Embed Size (px)
Citation preview
Jan Rice and Bill McGuiness are the co-conveners of the World of Wounds (WoW) located within the Division of Nursing and Midwifery at La Trobe University. WoW is aimed at facilitating wound care knowledge through education, supported research, and the provision of clinical consultation and wound care resources.
The following case studies were collected from two Wound Management Clinics, the Alfred Vascular Dressing Clinic and the Ashwood Medical Centre Wound Care Clinic.
IntroductionThe new 3M Coban 2 Layer Compression System was evaluated in the Wound Care Clinics to gain an understanding of its effectiveness in terms of clinical and patient outcomes. This paper comprises four case studies where Coban 2 Layer Compression System was used and concludes with an overall discussion. All names used in these case studies are fictitious to maintain confidentiality.
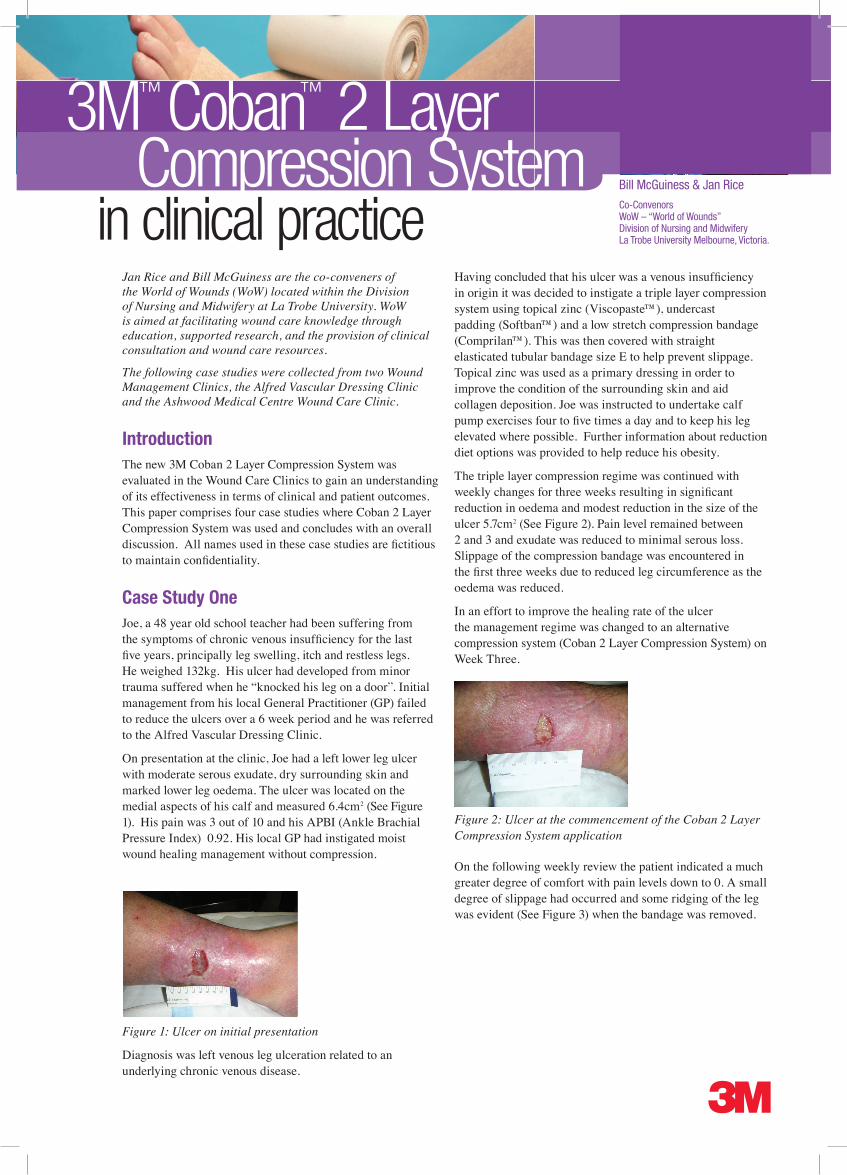
Case Study One Joe, a 48 year old school teacher had been suffering from the symptoms of chronic venous insufficiency for the last five years, principally leg swelling, itch and restless legs. He weighed 132kg. His ulcer had developed from minor trauma suffered when he “knocked his leg on a door”. Initial management from his local General Practitioner (GP) failed to reduce the ulcers over a 6 week period and he was referred to the Alfred Vascular Dressing Clinic.
