Embed Size (px)
Citation preview

4 PRIMARY AND SECONDARY BRAININJURY
A. David Mendelow and Peter J. Crawford
4.1 Introduction
Throughout most of the world, the majority of head-injured patients are initially managed by emergencymedical services that do not have specialized knowl-edge of the pathophysiology and treatment of headinjury. It is for this reason that the traditional divisioninto primary and secondary brain damage remainsuseful; primary brain damage occurs at the time ofimpact, produces its clinical effect almost immediatelyand is refractory to most treatment. By contrast,secondary brain damage occurs at some time after theprimary impact and is largely preventable and treata-ble. The clinician’s role, therefore, is to recognize anddocument the primary brain damage, then to preventand treat secondary brain damage. Recent researchhas shown that, although primary brain damage hasbeen regarded as irreversible, changes in ultrastruc-ture, the blood–brain barrier and neuronal functionmay progress over time and may provide somepotential for treatment (Povlishock 1992, 1995; Max-well, 1995).
Understanding this concept prepares the non-spe-cialist clinician for the main challenge in head injurymanagement: the prevention and treatment of second-ary damage. It is therefore essential that all the causesand consequences of secondary brain damage areknown and understood. In an ideal world, no second-ary brain damage would occur! Also, this conceptpaves the way for understanding how neuroprotectivestrategies (hemodynamic and pharmacological) maylimit secondary brain damage. There is also merit inclassifying brain damage into focal and diffuse types(Teasdale, 1995) but, from the clinical standpoint, thedivision into primary and secondary damage remainsthe most pragmatic and therapeutically usefulclassification.
Secondary brain damage may begin very rapidlyafter impact, so that decisions must be taken early andcorrectly.
Globally, many more lives would be saved and themorbidity from head injury would be more effectivelyreduced if head injury management and services werebetter organized than could ever be achieved byimproving the intensive care and pharmacologicaltreatments in already well-developed areas and cen-ters. Unfortunately it is this ‘high tech’ emphasis thathas dominated thinking and practice in head injurymanagement to date.
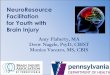
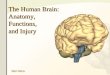
This concept and such organizational challengeshave been recognized for many years, and a group ofBritish neurosurgeons (Group of Neurosurgeons,1984) produced guidelines for head injury manage-ment that have become a consensus document adop-ted throughout the UK and now in many other partsof the world (Garibi, 1995, personal communication).More recently, such guidelines have been modified toinclude recommendations for children, and the Soci-ety of British Neurosurgeons has endorsed newguidelines. Their introduction has resulted in anincrease in the number of hematomas being detectedin large regional centers (Miller, 1993; Treadwell andMendelow 1994; Figures 4.1, 4.2). A similar set ofguidelines has recently been produced in the UnitedStates, under the auspices of the American Associationof Neurological Surgeons.
The prime aim of such guidelines is:
� to reduce initial hypoxic ischemic damage usingprinciples of resuscitation set out in the AdvancedTrauma Life Support system (ATLS – AmericanCollege of Surgeons, 1993);
� to increase the early detection of hematomas so thatdelay in treatment can be eliminated.
Although the ATLS recommendations play a vitallyimportant role in preventing hypoxia and ischemia,the ATLS approach to head injury is not practicalthroughout most of the world. The ATLS statement‘All head injuries except the most minor will require aCT scan’ would result in the successful diagnosis of
Head Injury. Edited by Peter Reilly and Ross Bullock. Published in 1997 by Chapman & Hall, London. ISBN 0 412 58540 5

72 PRIMARY AND SECONDARY BRAIN INJURY
most hematomas, but could not be implementeduniversally because of the lack of local 24-houremergency CT facilities in most countries (Hewer andWood, 1989). It is for this reason that guidelines forhead injury are more applicable to cities, towns andregions without local 24-hour CT scanning facilitiesfor all head injuries. Since they are based on riskfactors for traumatic hematomas (Mendelow, Teasdaleand Jennett, 1983; Teasdale et al., 1990), they shouldresult in correct diagnosis of the majority of traumatichematomas by selecting for transfer those head-injured patients who are most at risk of developinghematomas. They would be transferred to centralizedneurotrauma units where 24-hour scanning is avail-able. Similarly, the advanced pediatric life support(APLS) program (APLS, 1993) has made recommenda-
tions for CT scanning that may not be practical inmany small centers because of the limited availabilityof after-hours scanning.
4.2 Primary brain damage
The pathology of brain damage has been discussed inChapter 3 and will not be discussed in great detail here,other than referring to its importance in determiningthe initial level of consciousness and any focalneurological deficit. Also, the time-related ultrastruc-tural changes that take place within minutes of injuryare discussed because of their importance in relation topossible treatment. The clinical effects of this primary(or impact) damage may be greatly aggravated bysecondary brain damage (Bullock, Zauner et al., 1995;Ito, Barzo et al., 1995). Thus diffuse axonal injury(DAI), contusions and lacerations of the brain willproduce immediate clinical effects varying from con-cussion, with mild DAI (Oppenheimer, 1968), to comaand death. Focal primary damage, for example withcerebral laceration due to a penetrating injury, mayalso produce an immediate neurological deficitdepending upon the site of injury. Thereafter, anyincrease in neurological deficit or deepening of the levelof consciousness will be due to secondary braindamage.
Recent experimental research has shown that focalaxonal swelling occurs within 15 minutes of traumaticbrain injury (TBI) due to misalignment of microtubules(Maxwell, 1995) and that their disruption leads to‘nodal blebs’ within 2 hours. Later there is a change inthe axolemma permeability which, after 6 hours, leadsto retrograde and anterograde misalignment of neu-rofilaments (with compaction and mitochondrial
Figure 4.1 Effect of 1982 Edinburgh guidelines for manage-ment of head injuries on the pattern of traumatic hematomasdetected and operated on before (a) (1981) and after (b)(1986/1989) their introduction; odds ratio with 95% con-fidence limits. a = detected; b = operated. (Source: repro-duced from Miller et al., 1992, with permission.)
Figure 4.2 Effect of two editions of head injury guidelines on head injury admissions to Newcastle General Hospital in theNorthern Region of England and number of traumatic hematomas detected. (Source: data from Treadwell and Mendelow,1994, updated for 1995 data.)

SECONDARY BRAIN DAMAGE 73
abnormalities). Similarly, blood–brain barrier (BBB)breakdown begins within 3 minutes of injury, leadingto albumin extravasation (Fukuda et al., 1995). Theseearly changes following DAI have been confirmedclinically with diffusion-weighted magnetic resonanceimaging (MRI; Vink, 1995; Mikulis, 1995; Lenkinski,Gennarelli et al., 1995). Nevertheless, it is superaddedsecondary ischemic damage that results in cytotoxicedema and elevated intracranial pressure (ICP; Ito,Barzo et al., 1995). The combination of these earlychanges with DAI and hypoxia/ischemia as a second-ary event may provide some potential for pharmaco-logical neuroprotection since increases in glutamateconcentrations are maximal after secondary ischemiabut do not occur when DAI occurs in isolation(Bullock, Zauner et al., 1995).
Tsuji et al. (1995) have shown experimentally thatwith DAI in rats there is no change in excitatory aminoacid (EAA) or extracellular calcium levels unlesssecondary insults take place as well (PaO2 < 5.33 kPa;BP < 40 mmHg).
4.3 Secondary brain damage
The classification of secondary brain damage hastraditionally been into extra- and intracranial (Table4.1). There is merit in maintaining this classification.
4.3.1 EXTRACRANIAL SECONDARY BRAIN DAMAGE
Extracranial problems produce secondary brain dam-age either by hypoxia or by oligemia/ischemia (Table
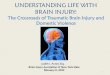
4.1). The ultimate consequence of either is a reductionin the availability of high-energy phosphate (adeno-sine triphosphate, ATP). This leads to failure ofmembrane pumps so that cells either die or becomeswollen (so called cytotoxic edema). The distributiondiffers in that hypotension with primary oligemia andischemia tends to affect the arterial boundary zones(Figure 4.3). By contrast, hypoxemia alone tends to bemore global, with neuronal loss, which leads tocortical atrophy in survivors.
The most extreme consequences of severe andprolonged hypoxia are the persistent vegetative state(PVS) or death. PVS may occur with preservation ofbrain-stem reflexes, but with loss of most of the cortex,although hallmarks of DAI are found in 77% of patientswho die in PVS (Graham, Jennett et al., 1995).Secondary brain damage due to hypoxia and hypoten-sion also occurs in patients who have already beenadmitted to intensive care units, when it is looked forcarefully: detailed monitoring studies by Jones andMiller (Jones et al., 1993, 1994; Andrews et al., 1990) withaccurate computerized recording have revealed thatsuch insults occur in 32% of head-injured patients evenwhen there is no evidence that these have been detectedon standard nursing charts.
If the extracranial insults are associated withintracranial lesions, then the penumbra of any regionof hemorrhage or compression becomes the primarytarget of hypoxemia or ischemia. It has been clearlyshown that intracerebral hemorrhage produces an areaof ischemia around the hematoma and that this issurrounded by a penumbra of functionally impaired
Table 4.1 Extracranial and intracranial causes ofsecondary brain damage
Extracranial causes
� Hypoxia� Hypotension� Hyponatremia� Hyperthermia� Hypoglycemia
Intracranial causes� Hemorrhage
– Extradural– Subdural– Intracerebral– Intraventricular– Subarachnoid
� Swelling– Venous congestion/hyperemia– Edema
VasogenicCytotoxicInterstitial
� Infection– Meningitis– Brain abscess Figure 4.3 CT scan showing bilateral boundary zone
infarcts from hypoxia–ischemia.

