Embed Size (px)
Citation preview

G
Case • 2A multilocular radiolucency
SUMMARYA 45-year-old African man presents in the accident and emergency department with an enlarged jaw. You must make a diagnosis and decide on treatment.
have cured the swelling. Although not in pain, he has finally decided to seek treatment.
Medical historyHe is otherwise fit and healthy.
Examination
Extraoral examinationHe is a fit-looking man with no obvious facial asymmetry but a slight fullness of the mandible on the right. Palpation reveals a smooth rounded bony hard enlargement on the buccal and lingual aspects. Deep cervical lymph nodes are palpable on the right side. They are only slightly enlarged, soft, not tender and freely mobile.
Intraoral examination� What do you see in Figure 2.1?
There is a large swelling of the right posterior mandible visible in the buccal sulcus, its anterior margin relatively well defined and level with the first premolar. The lingual aspect is not visible but the tongue appears displaced upwards and medially suggesting significant lingual expansion. The mucosa over the swelling is of normal colour, without evidence of inflammation or infection. There are two relatively small amalgams in the lower right molar and second premolar
If you could examine the patient you would find that all his upper right posterior teeth are extracted and that the lower molar and premolars are 2–3 mm above the height of the occlusal plane. Both teeth are grade 3 mobile but both are vital.
� What are the red spots on the patient’s tongue?
Fungiform papillae. They appear more prominent when the tongue is furred, as here, for instance when the diet is not very abrasive.
� On the basis of what you know so far, what types of condition would you consider to be present?
The history suggests a relatively slow-growing lesion, which is therefore likely to be benign. While this is not a definitive relationship, there are no specific features suggesting malignancy, such as perforation of the cortex, soft tissue mass, ulceration of the mucosa, numbness of the lip or devitalization of teeth. The character of the lymph node enlargement does not suggest malignancy.
The commonest jaw lesions that cause expansion are the odontogenic cysts. The commonest odontogenic cysts are the radicular (apical inflammatory) cyst, dentigerous cyst and odontogenic keratocyst. if this is a radicular cyst it could have arisen from the first molar, though the occlusal amalgam is relatively small and there seems no reason to suspect that the tooth is nonvital. a residual radicular cyst arising on the extracted second or third molar would be a possibility. a dentigerous cyst could be the cause if the third molar is unerupted. The possibility of an odontogenic keratocyst seems unlikely, because these cysts do not normally cause
Fig. 2.1 The patient on presentation.
History
ComplaintThe patient’s main complaint is that his lower back teeth on the right side are loose and that his jaw on the right feels enlarged.
History of complaintThe patient has been aware of the teeth slowly becoming looser over the previous 6 months. They seem to be ‘moving’ and are now at a different height from his front teeth, making eating difficult. He is also concerned that his jaw is enlarged and there seems to be reduced space for his tongue. He has recently had the lower second molar on the right extracted. It was also loose but extraction does not seem to
G
A m u l t i l o c u l A r r A d i o l u c e n c y
• 82CASE
much expansion. an odontogenic tumour is a possible cause and an ameloblastoma would be the most likely one, because it is the commonest, and arises most frequently at this site and in this age group. There is a higher prevalence in africans than other racial groups. an ameloblastoma is much more likely than an odontogenic cyst to displace the teeth and make them grossly mobile. a giant cell granuloma and numerous other lesions are possibilities but are all less likely.
Investigations� Radiographs are obviously indicated. Which views would
you choose? Why?
Several different views are necessary to show the full extent of the lesion. These are listed in the ‘radiographic view’ table above.