On presentation at the clinic, Joe had a left lower leg ulcer with moderate serous exudate, dry surrounding skin and marked lower leg oedema. The ulcer was located on the medial aspects of his calf and measured 6.4cm2 (See Figure 1). His pain was 3 out of 10 and his APBI (Ankle Brachial Pressure Index) 0.92. His local GP had instigated moist wound healing management without compression.
Figure 1: Ulcer on initial presentation
Diagnosis was left venous leg ulceration related to an underlying chronic venous disease.
Having concluded that his ulcer was a venous insufficiency in origin it was decided to instigate a triple layer compression system using topical zinc (Viscopaste™), undercast padding (Softban™) and a low stretch compression bandage (Comprilan™). This was then covered with straight elasticated tubular bandage size E to help prevent slippage. Topical zinc was used as a primary dressing in order to improve the condition of the surrounding skin and aid collagen deposition. Joe was instructed to undertake calf pump exercises four to five times a day and to keep his leg elevated where possible. Further information about reduction diet options was provided to help reduce his obesity.
The triple layer compression regime was continued with weekly changes for three weeks resulting in significant reduction in oedema and modest reduction in the size of the ulcer 5.7cm2 (See Figure 2). Pain level remained between 2 and 3 and exudate was reduced to minimal serous loss. Slippage of the compression bandage was encountered in the first three weeks due to reduced leg circumference as the oedema was reduced.
In an effort to improve the healing rate of the ulcer the management regime was changed to an alternative compression system (Coban 2 Layer Compression System) on Week Three.
Figure 2: Ulcer at the commencement of the Coban 2 Layer Compression System application
On the following weekly review the patient indicated a much greater degree of comfort with pain levels down to 0. A small degree of slippage had occurred and some ridging of the leg was evident (See Figure 3) when the bandage was removed.
Bill McGuiness & Jan Rice
Co-ConvenorsWoW – “World of Wounds”Division of Nursing and MidwiferyLa Trobe University Melbourne, Victoria.
3M™ Coban™ 2 Layer Compression System
in clinical practice

Figure 3: Ulcer after one week of Coban 2 Layer Compression System application. Note: ridging above the ulcer.
The size of the ulcer had reduced substantially in comparison to previous reductions. In one week of Coban 2 Layer Compression System the ulcer had reduced from 5.7cm2 to 3.6cm2. In an attempt to help reduce the ridging of the patients leg additional under cast padding (Softban™) was introduced in Week Two. This reduced the ridging of the patients leg but led to increased slippage of the bandage over the week. (See Figure 4).
Figure 4: Slippage after one week of wear following application of the Coban 2 Layer Compression System with the addition of an undercast padding to help reduce ridging.
Softban™ was ceased at the next application and care was taken to ensure even bandage distribution of Coban 2 Layer Compression System.
Coban 2 Layer Compression System was continued for a further three weeks resulting in complete healing of the ulcer. (See Figure 5).
Figure 5: Ulcer healed following four weekly applications of Coban 2 Layer Compression System
SummaryCoban 2 Layer Compression System resulted in a healed venous leg ulcer within a four week period and a substantial increase in patient comfort. Careful application ensuring even distribution of the two layers is needed to ensure the higher ambulatory pressures achieved with this system does not result in ridging and potential pressure injury.
Case Study TwoJulie, aged 62 years had been suffering from the symptoms of chronic venous insufficiency for the last fifteen years, principally leg swelling, itch and restless legs. She weighed 96kg. Her ulcer had developed from minor trauma suffered when she “knocked her leg in the garden”. Initial management from her local GP failed to reduce the ulcers over a 5 month period and she was referred to the Wound Clinic.
On presentation, Julie had a left lower lateral leg ulcer with heavy serous exudate, dry surrounding skin and marked bilateral lower leg oedema. The ulcer was located on the lateral aspects of her calf and measured 1.7cm2 (See Figure 1). Her pain was 6 out of 10 and her ABPI 0.87. Surrounding skin was indicative of stasis dermatitis. Her local GP had been using dry dressings as management without compression.
Figure 1: Initial presentation
Diagnosis was left lateral venous leg ulceration related to an underlying chronic venous disease.
Having concluded that her ulcer was a venous insufficiency in origin it was decided to instigate a triple layer compression system using topical zinc (Viscopaste™), under cast padding (Softban™) and a low stretch compression bandage (Comprilan™). This was then covered with straight elasticated tubular bandage size E to help prevent slippage. Topical zinc was used as a primary dressing in order to improve the condition of the surrounding skin as well as aid collagen deposition. Topical steroid was used for the first week to help reduce the dermatitis. Julie was instructed to undertake calf pump exercises four to five times a day and to keep her leg elevated when possible.