74 PRIMARY AND SECONDARY BRAIN INJURY
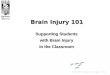
but potentially viable tissue (Figure 4.4; Mendelow etal., 1984).
Similarly, there is an area of ischemia that underliesan experimental subdural hematoma which is alsobounded by a penumbra (Bullock et al., 1990). In allthese situations, hypoxemic or ischemic extracranialinsults will aggravate the secondary damage in relationto the focal lesion. Similarly, extracranial secondaryinsults will aggravate primary DAI (Bullock et al., 1995;Ito, Barzo et al., 1995).
Regrettably, such hypoxic and hypotensive insultshave persisted in patients transferred to neurosurgeryunits, despite many efforts to prevent them (Gentlemanand Jennett, 1981; Gentleman, 1992; Kohi et al., 1984).The consequence is that ischemic brain damageremains a very frequent finding at autopsy in patientswho die with head injury. It has fallen only very slightlyfrom 91% in 1978 to just over 80% in 1989 (Graham,Adams and Doyle, 1978; Graham et al., 1989). Hope-fully, better emergency rescue and pre-hospital resusci-tation will reduce the incidence of ischemic braindamage. The ATLS and APLS courses will probablyachieve this with better initial resuscitation.
The effect of hypoxia/ischemia is particularly severein head-injured patients where ICP may be elevated, sothat cerebral perfusion pressure (CPP) is reduced.Levels of blood pressure that would normally be welltolerated are insufficient to maintain normal cerebral
perfusion when ICP is elevated. It has therefore becomerecognized that higher levels of CPP are associatedwith better outcomes from head injury (McGraw, 1989;Mendelow et al., 1994; Miller, 1993; Cortbus et al., 1995;Wong et al., 1995a,b; Contant et al., 1993).
Furthermore, autoregulation that has become so wellrecognized in normal physiological studies becomesdisordered following head injury (Figure 4.5).
These ischemic events may be missed when CBF ismeasured because it is often measured only in theintensive care unit after stabilization has taken place(Mendelow et al., 1985; Obrist et al., 1979; Enevoldsonet al., 1976; Matthews et al., 1995; Sharples et al., 1994,1995). However, studies early after head injury havenow confirmed reduced CBF with loss of autoregula-tion if measured within 8 hours of the injury (Schroderet al., 1993; Chapter 11). The result is that an adultpatient with a head injury may require a CPP of 80 or90 mmHg to maintain normal cerebral perfusion. Withincreased ICP (e.g. 30 mmHg) this may require a meanblood pressure (BP) of 120 mmHg – it is interesting torealize that the unanesthetized previously normalpatient with head injury may achieve this sponta-neous rise in BP with the Cushing response, which hasbeen recognized for almost a century now (Cushing,1901, 1903). However, deeply anesthetized patientsmay be unable to mount a Cushing response, soclinicians dealing with anesthetized head-injuredpatients in intensive care units, resuscitation roomsand operating theaters must be aware of the need tomaintain adequate levels of CPP. In some instances itmay be possible to determine the ‘breakpoint’ or‘inflection point’ for the lower limit of autoregulationby measuring middle cerebral velocity with tran-scranial Doppler (Wong et al., 1995a,b). In this way the
(a)
(b)Figure 4.4 (a) Cross-section of rat brain showing intra-cerebral hematoma. (b) Autoradiograph of same rat to showlarger area of ischemia.
Figure 4.5 Diagram showing loss of autoregulation follow-ing head injury. Cerebral blood flow (CBF) remains constantover a range of cerebral perfusion pressure (CPP) from50–150 mmHg. Continuous line represents loss ofautoregulation.

SECONDARY BRAIN DAMAGE 75
CPP could be tailored to the individual patient. Earlymonitoring of these parameters may lead to betteracute care of head-injured patients in future, althoughat present these sophisticated monitoring techniquesare not universally available. Nevertheless, less inva-sive techniques like jugular venous oxygen (JVO2)monitoring (Piper et al., 1995; Gopinath et al., 1994)and transcranial near infrared spectroscopy (NIRS)may become more practical in future (Germon, 1995).In a recent study, NIRS provided a sensitive means ofdetecting changes in cerebral oxygenation in 97% ofinsults detected with CPP, transcranial Doppler orlaser-Doppler (Kirkpatrick et al., 1995). By contrast,JVO2 detected only 53% of these insults.
Other causes of extracranial primary brain damageinclude hypocapnia (used to treat raised ICP) andsevere hypoxemia. Although hyperventilation withhypocapnia can reduce cerebral blood flow, there isdoubt about whether moderate hyperventilation canproduce ischemic brain damage unless cardiac outputis reduced by excessive hyperventilation. It is prob-ably best to maintain the PaCO2 at around 32 ± 2 mmHgin most patients (Chapter 18).
Hyponatremia after head injury is often due toexcess ADH secretion, which results from hypovole-mia caused either by fluid restriction or by hemor-rhage from other injuries. The excess ADH secretion istherefore appropriate to the hypovolemia but inap-propriate to the hyponatremia. Further fluid restric-tion may aggravate the problem by further increasingADH levels (Poon et al., 1989; Jackowski, 1992). A clearunderstanding of the water and electrolyte problemsfollowing head injury may need to be determined ineach case (Nelson et al., 1981). In general, uncorrectedhyponatremia may lead to reduced levels of con-sciousness and even epileptic seizures. Hyponatremiamay also result from the ill-advised and sometimesexcessive use of dextrose solutions without anysodium supplementation.
4.3.2 INTRACRANIAL SECONDARY BRAIN DAMAGE
The rate of development of secondary brain damagedepends upon the cause. It is universally recognizedthat hematomas should be evacuated expeditiously.The adverse effect of long delay times with extraduralhemorrhage and subdural hemorrhage has been docu-mented in studies from Edinburgh, UK (Figure 4.6;Mendelow et al., 1979) and Richmond, VA (Figure 4.7;Seelig et al., 1981).
With extradural hemorrhage, the time from firstrecorded deterioration in level of consciousness tooperation was less than 2 hours on average inpatients who made a good recovery or who were onlymoderately disabled. Similarly, with acute subduralhemorrhage the time from injury to operation strongly
influenced outcome, delays of more than 4 hours frominjury being the most significant.
In either case the mechanism of secondary braindamage is direct compression of the underlying cortexcausing local ischemic brain damage and brain shift,which causes local zones of ischemia in the brain stemand basal structures, and in the cingulate gyrus(Chapter 18). The ischemic brain damage tends to befocal, but if elevated ICP is unrelieved, leading toreduced CPP, then global ischemic brain damage mayoccur. Similarly, experimental studies have shownischemic brain damage surrounding intracerebralhemorrhage (Jenkins et al., 1990; Kingman et al., 1988;Mendelow et al., 1984; Nath et al., 1986, 1987; Nehls et al.,1988; Sinar et al., 1987) and clinical studies with SPECThave confirmed this (Figure 4.8; Wyper et al., 1995).
Ultimately the mechanism of neuronal death isalmost always a reduction in ATP with membranepump failure. This leads to activation of calciumchannels, with influx of calcium ions into cells resultingin cell death. The process also leads to a release ofexcitatory amino acids (EAA), including glutamate andaspartate. These activate the receptor-operated calciumchannels, with further calcium influx (Figure 4.9).Prevention of this calcium influx into cells has offeredscope for neuroprotective agents, such as nimodipine,
Figure 4.6 Effect of delay (from deterioration to surgery)on outcome from extradural hematoma. O = good recovery;D = death. (Source: reproduced from Mendelow et al., 1979,with permission.)

76 PRIMARY AND SECONDARY BRAIN INJURY
which block the voltage-operated calcium channels(Mohamed et al., 1985) or the receptor-operatedchannels (Hatfield et al., 1992; Chapter 7).
The potential for neuroprotective strategies insevere head injury is likely to be maximal whensecondary brain damage is due to hemorrhage (intra-cerebral, subdural and subarachnoid) and ischemia(Chapters 7 and 21).
(a) Traumatic subarachnoid hemorrhage andsecondary damage
Experimentally, SAH is associated with delayedbreakdown of the BBB (Fukuda et al., 1995), possiblybecause metallic ions in blood (e.g. iron and calcium)are potent catalysts of free radicals (Cortez et al., 1989).Clinical outcome in traumatic SAH is worse than in
Figure 4.7 Effect of delay (from injury to operation) in acute subdural hematoma. (Source: reproduced from Seelig et al.,1981, with permission.)
Figure 4.8 SPECT scan showing area of ischemia surrounding intracranial hemorrhage. (Source: reproduced fromChocksey et al., 1991, with permission.)

