Embed Size (px)
Citation preview
05/03/2013
1
Thyr
oid
Can
cer
-SP
ECT
/CT
“To
D
o /
Not
to
”
HK MohanDepartment of Nuclear Medicine
Guys & St Thomas’ Hospitals, London
SPECT/CT in Thyroid cancerTo do / not to?
48 year old – PT3 N1bMO
• TSH = 88• Tg = 129• Pre therapy 185MBq I131 study
05/03/2013
2
48 year old – PT3 N1bMO• Post Surgery – 5.5 Gbq I1316 months later• TSH = 113• Tg = 1.1
Aided surgery
Liver uptake - Gall bladder. No MRI required
05/03/2013
3
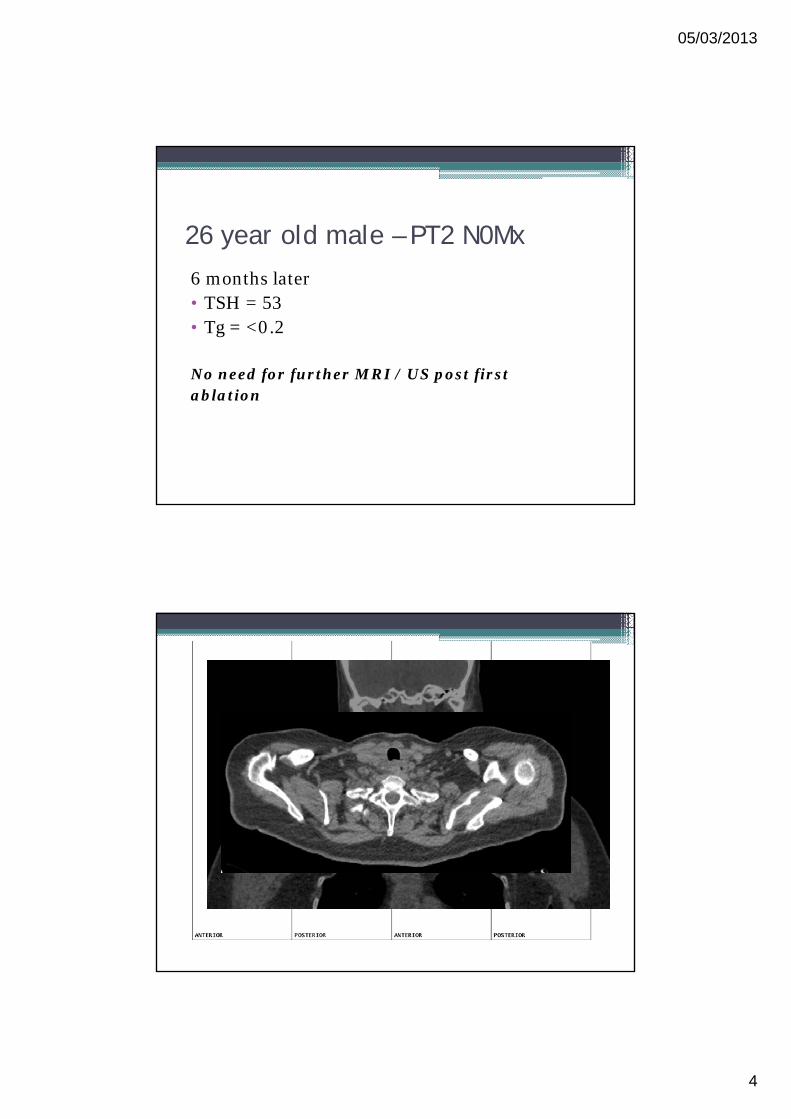
26 year old male – PT2 N0Mx
• TSH = 48• Tg = 12.9• 3.7 Gbq I131• Post Therapy imaging
05/03/2013
4
26 year old male – PT2 N0Mx
6 months later• TSH = 53• Tg = <0.2
No need for further MRI / US post firstablation
05/03/2013
5
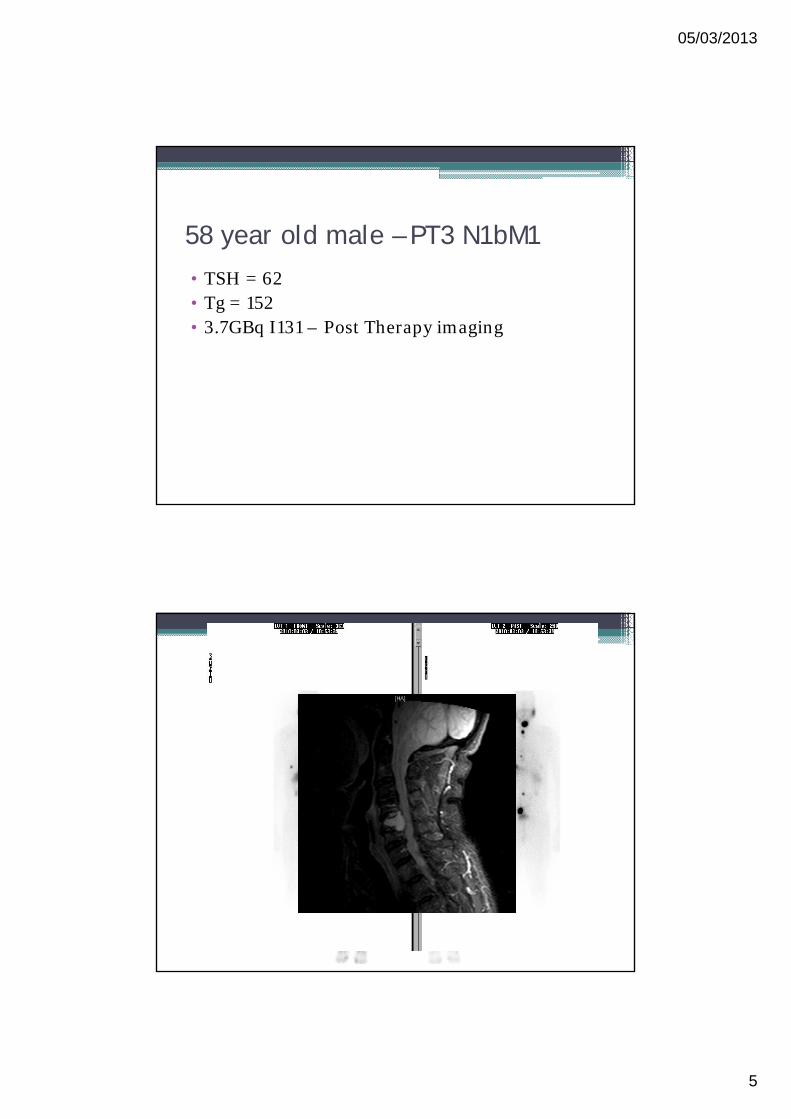
58 year old male – PT3 N1bM1
