Embed Size (px)
DESCRIPTION
Cubital tunnel syndrome
Citation preview

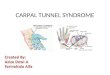
CUBITAL TUNNEL SYNDROME:
Diagnosis and Management

OUTLINE• Anatomy• Epidemiology • Clinical exam• Treatment options• Submuscular transposition technique• OITE relevant stuff• Statistics:
– Effect size– Meta-analysis

EPIDEMIOLOGY• Ulnar nerve compression at the elbow:
Second most common compression neuropathy of the upper limb
• Incidence: 25 per 100000 person years– USA: 75000 cases annually – World-wide: 1.5 million cases

HISTORY
• Treated surgically for the first time in 1816 by Henry Early

TREATMENT OPTIONS• Simple decompression• Medial epicondylectomy• Ulnar nerve transposition
– Subcutaneous– Intramuscular– Submuscular
ULNAR NERVE TRANSPOSITION IS THE MOST COMMON PROCEDURE (Dutch survey data)

PRO SIMPLE DECOMPRESSION
• Preserves blood supply to ulnar nerve• Shorter operation• Earlier recovery because anatomical
location of ulnar nerve is preserved

PRO TRANSPOSITION
• Only transposition addresses the dynamic compression of the ulnar nerve seen with elbow flexion

ANATOMY
• Osbornes ligament:– Between FCU heads where ulnar nerve
enters forearm • Struthers arcade
– Fascial thickening in medial upper arm intermuscular septum where ulnar nerve enters dorsal compartment

OSBORNE’S LIGAMENT


ARCADE OF STRUTHERS
INCIDENCE: 13.5%



STRUTHER’S LIGAMENT
-MEDIAN nerve passes between ligament and humerus and can be compressed
-Incidence: 1%
-Can be associated with bony spur visible on xrays
-Don’t confuse with Struther’s Arcade!!!

CLINICAL SIGNS
• Sensory changes in ulnar nerve distribution (little+ring finger)
• Intrinsic weakness (not always!)• Tinel’s sign at medial elbow• Elbow flexion test (3 min @ 120° flexion
reproduces symptoms)• Wartenberg’s sign • Fromment’s sign

AUTONOMOUS ULNAR NERVE SENSORY ZONE

• Most sensitive: 30 sec of elbow flexion in conjunction with direct pressure at ulnar nerve
93% SENSITIVITY

Wartenberg’s Sign
• Ulnar abduction of 5th digit due to due to intrinsic weakness and unopposed abduction by extensor digiti minimi (because of it’s slightly ulnar insertion)
• Don’t confuse with Wartenberg’s syndrome!

Wartenberg’s Syndrome
• Sensory RADIAL nerve neuritis• Pain in radial distal forearm

FROMMENT SIGN
• Can’t adduct thumb (ulnar nerve)• Flexes thumb IP joint instead (median nerve)

Martin-Gruber Anastomosis
• Median to ulnar nerve anastomosis• Mainly motor fibers• Incidence: 17%• Therefore intrinsic weakness not always
present in cubital tunnel syndrome

Is Nerve Compression or Traction causing
Symptoms?

BASIC SCIENCE
CLINICAL DATA


CROSS SECTION

Is Nerve Compression or Traction causing Symptoms?
Gelberman RH et al. Changes in interstitial pressure and cross-sectional area of the cubital tunnel and of the ulnar nerve with flexion of the elbow. JBJS Am. 1998


TRACTION IS THE PROBLEM - Simple decompression insufficient


LITERATURE REVIEW• A systematic review based on non-
randomized data • n=3024 patients in 60 studies• Potential selection bias: patients with less
severe symptoms were treated more frequently with simple decompression
Bartels RH, Menovsky T, Van Overbeeke JJ, Verhagen WI. Surgical management of ulnar nerve compression at the elbow: an analysis of the literature. J Neurosurg. 1998;89:722-7.

