Designing Successful Removable Partial DenturesA b stract:In
todays busy dental offices, removable partial denture design is
often abdicated by dentists, both as a result of a lack of
experience and consensus of design and because of educational
failure on the part of dental schools. The result is delegation of
the clinical design process to the lab technician. The lack of
clinical data provided to the dental technician jeopardizes the
quality of care. This article will focus on a logical and simple
approach to this problem, making removable partial denture design
simple and predictably achievable. The clinical evidence related to
removable partial denture design will be described, along with a
checklist to simplify the process and make it practical and
applicable to everyday clinical practice.
CE 3Tony Daher, DDS, MSEd, FACPAssociate Professor Director,
Advanced Prosthodontic Program
Dan Hall, DDS, FACD, FICDAssociate Professor Director of
International Dental Program
Charles J Goodacre, DDS, MSD, FACPProfessor and Dean Loma Linda
University School of Dentistry Loma Linda, California
Ivey of removable prosthodontic laboratories2 showed that 78% of
RPDs are designed by dental technicians at the dentists request.
Dental education has failed to adequately address this problem. A
2002 study by Hummel and colleagues3 demonstrated that RPD problems
are significant, and will continue to impact dentistry in the
future. A decrease in the curriculum time allocated to removable
prosthodontics may be inappropriate.3 At least a quarter of a
million people in the United States under the age of 40 wear RPDs,
and of those, at least one third report RPD defects, indicating
that there is a great need to improve RPDs.3 Improvements should
include new materials that are easy to use, repair, and maintain;
simplified designs and fabrication that enable most dentists to
provide well-fitting and functioning RPDs with an emphasis on
patient education, and need for followup care.3 Many
prosthodontists consider RPD fabrication to be a complete mouth
rehabilitation, and that it should be taught at the proficiency
level, not on a competency level. This has resulted in dental
school graduates who are more likely to delegate RPD design to lab
technicians and less likely to know the benefits of prosthodontic
specialty referral. Thus, the quality of dental care is
compromised. This article presents a simplified educational
approach to teaching RPD design that leads to predictable results.
The lack of a consensus on the design of a conventional RPD is
noticeable in the dental literature. Many variations of RPD design
have been used for the same clinical situation.4 Several published
books concur that RPD design begins by surveying the study cast
using a dental surveyor, marking survey lines, and selecting the
RPD components.5-9 The most logical approach to determine the
design of any RPD is to focus on a clinical approach based on
clinical evidence, rather than a laboratory decision-making
approach. The following checklist will simplify the process and
make it predictable.
n 1969, Atkinson and Elliot 1 showed that over half of all
dental school graduates could not design a removable partial
denture (RPD) that could be successfully fabricated by a dental
technician and worn by a patient. A 1984 sur1. Analyze the total
oral environment. 2. Draw the RPD design. 3. Survey the cast and
modify the design.
Learning Objecti es: vAfter readingthis article,the reader
should be able to: describe the recommended steps for designing a
successful removable partial denture. analyze the total oral
envi-
ronment necessary before drawing the removable partial denture
design. discuss the functions of different removable partial
denture components and their importance in fabricating a successful
removable partial denture.
186
C om pendiumMarch2006 /
Vol. 27, No. 3
including personal, medical, dental, and prosthetic histories;
necessary radiographs; articulat-
CE 3ed dental casts; and a visual and digital extraoral and
intraoral clinical exam.5 Many dentists often underestim ate the
practical usefulness of articulated dental casts. This results in
unforeseen future treatment problems and poor outcomes (Figures 1,
2A through 2D). These preliminary study casts are articulated at
the correct therapeutic occlusal vertical dimension in a retruded
contact position, on a semiadjustable articulator using an adjusted
facebow and often a protrusive record. When the plane of occlusion
and/or the vertical dimension of occlusion are not in harmony with
the dental arches, placement of denture teeth, restoration of
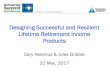
Figure1Tooth No. 31 dependson the correct vertical dimension. If
this occlusalverticaldimensionis the therapeuticdimension, then
tooth No. 31 must be sacrificedto create adequate interarchspaceand
adequatetissuecoveragefor the prosthesis. Howeve if the
occlusalverticaldimensionis to be restored5 r, mm posteriorl then
tooth No. 31 is retained. y.
