Embed Size (px)
Citation preview
PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 1
3.1 About project Z1 (E)
3.1.1 Title: Differential diagnosis and treatment of inflammatory cardiomyo-pathy
3.1.2 Principal investigators Schultheiss, Heinz-Peter, Prof. Dr., born 28.05.1948, German Phone: +49 30 8445 2344, Email: [email protected] Kühl, Uwe, Dr. rer. nat., born 23.09.1952, German Phone: +49 30 8445 4219, E-Mail: [email protected] Escher, Felicitas, Dr. Med., born 21.11.1975, German Phone: +49 30 8445 4219, E-Mail: [email protected] All: Charité – Universitätsmedizin Berlin, Medizinische Klinik II, Campus Benjamin Franklin, Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin, Hindenburgdamm 30, 12200 Berlin, Germany
3.2 Project history
The major task of Z1 was the screening and inclusion of patients with suspected DCMi by standardized clinical and diagnostic procedures, the gathering blood and heart tissue material for diagnostic and scientific evaluations, and the database-based documentation of clinical and scientific information. Biopsy information and continuous clinical follow-up of patients identified well characterized subgroups of patients and provided long-term information on the clinical cause of DCMi subgroups which were used by other scientific SFB projects to evaluate and test their experimental data in the human diseases. The baseline and follow-up information also established the basis for additional biomarker analyses by gene and microRNA profiling as predictive parameters of specific treatment options or evaluation of outcome. Biobank A biobank with heart tissue and blood from patients with identified specific disease entities or patients under specific treatment conditions has been gathered for scientific analyses of research groups. The biobank contains selected heart tissues, blood samples, samples of purified DNA and RNA (for further information see report Z2). Additionally, more than 800 blood samples especially prepared for miRNA analysis including follow-up sera for miRNA isolation and auto-antibody measurements as well as 650 pre-amplified samples for gene expression analyses (about 150 genes) were gathered. Documentation of data During the first eight years SFB period one scientist and one study nurse partially supported by two extern study nurses, both completely sponsored by the SFB-project, had been responsible for the acquisition and documentation of appropriate clinical data and patient materials of the newly included patients (indoor patient visits, n=1474) and the follow-up visits (n=11734), organization and planning of the follow-up-visits and treatment follow-ups (n=3063) including arrangements of required clinical tests (e.g. echocardiography, pulmonary functional tests, or blood counts), operating 6-minute walking tests, distributing, collecting and controlling the questionnaires, keeping phone contacts with patents, family doctors or other clinics, tracing not returned questionnaires or patients that did not appear at scheduled visits, and query information on survival of patients lost to follow-up. Despite the additional help of clinic stuff those time consuming tasks impeded an in time documentation in the SFB database (Z2), because a data input via VPN was not available at the start of the project and finally data input was extremely slow via this internet-based solution. Since this personal shortage was well recognized by the reviewers at the last SFB meeting 2012 in Greifswald, two additional positions were provided for additional 12 months in order to incorporate the missing clinical data. With the aid of the additional stuff and one additional 50% student position financed by non-SFB financial resources it up to now has been possible to document about 90% of the missing data in an inhouse database. The still missing data will be documented within the next 8 to 12 weeks.
PAGE 2 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Afterwards, the complete data sets of all patient visits will be transferred into the Z1 database. This indirect documentation of the missing clinical data of the outdoor visits became necessary because direct internet-based documentation into the Z1 database was, as mentioned above, too time consuming as mentioned above.
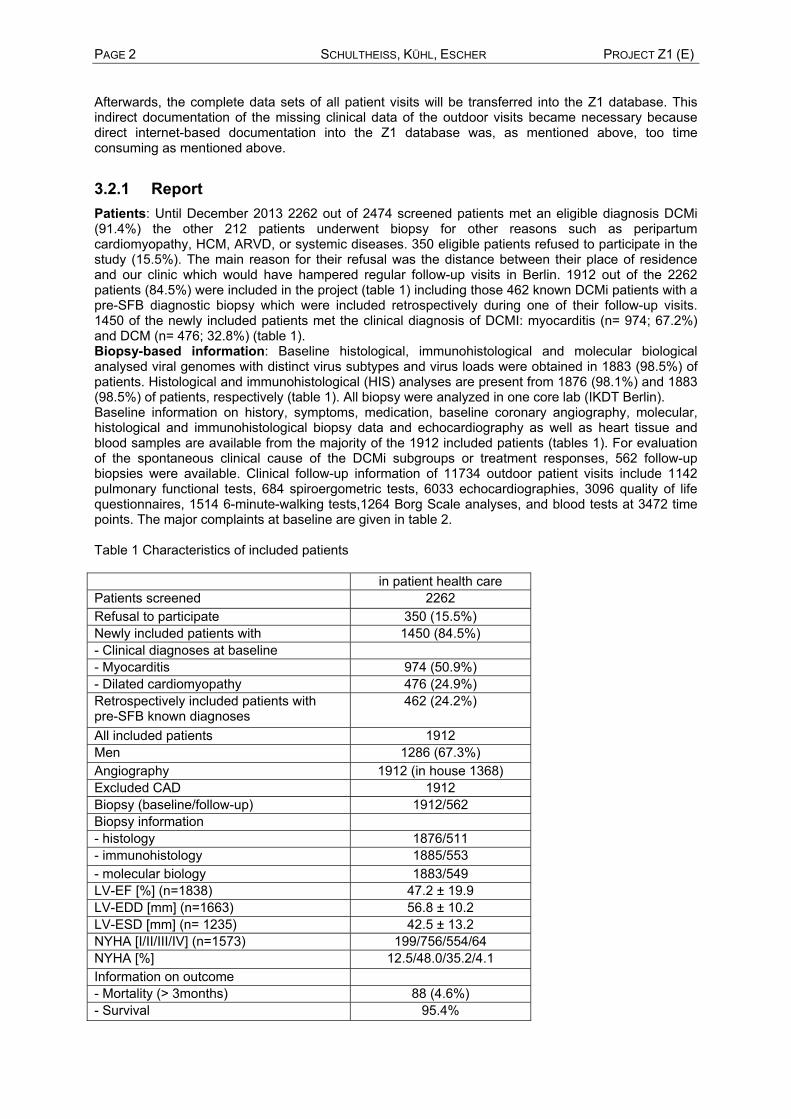
3.2.1 Report Patients: Until December 2013 2262 out of 2474 screened patients met an eligible diagnosis DCMi (91.4%) the other 212 patients underwent biopsy for other reasons such as peripartum cardiomyopathy, HCM, ARVD, or systemic diseases. 350 eligible patients refused to participate in the study (15.5%). The main reason for their refusal was the distance between their place of residence and our clinic which would have hampered regular follow-up visits in Berlin. 1912 out of the 2262 patients (84.5%) were included in the project (table 1) including those 462 known DCMi patients with a pre-SFB diagnostic biopsy which were included retrospectively during one of their follow-up visits. 1450 of the newly included patients met the clinical diagnosis of DCMI: myocarditis (n= 974; 67.2%) and DCM (n= 476; 32.8%) (table 1). Biopsy-based information: Baseline histological, immunohistological and molecular biological analysed viral genomes with distinct virus subtypes and virus loads were obtained in 1883 (98.5%) of patients. Histological and immunohistological (HIS) analyses are present from 1876 (98.1%) and 1883 (98.5%) of patients, respectively (table 1). All biopsy were analyzed in one core lab (IKDT Berlin). Baseline information on history, symptoms, medication, baseline coronary angiography, molecular, histological and immunohistological biopsy data and echocardiography as well as heart tissue and blood samples are available from the majority of the 1912 included patients (tables 1). For evaluation of the spontaneous clinical cause of the DCMi subgroups or treatment responses, 562 follow-up biopsies were available. Clinical follow-up information of 11734 outdoor patient visits include 1142 pulmonary functional tests, 684 spiroergometric tests, 6033 echocardiographies, 3096 quality of life questionnaires, 1514 6-minute-walking tests,1264 Borg Scale analyses, and blood tests at 3472 time points. The major complaints at baseline are given in table 2. Table 1 Characteristics of included patients in patient health care Patients screened 2262 Refusal to participate 350 (15.5%) Newly included patients with 1450 (84.5%) - Clinical diagnoses at baseline - Myocarditis 974 (50.9%) - Dilated cardiomyopathy 476 (24.9%) Retrospectively included patients with pre-SFB known diagnoses
462 (24.2%)
All included patients 1912 Men 1286 (67.3%) Angiography 1912 (in house 1368) Excluded CAD 1912 Biopsy (baseline/follow-up) 1912/562 Biopsy information - histology 1876/511 - immunohistology 1885/553 - molecular biology 1883/549 LV-EF [%] (n=1838) 47.2 ± 19.9 LV-EDD [mm] (n=1663) 56.8 ± 10.2 LV-ESD [mm] (n= 1235) 42.5 ± 13.2 NYHA [I/II/III/IV] (n=1573) 199/756/554/64 NYHA [%] 12.5/48.0/35.2/4.1 Information on outcome - Mortality (> 3months) 88 (4.6%) - Survival 95.4%

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 3 Table 2 Major clinical complaints at baseline Complaints at baseline biopsy frequency No reliable
information Angina at rest 416 (26.4%) 88 (5.3%) Angina on exertion 467 (29.6%) 96 (5.7%) Dyspnea at rest 521 (32.6%) 98 (5.8%) Dyspnea on exertion 1089 (71.0%) 102 (6.2%) Palpitations at rest 388 (26.4% 134 (8.3%) Palpitations on exertion 450 (30.7%) 139 (8.6%) Reduced physical ability 1174 (79.3%) 127 (7.9%) tiredness 758 (53.6%) 182 (11.4%) Specific treatments of patients with distinct DCMi subgroups
Depending on the biopsy-based diagnostic information and the individual clinical course of the disease, patients were treated with respect to the underlying pathologic condition on top of optimal heart failure medication (table 3). Patients with persisting viral infections were treated with interferon-α/β. Reactivated ciHHV6 and B19V were treated with ganciclovir/valganciclovir and telbivudine, respectively. During the 6 years of the SFB immunosuppression was not administered to virus-positive patients. Because about 60% of patients were erythovirus positive, immunosuppression was seldom initiated and restricted to patients with giant cell myocarditis (IGCM), cardiac sarcoidosis (CS), and virus-negative chronic inflammatory cardiomyopathy. During the last 2 years we have started with a prednisolon/azathioprin treatment in patients with overwhelming enterovirus and adenovirus negative acute myocarditis (>200 infiltrating Lymphocytes/mm2), patients with inflammatory cardiomyopathy and latent B19V-infection, if enteroviruses, adenoviruses, ciHHV6 and reactivated HHV6 and B19V had been excluded. Table 3 Specific treatments of patients with viral infections/reactivations or persisting inflammation and patients included in different studies Specific treatments Number of
patients Causes of treatment Number of
outdoor visits Interferon-β 59 EV, ADV, B19V, HHV6B 1282 Interferon-α 5 B19V 108 Ganciclovir 6 reactivated ciHHV6 121 Telbivudine 36 reactivatd B19V 454 Immunosuppression 75 myocarditis, GCM, sarcoidosis 852 Immunoadsorption 29 myocarditis 116 MRT-study myocarditis 21 active myocarditis 72 ETHICs-Study 19 clinically acute myocarditis 51 PPMC-Study 1 9ost partum cariomyopathy 7 Number of patients 251 3063
DCMi subgroups
The course of inflammatory cardiomyopathy is highly variable and not predictable from the initial clinical presentation (figure 1). Long term outcome depends on underlying causes such as distinct viruses, the grade and course of the inflammatory response and the extent of the consecutive myocardial injury. The proportion of an impaired outcome caused by the viral infection or myocardial inflammation and the long term effects of chronic infection or inflammation have not been characterized in detail and are only reported for distinct viruses or some acute inflammatory events. Clinical definition of disease entities The clinical diagnosis of acute or chronic heart failure due to myocarditis or DCM generally relies on routine non-invasive diagnostic criteria obtained from history and electrocardiographic, echocardiography or further imaging procedures which focus on potential features that may provide evidence to the etiology.

PAGE 4 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Patients that presented symptoms indicative of acute myocardial infarction including sudden onset of angina, ST-segment elevation, elevated kreatin kinase or Troponin T/I or patients with acute cardiac decompensation following a preceding viral infection (<12 weeks) were clinically classified as acute myocarditis. A preceding non-acute myocarditis in the recent past was taken into consideration if, according to available history, previously asymptomatic healthy patients unaware of any cardiac disease reported a timely defined onset of symptoms or lack of recovery from a preceding viral infection (<12 weeks) with distinct onset of symptomatic heart failure, global wall motion abnormalities (LV-EF below 45%) with or without ventricular dilatation or newly documented arrhythmias in the absence of documented electrocardiographic or laboratory signs of acute myocardial injury. Fatigue, weakness, chest pain at rest or on exertion, dyspnea on exertion, palpitations and reduced physical capacity were the dominant persisting complaints (table 3). This cohort of patients included clinically defined recent onset of “idiopathic” dilated cardiomyopathy. Patients were categorized as dilated cardiomyopathy (DCM) if presenting with symptoms of heart failure, left ventricular enlargement and global wall motion abnormalities of unknown origin with a documented reduced systolic left ventricular ejection fraction below 45% but no history or signs of myocarditis or acute myocardial injury. Spontaneous course of DCMi An echocardiographic follow-up (mean follow-up: 2.8±3.4 years) identified patients with spontaneous recovery or persisting systolic LV-EF dysfunction (figure 1). Reduced global LV-dysfunction recovered in about 25% of those patients who clinically present as DCM. Global LV-EF improved but remained impaired in 35%. An unchanged or deteriorated left ventricular function was observed in 40% of patients. In the myocarditis group, LV-EF remained impaired in 40% of patients whereas impaired systolic function further deteriorated in about 17% (figure 1).
Figure 1: Spontaneous hemodynamic course of patients with clinically suspected myocarditis and DCM (n=1098) Biopsy analysis After routine non-invasive diagnostic work-up and angiography had failed to elucidate any specific cause of heart failure, all patients underwent endomyocardial biopsy in order to obtain a more detailed information of the underlying cause of the disease. A minimum of eight endomyocardial biopsies was obtained from the right side of the ventricular septum or the left ventricle with a flexible bioptome (Westmed, Germany). Two specimens were fixed in 10% buffered formalin and embedded in paraffin for histological evaluation while immunohistochemical analyses (2 EMB) were carried out in TissueTec embedded frozen specimens. Inflammatory cells were counted by quantitative digital imaging analysis as reported elsewhere. The remaining 4 to 6 biopsy specimens were immediately frozen in liquid nitrogen and used for the
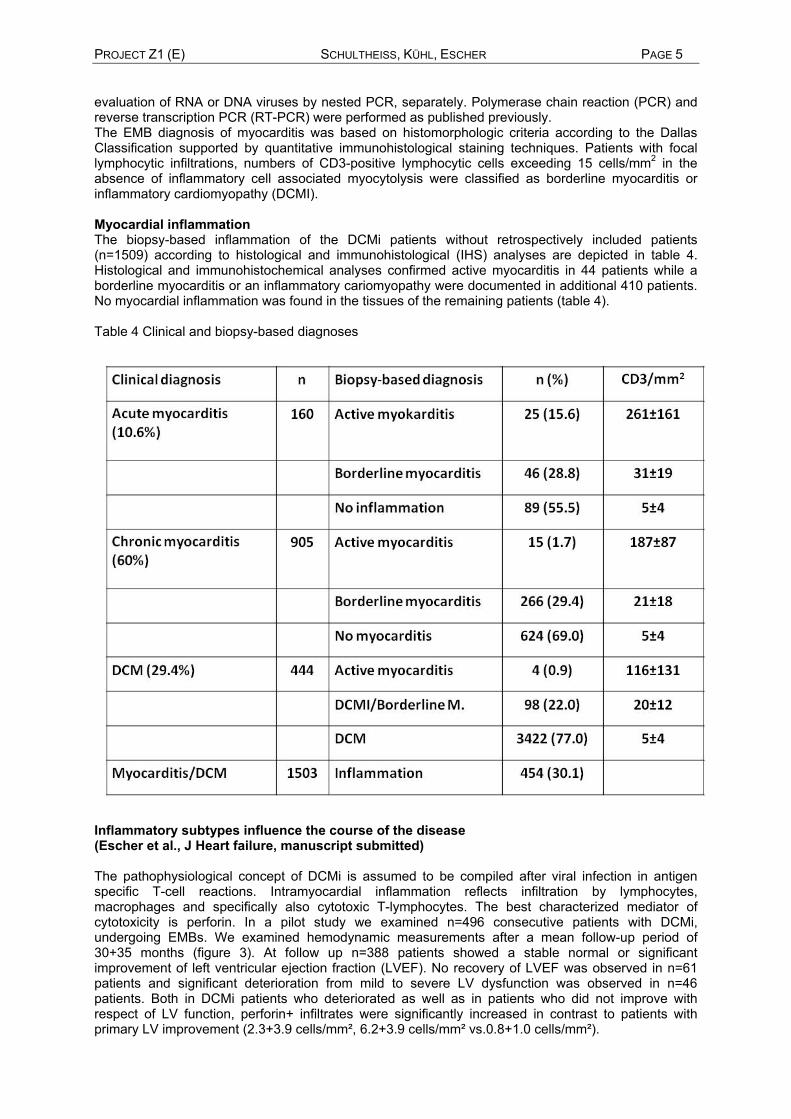
PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 5 evaluation of RNA or DNA viruses by nested PCR, separately. Polymerase chain reaction (PCR) and reverse transcription PCR (RT-PCR) were performed as published previously. The EMB diagnosis of myocarditis was based on histomorphologic criteria according to the Dallas Classification supported by quantitative immunohistological staining techniques. Patients with focal lymphocytic infiltrations, numbers of CD3-positive lymphocytic cells exceeding 15 cells/mm2 in the absence of inflammatory cell associated myocytolysis were classified as borderline myocarditis or inflammatory cardiomyopathy (DCMI). Myocardial inflammation The biopsy-based inflammation of the DCMi patients without retrospectively included patients (n=1509) according to histological and immunohistological (IHS) analyses are depicted in table 4. Histological and immunohistochemical analyses confirmed active myocarditis in 44 patients while a borderline myocarditis or an inflammatory cariomyopathy were documented in additional 410 patients. No myocardial inflammation was found in the tissues of the remaining patients (table 4). Table 4 Clinical and biopsy-based diagnoses
Inflammatory subtypes influence the course of the disease (Escher et al., J Heart failure, manuscript submitted) The pathophysiological concept of DCMi is assumed to be compiled after viral infection in antigen specific T-cell reactions. Intramyocardial inflammation reflects infiltration by lymphocytes, macrophages and specifically also cytotoxic T-lymphocytes. The best characterized mediator of cytotoxicity is perforin. In a pilot study we examined n=496 consecutive patients with DCMi, undergoing EMBs. We examined hemodynamic measurements after a mean follow-up period of 30+35 months (figure 3). At follow up n=388 patients showed a stable normal or significant improvement of left ventricular ejection fraction (LVEF). No recovery of LVEF was observed in n=61 patients and significant deterioration from mild to severe LV dysfunction was observed in n=46 patients. Both in DCMi patients who deteriorated as well as in patients who did not improve with respect of LV function, perforin+ infiltrates were significantly increased in contrast to patients with primary LV improvement (2.3+3.9 cells/mm², 6.2+3.9 cells/mm² vs.0.8+1.0 cells/mm²).

