Embed Size (px)
Citation preview

While patients with lung cancer are living longer
than before, more progress is essential because
many patients still succumb to the disease. Inves-
tigators in the Thoracic Oncology Program at
the NYU Cancer Institute — led by Harvey Pass,
MD, Professor of Surgery and Cardiothoracic
Surgery and Director, Division of Thoracic Sur-
gery and Thoracic Oncology, and Abraham
Chachoua, MD, Jay and Isabel Fine Associate
Professor of Oncology — are delineating the
pathways of lung carcinogenesis, pioneering the
exploration of biomarkers to detect the disease
in its earliest stages, and leading clinical trials of
new treatments for patients with all stages of
lung cancer.
Their efforts were greatly enhanced with the
recent $1.1 million gift from NYU Langone
Medical Center Trustee E. John Rosenwald, Jr.
and his wife, Patricia Rosenwald, to support lung
cancer research at the NYUCI. Mrs. Rosenwald
received treatment for lung cancer at NYU Lan-
You may have heard about the human genome,
the library of some 25,000 genes that dictate the
development of our bodies and the processes
within. But that’s not the end of the story — in
fact, it’s just the beginning, the tip of the iceberg.
Many chemical carcinogens directly damage
DNA, leading to cancer. There is growing evi-
dence, however, that some environmental expo-
sures cause cancer by turning genes on and off.
At the same time, researchers are learning how
to replicate this power by turning off bad genes
and turning on good ones using promising anti-
cancer drugs.
The field is called epigenetics (also called
epigenomics), and it’s one that the National
Institutes of Health (NIH) has made a priority
in its research portfolio, announcing in January
2008 its decision to allocate some $190 million
over five years to support investigations related
The NYUCI Thoracic Oncology Program: The Machine Driving the Discovery
continued on page 7
continued on page 4
NYU Cancer Institute
Harvey Pass, MD, and Margaret Huflejt, PhD, are evalu-ating a novel means of identifying biomarkers that couldserve as early indicators of lung cancer development.
Max Costa, PhD, is studying epi-genetic changes in people atincreased risk of cancer due toenvironmental exposures such asnickel and arsenic.
Genes Under SiegeNYUCI Scientists Study Epigenetics to Understand Cancer Development and Improve Treatment
IN THIS ISSUE
2 Director's Message
3 Goldstein Gift
6 Young Adults with Cancer FaceUnique Issues
8 Rajni Kannan’s Personal Crusade
9 Spring Health Quiz
10 Hormone ChangesDuring CancerTreatment
11 Events Calendar
newsSpring/Summer 2010
gone Medical Center; her cancer was found
early, thanks to periodic CT scans. “Lung cancer
has touched our lives and was successfully treat-
ed at NYU. When we were making a gift, it was
natural to aim our philanthropy at the program
that was most significant in our lives,” says
3184W1 4/28/10 5:25 AM Page 1

Although breast and prostate cancers remain the two most common cancers in the United
States, lung cancer is the leading cause of death from cancer for both men and women. While
the majority of lung cancers are caused by smoking, others are associated with occupational
exposures. And still others arise with no identifiable cause.
The NYU Cancer Institute has built a robust program to study the origins of lung can-
cer, pinpoint markers that may signal increased risk or its earliest stages of development, and
evaluate new drugs and treatment regimens for
patients diagnosed with the disease. I’d like to thank
NYU Langone Medical Center Trustee E. John
Rosenwald, Jr. and his wife, Patricia Rosenwald, who
generously contributed $1.1 million to support our
lung cancer research program, which you can read
about in this issue.
You may have been hearing the word “epigenet-
ics” more in the popular press these days. In fact, it
made the cover of TIME magazine last January.
While it’s true that some people have an increased
risk of cancer because of a genetic mutation they
inherited from one of their parents, many cancers
may be caused by DNA alterations — “epigenetic
changes”— that change the expression of genes but
do not alter the sequence itself. Epigenetic changes
may occur during our lifetimes, sometimes as a result of environmental exposures.
NYUCI investigators are collaborating to study such epigenetic changes and how they
may lead to cancer. Moreover, investigators are looking at how these changes occur and using
this knowledge to devise and assess drugs that work by inducing epigenetic changes that are
not favorable for cancer cell growth. Several of their efforts are described in this issue.
Our community education program continues to bring the latest news from cancer
research and advocacy to all of you. One such recent presentation focused on hormonal
changes that may occur during or as a result of cancer treatment. Another event armed
young adult cancer survivors with practical information to empower them as they move on
with their lives.
Finally, I’d like to note the story on page 8 about one of our nurse practitioners, Rajni
Kannan, who cares for patients with melanoma. She sees all too often the damage that
tanning beds can inflict on young patients, and is speaking out for stronger tanning bed
regulations.
Staff members like Ms. Kannan exemplify who we are at the NYU Cancer Institute: a
team of dedicated and compassionate individuals who work tirelessly not only to give our
own patients the very best care, but also to bring cancer awareness to others in our commu-
nity to reduce the burden of this disease. I’d like to take this moment to thank NYUCI staff
for all you do to care for our patients and to further the knowledge of cancer in our great
city and around the world.
Message from the Director
Disclaimer: The medical information provided is foreducational purposes only. It is not intended or impliedto be a substitute for professional medical advice.Always consult your physician or healthcare providerprior to starting any new treatment or with anyquestions you may have regarding a medical condition.