Step1: A nalyze TotalO ralEnvironm ent theDesigning an RPD
starts with a complete analysis of the total oral environment. The
dentist must determine how to establish an optimum plane of
occlusion, occlusal vertical dimension, occlusal scheme, and
esthetics for a proper prosthetic restoration. To do so, adequate
prosthodontic data must be collected,
A
C
the abutment teeth, and creation of a functional occlusion
becomes difficult or impossible to accomplish.6 The dentition in
both arches must be analyzed before designing the RPD. The
treatment plan should include restoring the plane of occlusion and
the vertical dimension, and what type of occlusal scheme is needed
for an optimum clinical result.
D
B
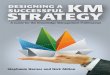
Figure2A through 2DMaxilla and mandibularRPD frameworksare
compatiblewith populardesign,but when we articulatedthe ry casts
(C, D) we were surprisedat the lack of intera distanceto arrangethe
prostheticteeth. rch Vol. 27, No. 3 Com pendium
187
CE 3
Figures 3A and Placingat least 1 dental implantin the distal
extensionarea will transformthe RPD from a tooth/tissue-borne a 3B
to tooth-borne(implant-borne) prosthesis.
The with a poorly fitted RPD. Unfortunately, responsibithough
many published research articles study lity for the ultimate
success of the RPD is often placed solely on the dentists
shoulders. the effects of vertical forces on RPDs, This responsibi
lity should be shared by both the a dearth of published research on
forces directdentist and ed on RPDs other than vertical forces. It
is certhe patient. In tainly helpful to the dentists to understand
how reviewan extension base of an RPD will respond to ing many
vertical forces,19 but the forces placed on prosperiodontal theses
can produce vertical, horizontal, rotationresearch al, or twisting
movements, or a combination of studies related to prosthodontics ,
it can be concluded that RPDs contribute to oral health if
above-average oral hygiene is practiced, adequate preprosthetic
periodontal therapy is executed, minimal standards for RPD design
are upheld, and periodic
there is
10-13 c a r e
A all 4.9 Ultimately the patient wants a stable, minimal
standard for
i s m a i n t a i n e d . RPD design well-fitting prosthesis,19
devoid of all movement, should be not just vertical movement.
simple and A tooth-borne prosthesis can be considered within the a
removable fixed bridge because it is the eascomprehensio iest to
design, most accepted by patients, and n of every has a longer
survival rate than the tooth/tissuepracticing dentist. The dentist
should note whether the patient has an anterior edentulous space in
addition to a posterior edentulous space. Anterior edentulous
spaces are best treated with fixed 7,20 p because it is easier to
achieve borne r prosthesi o s. s t h o d o n t i c s
The tooth/tissue-born e adequate esthetics, and it will decrease
the leverage effect of the forces generated during function on the
RPD. 7 In a case where soft tissue is lost, anterior edentulous
spaces are best replaced with an RPD if surgical correction is
contraindicate d. The presence of anterior replacement teeth for
RPDs was found to be a significant positive influence on denture
wearing.14 Next, the dentist must determin e if the clinical
situation is dentoalveolarsupported (tooth-borne), dentoalveolar
and mucoosseoussupported (tooth/tissueborne), or mucoosseous-
supported (tissue-borne).8 Each of these possible biomechanical
situations will respond differently to occlusal forces.9 Before
designing any dental prosthesis, the dentist must understand the
types of forces directed on the prosthesis. When the extension base
of a tooth/tissue-borne RPD with no guiding plates is subjected to
occlusal forces, many fulcrum lines come into play. These fulcrum
lines exist only
RPD is not well understood borne prosthesis). Therefore,
dentists can turn a by many dentists, tooth/tissue-borne situation
into a tooth-borne and its complexity depends situation by the use
of a dental implant on the on the span length edentulous side away
from the abutment of the edentulous area tooth, 21 (Figures 3A and
3B) or can opt to not and type of arch replace the missing teeth at
the extension base involved. with a prosthesis. In addition to this
previous Patients have a mechanical advantage, placing an implant
tendency to function under the RPD distal extension base has a
physand iological advantage. The amount of bone loss of use the
areas where the the distal edentulous area is reduced as a result
prosthesis is stable (for of its physiological stimulation by the
implant.22 example, the tooth-borne side If these choices are not
feasible, the dentist of a tooth/tissuecan create multiple opposing
guiding surfaces188Com pendiumMarch 2006 / Vol. 27, No. 3
CE 3
Figures 4A and RPD design is drawn on the cast in 3 steps: (1)
rests and minor connectors,(2) major and denture connectors, 4B (3)
direct retainers(claspsor attachments). Note that 3 guidingsurfaces
will be established: distal surfaces of teeth Nos. 6 and 12, and
the mesialsurface of tooth No. 12 where the minor connectoris
placed.15-18
Figures 5A and Tooth No. 32 has a guardedprognosis.The
mandibularRPD is designedand fabricatedwithouttaking tooth No. 5B
32 into consideration. Then a stainlesssteel wire occlusalrest is
made and connectedto the frameworkthrougha fabricatedloop, with the
denturebase acrylic. In case tooth No. 32 is lost, it is easily
repairedwithoutremakingthe RPD metal frame.
