Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
g C 28 (2008) 1347–1351www.elsevier.com/locate/msec
Materials Science and Engineerin
3-D biomodelling technology for maxillofacial reconstruction
Manuel Oliveira a, N. Sooraj Hussain b,c, A.G. Dias b,c, M.A. Lopes b,c, Luís Azevedo a,Horácio Zenha a, Horácio Costa a, J.D. Santos b,c,⁎
a Serviço de Cirurgia Plástica e Reconstructiva do Centro Hospitalar de Vila Nova de Gaia (CHVNG), Monte da Virgem – Vale Andorinho-o-Douro,4400 Vila Nova de Gaia, Porto, Portugal
b Instituto de Engenharia Biomédica (INEB), Laboratório de Biomateriais, Rua Campo Alegre, 823, 4150-180, Porto, Portugalc Departamento de Engenharia Metalúrgica e de Materiais (DEMM), Faculdade de Engenharia da Universidade (FEUP),
Rua Dr. Roberto Frias, 4200-465, Porto, Portugal
Received 7 November 2007; accepted 24 February 2008Available online 8 March 2008
Abstract
Biomodel is a product of rapid prototyping process that represents a new approach for surgical planning and simulation. Biomodels were foundto be particularly effective to locate an exact defect with good measurement accuracy and without any risk to the patients' health. These modelscould provide surgeons a realistic impression of complex structures before surgical intervention, allowing a define diagnosis and a precisepreoperative simulation of skeleton modifying interventions.
This work reports on the application of innovative 3-D biomodelling technology in the maxillofacial reconstruction. This technology allows forthe calculation of the exact contours, angulations, length and general morphology of iliac crest and fibula flaps for maxillofacial reconstruction in atotal of 28 clinical cases. Clinical results have shown that by using this technique, much better facial symmetry and improved functionality wereachieved after surgery, which resulted in enormous benefits for treated patients.© 2008 Elsevier B.V. All rights reserved.
Keywords: 3D Biomodelling; Maxillofacial reconstruction; Free flap designing
1. Introduction
Biomodelling is a technology that allows three-dimensional(3D) computed tomography (CT) and other image technologydata to be used to manufacture solid plastic replicas ofanatomical biomodels. Mathematical techniques for describingthe 3-dimensional (3D) morphology of the facial skeleton arebecoming increasingly sophisticated [1–3]. Biomodelling is ageneric term describing the ability to replicate the morphologyof a biological structure in a solid substance. Specifically,biomodelling uses radiant energy to capture morphological dataon a biological structure and processes such data by a computer
⁎ Corresponding author. Departamento de Engenharia Metalúrgica e deMateriais (DEMM), Faculdade de Engenharia da Universidade (FEUP), Rua Dr.Roberto Frias, 4200-465, Porto, Portugal. Tel./fax: +351 22 5081419.
E-mail address: [email protected] (J.D. Santos).
0928-4931/$ - see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.msec.2008.02.007
to generate the code required to manufacture the structure byrapid prototyping (RP) [4–6].
Stereolithography (SL) is a rapid prototyping (RP) process.Employing these technologies, it is possible to build 3D models,with all their complexity in a very short time, under computercontrol and without significant human intervention [7,8]. Almostall rapid prototyping processes, either currently available commer-cially or under development are based on layered manufacturingmethodology in which objects are built as a series of horizontalcross sections, each one being formed individually from therelevant raw materials and bonded to preceding layers until it iscompleted. The main process stage involved in fabricating theparts are common to most systems but the mechanisms by whichthe individual layers are formed may differ [9].
The accuracy of SL has been shown in the range of ±1 mm,which offers clinicians the ability to perform retrospective andprospective studies of facial aging, for example [1,10].

1348 M. Oliveira et al. / Materials Science and Engineering C 28 (2008) 1347–1351
In literature, D' Urso et al have studied on forty-five patientswith craniofacial, maxillofacial and skull base cervical spinalpathology [5]. The conclusion was that biomodels havesignificantly improved the operative planning and diagnosesto 82.2% and 95.2% respectively [5].