NYU Cancer Institute news
NYU Cancer Institute Board of Directors
Lori W. FinkChair
Ellen BannerSusan Block CasdinRoberta GreenbergJames M. KennyKenneth G. LangoneThomas H. LeeSandra MeyerEdward J. MinskoffShlomo PerlLaurie PerlmutterAmanda PullingerStanley B. ShopkornJoseph SteinbergBrian Walter
NYU Cancer Institute
William L. Carroll, MDDirector
Lauren E. HackettExecutive Director for Administration
Owen A. O’Connor, MD, PhDDeputy Director, Clinical Research and Cancer Treatment
Michele Pagano, MDDeputy Director, Basic Sciences
Associate DirectorsJohn Curtin, MDAcademic Affairs and Education
Silvia Formenti, MDClinical Research
Richard B. Hayes, DDS, PhDPopulation Sciences
Angel Pellicer, MDShared Resources
Mark Philips, MDBasic Research
Robert Schneider, PhDTranslational Research
James L. Speyer, MDClinical and Hospital Operations
Community Outreach and EducationDeborah Axelrod, MDMedical Director
Claudia AyashAdministrative Director
Danielle IavaroneSenior Coordinator
Rachael RennichProgram Associate
NYU Cancer Institute News Editorial Board
Deborah Axelrod, MDClaudia AyashStephanie V. Blank, MDMargo BloomWilliam L. Carroll, MDSteven GogelLauren E. HackettDanielle IavaroneMichelle Krogsgaard, PhD, MScMichele Pagano, MDMark Philips, MDRachael RennichFreya Schnabel, MDMarjorie ShafferJames L. Speyer, MD
Vice President for Communications &Public Affairs, NYU Langone Medical CenterDeborah Loeb Boren
www.nyuci.org
William L. Carroll, MD
Julie and Edward J. Minskoff Professor of Pediatrics
Professor of Pathology
Director, NYU Cancer Institute
3184W1 4/22/10 9:12 AM Page 2

NYU Cancer Institute news 3
Arlene and Arnold Goldstein, longtime
supporters of NYU Langone Medical Cen-
ter, have made a generous $1 million gift
to the NYU Cancer Institute to support a
breast cancer registry. The project is
designed to help investigators better
understand factors that influence the
development of the disease, response to
treatment, and long-term outcome.
The findings of the research will
advance the care of women diagnosed and
treated with breast cancer. Data generated
by the research could also lead to the
development of novel approaches for
identifying and monitoring women who
are most likely to develop the disease, with
the goal of finding it in its earliest, most
curable stages or even reducing breast can-
cer risk. The registry is directed by Freya
Schnabel, MD, Professor of Surgery, who
treated Mrs. Goldstein for breast cancer in
2009.
Both Mr. and Mrs. Goldstein were
very impressed with the care she received
at the NYUCI. “Arlene was overwhelmed
by the personal care and concern for her
well-being offered to her,” says Mr. Gold-
stein. “We could both see it was very gen-
uine. The NYU Cancer Institute staff are
like family.” When Dr. Schnabel told them
about the registry, Mrs. Goldstein liked the
idea of helping other women with breast
cancer by supporting the program.
Through this initiative, every person
who has breast cancer treatment at the
NYUCI and consents to the protocol will
be enrolled in the registry, along with de-
identified information about her medical
and family history, details of her cancer,
methods of treatment, and her outcome.
The program will enable investigators to
track women who are suspected of having
or are proven to have a genetic predisposi-
tion to breast cancer. This information
will allow them to understand the unique
issues of this patient population and assess
the possible benefits of risk-reducing
interventions. The registry data have the
potential to transform clinical practice
and frame public policy.
The Goldsteins’ contribution will also
support interactive educational programs
for healthcare providers and the public
through The Arlene and Arnold Goldstein
Seminars in Breast Cancer. Dr. Schnabel
plans to engage other physicians in an
educational dialogue throughout the
duration of the project.
“The Goldsteins’ gift supports a criti-
cal initiative that we need to look at
patient outcomes in a sophisticated way,”
says Dr. Schnabel. “It allows us to trans-
form every encounter we have with every
breast cancer patient into an opportunity
to learn something new. We’re going to
learn everything we can about our patients
and watch what happens over time. That’s
the best laboratory in the world.” ■
referrals • 212-731-5000
The NYU Cancer Institute honors the memory and commit-
ment of June Newmark, a member of our Board of Directors
since 2006 who passed away in February. Ms. Newmark was a
generous supporter of NYU Langone Medical Center, found-
ing the Ella and Saul Newmark Cancer Research Fund for the
study of women’s cancers in 1998 in honor of her parents. An
accomplished artist and wise investor, Ms. Newmark gra-
ciously supported various institutions in New York City
focusing on art, education, and medicine. As an artist, she
specialized in creating collages and paintings. Her work has
been exhibited at the Weill Cornell Medical College Library,
and a collage she once sent to President John F. Kennedy was
later displayed in the Kennedy Library. Her remarkable giving and support have enabled
us to make significant strides in the diagnosis and treatment of cancer in women, and
we will miss her presence.
Goldstein Gift Supports Breast Cancer Registry
Arlene and Arnold Goldstein
June Newmark
How You Can HelpDonations to the NYU Cancer Institutecan bring us closer to our goal ofdefeating cancer. Each gift — no matterwhat its size — furthers our researchefforts, enhances our clinical services, and expands our community programsso that we may help more people over-come this illness. You can give online atwww.nyuci.org, where you can:
• Create your own personal fundraisingpage
• Make an unrestricted gift• Direct your gift to fund a particular area• Honor your doctor, nurse, or loved one
Contributions can also be sent to:NYU Cancer InstituteNYU Langone Medical CenterOffice of DevelopmentOne Park Avenue, 17th FloorNew York, NY 10016
For more information, please contactMargo Bloom at 212-404-3638([email protected])
3184W1 4/22/10 9:12 AM Page 3

Mr. Rosenwald, Vice Chairman Emeritus at
J.P. Morgan. “We were impressed with the
team at the NYU Cancer Institute and are
truly excited about their work.”
“Our Thoracic Oncology Program is
unique in this city because the research
component is really blended in. Our basic
science and clinical investigators collabo-
rate as a team, talking on a regular basis
about what is going on in our labs and in
clinical trials,” explains Dr. Pass. “We are
the machine that drives the discovery and
the validation of novel biomarker and
therapeutic target molecules.”
The NYU Lung Cancer Biomarker CenterDr. Pass and William Rom, MD, Sol and
Judith Bergstein Professor of Medicine,
lead NYUCI’s participation in the National
Cancer Institute-funded Early Detection
Research Network — a national multicen-
ter effort to help accelerate the discovery
and evaluation of novel biomarkers for
detecting lung cancer early and identifying
people at increased risk for the disease. The
NYU Lung Cancer Biomarker Center,
established ten years ago, facilitates the
clinical validation and application of bio-
markers through this network and its own
investigations.