EXTRADURAL HEMATOMA 77
patients without SAH on CT scan and is associatedwith a higher incidence of secondary hypoxic/ische-mic insults (Green et al., 1995). In traumatic SAHKakarieka et al. (1995) have shown that the calciumantagonist nimodipine produced significantly fewerunfavorable outcomes (6-month Glasgow OutcomeScale) than placebo in a prospective randomizedcontrolled trial, confirming earlier suggestions fromthe ‘HIT II’ trauma trial with nimodipine that patientswith traumatic SAH may respond better to nimodi-pine than those without SAH (Braakman et al., 1994).
It should be remembered that ‘neuroprotectivestrategies’ can be organizational as well as pharma-ceutical: beneficial effects of early operative evacua-tion cannot be overemphasized because the deeper thelevel of consciousness at the time of operation inpatients with traumatic hematomas, the worse theoutcome (Figure 4.10; Bullock and Teasdale, 1990). Forthis reason early diagnosis and treatment of hemato-mas will always be the most effective ‘neuropro-tective’ strategy in dealing with head injury.
The severity of underlying primary brain damagewith trauma can vary from almost none (in a patientwho is fully conscious, but who later deteriorates) to
severe, where the patient may be in coma from theoutset. There is more likely to be severe primary braindamage with acute subdural and intracerebral hemor-rhage than with cases of extradural hemorrhage,where there may be very little primary damage. Thisaccounts for the classical ‘lucid interval’ that hasbecome so well known with extradural hemorrhage(Jamieson and Yelland, 1968). It puts an added burdenof responsibility on those clinicians who manage themany patients with minor head injuries with minimalprimary brain damage, because compression fromextradural hemorrhage may result from middlemeningeal bleeding with a skull fracture in anotherwise minor head injury. This is the basis forrecognition of the importance of skull fracture indetecting hematomas (Chan et al., 1990; Mendelow,Teasdale and Jennett, 1983; Teasdale et al., 1990; Santoset al., 1995). If free access to CT scanning is available,all head-injured patients will require a CT scan, asassumed in the ATLS and AANS guidelines. The useof a skull X-ray to detect a fracture then becomesunimportant, but in the absence of universal access toCT for head-injured patients, skull fracture remainsone of the most significant clinical and radiologicalfeatures to help detect hematomas (Table 4.2).
4.4 Extradural hematoma
Extradural hematomas (EDH) are extracerebral lesionsand thus there may be little or no primary brain
Figure 4.9 Calcium channel (receptor-activated) to illus-trate site of competitive and non-competitive antagonists.(Source: reproduced from Davis and Barer, 1995, withpermission.)
Figure 4.10 Effect of Glasgow Coma Score on outcome inpatients with traumatic intracranial hematoma. (Source:reproduced from Bullock and Teasdale, 1990, withpermission.)
Table 4.2 Risks of traumatic hematoma with skullfracture and altered consciousness for patients attendingAccident and Emergency (Source: from Teasdale et al.)
No. per millionper year
Absolute risk ofhematoma (1 in:)
Adults
No skull fractureFully conscious 7700 7900Impaired consciousness 550 180Coma 66 27
Skull fractureFully conscious 130 45Impaired consciousness 43 5Coma 41 4
Children
No skull fractureFully conscious 7200 13 000Impaired consciousness 250 580Coma 23 65
Skull fractureFully conscious 100 160Impaired consciousness 17 25Coma 11 12

78 PRIMARY AND SECONDARY BRAIN INJURY
damage, so that, initially, consciousness may recoveror be preserved – this accounts for the well known‘lucid interval’ that occurs with EDH (although itoccurs in less than 25% of cases). The frequency ofskull fracture with extradural hematoma in children is79.3% (Santos et al., 1995), which is as high as it is inadults. Furthermore, in infants the large head sizerelative to the body means that the volume of theextradural space is large in relation to the bloodvolume, so that hypovolemia may be the primarypresenting feature with an infantile extradural hema-toma. This, coupled with elevated ICP, leads to a rapidfall in CPP and consequent ischemic brain damage.This is seen particularly in non-accidental injury. Forthese reasons, monitoring of infants with even minorhead injury should include continuous pulse raterecording, and a CT may be indicated if a tachycardiadevelops.
Posterior fossa extradural hematomas,, though rare(less than 5% of all EDH) may give rise to a suddendeterioration in the level of consciousness due tohydrocephalus, and it is important to recognize theneed to scan the posterior fossa if an occipital skullfracture is present (Figure 4.11).
A posterior fossa extradural hematoma may extendabove the transverse sinus and compress the occipitalpole, so that great care must be taken to avoid majorblood loss from the confluens sinuum or the trans-verse sinus when operating on these cases. In children,extradural haematomas are often limited by theadherence of the dura to the sutures (Figure 4.12). Chronic venous extradural hematomas are rare but
may present with late deterioration in level of con-sciousness (Stevenson et al., 1964). Because these lie atthe vertex, CT scanning should include high cutswhen a high skull fracture extends over the superiorlongitudinal sinus.
When a patient with an EDH dies, neuropatho-logical studies usually show massive ischemic damagedue to brain compression and/or low CPP.
4.5 Intradural hemorrhage
Subdural hemorrhage and intracerebral hemorrhagewere often considered as two separate conditions, andthey may well be separate. However, CT and MRIhave clearly shown that subdural hematomas oftencoexist with intracerebral hemorrhage and with cere-bral contusions. Acute subdural hemorrhage tends toextend throughout the subdural space and lies mainlyon the surface. Although apparently thin, their exten-sive nature is associated with a larger intracranialvolume than would be expected from CT scanningalone. They are usually unilateral and are morefrequently associated with underlying primary braindamage, so that patients with acute subdural hemato-mas are more likely to present in coma, in contrast
Figure 4.11 CT scan showing posterior fossa extraduralhematoma with extension into the left occipital supratentor-ial region. Note right Sylvian subarachnoid hemorrhage.
Figure 4.12 CT scan showing extradural haematoma in achild, limited by sutures.

HERNIATION 79
with extradural hemorrhage where primary braindamage is often less severe. The acute subduralhematoma associated with anticoagulants is theexception because in these patients there is often littleor no primary brain damage so that they deteriorate,as they bleed into the subdural space, from fullconsciousness. With time, the subdural hematomabegins to liquefy and by 14–21 days it may havebecome predominantly liquid so that burr hole drain-age may drain it effectively, in contrast with acutesubdural hematoma where the solid clot has to beremoved via a craniotomy.
Chronic subdural hematomas represent a differentspectrum of head injury. The trauma is often minimalor even unrecognized in one-third of cases (Cameron,1978). Because there may be no primary brain damagein these patients, the outcome is much better thanfollowing the treatment of acute subdural hematomas(Nath et al., 1985). In some patients with chronicsubdural hemorrhage there is recent acute hemor-rhage so that different clot densities can be recognizedon CT scans. This recurrent hemorrhage may lead tothe development of pseudomembranes which, withtime, will result in further liquefaction of the clot.Also, chronic subdural hemorrhage may be bilateral.Such cases may present as dementia rather than as ahead injury.
4.6 Intracerebral hemorrhage
Traumatic intracerebral hemorrhage may occur inisolation or be part of a complex intradural hemor-rhage. Isolated intracerebral hemorrhage is muchmore common in the elderly and may at times bedifficult to distinguish from spontaneous intracerebralhemorrhage. This is because a primary spontaneoushemorrhage may result in a fall, which causes asecondary head injury. The mechanism of develop-ment of traumatic intracerebral hemorrhage is similarto spontaneous intracerebral hemorrhage: an artery orarteriole is disrupted by shearing forces, or rupturesspontaneously, allowing blood under arterial pressureto expand into the brain parenchyma. Bleeding stopswhen the tissue pressure around the clot reachesarterial pressure. Experimental studies have shownthat this type of intracerebral hemorrhage leads toacute ischemia in the immediately adjacent brain. Theclot may remain contained within the parenchyma orburst into the ventricle, the subdural space or thesubarachnoid space. In contained hemorrhage, there isa ring of ischemia around the hematoma, which inturn is surrounded by a penumbra of functionallyimpaired but potentially recoverable tissue (Mende-low et al., 1984). The uncontained type of hemorrhage,like subarachnoid hemorrhage, leads to a global fall inCPP with much more widespread ischemic neuronal
damage (Nornes, 1975). The pathogenesis of theischemia has been extensively studied. If an equiva-lent volume of fluid is injected instead of blood, thevolume of ischemia is less than when blood alone isinjected (Jenkins et al., 1990) and the area of ischemiais proportional to the volume of blood or fluid injected(Nath et al., 1986). This ischemia and oligemia may bedue to mechanical compression of the microcirculation(Kingman et al., 1988). The reduction in CBF andischemic neuronal damage is also related to theduration of compression, since deflation of a 50 �lmicroballoon inflated in the rat brain and removed in10 minutes still leaves extensive neuronal damage anda zone of reduced CBF (Nehls et al., 1988). Thissuggests that evacuation of intracerebral clots may dolittle to relieve surrounding ischemic neuronal dam-age, although removal may reduce ICP by relievingthe mass effect. This is clinically logical, since Gal-braith and Teasdale (1981) have reported that sub-sequent deterioration occurs if the ICP exceeds30 mmHg in patients with traumatic intracerebralhemorrhage. This suggests that surgical treatment iseffective for reducing ICP but not for reducing localischemic damage.
Acute intraventricular hemorrhage and subarach-noid hemorrhage may result in acute hydrocephalusnecessitating ventricular drainage although this israre.
4.7 Herniation
4.7.1 TENTORIAL HERNIATION
Apart from elevating ICP and reducing CPP (globaleffects) and causing local compression and vasocon-striction, hematomas may also cause herniation, thecommonest form of which is tentorial herniation. Theuncus of the temporal lobe is pushed through thetentorial edge, compressing the third cranial nerveand the posterior cerebral artery. It is common clinicalknowledge that a IIIrd nerve palsy following a headinjury is a sign of tentorial herniation due to ahematoma, but compression of the posterior cerebralartery is less well recognized. This will produce amedial occipital infarct, which may be the onlyresidual long-term consequence if the clot is removed.These patients may have an homonymous hemianopiaon recovery and the infarct may be demonstrable onmagnetic resonance imaging (Figure 4.13).
4.7.2 SUBFALCINE HERNIATION
Subfalcine herniation may occur as a result of dis-placement by hematomas. This may cause ischemiadue to compression of branches of the anteriorcerebral artery (Figure 4.14).