The triple layer compression regime was continued with weekly changes for eleven weeks resulting in a reduction in oedema and an increase in the size of the ulcer to 3.1cm2 (See Figure 2). Despite non-narcotic analgesic and anti-inflammatory medication, her pain level remained 3 to 5. The wound exudate remained at moderate levels of serous fluid. A punch biopsy was taken in week seven to exclude pyoderma gangrenosum and skin tumours. Return findings were compatible with venous disease only.
Figure 2: Prior to the commencement of Coban 2 Layer Compression System
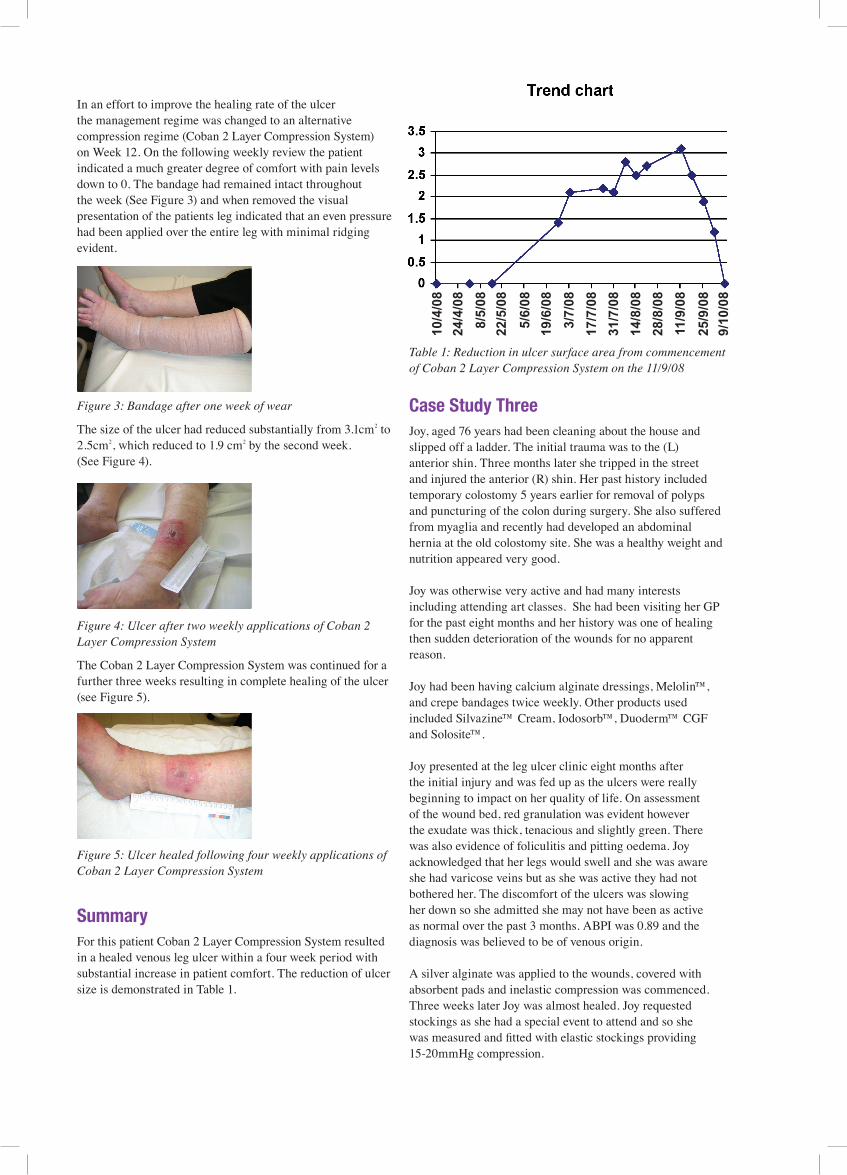
In an effort to improve the healing rate of the ulcer the management regime was changed to an alternative compression regime (Coban 2 Layer Compression System) on Week 12. On the following weekly review the patient indicated a much greater degree of comfort with pain levels down to 0. The bandage had remained intact throughout the week (See Figure 3) and when removed the visual presentation of the patients leg indicated that an even pressure had been applied over the entire leg with minimal ridging evident.
Figure 3: Bandage after one week of wear
The size of the ulcer had reduced substantially from 3.1cm2 to 2.5cm2, which reduced to 1.9 cm2 by the second week. (See Figure 4).