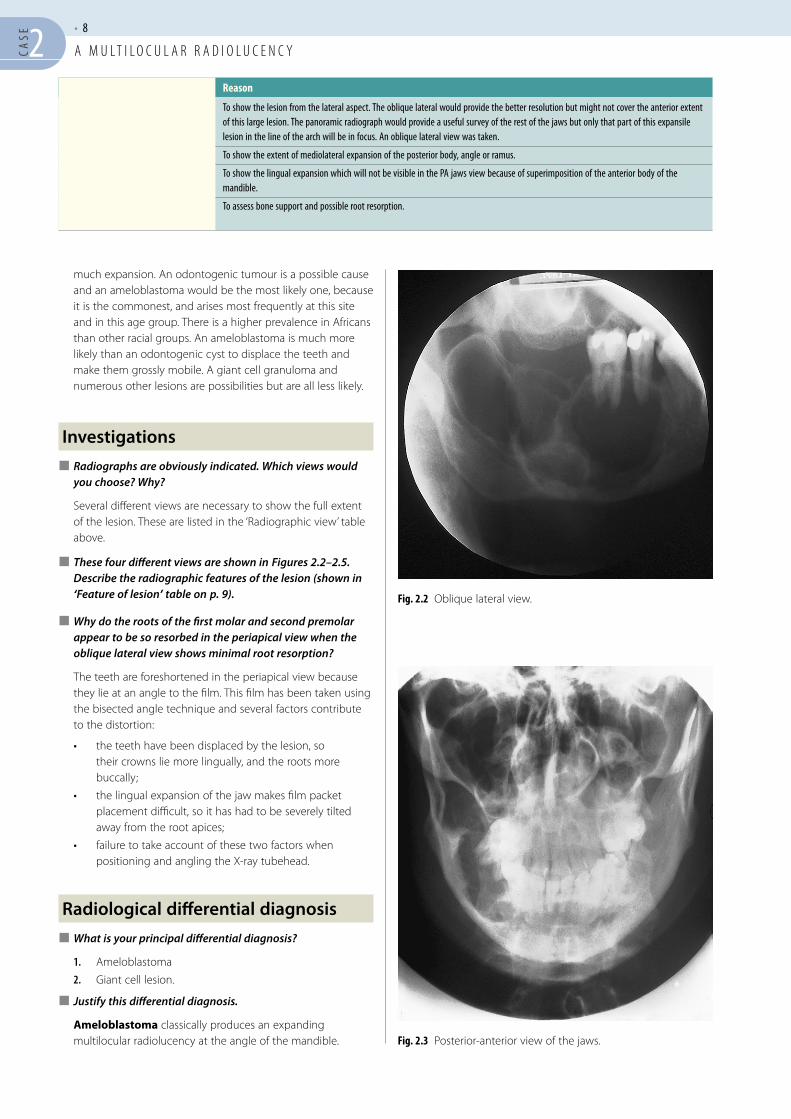
� These four different views are shown in Figures 2.2–2.5. Describe the radiographic features of the lesion (shown in ‘Feature of lesion’ table on p. 9).
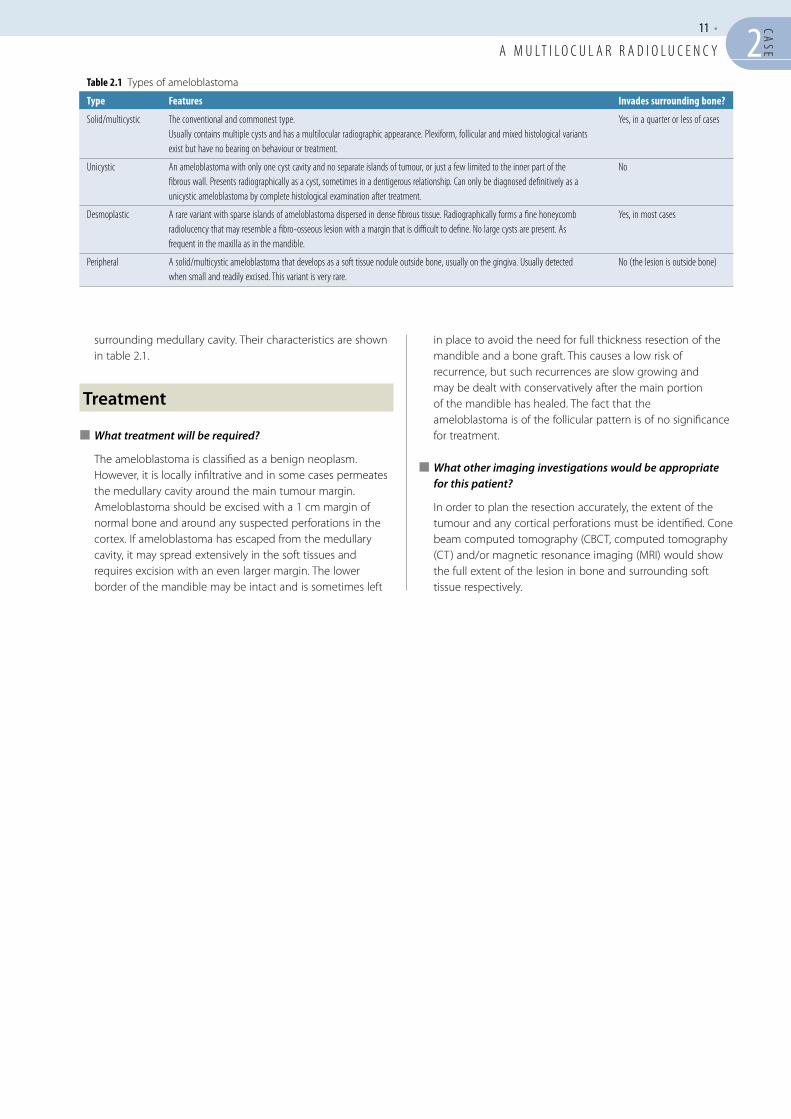
� Why do the roots of the first molar and second premolar appear to be so resorbed in the periapical view when the oblique lateral view shows minimal root resorption?
