Embed Size (px)
Citation preview
3D Ultrasound in
Gynecology
Dr. Juan Luis Alcázar
Department of Obstetrics and Gynecology
Clínica Universidad de Navarra. School of Medicine
University of Navarra, Pamplona, Spain

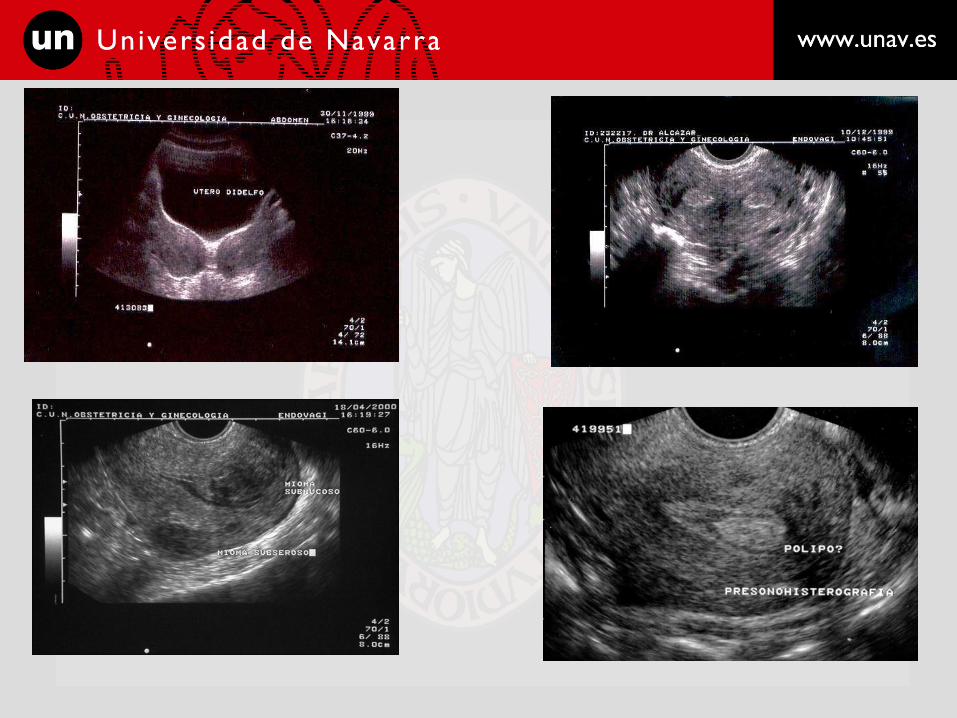
Ultrasound and the uterus
• Transvaginal ultrasound is a useful tool for