PAGE 6 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E)
Figure 3: Immunohistochemical characterization of perforin-positive inflammatory infiltrates with respect to the clinical course.
One future focus will be on the characterization of the prognostic value of cytotoxic T-lymphocytes and other biomarkers such as inflammatory cell subtypes in patients with DCMi subgroups with or without a simultaneous viral infection relevant for long term prognosis and future therapeutic interventions. The clinical course of giant cell myocarditis Giant cell myocarditis (GCM) is a rare disorder in which survival beyond 1 year without heart transplantation is uncommon and 40% of patients die within the first 2 to 4 weeks after onset and only 10% are alive after 5 years. Only immediate and aggressive immunosuppression improve outcome with partial recovery of systolic LV-function despite the fact that a high percentage of the myocardial tissue is already irreversibly damaged. In an attempt to gain first insight into the treatment associated outcome of patients with GCM, we have analyzed the long-term risk of death, transplantation and disease recurrence in GCM in collaboration with the Mayo Clinic (Prof. L. Cooper). We identified 26 patients with biopsy proven GCM from a multicenter GCM registry (8 from the Charite Berlin) who survived more than 1 year without heart transplantation. The incidence of death, transplantation, ventricular assist device placement and histologically proven disease recurrence was ascertained retrospectively. The rates of recurrent heart failure, ventricular arrhythmias, renal failure, and infectious complications were calculated. The mean age of the cohort was 51.6+/-14.1 yr. with 10 males and 16 females. The average duration of follow up was 5.4 years (range 1.0 to 16.6). There were 3 deaths (11.5%), 5 heart transplantations (19.2%), and 1 VAD placement (4%). 3 histologically confirmed recurrences of GCM (11.5%) occurred between 1.5 and 8 years after diagnosis. 2 of the 3 recurrences occurred in patients who recently discontinued immunosuppression. Fifty percent of the cohort (13/26) experienced a total of 29 heart failure episodes more than 1 year after initial diagnosis. There were 30 episodes of elevated creatinine in 12 patients, 42 infectious events in 13 patients, and 20 episodes of ventricular arrhythmias in 6 patients. Overall mortality after year 1 was greater in those patients who received 0 or 1 immunosuppressive drugs than in those who received 2 or more in drugs in the first year after GCM diagnosis (p=.027).Our data suggest that patients diagnosed with GCM who survive more than 1 year have nearly a 50% combined risk of death, transplantation, VAD placement and histologically confirmed disease recurrence. The risk of GCM recurrence continues to at least 8 years after diagnosis Classification of 4 chemically different amyloid types in routine endomyocardial biopsies by validated immunohistochemistry. (Lassner et al. Amyloid 2010 Cardiac amyloidosis, which is associated with interstitial and vascular deposition of amyloidotic proteins in the myocardium, may cause restrictive cardiomyopathy with a poor prognosis. Of the 3 major functional categories of the cardiomyopathies (dilated (DCM), hypertrophic (HCM), restrictive

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 7 (RCM)), restrictive cardiomyopathy is the least common form in adults and in children. Patients present with symptoms of heart failure, a decreased volume of both ventricles, biatrial enlargement and an increased wall thickness on echocardiogram are suspicious of amyloidosis. The identification of proteins causing cardiac amyloidosis is of paramount importance for further clinical management. Since the first therapeutic approaches have been established, it has been mandatory to identify the particular amyloid type in order to select the most efficient therapy for each patient. Endomyocardial biopsies from 275 patients with a suspected diagnosis of storage disease, hypertrophic or restrictive cardiomyopathy were additionally analyzed for the presence of amyloid deposits using Congo red staining.1 The results revealed the presence of amyloid in 31/275 (11.3%) of cases. The classification of 25 of these 31 patients using validated immunohistochemistry resulted in 25 correct diagnoses, including four different amyloid classes with the prevalence: ATTR (14/25; 56%), ALlambda (8/25; 32%), ALkappa (2/25; 8% ) and AA (1/25; 4%) demonstrating (a) amyloid-type specific cardiotropy and (b) the usefulness of validated immunohistochemistry on fixed paraffin-sections for amyloid typing as a method for every routine laboratory.
Figure X Frequency of different amyloidosis forms in endomyocardial biopsies of IKDT cohort in comparison with 3 published cohorts (#) of consecutive biopsy series of major organs (heart, liver, kidney). (Lassner, Amyloid 2010) These data using validated immunohistochemistry show that 100% of patients in this panel could be classified correctly. A right suspected diagnosis is essential for selection of possible amyloid positive patients. In case of suspected amyloidosis, storage diseases, unexplainable RCM and HCM should be performed an Congo Red staining for exclusion of amyloid protein in myocardial tissue. If Congo Red staining reveals a positive signal immunohistochemical staining is highly recommended.In our cohort 4/31 of suspected diagnosis (12%) were not directly associated with amyloidosis (DCM, sarcoidosis, diastolic dysfunction) Myocardial virus infection Viral involvement was identified through molecular biological analyses which identified distinct viral infections such as adenoviruses (ADV), enteroviruses (EV), erythrovirus genotypes 1 (B19V) and 2, human herpesvirus type-6 (HHV6 A/B), chromosomally integrated HHV6 (ciHHV6 A/B), and Ebstein Barr virus (EBV) as the most frequents infectious agents (table 5). If neither inflammatory infiltrates nor infectious agents were identified at the time of biopsy in the DCMi-cohort (n=1489) despite a typical history or clinical presentation, post-infectious or post-inflammatory DCMi disease stages were suggested, although such assumptions can never be proven in patients with a resolved inflammation or a cleared infection. The remaining patients with a questionable cause of heart failure included patients with systemic disorders such as sarcoidosis, vasculitis, amyloidosis, and others. Table 5: Frequency of cardiotropic viruses in the diagnosed patient groups

PAGE 8 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Virus (nPCR) Numbers (%) DCM DCMi Active
myocarditis Borderline myocarditis
Excluded myocarditis
1883 364 (24.5) 98 (6.6) 44 (3.0) 305 (20.5) 678 (45.5) Virus negative 462 (24.5) 89 (24.5) 31 (31.6) 11 (25.0) 74 (24.6) 164 (24.2) Enterovirus (EV) 48 (2.6) 4 (1.1) 1 (1.0) 0 5 (1.6) 12 (1.5) Adenovirus (ADV)
2 (0.3) 0 0 0 1 (0.3) 1 (0.1)
Erythro-/Parvovirus (B19V)
1316 (69.9) 212 (58.2) 56 (57.1) 21 (47.7) 175 (57.3) 388 (57.2)
Herpesvirus 6 (HHV6 A/B)
259 (13.8) 18 (5.0) 1 (1.0) 2 (4.6) 11 (3.6) 23 (3.4)
ciHHV6 19 0 0 0 18 (94.4) 1 Ebstein Barr virus (EBV)
17 (0.9)
Hepatisvirus (HCV)
1 (0.05) 0 0 0 0 1 (0.1)
Double infections
EV + B19V 20 (0.01) 3 (0.8) 0 1 (2.3) 7 (2.3) 5 (0.7) EV + HHV6 2 (0.001) 0 0 0 0 0 ADV + B19V 2 (0.0001) 0 0 2 (4.6) 0 0 B19V + HHV6 173 (0.09) 33 (9.1) 7 (7.1) 0 26 (8.5) 78 (11.5) B19V + EBV 10 (0.005) 2 (0.6) 2 (2.0) 2 (4.6) 1 (0.3) 1 (0.1) B19V + HCV 1 (0.0005) 0 0 0 0 1 (0.1) Multiple infections
EV + B19V +HHV6
3 (0.002) 1 (0.3) 0 0 1 (0.3) 1 (0.1)
EV + B19V + EBV
1 (0.0005) 0 0 0 0 1 (0.1)
ADV + B19V + HHV6
2 (0.001) 1 0 0 1 (0.3) 0
B19V + HHV6 + EBV
7 (0.004) 0 0 3 (6.8) 2 (0.7) 1 (0.1)
Erythrovirus subtypes within the myocardium (Kühl et at, JMV 2008) Human erythroviruses cluster into three genotypes 1 to 3 which share a high degree of homology between major structural proteins and may cause clinically and serologically indistinguishable infections. In human cardiac tissue erythrovirus genotypes other than parvovirus B19 (B19V) had not yet been reported. Using a new consensus PCR assay designed for the detection of the three erythrovirus sequences, 245 (51%) of 480 consecutive patients who underwent endomyocardial biopsy (EMB) for the elucidation of heart failure of unknown origin were erythrovirus-positive. In a first study, genotype 1-specific sequences (prototype virus B19V) were detected in 88/245 (34%) of positive biopsy samples, whereas genotype 2-specific sequences (prototyp virus LaLi) so far considered rare in human diseases and not yet been described in human heart tissue constituted the majority (157/245, 64%) of positive biopsy specimen. Genotype 1 was preferentially detected in young patients below 35 years of age, whereas in individuals above 45 years of age genotype 2 became predominant (figure 2).2 These data revealed for the first time that a distinct erythrovirus variant previously considered to be very rare in humans is preferentially associated with a human cardiac disease. The percentages of erythrovirus genotypes and the age distribution did not change significantly, since erythrovirus genotyping has been implemented 2008 in the routine molecular biological virus analysis of all DCMI patients undergoing EMB.

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 9
Figure 2: Age-dependent distribution of the erythrovirus genotypes 1 and 2.
Vasculotropic parvovirus infection impairs outcome in inflammatory cardiomyopathy (Kühl et al., manuscript submitted) Erythrovirus (parvovirus B19V) infections are acquired by majority in the childhood and persist lifelong within bone marrow precursor cells and the vascular endothelium in >70 of the adult population. Because many infected patients remain asymptomatic, the clinical relevance of erythrovirus detection in myocardial tissue has remained doubtful. The outcome of patients with parvovirus associated inflammatory cardiomyopathy is not known. To gain insight into the long-term effect of this chronic vasculotropic infection we followed patients with severe heart failure (LV-EF < 45%) due to clinically suspected myocarditis in the past or DCM from first diagnostic biopsy for 60 months and compared their outcome with respect to quantitative biopsy-based information on myocardial inflammation and infection. The study group comprised of 600 consecutive B19V positive or virus negative patients (441 man (73.6%), mean age 53.0±12.6 years) who were admitted to our institution between June 2004 and December 2011 to evaluate the cause of heart failure symptoms and global wall motion abnormalities (LV-EF<45%, mean EF 29.5±8.9%, median 30.0%, range 7% to 45%). According to history and presentation the patients were clinically categorized as suspected myocarditis in the past (n=310, 52.0%) or DCM (n=290, 48.0%). Follow-up information on outcome was available for 534/600 patients (89%). Patients with clinically acute myocarditis or patients with other virus infections were not included in the study. The EMB diagnosis of myocarditis was based on histomorphologic criteria according to the Dallas Classification supported by quantitative immunohistological staining techniques. Patients with focal lymphocytic infiltrations or numbers of CD3-positive lymphocytic cells exceeding 15 cells/mm2 in the absence of inflammatory cell associated myocytolysis were classified as borderline myocarditis or inflammatory cardiomyopathy (DCMI), respectively. 423 patients (71.5%) were B19V positive while no virus was detected in EMB of 177 patients (29.5%). Both cohorts presented with similar clinical features (table 2). The frequency of virus positive patients was not different between clinically suspected myocarditis in the past (n=221; 71.3%) and DCM (n=202; 69.7%) (p=0.661). In comparison with the DCM group the median B19V copy numbers were slightly elevated (p=0.038) in the myocarditis group (185 copies, range 0-405763 versus 125 copies, range 0-5692) while the portion of patients with B19V copies above 500/µg isolated myocardial DNA was increased in the myocarditis group (23.5% versus 13.1%, p=0.007) (table x). Histological and immunohistochemical analyses confirmed chronic inflammation in 118 out of 310 consecutive patients (38.1%) who clinically presented as suspected myocarditis in the past. No myocardial inflammation was found in the remaining 192 tissue specimens (61.9%). DCMI was confirmed in 79 (27.2%) of 290 patients clinically classified as “idiopathic DCM” according to the recommendations of the World Health Organization-International Society and Federation of Cardiology Task Force. The quantitative inflammatory cell characteristics were not different in virus negative and B19V-positive patients.