80 PRIMARY AND SECONDARY BRAIN INJURY
4.7.3 TONSILLAR HERNIATION (MEDULLARY CONE)
Herniation of the cerebellar tonsils is seen particularlywith posterior fossa hematomas. The cerebellar tonsilsbecome displaced through the foramen magnum andmay be found below the level of C2. This is associatedclinically with medullary compression and ultimatelybrain-stem death.
In conclusion, secondary brain damage from hema-tomas can have widespread manifestations and con-sequences but the principle of the diagnosis ofsecondary brain damage due to a hematoma must berecognized so that this rare complication of head injury(less than 1% of all head injuries who attend Emergencyrooms) can be recognized and treated rapidly.
Figure 4.13 MRI showing right medial occipital infarctmonths after posterior cerebral artery compression fromdelayed evacuation of an extradural hematoma with tentor-ial herniation.
Figure 4.14 MRI to show subdural hematoma with sub-falcine shift.
4.8 Brain swelling
Brain swelling may be due to vascular engorgement,or to brain edema. The recognition of venous conges-tion as a cause of elevated ICP, especially in children(Bruce et al., 1981) led to the widespread use ofhyperventilation and hypocapnia in the treatment ofraised ICP. More recently, the dangers of excessivehyperventilation have been recognized (Sharples et al.,1994). Venous congestion secondary to cerebrovas-cular dilatation is also thought to be the mechanismfor the generation of A-(plateau) waves of raised ICP(Rosner, 1993).
Brain edema is due to an increase in the watercontent of brain interstitial space, the neurons or theglia. It has been divided into vasogenic, cytotoxic andinterstitial types (Klatzo, 1979). Some have suggestedthat better terms would be ‘open barrier edema’ forvasogenic edema and ‘closed barrier edema’ forcytotoxic edema (Betz et al., 1989). Recent studies inanimal models (Fukuda, Tanno et al., 1995) have shownthat blood–brain barrier (BBB) breakdown may occurwithin a few minutes of injury, challenging the earlierview that vasogenic (open barrier) edema occurredonly late after head injury. These workers, however, didshow that late BBB breakdown often occurred follow-ing SAH, perhaps because the metallic ions in blood arepotent catalysts of free radicals (Cortez et al., 1989).Swelling of axons may occur soon after primary DAIbecause of changes in axolemma permeability (Pettusand Povlishock, 1995) but it is doubtful that this mildaxonal swelling would be sufficient to cause wholebrain swelling, although it may be associated withtransient axonal malfunction. After 6 hours, retrogradeand anterograde malalignment of neurofilaments takesplace in axons with compaction and mitochondrialswellings. That such mitochondrial abnormalities mayoccur following traumatic brain injury has beensuggested by recent clinical studies in severe headinjury in children (Matthews et al., 1996). Thesemitochondrial changes are rapidly reversible in mildinjuries, and may constitute an anatomical basis forconcussion (Petrus and Povlishock, 1995).
4.8.1 VASOGENIC EDEMA (OPEN BARRIER EDEMA)
As its name implies, open barrier edema is caused bya change to BBB so that protein leaks into the

BRAIN SWELLING 81
interstitial space (Milhorat, 1992). The increasedoncotic pressure draws water with it, so that wateraccumulates between cells. The interstitial space is theprimary pathway for clearing extracellular edemaproteins. The primary mechanism is diffusion that isindependent of pressure gradients (Ohata and Mar-marou, 1992). In the direct infusion edema model inthe rat, Ohata and Marmarou showed that high- andlow-molecular-weight dextrans, as edema markers,moved preferentially towards the cortical surfaces andthe subarachnoid CSF.
This type of edema may also develop later aroundcontusions and intracerebral hemorrhage after severaldays (Marmarou, 1994; Bullock, 1985; Teasdale, 1995;Figure 4.15). In general, vasogenic edema is morecommon in relation to tumors and abscesses than inhead injury. Dexamethasone is effective in reducingvasogenic edema (Todd and Teasdale, 1989). Dex-amethasone has not been shown to be effective in headinjury although, in one controlled trial of high dosesteroids, a subgroup of patients with traumatic intra-cerebral hemorrhage and contusions seemed to have abetter outcome when steroids were given (Grumme etal., 1995).
4.8.2 CYTOTOXIC EDEMA (CLOSED BARRIER EDEMA)
In this type of brain swelling, the cells themselvesswell, as the name ‘cytotoxic edema’ implies. Thecause is usually hypoxia/ischemia (either local orglobal) resulting in a loss of high-energy phosphatesand malfunction of the sodium/potassium pumps.Water enters the cells, and calcium channels open,
with influx of these ions into neurons. The influx ofcalcium is itself cytotoxic and results in cell death(Rappaport et al., 1987). Further ischemia may result inthe release of free radicals, which change the phospho-lipid membrane between the ion channels. This aspectis discussed more fully in Chapter 21. Damage to thephospholipid membrane may have a ‘knock-on effect’,so that the whole cell membrane starts to leak withfurther influx of calcium and water. Ischemic neuronsalso liberate excitatory amino acids (EAA) whichactivate receptor-operated calcium channels in the cellmembrane. These include n-methyl-D-aspartate(NMDA) receptors and AMPA (amino-3-hydroxy-5-methyl-4-isoxazole propionic acid) receptors which,when open, also allow the influx of calcium into thecells (Chapters 7 and 21).
Therapeutic initiatives have focused on the use ofcalcium-channel-blocking drugs and free-radical scav-engers as well as NMDA-receptor antagonists (com-petitive and non-competitive), both experimentallyand, more recently, clinically.
The distribution of cytotoxic edema will dependupon the distribution of ischemia, and it may bedetected by diffusion weighted MRI (Chapter14),T2-weighted MRI (if more severe) or CT, in its mostsevere forms (e.g. stroke), by 8–12 hours after onset. Ifthere is global ischemia due to reduced CPP, infarctionand edema will occur in the arterial boundary zones(Figure 4.3). Around or beneath hematomas, cytotoxicedema may remain focal. If large end-arteries aredamaged or compressed, there may be an infarct inthe appropriate arterial territory (middle, anterior orposterior cerebral artery territory). In each of thesesituations, there will be a surrounding penumbra ofoligemic tissue, which has the potential to benefit frompharmacological and intensive care treatment to opti-mize CBF and O2 delivery.
4.8.3 INTERSTITIAL EDEMA
Hydrocephalus results in increased intraventricularcerebrospinal fluid pressure, with transependymalexudation of CSF through the ependyma into thebrain tissue. This may manifest itself on CT or MRI asperiventricular lucency (PVL). Interstitial edema canbe relieved by ventricular drainage.
All three types of brain edema may coexist in ahead-injured patient, although cytotoxic edema isusually the earliest to appear. The degree of edema inpatients with head injury can be measured withgravimetric columns (Shigeno et al., 1982) and thiscorrelates well with the Hounsfield numbers on CTscan (Bullock et al., 1985) and with MRI proton densityfigures (Marmarou et al., 1990). It is therefore possibleto measure the degree of brain edema in patients usingCT and MR imaging. These techniques have clearly
Figure 4.15 CT scan demonstrating small left parietalcontusion with surrounding edema.

