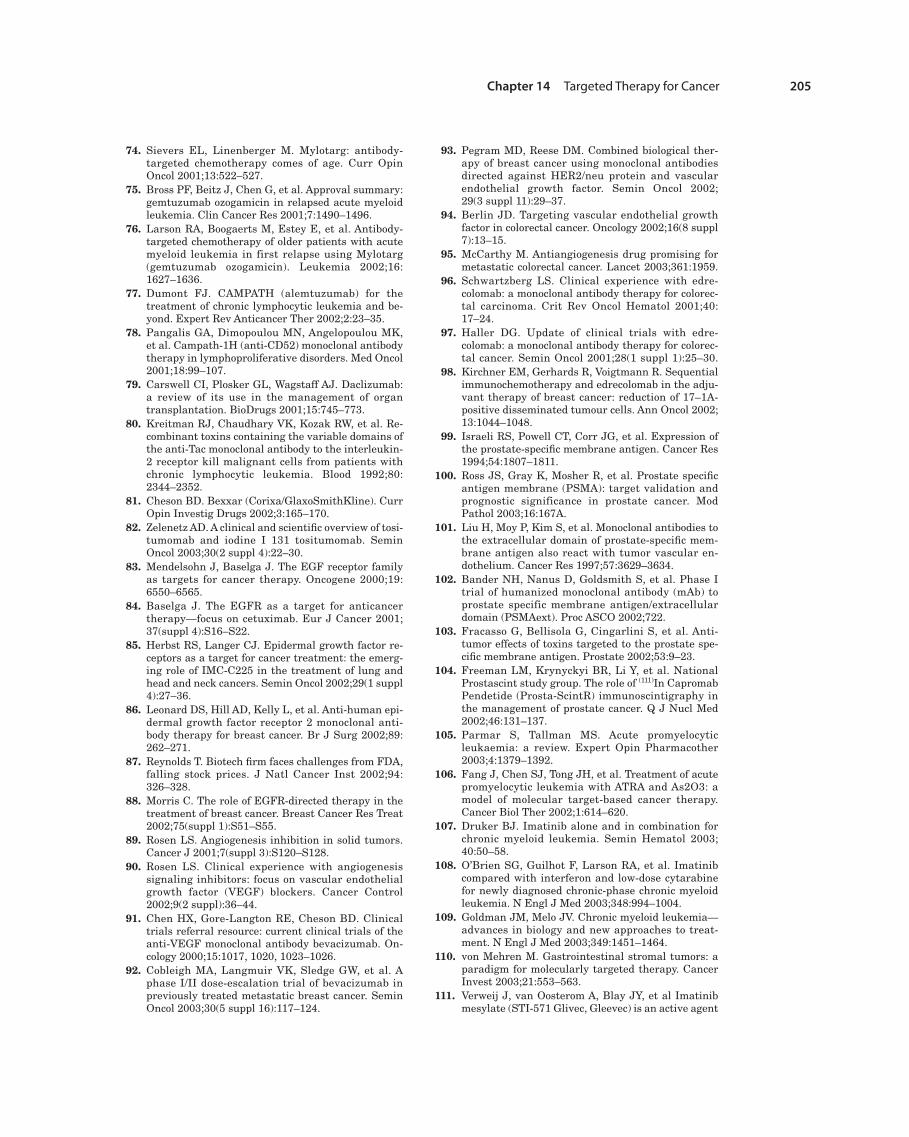
sensitive prostate cancer, and hormone refrac-tory metastatic disease.99–101 PSMA expressionis increased further in association with clini-cally advanced prostatic cancer, particularlyin hormone refractory disease, and is an idealsentinel molecule for use in targeting prostaticcancer cells. Increasing expression levels ofPSMA in resected primary prostate cancer isassociated with increased rates of subsequentdisease recurrence.100 In addition, significantPSMA expression has been identified in thetumor vasculature of a variety of nonprostatetumors, including breast cancer (FIG.14.3).101 Hu-manized and fully human antibodies specificfor the extracellular domain of PSMA havebeen developed. A phase I clinical trial of oneof these antibodies, huJ-591 conjugated with90Y, has yielded promising results.102 Pro-grams using toxin conjugates with anti-PSMAantibodies have completed preclinical devel-opment103 and are currently in early stageclinical trials for hormone-refractory advancedmetastatic prostate cancer. Finally, antibodiesto PSMA have been used as diagnostic imag-ing agents (FIG. 14.3), including the commerciallyavailable Prostascint®.104
Selected Targeted Anticancer TherapiesUsing Small Molecules
Table 14.3 lists selected small molecule drugsdesigned to target specific genetic events andbiologic pathways critical to cancer growthand progression.