for the control of these forces and make an altered cast
impression procedure for the mandibular RPD. This will limit any
possible RPD movements. At least 3 abutments should be selected and
set as wide apart as possible (Figure 4A). The biomechanical forces
are resisted by a good selection of sound abutment teeth. At least
3 positive rests must be placed on 3 sound abutments. Then, as many
guiding surfaces as possible must be established on the abutment
teeth. This is an important step in the support, stability, and
retention of the future prosthesis. However, using more than 5
abutments compromises the accuracy and fit of the prosthesis.17 If
one of the RPD abutments is compromised, it is wise to consider
creating a contingency design. A contingency design is defined as
an RPD framework design that takes into consideration the presence
of a compromised tooth so that, should it be lost, the RPD will
not have to be refabricated.7 Remaking an RPD is costly;
repairing or adding teeth is a more reasonable expense (Figures 5A
and 5B).
Step 2: D rawthe R PD DesignAfter thoroughly analyzing the oral
environment, the optimal design should be drawn on the preliminary
cast. The authors believe that it is necessary to draw the optimum
RPD design on the cast before it is surveyed (Figures 4A and 4B).
The RPD design sequence begins by drawing the most important
features of the RPD framework.5 First the rests and
minor connectors are drawn (Figure 4A), followed by the major
and denture base connectors, and finally the clasps or attachments
(Figure 4B).
The first step is to draw the rests and the minor connectors at
the same time. A mini-
Rests and Guiding Minor ConnectorsVol. 27, No. 3 C om
pendium
189
CE 3
Figures 6A and The path of placementand removalis
materializedeither with the fabricationof a preparationguide or
with the 6B placementof a line on the cast on a verticalsurface
that is parallelto the placementpath. Then align the handpiecebur
intraorallywith the establishedguide to executetooth modifications
to establishadequateguidingsurfaces. and
mum of 3 positive rests are selected on good abutments as widely
apart as possible. A positive rest5 is defined as: one that directs
the occlusal forces parallel to the long axis of the teeth one that
is strong enough to resist breakage. A strong rest is when it is
thick enough, at least 1 mm, for chromecobalt alloy framework.
There should be a rounded line angle between the rest and minor
connector. The thickness
of the minor connector must be half the width of the rest, and
excessive rest inclination must be avoided.23 Positive rests and
guiding plates will keep the RPD from moving and exerting excess
pressure on the edentulous ridges. Common rests used in modern RPD
design are cingulum rests and occlusal rests. Many other forms of
positive rests exist, but are rarely used because they are not
taught in most dental schools. Minor connectors, or guiding plates,
are strong and are rigid parts of an RPD framework, such as
proximal, lingual, or buccal-vertical connectors. Their role is to
guide the RPD during placement and removal, and to connect other
units, such as rests, with the major connector or the denture base
connectors. Guiding minor connectors play an important role in
modern RPDs. Their functions are to: distribute the occlusal load
to both sides of the arch limit the number of paths of placement
and removal ensure stability against lateral forces and retention
of the prosthesis by their frictional retentive properties against
dislodgement forces during function. Thus they
maintain arch integrity by anterior-posterior and lateral
bracing action. The buttressing action5 of well-fitted multiple
opposing guiding surfaces, in conjunction with positive occlusal
rests, provides support, stability, and retention for the
prosthesis. An objective in RPD design is to maximize the number of
opposing surfaces.24 Any minor connecto r that connects an occlusal
rest, to the major con nector is made to contact 2 mini guiding
surfaces prepared in the lingual occlusal embrasure of 2 adjacent
teeth (Figures 4A and 4B). For this190
reason, the authors prefer to place the rest on the mesial fossa
of a RPD distal abutment.