PAGE 10 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Since a B19V virus load above 500 copies has been considered a clinically relevant infection, we first calculated the five year outcome of B19V positive patients with copy numbers above and below the suspected threshold. Survival of both cohorts was nearly identical (figure 3A), suggesting that the virus load alone has no direct effect on outcome. Quantitative evaluation of myocardial inflammation revealed that outcome became impaired (p=0.01) if CD3-positive lymphocytes rose above a threshold value of 10 cells/mm2 (figure 3B). Additional consideration of the virus information indicated a more relevant increase in mortality (p<0.0002) in patients with B19V positive inflammation only (figure 3C) while outcome of B19V negative patient with or without an equal grade of inflammation was not significantly altered (p=0.863).
A B C Figure 3 A-C: Six year outcome of patients (n=600) with respect to B19V virus load (A), inflammation regardeless of the virus status (B) and inflammation in B19V positive and negative patients (C). If the biopsy diagnoses were taken into consideration, it became evident that inflammatory cell associated mortality was most pronounced (p<0.0006) in B19V-positive inflammatory cardiomyopathy (figure 3D). Despite identical clinical features, depression of systolic left ventricular function and inflammatory cell numbers, survival was not influenced in virus negative DCMI (p=0.674) (figure 3E).
D E Figure 3D-E: Six year outcome of patients with B19V positive (D) and B19V negative (E) inflammatory cardiomyopathy. The data show that in patients with inflammatory cardiomyopathy and significantly affected systolic function the presence of B19V infection of endothelial cells is associated with an impaired survival in comparison to virus negative patients presenting with a similar grade of inflammation. The underlying pathogenetic mechanisms are unknown but may involve either aggravation of inflammatory cell associated myocardial injury or affect outcome due to an additional chronic endothelial dysfunction both of which can be caused by the vasculotropic virus infection. B19V infected vascular endothelium thus may represent an important cofactor that strongly influences the clinical course of inflammatory cardiomyopathy.
Erythrovirus reactivation in-vitro and in-vivo: (Kühl et al., BRC 2013) Human erythrovirus (B19V) DNA is highly prevalent in endothelial cells lining up intramyocardial arterioles and postcapillary venules of patients with chronic myocarditis and cardiomyopathies. In cooperation with A5 we addressed the question of a possible stimulation of B19V gene expression in endothelial cells by infection with adenoviruses. A limited B19V genome replication could be

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 11 demonstrated in endothelial cells and adenovirus infection induced the appearance of putative dimeric replication intermediates. Thus the almost complete block in B19V gene expression seen in endothelial cells can be abrogated by infection with other viruses.3 In an translational approach we checked for erythrovirus replication in-vivo and evaluated in a prospective study using endomyocardial biopsy (EMB) specimens of 537 consecutive patients with clinically suspected myocarditis (n=383) or idiopathic dilated cardiomyopathy (n=154).4 For this study, patients with other virus genomes detected by nested polymerase chain reaction analysis (nPCR) in the routine molecular biological analysis were excluded from further analysis. 415 consecutive erythrovirus-positive patients were screened for erythroviral loads and the presence of erythrovirus-encoded VP1/VP2 mRNA using polymerase chain reaction (PCR) assays. Their genetic data were compared with those of the 122 virus-negative patients who presented with a similar frequency (p=0.222) of clinically suspected myocarditis or DCM at the symptomatic start of their disease.
Tables 6 A: Transcriptionally active B19V infection detected in subgroups of patients with myocarditis, clinically suspected myocarditis without biopsy-based confirmation of inflammation, inflammatory cardiomyopathy and DCM. B: The clinical complaints of these patients are not significantly different from those with latent B19V infection and virus negative cardiac tissue.
A B
For the gene expression analysis, differential gene expression was determined by real-time PCR of patients with sufficient biopsy material (latent B19V-infection: n=22, active infection: n=45, virus free hearts: n=23). Due to limited amounts of cDNA a pre-amplification technique was applied. Screening of erythrovirus-positive patients (n=415) revealed erythroviral transcriptional activity in 66 (15.9 %) EMB (“active infection”). Virus genome copy numbers were significantly elevated in VP1/VP2 mRNA-positive tissues: 189 (13-895) pg/isolated DNA vs. 277 (44-2678) pg/isolated RNA, respectively (p=0.002). Transcriptionally active erythrovirus mRNA was detected in 56/302 (18.5%) patients presenting as myocarditis and 10/113 (8.8%) of patients presenting as DCM/DCMI, respectively (table 6). Of note, “active infection” was present in inflamed and non-inflamed myocardium with similar frequencies and did not depend on the severity of systolic left ventricular dysfunction (table 6A). With respect to basic clinical characteristics, patients with latent and active B19V infection or virus free hearts did not differ significantly (table 6B).4 At the molecular level, highly significant deregulation of genes encoding proteins of the antiviral immune response, B19V receptor complex, and mitochondrial energy metabolism was detected between patients with active versus latent virus (figure 4A). Importantly, re-silencing of B19V in individual patients was associated with reversal of the cardiac expression pattern to baseline and genes returned to the pattern of latently infected or virus-negative human myocardium (figure 4B).
These data suggest that cardiac erythrovirus reactivation from latency, as reported here for the first time, appears to be a key viral factor for the induction of symptomatic heart disease. These findings are interesting from the virological point of view with regard to the generally important question which exogenous cofactors are required to turn a latent virus such as B19V into a highly pathogenic agent. Possible cofactors are secondary viral infections, e.g. by B19V-transactivating virus species such as adenoviruses,2 or immunosuppressive agents such as used in post-transplant patients. Two important recent studies have in fact demonstrated that cardiac graft survival is negatively influenced by the presence of B19V genome in the transplants, suggesting that reactivation of this vasculotropic virus may also be involved in the long-term pathogenesis of other cardiac diseases such as coronary microangiopathy. Those pioneering studies on transplant patients have employed virus genome
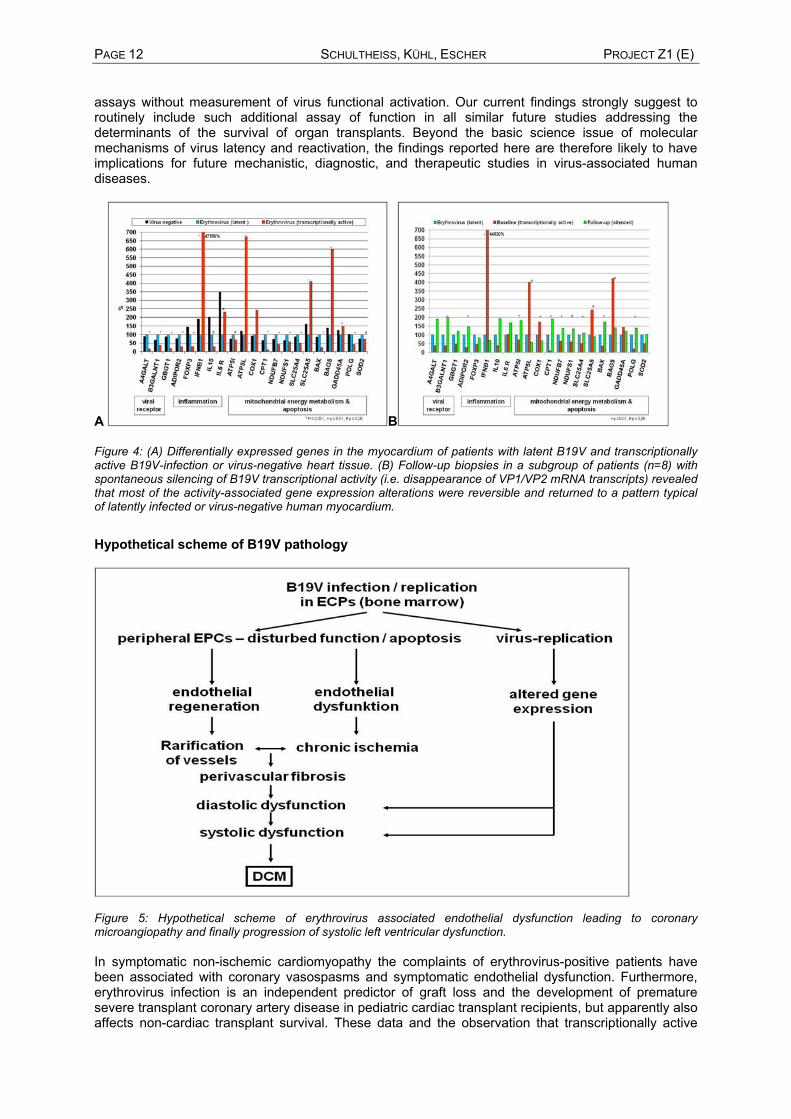
PAGE 12 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) assays without measurement of virus functional activation. Our current findings strongly suggest to routinely include such additional assay of function in all similar future studies addressing the determinants of the survival of organ transplants. Beyond the basic science issue of molecular mechanisms of virus latency and reactivation, the findings reported here are therefore likely to have implications for future mechanistic, diagnostic, and therapeutic studies in virus-associated human diseases.
A B
Figure 4: (A) Differentially expressed genes in the myocardium of patients with latent B19V and transcriptionally active B19V-infection or virus-negative heart tissue. (B) Follow-up biopsies in a subgroup of patients (n=8) with spontaneous silencing of B19V transcriptional activity (i.e. disappearance of VP1/VP2 mRNA transcripts) revealed that most of the activity-associated gene expression alterations were reversible and returned to a pattern typical of latently infected or virus-negative human myocardium.
Hypothetical scheme of B19V pathology
Figure 5: Hypothetical scheme of erythrovirus associated endothelial dysfunction leading to coronary microangiopathy and finally progression of systolic left ventricular dysfunction. In symptomatic non-ischemic cardiomyopathy the complaints of erythrovirus-positive patients have been associated with coronary vasospasms and symptomatic endothelial dysfunction. Furthermore, erythrovirus infection is an independent predictor of graft loss and the development of premature severe transplant coronary artery disease in pediatric cardiac transplant recipients, but apparently also affects non-cardiac transplant survival. These data and the observation that transcriptionally active

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 13 erythrovirus is associated with symptomatic endothelial dysfunction and significant deregulation of genes encoding proteins of the antiviral immune response, B19V receptor complex, and mitochondrial energy metabolism suggest that endothelial cell infection with this vasculotropic virus may favour a cardiac microangiopathy and, in the long run, cause progression of systolic left ventricular dysfunction (figure 8). B19V infected vascular endothelium thus may represent an additional cofactor that strongly influences the clinical course of B19V-positive inflammatory cardiomyopathy.
Cardiac involvement ofhuman herpesvirus 6 in patients with inflammatory cardiomyopathy (Escher et al., manuscript submitted) Human herpesvirus 6 (HHV-6) has recently been classified as two distinct species, HHV-6A and HHV-6B, with significant differences in their biological, immunological, and molecular properties. Both betaherpesviruses are closely related to the human cytomegalovirus, and establish a lifelong latency upon primary infection with a seroprevalence of >90% in adults. HHV-6B is commonly acquired during the first two years of life, whereas HHV-6A is acquired later in childhood with unknown prevalence.3, 5-8 HHV-6A and HHV-6B are lymphotropic viruses that can also infect a broad number of cell types including the vascular endothelium.5 HHV-6 reactivation results in subacute clinical presentations, especially in acquired or drug-induced immune deficiencies (e.g. transplant recipients) or in patients with autoimmune disorders. It has been suggested that HHV-6 enhances the pathogenicity of other viruses and is not always the causative agent. It can infect various organs, even though infectious virus cannot be isolated from the peripheral blood and the virus genome remains below the detection limit in these patients. Similarly, HHV-6 can persist in different organs such as brain tissue, heart and liver with little or no trace in the peripheral blood, discoverable only by biopsy or at autopsy. Recently, HHV-6 has been detected in the myocardium of patients with myocarditis and clinically suspected dilated cardiomyopathy (DCM) by PCR.9 Short-term follow-ups revealed an association with the clinical course of the disease.10 We analyzed the long-term spontaneous course of cardiac HHV-6 infections in follow-up biopsies of patients suffering from inflammatory cardiomyopathy (CMi). We prospectively evaluated patients (n=73) with biopsy-proven viral HHV-6 infection in endomyocardial biopsies (EMBs), followed up by reanalysis of EMBs and left ventricular ejection fraction (LV-EF) measurements after a median period of 8.8 months (range 4 to 73 months). Beyond, we studied HHV-6 prevalence in isolated peripheral blood cells (PBCs) and HHV-6 variants in EMBs. HHV-6 variant-specific cellular infection sites within the myocardium were identified by immunohistochemistry (IHC). We identified 73 patients with cardiac HHV-6 reactivation or newly detected in follow-up EMB (95.0% genotype B). Systemic HHV-6 reactivation was primarily associated with genotype A. Persistence of cardiac HHV-6 genome was significantly associated with cardiac dysfunction at follow-up (LV-EF deteriorated from 58.2+16.0 to 51.8+17.2%, p<0.001), and LV improvement was observed when HHV-6 reactivation resolved (LV-EF increased from 54.9+15.4 to 60.7+13.1%, p<0.001). Persistence of cardiac HHV-6 genomes was significantly associated with cardiac dysfunction, and hemodynamic parameters improved in association with HHV-6 clearance.
Chromosomally Integrated Human Herpesvirus 6 in Heart Failure- Prevalence and Treatment (Kühl et al., manuscript submitted) Intriguingly, HHV-6 is able to integrate its genomes into telomeres of human chromosomes, which allows transmission of HHV-6 via the germ line.6, 7 Chromosomally integrated HHV-6 (ciHHV-6) is present in approximately 0.2% of the Japanese and 0.85% of the UK and US populations, respectively and increases up to 3.3% in hospitalized patients. HHV-6A represents 1/3 of ciHHV6 cases, compared to only 1-3% of reactivation cases in transplant reactivations. The effects of ciHHV-6 on the health and development of the patients remain unknown. Since ciHHV-6 genomic integration affects every nucleated cell, and mRNA is detectable in the peripheral blood of these patients, we investigated the prevalence, germ line transmission and reactivation in ciHHV6 patients with persisting unexplained heart failure. We identified 19 patients that were presumed to be ciHHV6 due to high copy numbers above 105 copies/µg isolated DNA that persisted in both cardiac tissue and PBMC.11 The viral loads did not decrease in follow-up studies over years, as would be expected for ciHHV-6 patients. Sequencing confirmed that seven patients (36·8%) had ciHHV-6A and 12 (63·2%) ciHHV-6B. Of the 19 ciHHV6 patients, 14 had mRNA transcripts, and 12 had viral transcripts above 105 copies/ug RNA. At the first onset of symptomatic heart disease, 18 out of the 19 adult ciHHV-6 patients (94·7%) clinically
PAGE 14 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) presented as myocarditis. Inheritance of ciHHV6 would mean that other family members also harbour ciHHV-6 virus. We analyzed blood samples of first degree relatives of three index patients. Persisting HHV-6 copy numbers above 105 DNA copies/µg indicative of ciHHV-6 were detected in several family members as depicted in the pedigrees of the three families (figure 9).
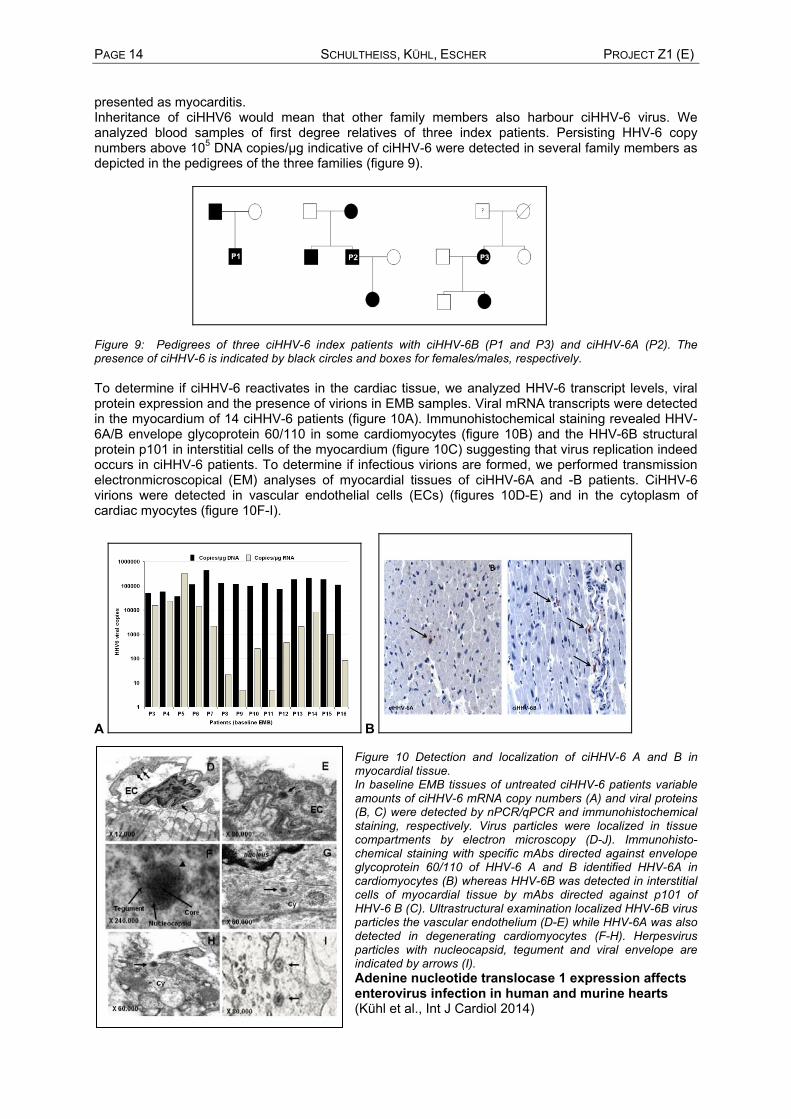
Figure 9: Pedigrees of three ciHHV-6 index patients with ciHHV-6B (P1 and P3) and ciHHV-6A (P2). The presence of ciHHV-6 is indicated by black circles and boxes for females/males, respectively. To determine if ciHHV-6 reactivates in the cardiac tissue, we analyzed HHV-6 transcript levels, viral protein expression and the presence of virions in EMB samples. Viral mRNA transcripts were detected in the myocardium of 14 ciHHV-6 patients (figure 10A). Immunohistochemical staining revealed HHV-6A/B envelope glycoprotein 60/110 in some cardiomyocytes (figure 10B) and the HHV-6B structural protein p101 in interstitial cells of the myocardium (figure 10C) suggesting that virus replication indeed occurs in ciHHV-6 patients. To determine if infectious virions are formed, we performed transmission electronmicroscopical (EM) analyses of myocardial tissues of ciHHV-6A and -B patients. CiHHV-6 virions were detected in vascular endothelial cells (ECs) (figures 10D-E) and in the cytoplasm of cardiac myocytes (figure 10F-I).
A B Figure 10 Detection and localization of ciHHV-6 A and B in myocardial tissue. In baseline EMB tissues of untreated ciHHV-6 patients variable amounts of ciHHV-6 mRNA copy numbers (A) and viral proteins (B, C) were detected by nPCR/qPCR and immunohistochemical staining, respectively. Virus particles were localized in tissue compartments by electron microscopy (D-J). Immunohisto-chemical staining with specific mAbs directed against envelope glycoprotein 60/110 of HHV-6 A and B identified HHV-6A in cardiomyocytes (B) whereas HHV-6B was detected in interstitial cells of myocardial tissue by mAbs directed against p101 of HHV-6 B (C). Ultrastructural examination localized HHV-6B virus particles the vascular endothelium (D-E) while HHV-6A was also detected in degenerating cardiomyocytes (F-H). Herpesvirus particles with nucleocapsid, tegument and viral envelope are indicated by arrows (I). Adenine nucleotide translocase 1 expression affects enterovirus infection in human and murine hearts (Kühl et al., Int J Cardiol 2014)