diagnosing uterine pathology such as uterine
myomas, adenomyosis and müllerian anomalies.
• It is quite difficult to differentiate myomas from
sarcomas using ultrasound
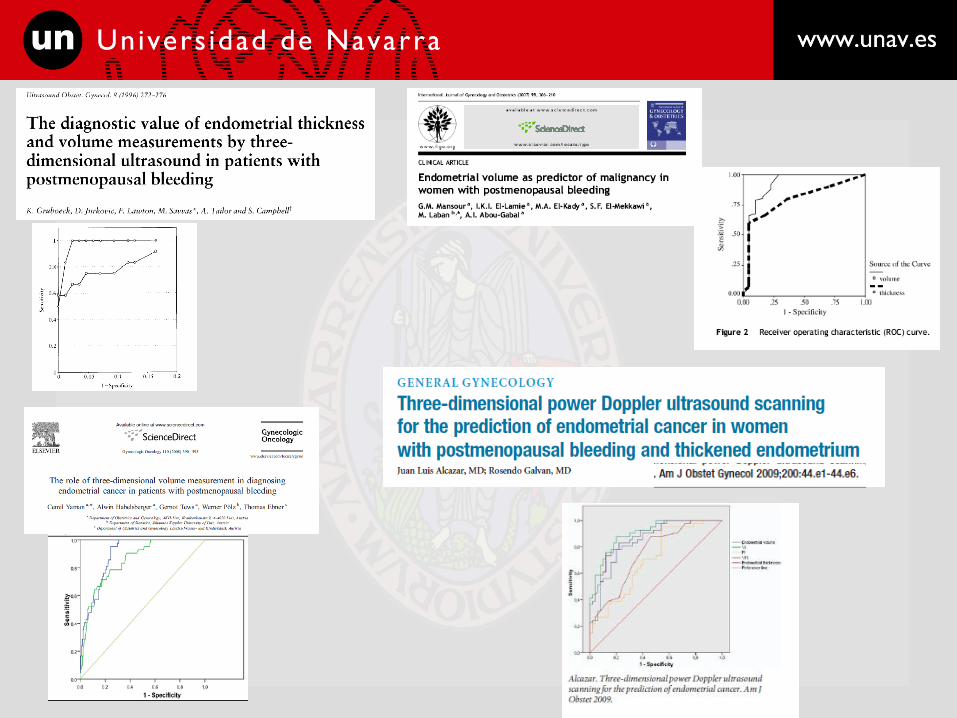
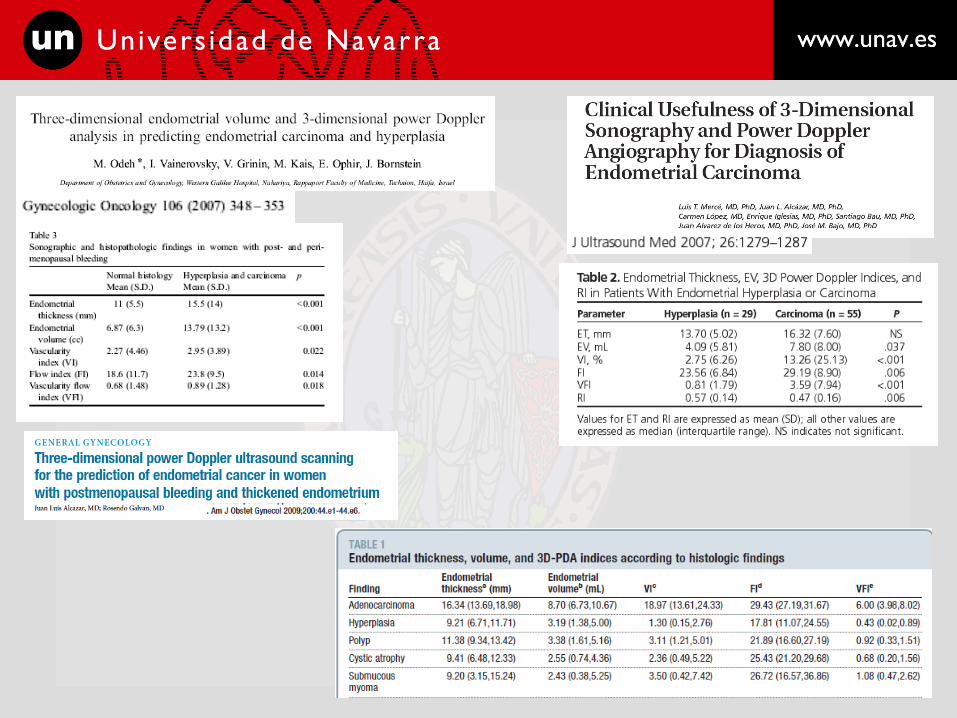
• Basic transvaginal ultrasound is a useful tool for
identifying endometrial pathology, but specificity
is moderate.

