-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
1/46
Dhssraj Singh, MDApril 2, 2012
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
2/46
Contents
Overview of inherited cardiomyopathies
Hypertrophic cardiomyopathy
Arrhythmogenic right ventricularcardiomyopathy
Non compaction cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
3/46
Genetically heterogeneous set of diseasesWithin each disease
there may be multiple diseasegenes
Different mutation within same gene mayproduce completely
different phenotypes (eg indilated vs. hypertrophic
cardiomyopathy)
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
4/46
Heritable
Cardiomyopathies
HCMARVC
LVNC
Michael J. Ackerman - Genomic Advances and Retreats in
Hypertrophic Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
5/46
Autosomal dominant
1:5000Unexplained hypertrophy of left ventricle,myocyte
disarray, fibrosis
Often predominant involvement of LV septum
Marked phenotypical variaty due to incompletepenetrance
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
6/46
Seventy percent of cases are due to sarcomeric
gene alterationsMutated genes are usually unique to familiesthat
inherit the gene
Cascade family screeningDiagnostic yield of sarcomeric gene
testing is60% - absence of sarcomere mutation cannotrule out
familial HOCM
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
7/46
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
8/46
Modified from Spirito P et al. NEJM336:775,1997
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
9/46
MYH7-HCMCh 14q11
Beta myosin
heavy chain
~15%
MYBPC3-HCM
Ch 11p11
Myosin binding
protein C
~20%
TNNT2-HCM
Ch 1q32
Troponin T
~2%
TNNI3-HCM
Ch 19p13
Troponin I
~1%
MYL2-HCM
Ch 12q23
< 1%
MYL3-HCM
Ch 3p21
< 1%
ACTC-HCM
Ch 15q14
-actin
< 1%
TPM1-HCM
Ch 15q22.1
-tropomyosin
~1%
Michael J. Ackerman - Genomic Advances and Retreats in
Hypertrophic Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
10/46
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
11/46
Septal Shape and Myofilament HCM
104/132 (79%)
+ve Genetic Test
15/181 (8%)
+ve Genetic Test
Binder et al. Mayo Clin Proc 81:459-467, 2006
Sigmoidal-HCM
47%
Reverse Curve-
HCM
35%
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
12/46
Septal Shape and HCM Genetic Testing
79%
Reversed
41%
Neutral
30%
Apical
8%
Sigmoid
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
13/46
Comprehensive or targeted (MYBPC3, MYH7,TNNI3, TNNT2) is
recommended for any patient
in whom a cardiologist has established a clinicaldiagnosis of
HCM based on examination ofpatients clinical history, family
history andelectrocardiographic/echocardiographic
phenotypeMutation specific confirmatory testing wouldbenefit
family members/relatives
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
14/46
Mutation specific genetic testing isrecommended for first degree
family members
(parents, siblings, offspring) followingidentification of
HCM-causative mutation inindex case
Better than clinical screening as EKG/echo changesmay be subtle
or develop late
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
15/46
Screening gene testing for HOCM also indicatedfor:
families with history of SCD
families in which clinical diagnosis is difficult,including
those with clinical complications ofHOCM despite only mild
hypertrophy
Genetic analysis of post mortem specimens ininstances of sudden
cardiac death where HOCMwas not previously known in family.
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
16/46
Genetic screening not recommended in:
Diagnosis of HOCM if non-diagnostic clinicalfeatures present
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
17/46
Developed in Collaboration with the American Association for
Thoracic Surgery,
American Society of Echocardiography, American Society of
Nuclear Cardiology,
Heart Failure Society of America, Heart Rhythm Society, Society
for CardiovascularAngiography and Interventions, and Society of
Thoracic Surgeons
American College of Cardiology Foundation and American Heart
Association, Inc.
G ti T ti St t i /F il S i
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
18/46
Evaluation of familial inheritance and genetic counseling is
recommendedas part of the assessment of patients with HCM.
Patients who undergo genetic testing should also undergo
counseling bysomeone knowledgeable in the genetics of
cardiovascular disease so thatresults and their clinical
significance can be appropriately reviewed with
the patient.
Screening (clinical, with or without genetic testing) is
recommended infirst-degree relatives of patients with HCM.
Genetic testing for HCM and other genetic causes of unexplained
cardiachypertrophy is recommended in patients with an atypical
clinicalpresentation of HCM or when another genetic condition is
suspected tobe the cause.
Genetic Testing Strategies/Family Screening
I IIa IIb III
I IIa IIb III
I IIa IIb III
I IIaIIb III
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
19/46
Genetic testing is reasonable in the index patient tofacilitate
the identification of first-degree family membersat risk for
developing HCM.
The usefulness of genetic testing in the assessment of riskof
SCD in HCM is uncertain.
Genetic Testing Strategies/Family Screening
I IIa IIb III
I IIa IIb III
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
20/46
Genetic Testing Strategies/Family Screening
Genetic testing is not indicated in relatives when theindex
patient does not have a definitive pathogenicmutation.
Ongoing clinical screening is not indicated in genotypenegative
relatives in families with HCM.
I IIa IIb III
I IIa IIb III
No Benefit
No Benefit
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
21/46
Genotype-Positive/Phenotype-
Negative Patients
Diagnosis
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
22/46
Genotype-Positive/Phenotype-Negative Patients
In individuals with pathogenic mutations who do notexpress the
HCM phenotype, it is recommended toperform serial ECG, TTE, and
clinical assessment at periodicintervals (12 to 18 months in
children and adolescents andabout every 5 years in adults), based
on the patients age
and change in clinical status.
