Embed Size (px)
Citation preview

c
C
G
mecteded
pr(
K
ep
tcfo
(d(p(wosl
www.AJOG.org Clinical Obstetrics, Diabetes, Labor, Medical-Surgical-Disease, Physiology/Endocrinology, Prematurity Poster Session II
Mean durations of labor were similar for multiparous and grand-multiparous parturients (table).CONCLUSION: Labor curves for Israeli parturients were more graduallysloped than Friedman’s curve. Our findings may encourage the phy-sician in the delivery room to take into account demographic criteriasuch as maternal origin when assessing labor progression.
339 Neuraxial analgesia may reduce the risk foresarean delivery during induced labor
Yael Hants1, Doron Kabiri1, Roi Gat1, Efrat Luttwak1,arolyn Weiniger2, Yossef Ezra1
1Hadassah-Hebrew University Medical Center, Department of Obstetrics andynecology, Jerusalem, Israel, 2Hadassah-Hebrew University Medical
Center, Department of Anesthesiology, Jerusalem, IsraelOBJECTIVE: The process of labor involves significant pain and stress for
ost women. Neuraxial analgesia (epidural/spinal) offers the mostffective form of pain relief. The impact of neuraxial analgesia onesarean delivery rates has been widely studied and an associate rela-ionship is recognized, not causative. Some evidence suggests thatpidural analgesia may speed up labor, however the advantage of epi-ural use on labor outcome is unclear. The current study evaluates theffect of neuraxial analgesia during induction of labor on the cesareanelivery rate.
STUDY DESIGN: A retrospective case control study including all womenwho underwent term labor induction in a tertiary university medicalhospital between July 2010 and June 2011. Women with and withoutneuraxial analgesia composed the study and the control group respec-tively. Statistical analysis was performed using Chi-square test, uni-variate models and multiple logistic regression.RESULTS: Seven hundred sixty-nine term inductions of labor were
erformed during the study period. Five hundred forty-three womeneceived neuraxial analgesia (study group), while 226 women did not
Duration of first and second stages of labor forIsraeli parturients, stratified by parity�
�Adjusted for: birthweight, epidural and oxytocin augmentation.
control group). The overall cesarean delivery rate was 17.0%. Sixty-
Supplem
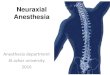
four women (11.8%) from the study group underwent cesarean de-livery compared to 67 women (29.6%) in the control group (Figure).After adjusting for potential confounders, women with neuraxialblock had significantly decreased odds of cesarean delivery. The ad-justed Odds Ratio for cesarean delivery among women with neuraxialanalgesia was 0.322 (95% confidence interval 0.219-0.474; 99% con-fidence interval 0.194-0.534) compared to women without neuraxialanalgesia (Table). The adjusted Odds Ratio for cesarean delivery was0.196 and 0.517 for primiparous and multiparous, respectively.CONCLUSION: Neuraxial analgesia during term labor induction has asignificant positive effect on delivery outcomes, reducing cesareandelivery rate. Future studies are warranted in order to considerwhether the connection is causative or associative.
340 Maternal BMI and pelvic arterial embolizationSarah Poggi1, Yesmean Wahdan1, Alessandro Ghidini1,
enneth Raholl2, Arletta VanBreda2, Keith Sterling2
1Inova Alexandria Hospital, Perinatal Diagnostic Center, Alexandria, VA,2Inova Alexandria Hospital, Interventional Radiology, Alexandria, VAOBJECTIVE: To determine whether maternal BMI affects the safety andfficacy of pelvic arterial embolization (PAE) for the treatment ofostpartum hemorrhage (PPH).
STUDY DESIGN: Retrospective single-center cohort study of 124 pa-ients undergoing PAE for primary PPH between 1999 to 2010. Ex-luded were cases missing maternal BMI at delivery or outcome in-ormation. Maternal BMI, demographic and obstetric characteristicsf the population and outcomes were recorded.
RESULTS: Average BMI at delivery in the population was 31.4�/�6.9range 22-58.2), with 49% being obese (BMI above 30). Maternal BMIid not correlate with cause of PPH (p�0.90), need for emergent PAEP�0.92), time from CVIR access to discharge from CVIR (P�0.80),resence of hemodynamic instability (P�0.85), need for transfusionP�0.35) or ICU admission (P�0.05). The results did not changehen the analysis was limited to PPH due to uterine atony only. Thenly immediate complications were hematoma at the vascular accessite (1 case) and post-embolization syndrome (1 case). There were noong term complications of PAE.
CONCLUSION: The success and safety of PAE is unrelated to maternal
Logistic regression model for influencingfactors on the cesarean delivery rate
BMI.
ent to JANUARY 2013 American Journal of Obstetrics & Gynecology S151