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 15 The adenine nucleotide translocase 1 (ANT1), the most abundant mitochondrial protein, facilitates mitochondrial energy transfer and modulates mitochondrion-related cell death. Several viruses target ANT or ANT binding partners to manipulate apoptosis for their own purposes. We previously found a shift towards an elevated ANT1 transcription especially in hearts of enterovirus (EV)-infected patients with clinically suspected myocarditis . In addition, increased myocardial ANT protein is link to this shift and has been detected in patients with DCM. In a cooperation with the SFB project C7 (A. Dörner) we tested whether the ANT1 expression is significant for EV infection and its prognosis and analyzed this linkage in EV-infected human and murine hearts.12
Thirteen patients with clinically suspected myocarditis, who showed EV persistence or spontaneous EV elimination, were analyzed for its myocardial transcription pattern by microarray analysis (Human Genome U133 Plus 2.0 GeneChip Array). Six EV negative patients with dilated or inflammatory cardiomyopathy served as control patients. Four controls were persons, whose examination led to exclusion of cardiac dysfunction, infection, inflammation, or structural cardiac disease. We additionally analyzed the ANT1 mRNA proportion by the PCR technique described in of 17 patients diagnosed as having DCM whose biopsies were EV-positive but no follow-up biopsies were available. Compared to controls and EVnegative patients with cardiomyopathy, EV positive patients with EV elimination showed a reduced ANT1 mRNA level, whereas an increased amount of ANT1 mRNA was linked to myocardial EV persistence (set 1). Thus, ANT1 is part of a gene program of components that is inversely expressed in patients who performed virus elimination and those with virus persistence. Compared to the uninfected controls, 14 of the 17 EVpositive DCM patients (set 2) showed an increased ANT1 mRNA proportion, further confirming the association between increased ANT1 expression and chronic heart disease based on EV infection (figure 11 (A/B).
Figure 11: Changes of the ANT1 mRNA levels in patients with enterovirus persistence and clearance in set 1 (A) and set 2 (B). Using the murine animal models of acute and chronic CVB3-induced viral myocarditis (VM) that are well known to reflect the conditions of human VM, we additionally verified that ANT1 expression is related to myocardial virus elimination or persistence. CVB3-infected C57BL/6 mice, which developed acute VM, healed and eliminated CVB3, revealed reduced myocardial ANT protein level during the acute phase of MC 8 days post infection. In contrast, ANT-specific protein was increased early in acute VM in CVB3-infected SWR/J mice shown to develop chronic VM and virus persistence. ANT remained elevated in these mice during chronic VM and virus persistence (figure 12 A/B). Thus, the same virus induced opposing ANT1 expression in different mouse strains, showing that altered ANT expression depends on the genetic/immunological background of the host(Figure 12).

PAGE 16 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E)
Figure 12: Changes of the ANT1 mRNA levels in mice which clear the enteroviral infection spontaneously (A) or develope enterovirus persistence (B)
We additionally tested the significance of elevated ANT1 for CVB3 infection in transgenic heart-specific ANT1 C57/BL6 mice. ANT1 over expression prevented the decrease in ANT1 expression during CVB3 infection and led to an elevation in replicating CVB3. We also found that ANT1 overexpression influenced the expression of genes like OxPhos subunits, actin, myosin, and tropomysin, and compensated, at least in part, for their decline during CVB3 infection. Thus, ANT1 controls a gene program that support viral replication. The data show that ANT1 overexpression results in up-regulation of co-regulated genes and increased the myocardial CVB3 titer, making ANT1 a regulator of a gene program that supports EV infection. Increased expression of ANT1 and its co-regulated genes is related to immunological processes, which degrades the activation of CD8+ lymphocytes. That is linked to virus persistence in human and murine EV-infected hearts, a condition with adverse prognosis. Spontaneous course of viral cardiomyopathy (Kühl et al., Circulation 2005, Kühl et al., JACC 2013)
If the antiviral immunity has elaborated fast and efficiently with subsequent rapid resolution of cellular processes, residual damage of the myocardium may be minor and the remaining myocardium can compensate sufficiently for the partial loss of contractile tissue. Depending on the severity of initial cardiac damage, other patients may retain residual myocardial impairment. Consequently, 60 to 70% of patients recover completely within 2 to 12 months with no or only minor residual clinical signs of heart injury. The clinical importance of persistent enteroviral genomes in the myocardium was investigated by Why and colleagues who demonstrated a higher mortality at 25 months (25% versus 4%) in the 41 patients with persistent enteroviral infection. Caforio and co-workers reported on a 2 year follow-up of patients with active (n=85) and borderline myocarditis (n=89) in which virus persistence was an univariate predictor of adverse prognosis, in addition to anti-heart autoantibodies and clinical signs or symptoms of left and right heart failure.
Figure 13 Spontaneous course if viral cardiomyopathy

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 17 These data are in accordance with our observations. When we initially followed 172 consecutive patients with left ventricular dysfunction and biopsy-proven viral infection by reanalysis of biopsies and hemodynamic measurements after a median period of 7 months, viral genomes persisted in 64% of patients with single virus infections (figure 13).9 50% of the enteroviral genomes were cleared spontaneously. Respective data for adenovirus, parvovirus B19 and herpesvirus 6 were 36%, 22% and 44%. These data on spontaneous clearance of the virus infection demonstrate that a single biopsy analysis can never prove virus persistence unambiguously.
Spontaneous clearance of the viruses was associated with a significant decrease in left ventricular dimensions and improvement in left ventricular ejection fraction. In contrast, LV function decreased mildly during this short follow-up in patients with persisting viral genomes. About five years later, 41% of the patients with enterovirus persistence had died (10 year mortality rate: 52.5%), whereas 92% of patients who spontaneously had cleared the infection where still alive after 10 years (figure 14). A similar course is found in patients with ADV infection.13
Figure 14 Interferon-β treatment significantly improves 10-years-survival of patients with entero-viral cardiomyopathy
Proof of disease-related gene mutations for cardiomyopathies
Current guidelines recommend genetic screening (evidence level A) for ARVD/C, HCM and DCM with conduction abnormalities or extra cardiac manifestations. Although for many cardiomyopathies a genetic predisposition is shown, the genetic analysis is costly and time consuming yet therapeutically relevant for only a few diseases.14-16 Next generation sequencing (NGS) technologies will enable each lab to perform genetic testing for a low price but the interpretation of genetic data is still requesting great expertise. Now NGS is entering the diagnostic level. Advantage of de novo sequencing of all cardiac genes is the identification of temporary unknown mutations in patients with expressed heart failure problems.14
Nevertheless recent studies identified a massive overrepresentation of previously described cardiomyopathy-related genetic variants in a healthy control cohort with genotype prevalence thousand fold higher than in diseased patients.16 This finding makes genetic testing without prior clinic-diagnostically definition questionable. Only an endomyocardial biopsy supported genetic study could identify genetic markers which are associated with occurrence of genetic cardiomyopathies excluding myocardial inflammation or microbial infections as reason for preceding heart muscle disease. 17
CCR5del32 polymorphism is a protective factor in non-ischemic cardiomyopathy
(Lassner et al., Int J Cardiol 2014)
A 32-basepair deletion (del32) in the CC chemokine receptor 5 (CCR5, RANTES) gene leads to deficiency of this receptor for various proinflammatory cytokines and homozygosity results in reduced susceptibility to HIV infections. This polymorphism is furthermore associated with an improved outcome in diabetes and coronary heart disease.
To gain insight into the long-term effect of the CCR5 genotype in patients with clinically suspected

PAGE 18 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) myocarditis or dilated cardiomyopathy (DCM) we determined its frequency by PCR in 300 consecutive patients (mean [±SD] age, 49.68±13.93 years; 194 men) with reliable information on the all cause six year mortality.18 All patients had previously been examined for the presence of intramyocardial inflammation and cardiotropic viruses by endomyocardial biopsy.
The percentage of the three CCR5 genotypes (wildtype (w/w), heterozygous (w/del32) and homozygous for deletion (del32/del32)) in our patient cohort (79.7/ 19.0/1.3) is comparable with the published frequencies for the German population. Fourteen out of 239 CCR5 wildtype individuals (group 1) had died within a 6-year period. Outcome did not depend on the primary clinical diagnosis of myocarditis (9/177) or DCM (5/62) (p=0.329). In contrast, all group 2 patients with a CCR5del32 polymorphism (w/del32 (n=57) and del32/del32 (n=4)) were alive at the end of the study (Figure 1A). The reduced mortality of patients with a 32-basepair deletion (del32) (p=0.032) of the CCR5 receptor possibly indicates the CCR5del32 polymorphism as a protective factor in patients with acquired cardiomyopathies (figure 15A).
Histologically, the CCR5 genotype did not correlate with a persisting myocardial inflammation. Moreover, Diabetes was only present in wildtype patients (24/194) but not in patients with impaired CCR5 receptor (0/46) (p=0.001) (figure 15B). Of note, the increased mortality rate for wildtype genotype was not associated with diabetes (p=0.182) as reported earlier for non-cardiac patients. DCM is frequently caused by myocardial infection and post-infectious inflammation in genetically predisposed patients and has a poor prognosis. In our cohort the frequency of cardiotropic viruses such as enteroviruses (EV), human herpesviruses 6 (HHV6) or erythroviruses (parvovirus B19V) was not significantly different between group 1 and 2 (EV: 12.2%, vs 9.4%; (p=0.568), B19V: 33.3%, vs 18.7%, (p=0.076) or HHV6: 20.1% vs 15.1%, (p=0.408), respectively). Furthermore, there was no correlation between myocardial infection by enterovirus, HHV6 or erythrovirus with the 6-year-mortality (EV: p=0.514; HHV6: p=0.818; B19V: p=0.510, respectively).
Figure 15: A. CCR5del32 polymorphism is associated with a higher survival rate in patients with acquired cardiomyopathies. (A) The overall mortality in our patient cohort (n=300) was 4.7 %. Survival curves were generated according to the Kaplan-Meier method and were compared with the log-rank statistic. No patient with a 32-basepair deletion of the CCR5 receptor (mutated) died during a 6-year-period (p=0.032). The average period of follow-up from biopsy-based diagnosis was 42±33 months (mean [±SD]). Inserted table presents number of patient at risk in 18-months’ intervals. (B) In comparison to patients with complete receptor gene, no patient with a CCR5del32 polymorphism had diabetes
Our data show, for the first time, that CCR5del32 polymorphism is an independent genetic factor that influences outcome in patients with clinically suspected myocarditis and DCM, not associated with myocardial inflammation, diabetes or viral infections. The underlying pathomechanism of the RANTES receptor polymorphism on distinct outcome in heart muscle diseases is currently unknown and requires further investigations.
Profiling technologies for miRNAs or gene expression – the way to organ-specific and systemic diagnosis Novel biomarkers (microRNA, gene expression profiles) in myocardial tissue, peripheral blood or serum and plasma will improve diagnosis of specific entities by overcoming biopsy-based sample error using non-focal expression pattern in next future.4, 17, 19 They could be used for primary diagnosis and for therapy monitoring changing their profiles during therapy indicating the change of molecular marker on focal or systemic level (figure 16)