Ultrasound and the uterus
• A “normal” ultrasound in symptomatic women has
a high negative predictive value.
• Pulsed Doppler has no role.
• Power Doppler mapping may be useful, increasing
specificity but it is only reproducible when
performed by expert examiners
• Sonohysterography is especially useful when
intracavitary lesions are suspected

Ultrasound in adnexal masses
• B-Mode gray-scale ultrasound: – Subjective diagnosis
• Mean sensitivity: 91%
• Mean specificity: 75%
– Scoring systems
• Mean sensitivity: 89%
• Mean specificity: 78%
• Pulsed - color Doppler
– Great variability (> 140 studies in 20 years)
– Overlapping in velocimetric indexes
– Flow location: consistent parameter
– Meta-analysis (Kinkel,Radiology 2000)
• Mean specificity: 90%
– Decrease FP rate
– Problem: How to integrate it? Reproducibility?

What may 3D ultrasound add?

• 3D ultrasound offers unique ways to
evaluate uterine and endometrial pathology:
– Virtual Navigation
– TUI (Tomographic Ultrasound Imaging)
– VOCAL™ (Virtual Organ Computer Aided
anaLysis)
– SRI (Speckle Reduction Imaging)
– VCI (Volume Contrast Imaging)
– Off-line assessment












Kappa: 0.97
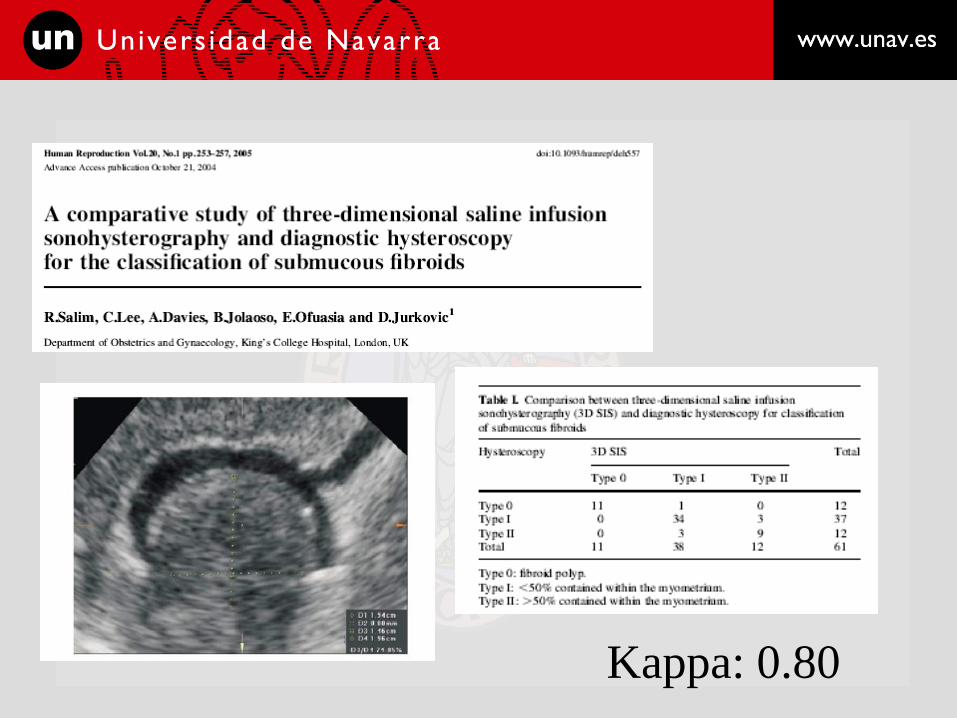
Kappa: 0.80




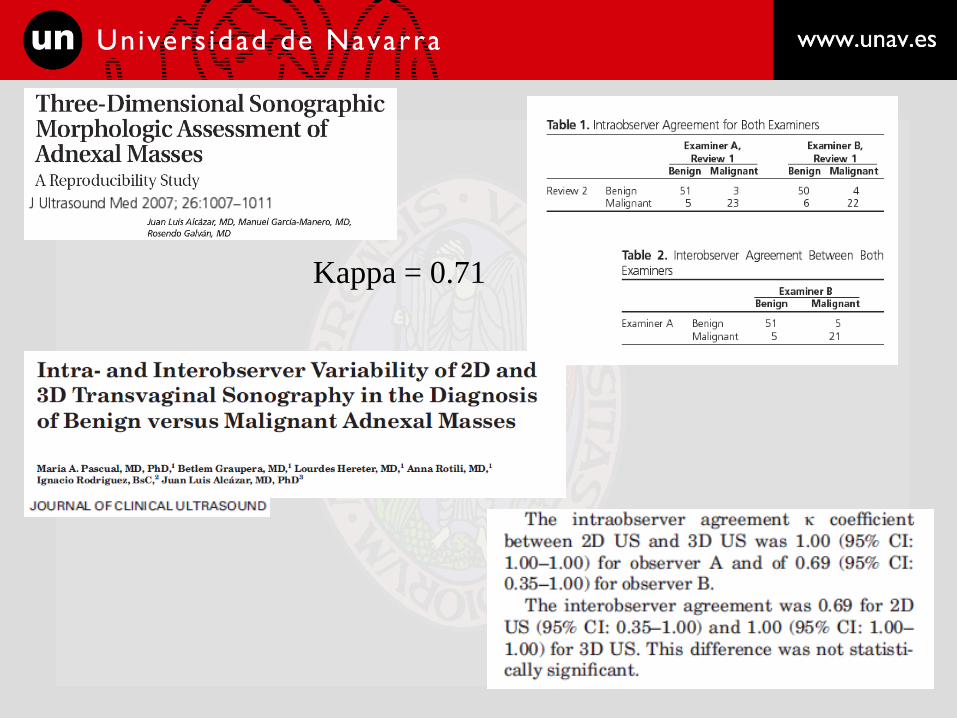
Kappa = 0.71
3D vascularity
What are we measuring?

Ultrasound assessment of tissue
vascularization • Conventional ultrasound
– Color / Power Doppler vessel mapping
– Pulsed Doppler indexes (RI / PI)
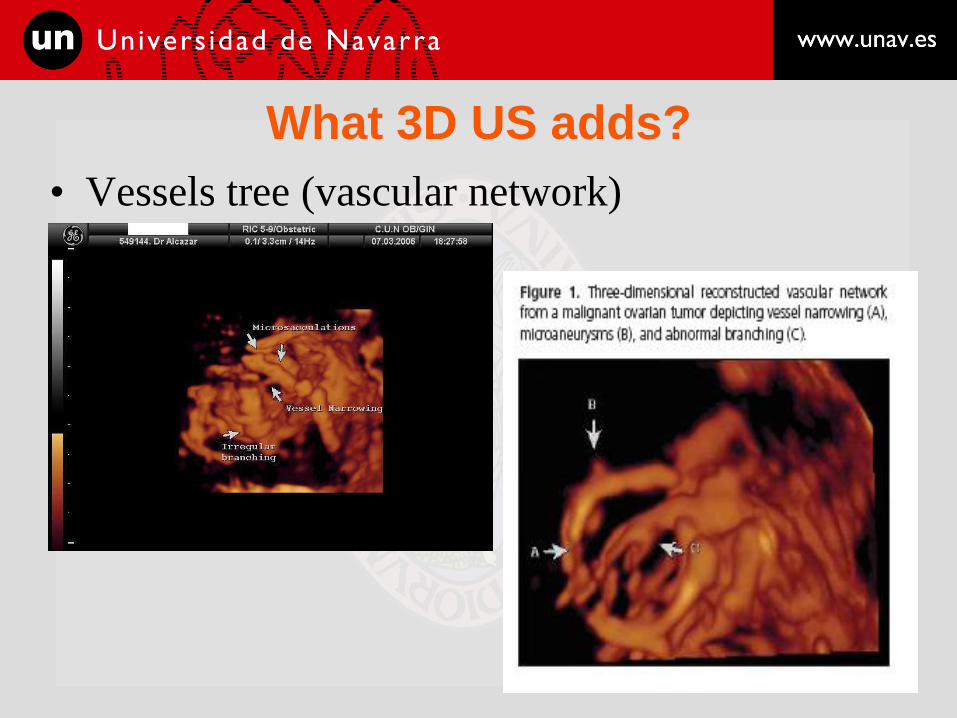
What 3D US adds?
• Vessels tree (vascular network)