Program members have recruited
nearly 1,200 people over age 50 from the
tri-state area, including people at risk for
lung cancer who have at least a 20-pack-
year smoking history, with or without
workplace exposure to asbestos. These
individuals include workers from Consoli-
dated Edison (who has provided funding
for the study) who have known asbestos
exposure, as well as other patients. Partici-
pants in a control population (those not at
increased risk for lung cancer) include
never-smokers over age 50 and ex-smokers
with less than a 20-pack-year smoking his-
tory who quit at least five years prior to
entering the study.
Individuals complete a questionnaire,
undergo lung function testing and spiral
chest CT scanning, and provide blood and
sputum samples. For patients undergoing
lung biopsy or surgery, tissue samples are
collected and banked. The researchers are
following the study participants to see who
develops lung cancer and to correlate their
findings with the questionnaire results,
imaging tests, and analysis of tissue, blood,
and sputum samples.
The goal is to use the information
gleaned from the study to learn more
about who is most likely to get lung cancer
and to identify biomarkers that may signal
which patients with lung nodules found in
imaging studies require additional treat-
ment. So far, 52 percent of participants
have been found to have lung nodules
more than 4 mm in diameter; 24 of them
had lung cancer, one had an asbestos-relat-
ed cancer called mesothelioma, and anoth-
er had a lymphoma.
NYUCI investigators are collaborating
with a number of biotechnology compa-
nies and other universities to develop and
validate biomarkers (proteins and genes)
in the blood that may signal which patients
with lung nodules should continue to have
periodic CT scans, which should have sur-
gery, and which may need less aggressive
monitoring. “We can’t keep repeating CT
scans in all of these patients because of the
high cost and the radiation exposure
involved,” says Dr. Rom. “If we had a
serum biomarker, it would guide us beau-
tifully.”
A New PlatformNinety-two percent of patients diagnosed
with stage I lung cancer are still alive five
years later, but only a quarter of patients
have their lung cancers detected at this
early stage. NYUCI investigators are evalu-
ating a novel means of detecting the cancer
early through what could ultimately be a
simple blood test.
Margaret Huflejt, PhD, Assistant Pro-
fessor of Cardiothoracic Surgery, has devel-
oped a unique cancer diagnostic approach
that utilizes a “printed glycan array.” This
novel high-throughput platform contains
286 synthetic molecules (glycans) that are
sugars often expressed on the surfaces of
lung cells, including abnormal sugars pro-
4 NYU Cancer Institute news www.nyuci.org
NYUCI investigators are assessing a "printed glycan array" for evaluating lung cancer risk.
The NYUCI Thoracic Oncology Program continued from page 1
3184W1 4/28/10 5:25 AM Page 4

NYU Cancer Institute news 5
duced by lung cancer cells in response to
changes induced by the cancer process.
Researchers can measure antibodies
against these abnormal glycans in the
blood of people with mesothelioma or
lung adenocarcinoma or those at risk for
these diseases. This test could also be a tool
for identifying new therapeutic targets.
“We are developing this array as a
global way of looking at molecules that
may serve as very early markers to tell us
something is wrong inside lung cells,”
explains Dr. Pass, who is collaborating with
Dr. Huflejt on this project. “This informa-
tion can tell us if someone is at risk for the
mesothelioma or lung cancer, or if some-
one who already has the disease is likely to
do poorly and may need more aggressive
therapy.”
Because lung adenocarcinoma is the
most common cell type in nonsmokers,
the array could also potentially be used to
identify which nonsmokers are most at risk
for lung cancer. Toward this goal, the
NYUCI is partnering with the Canary
Foundation, a non-profit group “dedicated
to the goal of identifying cancer early
through a simple blood test and then iso-
lating it with imaging.”
NYUCI investigators are also on a
hunt for early detection biomarkers in the
breath of people with lung cancer and
those at risk for the disease. The research is
based on the premise that dogs have been
known to be able to distinguish between
people with and without cancer by
smelling their breath.
Other NYU investigators are studying
how lung cancer develops. Moon-Shong
Tang, PhD, Professor of Environmental
Medicine, Pathology, and Medicine, is
exploring DNA adducts (pieces of DNA
linked to cancer-causing substances) on
the p53 and KRAS genes (which are com-
monly mutated in lung cancer patients) to
see if these adducts cause the mutations
associated with lung cancer development.
Novel Drugs and Drug CombinationsLed by Marc Ballas, MD, Assistant Profes-
sor of Medicine, and Dr. Chachoua,
NYUCI investigators are conducting a
number of clinical trials evaluating new
chemotherapy agents and new combina-
tions of existing anticancer drugs to fine-
tune treatment and optimize the outcome
of patients with lung cancer. Studies are
available for patients with non-small cell
lung cancers (NSCLC) and small cell lung
cancers, those whose disease is surgically
removable and whose disease is not, and
people who’ve never had treatment as well
as those whose disease has progressed
despite therapy.
Several of the studies are assessing tar-
geted therapies that zero in on specific
receptors on cancer cells. “We’re learning
that different types of lung cancer respond
to different drugs, depending on the profile
of the tumor,” explains Dr. Ballas.