ATRAArguably the first truly targeted therapyafter the development of hormonal therapyfor breast cancer was the development ofATRA for the treatment of acute promyelo-cytic leukemia, a subset of acute nonlympho-cytic leukemia featuring a disease-definingretinoic acid receptor activating t(15:17) recip-rocal translocation.105,106 For these selected pa-tients, direct targeting of the retinoic acidreceptor with ATRA has resulted in very highresponse rates, delay in disease progression,and long-term cures for these patients.105,106
Imatinib (Gleevec®)The development of imatinib for patients withchronic myelogenous leukemia in 2001 ush-ered in a new excitement both in the scientificand public communities for targeted anti-cancer therapy. Imatinib received fast-trackapproval by the FDA as an ATP-competitiveselective inhibitor of bcr-abl and has unprece-dented efficacy for the treatment of early stagechronic myelogenous leukemia typicallyachieving durable complete hematologic andcomplete cytogenetic remissions, with mini-mal toxicity.107–109 Imatinib is a true targetedtherapy for leukemia in that a test for thebcr/abl translocation must be performed be-fore a patient will be considered as eligible toreceive the drug.
Imatinib has also achieved regulatory ap-proval for the treatment of relapsed andmetastatic gastrointestinal stromal tumors(GISTs), which characteristically feature anactivating point mutation in the c-kit receptortyrosine kinase gene.110 For GISTs, the re-sponse to imatinib treatment appears to bepredictable based on the location of the c-kitmutation.111 The use of imatinib in GISTis also an example of targeted therapy as ameasurement of c-kit expression usually per-formed by IHC, required to confirm the di-agnosis and render the patient eligible fortreatment. Interestingly, most commerciallyavailable antibodies for c-kit recognize the
FIGURE 14.3 PSMA expression in non-prostate cancer. (Top) Tradi-tional bone scan demonstrating bilateral activity in the femur in-directly indicating the presence of metastatic renal cell carcinoma.(Bottom) 111I-huJ591EXT diagnostic immunoscintiscan of the samepatient showing direct localization of the anti-PSMA antibodyconjugate to the sites of metastatic renal cell carcinoma that fea-ture PSMA expression in the tumor neovasculature.

Chapter 14 Targeted Therapy for Cancer 201
an internal tandem duplication that creates anabnormal FLT-3 receptor that promotes thegrowth and survival of the leukemic cells.113–115
Three small molecule compounds are in clinicaltrials for the treatment of acute myelogenousleukemia by targeting the flt-3 internal tandemduplication (ITD). These drugs are also exam-ples of potential true targeted therapies in thata test for detecting an internal tandem duplica-tion that causes the flt-3 gene activation willlikely be required and incorporated into theFDAdrug approval label should these agents besuccessful in future clinical trials.
Gefitinib (Iressa®)Gefitinib was approved by the FDA in 2003 asmonotherapy for the treatment of patientswith locally advanced or metastatic non–smallcell lung cancer after failure of both platinumbased and docetaxel chemotherapies.116,117
total c-kit and do not distinguish the activatedor phosphorylated version, which is the actualtarget of imatinib.
Currently, the high treatment failure rateis directly linked to the test used to character-ize the patients. It is anticipated that eitherthe use of specific antibodies designed to iden-tify the activated c-kit gene or directed se-quencing of the c-kit gene may be requiredbefore imatinib is prescribed for patients withrecurrent or metastatic GIST. Although c-kitactivation has not been linked to breast can-cer, the platelet derived growth factor �, an-other target of imatinib, has been associatedwith breast cancer biology.112
FLT-3 Targeted TherapyIn approximately 30% of cases of acute mye-logenous leukemia and less frequently in otherforms of leukemia, a flt-3 gene mutation creates
Table 14.3 Selected Small Molecule Drugs Designed to Target Specific Genetic Events and Biologic Pathways Critical to CancerGrowth and Progression
Clinical DevelopmentTarget Drug Source Status Comment
PML-RAR-� ATRA Promega Approved First true targeted therapy sincein PML the introduction of ER testing and
hormonal therapy for breast cancer
bcr/abl Imatinib Novartis Approved Has emerged as standard of carein CML for early stage CML
c-kit in GIST Imatinib Novartis Approved Responses in relapsed/metastaticPDGF-� GIST can be predicted by the location
of the activating c-kit mutation
Flt-3 in AML SU5416 Pfizer Early stage Small molecule drugs that targetPKC412 Novartis clinical trials the flt-3 internal tandem MLN-518 Millennium duplication seen in 30% of AML
EGFR in NSCLC Gefitinib Astra Zeneca Approved Preclinical activity in breast cancer; clinical trials are ongoing
EGFR in Erlotinib Genentech/OSI Pending In late stage trials in NSCLC and glioblastoma recently (ASCO 2003) shown
efficacy in treatment of high grade malignant gliomas
Antiangiogenesis Thalidomide Celgene Pending Thalidomide is approved for SU 5416 Pfizer/Sugen treatment of leprosy and widely ZD6474 Astra Zeneca used to treat multiple myeloma;Endostatin Entremed other agents are in early and Marimastat British Biotech mid-stage clinical trialsOthers Others
Bcl-2 G3139 Genta Pending Antisense oligonucleotide targetsthe antiapoptotic gene, bcl-2
Proteasome in Bortezomib Millennium Approved Proteasome inhibition effectivemultiple myeloma in hematologic malignancies, but
of uncertain potential for thetreatment of solid tumors
AML, acute myelogenous leukemia; CML, chronic myelogenous leukemia; NSCLC, non–small cell lung cancer; PDGF, platelet derived growth factor; PML, acutepromyelocytic leukemia; RAR, retinoic acid receptor.

