PHARMACOGENOMICS
PHARMACOGENOMICSDr. Santoshkumar.Jeevangi M.DAssociate
ProfessorDept. of PharmacologyMR Medical collegeGulbarga
1.Introduction2. The goal of Pharmacogenomics3. History4.
Development of Pharmacogenomics 5. Human Genome 6. Types of genetic
variants.7. Adverse Drug Reactions Attributed to Genetic
Differences8. Genetic Polymorphism in Drug Transport 9. Genetic
Polymorphism in Drug Targets10. Pharmacogenomics and Drug
development11. Pharmacogenomics in clinical practice12.
Conclusion
IntroductionThis is recent branch which overlaps
pharmacogenetics.
Pharmacogenetics is the study of the genetic basis for variation
in the drug response.
DefinitionPharmacogenomics: The use of genetic information to
explain inter-individual differences in drug responses or to
individualized dosage of drugs for patients with known genetic
polymorphisms is referred to as Pharmacogenomics.Pharmacogenetics
(PGT)and pharmacogenomics(PGX) are both important disciplines
involved in the study of genes that code for drug-metabolizing
enzymes, drug receptors, drug transporters, and ion channels or
efflux pumps. Many of the above are new factors involved in
determining how genetic variation contributes to variation in the
response to drugs, including the ultimate fate of the drug and its
ability to exert a therapeutic response without undue side
effects.
The environment, diet, age, lifestyle, and state of health can
influence a person's response to drug. An understanding of an
individual's genetic makeup is thought to be the key to creating
personalized drugs with greater efficacy and
safety.Pharmacogenomics involves study of the role of genes and
their genetic variations (DNA, RNA level) in the molecular basis of
disease, and therefore, the resulting pharmacologic impact of drugs
on that disease.
Understanding the genetic and molecular differences in disease
etiology and drug mechanism produce insight on how a patient will
respond to a given drug. For example, the monoclonal antibody
Herceptin was designed to treat a subset of breast cancer patients
who overexpress the HER-2 (human epidermal growth factor
receptor-2) gene. Patients who lack HER-2 overexpression are
considered to be non-responders to Herceptin therapy.
In the past, such differences would be apparent only after a
trial-and-error period. This genetic knowledge improves our ability
to select or design the proper drug for individuals suffering from
a disease with a varying range of genetic defects.
The goal of PharmacogenomicsPatient or population specific
treatments.Avoidance of adverse effects or inefficacy of
drugs.Drug-target design.
History1st century A.D: Favism After eating fava beans,
Hemolytic anemia, G6PD deficiency.1950s:Isoniazid (neuropathy),
succinylcholine (apnea)1980s: Debrisoquine metabolism (1st
cytochrome P450-mediated polymorphism)
Development of Pharmacogenomics Pharmacogenomics developed
rapidly as a result of advances in molecular genetics and genomics.
High-throughput tests such as microarray technology allow many
human genes and their sequences to be detected rapidly. The
previously held notion of the monogenic nature of disease (one gene
causing one disorder) is yielding to the concept of polygenic
disorders, by which several, or even dozens, of genes may be
differentially expressed compared to normal, healthy tissue.
Recognition of the genotypes associated with drug disposition
and metabolism and the ability to obtain a "specific
pharmacogenetic profile" for the patient will individualize drug
therapy and reduce drug interactions. To realize this lofty
objective, pharmacogenomics research aims to elucidate these
polygenic (multiple-gene) determinants of drug effects. The
interplay of genetic polymorphism with inter-individual differences
in pharmacokinetics and pharmacodynamics is well reviewed.
Human Genome The human genome has 2.91 billion base pairs.
and approximately 35.000 genes.
NucleotidesThe genetic information is coded in the two helical
strands of DNA. DNA consists of four basic nitrogenous substance or
bases (C, cytosine; A, adenine; T, thymine; and G, guanine), which
combine with deoxyribose and phosphate to form the respective
nucleotides. The four nucleotides are combined in unique sequences
for each gene. Genes are coded in a special region or locus in the
DNA.