Peckitt [11] has reported on the current and future develop-ments in stereoscopic lithography customized titanium implantsin orofacial reconstruction. All patients were reported to have anacceptable quality of life and in another report, benefits ofstereolithography in orbital reconstruction in two patients werestudied [12]. In these cases, SL offered highly accurate models ofthe bony orbit for preoperative evaluation, surgical planning andincreased the orbital surgeon's options in managing complexorbital pathology. SL is an accurate technology that may find a
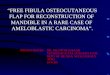
Fig. 1. Image sequence starting from (A) a pre-operative frontal view, lateral view (B)of restoring the facial symmetry of the patient using RP surgical guides (C), radiologicfrom the peroneal bone was designed according to the surgical guide (E), the radiolosurgery (F) and complete restoration of the defect and biofunctionality was observe
significant application in the study of facial aging sincedifferential growth of the facial skeleton may occur throughoutlife, specifically in the maxillary regions [13].
Very recently, the authors studied the application of thistechnology in a case report of opening wedge high tibialosteotomy [14]. Results have shown that these 3D Bonelike®macroporous scaffolds was an excellent option in the treatmentof medial compartment osteoarthritis varus knee, as they offer aframework for new bone tissue formation and anchorage byproviding surface and volume that will allow for cell ingrowthand an accurate cell distribution throughout the porous structure[14–18].
This paper reports the application of an innovative 3-DBiomodelling approach for the calculation of the exact
of the patient, an extensive virtual manipulation had to be performed with the aimal image showing the Ti plate that had been implanted (D), the free flap harvestedgical examination showing the implanted free flap and restored symmetry afterd after 6 months of the surgery in the post operative image (G).

1349M. Oliveira et al. / Materials Science and Engineering C 28 (2008) 1347–1351
contours, angulations, length and general morphology of iliaccrest and fibula flaps for mandible and maxilla reconstruction ina total of 28 clinical cases. This work is a part of a moreextensive application of this innovative technology on othertypes of free flaps both for soft hard and soft tissue transfer.Examples of possible usage include groin flap, deep circumflexiliac groin flap, dorsalis pedis flap, lactissimus dorsi flap,scapular flaps, the deltoid flap, the lateral arm flap and serratusanterior free flap. The latter is currently being applied by thismultidisciplinary research group.
2. Materials and Methods
2.1. Biomodel manufacture
For the construction of the physical 3D model, first aconventional scan CT was performed of the patient's anatomyand converted into 3D model using appropriate software. Thistechnology is a powerful solution that combines DICOMnetwork retrieval and truly interactive 3D visualisation ofvolumetric image data. This software contains a unique patentedoptimisation algorithm that automatically generates optimalsurface-based STL files and contour-based SLC files for solidmodelling via rapid prototyping (RP). Most 3D volumes can beedited, viewed in 3D, and converted to RP files in a matter ofminutes. These 3D models accurately mimicked the patient'sanatomical structures of interest.
Fig. 2. (A) A pre-operative image of the patient suffered from a tumoral lesion of therestore facial symmetry, (C) an excision of the patient mandible, (D) the symmetryoperative frontal view.
2.2. Clinical cases
Two representative clinical cases were reported in this work.One case reports a patient who was victim of a facial gunshotwound resulting in partial destruction of the mandible and ofother bone structures. Previous surgery performed by surgicalteam, implanted one Ti plate in the right part of the mandible, inorder to restore the facial symmetry of the patient and increasethe biofunctionality (i.e. correction of the occlusal plan andother bone structures), it was necessary to determine the generalmorphology of the free flap obtained from autologous peronealbone, in terms of its volume, length, and angulation andtherefore the 3D biomodelling and rapid prototyping technol-ogies were used.
The second case reports a patient that suffered from atumoral disease in the mandible (ameloblastome). The surgeryinvolved the total resection of the tumor followed by free flapimplantation that was collected from peroneal bone. Therequired volume, length and general morphology of the freeflap was obtained according to the 3D Biomodel and custom-made surgical guides that were manufactured.
3. Results and discussion
The 3D Biomodelling associated with rapid prototyping hasbecome one fundamental tool in reconstructive surgery in recentyears [1–3,19]. From computer tomography (CT) scans, virtual
mandible, (B) 3D biomodel and surgical guides were manufactured in order toof the mandible was restored due to the use of surgical guides, and (E) a post-

Table 1The application of 3D Biomodelling has been used in 28 clinical cases for thedesigning of the morphology of free flaps obtained from peroneal bone and iliaccrest in last 3 years
Clinical cases
Year No of Patients Peroneal bone Iliac crest
2004 10 6 42005 8 6 22006 10 9 1Total 28 21 7
1350 M. Oliveira et al. / Materials Science and Engineering C 28 (2008) 1347–1351
3D images of the patient's anatomy were converted into 3Dphysical models by using appropriate software and selectivelaser stereolithography (SL) technology [9]. The 3D medicalimaging associated with rapid prototyping has been consideredas a recent advanced technology in the medical fields of cranio-maxillofacial surgery [5] and cardiogenesis [20] for example.