Vascular Network.
Rationale

Vascular network. Problems
• Reproducibility: Just moderate.
– Sladkevicius UOG 2007
– Alcazar JUM 2008
K= 0.49

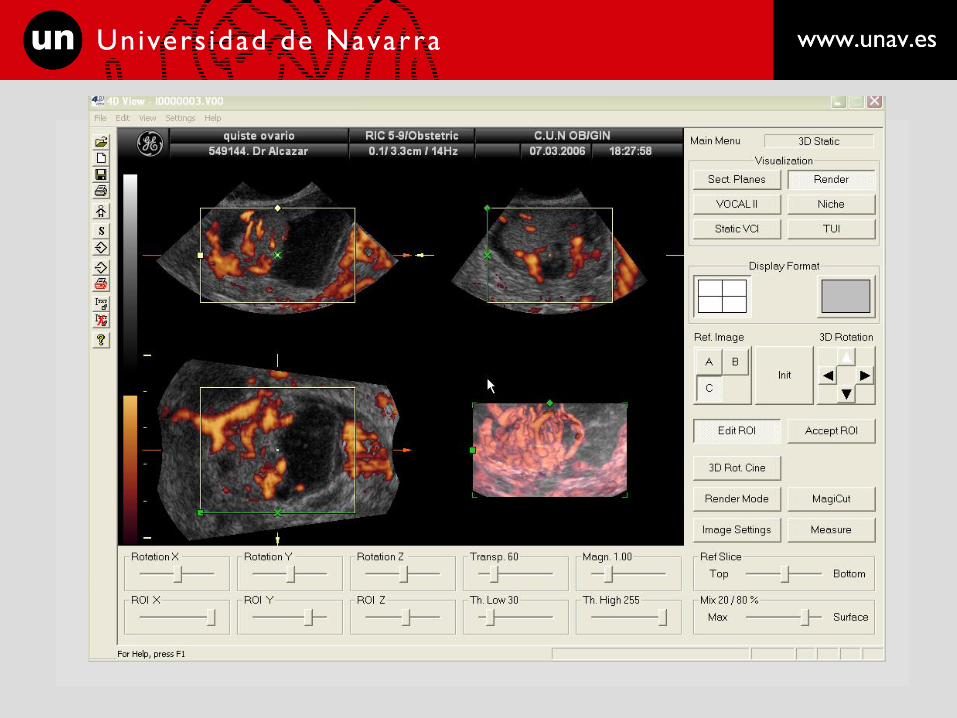
What 3D US adds?