82 PRIMARY AND SECONDARY BRAIN INJURY
demonstrated the different patterns of distribution ofedema in various patients (Figure 4.3). For example, inglobal ischemia there may be boundary zone ischemiawith edema visible on both CT and MRI. Focal edemamay occur with infarction as a result of vasospasmfrom subarachnoid blood (Wilkins and Odom, 1970)or of vessel occlusion (Figure 4.16). Edema may alsooccur around contusions (Figure 4.15) and intra-cerebral hemorrhage (Figure 4.17).
4.8.4 PATHOPHYSIOLOGY OF EDEMA
Magnetic resonance imaging with diffusion weight-ing (DWI) has made it possible to characterizedifferent types of edema with apparent diffusioncoefficients (ADC), which are reduced in cytotoxicedema and increased in vasogenic edema (Ito et al.,1995). Following DAI in the rat acceleration model,cytotoxic edema has been shown to follow secondaryinsults. It is likely that these diffusion-weightedtechniques will detect changes in tissue water diffu-sion in the early stages of head injury (Vink, 1995;Chapter 14). Functional imaging, in particular MRspectroscopy, (e.g. N-acetyl aspartate), is likely toreveal lesions that will correlate with clinical andfunctional deficits.
The plethora of second messenger molecules thatproduce ischemic neuronal damage and increasedwater content experimentally is also being shown tobe involved clinically, using a variety of techniques,including MR spectroscopy, microdialysis and meas-urement of CSF and blood/serum levels in patients.
The variability of the nature and distribution ofedema makes imaging and more accurate time sequencemonitoring desirable if effective treatments are to befound in head injury. Using new MRI modalities, itshould be possible in the future to differentiate thedifferent causes and time courses of focal and globalswelling, each of which may require different treat-ments – mannitol, steroids, calcium antagonists,NMDA-receptor antagonists, ventricular drainage,free radical scavengers or decompressive surgery.
Perhaps only when we are able to divide thepathology in head-injured patients into relevant cate-gories will we be able to improve outcome. To classifyall severely head-injured patients into one diseasegroup (‘head injury’) is unlikely to provide a singleeffective therapeutic option. This has been well dem-onstrated in the several large multicenter trials thathave failed to identify an individual strategy effectivein large heterogeneous groups of head-injuredpatients (Bailey et al., 1991; Todd and Teasdale, 1989;Ward et al., 1985).
4.8.5 BRAIN SWELLING IN CHILDREN
It has long been recognized that brain swelling mayoccur after even relatively minor head injuries inchildren (Bruce et al., 1981). Onset may be rapid butsometimes may not occur until days later. Twoexplanations exist for this rapid onset swelling.
Figure 4.16 CT scan showing focal ischemia due totraumatic internal carotid artery occlusion (note contral-ateral subdural hematoma).
Figure 4.17 CT scan showing acute subdural hematoma,contralateral contusions with surrounding edema and sub-arachnoid hemorrhage beneath the tentorium and in theperimesencephalic cistern.

INFECTION 83
� There is very little space available for expansionwithin the skull of a child, so that a minor degree ofbrain swelling produces a marked increase in ICP.
� Children may have a cerebral circulation whichresponds more actively to trauma than that ofadults. Bruce et al. (1981) favor the latter, but studiesin Newcastle upon Tyne using receiver-operating-characteristic (ROC) curves were able to demon-strate that ICP and CPP have a much greater effecton outcome in children and young adult patientsunder the age of 40 than in older patients, wherethere may be more space available within thecranium (Chambers et al., 1995). This type ofsecondary brain damage should therefore be antici-pated in children and there should therefore be alower threshold for the institution of ICP monitor-ing, and (if necessary) ventilation in children than inadults.
It is generally considered that hyperemia is morecommon in children and, therefore, if there is a role forhyperventilation in the treatment of any patients withhead injury, it is likely to be more effective in childrenand adolescents. Recent studies in children with headinjury in intensive care units have shown that cerebralblood flow may fall with long-term hyperventilationused to treat hyperemia (Sharples et al., 1994) so that itmay be as harmful as in adults.
The reason for the dangerous delayed brain swellingthat sometimes occurs in children with head injuryremains uncertain. In 36 children with severe headinjury, CBF, CMRO2 and CMR lactate was measuredand it was demonstrated that CMRO2 fell sig-nificantly between 12 and 48 hours while lactateproduction increased, suggesting a shift to anaerobicmetabolism of glucose (Matthews et al., 1996a).Improvement in outcome from severe head injury inchildren may therefore occur only when continuousmonitoring of many biochemical and functional para-meters is undertaken and when such results areimmediately available to the medical and nursingstaff. In addition, monitoring to detect such secondaryinsults should be undertaken with equipment pro-grammed to provide an alarm when abnormalitiestake place, because of the unreliability of routinenursing data (Jones et al., 1994).
4.8.6 POTENTIAL THERAPEUTIC INITIATIVES TOLIMIT BRAIN EDEMA AND CELL DAMAGE
The stage in the ischemic cascade at which edemabegins to occur is not yet clear and may vary frompatient to patient. In the early stages, maintaining CPPmay be most important. Later, preventing and treatingbrain edema may reduce focal damage and elevatedICP. Neuroprotective strategies may limit the size of
the penumbra around areas of ischemia. Strategiesmay include the use of free radical scavengers toprevent lipid peroxidation, NMDA- and AMPA-recep-tor antagonists to limit damage from excitatory aminoacids such as glutamate, and calcium antagonists toprevent influx of calcium into cells.
Finally, progressive edema may result from therelease of leukotrienes from white cells and platelets(Hallenback et al., 1986). It is of interest to note thatprofound degrees of ischemia and oligemia can betolerated in hibernating ground squirrels where CBFfalls to 8 ml/100 g/min (Frerichs et al., 1993). In thatstudy it was shown that the hemoglobin level remainsnormal during hibernation, but a severe leukopeniaand thrombocytopenia occur. It is thus possible thatdepletion of platelets and leukocytes may be a‘natural’ form of neuroprotection during hypothermia.Leukopenia and thrombocytopenia may thereforeoffer some form of protection by limiting the pro-gressive edema that follows ischemia. Studies in theintracerebral hemorrhage and middle cerebral arteryocclusion models in the rat have shown that immuno-suppression with whole-body irradiation reduces thewhite cell and platelet count and limits brain edema(Kane et al., 1992; Strachan et al., 1992). Further studiesare required to discover whether or not influencingthe function of white cells and platelets may be ofsome therapeutic value.
4.9 Infection
Infection complicates 5–8% of severely head-injuredpatients. It will usually become evident a few daysafter the injury and will take the form of either a brainabscess or meningitis. It is an important cause ofsecondary deterioration and brain damage. The organ-ism is almost always bacterial and enters the nervoussystem via a breach in the dura associated with afracture either of the vault or of the skull base.
4.9.1 INFECTION AFTER SKULL FRACTURE
(a) Fracture of the vault
It is very unusual for linear fractures without skindisruption to lead to secondary infection. By contrast,compound linear fractures may allow entry of con-taminating bacteria. Compound depressed fracturesare far more likely to lead to secondary infection,although the risk depends to a great extent upon thedegree of depression, the extent of any contaminationand whether or not there has been any penetration.There is also a difference between higher-velocitymissile injuries, which impart kinetic energy to thetissues, causing necrosis and extensive destruction oftissue, and the low-velocity (non-missile) type of injury

84 PRIMARY AND SECONDARY BRAIN INJURY
more common in civilian experience. The latter is lesslikely to cause such severe tissue destruction, sorecovery of vital tissue is more likely to occur. This mayexplain why it was always the custom to debride andelevate compound depressed fractures in wartime, andwhy this teaching influenced the management of non-missile head injuries for many years in civilian practice.Non-missile compound depressed fractures that arenot contaminated may be associated with less extensivetissue destruction and may not therefore requireextensive debridement and elevation of the fracture(van der Heever and van de Merwe, 1986).
The simple linear and depressed fractures of thevault seen with closed head injury are rarely asso-ciated with infection.
(b) Basal skull fracture
This is more common than linear vault fracture aftersevere closed head injury and may involve the anteriorand/or middle fossa. Anterior fossa fractures mayinitially result in bleeding into paranasal sinuses withepistaxis and later with CSF rhinorrhea. However,anterior fossa fractures may result in free communica-tion between the paranasal sinuses and a dural tearwithout overt CSF rhinorrhea. The patient may there-fore present days, weeks, or even years after headinjury with meningitis without ever developing a CSFleak. Therefore a high index of suspicion is necessary inpatients with severe closed head injury where epi-staxis, periorbital bruising (so called ‘raccoon/pandaeyes’) and extensive subconjunctival hemorrhage (Fig-ure 4.18) occurs. Similarly, middle fossa fractures mayor may not be associated with CSF otorrhea. Initially,the only clinical sign of fracture may be bleeding fromthe ear or bruising over the mastoid process (Battle’ssign; Figure 4.19). Fractures of the petrous bone mayalso cause deafness or a lower motor neuron facialnerve palsy. Again, a high index of suspicion of a CSFfistula is needed because, if present, these patients maylater present with meningitis.
4.9.2 MENINGITIS
Whichever the portal of entry, with basal skullfractures organisms tend to be commensals from theparanasal sinuses or middle ear. Pneumococcal infec-tion is therefore commonest, unless patients receiveprophylactic antibiotics, which are more likely toencourage the overgrowth of resistant organisms.With vault fractures, staphylococci are the most likelyorganisms to cross the dura. Staphylococcal meningi-tis is also more likely to follow postoperative woundinfection when a craniotomy has been performed, forexample, for evacuation of a hematoma. Secondaryinfection may also occur with prolonged ventriculardrainage. Meningitis may give rise to hydrocephalus,so that late deterioration in the level of consciousnesswith elevated ICP may occur some days after injury ina patient with very little primary brain damage. Thisagain reinforces the usefulness of the concept ofprimary and secondary brain damage in the manage-ment of patients with head injury.
4.9.3 BRAIN ABSCESS
Post-traumatic brain abscess formation is generallyrare and is almost always associated with a penetrat-ing injury, particularly if there is in-driven foreign
Figure 4.18 Anterior fossa fracture with bilateral ‘pandaeyes’ (note subconjunctival hemorrhage).
Figure 4.19 Middle fossa fracture with Battle’s sign.