Examples of lung cancer clinical trials
available at the NYUCI include:
➤ ECOG 1505: comparing four differentcisplatin-based chemotherapy regimenswith and without bevacizumab (Avastin®)in patients with stage I-III NSCLC that hasbeen surgically removed
➤ 07–306 GSK: evaluating a vaccine
called MAGE-A3 for patients with stageIB-IIIA NSCLC that has been surgicallyremoved and whose tumors express thetarget protein MAGE-A3; patients receivethe vaccine in addition to any plannedchemotherapy to see if it can furtherreduce the risk of cancer recurrence
➤ RTOG 0617: assessing high-dose versuslow-dose radiation therapy plus carbo-platin/paclitaxel with or without cetux-imab in patients with stage III lung cancer
➤ RTOG 08-027: a study of stereotacticradiosurgery for stage I lung cancer pa-tients whose disease can be surgically re-moved but who don’t want to have surgery
➤ 08–756 Imclone: initial therapy withcarboplatin/paclitaxel plus a new investiga-tional drug called IMC 1121B (a humanantibody that interferes with the signalsgoverning the growth of blood vessels thatfeed a tumor) in patients with metastaticNSCLC
➤ ECOG 1508: a study of patients withsmall cell lung cancer comparing the cur-rent standard regimen versus the same reg-imen plus an investigational drug that is a“hedgehog inhibitor” (which interfereswith cancer cell growth and maturation),versus the standard regimen plus an inves-tigational “insulin growth factor antibody”(which interferes with cancer cell growthand division)
“We’ve made tremendous advances in
the treatment of advanced lung cancer, and
we’ve learned how specific chemotherapy
drugs work in specific settings, which is
very exciting,” concludes Dr. Ballas. “The
new trials of targeted therapies are very
promising and may help us learn how to
extend survival, and even manage lung can-
cer the same way we treat chronic diseases
such as diabetes and hypertension.” ■
People who are interested in participating in
the NYU Lung Cancer Biomarker Center
clinical trial may contact Ellen Eylers, RN,
Research Nurse, at 212-263-6126. For infor-
mation about clinical trials of lung cancer
treatments, call Genevieve Breeze, RN, at
212-731-5637.
referrals • 212-731-5000
The NYUCI is part of a national multicenter effort
to help accelerate the discovery and evaluation of
novel biomarkers for detecting lung cancer early and
identifying people at increased risk for the disease.
3184W1 4/22/10 9:12 AM Page 5

6 NYU Cancer Institute news www.nyuci.org
The young adult years can be filled with
promise: preparing for a new career, look-
ing for a first job, renting a first apart-
ment, getting married, starting a family. A
diagnosis of cancer can throw a serious
wrench into the works, sidelining personal
and career plans and filling a person with
uncertainty about the future. Some 70,000
young adults in the United States between
the ages of 15 and 40 face those quan-
daries each year when they learn they have
cancer.
That’s exactly what happened to
Matthew Zachary, who at age 21 was
studying at SUNY-Binghamton in 1995
for a career as a concert pianist when he
began to experience problems with his left
hand. The cause: a brain tumor called
medulloblastoma, which was successfully
treated, but which detoured Mr. Zachary’s
music career.
Instead he began a career in advertis-
ing and information technology, all the
while slowly regaining use of his left hand
— enough to release two acclaimed
albums by the fifth anniversary of his
diagnosis. Noticing the dearth of informa-
tion for young adults about cancer, and
feeling that physicians were less educated
about cancer in this age group than in
younger and older patients, Mr. Zachary
became increasingly active in the cancer
advocacy community. In 2004 he founded
a group called Steps for Living, which
became the I’m Too Young for This Can-
cer Foundation in 2007 (i[2]y for short).
He now leads i[2]y full-time.
“Our mission is to empower young
adults with cancer to get their lives back,
to redeem themselves and not become vic-
tims,” says Mr. Zachary. The i[2]y Web site
frequently encourages survivors to “get
busy living.”
He joined fellow cancer survivor and
advocate Curt Balch and NYU social
worker Leora Lowenthal, LCSW, MPA, at a
seminar hosted by the NYUCI in February
called Insurance Boot Camp for Young
Adults Affected by Cancer.
Mr. Balch was in a similar position in
2002, when he was diagnosed with stage
III testicular cancer at 23. He was an
Infantry Officer in the U.S. Army at the
time, with every intention of being a
career military officer. “I was deeply con-
fused,” he recalls. “I thought I had figured
out what I was going to do with my life,
and I had to change paths.” He was grant-
ed an honorable discharge from the Army
and relied on his economics degree from
Colgate University to become a financial
advisor.
Today he works full-time for a major
financial firm, and also donates his skills
to educate other young adults with cancer
about the unique issues they may face and
how to address them. These include:
➤ denial of medical, life, or disabilityinsurance due to a cancer history
➤ gaps in employment history due totime off for cancer treatment
➤ discrimination by prospective employ-
ers who fear that the survivor may experi-ence a recurrence
➤ discrimination by current employerswho may not be aware of their legalrequirement to give employees time off fortreatment or reasonable on-the-jobaccommodations when needed
“Concerns linger for us as young adult
cancer survivors that a relapse could destroy
everything we worked so hard to build back
up,” says Mr. Balch. He encourages young
adult cancer survivors to speak with their
hospital social workers to get referrals to
financial advice resources, and to their
workplace benefits coordinators to under-
stand their rights as an employee with can-
cer. His top pieces of advice are:
➤ Understand the Family Medical LeaveAct: employers with 50 or more employ-ees in a 75-mile radius must grant an eli-gible employee up to a total of 12 work-weeks of unpaid leave during a 12-monthperiod if the employee cannot workbecause of a serious medical condition, orif the employee must take off work to carefor an immediate family member with aserious medical condition. Employeesworking at companies with fewer than 50staff members may still be eligible to taketime off for medical reasons under theAmericans with Disabilities Act or NewYork State and City Human Rights Laws.
➤ Understand your right to reasonableaccommodations under the Americanswith Disabilities Act: employees may beable to negotiate flexible work hours, workspace alterations, writing aids, and otheraccommodations to ensure they can per-form the essential functions of their jobs.
➤ Ensure that your financial needs aremet: see a financial advisor for guidance.
➤ Understand your work benefits: seeyour human resources representative. ■
For more information, visit the i[2]y Web
site at www.i2y.com.
Young Adults with Cancer Face Unique Issues
3184W1 4/22/10 9:12 AM Page 6

to gene regulation. Because there is huge
variability in epigenetic changes from one
individual to another, and even within dif-
ferent tissues in the same individual, the
field offers an enormous array of research
opportunities. The NIH noted that epige-
netics will build upon our new knowledge
of the human genome, and help us better
understand the role of the environment in
regulating genes that protect our health or
make us more susceptible to disease.