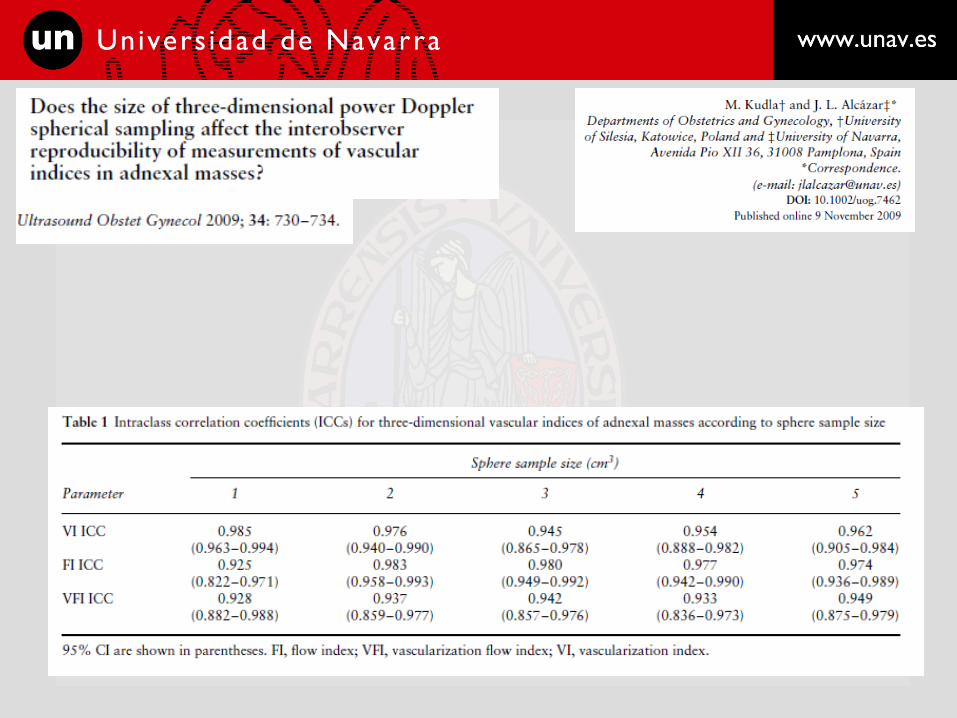
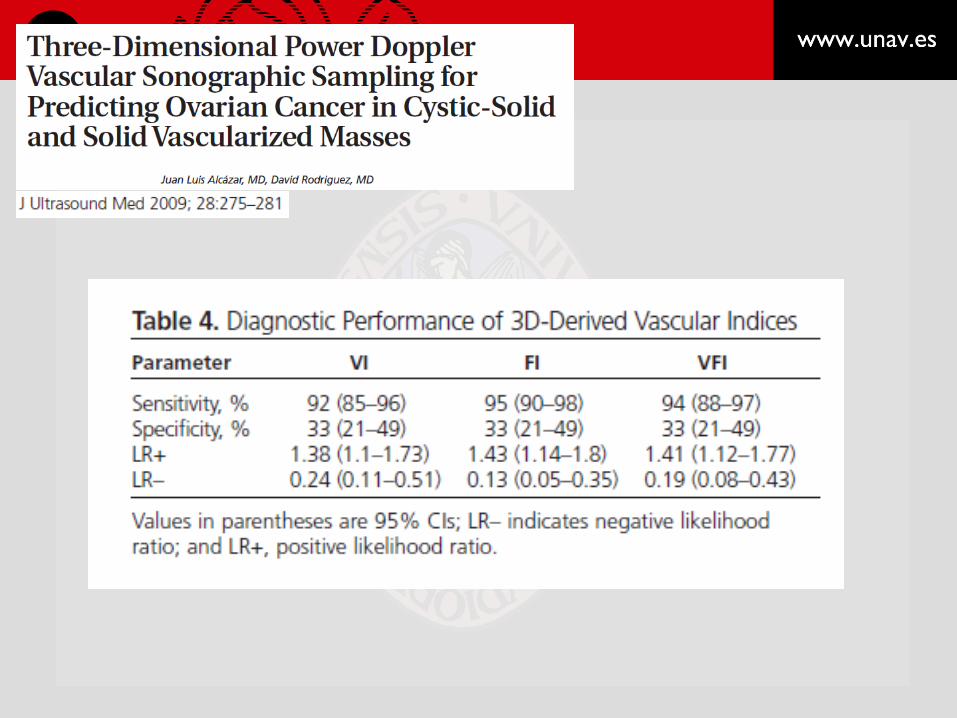
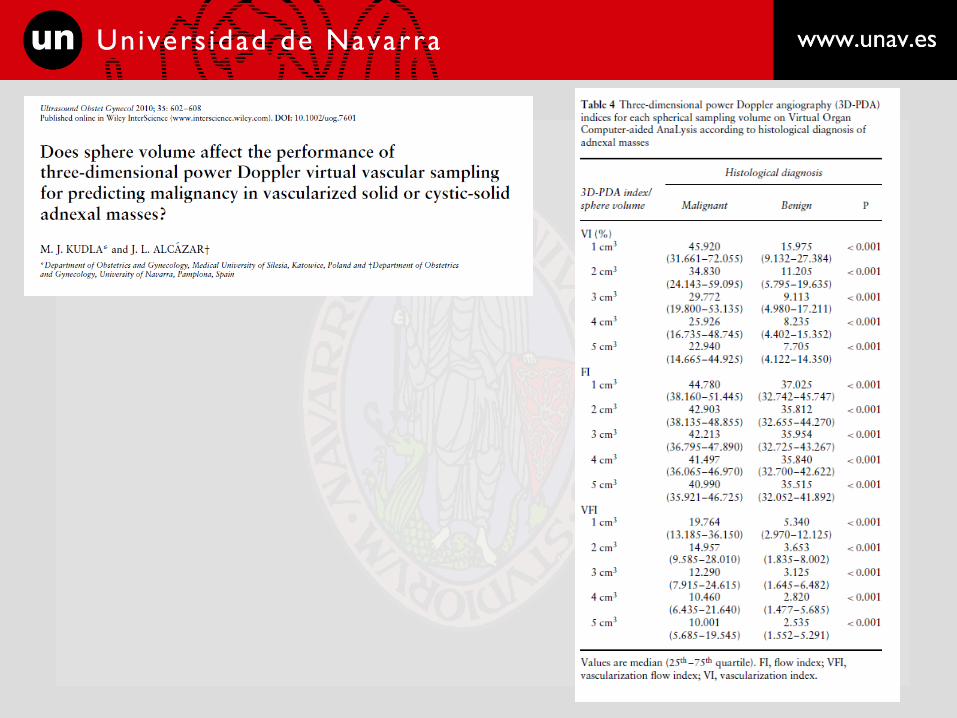
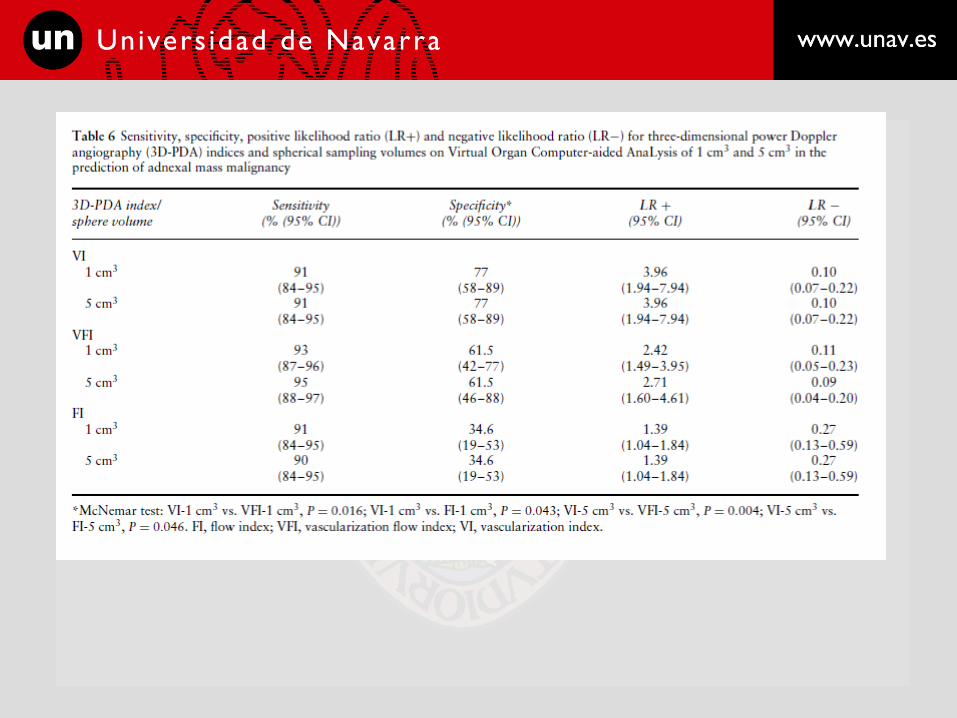
• 3D power Doppler indexes. Virtual vascular “sampling”