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 19
Figure 16: Flowchart of routine diagnostic procedure for detection of cardiotropic viruses (A) and future application of novel biomarker (B) for detection of viral infections, inflammatory diseases or genetic variants predicting development of cardiomyopathies.17
Positive diagnostic findings in examined biopsies are confirming the myocardial condition, but negative results will not exclude infections or intramyocardial inflammation. Increasing number of biopsies will reduce biopsy-depending sampling error, but could never overcome it completely. This fact is indicating the need of global and stable biomarkers to identify disease entities in the effected organ preventing and overcoming sampling error (figure 17).
Figure 17: Biopsy-independent novel biomarkers for reduction of sampling error at a limited number of biopsies.17
First investigations indicate that deregulation of myocardial gene expression is not limited to focal biopsy area, and therefore allows the identification of specific disease situations of the examined patient analyzing neighbouring biopsies.20 It becomes difficult to diagnose complex diseases by one parameter. Current diagnostic biomarker panels are consisting of a few deregulated genes. Viral infections or massive infiltration of inflammatory cells in myocardium could be diagnosed in neighbouring tissue samples without histological confirmation of these agents. We identified a gene pattern differentiating virally-induced or inflammatory cardiomyopathies like active myocarditis or giant cell myocarditis from inflammation-free or non-infected myocardium. Such disease specific profiles will change during effective treatment and thereby could also be applied for therapy monitoring. MicroRNAs (miRNAs) are small non-coding regulatory molecules (17-24nt) and were recently identified as important regulators of genetic expression in myocardial tissue. They modulate gene expression by enhanced degradation of protein-coding mRNAs or sequestration from the translational apparatus. The role of miRNAs in physiologic and pathologic processes and the capability to correlate expression changes with disease states highlights their value as novel molecular biomarkers. Currently available miRNA profiles allow the identification of preceding cardiotropic infection even in PCR-negative biopsies. The clinical course of such patients become predictable at the point of primary biopsy and a disease-directed therapy may be initiated immediately to prevent myocardial injuries.19, 21 miRNAs have been demonstrated to play crucial roles in the etiology of a variety of common human diseases. They are involved in intra- and intercellular communication. miRNAs were detected not only in human tissue but also in serum or plasma influencing systemic response on organ-specific
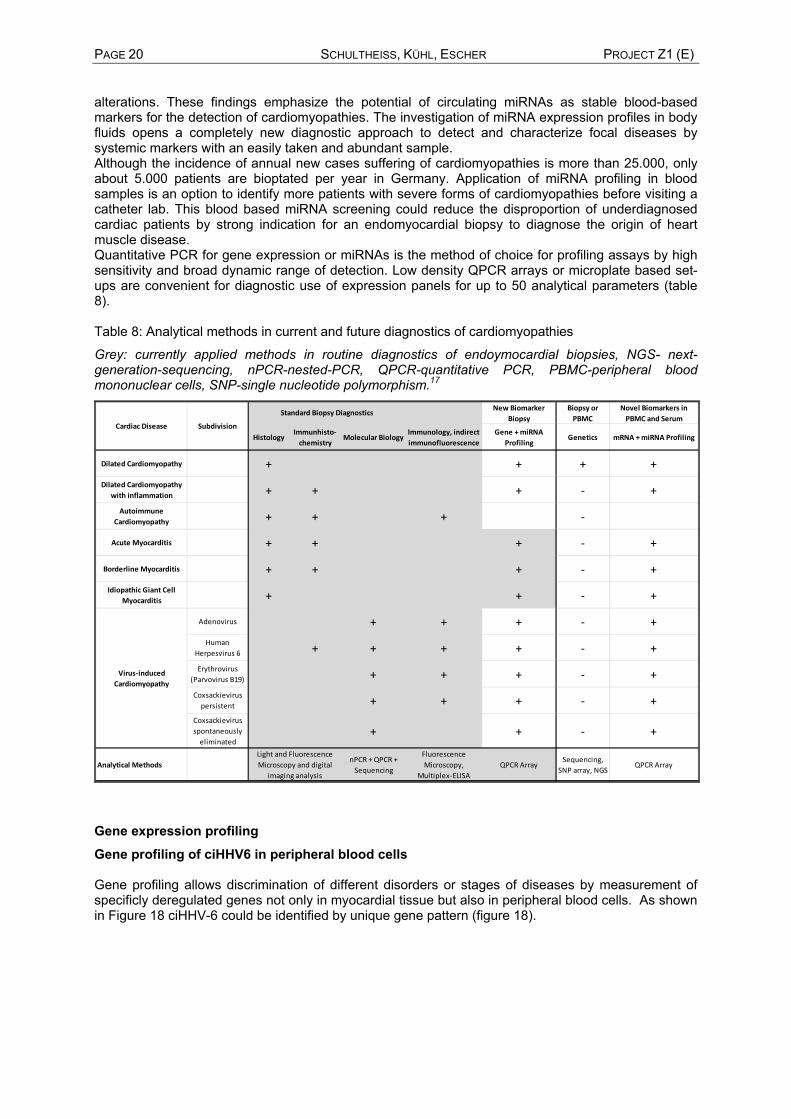
PAGE 20 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) alterations. These findings emphasize the potential of circulating miRNAs as stable blood-based markers for the detection of cardiomyopathies. The investigation of miRNA expression profiles in body fluids opens a completely new diagnostic approach to detect and characterize focal diseases by systemic markers with an easily taken and abundant sample. Although the incidence of annual new cases suffering of cardiomyopathies is more than 25.000, only about 5.000 patients are bioptated per year in Germany. Application of miRNA profiling in blood samples is an option to identify more patients with severe forms of cardiomyopathies before visiting a catheter lab. This blood based miRNA screening could reduce the disproportion of underdiagnosed cardiac patients by strong indication for an endomyocardial biopsy to diagnose the origin of heart muscle disease. Quantitative PCR for gene expression or miRNAs is the method of choice for profiling assays by high sensitivity and broad dynamic range of detection. Low density QPCR arrays or microplate based set-ups are convenient for diagnostic use of expression panels for up to 50 analytical parameters (table 8). Table 8: Analytical methods in current and future diagnostics of cardiomyopathies
Grey: currently applied methods in routine diagnostics of endoymocardial biopsies, NGS- next-generation-sequencing, nPCR-nested-PCR, QPCR-quantitative PCR, PBMC-peripheral blood mononuclear cells, SNP-single nucleotide polymorphism.17
New Biomarker Biopsy
Biopsy or PBMC
Novel Biomarkers in PBMC and Serum
HistologyImmunhisto‐chemistry
Molecular BiologyImmunology, indirect immunofluorescence
Gene + miRNA Profiling
Genetics mRNA + miRNA Profiling
Dilated Cardiomyopathy + +
Dilated Cardiomyopathy with inflammation + + + ‐ +
Autoimmune Cardiomyopathy + + + ‐
Acute Myocarditis + + + ‐ +
Borderline Myocarditis + + + ‐ +
Idiopathic Giant Cell Myocarditis + + ‐ +
Adenovirus + + + ‐ +
Human Herpesvirus 6 + + + + ‐ +
Erythrovirus (Parvovirus B19) + + + ‐ +
Coxsackievirus persistent + + + ‐ +
Coxsackievirus spontaneously eliminated
+ + ‐ +
Analytical MethodsnPCR + QPCR + Sequencing
Fluorescence Microscopy,
Multiplex‐ELISAQPCR Array
Sequencing, SNP array, NGS
QPCR ArrayLight and Fluorescence Microscopy and digital
imaging analysis
Virus‐induced Cardiomyopathy
Cardiac Disease Subdivision
Standard Biopsy Diagnostics
+ +
Gene expression profiling
Gene profiling of ciHHV6 in peripheral blood cells Gene profiling allows discrimination of different disorders or stages of diseases by measurement of specificly deregulated genes not only in myocardial tissue but also in peripheral blood cells. As shown in Figure 18 ciHHV-6 could be identified by unique gene pattern (figure 18).

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 21
Figure 18: Differentially expressed genes in the peripheral blood cells (PBC) of patients with chromo-someally integrated HHV6 (ciHHV6) or patients with virus- and inflammation- free endomyo-cardial biopsies (MCNo).Gene profile suggest ciHHV6 may be a distinct disease subgroup.
Improved diagnosis of idiopathic giant cell myocarditis and cardiac sarcoidosis by myocardial gene expression profiling (Lassner et al., EHJ 2014, Elezkurtaj et al., 2013) Most patients with idiopathic giant cell myocarditis (IGCM) present with acute fulminant heart failure due to rapidly progressive myocyte necrosis. Immunosuppressive therapies, including high-dose steroids and cyclosporine, have only modestly improved the prognosis in IGCM. Morbidity and mortality remain high and many patients still require heart transplantation. IGCM has been reported in association with autoimmune disorders. This supports an autoimmune etiologic role. Nevertheless, autoantigens in IGCM remain poorly defined. To gain insight into the pathogenesis of this mercurial disease, we studied patients with IGCM with regard to histopathological appearances and gene expression pattern of inflammation in endomyocardial biopsies (EMB).20, 22
Figure 19: Cardiac gene expression shifts is associated with presence of giant cells. Genes coding for cellular and toll-like receptors (A), cytokines and chemokines (B) and mitochondrially or genomic coded proteins of energy supply chain (C)
The diagnosis of idiopathic giant-cell myocarditis and its differentiation from cardiac sarcoidosis can be a difficult task because giant cells and ganuloma, although distinct morphology, may be present in both diseases and are often focally distributed within the myocardium. In an attempt to improve the

PAGE 22 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) biopsy-based differential diagnosis and to gain additional insight into the underlying inflammatory process of these frequently fatal diseases we examined the gene expression profiles in endomyo-cardial biopsies of patients with histopathologically proven idiopathic giant-cell myocarditis n=10), cardiac sarcoidosis (n=10), active myocarditis (n=13) and inflammation and virus free controls n=80). The differential expression of 27 genes coding for cellular and toll-like receptors, cytokines, hemokines, and proteins involved in the mitochondrial energy supply chain were analyzed in extracted RNA from endomyocardial biopsies (Figure 19). The obtained expression profiles were significaltly different in the three inflammatory disease entities even in tissue specimens where giant cells or granuloma were missed due to the sampling error. According to the actual data, gene profiling in endomyocardial tissue may allow to diagnose a multinuclear giant cell myocarditis and thus to overcome a non-diagnostic information caused by the focal distribution of the characteristic cells. Furthermore it may allow a better discrimination of IGCM giant-cell myocarditis from cardiac sarcoidosis.20 The diagnostic potential of the above disease-specific gene expression profiles and their potential to influence patient management, which are in urgent need immediate immunosuppressive treatment, has to be further explored prospectively in a larger cohort of patents.
Improvement of diagnosis using cardiac microRNA profiles
Archived patient material (biopsies, blood cells, serum/plasma) of these exactly characterized patients was used for screening on biomarkers (microRNAs, whole genome analysis, autoantibodies, gene profiling) in search of diagnostically and therapeutically applicable parameters. One important focus of this approach was the analysis of potential biomarkers for prediction or monitoring of applied therapies MicroRNA as activity markers in parvovirus B19 associated heart disease (Kühl et al. Herz 2012) Parvovirus B19 is a frequent virus detected in endomyocardial biopsies of patients with clinically suspected myocarditis or dilated cardiomyopathy (DCM). Viruses often cause a more symptomatic disease with increased tissue injury, if they become reactivated. A disease-specific differential expression of micro RNAs (miRNAs) has been described in the regulation of replicating viruses. Analyzing patients with latent and reactivated B19V infection, we found 29 differentially regulated miRNAs and in order to test whether predicted genes are differentially expressed selected mRNAs were tested by TaqMan-QPCR.19
Figure 20 (A) Heatmap of the hierarchical clustering of 75 miRNA expression pattern for latent and active B19V infection showing a good clustering of the two patient groups. (B) Furthermore two examples for differentially regulated miRNAs (Type I and Type II) in these patient groups.
PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 23 Endomyocardial tissue specimens of B19V positive patients who presented as clinically suspected non-acute myocarditis were first screened for the presence of B19V-VP1-VP2 mRNA in order to identify patients with or without transcriptionally active infection. Patients with other cardiotropic viruses, patients with multiple infections, and patients with cardiac diseases other than suspected chronic myocarditis were excluded from further analysis. To exclude an effect of myocardial inflammation on miRNA expression, only patients without any biopsy-based proof of myocardial inflammation according to histological and immunohistological analyses were included in the subsequent miRNA analyses.
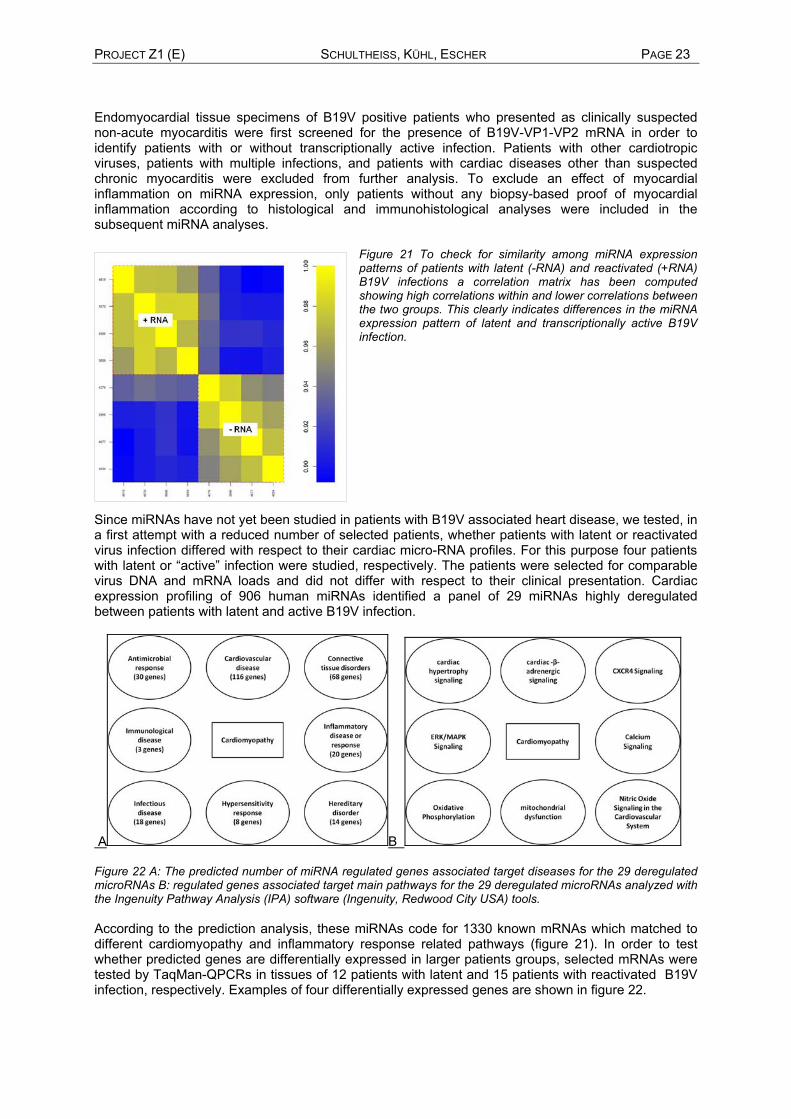
Figure 21 To check for similarity among miRNA expression patterns of patients with latent (-RNA) and reactivated (+RNA) B19V infections a correlation matrix has been computed showing high correlations within and lower correlations between the two groups. This clearly indicates differences in the miRNA expression pattern of latent and transcriptionally active B19V infection.
Since miRNAs have not yet been studied in patients with B19V associated heart disease, we tested, in a first attempt with a reduced number of selected patients, whether patients with latent or reactivated virus infection differed with respect to their cardiac micro-RNA profiles. For this purpose four patients with latent or “active” infection were studied, respectively. The patients were selected for comparable virus DNA and mRNA loads and did not differ with respect to their clinical presentation. Cardiac expression profiling of 906 human miRNAs identified a panel of 29 miRNAs highly deregulated between patients with latent and active B19V infection.
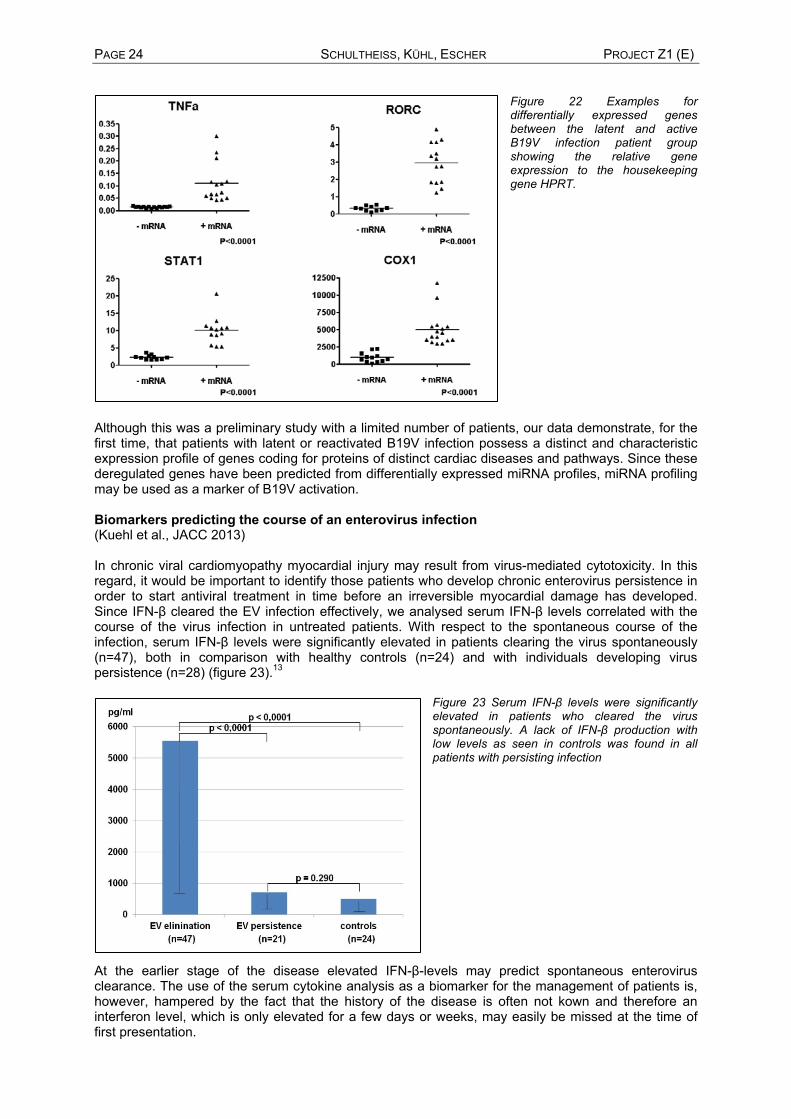
A B Figure 22 A: The predicted number of miRNA regulated genes associated target diseases for the 29 deregulated microRNAs B: regulated genes associated target main pathways for the 29 deregulated microRNAs analyzed with the Ingenuity Pathway Analysis (IPA) software (Ingenuity, Redwood City USA) tools. According to the prediction analysis, these miRNAs code for 1330 known mRNAs which matched to different cardiomyopathy and inflammatory response related pathways (figure 21). In order to test whether predicted genes are differentially expressed in larger patients groups, selected mRNAs were tested by TaqMan-QPCRs in tissues of 12 patients with latent and 15 patients with reactivated B19V infection, respectively. Examples of four differentially expressed genes are shown in figure 22.
PAGE 24 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E)
Figure 22 Examples for differentially expressed genes between the latent and active B19V infection patient group showing the relative gene expression to the housekeeping gene HPRT.
Although this was a preliminary study with a limited number of patients, our data demonstrate, for the first time, that patients with latent or reactivated B19V infection possess a distinct and characteristic expression profile of genes coding for proteins of distinct cardiac diseases and pathways. Since these deregulated genes have been predicted from differentially expressed miRNA profiles, miRNA profiling may be used as a marker of B19V activation. Biomarkers predicting the course of an enterovirus infection (Kuehl et al., JACC 2013) In chronic viral cardiomyopathy myocardial injury may result from virus-mediated cytotoxicity. In this regard, it would be important to identify those patients who develop chronic enterovirus persistence in order to start antiviral treatment in time before an irreversible myocardial damage has developed. Since IFN-β cleared the EV infection effectively, we analysed serum IFN-β levels correlated with the course of the virus infection in untreated patients. With respect to the spontaneous course of the infection, serum IFN-β levels were significantly elevated in patients clearing the virus spontaneously (n=47), both in comparison with healthy controls (n=24) and with individuals developing virus persistence (n=28) (figure 23).13
Figure 23 Serum IFN-β levels were significantly elevated in patients who cleared the virus spontaneously. A lack of IFN-β production with low levels as seen in controls was found in all patients with persisting infection
At the earlier stage of the disease elevated IFN-β-levels may predict spontaneous enterovirus clearance. The use of the serum cytokine analysis as a biomarker for the management of patients is, however, hampered by the fact that the history of the disease is often not kown and therefore an interferon level, which is only elevated for a few days or weeks, may easily be missed at the time of first presentation.