Biomodelling offers the following specific advantages in themedical field [21]. For example, it optimises preoperativesurgical planning and rehearsal because biomodels may be usedrealistically and interactively to simulate reconstruction usingstandard power tools. It may be used to create templates for thepre-fabrication of customised prosthetic and bioinert andbioactive implants, improving implant design and fit, whilstreducing operative time. Biomodelling enhances team commu-nication, and teaching demonstrations with ‘hands on' inte-grative use of patient data. Finally biomodels require nospecialised equipment or knowledge for interpretation and useare rugged and may easily be transported [21].
Authors have applied 3D Biomodelling techniques tomanufacture high-precision macroporous structures of bioactivebone scaffolds for opening wedge high tibial osteotomy (HTO)in the orthopaedic field [14]. In this study, after 4 months ofpartial weight bearing, signs of fusion at the osteotomy site andgood osteointegration of the implanted wedges were observed.Therefore, 3D porous scaffolds seem to be an excellent optionfor bone regeneration applications, as they offer a frameworkfor new bone tissue formation [14].
This work describes the use of 3D Biomodelling in twoexamples of maxillofacial surgery during the last three years.Fig. 1(A) and (B) shows the pre-operative frontal and lateralviews of the patient and the radiological image the Ti plate thathad been implanted in the previous surgery (Fig. 1D). Anextensive virtual manipulation had to be performed with the aimof restoring the facial symmetry of the patient using RP surgicalguide as shown in Fig. 1(C). The 3-D RP model revealed thepatient's right mandible defect, and the computer simulation ofthe mirrored mandible was obtained with the exact positioningof the surgical guides. The required volume, length, angles andthe general morphology of the free flaps were determined by thesurgical guides, which allowed the facial symmetry of thepatient to be restored. After the manufacture of surgical guides,a fibula flap was designed and the free flap harvested from theperoneal bone, as shown in Fig. 1(E), and then transferred andrevascularized in the patient's mandible. The radiologicalexamination revealed that anatomical symmetry has beenrestored, as depicted in Fig. 1(F). Complete restoration of thedefect and biofunctionality was observed after 6 months of thesurgery, as seen by comparison of Fig. 1(A) and (G).
In the second mandible reconstruction study, the patientsuffered from a tumoral lesion of the mandible (ameloblastome)as shown in Fig. 2 (A). The surgery was performed on themandible for the total resection of the tumour followed byautologous bone graft implantation collected from the patientperoneal bone. In order to restore the facial symmetry, one 3Dbiomodel and surgical guides were manufactured as seen inFig. 2 (B). Therefore, the required volume, length, angles andgeneral morphology of the bone was obtained from the 3 D
biomodel and without its use it would have not been possible toknow the exact defect, dimensions and positioning. In Fig. 2(C),an excision of the patient mandible was performed, and thesymmetry of the mandible was restored due to the use ofsurgical guides in Fig. 2(D). Finally, a post-operative frontalview was shown in Fig. 2(E).
Table 1 describes the application of 3D Biomodelling hasbeen used in 28 clinical cases for the designing of themorphology of free flaps obtained from peroneal bone (21)and iliac crest (7) in the last 3 years. Throughout all the casesstudied, 3D biomodels have demonstrated their clinicalrelevance in the maxillofacial reconstruction area bringingenormous benefits for patients. In fact, biomodels can help toimprove operative planning for surgeons, thus reducingoperation times and improving the measurement accuracy.When compared with standard images alone, biomodelscombined with image data have greater utility in surgery tominimize errors and risks [5].
4. Conclusions
In the maxillofacial reconstruction surgery, complex defectsof the face can benefit enormously from a multidisciplinaryapproach that combines computer based technologies andadvanced surgical techniques. Free tissue transfer that mimicsanatomical structures is thus possible with an enormousimprovement in the aesthetical and biofunctional outcome.