202 MOLECULAR ONCOLOGY OF BREAST C ANCER
Gefitinib is a small molecule drug that tar-gets the EGFR. In contrast with the approvalof trastuzumab, the approval of gefitinib didnot include an eligibility requirement refer-ence to a specific tumor diagnostic test de-signed to select patients that were more likelyto respond to the drug. Overexpression ofEGFR typically identified by IHC is extremelycommon in both lung and breast cancers,116–118
but in contrast with HER-2 overexpression,which is virtually limited to cases with geneamplification, multiple mechanisms of dysreg-ulation of EGFR and associated activation ofsignaling pathways have been described forboth of these tumors (see Chapter 17).116–118
Thus, it has been difficult to develop this drugfor expanded indications or combination thera-pies in the absence of a well-defined efficacytest. However, more recently, two independentgroups reported their similar discovery of aspecific activating mutation in the tyrosine ki-nase domain of the EGFR receptor that was as-sociated with a high response of patients withnon-small cell lung cancer to gefitinib.119–120
The clinical significance of this important find-ing for the development of gefitinib in breastcancer is currently unknown. Preclinical stud-ies of gefitinib have demonstrated activity ionbreast cancer cell lines,118 and clinical trialsusing the drug in combination with standardcytotoxic drugs are underway (see Chapter 17).
Erlotinib (Tarceva®)Erlotinib is another targeted inhibitor ofEGFR currently in late stage clinical trials forthe treatment of non–small cell lung cancerand pancreatic cancer.121,122 Clinical studies oferlotinib in breast cancer are ongoing (seeChapter 17). Erlotinib has shown efficacy inpreclinical models of brain tumors123 and hasrecently shown promising results in the treat-ment of high grade malignant gliomas. Todate, similar to gefitinib, the clinical trials forerlotinib have not included an assessment ofthe EGFR status or other diagnostic test foreligibility to receive the drug.
Antiangiogenesis (SU5416, Thalidomide,Endostatin/Angiostatin, and Marimastat)A variety of small molecule drugs is currentlyin clinical trials for breast cancer and othermalignancies that target the establishmentand growth of tumor blood vessels.124–127
Additional compounds that target matrix me-talloproteases, such as the drug marimastat,are also considered to be angiogenesis in-hibitors.128,129 To date, none of these compoundshas linked a diagnostic test such as tumormicrovessel density or the expression of an an-giogenesis promoting gene or protein in theirclinical development plans. Matrix metallopro-tease inhibitors are discussed in Chapter 18,and antiangiogenesis therapies are discussedin detail in Chapter 19.
G3139 (Genasense®)Another emerging strategy in anticancertherapy is the targeting of chemotherapyresistance by overcoming the antiapoptosismechanisms of cancer cells. An example of thisapproach is the novel antisense oligonu-cleotide G3139, which targets the antiapop-totic gene bcl-2.130,131 This agent has beentested mostly in hematologic malignanciesand has not been used widely in either pre-clinical experiments or clinical trials in breastcancer. Therapeutic strategies targeting apop-tosis are covered in depth in Chapter 21.
Bortezomib (Velcade®)Recently, drugs targeting the proteasome havebeen developed that are designed to impactdownstream pathways regulating angiogene-sis, tumor growth, adhesion, and resistance toapoptosis.132,133 One of these agents, borte-zomib (PS-341), has recently been approvedfor the treatment of advanced refractory mul-tiple myeloma.134 Bortezomib has shown pre-clinical activity in breast cancer as a singleagent and is being tested in combination ther-apy strategies in multiple clinical trials.135
Proteasome biology and proteasome inhibitorsare discussed in detail in Chapter 24.
The Future Is Now: Pharmacogenomicsand Personalized Medicine
Targeted therapy in oncology has been a majorstimulus for the evolving field of pharmacoge-nomics (see Chapter 28). In its broadest defini-tion, pharmacogenomics can encompass bothgermline and somatic (disease) gene and pro-tein measurements used to predict the likeli-hood that a patient will respond to a specificsingle or multiagent chemotherapy regimen

Chapter 14 Targeted Therapy for Cancer 203
17. Jordan VC. Antiestrogens and selective estrogenreceptor modulators as multifunctional medicines.1. Receptor interactions. J Med Chem 2003;46:883–908.
18. Jordan VC. Antiestrogens and selective estrogenreceptor modulators as multifunctional medicines.2. Clinical considerations and new agents. J MedChem 2003;46:1081–1111.
19. Rubnitz JE, Pui CH. Molecular diagnostics in thetreatment of leukemia. Curr Opin Hematol 1999;6:229–235.
20. Gleissner B, Thiel E. Detection of immunoglobu-lin heavy chain gene rearrangements in hemato-logic malignancies. Expert Rev Mol Diagn 2001;1:191–200.
