Embed Size (px)
Citation preview
Diverticular Disease
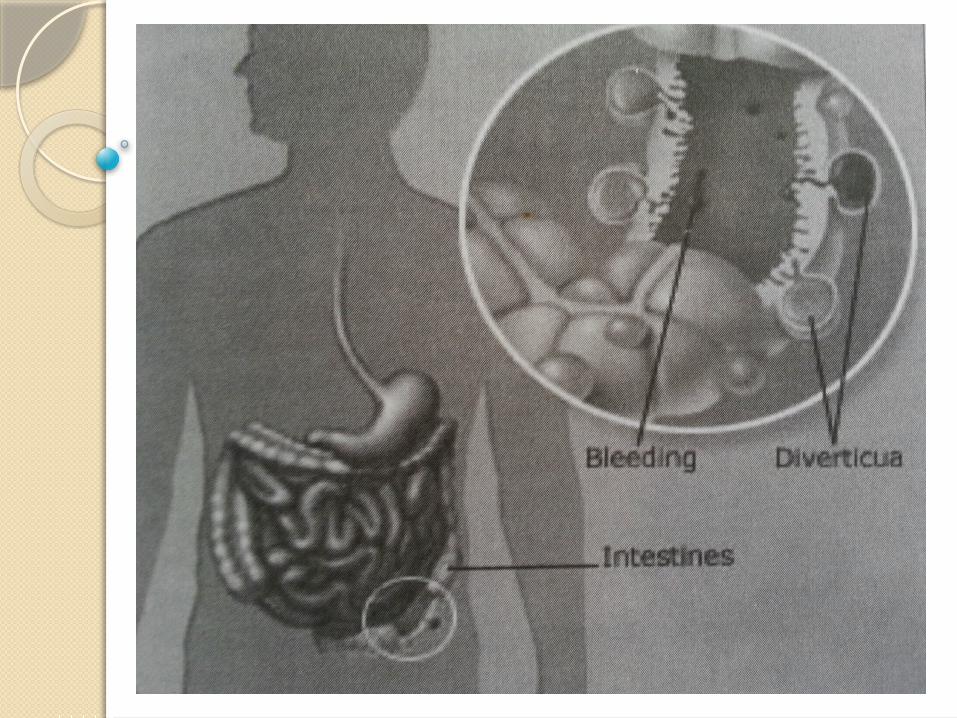
Diverticulum
is a saclike herniation of the lining of the bowel that extends through a defect in the muscle layer.
Diverticula may occur anywhere in the small intestine or colon but most commonly occur in the sigmoid colon (at least 95%)
Persons of Asian heritage tend to develop diverticula in the right colon, probablybecause of genetic differences.
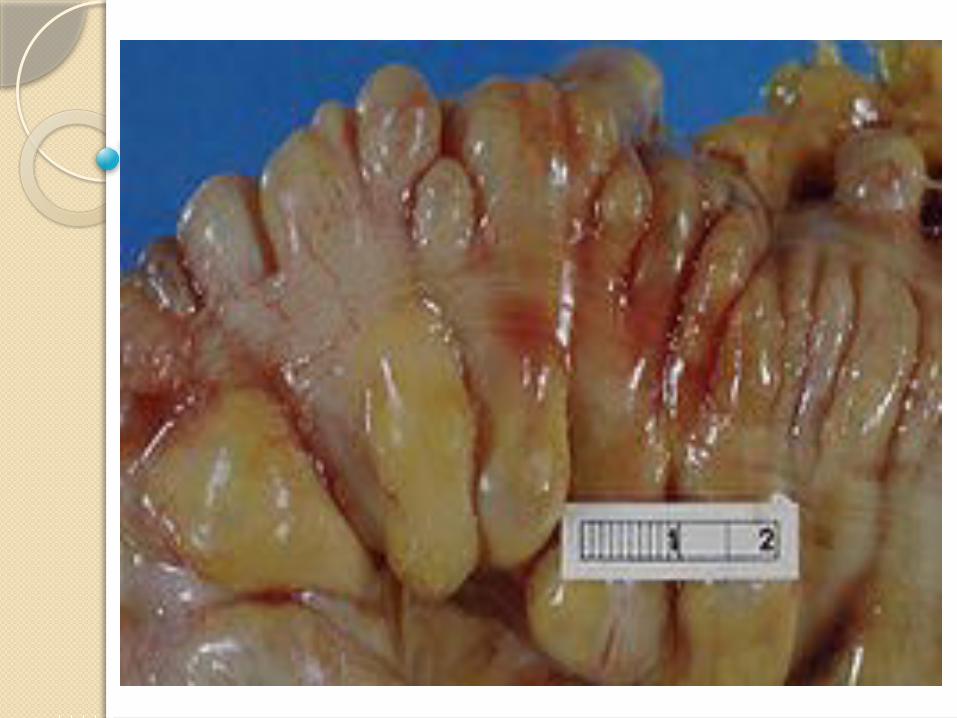
Diverticulosis
exists when multiple diverticula are present without inflammation or symptoms.