The teeth are foreshortened in the periapical view because they lie at an angle to the film. This film has been taken using the bisected angle technique and several factors contribute to the distortion:
• the teeth have been displaced by the lesion, so their crowns lie more lingually, and the roots more buccally;
• the lingual expansion of the jaw makes film packet placement difficult, so it has had to be severely tilted away from the root apices;
• failure to take account of these two factors when positioning and angling the X-ray tubehead.
Radiological differential diagnosis� What is your principal differential diagnosis?
1. ameloblastoma
2. Giant cell lesion.
� Justify this differential diagnosis.
Ameloblastoma classically produces an expanding multilocular radiolucency at the angle of the mandible.
Fig. 2.2 Oblique lateral view.
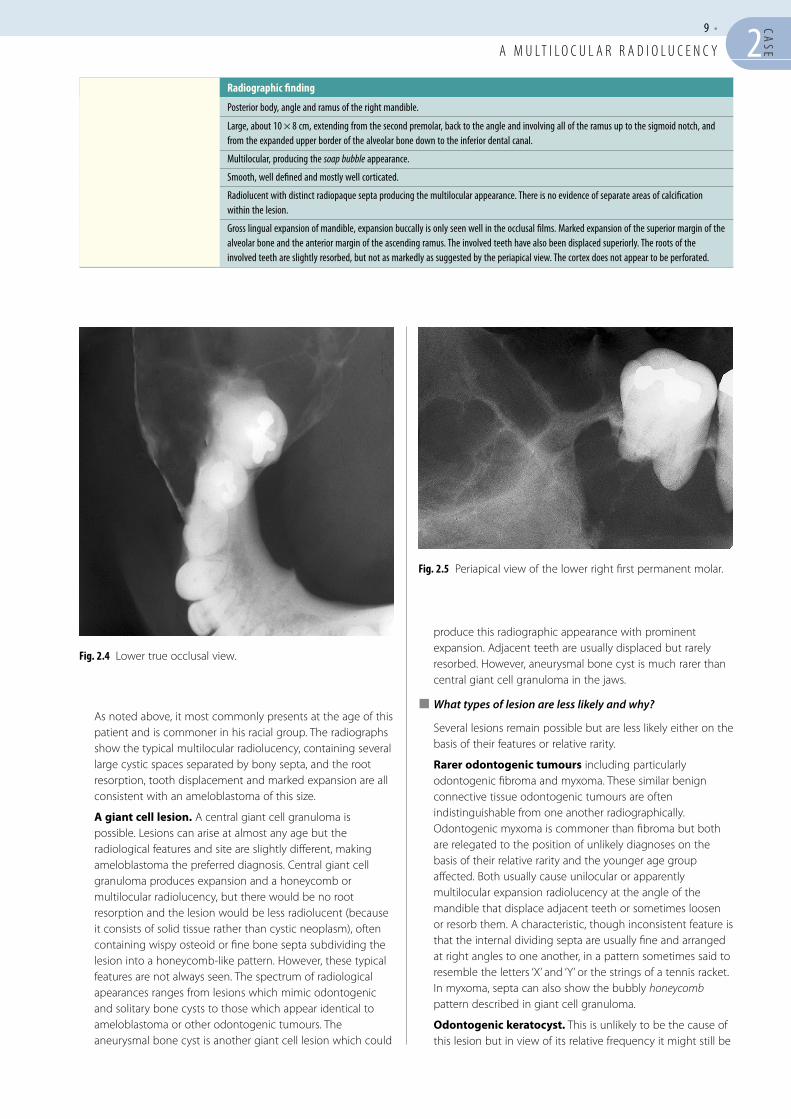
Fig. 2.3 Posterior-anterior view of the jaws.