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 25 Differential Cardiac microRNA Expression Predicts the Clinical Course in Human Enterovirus Cardiomyopathy (Cooperation with SFB Project C5) (Kuhl et al., JHJ, manuscript submitted) Test cohort In search for a more reliable and history independent biomarker predicting the course of the EV infection we analyzed a preselected test cohort of patients with biopsy based information on the course of the viral infection. One fraction of the patients was able to eliminate the cardiac virus spontaneously, with resulting recovery of their initially impaired cardiac function, while the others continued to harbour the enterovirus and did not improve clinically.
Figure 24 (A) The long lncRNA MALAT-1 is one of the most significantly elevated transcript in patients who spontaneously clear the EV infection. Together with a small panel of characteristically altered miRNAs (figure 25B), these changes are highly predictive for the spontaneous EV course.
In a genome-wide array-based analysis the expression profiling of protein-coding genes in endomyo-cardial biopsies of patients with coxsackievirus B3 and adenovirus cardiomyopathies performed at initial presentation did not identify major predictive differences in correlation with the spontaneous course of the enteroviral infection. Unexpectedly, and in contrast to previous cardiac expression profiling work using Affymetrix mRNA arrays from our group and others, ncRNAs were the most strongly deregulated and distinctive transcripts, including a lncRNA (Malat-1) conserved during evolution and processed to a peculiar tRNA-like structure of 61 nucleotides length mascRNA (figure 24A, for more details and experimental information on the importance of mascRNA on antiviral defence mechanisms see the report of the cooperating project C5) in EV positive patients. Additional profiling of the cardiac expression levels of 756 human miRNAs by Taqman arrays revealed highly significant differences with distinct miRNA response types (figure 25B).
Figure 25 (A) Patient cohorts used for gene expression and miRNA profiling (B) Differential Cardiac miR Expression Patterns in Human Viral Cardiomyopathies

PAGE 26 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) A series of patients with CVB3 cardiomyopathy with either spontaneous elimination (CVB3-ELIM) or persistence of their cardiotropic virus (CVB3-PERS) were selected for EMB-based transcriptome mapping. These two groups were not significantly different regarding clinical symptoms, hemodynamic, or echocardiographic parameters at initial presentation (left part, redbar). CVB3-ELIM patients had significantly improved symptoms and left ventricular ejection fraction (LVEF) after 6 months (time point of control biopsy) (yellow bar) and normalized hemodynamics after one year (green bar). In contrast, CVB3-PERS patients with CVB3 persistence (right part of panel) had no improvement of symptoms or LVEF after 6 months (yellow bar) and subcutaneous IFN-β therapy was initiated at this time. IFN-β led to clinical and function improvement, still LVEF remained significantly impaired at the end of the 6 months treatment period (red bar). This improvement but lack of normalization emphasizes the need to start treatment as early as possible to prevent irreversible cardiac injury and adverse long-term prognosis due to cardiac persistent CVB3. Primary comparison was CVB3-ELIM vs. CVB3-PERS. In addition, adenoviral (AdV) cardiomyopathy hearts with severely impaired LVEF, and control hearts (CONT) were analyzed. The latter had initially presented with suspected cardiac origin of their complaints, but had exclusion of cardiac pathology at the end of the diagnostic workup.
Validation cohort Initial miRNA profiling in the test cohort revealed highly significant differences in the expression levels of 16 miRNAs (figure 25 B), but not in protein-coding genes, suggesting determination of antiviral capacity by noncoding genomic elements. Further evaluation of this primary distinctive miRNA pattern in a major validation cohort, and multivariate statistical analysis of the miR data set, led to definition of a secondary, significantly simplified predictive miRNA profile suggested for future clinical use. Univariate statistical analysis confirmed high predictive potential for 8 of the miRNAs preselected from the test cohort, all of which were suitable for inclusion in a predictive profile.21
EMBs from the four test patient cohorts underwent miRNA expression profiling addressing 756 human miRNAs. Primary comparison was CVB3-ELIM vs. Cox-PERS. In addition, AdV cardiomyopathy patients and controls without cardiac pathology were analyzed by the same assays. If the four test cohorts are jointly considered, the miRNAs deregulated in CVB3-ELIM vs. CVB3-PERS may be assigned to different "response types" as indicated by red and blue colour, respectively. 8 miRNAs (Panels A-H) show a type I response characterized by strong induction in only one of the test cohorts (CVB3-PERS), whereas in all other groups they are undetectable or very low. These miR-135b-5p, miR-155-5p, miR-190a-5p, miR-422a, miR-489-3p, miR-590-5p, miR-601, and miR-1290 distinguish (** p<0.01) not only CVB3- PERS from CVB3-ELIM, but also from controls and AdV group. Opposite is the behaviour of 8 type II response miRs (Panels I-P) which include let-7a-5p, let-7f-5p, miR-296-5p, miR-339-5p, miR-365a-3p, miR-532-5p, miR-660-5p, and miR-520e. They are undetectable in CVB3-PERS and thus distinguish (** p<0.01) them from CVB3-ELIM. Seven are also expressed in controls and AdV cardiomyopathy hearts, distinguishing CVB3-PERS from all other groups. Type II miR-520e differs since it is strongly induced in CVB3-ELIM and AdV hearts, but not detectable in normal hearts.
Our findings have implications for clinical practice, by defining a predictive expression set of ncRNAs and miRNAs which allows assessment of the likelihood of cardiac virus elimination from a CoxB3-infected patient, based on a single EMB sample taken during the initial diagnostic workup. At this time, already a simple ncRNA profile allowed unequivocal distinction of patients who later spontaneously eliminated the virus with clinical recovery, from those unable to eliminate it within 6 months and remaining clinically impaired. After that delay, IFN-β therapy was initiated in this group as reported and virus elimination achieved in all cases, as documented by follow-up biopsies, associated with clinical improvement but no complete recovery.23
An immediate clinical aspect and translational perspective of these data are the use of cardiac miR profiling to assess the likelihood of virus persistence and progressive clinical deterioration in enterovirus cardiomyopathy patients. Patients at risk are eligible for immediate antiviral interferon-β therapy to minimize irreversible cardiac damage. A basic science aspect is the observation that conventional expression profiling of protein-encoding genes failed to identify a significant predictor, suggesting that individual antiviral capacity is rather determined or reflected at the level of noncoding genomic elements. In the future, further analysis of three primate-specific miRNAs shown to be associated with low antiviral capacity may reveal new therapeutic targets to address in human viral diseases.

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 27 Biopsy-based treatment decisions Since a significant proportion of acute myocardial diseases heals spontaneously and associated arrhythmias and LV dysfunction may resolve completely, mechanical circulatory support and implantation of permanent pacemakers or automatic defibrillators (ICD's) should be only used if it is not possible to stabilize the patients by a symptomatic therapy or if patients do not recover of heart failure. These measures are often the only therapeutic option for genetic cardiomyopathies. If patients develop a rapid progressive ventricular dysfunction despite optimal medical treatment, the prognosis can often be improved by rapid and sustained cause-oriented treatment. Therefore biopsy-based information is mandatory in acute heart failure in order to recognize e.g. virus negative inflammation that requires immediate and tailored immunosuppression in order to reduce early mortality and improve long-term outcome. This is particular important in eosinophilic, the necrotic and giant cell myocarditis (GCM) where the treatment should be started immediately after biopsy diagnostics which often respond well to early immunosuppressive treatment while untreated a very high mortality occurs.8, 24-47
Figure 26: Biopsy-based treatment options for DCMi
Over the past decade clinical investigations have revealed at least one therapeutic option for the four most important cardiotropic viruses (adenovirus, enterovirus, erythrovirus, HHV-6) with different grades of efficacy.39, 40, 42, 44, 45, 47-50 In chronic inflammation, virus-negative patients with post-infectious or auto-immune inflammatory processes responded well to immunosuppression or immunoadsorption. Myocardial injury is also occurring under optimal heart failure therapy due to persistence of cardiotropic viruses. Virus-positive patients do not improve or even deteriorate upon anti-inflammatory treatment. For antiviral treatment currently two approaches are existing: immunomodulation supporting intrinsic immune response or antiviral drugs affecting life cycle of corresponding virus. Patients with chronic heart failure due to persistent enterovirus and adenovirus infections of the myocardium responded well to a six months’ interferon-beta (IFN-β) course, but have untreated a really poor prognosis.13, 23 Complete elimination of viral genome was proven by follow-up biopsies taken three month after termination of the antiviral therapy. Virus clearance was paralleled by an improvement of mean left ventricular function, a decrease in ventricular size, an amelioration of heart failure symptoms. The long-term mortality for patients with enterovirus persistence is significantly reduced in comparison with spontaneous elimination or after ß-Interferon treatment (Fig.8).13

PAGE 28 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Treatment of patients with viral cardiomyopathy
Long-term outcome of interferon-β treated patients with enterovirus infection (Kühl et al. JACC 2013).
Enteroviruses (90% Coxsackievirus B3) are detected up to 12% of analyzed tissues patients presenting with DCM (information from BICC cohort). We previously demonstrated a six-months’ treatment course with interferon-β (IFN-β) to effectively clear the virus from the heart of all treated patients with chronic enteroviral cardiomyopathy and to improve medical conditions significantly.23 In the short run, spontaneous and treatment induced virus clearance was associated with clinical and hemodynamic improvement not observed in patients with persisting infection.10 To gain insight into the long-term effects of IFN-β treatment, we followed the patients from first diagnostic biopsy up to 120 months and compared the outcome of treated and untreated enterovirus infections.13
Figure 27: 10 years mortality rate in enterovirus-positive patients (unadjusted survival according to virus analysis at follow-up). Spontaneous or drug-induced entero-virus clearance was associated with a significantly reduced mortality rate in comparison to patients with enterovirus persistence (p = 0.0005 by the log-rank test).
Patients with persisting virus infection had significantly lower left ventricular ejection fraction (LV-EF) than patients who had cleared the virus from their myocardium (p=0.003). Patients with spontaneous EV elimination confirmed by follow-up biopsy were significantly less likely to die during a mean follow-up of 91±37 months than were patients with virus persistence (mean follow-up: 84.4±45 months). Upon IFN-β treatment all 28 patients had cleared the enteroviral infection from the myocardium. In the long-term survival analysis (mean follow-up: 95.8±36 months), outcome of treated patients was considerably improved. As shown in Figure xa, the mortality rate was low in patients who spontaneously cleared their cardiac viral infection, whereas 52.5% of patients with biopsy-proven enterovirus persistence met the endpoint of death. At five years, 92% of patients who had cleared the virus (n=47, 29 male, mean age 47±15, EF 53±16) were alive, in contrast to only 69% of those with virus persistence (n=21, 17 male, mean age 55±14, EF 39±18) determined by follow-up biopsy. Remarkably, all IFN-β-treated patients (n=28, 16 male, mean age 48±11, EF 56±17) who had cleared the virus in each case were alive at the end of study. These data show for the first time that in the long run EV persistence is associated with and impaired prognosis while IFN-β treatment induced EV elimination from the myocardium improves long-term outcome of patients with EV cardiomyopathy.13
Interferon-β 1a treatment of patients with adenovirus-associated cardiomyopathy (Kühl et al., Circulation 2003)
While coxsackievirus involvement is well established in myocarditis of children and adults with “idio-pathic” heart failure, adenovirus-infection has less frequently been reported in the myocardium of adults. Despite symptomatic heart failure therapy, persisting adenovirus infection of the myocardium is often associated with symptoms of heart failure and a lack of clinical improvement. The nine studied patients had not improved clinically during the documented 37.5±28.4 months pre-treatment period.23
Figure 28 Hemodynamic improvement of ADV-positive patients upon interferon-β treatment