• TSH = 62• Tg = 152• 3.7GBq I131 – Post Therapy imaging
05/03/2013
6
58 year old male – PT3 N1bM1
6 months later pre second ablation• TSH = 77• Tg = 22• 5.5 GBq I131
Revealed destructive nature promptingfurther investigation and EBRT
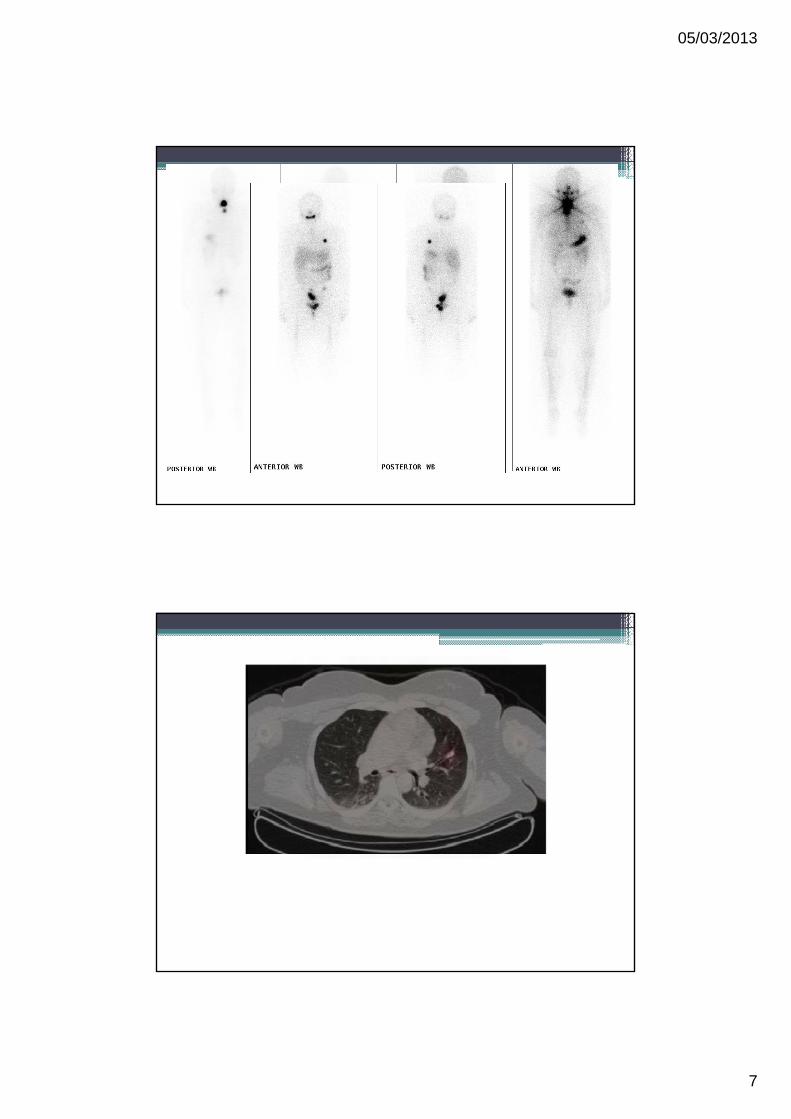
32 year old female – PT2 N0MO
• TSH = 52• Tg = 24• 5.5 Gbq I131- Post therapy study
05/03/2013
7
05/03/2013
8
32 year old female – PT2 N0MO
Prior to 4th ablation• TSH = 44• Tg = 1.8• 5.5 Gbq I131
Aided decision re surgery and monitoring response to therapy
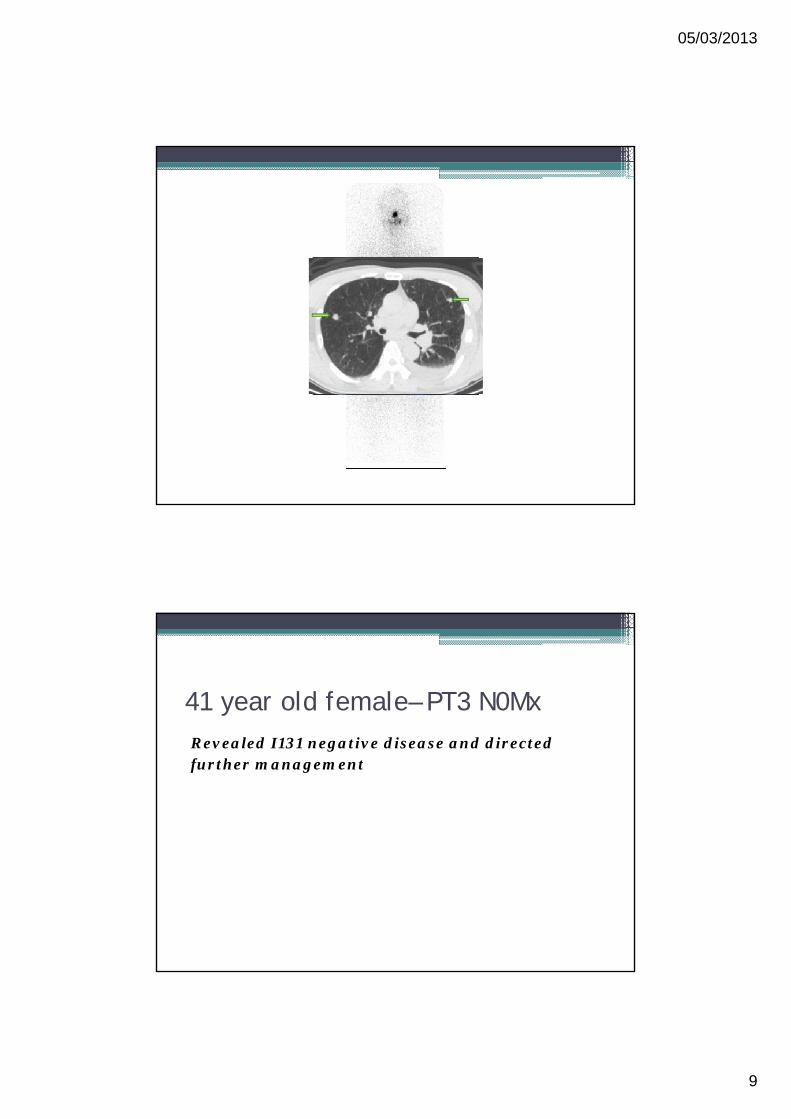
41 year old female– PT3 N0Mx
• TSH = 88• Tg = 152• 3.7 GBq I131 study
05/03/2013
9
41 year old female– PT3 N0MxRevealed I131 negative disease and directed further management
05/03/2013
10
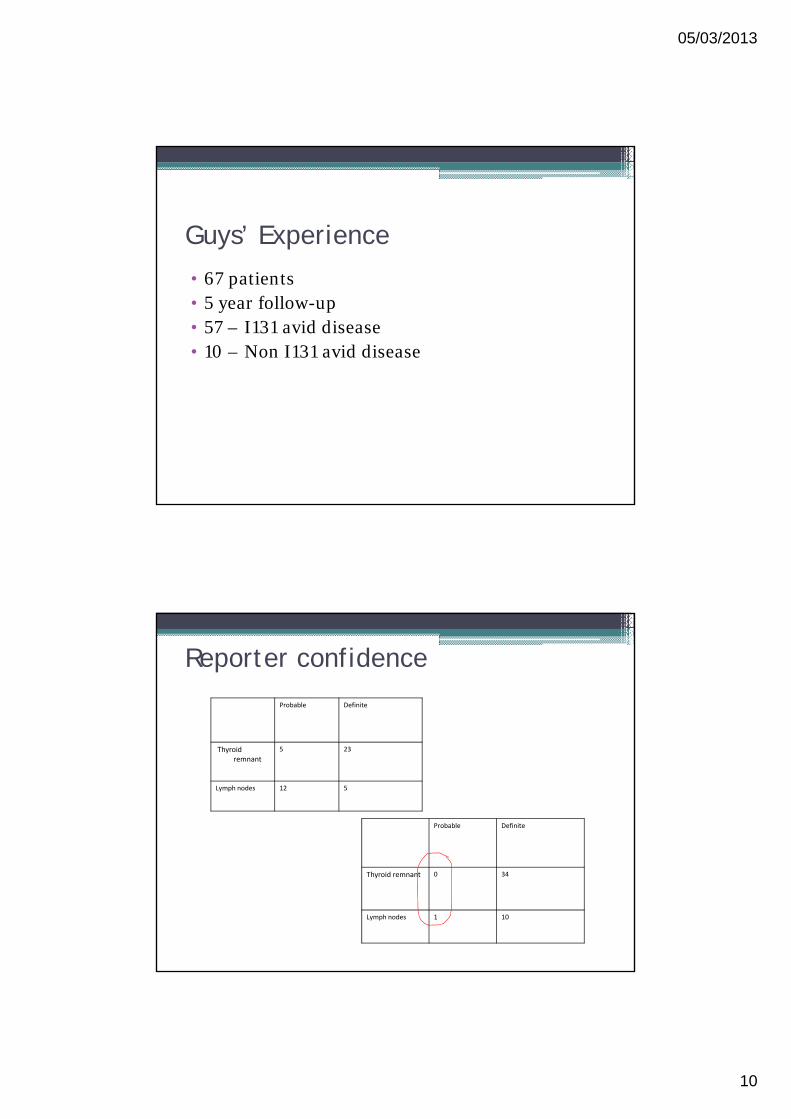
Guys’ Experience