We’re all born with 46 chromosomes
containing the DNA blueprint for our bod-
ies. But epigenetics is what makes your brain
a brain and your liver a liver, and not some
other organ. At the NYUCI, researchers are
exploring epigenetic changes resulting from
carcinogenic environmental exposures
around the world, and developing and eval-
uating novel anticancer drugs that work by
regulating gene activity.
“Epigenetics is related to the structure
of DNA in a complex fashion,” says Richard
Hayes, DDS, PhD, Associate Director for
Population Sciences at the NYU Cancer
Institute and Director of the Division of
Epidemiology in the Department of Envi-
ronmental Medicine at NYU School of
Medicine. “As we learn how to kill or rereg-
ulate cells with aberrant behavior by inter-
fering with epigenetic processes, we can cre-
ate new targets for cancer therapies.”
Lining Up at the WellIn a search for clean drinking water in the
1970s, the Army Corps of Engineers dug
new wells for the people of Bangladesh. But
high levels of arsenic contaminated many of
the wells, leading to elevated rates of skin
cancer among residents. Today contaminat-
ed wells are marked with a flag, leading to
long lines behind the uncontaminated wells
as people wait to obtain their daily ration of
clean water. But some choose not to wait
and continue to drink the water from the
tainted wells.
“We know that cancer is a disease of
epigenetic changes,” says Max Costa, PhD,
the Fred Wild Professor and Chair of Envi-
ronmental Medicine, Professor of Pharma-
cology, and Director of NYU’s Nelson Insti-
tute of Environmental Medicine. “Epigenet-
ics is like a computer program telling the
genome what to do. It tells it what’s going to
happen, when it’s going to happen, and how
it’s going to happen. There’s almost no dis-
ease that doesn’t have epigenetics as some
part of it.”
He is collaborating with researchers at
Columbia University to study epigenetic
changes in the white blood cells of people in
Bangladesh to see how those who have not
been exposed to arsenic differ from those
who have. The results will glean insights
into the molecular mechanisms through
which arsenic causes skin cancer.
Dr. Costa and his colleagues have been
collaborating with investigators at Princeton
University to explore the epigenetic changes
caused by arsenic and nickel (a particulate
component of air pollution). Princeton has
the only lab in the world that offers a form
of mass spectrometry that can be used to
study how “histones” are modified. Histones
are spool-like proteins that package DNA
neatly into chromosomes, and the modifi-
cation of histone tails forms the basis of
epigenetic changes.
Methyl groups (a carbon atom attached
to three hydrogen atoms) can attach to the
histones, coiling them tighter (turning genes
off) or uncoiling them (turning genes on).
Enzymes called demethylases remove methyl
groups from the histones, but metals such
as arsenic and nickel may bind to these
enzymes and inactivate them.
Nickel refining is still big business in
China, exposing workers to levels that raise
their risk of lung cancer fourfold. Dr. Costa
and his colleagues have received permission
from the Chinese government to obtain
samples of blood and mouth tissue from
nickel refinery workers in China for analy-
sis. They are also studying white blood cells
from foundry workers in Brescia, Italy
exposed to both nickel and arsenic. The
investigators will compare epigenetic
changes in white blood cells from exposed
and unexposed people.
They’ve already found that nickel inac-
tivates a tumor suppressor gene, which nor-
mally puts the brakes on rampant cell
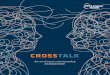
CHROMOSOME
DNA
HISTONE TAIL
HISTONE TAIL
DNA accessible, gene turned on
DNA hidden, gene turned off
HISTONE
GENE
METHYL GROUP
CHEMICALTAG
The epigenome can mark DNA in two ways that play a role in turning genes off or on. The first occurswhen chemical tags called “methyl groups” attach to the backbone of a DNA molecule. The second occurswhen chemical tags attach to the tails of histones.
Genes Under Siege continued from page 1
NYU Cancer Institute news 7referrals • 212-731-5000
continued on page 8
3184W1 4/22/10 9:12 AM Page 7

8 NYU Cancer Institute news www.nyuci.org
Reserving a limousine and ordering a cor-
sage have become staples of pre-prom
preparations for high school seniors
around the country. But there’s one more
ritual that many prom-going girls have
added to their lists: visits to their local
tanning salons. It’s a trend that has grown
in popularity over the years — and not
just at prom time, but all year long.
And it’s a disturbing trend. Last year
the World Health Organization announced
that it reclassified tanning beds to its highest
cancer risk category —“carcinogenic to
humans”— the same classification as tobac-
co, asbestos, and uranium. Studies have
linked these ultraviolet radiation-emitting
beds to melanoma, with people under age
30 who use them having up to a 75 per-
cent increased risk. And according to the
American Cancer Society, melanoma rates
among young women (ages 15–34) have
been rising at an alarming 3.8 percent per
year since 1995.
Rajni Kannan knows about the prob-
lem all too well, and is working with gov-
ernment officials to advocate for stronger
warnings and restrictions
for tanning beds. As an
Adult Nurse Practitioner
at the NYU Cancer Insti-
tute who works with
melanoma patients, she
has witnessed the prob-
lem firsthand.
She describes a young
woman in her 20s who
frequently used tanning
beds before cheerleading
competitions and before
prom when she was in
high school, and who is
now battling stage III
melanoma. “She’s a cute young girl who is
spending the majority of her 20s having
surgeries and getting treatment for
melanoma, instead of enjoying the life that
young women her age should be enjoy-
ing,” says Ms. Kannan.