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 29 Complete elimination of adenoviral genome in all treated patients was proven by follow-up biopsies taken three month after termination of the antiviral therapy (table 9). Virus clearance was paralleled by an improvement of mean left ventricular function (figure 28), a decrease in ventricular size, an amelioration of heart failure symptoms and a mild decrease of infiltrating inflammatory cells. Heart failure symptoms (NYHA) improved by one class in 6 patients (67%) who presented as DCM. Symptomatic improvement was associated be a decrease CD3-positive inflammatory cells (7.2±8.9 vs. 3.8±5.2 cells/mm2, p=0.88) while the number of infiltrating lymphocytes did not change in the three patients with unchanged heart failure symptoms (5.5±2.5 vs. 6.0±2.4 cells/mm2, p=0.28). Heart failure symptoms did not change in the group of 3 patients (all NYHA II) with chronic heart failure presenting with an LV-EF above 60%.
Table 9: Molecular biological and immunohistochemical changes of IFN-β treated ADV positive cardiomyopathy
Biopsy Baseline Follow-up p
Molecular biology (nPCR)
Adenoviral DNA-positive 9 0 <0.01
Histology
myocarditis/borderline myocarditis 0 0 ns
Immunohistology
CD3+ lymphocytes (cells/mm2) 6.6 ± 7.2 4.5 ± 4.4 0.35
CD4+ lymphocytes (cells/mm2) 3.8 ± 3.4 1.5 ± 1.2 0.12
CD8+ lymphocytes (cells/mm2) 3.1 ± 3.6 1.6 ± 2.0 0.17
CD45R0+ lymphocytes (cells/mm2) 3.6 ± 2.4 1.9 ± 1.3 0.04
27E10+ activated macrophages (cells/mm2) 3.7 ± 2.9 2.4 ± 1.3 0.13
Despite the small number of currently IFN-β-treated adenovirus-positive heart patients the data suggest that, similar to chronic enteroviral heart disease, adenoviral infection of the myocardium is cleared by a subcutaneously administered six months’ IFNB therapy. 60% of the patients improved both clinically and hemodynamically, despite a long disease history.
Interferon-β treatment of patients with erythrovirus infection/reactivation (Schmidt-Lucke et al., JID 2010) In contrast to enterovirus and adenovirus infections, IFN-β does not clear erythrovirus genomes from the myocardium. According to the first pilot studies virus load is reduced and clinical symptoms improve in about 30 to 35% of treated patients. These data were confirmed by a randomized, placebo controlled multicenter study, which primarily included erythrovirus positive patients, by demonstrating a significant virus load reduction (p=0.048) and clinical improvement (p=0.028) although erythrovirus genomes were still detectable in the control biopsy after treatment. At the time of these studies neither the frequency of two distinct erythovirus subtypes nor the presence of transcriptionally active erythrovirus infection wer known and thus could not been taken into consideration for the analyses of the studies. Our current data suggest that during spontaneous re-silencing of the erythrovirus mRNA the IFN-β response induced by transcriptionally active B19V infection suffices to suppress viral transcriptional activity with consecutive improvement of endothelial function (see figure 4), but that the response rate is not sufficient to induce a coordinated adaptive immune response leading to definitive virus elimination. The same may hold true for IFN-β therapy. Recently we could show that symptomatic endothelial dysfunction improves upon antiviral treatment with interferon-beta (IFN-β) despite incomplete virus clearance.48 Since IFN-β is capable of inhibiting B19V-replication in infected human endothelial cells, we hypothesized that clinical improvement of treated patients is due to drug effects on virus replication or transcriptional activity, rather than on virus clearance. To test this hypothesis, a

PAGE 30 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) first pilot trial with symptomatic B19V-positive patients was initiated (figure 29).
Figure 29 Improvement of endothelial dysfunction upon IFN-β treatment in B19V-positive patients
We could show that symptomatic B19V-associated endothelial dysfunction improves upon IFN-β treatment, despite incomplete virus clearance.48 IFN-β also improved the viability and replication of infected human endothelial cells and suppresses B19V replication in infected human endothelial cells (for
further details see collaboration with SFB project B7, Schmidt-Lucke). Treatment of B19V-reactivation with the nucleoside analogon (Kühl et al., manuscript submitted) Transcriptionally active erythrovirus (B19V) is frequently associated with endothelial dysfunction and persisting symptomatic heart failure (table 6). Antiviral treatment with IFN-β improves symptoms and endothelial function in a subgroup of patients despite incomplete virus clearance (figure 29). Since telbivudine modulates the innate and adaptive immune system through IFN-like functions in addition to its antiviral potential in B19V-infected endothelial cells (Bock, SFB project B5), we tested whether this nucleotide analogue effects clinical outcome of patients with reactivated B19V infection and persisting symptomatic heart failure. 17 patients (13 male) with persisting symptoms of heart failure and biopsy-proven transcriptional active B19V infection were treated with 600 mg p.o. of telbivudine for 6 months. Viral loads, B19V transcripts and inflammatory cell counts were analyzed in baseline and follow-up biopsies using quantitative real time PCR and immunohistochemical cell counts. After treatment biopsy B19V-transcriptional activity was silenced or considerably reduced in 16 out of 17 patients (figure 30). Median viral transcripts declined from 431 to 92 genome equivalents (GE)/µg isolated nucleic acids (p<0.05) with consecutive reduction of B19V DNA loads from 1898 to 539 copies (p<0.05). Patients under treatment reported rapid improvement of angina and physical disability within the first weeks of treatment (p=0.007). After treatment NYHA classification (p=0.004), quality-of-life scores (p=0.001), and 6-min-walking distance (p<0.0001) had improved significantly. Left ventricular ejection fraction increased from 49% to 57% (p<0.0001). A subgroup of patients with symptomatic transcriptionally active B19V-infection improves clinically upon telbivudine treatment paving the way for a randomized controlled clinical study.
Figure 30: Clinical course upon telbivudine treatment of patients with
transcriptionally active B19V infection.
The telbivudine treatment trial is the first approach of an antiviral treatment strategy of symptomatic chronic myocarditis associated with reactivated B19V-infection. The mechanism of interaction of telbivudine with the complex B19V replication system needs further detailed dissection. However, the data of this pilot trial demonstrate the potential clinical benefit of the antiviral treatment of B19V-infection in chronic myocarditis with respect to improved quality-of-life for the concerned patients.

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 31 Suppression of HHV6 replication and viral RNA synthesis by antiviral therapy (Kühl et al., manuscript submitted) HHV-6 is the second frequent virus and detectable in over 14% of biopsies from analysed patients (table 5) with low viral loads and the clinical relevance with respect to the pathogenesis of cardiomyopathies is still uncertain. In about 1% of all EMBs HHV6 could be detected with persistent high viral loads (over 50.000 copies per µg myocardial DNA) characteristic for chromosomally integrated HHV-6 (ciHHV-6) (table 5). Chromosomal integration and permanent virus reactivation may cause rarely recognized symptomatic diseases including cardiomyopathies. Condition in patients with ciHHV6 is comparable with immunosuppression. Ganciclovir is an effective antiviral drug for treatment of cytomegalovirus (CMV) infections, another member of herpesvirus family, in immunocompromised transplant patients. The life-long infection of HHV6 and ciHHV6 is characterized by permanent generation of virus and resulting in a clinical situation similar to immunosuppression.7, 8 The treatment with Ganciclivir does not influence the load of viral DNA in these patients but it reduces or eliminating the viral RNA thereby hindering a de novo synthesis of virus particles. Upon treatment the general condition improves by overcoming the immunocompromising effect of HHV6. Consequently, ganciclovir should be an effective drug for conventional HHV-6 infections too, but corresponding trials are still missing due to low viral titers in myocardium and few patients identified with HHV-6 myocarditis. If HHV-6 is involved in the clinical symptoms, an improvement should occur under antiviral treatment of ciHHV-6 patients. Response to therapy was determined by EMB diagnostics before and after six months treatment. Six patients with severe persisting symptoms of heart failure were treated with 900mg valganciclovir/day a herpesvirus specific inhibitor of virus replication, for six months. After two weeks of treatment, all six reported a reduction of angina pectoris, dyspnea, fatigue and an improvement of physical capacity. Measurements of HHV-6 mRNA levels in PBMCs revealed that DNA replication and RNA synthesis were eliminated after antiviral therapy (figure 31). The absence of DNA replication was confirmed by fluorescence in situ hybridization (FISH), which detected only the integrated HHV-6 genome in interphase nuclei of the treated patients (figure 32).
Figure 31: A: Ganciclovir treatment of a ciHHV-6 B-positive female patient (P3) with persisting high cardiac and systemic virus loads and cardiac involvement (A). HHV-6 RNA levels are shown as viral copy numbers per 1 µg RNA. A symptomatic increase of mRNA (S) was noted between days 13 to 21 when i.v. ganciclovir was changed to oral administration. During short symptomatic phases (S) at day 41 and 75, again mild increases of mRNA were detected. B Fluorescent in situ hybridization (FISH) analysis detecting the HHV-6 genome (anti-DIG FITC, green) in interphase nuclei (DAPI stain, blue) of lymphocytes from two patients with ciHHV-6A (B) and ciHHV-6B (C) treated with Valganciclovir. In contrast to uninfected (F) JJhan cells (E, F), HHV-6A (D) and HHV6B JJhan infected cells (G) exhibit strong fluorescent signals. Representative images are shown for each patient and the viral genome(s) are highlighted by arrows.
Outcome from ganciclovir treatment Long term follow up of the three patients without prolonged treatment revealed that symptomatic heart failure with impairment of myocardial function that had improved after the six months treatment course reappeared again about one year later. Alternating elevated blood mRNA levels could be detected in these patients. Symptoms improved upon beta-herpesvirus specific antiviral treatment in six treated patients but three of them needed constant treatment to maintain this condition. Discontinuation of treatment resulted in the appearance of both cardiac symptoms and viral mRNA, indicating a direct involvement of HHV-6 in these symptoms.
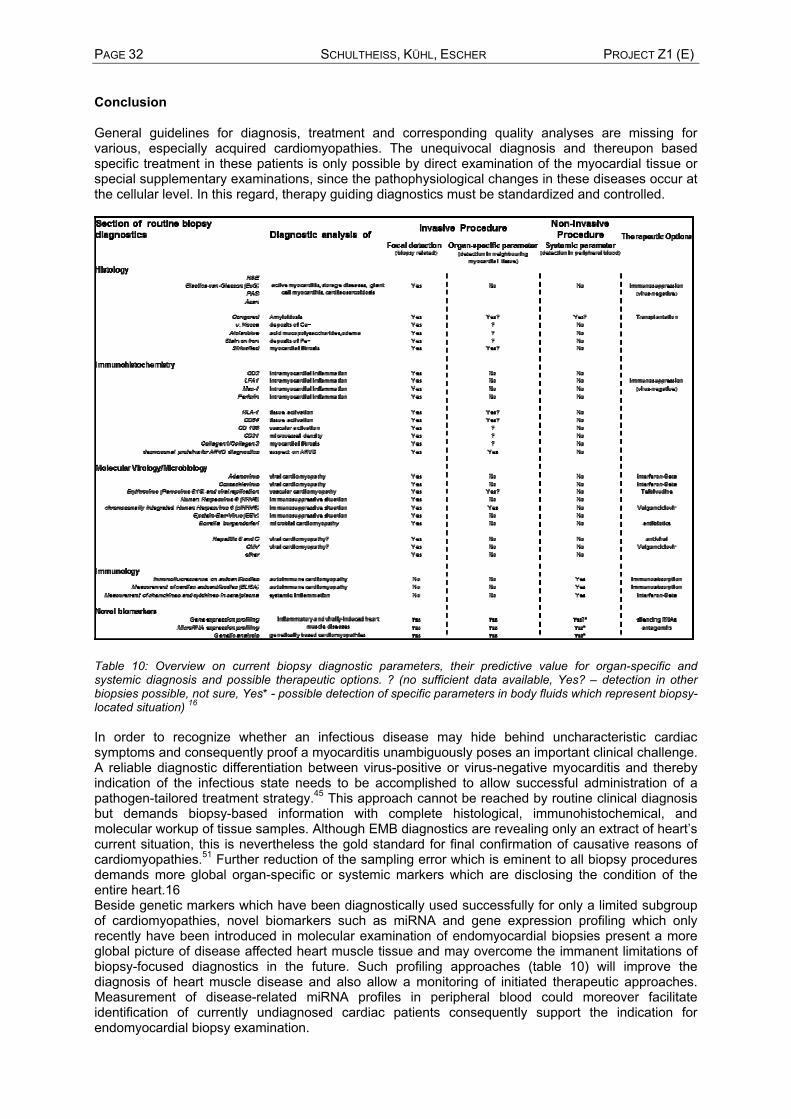
PAGE 32 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) Conclusion
General guidelines for diagnosis, treatment and corresponding quality analyses are missing for various, especially acquired cardiomyopathies. The unequivocal diagnosis and thereupon based specific treatment in these patients is only possible by direct examination of the myocardial tissue or special supplementary examinations, since the pathophysiological changes in these diseases occur at the cellular level. In this regard, therapy guiding diagnostics must be standardized and controlled.
Table 10: Overview on current biopsy diagnostic parameters, their predictive value for organ-specific and systemic diagnosis and possible therapeutic options. ? (no sufficient data available, Yes? – detection in other biopsies possible, not sure, Yes* - possible detection of specific parameters in body fluids which represent biopsy-located situation) 16 In order to recognize whether an infectious disease may hide behind uncharacteristic cardiac symptoms and consequently proof a myocarditis unambiguously poses an important clinical challenge. A reliable diagnostic differentiation between virus-positive or virus-negative myocarditis and thereby indication of the infectious state needs to be accomplished to allow successful administration of a pathogen-tailored treatment strategy.45 This approach cannot be reached by routine clinical diagnosis but demands biopsy-based information with complete histological, immunohistochemical, and molecular workup of tissue samples. Although EMB diagnostics are revealing only an extract of heart’s current situation, this is nevertheless the gold standard for final confirmation of causative reasons of cardiomyopathies.51 Further reduction of the sampling error which is eminent to all biopsy procedures demands more global organ-specific or systemic markers which are disclosing the condition of the entire heart.16 Beside genetic markers which have been diagnostically used successfully for only a limited subgroup of cardiomyopathies, novel biomarkers such as miRNA and gene expression profiling which only recently have been introduced in molecular examination of endomyocardial biopsies present a more global picture of disease affected heart muscle tissue and may overcome the immanent limitations of biopsy-focused diagnostics in the future. Such profiling approaches (table 10) will improve the diagnosis of heart muscle disease and also allow a monitoring of initiated therapeutic approaches. Measurement of disease-related miRNA profiles in peripheral blood could moreover facilitate identification of currently undiagnosed cardiac patients consequently support the indication for endomyocardial biopsy examination.
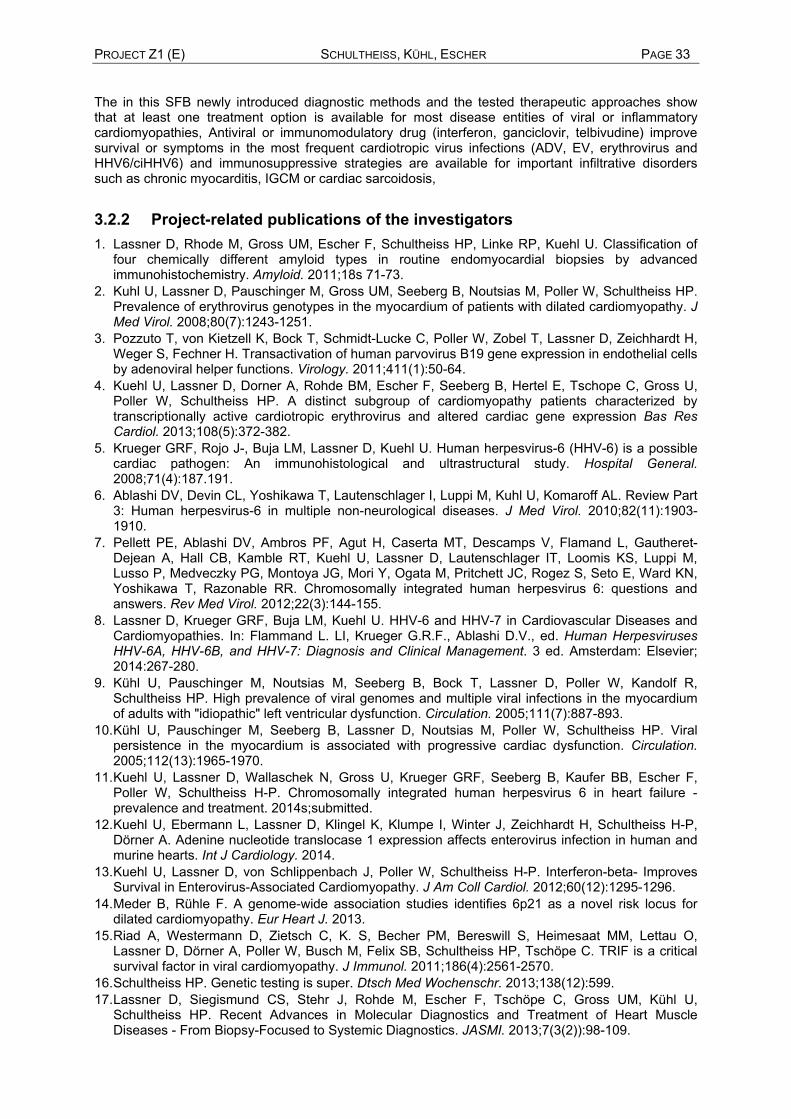
PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 33 The in this SFB newly introduced diagnostic methods and the tested therapeutic approaches show that at least one treatment option is available for most disease entities of viral or inflammatory cardiomyopathies, Antiviral or immunomodulatory drug (interferon, ganciclovir, telbivudine) improve survival or symptoms in the most frequent cardiotropic virus infections (ADV, EV, erythrovirus and HHV6/ciHHV6) and immunosuppressive strategies are available for important infiltrative disorders such as chronic myocarditis, IGCM or cardiac sarcoidosis,
3.2.2 Project-related publications of the investigators 1. Lassner D, Rhode M, Gross UM, Escher F, Schultheiss HP, Linke RP, Kuehl U. Classification of
four chemically different amyloid types in routine endomyocardial biopsies by advanced immunohistochemistry. Amyloid. 2011;18s 71-73.
2. Kuhl U, Lassner D, Pauschinger M, Gross UM, Seeberg B, Noutsias M, Poller W, Schultheiss HP. Prevalence of erythrovirus genotypes in the myocardium of patients with dilated cardiomyopathy. J Med Virol. 2008;80(7):1243-1251.
3. Pozzuto T, von Kietzell K, Bock T, Schmidt-Lucke C, Poller W, Zobel T, Lassner D, Zeichhardt H, Weger S, Fechner H. Transactivation of human parvovirus B19 gene expression in endothelial cells by adenoviral helper functions. Virology. 2011;411(1):50-64.
4. Kuehl U, Lassner D, Dorner A, Rohde BM, Escher F, Seeberg B, Hertel E, Tschope C, Gross U, Poller W, Schultheiss HP. A distinct subgroup of cardiomyopathy patients characterized by transcriptionally active cardiotropic erythrovirus and altered cardiac gene expression Bas Res Cardiol. 2013;108(5):372-382.
5. Krueger GRF, Rojo J-, Buja LM, Lassner D, Kuehl U. Human herpesvirus-6 (HHV-6) is a possible cardiac pathogen: An immunohistological and ultrastructural study. Hospital General. 2008;71(4):187.191.
6. Ablashi DV, Devin CL, Yoshikawa T, Lautenschlager I, Luppi M, Kuhl U, Komaroff AL. Review Part 3: Human herpesvirus-6 in multiple non-neurological diseases. J Med Virol. 2010;82(11):1903-1910.
7. Pellett PE, Ablashi DV, Ambros PF, Agut H, Caserta MT, Descamps V, Flamand L, Gautheret-Dejean A, Hall CB, Kamble RT, Kuehl U, Lassner D, Lautenschlager IT, Loomis KS, Luppi M, Lusso P, Medveczky PG, Montoya JG, Mori Y, Ogata M, Pritchett JC, Rogez S, Seto E, Ward KN, Yoshikawa T, Razonable RR. Chromosomally integrated human herpesvirus 6: questions and answers. Rev Med Virol. 2012;22(3):144-155.
8. Lassner D, Krueger GRF, Buja LM, Kuehl U. HHV-6 and HHV-7 in Cardiovascular Diseases and Cardiomyopathies. In: Flammand L. LI, Krueger G.R.F., Ablashi D.V., ed. Human Herpesviruses HHV-6A, HHV-6B, and HHV-7: Diagnosis and Clinical Management. 3 ed. Amsterdam: Elsevier; 2014:267-280.
9. Kühl U, Pauschinger M, Noutsias M, Seeberg B, Bock T, Lassner D, Poller W, Kandolf R, Schultheiss HP. High prevalence of viral genomes and multiple viral infections in the myocardium of adults with "idiopathic" left ventricular dysfunction. Circulation. 2005;111(7):887-893.
10. Kühl U, Pauschinger M, Seeberg B, Lassner D, Noutsias M, Poller W, Schultheiss HP. Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation. 2005;112(13):1965-1970.
11. Kuehl U, Lassner D, Wallaschek N, Gross U, Krueger GRF, Seeberg B, Kaufer BB, Escher F, Poller W, Schultheiss H-P. Chromosomally integrated human herpesvirus 6 in heart failure - prevalence and treatment. 2014s;submitted.
12. Kuehl U, Ebermann L, Lassner D, Klingel K, Klumpe I, Winter J, Zeichhardt H, Schultheiss H-P, Dörner A. Adenine nucleotide translocase 1 expression affects enterovirus infection in human and murine hearts. Int J Cardiology. 2014.
13. Kuehl U, Lassner D, von Schlippenbach J, Poller W, Schultheiss H-P. Interferon-beta- Improves Survival in Enterovirus-Associated Cardiomyopathy. J Am Coll Cardiol. 2012;60(12):1295-1296.
14. Meder B, Rühle F. A genome-wide association studies identifies 6p21 as a novel risk locus for dilated cardiomyopathy. Eur Heart J. 2013.
15. Riad A, Westermann D, Zietsch C, K. S, Becher PM, Bereswill S, Heimesaat MM, Lettau O, Lassner D, Dörner A, Poller W, Busch M, Felix SB, Schultheiss HP, Tschöpe C. TRIF is a critical survival factor in viral cardiomyopathy. J Immunol. 2011;186(4):2561-2570.
16. Schultheiss HP. Genetic testing is super. Dtsch Med Wochenschr. 2013;138(12):599. 17. Lassner D, Siegismund CS, Stehr J, Rohde M, Escher F, Tschöpe C, Gross UM, Kühl U,
Schultheiss HP. Recent Advances in Molecular Diagnostics and Treatment of Heart Muscle Diseases - From Biopsy-Focused to Systemic Diagnostics. JASMI. 2013;7(3(2)):98-109.