Major and Denture Base ConnectorsCross arch stabilization is
provided by a rigid major connector. A main requirement for
adequate major connectors is rigidity.25 Also, they must be placed
in proper location to minimize the impingement on the oral
tissues.8 The difference between maxillary and mandibular major
connectors for RPDs is support.8 The horizontal portion of the
palate will resist vertical forces and thus play an important role
in the support of the tissue/tooth-borne RPD. The vertical portion
of the RPD intaglio surface plays a role in the stability of the
prosthesis. The maxillary and mandibular major connectors differ in
shape but not in function as a result of the different type of oral
anatomy. In the authors opinion, the maxillary major connector
should not cover the anterior rugae, the playground of the tongue,
or the posterior soft palate. The broad central palatal connector
or strap is most accepted by patients.26Vol. 27, No. 3
Com pendiumMarch 2006 /
Single straps are not rigid unless they are wide enough or cover
2 different planes of the hard palate.25 An anterior-posterior
(A-P) palatal connector is indicated when a palatal torus is
present and its surgical removal is contraindicated. Mechanically
speaking, the double strap A-P connector provides maximum rigidity
for the least amount of metal bulk present.5 Its major disadvantage
is that it has 4 borders that the patient can feel with the tongue
inside the mouth. 26 Whenever possible, the border of the anterior
strap of the A-P major connector should end in the valleys of the
incisal rugae, making it less obtrusive. Complete coverage of the
palatal connector is rarely used, and in clinical situations where
it is needed, the authors prefer acrylic coverage for practical
reasons.
The purpose of the denture base connector is to connect the
denture acrylic base to the framework. Large openings supply
stronger resin attachments, 28 and they should be located parallel
or lingual to the crest of the residual ridge so that they do not
interfere with the length of the buccal surfaces of the denture
teeth.5 They start and end in a butt joint in the major connector
at the internal and external acrylic finish lines. In a narrow
edentulous area or in the anterior edentulous area, posts must be
placed to retain the anterior teeth. When it is certain that a
narrow edentulous area will need to be relined, or in areas of
recent extractions, ladder retention must be used. A minimum of 1
thickness of baseplate wax should be used as the relief pad rather
than the usual 24- to 28-gauge wax.7 In every other instance, a
metal base with appropriate retentive lugs or loops is
indicated.5
CE 3
Direct Retainers
ental school graduates are more likely to delegate RPD design to
lab techniciansand less likely to know the benefitsof prosthodontic
specialtyreferral.
Selecting a major connector for the mandibular arch is limited
to either a lingual bar or a lingual plate. In the authors opinion,
the lingual bar is the better choice because it covers the minimum
amount of soft tissues.26 A lingual plate or a sublingual bar are
acceptable alternatives to a lingual bar when the vertical lingual
space is not available.27 Lingual plates are widely used when the
height of the anterior lingual vestibule is minimal as a result of
the common presence of lingual gingival recession, high lingual
frenum, and/or periodontally treated anterior teeth.5 The presence
of diastemas on the mandibular anterior teeth and the lack of
adequate height of the lingual vestibule dictate the use of the
sublingual bar. Labial or buccal bars are used when the mandibular
teeth are severely tilted lingually, or when large tori are present
and surgery is contraindicated.Vol. 27, No. 3
Retainers in modern RPDs must be passive in placement and
passive at rest.5 Retainers can be either clasps or attachments.
Popular clasps used currently are circumferential, I-bar, and
wrought wire.29 In the authors experience, I-bar or circumferential
clasps are good choices for almost any clinical situation. Wrought
wire clasps are technique-sensitive, easily deformed by the
patient, and costly. Direct retainers are the least important
component of the RPD because their retentive quality is impaired in
6 months because of permanent deformation.30 In the authors
clinical experience, clasps used in a situation with multiple
opposing guiding surfaces will not easily lose retention. I-bars
are considered the best option because they are more retentive than
a circumferential clasp for the same undercut, and because they
require only minimal tooth coverage. On the other hand,
circumferential clasps are preferred over I-bars when there is a
lack of vestibular depth, or when undercuts, exostoses, or labially
inclined abutments exist.5 Many clasp assemblies are used on the
distal abutment of an extension base RPD, such as distal rest and
circumferential clasp assemblies, I-bar system,6 Rest-Proximal
Plate-I Bar,9 RestProximal plate-Ackers Clasp,18 combination
clasps,33 or rigid clasp assemblies with splitC om pendium
191
CE 3
selected RPD design. The optimum RPD path major connectors.34
The efficiency of these of placement approximates the perpendicular
various clasp assemblies is described using photoelastic to the
plane of occlusion.40 In rare clinical situstudies in ations and
during the cast survey, it is necessary the vertical to modify the
optimum selected design to minplane. The imize the intraoral
preparation. purThe dentist has 2 options in this area. pose of all
clasp assemblies is to avoid the tilting and torque of abutment
teeth. However, no clinical evidence has been presented that RPDs
cause tilting forces on abutment teeth in A retrospective study
comEither the dentist locates a surveyor and sur-
D35,36 the long term .