Radiographic view Reason
Panoramic radiograph or an oblique lateral
To show the lesion from the lateral aspect. The oblique lateral would provide the better resolution but might not cover the anterior extent of this large lesion. The panoramic radiograph would provide a useful survey of the rest of the jaws but only that part of this expansile lesion in the line of the arch will be in focus. An oblique lateral view was taken.
A posterior-anterior (PA) of the jaws To show the extent of mediolateral expansion of the posterior body, angle or ramus.
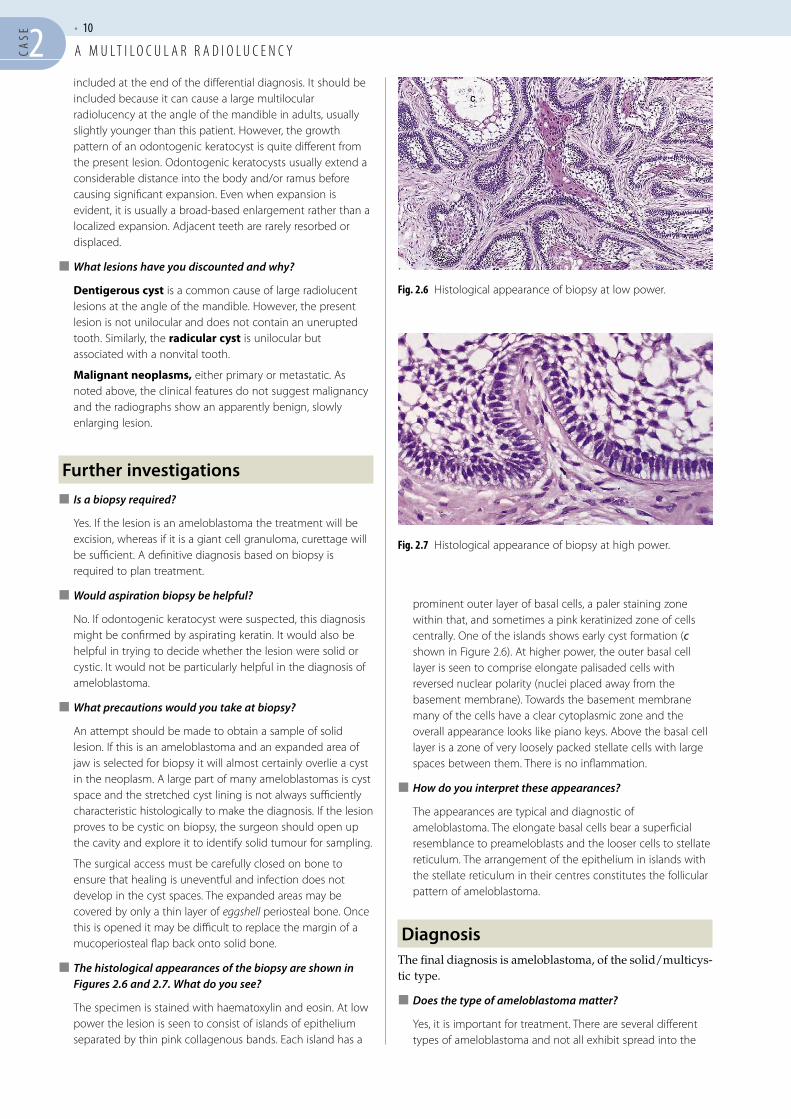
A lower true (90°) occlusal To show the lingual expansion which will not be visible in the PA jaws view because of superimposition of the anterior body of the mandible.
A periapical of the lower right second premolar and the first molar
To assess bone support and possible root resorption.
G
A m u l t i l o c u l A r r A d i o l u c e n c y
9 • 2CA
SE
produce this radiographic appearance with prominent expansion. adjacent teeth are usually displaced but rarely resorbed. However, aneurysmal bone cyst is much rarer than central giant cell granuloma in the jaws.
� What types of lesion are less likely and why?
Several lesions remain possible but are less likely either on the basis of their features or relative rarity.
rarer odontogenic tumours including particularly odontogenic fibroma and myxoma. These similar benign connective tissue odontogenic tumours are often indistinguishable from one another radiographically. Odontogenic myxoma is commoner than fibroma but both are relegated to the position of unlikely diagnoses on the basis of their relative rarity and the younger age group affected. Both usually cause unilocular or apparently multilocular expansion radiolucency at the angle of the mandible that displace adjacent teeth or sometimes loosen or resorb them. a characteristic, though inconsistent feature is that the internal dividing septa are usually fine and arranged at right angles to one another, in a pattern sometimes said to resemble the letters ‘X’ and ‘Y’ or the strings of a tennis racket. in myxoma, septa can also show the bubbly honeycomb pattern described in giant cell granuloma.