I IIa IIb III
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
23/46
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
24/46
First described by Fontaine in 1977
Prevalence : 1:5000 in the US
Progressive dystrophy or cardiomyopathy of theright
ventricle
Replacement of right ventricular myocardiumwith fatty tissue
may involve either/both ventricles
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
25/46
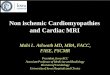
Normal Myocardium
ARVD Fat Infiltration
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
26/46
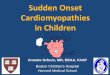
Leads to electrical instability, ventriculararrhythmias and
sudden death
Morphology may resemble DCM, but clinicallyusually presents as
arrhythmia rather than HF.
ARVD/C accounts for3-4 % of SCD in young
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
27/46
Early concealed phase characterized bypropensity toward
ventricular arrhythmia insetting of preserved morphology,
histology,
ventricular function
As disease progresses, myocyte loss,inflammation fibroadiposis
becomes evident.
Structural changes include regional WMA,ventricular aneurysms,
increased trabeculationto global ventricular dilation and
dysfunction
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
28/46
Type Chromosome Gene Comment
ARVD/C 1 14q24.3 TGFb3 Progressive RV cardiomyopathy
ARVD/C 2 1q42-1q43 RyR2 ? Assoc. with CPVT
ARVD/C 3 14q11-14q12 ?
ARVD/C 4 2q32.1-q32.3 ? Localized LV involvementARVD/C 5 3p23
LAMR1 Seen in New Foundland
ARVD/C 6 10p12-14 Tyr Phos Early onset disease
ARVD/C 7 10q22 DES Assoc with myofibrillar myopathy
ARVD/C 8 6p24 Desmoplakin DSP Keratoderma and wooly hair
(6-16%)
ARVD/C 9 12p11 Plakophilin PKP2 Intracellular disruption
(11-43%)
ARVD/C 10 18q12.1-q12.2 Desmoglein DSG2 (10-12%)
ARVD/C 11 18q11 DesmocollinDSC2
(1-5%)
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
29/46
Most genes involved encode for desmosomalproteins
30 70 percent of cases harbor noted above
Once confirmed in index case, cascadescreening applied to
relatives.
Failure to identify genes does not excludedisease
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
30/46
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
31/46
Most symptoms occur in 2nd-5th decades oflife
Chest, palpitations, dizziness, syncope
First symptom may be sudden death
Subclinical form of ARVD/C in younger pts
concealed phase
Symptoms and RV cardiomyopathy
precipitated by stress or exercise
Frank J. Zimmerman, MD - Arrhythmogenic Right Ventricular
Dysplasia / Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
32/46
Comprehensive or targeted (DSC2, DSG2, DSP,JUP, PKP2,and TMEM43)
ACM/ARVC genetictesting can be useful for patients satisfying
task
force diagnostic criteria for ACM/ARVC.Genetic testing may be
considered for patientswith possible ACM/ARVC (1 major or 2
minor
criteria) according to the 2010 task forcecriteria.
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
33/46
Genetic testing is not recommended forpatients with only a
single minor criterionaccording to the 2010 task force
criteria.
Mutation-specific genetic testing isrecommended for family
members andappropriate relatives following the identificationof the
ACM/ARVC-causative mutation in an
index case.
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
34/46
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
35/46
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
36/46
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
37/46
Dogged by variable penetrance, age relatedexpression,
unpredictable flare ups
A family history of SCD is not necessarily a keyindicator of
adverse prognosis
Unremarkable clinical evaluation does notpreclude transmission
or expression of diseasein the near future
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
38/46
Lead to centers offering periodic reassessmentof first, second
or even third degree relatives
Prospects of lifelong screening withoutdefinitive prospect of
negative reassurance maylead to anguish
Gene negative with negative clinical exams mayrarely present
later with catastrophic arrest
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
39/46
Michael J. Ackerman - Genomic Advances and Retreats in
Hypertrophic Cardiomyopathy
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
40/46
Excessive unusual trabeculations within themature left
ventricle
Developmental failure of heart to fully compactthe myocardium
during initial stages ofdevelopment
spongy morphological appearance of the
myocardium occurring primarily in the LV, withthe abnormal
trabeculations typically beingmost evident in the apical and
midlateral/-inferior portions of the LV.
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
41/46
thickening of the myocardium in two distinctlayers composed of
compacted and non-
compacted myocardium also classically is noted.Ratio of
non-compacted versus compactedmyocardium is often larger than
2.0.
May have systolic +/- diastolic dysfunction
Associated with thromboembolism, especially inpatients with
lower ejection fraction
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
42/46
Disease may be seen in family members of LVNCbut also
occasionally seen in relatives ofpatients with HOCM, dilated or
restrictivecardiomyopathy.
May represent a spectrum of cardiomyopathybetween dilated and
hypertrophic
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
43/46
X linked, Autosomal dominant, autosomalrecessive or
mitochondrial inheritance pattern
Sporadic in 60 70 percent.Fifteen genes have been implicated,
althoughnone are predominantly involved
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
44/46
LVNC genetic testing can be useful for patients in
whom a cardiologist has established a clinicaldiagnosis of LVNC
based on examination of thepatients clinical history, family
history, and
electrocardiographic/echocardiographicphenotype.
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
45/46
Mutation-specific genetic testing isrecommended for family
members andappropriate relatives following the identificationof an
LVNC-causative mutation in the index
case.Patients with LVNC should be assessed with at leasta 3
generational family history, and all first degreerelatives of
patients with LVNC should be evaluated
echocardiographicaly
2011 HRS/EHRA Expert Consensus Statement
-
8/2/2019 4.2 Heriditary Cardiomyopathies Singh
46/46
Thank you!