21. Grimwade D, Lo Coco F. Acute promyelocyticleukemia: a model for the role of molecular diagno-sis and residual disease monitoring in directingtreatment approach in acute myeloid leukemia.Leukemia 2002;16:1959–1973.
22. Reichert JM. Monoclonal antibodies in the clinic.Nat Biotechnol 2001;19:819–822.
23. Kiyoi H, Naoe T. FLT3 in human hematologic malig-nancies. Leuk Lymph 2002;43:1541–1547.
24. Ross JS, Fletcher JA, Linette GP, et al. TheHer-2/neu gene and protein in breast cancer 2003:biomarker and target of therapy. Oncologist 2003;8:307–325.
25. Slamon DJ, Leyland-Jones B, Shak S, et al. Useof chemotherapy plus a monoclonal antibodyagainst HER2 for metastatic breast cancer thatoverexpresses HER2. N Engl J Med 2001;344:783–792.
26. Schnitt SJ, Jacobs TW. Current status of HER2 test-ing: caught between a rock and a hard place. Am JClin Pathol 2001;116:806–810.
27. Hayes DF, Thor AD. c-erbB-2 in breast cancer: devel-opment of a clinically useful marker. Semin Oncol2002;29:231–245.
28. Masood S, Bui MM. Prognostic and predictive valueof HER2/neu oncogene in breast cancer. Microsc ResTech 2002;59:102–108.
29. Paik S, Tan-chui E, Bryan J, et al. Successful qualityassurance program for HER-2 testing in the NSAPBtrial for Herceptin. Breast Cancer Res Treat 2002;76(suppl 1):S31.
30. Wang S, Saboorian MH, Frenkel EP, et al. Assess-ment of HER-2/neu status in breast cancer. Auto-mated Cellular Imaging System (ACIS)-assistedquantitation of immunohistochemical assay achieveshigh accuracy in comparison with fluorescence insitu hybridization assay as the standard. Am J ClinPathol 2001;116:495–503.
31. Wang S, Saboorian MH, Frenkel E, et al. Laboratoryassessment of the status of Her-2/neu protein andoncogene in breast cancer specimens: comparison ofimmunohistochemistry assay with fluorescence insitu hybridization assays. J Clin Pathol 2000;53:374–381.
32. Tanner M, Gancberg D, Di Leo A, et al. Chromogenicin situ hybridization: a practical alternative for fluo-rescence in situ hybridization to detect HER–2/neuoncogene amplification in archival breast cancersamples. Am J Pathol 2000;157:1467–1472.
33. Zhao J, Wu R,AuA, et al. Determination of HER2 geneamplification by chromogenic in situ hybridization
and to predict the risk of toxic side ef-fects.136,137 During the next several years, thefield of oncology drug development will see nu-merous products pass through the approvalprocess and enter the market accompanied bydiagnostic tests designed to “personalize” theiruse, dosage, route of administration, andlength of treatment for each patient, one at atime. Only time will tell whether this new ap-proach to anticancer pharmaceuticals willyield breakthrough results, reducing morbid-ity and mortality and improving outcomes forall who will be afflicted with the disease.
References1. O’Dwyer ME, Druker BJ. Chronic myelogenous
leukaemia—new therapeutic principles. J InternMed 2001;250:3–9.
2. Mauro MJ, Druker BJ. STI571: targeting BCR-ABLas therapy for CML. Oncologist 2001;6:233–238.
3. Lemonick MD, Park A. New hope for cancer. Time2001;157:62–69.
4. Brown E, Lewis PH, Nocera J. In search of the silverbullet. Fortune 2001;143:166–170.
5. Amos J, Patnaik M. Commercial molecular di-agnostics in the U.S.: the Human Genome Projectto the clinical laboratory. Hum Mutat 2002;19:324–333.
6. Bottles K. A revolution in genetics: changing medi-cine, changing lives. Physician Exec 2001;27:58–63.
7. Evans WE, McLeod HL. Pharmacogenomics—drugdisposition, drug targets, and side effects. N Engl JMed 2003;348:538–549.
8. Weinshilboum R. Inheritance and drug response.N Engl J Med 2003;348:529–537.
9. Osborne CK. Steroid hormone receptors in breastcancer management. Breast Cancer Res Treat 1998;51:227–238.
10. Wilbur DC, Willis J, Mooney RA, et al. Estrogen andprogesterone detection in archival formalin-fixedparaffin embedded tissue from breast carcinoma: acomparison of immunocytochemistry with dextrancoated charcoal assay. Mod Pathol 1992;5:79–84.
11. Ciocca DR, Elledge R. Molecular markers for pre-dicting response to tamoxifen in breast cancerpatients. Endocrine 2000;13:1–10.
12. Jordan VC. Tamoxifen: a most unlikely pioneeringmedicine. Nat Rev Drug Discov 2003;2:205–213.
13. Locker GY. Hormonal therapy of breast cancer. Can-cer Treat Rev 1998;24:221–240.
14. Ibrahim NK, Hortobagyi GN. The evolving role ofspecific estrogen receptor modulators (SERMs) SurgOncol 1999;8:103–123.