COMPRESSION IS THE PROBLEM
BETTER RESULTS WITH SIMPLE DECOPMPRESSION

BASIC SCIENCE: Traction is the problem!
CLINICAL DATA: Compression is the
problem!


PURPOSE OF THIS STUDY
• Less biased estimate of the true treatment effects
• Randomized data only

ELIGIBILITY CRITERIA
• No previous elbow trauma • No previous surgery • All patients failed initial
conservative treatment• Only randomized trials were
included to limit selection bias

DIAGNOSIS CONFIRMED BY EMG IN ALL CASES

STUDY IDENTIFICATION• Medline• Embase• Cochrane Database of Systematic Reviews • Cochrane Central Register of Controlled Trials • CINAHL • Annual meeting archives:
– Academy of Orthopaedic Surgeons (2004-2006) – American Association of Plastic Surgeons (2005-2006) – American Association of Neurological Surgeons (2001-2006) – American Society for Surgery of the Hand (2001-2006)
INDPENDENT SEARCH BY 2 OF US

METHODS
• Duplicate assessment of methodological quality (Detsky scale)
• Duplicate data abstraction independently by two of us
• Assessment of heterogeneity(Hedges & Olkin)
• Assessment of publication bias• Random effects model for pooling data• Outcome parameters converted to effect sizes

OUTCOME PARAMETER
•Post-op EMG•Post clinical score
– McGowan score– Bishop score– Medical Research Council score

RESULTS

Screening

STUDY CHARACTERISTICS• 4 studies identified
– 2 studies: simple decompression versus submuscular ulnar nerve transposition (n=117)
– 2 studies: simple decompression versus subcutaneous ulnar nerve transposition (n=218).
• Total of 335 randomized patients, 327 of whom were followed up (98%).
• Sample sizes: 47 to 152 • Average age: 51 years • 65% males

AUTHORS OF IDENTIFIED STUDIES WERE CONTACTED AND ALL PROVIDED
THE RAW DATA

SEVERITY OF SYMPTOMS
• Majority of patients with moderate or severe symptoms – Dellon grade (II or III)– Pre-operative Medical Research Council grade
(avg. of 4.3 on 1-7 scale)– Pre-op EMG (avg. NCV of 35 m/s)

Pre-op Nerve Conduction Velocity
Post-op Nerve Conduction Velocity

Post-op Clinical Scores: Effect Size

WHAT IS EFFECT SIZE?
• A number that expresses a difference between two groups as a multitude of standard deviations


COHEN’s EFFECT SIZE
•Mild: 0.2•Moderate: 0.5•Large: 0.8
CLINICAL SCORE EFFECT SIZE BETWEEN AT AND SD: -0.04 (-0.36 to 0.28)

CONCLUSIONS
1. No difference in motor nerve conduction velocities and clinical outcome scores
2. Confidence intervals around the points of estimate are narrow probably excluding clinically meaningful differences

SINCE ULNAR NERVE TRANSPOSITION IS THE MORE
INVASIVE OF THE TWO PROCEDURES, THIS DATA
SUPPORTS THE USE OF SIMPLE DECOMPRESSION OF THE
ULNAR NERVE.

TREND TOWARDS BETTER RESULTS WITH TRANSPOSITIONBEWARE: INCLUDES NON-RANDOMIZED DATA!!!

MEDIAL EPICONDYLECTOMY


NO MAJOR DIFFERENCES, BUT HIGHER SATISFACTION AFTER MEDIAL EPICONDYLECOMY


BOTTOMLINE:NO CONSENSUS
ON BEST TREATMENT

ANTERIOR TRANSPOSITION INDICATIONS
• Prior injury to elbow• Revision surgery • Intra-operative ulnar nerve subluxation

SUBMUSCULAR / INTRAMUSCULAR TRANSPOSITION
TECHNIQUE
















OITE Reminder:• Struther’s Arcade• Wartenberg’s sign
• Struther’s ligament
• Wartenberg syndrome
ULNAR NERVE
MEDIAN NERVE
RADIAL NERVE

CASE ID: 19

THANK YOU