She had attended a seminar teaching
her how to become a nurse advocate,
and this past January was sitting with
U.S. Reps. Carolyn Maloney (D-NY) and
Charlie Dent (R-PA), the editor-in-chief of
Cosmopolitan magazine (a staunch advo-
cate of safe sun approaches), and others at
a press conference announcing the intro-
duction of the Tanning Bed Cancer Con-
trol Act before Congress. The bill seeks to
expand the U.S. Food and Drug Adminis-
tration’s regulation of tanning beds from
their current Class I medical device clas-
sification (those that pose minimal harm,
Rajni Kannan’s Personal Crusade
NYUCI Adult Nurse Practitioner Rajni Kannan is advocating for strongerwarnings and restrictions for tanning beds.
growth, but when inactivated can lead to
cancer. They also discovered that nickel dis-
rupts iron levels in cells, altering demeth-
ylases by interfering with cell signaling
pathways. As a result, cancer cells learn to
live with little or no oxygen, enabling them
to grow and multiply unabated.
Why should we be concerned about
nickel and arsenic exposures in other coun-
tries? Says Dr. Costa, “Elucidating the roots
of cancer induced by these chemicals may
help us identify targets for new therapies, or
even preventive approaches.”
Taking It to the ClinicDr. Costa is working with Owen A. O’Con-
nor, MD, PhD, Deputy Director for Clinical
Research and Cancer Treatment and Direc-
tor of the Division of Hematologic Malig-
nancies and Medical Oncology in the NYU
Cancer Institute, to develop and assess “epi-
genetic agents” that interfere with enzymes
called histone deacetylases (HDAC) and a
protein called BCL6, which are involved in
certain types of lymphoma.
“The potential of epigenetics is spectac-
ular,” says Dr. O’Connor. “The idea of turn-
ing off bad genes and turning on good ones
sounds like science fiction, but we are
already doing it. By understanding the biolo-
gy of cancer, we can use epigenetic strategies
to learn how to modulate that biology in the
right therapeutic direction.”
Epigenetic drugs are already on the
market and in clinical use. Dr. O’Connor
was part of the team who developed an
HDAC inhibitor called vorinostat (marketed
as Zolinza®), which is approved for the
treatment of cutaneous T-cell lymphoma
(CTCL). Two other drugs — romidepsin
(Istodax®) for CTCL and valproate
(Depakote®) for seizures — also work by
inhibiting HDAC.
Investigators are assessing new combi-
nations of epigenetic agents and other
drugs, primarily in hematologic cancers
such as lymphoma and leukemia. For exam-
ple, the NYUCI is conducting a clinical trial
to evaluate vorinostat plus bortezomib
(Velcade®, which is approved for multiple
myeloma and mantle cell lymphoma) in
patients with multiple myeloma that has
become resistant to bortezomib. The ration-
ale is that vorinostat acts on the pathway
through which a myeloma cell develops
resistance to bortezomib, restoring sensitivi-
ty to the cancer-killing effects of bortezomib.
In another approach, vorinostat is
being combined with a vitamin called nia-
cinamide. Vorinostat turns off a cancer-
Genes Under Siege continued from page 7
3184W1 4/28/10 5:25 AM Page 8

NYU Cancer Institute news 9referrals • 212-731-5000
equivalent to Bands-Aids® and tongue
depressors) to a higher-level classification
which would place the beds on par with
tobacco and alcohol.
The new classification would require
tanning salons to post warnings more
conspicuously; current warnings are post-
ed on the machines themselves, and are
not always easily visible. The bill also seeks
performance standards that restrict the
strength of the ultraviolet rays emitted
and the amount of time a consumer
should remain in the bed. In March, Ms.
Kannan spoke before Congress in support
of the bill. “Each patient has a face and a
story. With education and better regula-
tion, we can save lives,” she says.
“Rajni’s dynamic involvement in
changing healthcare policy not only
demonstrates her personal mission to
impact the outcome of melanoma
patients, but also reflects the NYUCI
melanoma program’s commitment to
melanoma awareness and prevention on a
national level,” adds Anna Pavlick, DO,
Associate Professor of Medicine and Der-
matology. “We are very proud to have her
on our team.” ■
causing oncogene, while niacinamide turns
on a tumor-suppressing gene. The combina-
tion is under evaluation at the NYUCI in
patients with diffuse large B-cell lymphoma
whose disease persists despite up to ten
prior regimens of chemotherapy.
“This approach represents the ultimate
in tailored and targeted therapies, where we
are combining epigenetic agents and exploit-
ing their effects on various proteins in a way
that turns off bad genes and turns on good
genes,” Dr. O’Connor explains. “Once we can
sort out how best to combine these classes of
drugs, we can rationally use them to sensitize
cancer cells to conventional chemotherapy
and hopefully design more effective and less
toxic approaches to cancer treatment.” ■
To learn more about epigenetics, read the NIH
fact sheet at www.genome.gov/27532724.
Does alcohol cause cancer? Can losing weight
reduce your cancer risk? Are artificial sweeteners
bad news? Take this quiz to test your knowledge
of cancer fact versus fiction!
1. True or False: There is no association between
alcohol and cancer.
2. True or False: NutraSweet® (aspartame) causes
cancer.
3. True or False: Vitamin D may possibly reduce
the risk of certain cancers.
4. True or False: There is no link between obesity
and cancer risk.
5. True or False: Consuming only organic foods can
lower cancer risk.
6. True or False: Physical activity lowers the risk of
developing certain cancers.
Answers:
1. False.Alcohol increases the risk of developing cancers of the mouth,
throat, larynx, esophagus, liver, and breast, and may elevate colorectal can-
cer risk. If you drink alcohol, you should limit your intake to no more than
two drinks per day for men and one drink per day for women.
2. False.To date there is no evidence demonstrating a link between aspar-
tame and an increased risk of cancer.
3.True. There is a growing body of evidence from studies of large groups of
people that vitamin D may be helpful against some types of cancer, includ-
ing cancers of the colon, prostate, and breast. However, more research is
necessary to identify the optimal levels of intake and blood levels of vitamin
D required to reduce cancer risk.
4. False.Being overweight or obese has been associated with an elevated
risk of cancers of the breast (among women after menopause), colon,
endometrium, esophagus, and kidney, and possibly other sites as well.
Achieving and maintaining a healthy weight can not only lower your cancer
risk, but your risk of cardiovascular disease and diabetes as well.
5. False.To date, there are no studies suggesting that organic foods (which
are produced without pesticides or genetic modifications) are more effec-
tive for reducing cancer risk than foods produced by other methods.