AllelesThe cell is homozygous if the genetic sequences occupying
the locus are the same on the maternal and paternal chromosome. If
they are different, the cell is heterozygous. When more than one
alternative forms of a gene exists, they are referred to as alleles
of the gene.
PhenotypingPhenotyping is an observable biochemical measure. It
could determine the presence and activity of a particular enzyme in
the tissue biopsy. Metabolic phenotyping measure the level of
metabolites in a person after administration of a drug.Phenotyping
is usually straight forward, but also more invasive and
dangerous.
Genotyping Genotyping determine the specific genetic code of an
individual. It is safer because it can be done on an easily
obtainable sample of the tissue ( Buccal cells).DNA is extremely
stable if appropriately extracted and stored and unlike many
laboratory tests, genotyping need to be performed only once,
because DNA sequence is generally invariant throughout an
individual lifetime. Results often are harder to interpret.
Genotypes to PhenotypesPhenotyping gives the end result of
pharmacogenetic difference between people and genotyping gives the
root cause of different response.
Types of genetic variants.1.SNPs.2.Indels
(Insertions/Deletions).3.Copy number variations (CNVs).Genetic
PolymorphismGenetic Polymorphism: A difference in DNA sequence
among individuals, groups, or populations. Genetic Mutation: A
change in the nucleotide sequence of a DNA molecule. Genetic
mutations are a kind of genetic polymorphism.
1.SNPs Single Nucleotide PolymorphismA Single Nucleotide
Polymorphism is a source variance in a genome. A SNP is a single
base mutation in DNA. SNPs are the most simple form and most common
source of genetic polymorphism in the human genome (90% of all
human DNA polymorphisms).
SNPs occur in about one of every 1001500 base pairs between two
unrelated individuals. Any two individuals may differ by 0.1% of
their more than 2.91 billion base pairs. Common SNPs are those that
occur at frequencies of greater than 1%. Once a large number of
these SNPs and their frequencies in different populations are
known, they can be used to correlate a patient's genetic
"fingerprint" and the patient's probable individual drug
response.
Two types substitutionsThere are two types of nucleotide base
substitutions resulting in SNPs:Transition: Substitution between
purines (A, G) or between pyrimidines (C, T). Constitute two thirds
of all SNPs.Transversion: Substitution between a purine and a
pyrimidine.
Types of Coding Region SNPs.
Synonymous: The substitution causes no amino acid change to the
protein it produces.This is also called a silent
mutation.Non-Synonymous: The substitution results in an alteration
of the encoded amino acid. One half of all coding sequence SNPs
result in non-synonymous codon changes.
Haplotype
In the most basic sense, a haplotype is a haploid
genotype.Haplotype: Particular pattern of sequential SNPs (or
alleles) found on a single chromosome. These SNPs tend to be
inherited together over time.
Microarrays, Mass spectrometry and Sequencing are all used to
accomplish haplotyping.Detection of known SNPs SNP Genotyping and
HaplotypingDetection, high-throughput genotyping, haplotyping, the
haplotype map. High-Throughput SNP GenotypingHigh-throughput SNP
genotyping is the process of quickly and cost-effectively
identifying the SNP values in as many different individual human
genomes as possible.Technology exists for performing 1,00,000
genotypes/day (Orchid and Affymetrix).Steps of SNP genotyping
involve , DNA sample preparation, PCR amplification , Microarray
assays.
2.Indels & 3.CNVs 2.IndelsInsertions/DeletionsEx.68bp
insertion in Cystathionine beta synthase.Ex . TA repeat in UGT1A1 (
UDP-glucuronosyl-transferase ) ,Toxicity of Irinotecan
3.CNVs Gene Duplications.Ex.CYP2D6,upto 13 copies Large
deletionsEx . entire GSTT1 and GSTM1. (Thiopurine Methyltransferase
)
SNP Applications
Pharmacogenomics ,diagnostic genomics ,functional proteomics and
therapeutic genomics.