PAGE 34 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E) 18. Lassner D, Kuehl U, Schultheiss H-P. CCR5del32 polymorphism is a protective factor for mortality
in cardiomyopathy Int J Cardiol. 2014:in press. 19. Kuehl U, Rohde M, Lassner D, Gross U, Escher F, Schultheiss H-P. miRNA as activity markers in
Parvo B19 associated heart disease. Herz. 2012;37:637-643. 20. Lassner D, Kuehl U, Siegesmund CS, Rohde BM, Elezkurtaj S, Escher F, Tschope C, Gross U,
Poller W, Schultheiss H-P. Improved Diagnosis of Idiopathic Giant Cell Myocarditis and Cardiac Sarcoidosis by Myocardial Gene Expression Profiling. Eur Heart J. 2014.
21. Kuehl U, Lassner D, Gast M, Stroux A, Rohde BM, Siegesmund CS, Wang X, Escher F, Gross M, Skurk C, Tschope C, Loebel M, Scheibenbogen C, Schultheiss H-P, Poller W. Differential cardiac microRNA expression predicts the clinical course in human enteroviral cardiomyopathy. Eur Heart J. 2014;submitted.
22. Elezkurtaj S, Lassner D, Schultheiss H-P, Escher F. Vaskular involvement in cardiac giant cell Myocarditis: a new pathophysiological aspect. Clin Res Cardiol. 2014;103:161-163.
23. Kühl U, Pauschinger M, Schwimmbeck PL, Seeberg B, Lober C, Noutsias M, Poller W, Schultheiss HP. Interferon-beta treatment eliminates cardiotropic viruses and improves left ventricular function in patients with myocardial persistence of viral genomes and left ventricular dysfunction. Circulation. 2003;107(22):2793-2798.
24. Noutsias M, Pauschinger M, Poller WC, Schultheiss HP, Kuhl U. Immunomodulatory treatment strategies in inflammatory cardiomyopathy: current status and future perspectives. Expert Rev Cardiovasc Ther. 2004;2(1):37-51.
25. Schultheiss HP. Neue Diagnostische und Therapeutische Ansätze bei entzündlichen Kardiomyopathien. Cardiovasc. 2005.
26. Strauer B, Schultheiß HP, Kühl U, Brehm M. Kardiomyopathien. In: Schölmerich J, ed. Medizinische Therapie. Vol Kapitel 13.4. 2 ed: Springer; 2005:1120-1129.
27. Kühl U, Noutsias M, Pauschinger M, Schultheiss H. Kontroversen zur Myokardbiopsie - Differentialindikation bei Myokarditis. Kardiologie up2date; 2006:1-9.
28. Kühl U, Pauschinger M, Poller W, Schultheiss HP. Anti-viral treatment in patients with virus-induced cardiomyopathy. Ernst Schering Res Found Workshop. 2006(55):323-342.
29. Poller W, Fechner H, Kuhl U, Pauschinger M, Schultheiss HP. New therapeutics targets in chronic viral cardiomyopathy. Ernst Schering Res Found Workshop. 2006(55):287-303.
30. Schultheiss HP, Kuhl U. Overview on chronic viral cardiomyopathy/chronic myocarditis. Ernst Schering Res Found Workshop. 2006(55):3-18.
31. Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, Levine GN, Narula J, Starling RC, Towbin J, Virmani R. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation. 2007;116(19):2216-2233.
32. Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kuhl U, Maisch B, McKenna WJ, Monserrat L, Pankuweit S, Rapezzi C, Seferovic P, Tavazzi L, Keren A. The new European definition of cardiomyopathies: which space for muscle dystrophies? reply. Eur Heart J. 2008.
33. Kuehl U. How does viral infection of the heart cause chest pain, arrhythmias, and heart failure? Dialogues in Cardiovascular Medicine. Vol 14; 2009:171-177.
34. Kuhl U, Schultheiss HP. Viral myocarditis: diagnosis, aetiology and management. Drugs. 2009;69(10):1287-1302.
35. Schultheiss HP, Kuehl U. What are the current treatment options for myocarditis? Dialogues in Cardiovascular Medicine Vol Dialogues in Cardiovascular Medicine - Vol 14; 2009:187-193.
36. Schultheiss HP, Kuhl U. [Endomyocardial biopsy in cardiomyopathy: when and why?]. Dtsch Med Wochenschr. 2009;134(15):769-772.
37. Schultheiss HP, Lassner D, Kuehl U. Qualitätsanalysen der Therapie von Herzmuskelerkrankungen. Dtsch Med Wochenschr. 2009;134:9-11.
38. Kuehl U, Schultheiss HP. Myocarditis in Children. In: Towbin J, ed. Heart Failure Clinics. Vol 6. Philadelphia: Elsevier Saunders; 2010:483-496.
39. Schultheiss HP, Kuehl U. Cardiovascular Viral Infections. In: Lennette EH, ed. Lennette's Laboratory Diagnosis of Viral Infections. 4 ed; 2010:304-318.
40. Schultheiss HP, Kuehl U. Drugs and/or Devices in dilated Cardiomyopathy. Heart and Metabolism. 2010;49:1-5.
41. Kuehl U. Myokarditis. Klinikarzt. 2011;40(4):196-201. 42. Kuehl U, Schultheiss HP. Myocarditis in children. Heart Fail Clin. 2011;6(4):483-496, viii-ix.

PROJECT Z1 (E) SCHULTHEISS, KÜHL, ESCHER PAGE 35 43. Kuehl U, Schultheiss HP. Spezifische Therapie der inflammatorischen Kardiomyopathie und viralen
Herzmuskelerkrankung. J Kardiol. 2011;18:16-23. 44. Schultheiss HP, Kuehl U. Why is the diagnosis of myocarditis such a chellange? Exp Rev Anti-
infective Therapy. 2011;9(12):in press. 45. Schultheiss HP, Kuehl U, Cooper LT. The Management of Myocarditis. Eur Heart J. 2011;32:2616-
2665. 46. Kuehl U, P. SH. Myocarditis—early biopsy allows for tailored regenerative treatment. Dtsch Arztebl
Int. 2012;109(20):361-368. 47. Kuehl U, Schultheiss HP. Myocarditis. Deutsches Ärzteblatt. 2012;109(20):361-368. 48. Schmidt-Lucke C, Spillmann F, Bock T, Kuhl U, Van Linthout S, Schultheiss HP, Tschope C.
Interferon Beta Modulates Endothelial Damage in Patients with Cardiac Persistence of Human Parvovirus B19 Infection. J Infect Dis. 2010;201(6):936-945.
49. Schultheiss HP, Kuehl U. Acute Myocarditis. In: Hung-Fat Tse GYL, Andrew Coats, ed. Oxford Desk Reference Cardiology. New York: Oxford University Press; 2011:242-245.
50. Kuehl U. Myocarditis - the causes. Heart & Metabolism. 2014;62:4-9. 51. Caforio AL, Pankuweit S, Arbusti E, Basso C, Gimeno-Blanes J, Felix SB, Fu M, Helio T, Heymans
S, Jahns R, Klingel K, Linhart A, Maisch B, McKenna WJ, Mogensen J, Pinto YM, Ristic A, Schultheiss HP, Seggewiss H, Tavazzi L, Thiene G, Yilmaz A, Charron P, Elliott PM. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Europ Heart J. 2013;34:2636–2648.
3.3 Funding Funding of the project within the Collaborative Research Centre started July 2004. Funding of the project ended December 2013.
3.3.1 Project staff in the ending funding period No. Name,
academic degree, position
Field of research
Department of university or non-
university institution
Commitment in
hours/week
Category
Funded through
:
Available 1 Schultheiss,
Heinz-Peter, Prof. Dr., Project leader
Cardiology Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
12 Charité
2 Kühl, Uwe, Dr. rer. nat., Project leader
Cardiology Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
42 Charité
3 Escher, Felicitas, Dr. med., Project leader
Cardiology Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
12 Charité
Research staff
4 Lassner, Dirk, Dr. rer. nat.
Cardiology IKDT Berlin*) 10 extern
Non-research staff
Requested
Research staff

PAGE 36 SCHULTHEISS, KÜHL, ESCHER PROJECT Z1 (E)
1 Willner, Monika, Study nurse
Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
29.25 (9 months)
Research helper
2 Hertel, Ewa, Study nurse
Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
39 (9 months)
Research helper
3 Sosnowski, Marzena, Technical assistant
Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
39 (4.5 months)
Research helper
Non-research staff
4 Winter, Julia, Doctoral student
Charité Centrum 11 Herz- und Kreislauf- und Gefäßmedizin
24 (4 months)
Doctoral student
*) Institute for Cardiac Diagnostics and Therapies, Berlin Job description of staff (supported through available funds): 1-+ 2 Schultheiss H.-P. and Kühl U. Scientific guidance and coordination of the project; coordination of co-operations with partners within the SFB, data analyses (Kühl); provision of clinical samples, patient management and clinical follow-up (Schultheiss, Kühl), screening and inclusion of patients (Kühl), diagnostic procedures and clinical studies (Kühl), publication of results (Schultheiss, Kühl). 3 Escher F. Inclusion and management of patients, immunohistochemical diagnostics, data analyses, publication of results. 4 Lassner D. Management of sample acquisition, sample preparation and storage, specific immunohistochemical staining procedures Job description of staff (requested): 1-4 Willner M., Hertel E., Sosnowsky M., Winter J., Acquisition of clinical data and indoor patient materials, organization of clinical studies and of outdoor patient follow-up, data base inclusion of clinical data and inquiries at the registration office for mortality statistics.