Odontogenic keratocyst. This is unlikely to be the cause of this lesion but in view of its relative frequency it might still be
as noted above, it most commonly presents at the age of this patient and is commoner in his racial group. The radiographs show the typical multilocular radiolucency, containing several large cystic spaces separated by bony septa, and the root resorption, tooth displacement and marked expansion are all consistent with an ameloblastoma of this size.
A giant cell lesion. a central giant cell granuloma is possible. Lesions can arise at almost any age but the radiological features and site are slightly different, making ameloblastoma the preferred diagnosis. Central giant cell granuloma produces expansion and a honeycomb or multilocular radiolucency, but there would be no root resorption and the lesion would be less radiolucent (because it consists of solid tissue rather than cystic neoplasm), often containing wispy osteoid or fine bone septa subdividing the lesion into a honeycomb-like pattern. However, these typical features are not always seen. The spectrum of radiological apearances ranges from lesions which mimic odontogenic and solitary bone cysts to those which appear identical to ameloblastoma or other odontogenic tumours. The aneurysmal bone cyst is another giant cell lesion which could
Fig. 2.4 Lower true occlusal view.
Fig. 2.5 Periapical view of the lower right first permanent molar.
Feature of lesion Radiographic finding
Site Posterior body, angle and ramus of the right mandible.
Size Large, about 10 × 8 cm, extending from the second premolar, back to the angle and involving all of the ramus up to the sigmoid notch, and from the expanded upper border of the alveolar bone down to the inferior dental canal.
Shape Multilocular, producing the soap bubble appearance.
Outline/edge Smooth, well defined and mostly well corticated.
Relative radiodensity Radiolucent with distinct radiopaque septa producing the multilocular appearance. There is no evidence of separate areas of calcification within the lesion.
Effects on adjacent structures Gross lingual expansion of mandible, expansion buccally is only seen well in the occlusal films. Marked expansion of the superior margin of the alveolar bone and the anterior margin of the ascending ramus. The involved teeth have also been displaced superiorly. The roots of the involved teeth are slightly resorbed, but not as markedly as suggested by the periapical view. The cortex does not appear to be perforated.
G
A m u l t i l o c u l A r r A d i o l u c e n c y
• 102CASE
prominent outer layer of basal cells, a paler staining zone within that, and sometimes a pink keratinized zone of cells centrally. One of the islands shows early cyst formation (c shown in Figure 2.6). at higher power, the outer basal cell layer is seen to comprise elongate palisaded cells with reversed nuclear polarity (nuclei placed away from the basement membrane). Towards the basement membrane many of the cells have a clear cytoplasmic zone and the overall appearance looks like piano keys. above the basal cell layer is a zone of very loosely packed stellate cells with large spaces between them. There is no inflammation.
� How do you interpret these appearances?
The appearances are typical and diagnostic of ameloblastoma. The elongate basal cells bear a superficial resemblance to preameloblasts and the looser cells to stellate reticulum. The arrangement of the epithelium in islands with the stellate reticulum in their centres constitutes the follicular pattern of ameloblastoma.
DiagnosisThe final diagnosis is ameloblastoma, of the solid/multicys-tic type.
� Does the type of ameloblastoma matter?
Yes, it is important for treatment. There are several different types of ameloblastoma and not all exhibit spread into the
included at the end of the differential diagnosis. it should be included because it can cause a large multilocular radiolucency at the angle of the mandible in adults, usually slightly younger than this patient. However, the growth pattern of an odontogenic keratocyst is quite different from the present lesion. Odontogenic keratocysts usually extend a considerable distance into the body and/or ramus before causing significant expansion. Even when expansion is evident, it is usually a broad-based enlargement rather than a localized expansion. adjacent teeth are rarely resorbed or displaced.
� What lesions have you discounted and why?
Dentigerous cyst is a common cause of large radiolucent lesions at the angle of the mandible. However, the present lesion is not unilocular and does not contain an unerupted tooth. Similarly, the radicular cyst is unilocular but associated with a nonvital tooth.
malignant neoplasms, either primary or metastatic. as noted above, the clinical features do not suggest malignancy and the radiographs show an apparently benign, slowly enlarging lesion.