All of these mechanism have been implicated in common germ line
Pharmacogenetic Polymorphisms examples.
1.TPMT( Thiopurine Methyltransferase)2.ABCB1 (Multidrug
resistance transporter-PGP)3.CYP450 (Cysta-thionine beta synthase)
4.UGT ( UDP-glucuronyl transferase)5.GST (Glutathione
s-transferase)
Adverse Drug Reactions Attributed to Genetic Differences
In 1950s, researchers realized that some adverse drug reactions
were caused by genetically determined variations in enzyme
activity. More recently, a review of the Pharmacogenetic literature
showed that a sizable portion of ADRs (~30%) involved in drug
therapy implicated genetic polymorphism of drug metabolism by
CYP2D6.
Examples Prolonged muscle relaxation in some subjects after
receiving Succinylcholine was explained by an inherited deficiency
of a plasma pseudo-cholinesterase. Hemolysis caused by Primaquine
is recognized as being caused by inherited variants of G6PD. Slow
metabolism of isoniazid in some patients has been found to be the
cause of peripheral neuropathy. More recently, adverse drug
reactions of debrisoquin have led to the discovery of the genetic
polymorphism of the drug-metabolizing enzyme (CYP2D6).
It is important to determine whether the variation in ADR is
truly genetic or due to other factors. A method used to distinguish
hereditary and environmental components of variability is the
comparison of monozygotic and dizygotic twins, or
pharmacokinetically by repeated drug administration and comparison
of the variability of the responses within and between
individuals.
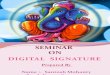
If test carried in a large number of subjects, their response
can be plotted as uni-model/Bell-shaped, Bi-modal and Tri-modal. A
uni-model distribution (continuous variation) implies that the drug
metabolism in under of many genes (Polygenic).Bimodal and Tri-modal
(Dis-continuous variation) implies that the drug metabolism in
under of one gene.( Monogenic)
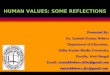
If normal metabolism of drug is controlled by a dominent gene
R,and if some people are unable to metabolize the drug because they
have homozygous for a recessive gene r, then there will be 3
classes of individuals:RR,Rr,rr. If the responses of RR and Rr are
indistinguishable ,then then a Bio-model distribution will
result.If RR and Rr are distinguishable, then a Tri-modal
distribution will result.Each peak or mode representing a different
phenotype.
Uni-modal (Polygenic)
Number of individualsResponse to drugs35Tri-modal Distribution
(Monogenic)
From Pratt WB,Taylor P. Fig 7-5b36
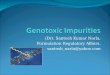
From: Evans WE, Relling MV. Pharmacogenomics: Translating
functional genomics into rational therapeutics. Science
286:487-491, 1999.II. Genetic polymorphisms in drug metabolizing
enzymes
Table 12.2 Clinically Important Genetic Polymorphisms of Drug
Metabolism that Influence Drug ResponseEnzyme/ReceptorFrequency of
PolymorphismDrugDrug Effect/Side EffectCYP2C91428%
(heterozygotes)Warfarin Hemorrhage 0.21% (homozygotes)Tolbutamide
HypoglycemiaPhenytoin Phenytoin toxicityGlipizide Hypoglycemia
Losartan Decreased antihypertensive effect CYP2D6510% (poor
metabolizers)Antiarrhythmics Proarrhythmic and other toxic
effectsToxicity in poor metabolizers110% (ultrarapid
metabolizers)Antidepressants Inefficacy in ultrarapid
metabolizersAntipsychotics Tardive dyskinesiaOpioidsInefficacy of
codeine as analgesic, narcotic side effects,
dependenceBeta-adrenoceptor antagonistsIncreasedblockadeCYP2C1936%