15. Miller WR, Anderson TJ, Dixon JM. Anti-tumoreffects of letrozole. Cancer Invest 2002;20:15–21.
16. Buzdar AU, Robertson JF, Eiermann W, et al. Anoverview of the pharmacology and pharmacokineticsof the newer generation aromatase inhibitors anas-trozole, letrozole, and exemestane. Cancer 2002;95:2006–2016.

204 MOLECULAR ONCOLOGY OF BREAST C ANCER
(CISH) in archival breast carcinoma. Mod Pathol2002;15:657–665.
34. Hortobagyi GN. Overview of treatment results withtrastuzumab (Herceptin) in metastatic breast can-cer. Semin Oncol 2001;28:43–47.
35. McKeage K, Perry CM. Trastuzumab: a review of itsuse in the treatment of metastatic breast canceroverexpressing HER2. Drugs 2002;62:209–243.
36. Shawver LK, Slamon D, Ullrich A. Smart drugs: ty-rosine kinase inhibitors in cancer therapy. CancerCell 2002;1:117–123.
37. Ligibel JA, Winer EP. Trastuzumab/chemotherapycombinations in metastatic breast cancer. SeminOncol 2002;29:38–43.
38. Mass RD, Press MF, Anderson S, et al. Improved sur-vival benefit from Herceptin (trastuzumab) in pa-tients selected by fluorescence in situ hybridization(FISH). Proc Am Soc Clin Oncol 2001;85.
39. Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacyand safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastaticbreast cancer. J Clin Oncol 2002;20:719–726.
40. Seidman AD, Fornier MN, Esteva FJ, et al. Weeklytrastuzumab and paclitaxel therapy for metastaticbreast cancer with analysis of efficacy by HER2 im-munophenotype and gene amplification. J ClinOncol 2001;19:2587–2595.
41. Fornier M, Risio M, Van Poznak C, et al. HER-2 test-ing and correlation with efficacy in trastuzumabtherapy. Oncology 2003;16:1340–1358.
42. Carter P. Improving the efficacy of antibody-basedcancer therapies. Nat Rev Cancer 2001;1:118–129.
43. Goldenberg DM. Targeted therapy of cancer with ra-diolabeled antibodies. J Nucl Med 2002;43:693–713.
44. Reichert JM. Therapeutic monoclonal antibodies:trends in development and approval in the US. CurrOpin Mol Ther 2002;4:110–118.
45. Ross JS, Gray K, Gray GS, et al. Anticancer antibod-ies. Am J Clin Pathol 2003;119:472–485.
46. Hemminki A. From molecular changes to customisedtherapy. Eur J Cancer 2002;38:333–338.
47. Milenic DE. Monoclonal antibody-based therapystrategies: providing options for the cancer patient.Curr Pharm Des 2002;8:1749–1764.
48. Reilly RM, Sandhu J, Alvarez-Diez TM, et al.Problems of delivery of monoclonal antibodies. Phar-maceutical and pharmacokinetic solutions. ClinPharmacokinet 1995;28:126–142.
49. Winter G, Harris WJ. Humanized antibodies. Im-munol Today 1993;14:243–246.
50. Merluzzi S, Figini M, Colombatti A, et al. Human-ized antibodies as potential drugs for therapeuticuse. Adv Clin Path 2000;4:77–85.
51. Kuus-Reichel K, Grauer LS, Karavodin LM, et al.Will immunogenicity limit the use, efficacy, and fu-ture development of therapeutic monoclonal anti-bodies? Clin Diagn Lab Immunol 1994;1:365–372.
52. Pimm MV. Possible consequences of human antibodyresponses on the biodistribution of fragments ofhuman, humanized or chimeric monoclonal antibod-ies: a note of caution. Life Sci 1994;55:PL45–PL49.
53. Jones PT, Dear PH, Foote J, et al. Replacing the com-plementarity-determining regions in a human anti-body with those from a mouse. Nature 1986;321:522–525.
54. Isaacs JD. From bench to bedside: discovering rulesfor antibody design, and improving serotherapy
with monoclonal antibodies. Rheumatology 2001;40:724–738.
55. Watkins NA, Ouwehand WH. Introduction to anti-body engineering and phage display. Vox Sang 2000;78:72–79.
56. Reff ME, Hariharan K, Braslawsky G. Future ofmonoclonal antibodies in the treatment of hemato-logic malignancies. Cancer Control 2002;9:152–166.
57. Chester KA, Hawkins RE. Clinical issues in anti-body design. Trends Biotechnol 1995;13:294–300.
58. Reff ME, Heard C. A review of modifications to re-combinant antibodies: attempt to increase efficacy inoncology applications. Crit Rev Oncol Hematol 2001;40:25–35.
59. Nielsen UB, Marks JD. Internalizing antibodies andtargeted cancer therapy: direct selection from phagedisplay libraries. PSTT 2000;3:282–291.