PYREXIA FOLLOWING HEAD INJURY 85
material. It is extremely rare to develop a brain abscessfollowing severe closed head injury unless there isfracturing of the posterior wall of the frontal sinus,although it may sometimes be impossible to detectthat a penetrating injury has occurred. Such a case wasseen several years after an apparently closed headinjury. A frontal brain abscess was drained viacraniotomy, and a non-radio-opaque wooden arrow-head was found within the abscess cavity. Thefragment had entered unrecognized at the time of theoriginal head injury. Although rare, such cases demon-strate that brain abscess may be a late complication ofan apparently closed head injury.
4.10 Post-traumatic vascular damage
4.10.1 CAROTID AND MIDDLE CEREBRAL ARTERY(MCA) OCCLUSIONS
The internal carotid artery (ICA) may be damaged inthe neck by acute flexion (Zelenock et al., 1982),extension (Stringer and Kelly, 1980) or directly by asafety belt, in which case a cutaneous abrasion overthe cervical carotid artery is usually seen. These bluntinjuries cause dissection of the intima with stenosis(Ueda et al., 1986), occlusion (Schultz et al., 1984) orthrombosis with distal embolization (Janon, 1970).Total occlusion of the internal carotid artery may leadto major hemisphere infarction that is visible on CTscan. The absence of flow in the internal carotid or theipsilateral middle cerebral artery (MCA) may bedetected with transcranial Doppler (TCD; Schneider etal., 1988). These patients may have relatively slightprimary brain damage but a dense focal deficit(mimicking a stroke).
The ICA may also be damaged at the skull base bybasal skull fractures (Aarabi and McQueen, 1978), inwhich case the patient may have associated severeprimary brain damage and may therefore be coma-tose. The diagnosis of traumatic ICA occlusion istherefore more difficult in these cases, although itshould be suggested by the characteristic infarct on CTor absent MCA flow on TCD.
Occlusion of intracranial arteries may also resultfrom the herniations referred to above. These com-press and occlude the anterior or posterior arteries.Survivors of such herniation may display a classicalinfarct in the vascular territory of that vessel (Figure4.16). The intracranial ICA or MCA may becomedamaged with rapid acceleration or decelerationagainst the sharp sphenoid wing. Primary traumaticMCA occlusions are well recognized in young patientswith closed head injury and may be associated withdissecting aneurysms (Kunze and Schiefer, 1971; Satoet al., 1971) and were more easily recognized in the
pre-CT era, when angiography was used commonly inclosed head injury.
4.10.2 TRAUMATIC SUBARACHNOID HEMORRHAGE
Traumatic subarachnoid hemorrhage (SAH) is knownto be associated with cerebral vasospasm in more than40% of cases (Macpherson and Graham, 1973) andwith cerebral blood flow and TCD monitoring tech-niques the incidence of vasospasm was found to be27% (Martin et al., 1992). Traumatic vasospasm follow-ing closed head injury is therefore an important causeof cerebral ischemia which is analogous to that foundin spontaneous SAH.
4.10.3 ANEURYSMS
It may be difficult to differentiate a pre-existinganeurysm that ruptures as a result of trauma from atrue post-traumatic aneurysm. Undoubtedly bothtypes exist but it may be impossible to distinguish onefrom the other, although true post-traumatic aneur-ysms tend to be more common in the distal MCA(Fleischer et al., 1975). The true trauma-inducedaneurysm may also enlarge (Bendoit and Wortzman,1973) and is at risk of rupturing.
4.10.4 FISTULAE
Blunt injuries may lead to arteriovenous fistulae,which are usually associated with a cranial bruit. Thecommonest site is the carotid cavernous fistula, whichoften develops several days after the injury. It ischaracterized by proptosis with vasodilation of thesclera and may go on to cause SAH (Dohrmann et al.,1985). Fistulae may occur at other sites related to skullfractures (Feldman et al., 1980). They may also giverise to late SAH or even subdural hemorrhage inpatients who otherwise have little or no primary braindamage.
4.11 Pyrexia following head injury
The development of pyrexia following head injurymay be a sign of brain-stem damage. However theoccurrence of pyrexia was one of the most significantpredictors of mortality and morbidity in a series of 124adult head-injured patients who were monitoredcontinuously (minute by minute) in Edinburgh (Joneset al., 1994). There is also a revived interest inhypothermia as form of neuroprotection in head-injured patients: a multicenter prospective random-ized controlled trial is currently under way in theUSA, funded by the National Institute of Health.

86 PRIMARY AND SECONDARY BRAIN INJURY
4.12 Conclusion
While many classifications of brain damage are basedon pathological findings, biochemical and radiologicalfeatures, the importance of classifying brain damageclinically into primary and secondary types is that anunderstanding of the pathology will lead to moreappropriate management. Most importantly, it helpsnon-specialists to understand the role of the preven-tion and treatment of brain swelling, hemorrhage andinfection. It is important to teach medical students,nurses and doctors how to recognize primary andsecondary brain damage. They may then be better ableto prevent it from occurring in the first place or tominimize the effects once the cycle of secondary braindamage is initiated. In this way, through team coop-eration, the gold standard of head injury management– eliminating secondary brain damage – may bereached.
4.13 References
Aarabi, B. and McQueen, J. (1978) Traumatic internal carotid occlusion at thebase of the skull. Surgical Neurology, 10, 233.
American College of Surgeons (1993) Advanced Trauma Life Support CourseManual, American College of Surgeons, Washington, DC, p. 168.
Andrews, P., Piper, I. et al. (1990) Secondary insults during intrahospitaltransport of head injured patients. Lancet, 335, 327.
APLS (1993) Advanced Paediatric Life Support Manual. British Medical JournalPublications, London, p. 155.
Bailey, I., Bell, A., Gray, J. et al. (1991) A trial of the effect of nimodipine onoutcome after head injury. Acta Neurochirurgica (Vienna), 110, 97–105.
Benoit, B. and Wortzman, G. (1973) Traumatic cerebral aneurysms. Clinicalfeatures and natural history. Journal of Neurology, Neurosurgery and Psy-chiatry, 36, 127.
Betz, A., Iannotti, F. et al. (1989) Brain oedema: a classification based on blood-brain barrier integrity. Cerebrovascular Brain Metabolism Review, 1, 133.
Braakman, T. and the European study group on Nimodipine in severe headinjury (1994) A multicentre trial of the efficacy of Nimodipine on outcomeafter severe head injury. Journal of Neurosurgery, 80, 797.
Bruce, D. A., Alavi, A., Bilaniuk, L. et al. (1981) Diffuse cerebral swellingfollowing head injuries in children: the syndrome of ‘malignant brainoedema’. Journal of Neurosurgery, 54, 170–178.
Bullock, R. and Teasdale, G. (1990) Surgical management of traumaticintracranial haematomas, in Handbook of Clinical Neurology, vol. 13(57), HeadInjury, (eds P. J. Vinken, G. W. Bruyn and R. Braakman), Elsevier,Amsterdam, pp. 249–298.
Bullock, M., Smith, R. et al. (1985) Brain specific gravity and CT scan densitymeasurements after human head injury. Journal of Neurosurgery, 63, 64.
Bullock, R., McCulloch, J. et al. (1990) Focal ischemic damage is reduced byCPP-ene. Studies in two animal models. Stroke, 21(Suppl. III), 32.
Bullock, R., Zauner, A. et al. (1995) Excitatory amino acid release patterns aftersevere human head injury – experience with microdialysis in 30 patients.Journal of Neurotrauma, 12, 372.
Cameron, M. (1978) Chronic subdural haematoma: a review of 114 cases.Journal of Neurology, Neurosurgery and Psychiatry, 41, 834.
Chambers, I., Choksey, M. et al. (1995) Receiver operator characteristic (ROC)curves: a new approach to the analysis of cerebral perfusion pressure andintracranial pressure in relation to outcome in severe head injury. Journal ofNeurology, Neurosurgery and Psychiatry, 58, 386.
Chan, K.-H., Mann, K. et al. (1990) The significance of skull fracture in acutetraumatic intracranial haematomas in adolescents. Journal of Neurosurgery,72, 189.
Choksey, M. S., Costa, D. C., Iannotti, F. et al. (1991) 99Tc-M-HMPAO SPECTstudies in traumatic intracerebral haematoma. Journal of Neurology, Neu-rosurgery and Psychiatry, 54, 6–11.
Contant, C. F., Robertson, C. S., Gopinath, S. P. et al. (1993) Determination ofclinically important thresholds in continuously monitored patients withhead injury (abstract). Journal of Neurotrauma, 10, S57.
Cortbus, F., Jones, P. A., Miller, J. D. et al. (1995) Cause distribution andsignificance of episodes of reduced cerebral perfusion pressure followinghead injury (abstract). Journal of Neurotrauma, 12, 368.
Cortez, S., McIntosh, T. et al. (1989) Experimental fluid percussion braininjury: vascular disruption and neuronal and glial alterations. BrainResearch, 482, 271.
Cushing, H. (1901) Concerning a definite regulatory mechanism of thevasomotor centre which controls blood pressure during cerebral compres-sion. Bulletin of the Johns Hopkins Hospital, 12, 290.
Cushing, H. (1903) The blood pressure reaction of acute cerebral compression,illustrated by cases of intracranial haemorrhage. American Journal of MedicalScience, 125, 1017.
Davis, M. and Barer, D. (1995) Theoretic aspects of neuroprotection in acuteischaemic stroke. 1: Basic mechanisms. Vascular Medicine Review, 6,283–298.
Dohrmann, P., Batjer, H. et al. (1985) Recurrent subarachnoid haemorrhagecomplicating a traumatic carotid cavernous fistula. Neurosurgery, 17, 480.
Enevoldsen, E. M., Cold, G. E., Jensen, F. T. et al. (1976) Dynamic changes inregional cerebral blood flow, intraventricular pressure, cerebrospinal fluidpH and lactate levels during the acute phase of head injury. Journal ofNeurosurgery, 44, 191–214.
Feldman, R., Hieshima, G. et al. (1980) Traumatic dural arteriovenous fistulasupplied by scalp, meningeal, and cortical vessels: case report. Neurosurgery,6, 670.
Fleischer, A., Patton, J. et al. (1975) Cerebral aneurysms of traumatic origin.Surgical Neurology, 4, 233.
Frerichs, K., Kennedy, C. et al. (1993) Local cerebral blood flow and glucosemetabolism during hibernation, a model for natural tolerance to cerebralischaemia. Journal of Cerebral Blood Flow and Metabolism, 13(Suppl. 1),S422.
Fukuda, K., Tanno, H. et al. (1995) The Blood–Brain Barrier disruption tocirculating proteins in the early period after fluid percussion brain injury inrats. Journal of Neurotrauma, 12, 315.
Galbraith, S. and Teasdale, G. (1981) Predicting the need for operation in thepatient with an occult traumatic intracranial haematoma. Journal ofNeurosurgery, 55, 75.
Gentleman, D. (1992) Causes and effects of systemic complications amongseverely head injured patients transferred to a neurosurgical unit. Inter-national Surgery, 77, 297.
Gentleman, D. and Jennett, B. (1981) Hazards of interhospital transfer ofcomatose head injured patients. Lancet, ii, 853.
Germon, T. J., Picydell-Pearce, C. W. et al. (1995) Can near infraredspectroscopy detect changes in regional oxyhaemoglobin due to functionalactivation? Journal of Neurology, Neurosurgery and Psychiatry, 60, 2421.
Gopinath, S. P,. Robertson, C. S., Contant, C. F. et al. (1994) Jugular venousdesaturation and outcome after head injury. Journal of Neurology, Neu-rosurgery and Psychiatry, 57, 717–723.
Graham, D. I., Adams, J. H. and Doyle, E. (1978) Ischaemic brain damage infatal non-missile head injuries. Journal of the Neurological Sciences, 39,213–234.
Graham, D., Ford, I. et al. (1989) Ischaemic brain damage is still common infatal non-missile head injury. Journal of Neurology, Neurosurgery andPsychiatry, 52, 346.
Graham, D., Jennett, B. et al. (1995) The structural basis of the vegetative stateafter acute head injury. Journal of Neurotrauma, 12, 345.
Green, M., Marciano, F. et al. (1995) Traumatic subarachnoid haemorrhage:impact on clinical course and outcome during acute hospitalisation in non-penetrating head injury. Journal of Neurotrauma, 12, 476.
Group of Neurosurgeons (1984) Guidelines for initial management after headinjury in adults. British Medical Journal, 288, 983.
Grumme, T., Baethmann, A. Kolodziejcvyk, D. et al. (1995) Treatment ofpatients with severe head injury by triamcinolone – a prospective,controlled multicenter clinical trial of 396 cases. Research in ExperimentalMedicine, 195, 217–229.
Hallenback, J., Dutka, A. et al. (1986) Polymorphonuclear leucocyte accumula-tion in brain regions with low blood flow during the early postischaemicperiod. Stroke, 17, 246.
Hatfield, R., Gill, R. et al. (1992) Dose response relationship and therapeuticwindow for Dizocilpine (MK801) in a rat focal ischaemia model. EuropeanJournal of Pharmacology, 216, 1–7.
Hewer, R. and Wood, V. (1989) Availability of computed tomography of thebrain in the United Kingdom. British Medical Journal, 298, 1219.
Ito, J., Barzo, P., Fatouros, P. et al. (1995) Characterization of edema bydiffusion weighted imaging following closed head injury and secondaryinsult in the rat. Journal of Neurotrauma, 12, 475.
Jackowski, A. (1992) Disordered sodium and water in neurosurgery. BritishJournal of Neurosurgery, 6, 173.
Jamieson, K. and Yelland, J. (1968) Extradural hematoma: report of 167 cases.Journal of Neurosurgery, 29, 13.
Janon, E. (1970) Traumatic changes in the internal carotid artery with basalskull fractures. Radiology, 96, 55.
Jenkins, A., Mendelow, A. D., Graham, D. I. et al. (1990) Experimentalintracerebral haematoma: the role of blood constituents in early ischaemia.British Journal of Neurosurgery, 4, 45–52.
Jones, P., Piper, I. et al. (1993) Microcomputer based detection of secondaryinsults and 12 month outcome after head injury. Journal of Neurotrauma,10(Suppl. 1), S102.