paring the effectivene ss of 2 clasp designs, the distal rest
and circumfere ntial clasps system and the Ibar system, found that
the success rate of either design is 74%.37 This study emphasize d
that a
well-fabricated RPD is an acceptable modality, no matter what
type of retainer is used. Tebrock and colleagues35 and Maxfield and
colleagues38 attempted to measure abutment mobility in the mouth
with different clasp designs and different rest placements. They
reported no measurable mobility, regardless of rest position and
clasp design, when the altered cast procedure had been used. Good
base adaptation, good oral hygiene, and adequate occlusion are the
critical factors that minimize the need to design a
stress-releasing clasp assembl . y In the past, indirect retention
was a vital element in the design of an RPD. Frank and Nicholls39
showed that indirect retainers have little to do with retention of
tooth/tissue RPDs; they found that the guiding surfaces create
retention and stability in an RPD. In the authors opinion,
fabrication of indirect retainers should not be included when
teaching RPD design. Placing 1 or 2 additional rests and their
31,32
correspond ing guiding plates as far as possible from the
abutment rests will help with force distribution over a wider area,
thus improving the support, stability, and retention of the RPD.
This will eliminate the need for a socalled indirect retainer. In
addition, the additional rest(s) could be considered as points of
reference and visual cues during altered cast impression and reline
procedures.
the D esignThe purpose of surveying the cast is to check the
feasibility of the optimum selected drawn design. Surveying the
cast with the RPD design drawn on it will help to identify the
intraoral preparation needed to meet the
Step 3: Survey the C ast and M odify
veys the cast, or consults base plate wax, then trim excess wax
with with the laboratory the surveyor. Lubricate the selected area
technician during the with petroleum jelly, apply a small amount
surveying procedure to of autopolymerizing acrylic, and embed a
identify areas requiring friction grip bur, using the surveyor
(Figure intraoral modification. 6A). Allow the acrylic to set, then
finish Once this step is and polish. The bur direction is parallel
to completed, the the selected path of insertion of the dentist or
designed RPD. The device is placed in the the lab technician
tripods mouth and used as a reference to align the the cast for
future use handpiece bur to execute the shaping of and makes a
preparation the selected guiding surfaces. guide that will be used
2. Select a tooth surface that is parallel to the in the mouth to
shape the path of placement, mark it on the cast as a guiding
surfaces and reference, and use it in the clinical situation tooth
contours, and to to align the bur direction during the
intraeliminate undesirable oral preparation procedures (Figure 6B).
undercuts on the The second approach will save the practicabutment
teeth. The ing dentist time and result in a more successful
preparaprosthesis. tion guide is formed in 2 different ways on the
C on clus io n cast using the surveyor: This article has focused on
a simplified, 1. Select 2 adjacent organized approach to designing
modern RPDs. teeth situated equidistant Three steps are enumerated:
analyze the total to all guiding environment, draw the RPD design,
and check surfaces. Block out the feasibility of the design using
the surveyor. cervical This article also describes the different
RPD and embrasure tooth components and their function, and relates
undercuts with pink some clinical evidence to their use.192Com
pendiumMarch 2006 / Vol. 27, No. 3
R eferences1. Atkinson RA, Elliot RW. Removable partial denture
designed for laboratory fabrication by recent dental school
graduates. J Prosthet Dent. 1969;22:528-543. Taylor TD, Matthews
AC, Aquilino SA, et al. Prosthodontic survey. Part 1: Removable
prosthodontic laboratory survey. J Prosthet Dent. 1984;52:598-601.
Hummel SK, Wilson MA, Marker VA, et al. Quality of removable
partial dentures worn by the adult US population. J Prosthet Dent.