Diverticular disease of the colon is very common in developed countries, Prevalence increases with age:A low intake of dietary fiber is considered a predisposing factorChronic constipation often precedes the development of diverticulosis by many years.
Diverticulitis
results when food and bacteria retained in a diverticulum produce infection and inflammation that can impede drainage and lead to perforation or abscess formation.
At least 10% of patients with diverticulosis have diverticulitis at some point.
A congenital predisposition is suspected when the disorder occurs in those younger than 40 years.

Clinical Manifestations:
bowel irregularity diarrheanauseaanorexiabloating or abdominal distention
For diverticulitis:
mild to severe pain in the left lower quadrantnausea and vomitingfeverchills leukocytosis
Assessment and Diagnostic Findings
Diverticulosis is typically diagnosed by colonoscopy, which permits visualization of the extent of diverticular disease and allows the physician to biopsy tissue to rule out other diseases.
Until recently, barium enema had been the preferred diagnostic test, but it is now used less frequently than colonoscopy. If there are symptoms of peritoneal irritation when the diagnosis is diverticulitis, barium enema is contraindicated
because of the potential for perforation.
CT with contrast agent is the diagnostic test of choice if the suspected diagnosis is diverticulitis; it can also reveal abscesses.
Abdominal x-rays may demonstrate free air under the diaphragm if a perforation has occurred from the diverticulitis.
Laboratory tests that assist in diagnosis include a complete blood cell count, revealing an elevated white blood cell count, and elevated erythrocyte sedimentation rate (ESR).