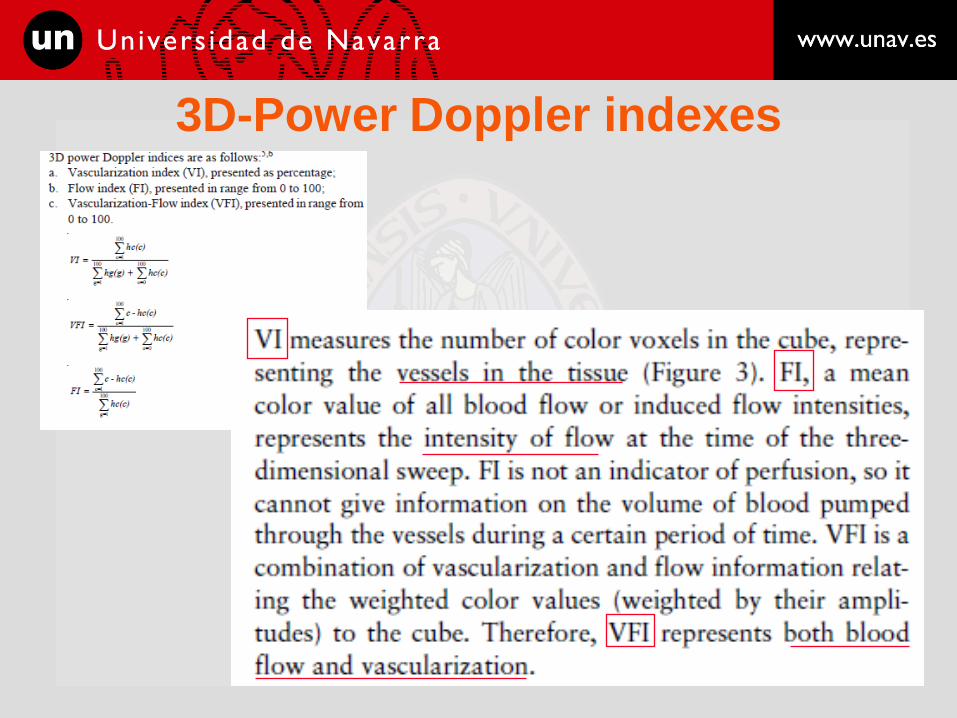
3D-Power Doppler indexes
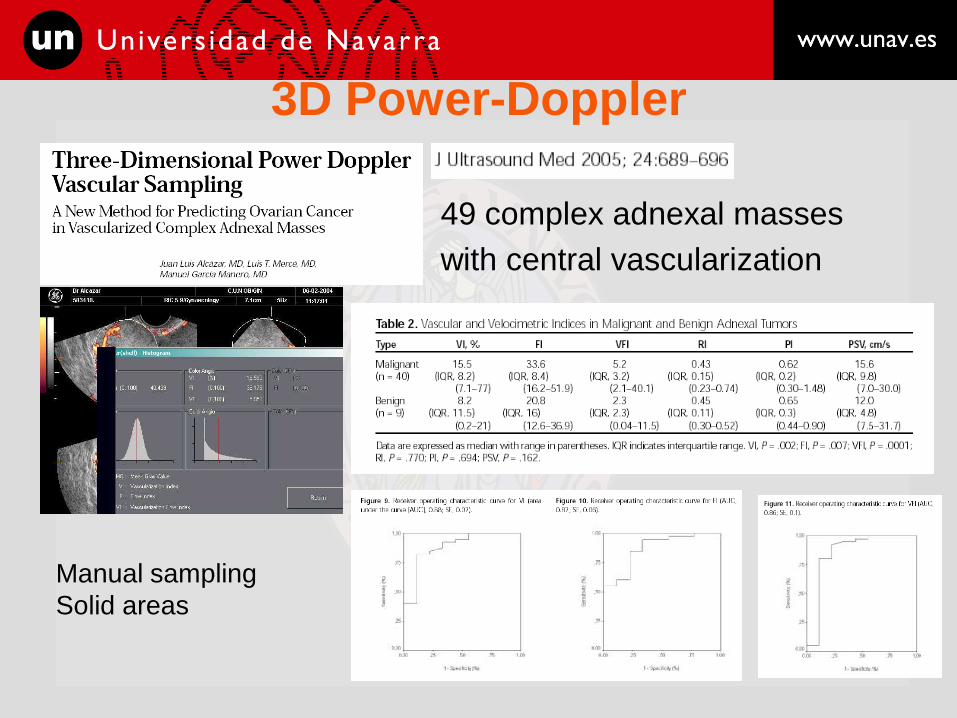
3D Power-Doppler
49 complex adnexal masses
with central vascularization
Manual sampling
Solid areas