(whites)Omeprazole Peptic ulcer response to omeprazole823%
(Asians)Diazepam Prolonged sedationDihydropyrimidine
dehydrogenase0.1%Fluorouracil Myelotoxicity, NeurotoxicityPlasma
pseudo-cholinesterase1.5%Succinylcholine Prolonged
apneaN-acetyltransferase4070%
(whites)SulphonamidesHypersensitivity1020%
(Asians)AmonafideMylelotoxicity (rapid acetylators)Procainamide,
hydralazine, Isoniazid Drug-induced lupus
erythematous,P.NeuropathyThiopurine Methyltransferase
(GSTM1)0.3%Mercaptopurine, Thioguanine,
AzothioprineMyelotoxicityUDP-glucuronosyl-transferase
(UGT1A1)1015%Irinotecan Diarrhea, myelosuppressionACEEnalapril,
lisinapril captopril Renoprotective hypotension,left ventricular
mass Potassium channelsQuinidine Drug-induced QT
syndromeHERGCisapride Drug-induced torsade de
pointesKvLQT1Terfenadine Drug-induced long-QT
syndromeApolipoprotein ESimvastatin, TacrineADMTHFRMethotrexateGI
ToxicityVitamin K oxidoreducatase (VKORC1)Warfarin Bleeding
riskRyanodine receptor (RYR1)HalothaneMalignant hyperthermiaGenetic
Polymorphism in Drug Metabolism: Cytochrome P-450 enzymes:
CYP2D6CYP2D6 is highly polymorphic and was first investigated with
debrisoquine . More than 70 variant alleles of the CYP2D6 locus
have been reported. The metabolism of the tricyclic antidepressants
amitriptyline, clomipramine, desipramine, imipramine, nortriptyline
is influenced by the CYP2D6 polymorphism to various degrees.
Adverse effects may occur more frequently in poor metabolizers and
may be misinterpreted as symptoms of depression and may further
lead to erroneous increases in the dose. When determining CYP2D6
metabolic status (slow versus fast metabolizers) in patients on
tricyclic antidepressants, co-administration of other CYP2D6
substrates such as SSRI may result in erroneously concluding poor
CYP2D6 metabolic status.
Genetic Polymorphism in Drug Transport: PGP and Multidrug
Resistance
Transporter Pharmacogenetics is concerned with drug uptake and
efflux into or through tissues. Significant problems in the
clinical application of drugs result from poor or variable oral
drug bioavailability, and high intra- and inter-individual
variation in pharmacokinetics. The multidrug resistance-associated
proteins (MRPs) are members of the ATP-binding cassette (ABC)
superfamily with six members currently, of which MRP1, MRP2, and
MRP3 are commonly known to affect drug disposition.
Substrates for MRP1 include glutathione, glucuronide, and
sulfate.
MRP1 is expressed baso-laterally in the intestine, although its
role in extruding drugs out of the enterocytes is still uncertain.
Genetic Polymorphism in Drug Targets
In the future, proteins involved in disease will become
identified as important biomarkers for pharmacodynamics studies.
Genomics has led to the development of proteomics, which involves
the study of biologically interesting proteins and their variants.
Proteins can be used as probes for drug discovery or as biomarkers
for drug safety, such as cell surface proteins (eg, COX-2, D-2R),
intracellular proteins (eg, troponin I), and secreted proteins (eg,
MCP-l).
The physiologic response of the body to a drug is generally the
result of interaction of the drug at a specific target site in the
body. It is estimated that about 50% of drugs act on membrane
receptors, about 30% act on enzymes, and about 5% act on ion
channels. Many of the genes encoding these target proteins exhibit
polymorphisms that may alter drug response. Clinically relevant
examples of polymorphism leading to variable responses are listed
below.