Further investigations� Is a biopsy required?
Yes. if the lesion is an ameloblastoma the treatment will be excision, whereas if it is a giant cell granuloma, curettage will be sufficient. a definitive diagnosis based on biopsy is required to plan treatment.
� Would aspiration biopsy be helpful?
No. if odontogenic keratocyst were suspected, this diagnosis might be confirmed by aspirating keratin. it would also be helpful in trying to decide whether the lesion were solid or cystic. it would not be particularly helpful in the diagnosis of ameloblastoma.
� What precautions would you take at biopsy?
an attempt should be made to obtain a sample of solid lesion. if this is an ameloblastoma and an expanded area of jaw is selected for biopsy it will almost certainly overlie a cyst in the neoplasm. a large part of many ameloblastomas is cyst space and the stretched cyst lining is not always sufficiently characteristic histologically to make the diagnosis. if the lesion proves to be cystic on biopsy, the surgeon should open up the cavity and explore it to identify solid tumour for sampling.
The surgical access must be carefully closed on bone to ensure that healing is uneventful and infection does not develop in the cyst spaces. The expanded areas may be covered by only a thin layer of eggshell periosteal bone. Once this is opened it may be difficult to replace the margin of a mucoperiosteal flap back onto solid bone.
� The histological appearances of the biopsy are shown in Figures 2.6 and 2.7. What do you see?
The specimen is stained with haematoxylin and eosin. at low power the lesion is seen to consist of islands of epithelium separated by thin pink collagenous bands. Each island has a
Fig. 2.6 Histological appearance of biopsy at low power.
Fig. 2.7 Histological appearance of biopsy at high power.
G
A m u l t i l o c u l A r r A d i o l u c e n c y
11 • 2CA
SE
in place to avoid the need for full thickness resection of the mandible and a bone graft. This causes a low risk of recurrence, but such recurrences are slow growing and may be dealt with conservatively after the main portion of the mandible has healed. The fact that the ameloblastoma is of the follicular pattern is of no significance for treatment.
� What other imaging investigations would be appropriate for this patient?
in order to plan the resection accurately, the extent of the tumour and any cortical perforations must be identified. Cone beam computed tomography (CBCT, computed tomography (CT) and/or magnetic resonance imaging (Mri) would show the full extent of the lesion in bone and surrounding soft tissue respectively.
surrounding medullary cavity. Their characteristics are shown in table 2.1.
Treatment
� What treatment will be required?
The ameloblastoma is classified as a benign neoplasm. However, it is locally infiltrative and in some cases permeates the medullary cavity around the main tumour margin. ameloblastoma should be excised with a 1 cm margin of normal bone and around any suspected perforations in the cortex. if ameloblastoma has escaped from the medullary cavity, it may spread extensively in the soft tissues and requires excision with an even larger margin. The lower border of the mandible may be intact and is sometimes left
Table 2.1 Types of ameloblastoma
Type Features Invades surrounding bone?
solid/multicystic the conventional and commonest type.usually contains multiple cysts and has a multilocular radiographic appearance. plexiform, follicular and mixed histological variants exist but have no bearing on behaviour or treatment.
yes, in a quarter or less of cases
unicystic An ameloblastoma with only one cyst cavity and no separate islands of tumour, or just a few limited to the inner part of the fibrous wall. presents radiographically as a cyst, sometimes in a dentigerous relationship. can only be diagnosed definitively as a unicystic ameloblastoma by complete histological examination after treatment.
no
desmoplastic A rare variant with sparse islands of ameloblastoma dispersed in dense fibrous tissue. radiographically forms a fine honeycomb radiolucency that may resemble a fibro-osseous lesion with a margin that is difficult to define. no large cysts are present. As frequent in the maxilla as in the mandible.
yes, in most cases
peripheral A solid/multicystic ameloblastoma that develops as a soft tissue nodule outside bone, usually on the gingiva. usually detected when small and readily excised. this variant is very rare.
no (the lesion is outside bone)

G
This page intentionally left blank


![TX 1:ABS~AT/TX 2:ABS~AT€¦ · revealed severe attrition of the right lower first molar [Figure 1]. Radiographic examination showed radiolucency involving enamel, dentin, and pulp](https://img.pdfslide.us/doc/110x75/5f036bee7e708231d409203f/tx-1absattx-2absat-revealed-severe-attrition-of-the-right-lower-first-molar.jpg)


