2002;38:37-43. Frantz WR. Variations in a removable maxillary
partial denture design by dentists. J Prosthet Dent.
1975;34:625-633. Kratochvil FJ. Partial removable prosthodontics.
In: Dentistry. Philadelphia: Saunders Core Textbook; 1988:
11,27,67,83-110,132. Stewart KL, Rudd KD, Kuebker WA. Stewarts
Clinical Removable Partial Prosthodontics 3rd ed. Quintessence .
Publishing Co Inc; 2003:274-282. Brudvik JS. Advanced Removable
Partial Dentures. Quintessence Books; 1999:Chapter 2. Krol AJ,
Jacobson TE, Finzen FC. RemovablePartial Design. Outline Syllabus.
1999;5th Edition 14,33,48. McGivney GP, Carr AB. Biomechanicsof
removable partial dentures. In: McCrackens Removable Partial
Prosthodontics. 10th ed. Mosby; Chapter 4. Bergman B, Ericson G.
Cross-sectional study of the periodontal status of removable
partial denture patients. J Prosthet Dent. 1989;61:208-211. Bergman
B, Hugoson A, Olsson CO. Caries, periodontal and prosthetic
findings in patients with removable partial dentures: A ten-year
longitudinal study. J Prosthet Dent. 1982;48:506-514. Petridis H,
Hempton TJ. Periodontal considerations in removable partial denture
treatment: a review of the literature. Int J Prosthodont.
2001;14:164-172. Chandler JA, Brudvik JS. Clinical evaluation of
patients eight to nine years after placement of removable partial
dentures. J Prosthet Dent. 1984;51:736-743. Jepson NJA, Thomason
JM, Steele JG. The influence of denture design on patient
acceptance of partial dentures. J Prosthet Dent. 1995:178;296-300.
Kratochvil FJ, Caputo AA. Photoelastic analysis of pressure on
teeth and bone supporting a removable partial dentures. J Prosthet
Dent. 1974;32:52-61. Thompson WD, Kratochvil FJ, Caputo AA.
Evaluation of photoelastic patterns produced by various designs of
bilateral distal-extension removable partial dentures. J Prosthet
Dent. 1977;38:261-273. Eliason CM. RPA clasp design for
distal-extension removable partial dentures. J Prosthet Dent.
1983;49:25-27. Aviv I, Ben-Ur Z, Cardash HS. An analysis of
rotational movement of asymmetrical distal-extension removable
partial dentures. J Prosthet Dent. 1989;61:211-214. Frank RP,
Brudvik JS, Leroux B, et al. Relationship between the standards of
removable partial denture construction, clinical acceptability, and
patient satisfaction. J Prosthet Dent. 2000;83:521-527. Vermeulen
A, Keltjens H, vant Hof MA, et al. Ten year evaluation of removable
partial dentures: Survival rates based on retreatment, not wearing
and replacement. J Prosthet Dent. 1996;76:267-272.
21.
22.
2.
23.
3.
24.
4. 5.
25.
6.
26.
7. 8. 9.
27.
28.
10.
29.
11.
30.
31.
12.
32. 33.
13.
14.
34.
15.
35.
16.
36.
17. 18.
37.
19.
38.
39. 40.
20.
Kuzmanovic DV, Payne AG, Purton DG. Distal implants to modify
the Kennedy classification of a removable partial denture: A
clinical report. J Prosthet Dent. 2004;92:8-11. Wyatt CC. The
effect of prosthodontic treatment on alveolar bone loss: A review
of the literature. J Prosthet Dent. 1998;80:362-366. Sato Y,
Shindoi N, Koretake K, et al. The effect of occlusal rest size and
shape on yield strength. J Prosthet Dent. 2003;89:503-507. Sato Y,
Shindoi N, Hosokawa R. Proximal plate in conventional
circumferential cast clasp retention. J Prosthet Dent.
2000;83:319-322. Ben-Ur Z, Mijiritsky E, Gorfil C, et al. Stiffness
of different designs and cross-sections of maxillary and mandibular
major connectors of removable partials dentures. J Prosthet Dent.
1999;81:526-532. Wagner AG, Traweek FC. Comparison of major
connectors for removable partial dentures. J Prosthet Dent. 1982;
47:242-245. Hansen CA, Campbell DJ. Clinical comparison of two
mandibular major connector designs: The sublingual bar and the
lingual plate. J Prosthet Dent. 1985;54:805-809. Dunny JA, King GE.