Acknowledgments
The authors express their grateful thanks to a FCT –Fundação para a Ciência e a Tecnologia for their support inthis work through a project “New generation of bioactive andbioresorbable materials for bone regenerative surgery using 3Dbiomodelling” and also through Post-Doctoral grant SFRH/BPD/6010/2001 & SFRH/BPD/14969/2004.
References
[1] J.E. Pessa, Am. J. Orthod. Dentofac. Orthop. 119 (2001) 117.[2] J. Poukens, J. Haex, D. Riediger, Comput. Aided Surg. 8 (3) (2003) 146.[3] G.A. Brown, B. Milner, K. Firoozbakhsh, J. Orthop. Trauma 16 (5) (2002)
347.[4] E. Berry, J.M. Brown, M. Connell, C.M. Craven, N.D. Efford, A.
Radjenovic, M.A. Smith, Med. Eng. Phys. 19 (1) (1997) 90.[5] P.S.D. Urso, T.M. Barker, W.J. Earwaker, L.J. Bruce, R.L. Atkinson, M.W.
Lanigan, J.F.Arvier,D.J. Effeney, J. Cranio-Maxillo-Facial Surg. 27 (1999) 30.

1351M. Oliveira et al. / Materials Science and Engineering C 28 (2008) 1347–1351
[6] P.S.D. Urso, R.G. Thompson, Aust. N.Z. J. Obstet. Gynaecol. 38 (1998)205.
[7] J.J. Clair, J. Mater. Process. Technol. 57 (1996) 393.[8] D.T. Pham, R.S. Gault, Int. J. Mach. Tools Manuf. 38 (1998) 1257.[9] S.O. Onuh, K.K.B. Hon, Int. J. Mach. Tools Manuf. 38 (1998) 329.[10] T.M. Barker, W.J. Earwaker, D.A. Lisle, Australas. Radiol. 38 (1994) 106.[11] N.S. Peckitt, Br. J. Oral Maxillofac. Surg. 37 (1999) 353.[12] D.E.E. Holck, E.M. Boyd Jr., J. Ng, R.O. Mauffray, B, Ophthalmology 106
(1999) 1214.[13] J.E. Pessa, L.D. Desvigne, V.S. Lambros, J. Nimerick, B. Sugunan, V.P.
Zadoo, Aesthet. Plast. Surg. 23 (1999) 337.[14] M. Gutierres, A.G. Dias, M.A. Lopes, N. Sooraj Hussain, A.T. Cabral, L.
Almeida, J.D. Santos, J. Mater. Sci. Mater. Med. 18 (2007) 2377.
[15] O. Gauthier, J.M. Bouler, E. Aguado, P. Pilet, G. Daculsi, Biomaterials 19(1-3) (1998) 133.
[16] J.X. Lu, B. Flautre, K. Anselme, P. Hardouin, A. Gallur, M. Descamps, B.Thierry, J. Mater. Sci., Mater. Med. 10 (2) (1999) 111.
[17] M. Martina, G. Subramanyam, J.C. Weaver, D.W. Hutmacher, D.E. Morse,S. Valiyaveettil, Biomaterials 26 (28) (2005) 5609.
[18] L.Moroni, J.R. deWijn, C.A. vanBlitterswijk, Biomaterials 27 (7) (2006) 974.[19] B. Sanghera, S. Naique, Y. Papaharilaou, A. Amis, Rapid Prototyping J. 7
(5) (2001) 275.[20] J.O. Pentecost, J. Icardo, K.L. Thornburg, Comput. Med. Imaging Graph.
23 (1999) 45.[21] P.S.D. Urso, R.L. Atkinson, M.W. Lanigan, W.J. Earwaker, L.J. Bruce, A.
Holmes, T.M. Barker, RG. Thompson, Br. J. Plast. Surg. 51 (1998) 522.



![ReconstructionofMandibularDefectsUsingBone ...Herford and Boyne [ 4] Reconstruction of mandibular continuity defects with bone morphogenetic Protein-2 (rhBMP-2) Journal and Maxillofacial](https://img.pdfslide.us/doc/110x75/60b0d597fd96e12ede3dcaef/reconstructionofmandibulardefectsusingbone-herford-and-boyne-4-reconstruction.jpg)