• 67 patients• 5 year follow-up• 57 – I131 avid disease• 10 – Non I131 avid disease
Reporter confidence
Probable Definite
Thyroid remnant 0 34
Lymph nodes 1 10
Probable Definite
Thyroidremnant
5 23
Lymph nodes 12 5
05/03/2013
11
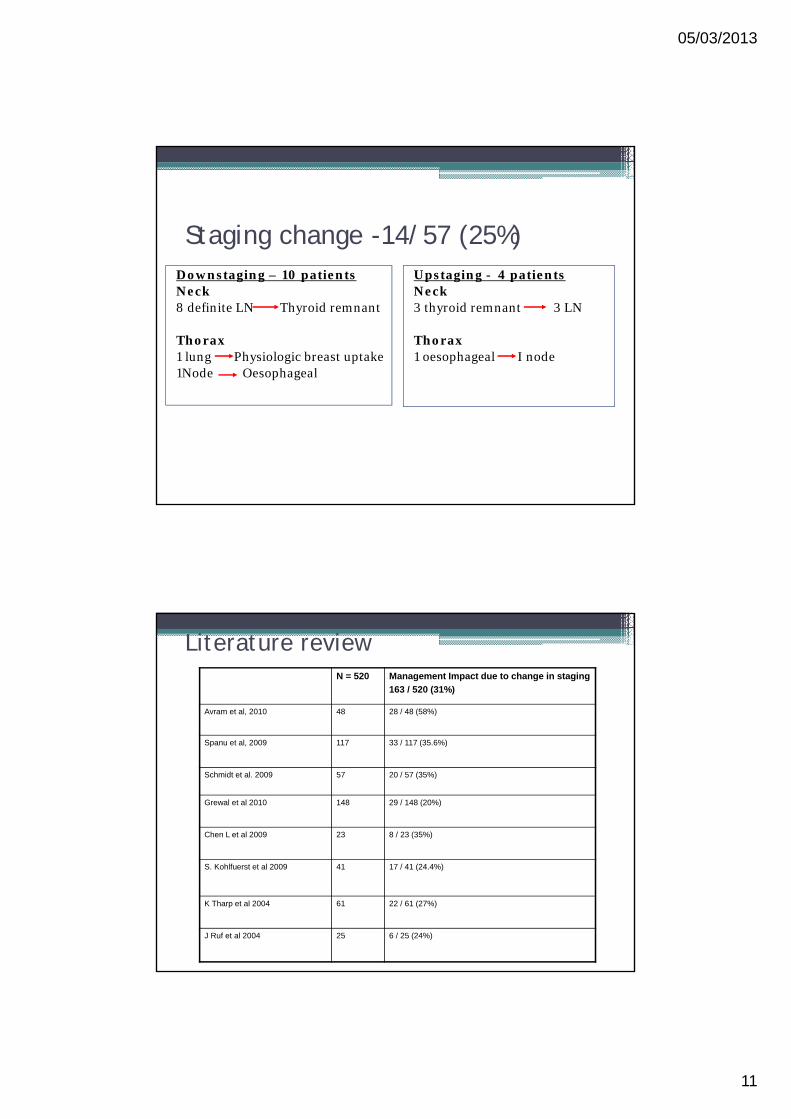
Staging change -14/57 (25%)Downstaging – 10 patientsNeck8 definite LN Thyroid remnant
Thorax1 lung Physiologic breast uptake1Node Oesophageal
Upstaging - 4 patientsNeck3 thyroid remnant 3 LN
Thorax1 oesophageal I node
Literature reviewN = 520 Management Impact due to change in staging
163 / 520 (31%)
Avram et al, 2010 48 28 / 48 (58%)
Spanu et al, 2009 117 33 / 117 (35.6%)
Schmidt et al. 2009 57 20 / 57 (35%)
Grewal et al 2010 148 29 / 148 (20%)
Chen L et al 2009 23 8 / 23 (35%)
S. Kohlfuerst et al 2009 41 17 / 41 (24.4%)
K Tharp et al 2004 61 22 / 61 (27%)