60. Burke JM, Jurcic JG, Scheinberg DA. Radioim-munotherapy for acute leukemia. Cancer Control2002;9:106–113.
61. Linenberger ML, Maloney DG, Bernstein ID.Antibody-directed therapies for hematological ma-lignancies. Trends Mol Med 2002;8:69–76.
62. Stevenson GT, Anderson VA, Leong WS. Engineeredantibody for treating lymphoma. Recent ResultsCancer Res 2002;159:104–112.
63. Wiseman GA, Gordon LI, Multani PS, et al. Ibritu-momab tiuxetan radioimmunotherapy for patientswith relapsed or refractory non-Hodgkin lymphomaand mild thrombocytopenia: a phase II multicentertrial. Blood 2002;99:4336–4342.
64. Dillman RO. Monoclonal antibody therapy for lym-phoma: an update. Cancer Pract 2001;9:71–80.
65. Grillo-Lopez AJ, Hedrick E, Rashford M, et al. Ri-tuximab: ongoing and future clinical development.Semin Oncol 2002;29(1 suppl 2):105–112.
66. Coiffier B. Rituximab in the treatment of dif-fuse large B-cell lymphomas. Semin Oncol 2002;29(1 suppl 2):30–35.
67. Grillo-Lopez AJ. AntiCD20 mAbs: modifying thera-peutic strategies and outcomes in the treatment oflymphoma patients. Expert Rev Anticancer Ther2002;2:323–329.
68. Krasner C, Joyce RM. Zevalin: 90yttrium labeledanti-CD20 (ibritumomab tiuxetan), a new treatmentfor non-Hodgkin’s lymphoma. Curr Pharm Biotech-nol 2001;2:341–349.
69. Gordon LI, Witzig TE, Wiseman GA, et al. Yttrium90 ibritumomab tiuxetan radioimmunotherapy forrelapsed or refractory low-grade non-Hodgkin’s lym-phoma. Semin Oncol 2002;29(1 suppl 2):87–92.
70. Wagner HN Jr, Wiseman GA, Marcus CS, et al. Ad-ministration guidelines for radioimmunotherapy ofnon-Hodgkin’s lymphoma with (90)Y-labeled antiCD20 monoclonal antibody. J Nucl Med 2002;43:267–272.
71. Dillman RO. Radiolabeled anti-CD20 monoclonalantibodies for the treatment of B-cell lymphoma.J Clin Oncol 2002;20:3545–3557.
72. Stadtmauer EA. Trials with gemtuzumab ozogam-icin (Mylotarg®) combined with chemotherapy regi-mens in acute myeloid leukemia. Clin Lymphoma2002;2(suppl 1):S24–S28.
73. Nabhan C, Tallman MS. Early phase I/II trialswith gemtuzumab ozogamicin (Mylotarg®) in acutemyeloid leukemia. Clin Lymph 2002;2(suppl 1):S19–S23.
Chapter 14 Targeted Therapy for Cancer 205
93. Pegram MD, Reese DM. Combined biological ther-apy of breast cancer using monoclonal antibodiesdirected against HER2/neu protein and vascularendothelial growth factor. Semin Oncol 2002;29(3 suppl 11):29–37.
94. Berlin JD. Targeting vascular endothelial growthfactor in colorectal cancer. Oncology 2002;16(8 suppl7):13–15.
95. McCarthy M. Antiangiogenesis drug promising formetastatic colorectal cancer. Lancet 2003;361:1959.
96. Schwartzberg LS. Clinical experience with edre-colomab: a monoclonal antibody therapy for colorec-tal carcinoma. Crit Rev Oncol Hematol 2001;40:17–24.
97. Haller DG. Update of clinical trials with edre-colomab: a monoclonal antibody therapy for colorec-tal cancer. Semin Oncol 2001;28(1 suppl 1):25–30.
98. Kirchner EM, Gerhards R, Voigtmann R. Sequentialimmunochemotherapy and edrecolomab in the adju-vant therapy of breast cancer: reduction of 17–1A-positive disseminated tumour cells. Ann Oncol 2002;13:1044–1048.
99. Israeli RS, Powell CT, Corr JG, et al. Expression ofthe prostate-specific membrane antigen. Cancer Res1994;54:1807–1811.
100. Ross JS, Gray K, Mosher R, et al. Prostate specificantigen membrane (PSMA): target validation andprognostic significance in prostate cancer. ModPathol 2003;16:167A.
101. Liu H, Moy P, Kim S, et al. Monoclonal antibodies tothe extracellular domain of prostate-specific mem-brane antigen also react with tumor vascular en-dothelium. Cancer Res 1997;57:3629–3634.
102. Bander NH, Nanus D, Goldsmith S, et al. Phase Itrial of humanized monoclonal antibody (mAb) toprostate specific membrane antigen/extracellulardomain (PSMAext). Proc ASCO 2002;722.
103. Fracasso G, Bellisola G, Cingarlini S, et al. Anti-tumor effects of toxins targeted to the prostate spe-cific membrane antigen. Prostate 2002;53:9–23.