REFERENCES 87
Jones, P. A., Andrews, P. J. D., Midgley, S. et al. (1994) Measuring the burdenof secondary insults in head-injured patients during intensive care. Journalof Neurosurgery and Anaesthetics, 6, 4–14.
Kakarieka, A., Harders, A. et al. (1995) Traumatic subarachnoid haemorrhage:a clinical entity and its treatment with nimodipine. Journal of Neurotrauma,12, 375.
Kane, P., Modha, P. et al. (1992) The effect of immunosuppression on thedevelopment of cerebral oedema in an experimental model of intracerebralhaemorrhage: whole body and regional irradiation. Journal of Neurology,Neurosurgery and Psychiatry, 55, 781.
Kane, P., Cook, S. et al. (1994) Cerebral oedema following intracerebralhaemorrhage: the effect of the NMDA receptor antagonists MK-801 andD-CPPene. Acta Neurochirurgica, 60(Suppl.), 561.
Kingman, A., Mendelow, A. et al. (1988) Experimental intracerebral mass:description of model, intracranial pressure changes and neuropathology.Journal of Neuropathology and Experimental Neurology, 47, 128.
Kirkpatrick, P., Smielewski, P. et al. (1995) Detection of cerebral hypoxic eventsusing near infrared spectroscopy in head injured patients. Journal ofNeurotrauma, 12, 374.
Klatzo, I. (1979) Cerebral oedema and ischaemia, in Recent Advances inNeuropathology, (ed. W. T. Smith and J. B. Cavanagh) Churchill Livingstone,Edinburgh, p. 27.
Kohi, Y., Mendelow, A. et al. (1984) Extracranial insults and outcome inpatients with acute head injury – relationship to the Glasgow Coma Scale.Injury, 16, 25.
Kossmann, T., Morganti-Kossmann, M. et al. (1995) Production of complementproteins in human brain injury correlates to intraventricular cerebrospinalfluid interleukin-6 levels. Journal of Neurotrauma, 12, 461.
Kunze, S. and Schiefer, W. (1971) Angiographic demonstration of a dissectinganeurysm of the middle cerebral artery. Neuroradiology, 2, 201.
Lenkinski, R. E., Gennarelli, T. A., McIntosh, T. K. et al. (1995) Magneticresonance spectroscopy of the injured brain. Journal of Neurotrauma, 12, 351.
McGraw, C. (1989) A cerebral perfusion pressure of greater than 80 mmHg ismore beneficial, in Intracranial Pressure VII, (eds J. T. Hoff and A. L. Betz),Springer-Verlag, Berlin.
Macpherson, P. and Graham, D. (1973) Arterial spasm and slowing of thecerebral circulation in the ischaemia of head injury. Journal of Neurology,Neurosurgery and Psychiatry, 36, 1069.
Marmarou, A., Fatouros, P. et al. (1990) In vivo measurement of brain water byMRI. Acta Nerurochirurgica (Supplement), 51, 123.
Marmarou, A. (1994) Traumatic brain oedema – an overview. Acta Neurochir-urgica, S60, 421–424.
Martin, N. A., Doberstein, C., Zane, C. et al. (1992) Postraumatic cerebralarterial spasm: transcranial Doppler ultrasound, cerebral blood flow, andangiographic findings. Journal of Neurosurgery, 77, 575–583.
Matthews, D., Matthews, J. et al. (1995) Changes in cerebral oxygenconsumption are independent of changes in body oxygen consumptionafter severe head injury in childhood. Journal of Neurology, Neurosurgery andPsychiatry, 59, 359.
Matthews, D., Aynsley-Green, A. et al. (1996a) Modified hormonal effects onfat metabolism following severe head injury in children. PaediatricResearch.
Matthews, D., Sharples, P. et al. (1996) Evidence for progressive changes incerebral mitochondrial function in severely head-injured children. Journal ofNeurology, Neurosurgery and Psychiatry, 59, 359.
Maxwell, W. (1995) Microtubular changes in axons after stretch injury. Journalof Neurotrauma, 12, 363.
Mendelow, A., Karmi, M. et al. (1979) Extradural haematoma: effect of delayedtreatment. British Medical Journal, i, 1240.
Mendelow, A. D., Teasdale, G. M., Jennett, B. et al. (1983) Risks of intracranialhaematoma in head injured patients. British Medical Journal, 287,1173–1176.
Mendelow, A., Bullock, R. et al. (1984) Intracranial haemorrhage induced atarterial pressure in the rat: Part 2. Short term changes in local cerebral bloodflow measured by autoradiography. Neurology Research, 6, 189.
Mendelow, A. D., Teasdale, G. M., Russell, T. et al. (1985) Effect of mannitol oncerebral blood flow and cerebral perfusion pressure in human head injury.Journal of Neurosurgery, 63, 43–48.
Mendelow, A., Chambers, I. et al. (1994) Cerebral perfusion pressure: the 60minute average minimum value and outcome from head injury. Journal ofNeurotrauma, 10(Suppl 1).
Mikulis, D. (1995) Functional imaging in neurotrauma. Journal of Neurotrauma,12, 351.
Milhorat, T. (1992) Classification of the cerebral oedemas with reference tohydrocephalus and pseudotumour cerebri. Child’s Nervous System, 8, 301.
Miller, J. (1993) Monitoring the brain of patients with head injury: transcranialDoppler sonography. Journal of Neurotrauma, 10(Suppl. 1), S109.
Mohamed, A., Gotoh, O. et al. (1985) Effect of pretreatment with the calciumantagonist, Nimodipine on local cerebral blood flow and histopathologyafter middle cerebral artery occlusion. Annals of Neurology, 18, 705.
Nath, F., Mendelow, A. et al. (1985) Chronic subdural haematoma in the CTscan era. Scottish Medical Journal, 30, 152.
Nath, F., Jenkins, A. et al. (1986) Early haemodynamic changes in experimentalintracerebral haemorrhage. Journal of Neurosurgery 65, 697.
Nath, F., Kelly, P. et al. (1987) Experimental intracerebral haemorrhage: effectson blood flow, capillary permeability and histochemistry. Journal ofNeurosurgery, 66, 555.
Nehls, D., Mendelow, A. et al. (1988) Experimental intracerebral haemorrhage:progression of haemodynamic changes after production of a spontaneousmass lesion. Neurosurgery, 23, 439.
Nelson, P. B., Seif, S. M., Maroon, J. C. and Robinson, A. G. (1981)Hyponatraemia in intracranial disease. Perhaps not the syndrome ofinappropriate secretion of antidiuretic hormone (SIADH). Journal ofNeurosurgery, 55, 938–941.
Nornes, H. (1975) Monitoring patients with intracranial aneurysms. ClinicalNeurosurgery, 22, 231–331.‘
Obrist, W. D., Gennarelli, T. A., Segawa, H. et al. (1979) Relation of cerebralblood flow to neurological status and outcome in head-injured patients.Journal of Neurosurgery, 51, 292–300.
Ohata, K. and Marmarou, A. (1992) Clearance of brain oedema andmacromolecules through the cortical extracellular space. Journal of Neuro-surgery, 77, 387.
Oppenheimer, D. (1968) Microscopic lesions in the brain following headinjury. Journal of Neurology, Neurosurgery and Psychiatry, 31, 299.
Pettus, E. and Povlishock, J. (1995) Evidence for prolonged alterations inaxolemmal permeability following traumatic brain injury. Journal ofNeurotrauma, 12, 475.
Piper, I., Midgely, S. et al. (1995) Intracranial pressure waveform indicescorrelate with cerebral perfusion pressure but fail to predict efficacy ofmannitol therapy for raised ICP: a prospective study in head injuredpatients. Journal of Neurology, Neurosurgery and Psychiatry, 58, 387.
Poon, W., Mendelow, A. et al. (1989) Secretion of antidiuretic hormone inneurosurgical patients: appropriate or inappropriate? Australian and NewZealand Journal of Surgery, 59, 173.
Povlishok, J. (1992) Traumatically induced axonal injury: pathogenesis andpathobiological implications. Brain Pathology, 2, 1.
Povlishock, J. (1995) Traumatically induced delayed axotomy triggered byvaried cytoskeletal and axolemmal abnormalities. Journal of Neurotrauma,12, 363.
Rappaport, Z., Young, W. et al. (1987) Regional brain calcium changes in therat middle cerebral artery occlusion model of ischaemia. Stroke, 18, 760.
Rosner, M. (1993) Cyclic CSF pressure waves causally related to systemicarterial blood pressure, in Intracranial Pressure VIII, (eds C. J. J. Avezaat, J. H.M. van Eindhoven, A. I. R. Maas and J. T. J. Tans), Springer-Verlag,Berlin.
Santos, A., Shu, E. et al. (1995) Extradural haematoma in children: analysis of74 cases. Journal of Neurotrauma, 12, 389.
Sato, O., Bascom, J. et al. (1971) Intracranial dissecting aneurysm: case report.Journal of Neurosurgery, 35, 483.
Schneider, P., Rossman, M. et al. (1988) Effect of internal carotid arteryocclusion on intracranial haemodynamics: transcranial Doppler evaluationand clinical correlation. Stroke, 19, 589.
Schroder, M., Muizelaar, J. et al. (1993) Regional ischemia and regionalcerebral blood volume (CBV) after severe head injury in man. Journal ofNeurotrauma, 10(Suppl. 1), S57.
Schultz, U., Kutemeyer, et al. (1984) Traumatic occlusion of both internalcarotid arteries. Journal of Neurology, 231, 233.
Seelig, J. M., Becker, D. P., Miller, J. D. et al. (1981) Traumatic acute subduralhaematoma. Major mortality reduction in comatose patients treated withinfour hours. New England Journal of Medicine, 304, 1511–1518.
Sharples, P. M., Stuart, A. G., Matheras, D. S. et al. (1994) Cerebral blood flowand metabolism in children with severe head injuries. Part I: Relation toage, Glasgow Coma Score, outcome, intracranial pressure and time afterinjury. Journal of Neurology, Neurosurgery and Psychiatry, 57, 145–152.
Sharples, P., Matthews, D. et al. (1995) Cerebral blood flow and metabolism inchildren with severe head injuries. Part 2: Cerebrovascular resistance and itsdeterminants. Journal of Neurology, Neurosurgery and Psychiatry, 58, 153–159.
Shigeno, T., Brock, M. et al. (1982) The determination of brain water content:microgravimetry versus drying–weighing method. Journal of Neurosurgery,57, 99.
Sinar, E., Mendelow, A., Graham, D. and Teasdale, G. (1987) Experimentalintracerebral haemorrhage: effects of a temporary mass lesion. Journal ofNeurosurgery, 66, 568–576.
Stevenson, G., Brown, H. et al. (1964) Chronic venous epidural haematoma atthe vertex. Journal of Neurosurgery, 21, 887.
Strachan, R., Kane, P. et al. (1992) Immunosuppression by whole-bodyirradiation and its effect on oedema in experimental cerebral ischaemia.Acta Neurologica Scandinavica, 86, 256.
Stringer, W. and Kelly, D. (1980) Traumatic dissection of the extracranialinternal carotid artery. Journal of Neurosurgery, 6, 123.
Teasdale, G. (1995) Head injury. Journal of Neurology, Neurosurgery andPsychiatry, 58, 526–539.
Teasdale, G., Murray, G. et al. (1990) Risks of acute traumatic intracranialhaematoma in children and adults: implications for the management ofhead injuries. British Medical Journal, 300, 363.
Todd, N. V. and Teasdale, G. M. (1989) Steroids in human head injury. Clinicalstudies, in Steroids in Diseases of the Central Nervous System, (ed. R. Capildio),John Wiley & Sons, New York, pp. 151–161.