6. True.Getting regular exercise can reduce the risk of colon and breast
cancers. And it does not have to be vigorous; daily walking can be quite
beneficial.
Source: American Cancer Society
Spring Health Quiz: Fact versus Fiction
3184W1 4/28/10 5:25 AM Page 9

10 NYU Cancer Institute news
Depression. Anxiety. Insomnia. Lack of
libido. Many of the therapies commonly
used to treat cancer today result in hor-
monal imbalances that can produce these
symptoms, impairing patients’ quality of
life. The good news is that help is avail-
able, in the form of medication and psy-
chotherapy that can relieve or alleviate
symptoms and make patients feel better.
“In general, just having cancer can
make some people feel anxious or
depressed and experience a loss of con-
trol,” says Carol Bernstein, MD, Associate
Professor of Psychiatry at NYU School of
Medicine. “But there is no reason to suffer.
There are treatments available to help
patients feel better.”
Dr. Bernstein spoke in January with
Andrew McCullough, MD, Associate Pro-
fessor of Urology, and Samantha M. Dun-
ham, MD, Assistant Professor of Obstet-
rics and Gynecology, at a presentation
hosted by the NYUCI that addressed hor-
monal changes during cancer treatment.
Such changes can result from hormonal
therapies as well as other treatments such
as surgery, chemotherapy, and radiation
therapy.
Hormonal therapies are most com-
monly used for the treatment of breast
and prostate cancers. Women with breast
cancer may receive tamoxifen or ralox-
ifene to reduce the risk of breast cancer
recurrence; both drugs interfere with
estrogen activity. Women taking these
drugs may experience menopause-like
symptoms such as hot flashes, vaginal dry-
ness, pain on intercourse, mood swings,
and weight gain. These symptoms may
also be brought upon by surgery to
remove the ovaries, certain chemotherapy
drugs, and radiation therapy to the pelvis.
Some men with prostate cancer, par-
ticularly those with advanced-stage dis-
ease, may receive therapies that lower can-
cer-fueling testosterone. Examples include
leuprolide and goserelin. While these
drugs have been shown to be effective for
shrinking prostate tumors, the lowered
testosterone levels they produce may cause
a loss of libido, depression, sluggishness,
and even occasional menopause-like
symptoms such as hot flashes. Certain
chemotherapy agents can also reduce
testosterone levels, generating these symp-
toms.
About a quarter of all people with
cancer are likely to feel depressed enough
at some point in the course of their dis-
ease to warrant evaluation and treatment.
Higher rates of depression are observed in
patients being treated for pancreatic,
breast, and lung cancers. Many patients
complain of cognitive impairment, such as
memory lapses and trouble concentrating.
Patients experiencing symptoms of
hormonal changes are encouraged to
speak to the physician who is overseeing
their cancer treatment. As for the choice
of therapy, “that’s a discussion between
the doctor and the patient,” says Dr. Bern-
stein. “It’s important to give people with
cancer a choice, since they may already be
feeling like they have so little control over
what is going on in their bodies.”
Some patients feel more comfortable
starting with medication, while others
may opt for psychotherapy first. Com-
monly used medications include:
➤ antidepressants, some of which havebeen shown not only to help with depres-sion but also relieve symptoms such as hotflashes and night sweats
➤ psychostimulants, which may promotea sense of well-being, decrease fatigue, andimprove cognitive abilities
➤ anti-anxiety drugs
➤ hormone replacement therapy forwomen who are eligible (may not beappropriate for women with breast orgynecologic cancers)
➤ testosterone replacement therapy formen who do not have prostate cancer
Supportive therapeutic approaches that
help many patients include:
➤ individual psychotherapy
➤ group therapy or support groups
➤ online self-help groups, thoughpatients are encouraged to speak to theirphysicians for recommendations aboutreputable Web sites
➤ exercises to improve cognition, such asdoing crossword puzzles or learning a newlanguage
➤ sex and couples therapy for patientsconcerned about their libido
➤ relaxation techniques such as yoga, taichi, and meditation
“You don’t have to go it alone,” con-
cludes Dr. Bernstein. “Help is out there if
you need it.” ■
Hormone Changes During Cancer Treatment?You Don’t Have to Go It Alone
www.nyuci.org
3184W1 4/22/10 9:12 AM Page 10

Registration is required for all events, and seating may be limited. Please call 212-263-2266 or e-mail [email protected] for more information and to register, unless otherwise noted.
events calendar
referrals • 212-731-5000
PANCREATIC CANCER LUNCHTIME AWARENESS PROGRAM
Thursday, May 13, 11:00 AM – 12:30 PM, Location A*Description: The exact cause of pancreatic cancer is still largely unknown,but certain factors are known to increase risk, such as age, gender, race, ciga-rette smoking, diet, environment, and family history. But risk factors do nottell us everything. Having a risk factor, or even several risk factors, does notmean that you will get the disease. And some people who get the disease donot have any known risk factors. Learn the latest facts about pancreatic canceras well as recent advances.
Presenters: Howard Hochster, MD, Elliot Newman, MD, Rebecca Yee, MS,CGC (certified genetic counselor), Kimberly Johnke, LMSW, Manager, Publicand Patient Information, The Lustgarten Foundation
A healthy lunch will be provided after the program. This program is co-sponsored with The Lustgarten Foundation, whose mission is to advance sci-entific and medical research related to the diagnosis, treatment, cure, and pre-vention of pancreatic cancer.
GYNECOLOGIC CANCER FOUNDATION’SOVARIAN CANCER SURVIVORS COURSE
Saturday, May 15, 9:00 AM – 4:00 PM, Location A*Description: The Gynecologic Cancer Foundation is pleased to offer thisfree course for all ovarian cancer survivors, friends, family members, andothers who are interested in hearing about ovarian cancer research andpatient care. Experts will share new information about the disease, includ-ing screening and early detection, symptoms, genetics, and clinical trials.Registration/check-in begins at 8:00 AM. Registration for the course willalso be available online at www.wcn.org.