104. Freeman LM, Krynyckyi BR, Li Y, et al. NationalProstascint study group. The role of (111)In CapromabPendetide (Prosta-ScintR) immunoscintigraphy inthe management of prostate cancer. Q J Nucl Med2002;46:131–137.
105. Parmar S, Tallman MS. Acute promyelocyticleukaemia: a review. Expert Opin Pharmacother2003;4:1379–1392.
106. Fang J, Chen SJ, Tong JH, et al. Treatment of acutepromyelocytic leukemia with ATRA and As2O3: amodel of molecular target-based cancer therapy.Cancer Biol Ther 2002;1:614–620.
107. Druker BJ. Imatinib alone and in combination forchronic myeloid leukemia. Semin Hematol 2003;40:50–58.
108. O’Brien SG, Guilhot F, Larson RA, et al. Imatinibcompared with interferon and low-dose cytarabinefor newly diagnosed chronic-phase chronic myeloidleukemia. N Engl J Med 2003;348:994–1004.
109. Goldman JM, Melo JV. Chronic myeloid leukemia—advances in biology and new approaches to treat-ment. N Engl J Med 2003;349:1451–1464.
110. von Mehren M. Gastrointestinal stromal tumors: aparadigm for molecularly targeted therapy. CancerInvest 2003;21:553–563.
111. Verweij J, van Oosterom A, Blay JY, et al Imatinibmesylate (STI-571 Glivec, Gleevec) is an active agent
74. Sievers EL, Linenberger M. Mylotarg: antibody-targeted chemotherapy comes of age. Curr OpinOncol 2001;13:522–527.
75. Bross PF, Beitz J, Chen G, et al. Approval summary:gemtuzumab ozogamicin in relapsed acute myeloidleukemia. Clin Cancer Res 2001;7:1490–1496.
76. Larson RA, Boogaerts M, Estey E, et al. Antibody-targeted chemotherapy of older patients with acutemyeloid leukemia in first relapse using Mylotarg(gemtuzumab ozogamicin). Leukemia 2002;16:1627–1636.
77. Dumont FJ. CAMPATH (alemtuzumab) for thetreatment of chronic lymphocytic leukemia and be-yond. Expert Rev Anticancer Ther 2002;2:23–35.
78. Pangalis GA, Dimopoulou MN, Angelopoulou MK,et al. Campath-1H (anti-CD52) monoclonal antibodytherapy in lymphoproliferative disorders. Med Oncol2001;18:99–107.
79. Carswell CI, Plosker GL, Wagstaff AJ. Daclizumab:a review of its use in the management of organtransplantation. BioDrugs 2001;15:745–773.
80. Kreitman RJ, Chaudhary VK, Kozak RW, et al. Re-combinant toxins containing the variable domains ofthe anti-Tac monoclonal antibody to the interleukin-2 receptor kill malignant cells from patients withchronic lymphocytic leukemia. Blood 1992;80:2344–2352.
81. Cheson BD. Bexxar (Corixa/GlaxoSmithKline). CurrOpin Investig Drugs 2002;3:165–170.
82. Zelenetz AD. A clinical and scientific overview of tosi-tumomab and iodine I 131 tositumomab. SeminOncol 2003;30(2 suppl 4):22–30.
83. Mendelsohn J, Baselga J. The EGF receptor familyas targets for cancer therapy. Oncogene 2000;19:6550–6565.
84. Baselga J. The EGFR as a target for anticancertherapy—focus on cetuximab. Eur J Cancer 2001;37(suppl 4):S16–S22.
85. Herbst RS, Langer CJ. Epidermal growth factor re-ceptors as a target for cancer treatment: the emerg-ing role of IMC-C225 in the treatment of lung andhead and neck cancers. Semin Oncol 2002;29(1 suppl4):27–36.
86. Leonard DS, Hill AD, Kelly L, et al. Anti-human epi-dermal growth factor receptor 2 monoclonal anti-body therapy for breast cancer. Br J Surg 2002;89:262–271.
87. Reynolds T. Biotech firm faces challenges from FDA,falling stock prices. J Natl Cancer Inst 2002;94:326–328.
88. Morris C. The role of EGFR-directed therapy in thetreatment of breast cancer. Breast Cancer Res Treat2002;75(suppl 1):S51–S55.
89. Rosen LS. Angiogenesis inhibition in solid tumors.Cancer J 2001;7(suppl 3):S120–S128.
90. Rosen LS. Clinical experience with angiogenesissignaling inhibitors: focus on vascular endothelialgrowth factor (VEGF) blockers. Cancer Control2002;9(2 suppl):36–44.
91. Chen HX, Gore-Langton RE, Cheson BD. Clinicaltrials referral resource: current clinical trials of theanti-VEGF monoclonal antibody bevacizumab. On-cology 2000;15:1017, 1020, 1023–1026.
92. Cobleigh MA, Langmuir VK, Sledge GW, et al. Aphase I/II dose-escalation trial of bevacizumab inpreviously treated metastatic breast cancer. SeminOncol 2003;30(5 suppl 16):117–124.