88 PRIMARY AND SECONDARY BRAIN INJURY
Treadwell, l. and Mendelow, A. (1994) Audit of head injury management inthe Northern Region. British Journal of Nursing, 3, 136.
Tsuji, O., Marmarou, A. et al. (1995) Electrolyte and excitatory amino acidsurge following closed head injury and secondary insult in the rat. Journalof Neurotrauma, 12, 475.
Ueda, T., Kikuchi, H. et al. (1986) Traumatic stenosis of the internal carotidartery in children. Surgical Neurology, 26, 368.
Van der Heever, C. and van de Merwe, D. (1986) Management of depressedskull fractures: selective conservative management of non-missile injuries.Journal of Neurosurgery, 71, 186.
Vink, R. (1995) Functional magnetic resonance characterization of the injuredbrain: can MR provide clinically relevant information beyond conventionalimaging? Journal of Neurotrauma, 12, 351.
Ward, J. D., Becker, D. P., Miller, J. D. et al. (1985) Failure of prophylactic
barbiturate coma in the treatment of severe head injury. Journal ofNeurosurgery, 62, 383.
Wilkins, R. and Odom, G. (1970) Intracranial arterial spasm associated withcraniocerebral trauma. Journal of Neurosurgery, 32, 626.
Wong, F., Piper, I. et al. (1995a) Determination of cerebral perfusion pressurethresholds in head injury patients. Journal of Neurology, Neurosurgery andPsychiatry, 58, 387.
Wong, F., Piper, I. et al. (1995b) Differences in treatment thresholds of cerebralperfusion pressure in head injuries. Journal of Neurotrauma, 12, 413.
Wyper, D., Hadley, D. et al. (1995) Recovery after closed head injury:functional image correlates. Journal of Neurotrauma, 12, 472.
Zelenock, G. B., Kazmers, A. et al. (1982) Extracranial internal carotid arterydissections. Non-iatrogenic traumatic lesions. Archives of Surgery, 117,425.