Table 12.3 Clinically Important Genetic Polymorphisms of Drug
Targets and Drug TransportersGeneFrequencyDrugDrug EffectMultidrug
resistance gene (MDR1)24%Digoxin Increased concentrations of
digoxin in plasmaBeta-2 adrenergic receptor gene (2AR)37%Albuterol
Decreased response to Beta-2 adrenergic agonists Sulphonylurea
receptor gene (SUR1)23%Tolbutamide Decreased insulin responseFive
genes coding for cardiac ion channels12%Antiarrhythmics,
terfenadine, many other drugsSudden cardiac death due to long-QT
syndromePharmacogenomics and Drug developmentApplication of PGX/PGT
in various stages of drug development.Stage Application of
PGX/PGT
Drug target identificationIdentification &
characterification of gene coding for the drug targetPhage I
clinical trial ---------Inclusion /Exclusion criteriaPhage II
clinical trial ---------
Dose range selectionDose modification
Phage III clinical trial ------
Interpretation of trial result based on pharmacogenetic
tests.Phage IV clinical trial
Analysis of reported adverse events with pharmacogenetic
tests.
Regulatory issueRequirements for submission of PGT data during
development of by FDAPatient therapeuticsPersonalization of drug
therapy ,PGT data in drug labelling,Identification of responder
,nonresponders &high risk groups of adverse eventsLable of
genetic information.The FDA has approved inclusion of PGT data in
the product lable of warfarin and warfarin product now carries the
genetic information .This makes warfarin therapy safer during
initiation and maintenance of treatment.However this change of
labeling can be productive only if there are genotyping facilities
avalible,which is yet to happen in India.PGX/PGT in clinical
practice Despite considerable research activity ,PGT not yet widely
utilized in clinical practice.Screen tissue from multiple humans
linking's the polymorphic to a trait.
Preclinical studies plausibly linking with the phenotype.
Clinical phenotype /genotype association studies.
PGX/PGT in clinical practiceThere are several database that
contain information on polymorphism and mutations in human genes.
(www.pharmGKB.org). These database allow the investigator to search
by gene for reported polymorphisms.Clinician may hesitate to use a
product that requires Pharmacogenetic testing, as it would require
additional cost for the patient.Much more hesitation from the
clinicians to adjusting doses based on genetic testing than on
indirect clinical measures of renal and liver function.The
successful application of genetic screening tests to identify
patients with specific risks in drug response or drug toxicity
depends on many factors. Large amounts of relevant genetic
information must be monitored. High-throughput, high-positive and
low-negative predictive tests must be developed and implemented.
Such an endeavor will also involve considerable training,
adaptation, and acceptance of the new technology by physicians and
other health care personnel.
ConclusionWith genetic diagnostic tests becoming more common and
affordable, it is expected that individual drug dosing will become
more accurate and ultimately result in vast improvements in
therapeutic response and better drug tolerance.
References.
Meyer UA: Pharmacogenetics and adverse drug reactions.
Lancet356:11671171, 2000 Pillips KA et al: Potential role of
pharmacogenetics in reducing adverse drug reactionsA systematic
review. JAMA286:2270, 2001 Roses AD: Pharmacogenetics and future
drug development and delivery. Lancet355:13551361, 2000
References.
Clark EA, Golub TR, Lander ES, Hynes RO: Genomic analysis of
metastasis reveals an essential role for RhoC.
Nature406(6795):532535, 2000
Dahl, ML: Cytochrome P450Phenotyping/genotyping in patients
receiving antipsychotics: Useful aid to prescribing? Clin
Pharmacokinet41:453470, 2002 Evans WE, McLeod HL:
PharmacogenomicsDrug disposition, drug targets and side effects. N
Engl J Med348:538549, 2003 [PMID: 12571262].Goodman & Gilmans
The Pharmacological basis of Therapeutics,12th edition . Applied
Biopharmaceutics & Pharmacokinetics, 5th Edition
Resources
http://www.genomicglossaries.comwww.pharmGKB.org)www.hgvbase2p.orghttp://genome.ucsc.edu.http://symaltas.gnf.org/symAtlas/www.hapmap.org
THANK YOU