J Ruf et al 2004 25 6 / 25 (24%)
05/03/2013
12
Clinical ImpactDown staging
• Patient reassurance
• Efficient use of facilitiesAvoiding US / CT / MRI
• Reduced cost
Upstaging• Targetted surgery / EBRT
• Tailoring I131 dose• Reduced therapies
Reduced side effects
• Reduced recurrence rates
Improved survival
Significant incidental findings
Does is impact survival?
• >90% 10 yr survival• 43 % of all relapses in 1st year • 23 % years 2-5 • 9 % > 10 years
05/03/2013
13
PrognosisCR 10YS %
• Lung only 131 I +ve 46% 62 • Lung only 131 I -ve 11 • Lung + other (bone) 10
Impact on Survival
• Early days• 3-5 year followup currently available• Lymphnode metastases - Still has >90% 10 year
survival rate• Distant metastases 50 - 60% 10 year survival
rate • Non I131 avid disease - Limited treatment
options
2626
05/03/2013
14
Current indications for SPECT/CT
• High risk patients. • Iodine uptake in neck which is disproportionate
to initial disease and staging.• Any abnormal uptake outside neck for accurate
localisation and characterisation.• Patients with raised thyroglobulin with negative
iodine whole body scintigraphy.
Imaging protocol• Imaged 3-5 days post I131 administration
• WBSAnterior and Posterior whole body images Scanning speed - 3-8mm/sec
• SPECTHEHR collimatorMatrix size - 64 x 64. 64 projectionsProcessing – FBP and OSEM
• CT Voltage - 120 KV, Tube current - 100mAs/sliceSlice thickness -1.5mmCT dose exposure – 3 mSv
05/03/2013
15
Thanks for listening!!!
BTA / RCP - Guidelines for management of thyroid cancer, 2nd ed, 2007EANM - Guidelines for radioiodine therapy of differentiated thyroidcancer 2008