Minor connector designs for anterior acrylic resin bases: A
preliminary study. J Prosthet Dent. 1975;34:496-502. Phoenix RD,
Cagna DR, DeFreest CF. Clinical Removable Partial
Prosthodontics.3rd ed. Quintessence Publishing Co; 2003: Chapter 3.
Ghani F, Mahood M. A laboratory examination of the behavior of cast
cobalt-chromium clasps. J Oral Rehabil. 1990;17:229-237. Benson D,
Spolsky VW. A clinical evaluation of removable partial dentures
with I-bar retainers. Part I. J Prosthet Dent. 1979;41:246-254.
Stone E. Tripping action of bar clasps. J Am Dent Assoc.
1936;23:596. Brudvik JS, Wormley JH. Construction techniques for
wrought wire retentive clasp arms as related to clasp flexibility.
J Prosthet Dent. 1973;30:769-774. Reitz PV, Caputo AA. A
photoelastic study of stress distribution by a mandibular split
major connector. J Prosthet Dent. 1985;54:220-225. Tebrock OC,
Rohen RM, Fenster RK, et al. Effects of various clasping systems on
mobility of abutment teeth for distal extension removable partial
dentures. J Prosthet Dent. 1979;41:511-516. Hosman HJ. The
influence of clasp design of distal extension removable partial
dentures on the periodontuim of the abutment teeth. Int J
Prosthodont. 1990;3:256-265. Kapur KK, Deupree R, Dent RJ, et al. A
randomized clinical trial of two basic removable partial denture
designs. Part I: Comparisons of five-year success rates and
periodontal health. J Prosthet Dent. 1994:72;268-282. Maxfield JB,
Nicholls JI, Smith DE. Measurement of forces transmitted to
abutment teeth of removable partial dentures. J Prosthet Dent.
1979;41:134-142. Frank RP, Nicholls JI. An investigation of the
effectiveness of indirect retainers. J Prosthet Dent.
1977;38:494-506. Bezzon OL, Mattos MG, Ribero RF. Surveying
removable partial dentures: the importance of guiding planes and
path of insertion for stability. J Prosthet Dent.
1997;78:412-418.
CE 3
Vol. 27, No. 3
C om pendium
193
Quiz31. What percentage of removable partial dentures (RPDs) are
designed by dental technicians at the dentists request? a. 28% b.
58% c. 78% d. 88% 2. Designing an RPD starts with: a. b. c. d.
drawing the RPD design. surveying the cast with a surveyor.
complete analysis of the total oral environment. clasp and rest
seat preparation. 5. When drawing the RPD design, 8. The purpose of
surveying the first draw: cast is to: a. rests and minor
connectors, a. draw the survey line and to then the major and
denture select the type of clasp needconnectors, then the clasps
ed. or attachments. b. check the feasibility of the b. direct
retainers, then the optimum selected drawn major and denture
connecdesign. tors, then the rests and guidc. check all the
undercuts that ing minor connectors. exist on the dental arch. c.
major and denture connecd. place 3 rests as far apart as tors, then
the direct retainpossible. ers, then the rests and guid9. The
optimum RPD path of ing minor connectors. placement: d. major and
denture conneca. approximates the perpendictors, then the rests and
guiding minor connectors, then ular to the plane of occlusion. the
direct retainers. b. is when at least 2 rest seats can be found. 6.
The functions of guiding minor c. is when at least 1 retention
connectors are to: clasp can be placed. a. distribute the occlusal
load d. is when no tooth preparato both sides of the arch. tion is
required. b. limit the number of paths of 10. A preparation guide
is used to placement and removal. shape the: c. ensure stability
against latera. rest seats. al forces. d. all of the above b.
guiding surfaces. c. major connectors. 7. What creates retention
and stad. undercuts. bility in an RPD? a. poor base adaptation b.
guiding surfaces c. indirect retention d. rest seats
3. Anterior edentulous spaces are best treated with: a. a fixed
partial denture prosthesis. b. the same type of RPD, especially
when soft tissue is present. c. the same type of RPD, especially
when soft tissue surgery is indicated. d. an interim removable
prosthesis. 4. The tooth-tissue-borne RPD: a. could be considered a
removable fixed bridge. b. is very well understood by many dentists
because of its simplicity in design. c. complexity depends on the
span length of the edentulous area and type of arch involved. d.
does not need multiple opposing guiding surfaces.