206 MOLECULAR ONCOLOGY OF BREAST C ANCER
for gastrointestinal stromal tumours, but does notyield responses in other soft-tissue sarcomas thatare unselected for a molecular target. Results froman EORTC Soft Tissue and Bone Sarcoma Groupphase II study. Eur J Cancer 2003;39:2006–2011.
112. de Jong JS, van Diest PJ, van der Valk P, et al. Ex-pression of growth factors, growth-inhibiting factors,and their receptors in invasive breast cancer. II.Correlations with proliferation and angiogenesis.J Pathol 1998;184:53–57.
113. Gilliland DG, Griffin JD. The roles of FLT3 inhematopoiesis and leukemia. Blood 2002;100:1532–1542.
114. Sawyers CL. Finding the next Gleevec: FLT3 tar-geted kinase inhibitor therapy for acute myeloidleukemia. Cancer Cell 2002;1:413–415.
115. Kelly LM, Yu JC, Boulton CL, et al. CT53518, a novelselective FLT3 antagonist for the treatment of acutemyelogenous leukemia (AML). Cancer Cell 2002;1:421–432.
116. Schiller JH. New directions for ZD1839 in the treat-ment of solid tumors. Semin Oncol 2003;30(1 suppl1):49–55.
117. Ranson M. ZD1839 (Iressa): for more than just non-small cell lung cancer. Oncologist 2002;7(suppl 4):16–24.
118. Campiglio M, Locatelli A, Olgiati C, et al. Inhibitionof proliferation and induction of apoptosis in breastcancer cells by the epidermal growth factor receptor(EGFR) tyrosine kinase inhibitor ZD1839 (“Iressa”)is independent of EGFR expression level. J CellPhysiol 2004;198:259–268.
119. Paez JG, Janne PA, Lee JC, et al. EGFR mutationsin lung cancer: Correlation with clinical response togefitinib therapy. Science 2004;304:1497–1500.
120. Lynch TJ, Bell DW, Sordella R et al. Activatingmutations in the epidermal growth factor receptorunderlying responsiveness of non-small-cell lungcancer to Gefitinib. N Engl J Med 2004;350:2129–2139.
121. Bonomi P. Erlotinib: a new therapeutic approach fornon-small cell lung cancer. Expert Opin InvestDrugs 2003;12:1395–1401.
122. Khalil MY, Grandis JR, Shin DM. Targeting epider-mal growth factor receptor: novel therapeutics in themanagement of cancer. Expert Rev Anticancer Ther2003;3:367–380.
123. Newton HB. Molecular neuro-oncology and develop-ment of targeted therapeutic strategies for braintumors. Part 1. Growth factor and Ras signaling
pathways. Expert Rev Anticancer Ther 2003;3:595–614.
124. Zogakis TG, Libutti SK. General aspects of anti-angiogenesis and cancer therapy. Expert Opin BiolTher 2001;1:253–275.
125. Thomas DA, Kantarjian HM. Current role of thalido-mide in cancer treatment. Curr Opin Oncol 2000;12:564–573.
126. Mendel DB, Laird AD, Smolich BD, et al. Develop-ment of SU5416, a selective small molecule inhibitorof VEGF receptor tyrosine kinase activity, as ananti-angiogenesis agent. Anticancer Drug Des 2000;15:29–41.
127. Dell’Eva R, Pfeffer U, Indraccolo S, et al. Inhibitionof tumor angiogenesis by angiostatin: from recombi-nant protein to gene therapy. Endothelium 2002;9:3–10.
128. Brown PD. Ongoing trials with matrix metallo-proteinase inhibitors. Expert Opin Investig Drugs2000;9:2167–2177.
129. Miller KD, Gradishar W, Schuchter L, et al. A ran-domized phase II pilot trial of adjuvant marimastatin patients with early-stage breast cancer. AnnOncol 2002;13:1220–1224.
130. Tolcher AW. Regulators of apoptosis as anticancertargets. Hematol Oncol Clin North Am 2002;16:1255–1267.
131. Tamm I, Dorken B, Hartmann G. Antisense therapyin oncology: new hope for an old idea? Lancet 2001;358:489–497.
132. Adams J. Development of the proteasome inhibitorPS-341. Oncologist 2002;7:9–16.
133. Elliott PJ, Ross JS. The proteasome: a new targetfor novel drug therapies. Am J Clin Pathol 2001;116:637–646.
134. Richardson PG, Barlogie B, Berenson J, et al. Aphase 2 study of bortezomib in relapsed, refractorymyeloma. N Engl J Med 2003;348:2609–2617.
135. Orlowski RZ, Dees EC. The role of the ubiquitination-proteasome pathway in breast cancer: applyingdrugs that affect the ubiquitin-proteasome pathwayto the therapy of breast cancer. Breast Cancer Res2003;5:1–7.
136. Weinstein JN. Pharmacogenomics—teaching olddrugs new tricks. N Engl J Med 2000;343:1408–1409.
137. Slonim DK. Transcriptional profiling in cancer: thepath to clinical pharmacogenomics. Pharmacoge-nomics 2001;2:123–136.