Medical ManagementDietary and Pharmacologic Management
a clear liquid diet is consumed until the inflammation subsides
A high-fiber, low-fat diet is recommended. This
type of diet helps increase stool volume, decrease colonic transit time, and reduce intraluminal pressure.
Oral intake is gradually increased as symptoms subside.
Bulk-forming laxatives
Antispasmodics such as propantheline bromide and oxyphencyclimine (Daricon)
Broadspectrum antibiotics are prescribed for 7 to 10 days.
Opioids (eg, meperidine [Demerol]) for pain
Morphine is contraindicated because it can increase intraluminal pressure in the colon, exacerbating symptoms.

if vomiting or distention occurs, these are used to rest the bowel:
Withholding oral intake
Administering IV fluids
Instituting nasogastric suctioning
Medical ManagementSurgical Management
Immediate surgical intervention is necessaryif complications (eg, perforation, peritonitis, hemorrhage, obstruction) occur.
In cases of abscess formation withoutperitonitis, hemorrhage, or obstruction:
CT-guided percutaneous drainage may be performed to drain the abscess, and IV antibiotics are administered.
After the abscess is drained and the acute episode of inflammation has subsided (after approximately 6 weeks), surgery may be recommended to prevent repeated episodes.
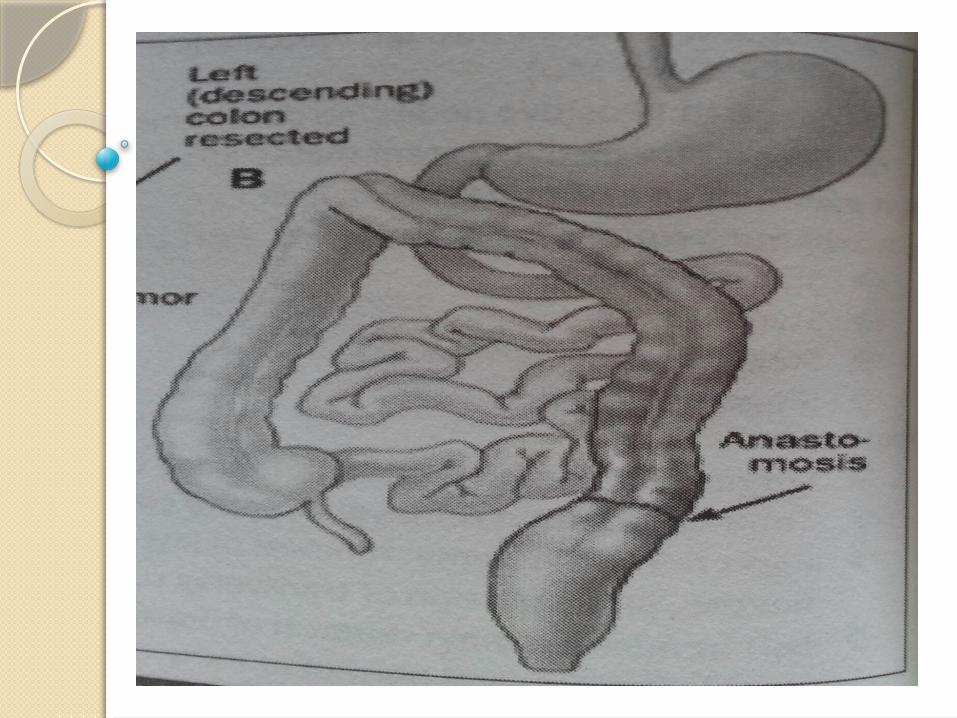
Two types of surgery are typically considered either to treat acute complications or preventfurther episodes of inflammation:
primary resection and end-to-end
anastomosis
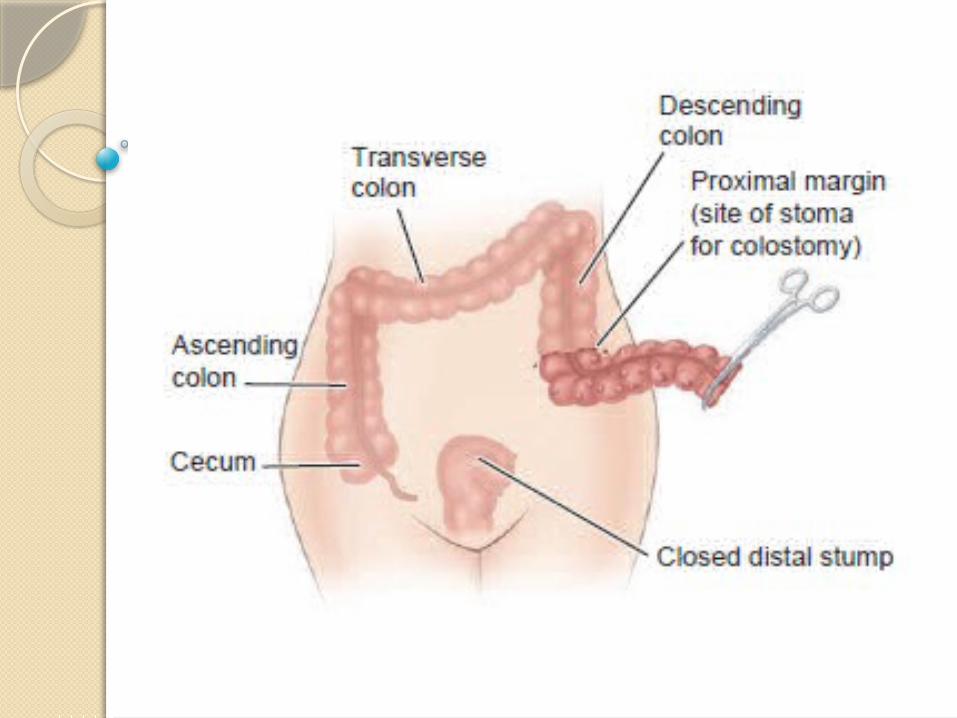
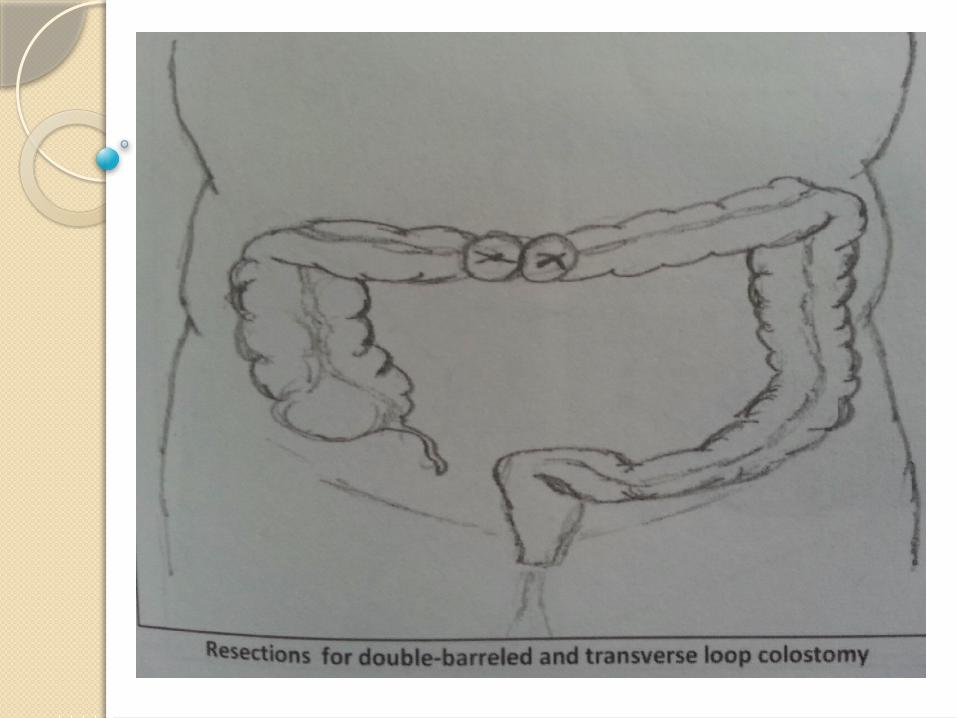
Hartmann’s procedure or double-barrel colostomies