Please see tester form on page 195.This article provides 1 hour
of CE credit from Ascend Medias Dental Learning Systems, in
association with the University of Southern California School of
Dentistry and the University of Pennsylvania School of Dental
Medicine, representatives of which have reviewed the articles in
this issue for acceptance. Record your answers on the enclosed
answer sheet or submit them on a separate sheet of paper. You may
also phone your answers in to (888) 596-4605 or fax them to (703)
404-1801. Be sure to include your name, address, telephone number,
and the last 4 digits of your Social Security number.
194
C om pendiumMarch 2006 /
Vol. 27, No. 3
CE ANSWE FORM RCE 11. b d 2. b d 3. b d 4. b d 5. b d 6. b d 7.
b d 8. b d 9. b d 10. b d a c a c a c a c a c a c a c a c a c c
a
Compendium, March 2006 CE 21. d 2. d 3. d 4. d 5. d 6. d 7. d 8.
d 9. d 10. d
CE 3a a a a a a a a a a b b b b b b b b b b c c c c c c c c c c
1. d 2. d 3. d 4. d 5. d 6. d 7. d 8. d 9. d 10. d a a a a a a a a
a a b b b b b b b b b b c c c c c c c c c c
n Presently Enrolled in CE Program
Not Enrolledn 1 exam completed = $14.00 n 2 exams completed =
$24.00 n 3 exams completed = $38.00
Please enroll me in the The Compendium Continuing Education
Program marked below: n Please enroll me in the 12-month CE Program
for $234.00 (a 36% saving versus paying for each exam
individually). Program includes all 36 exams in The Compendium for
1 year (plus selected supplements). n CHECK (payable to Ascend
Medias Dental Learning Systems) n CREDIT CARD Please complete inf
ormation and sign below: Card Number n Visa n MasterCard n American
Express ______________________________________ ______________
Expiration Date: Mo/Y
(PLEASE PRINT CLEARLY ) Last 4 digits of the SSN
ADA Number AGD Number Month/Date of Birth_________________
The Month and Day (not year) of Birth. Example, Jan 23 is
01/23.
Name
________________________________________________________________________________
Address
______________________________________________________________________________
City
_________________________________________________________________________________
State ________ Zip _____________ Daytime
Phone_________________________Please mail completed forms with your
payment to: ASCEND MEDIAS DENTAL LEARNING SYSTEMS CE Department,
405 Glenn Drive, Suite 4, Sterling, VA 20164-4432 SCORING SERVICES:
By Mail Fax: 703-404-1801 Phone-in: 888-596-4605 (9am-5pm ET,
Mon.-Fri.) Customer Service Questions? Please Call 888-596-4605
PROGRAM EVALUATION
Please mark your level of agreement with the following
statements. (4 = Strongly Agree; 0 = Strongly Disagree)
CE 14
CE 23 2 1 0 4
CE 33 2 1 0
1) Clarity of objectives . . . . . .............. ..............
...... 2) Usefulness of the content . . . . ........... ...........
......... 3) Benefit to your clinical practice . . . . . . .
.............. .......... 4) Usefulness of the references
.............. .............. .... 5) Quality of the written
presentation . . . .............. ........... 6) Quality of the
illustrations . ........... ........... ........... . 7) Clarity of
review questions .............. .............. ...... 8) Relevance
of review questions .............. .............. .. 9) Did this
lesson achieve its educational objectives? . . . . . . . . . . . .
. . 10) Did this article present new information? . . . . . . . . .
. . . . . . . . . . . . 11) How much time did it take you to
complete this lesson? . . . . . . . . . . Yes No Yes No ______min
Yes No Yes No ______min Yes No Yes No ______min4 3 2 1 0 4 3 2 1 0
4 0 3 2 1 4 3 2 1 0 4 3 2 1 0 4 0 3 2 1
4 0 4 0 4 0
3 3
2 2
1 0 1 0
4 4
3 3
2 2
1 4 1 4 4
3 3 3
2 2 2
1 0 1 0 1 0
3
2
1 0
4
3
2
1
4 0 4 0
3 3
2 2
1 0 1 0
4 4
3 3
2 2
1 4 1 4
3 3
2 2
1 0 1 0
DEADLINE FOR SUBMISSION OF ANSWERS IS 12 MONTHS AFTER THE DATE
OF PUBLICATION.