This course is sponsored by the Gynecologic Cancer Foundation and ismade possible through sponsorship support from the NYU Cancer Instituteand the Ovarian Cancer Research Fund. For more information, please callthe Gynecologic Cancer Foundation at 312-578-1439.
WHAT YOU NEED TO KNOW ABOUT THYROID CANCER
Tuesday, May 18, 6:00 PM – 7:30 PM, Location B*Description: Thyroid cancer is the most common endocrine cancer and isone of the few cancers that has increased in incidence in recent years. Itoccurs in all age groups. This program will describe the different types ofthyroid cancer, incidence, risk factors, signs and symptoms, diagnosis, treat-ment options, and prognosis.
Presenters: David Myssiorek, MD, FACS, Kent Parks Friedman, MD, Jennifer Braemar Ogilvie, MD, FACS, Kepal Patel, MD, FACS, Rebecca M.Fenichel, MD
*Locations:
A: NYU Langone Medical Center, 550 First Avenue, Farkas Auditorium B: NYU Langone Medical Center, 550 First Avenue, Alumni Hall A
C: NYU Clinical Cancer Center, 160 East 34th Street, Room 1121 D: NYU Langone Medical Center, 550 First Avenue, Smilow Multipurpose Room
THE AMERICAN CANCER SOCIETY’S MAN TO MAN®PROSTATE CANCER EDUCATION AND SUPPORT PROGRAMDesigned to help men and their families cope with prostate cancer, Man to Man providesa comfortable setting among peers for discussion, education, and support through therecovery process. Spouses, partners, and family members are encouraged to attend.
Thursday, May 27, 5:30 PM – 7:30 PM, Location C*Topic: Complementary and Alternative Medicine for Prostate CancerPresenter: Geovanni Espinosa, ND, L.Ac, CNS, RH (AHG)
Thursday, June 10, 5:30 PM – 7:30 PM, Location C*Topic: Salvage Therapy OptionsPresenter: Stephen M. Scionti, MD
Thursday, July 22, 5:30 PM – 7:30 PM, Location C*Topic: Sexual Health and Fertility After Prostate CancerPresenter: Joseph Alukal, MD
RELAX…IT DOESN’T HURT
Tuesday, June 1, 6:00 PM – 7:30 PM, Location D*Description: Acupuncture has been used in the United States for many years as a treat-ment for chronic muscle pain. Only recently has it been tried as a remedy for other typesof pain, including cancer pain. Cancer patients who are not getting enough pain controlfrom conventional medications may be able to find relief in this ancient Chinese practice.Join us for a discussion about the history of acupuncture and the use of acupuncturewhile being treated for cancer. This program will also include a demonstration.
Presenter: Alex Moroz, MD
THE MANY FACES OF BREAST CANCERSaturday, June 19, 10:00 AM – 12:00 PM, Location A*
Description: The Many Faces of Breast Cancer is coming to New York City. Please join usfor this event, which will explore the unique needs and issues of those living with a can-cer diagnosis and provide the latest information on breast cancer. An engaging panel ofNYU Cancer Institute medical experts, breast cancer survivors, and advocates will discussissues that directly affect 2.5 million breast cancer survivors in the U.S. today, offeringinsights into the latest data surrounding treatment and key survivorship issues.
Please RSVP by calling 1-877-814-9421 or [email protected].
DAILY NEWS FREE PROSTATE CANCER SCREENING
Sunday, June 20 – Sunday, June 27Description: For screening locations and dates at the NYU Cancer Institute, please call212-263-2266 or visit www.nyuci.org. Co-sponsored by the Department of Urology.
3184W1 4/22/10 9:12 AM Page 11

The NYU Cancer Institute helps advance the care ofpatients with the most common types of cancer andblood disorders, including those of the:• Breast• Gynecologic Cancers• Gastrointestinal Tract• Genitourinary System (such as prostate cancer)• Neuro-Oncology (including brain cancer)• Lung• Head and Neck• Melanoma• Hematologic Cancers and other blood disorders• Sarcoma• Pediatric Cancers
NYU Clinical Cancer Center160 East 34th StreetNew York, NY 10016
As the principal outpatient facility of the NCI-designat-ed NYU Cancer Institute, the NYU Clinical Cancer Centerserves as home base for our patients and their care-givers. The center and its multidisciplinary team ofexperts provide convenient access to the latest treat-ment options and clinical trials, along with a variety ofprograms in cancer prevention, screening, diagnostics,genetic counseling, and supportive services.
IMPORTANT PHONE NUMBERS
New Patient Physician Referral Line 212-731-5000
Clinical Trials Information 212-263-6485
Mammography and/or Related Procedures 212-731-5002
Lucille Roberts Wellness Boutique 212-731-5198managed by Underneath It All
Lynne Cohen Breast Cancer 212-731-5452Preventive Care Program160 East 34th Street
Lynne Cohen Cancer Screening and 212-263-3198Prevention Project for High Risk WomenBellevue Hospital Center
Stephen D. Hassenfeld Children’s Center 212-263-8400for Cancer and Blood Disorders
100 Women in Hedge Funds 212-731-5345National Ovarian Cancer Early Detection Program
NYU Clinical Cancer Center 212-731-5480Support Group Information Line
Speakers Bureau & Community 212-263-8043Outreach Programs
Media Inquiries 212-404-3555
Office of Development 212-404-3640
NYULMC Office of Communications 212-404-3555
NYUCI Office of the Director 212-263-3276
215 Lexington Avenue, 15th Floor New York, NY 10016
FOR A PHYSICIAN REFERRAL , PLEASE CALL 212-731-5000
NYU Cancer Institute news IF YOU WOULD LIKE TO RECEIVE THIS NEWSLETTER, PLEASE SIGN UP FOR OUR MAILING LIST AT WWW.NYUCI.ORG.
NYU Cancer Institute newsDesign Tanya KrawciwContributing Writer Rosie FosterPhotography Gordon Cook p. 1, Cosmopolitan Magazine p. 8, istock p. 9, 10, 11
3184W1 4/22/10 9:12 AM Page 12