Figure 4: Ulcer after two weekly applications of Coban 2 Layer Compression System
The Coban 2 Layer Compression System was continued for a further three weeks resulting in complete healing of the ulcer (see Figure 5).
Figure 5: Ulcer healed following four weekly applications of Coban 2 Layer Compression System
SummaryFor this patient Coban 2 Layer Compression System resulted in a healed venous leg ulcer within a four week period with substantial increase in patient comfort. The reduction of ulcer size is demonstrated in Table 1.
Table 1: Reduction in ulcer surface area from commencement of Coban 2 Layer Compression System on the 11/9/08
Case Study ThreeJoy, aged 76 years had been cleaning about the house and slipped off a ladder. The initial trauma was to the (L) anterior shin. Three months later she tripped in the street and injured the anterior (R) shin. Her past history included temporary colostomy 5 years earlier for removal of polyps and puncturing of the colon during surgery. She also suffered from myaglia and recently had developed an abdominal hernia at the old colostomy site. She was a healthy weight and nutrition appeared very good.
Joy was otherwise very active and had many interests including attending art classes. She had been visiting her GP for the past eight months and her history was one of healing then sudden deterioration of the wounds for no apparent reason.
Joy had been having calcium alginate dressings, Melolin™, and crepe bandages twice weekly. Other products used included Silvazine™ Cream, Iodosorb™, Duoderm™ CGF and Solosite™.
Joy presented at the leg ulcer clinic eight months after the initial injury and was fed up as the ulcers were really beginning to impact on her quality of life. On assessment of the wound bed, red granulation was evident however the exudate was thick, tenacious and slightly green. There was also evidence of foliculitis and pitting oedema. Joy acknowledged that her legs would swell and she was aware she had varicose veins but as she was active they had not bothered her. The discomfort of the ulcers was slowing her down so she admitted she may not have been as active as normal over the past 3 months. ABPI was 0.89 and the diagnosis was believed to be of venous origin.
A silver alginate was applied to the wounds, covered with absorbent pads and inelastic compression was commenced. Three weeks later Joy was almost healed. Joy requested stockings as she had a special event to attend and so she was measured and fitted with elastic stockings providing 15-20mmHg compression.
10/4
/08
24/4
/08
8/5/
08
22/5
/08
5/6/
08
19/6
/08
3/7/
08
17/7
/08
31/7
/08
14/8
/08
28/8
/08
11/9
/08
25/9
/08
9/10
/08
3M and Coban are trademarks of 3M company.Please recycle. Printed in Australia.© 3M 2008. All rights reserved.PB 3805/0109
3M Medical
3M Australia Pty Ltd950 Pacific HighwayPymble NSW, 2073Phone: 1300 363 878 Web: www.3m.com.au/healthcare
However, the next visit the wounds had deteriorated from slippage caused by the hoisery. Coban 2 Layer Compression System was commenced.
Unfortunately, the wounds did not recover well however the bandage performed exceptionally well. After three weeks despite excellent bandage performance there was still no improvement and so the patient was referred back to her GP with a request to consider that the underlying diagnosis may be vasculitis or at least an inflammatory ulcer. Three weeks later the wounds were healed.
SummaryThe purpose of this case study was not to demonstrate the healing outcome using Coban 2 Layer Compression System but rather to show that it remained in place and addressed the slippage that was caused by the hosiery. The patient satisfaction with Coban 2 Layer Compression System was overwhelming and she stated that there was no discomfort at night as she had previously experienced with other bandages. Joy said she had spent the entire weekend gardening after the first Coban 2 Layer Compression System was applied because she was so comfortable.
Case Study FourAngelina, aged 82 years presented at the leg ulcer clinic with bilateral pitting oedema to the top of her thighs. There were no wounds but severe discomfort as she had little strength to lift her legs to walk. It appeared that the osteoporosis caused her severe back pain and this limited her normal active lifestyle where she would walk up to 5kms per day. Angelina was a thin woman but not severely underweight, as she had always been of slight build.
Relevant history included severe osteoporosis, otherwise there was no significant past medical history. The current diagnosis was bilateral lower leg oedema of unknown origin. ABPI was 0.9.