5-cc spherical sampling could not
be performed in 19% of the cases



• Is it this true?
– Is VI related to number of vessels within ROI?
– Does FI reflect blood flow within ROI?
– Does VFI reflect tissue perfusion?
• Power Doppler = shift in signal amplitude (energy)
Which factors affect PD signal?
– Machine settings
• PRF. Gain. WF. Power (dB).
– Physiological-Rheological-Hemodynamic factors
• Volume flow. Hematocrit. Depth. Type of flow (Laminar,
Turbulent). Cardiac cycle. Heart rate.

Machine settings




Physiological-Rheological-Hemodynamic factors

Physiological-Rheological-Hemodynamic factors

3D-PD indexes and Number of
vessels

3D-PD indexes and Number of
vessels

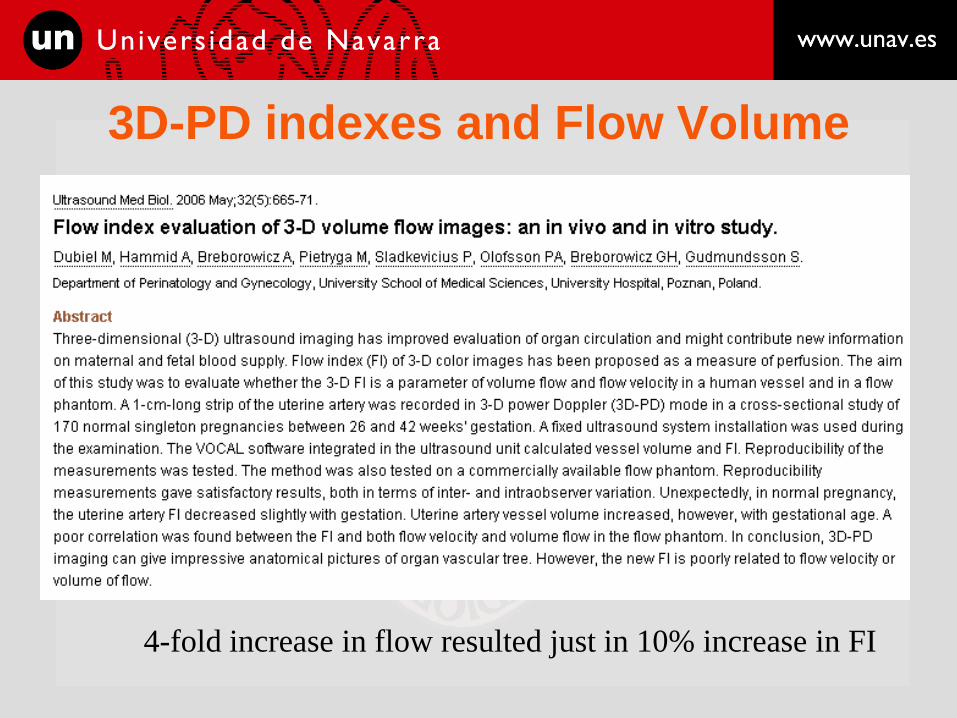
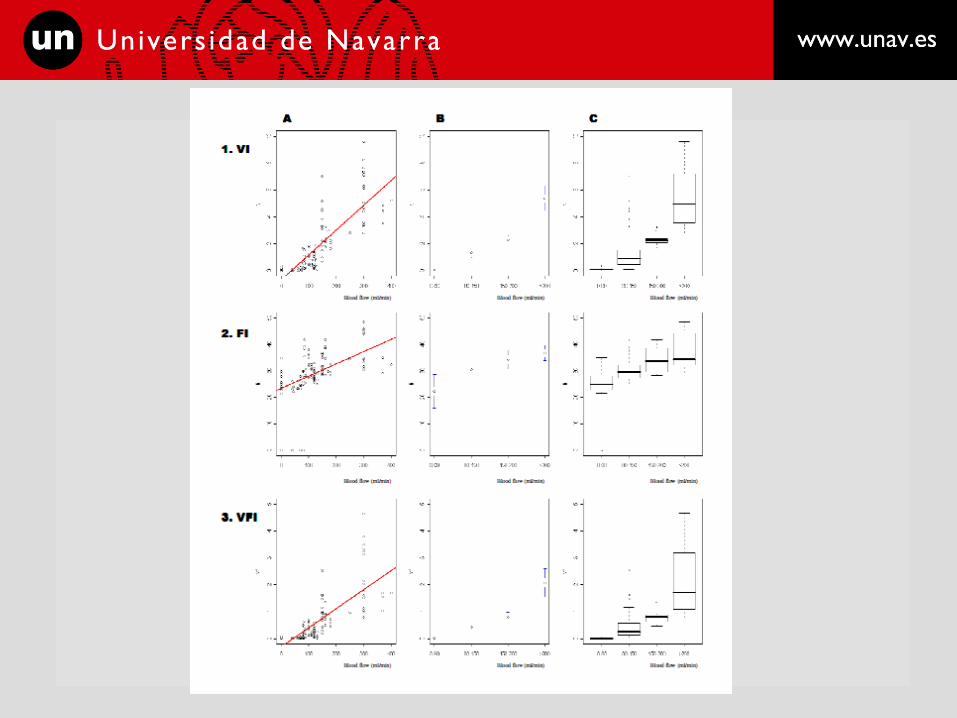
3D-PD indexes and Flow Volume
4-fold increase in flow resulted just in 10% increase in FI

3D-PD indexes and Flow Volume


Summary of findings
• Machine settings, especially power, gain and PRF affect
significantly all 3D PD indexes.
• Depth affects significantly all 3D PD indexes.
• Hematocrit affects significantly all 3D PD indexes.
• VI seems to be related not only to vessel number but also to
volume flow within ROI
• FI does not seem to be related linearly to volume flow.

Explanations
• Factors not considered
– Type of flow.
– Blood pressure.
– Cardiac cycle.
• Hemodynamic phenomena

Explanations
• FACT: VI increases linearly as flow increases
• EXPLANATION
– Assuming parabolic laminar flow: Q = v·a
• Increase flow velocity
• Change vessel caliber
– Increase blood pressure Small vessels opened
Lower volume flow Higher volume flow
Higher nº of voxels detected
Explanations
• Cardiac cycle
– Do indices change in systole as compared with
diastole?


Explanations
• FACT: FI is poorly and not linearly related to flow
• EXPLANATION
– FI is just expressing mean quantification of change in
signal amplitude (color intensity)
– Is it FI absolutely independent from VI?
• “Dilutional effect” of voxels.
– Increasing VI may “dilute” FI value: More voxels detected but with
lower intensity, so disminish mean color intensity (FI)
– Hematocrit affects more intensely to FI than VI
• Effect on inflow hydrostatic pressure (IHP)

• Technical standardization is needed for both
gynecologic and obstetrics examinations.



Conclusions
• VI is related to number of vessels but also
to volume flow
• FI is poorly related to flow
• Standardization is essential for reproducible
results among different observers.

www.cun.es [email protected]






