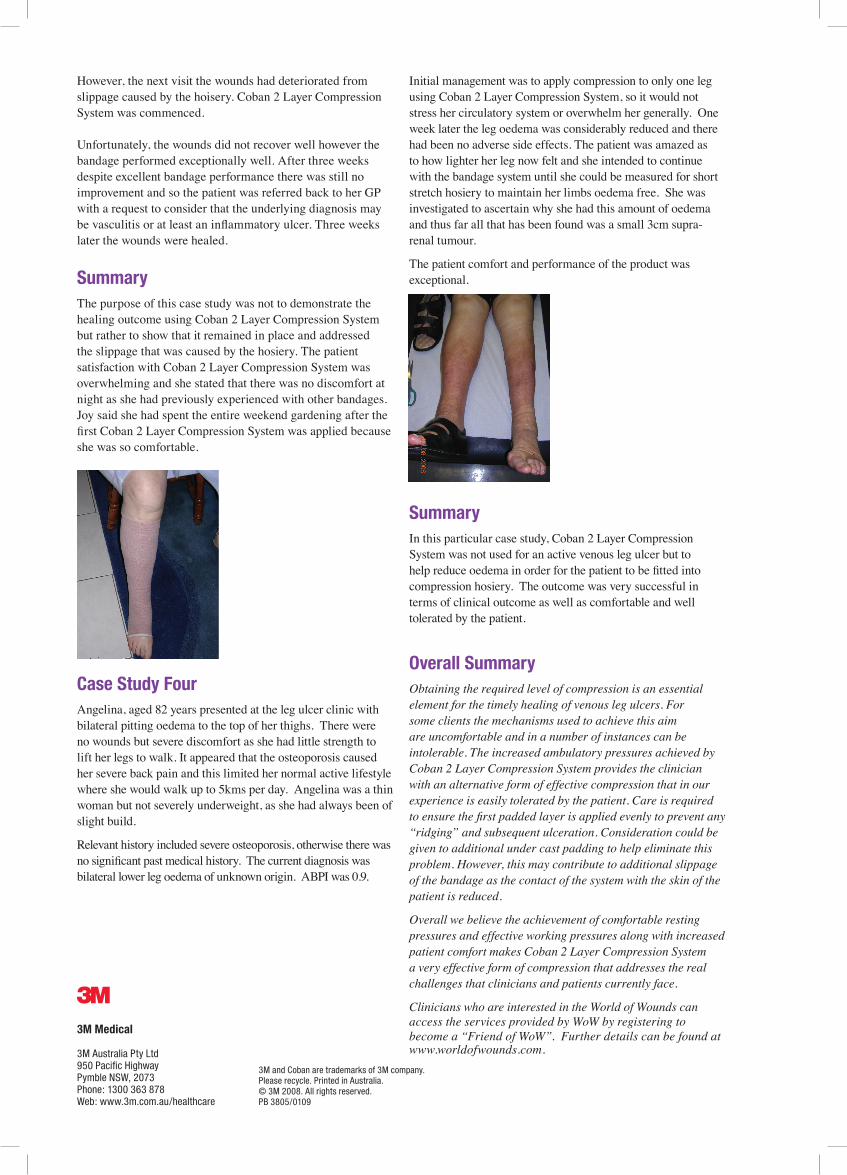
Initial management was to apply compression to only one leg using Coban 2 Layer Compression System, so it would not stress her circulatory system or overwhelm her generally. One week later the leg oedema was considerably reduced and there had been no adverse side effects. The patient was amazed as to how lighter her leg now felt and she intended to continue with the bandage system until she could be measured for short stretch hosiery to maintain her limbs oedema free. She was investigated to ascertain why she had this amount of oedema and thus far all that has been found was a small 3cm supra-renal tumour.
The patient comfort and performance of the product was exceptional.
SummaryIn this particular case study, Coban 2 Layer Compression System was not used for an active venous leg ulcer but to help reduce oedema in order for the patient to be fitted into compression hosiery. The outcome was very successful in terms of clinical outcome as well as comfortable and well tolerated by the patient.
Overall SummaryObtaining the required level of compression is an essential element for the timely healing of venous leg ulcers. For some clients the mechanisms used to achieve this aim are uncomfortable and in a number of instances can be intolerable. The increased ambulatory pressures achieved by Coban 2 Layer Compression System provides the clinician with an alternative form of effective compression that in our experience is easily tolerated by the patient. Care is required to ensure the first padded layer is applied evenly to prevent any “ridging” and subsequent ulceration. Consideration could be given to additional under cast padding to help eliminate this problem. However, this may contribute to additional slippage of the bandage as the contact of the system with the skin of the patient is reduced.
Overall we believe the achievement of comfortable resting pressures and effective working pressures along with increased patient comfort makes Coban 2 Layer Compression System a very effective form of compression that addresses the real challenges that clinicians and patients currently face.
Clinicians who are interested in the World of Wounds can access the services provided by WoW by registering to become a “Friend of WoW”. Further details can be found at www.worldofwounds.com.