Embed Size (px)
Citation preview

Results: A total of 88 EPIs were evaluated. The mean systematic displacements of endorectal balloon to bony landmark were1.0 mm in anterior-posterior (AP), 2.2 mm in superior-inferior (SI), and 0.6 mm in left-right (LR) directions, respectively (Table1). The random (interfraction) error was greater in SI direction (4.3 mm) than that in AP (3.4 mm) and LR (3.0 mm) direction.In displacement of balloon to treatment isocenter, a larger random error was observed in SI (4.1 mm) and AP (4.2 mm)directions, compared with that in LR directions (2.9 mm). During the whole treatment course, a larger variation in balloondiameter in SI view (2.2 mm) was observed, compared with that in AP (2.0 mm) and LR views (1.8 mm).
Conclusions: On EPIs, a larger interfraction displacement of endorectal balloon was evident in SI direction during the treatmentcourse. Similarly, a greater deformation of balloon in SI directions was shown in variation of balloon diameter. A setupuncertainty in placing endorectal balloon with 5 mm or less seems acceptable in treatment design.
Author Disclosure: C.W. Wang, None; J.K. Wu, None; J.C. Cheng, None.
2774 The Use of Image Registration and a Head Frame With Dental Block Assembly for Non-InvasiveRadiosurgery/Radiotherapy
A. S. Shiu, C. Wang, S. Y. Woo, E. L. Chang, A. Mahajan, C. H. Wang
M.D. Anderson Cancer Center, Houston, TX
Purpose/Objective(s): Stereotactic radiosurgery (SRS) delivers a high-dose during a single session to shrink or destroy tumorsand vascular malformations of the brain. Because a single radiosurgery dose is more damaging than multiple fractionatedradiotherapy doses, the target area must be precisely located and completely immobilized with a stereotactic head frame. Thedownside of this procedure is the fixation of the head frame to the patient’s skull is invasive and painful for the patient. Thepatient also has to wear the head ring till the treatment is delivered. The objective of this study is to demonstrate that the useof image registration and a non-invasive head frame for SRS can achieve the same accuracy as the current invasive head-ringSRS technique.
Materials/Methods: First, a head phantom was used to evaluate the accuracy of this procedure for aiming the target. Then, twoSRT patients fixed with the GTC frame were treated with the proposed technique for ten treatments. The five-point GTCalignment device was used to aid the repositioning of the GTC frame with respect of the original setup. This alignment deviceminimized the misalignment of the GTC frame in AP, lateral, and axial translations and the angular deviations about each ofthese axes on roll, tilt, and spin. Prior to each treatment, a daily CT scan with a localization device was acquired. Daily CTimages were registered with planning CT and MRI images. The 9 rods on the daily CT images were then identified, such thatall the target, critical structures, and external contours from the planning images were transferred to the daily stereotacticcoordinates. A new plan was generated.
Results: In the head phantom study, the daily isocenter setup was verified to be within 0.2 mm accuracy based upon the portalimages verse the planned DRRs. Optimized the dose distributions for each daily CT images of ten SRT treatments, the meandeviations of the daily isocenter from the planned isocenter were 0.2�0.12, -0.4�0.24, and -0.1�0.07 mm in AP-, LAT-, andVERT-direction, respectively. For each treatment, the daily isocenter was updated on the laser-target localization-frame to aimthe target-isocenter correctly. The comparison of dose-volume histograms was clearly revealed the prescribed dose enclosed thePTV for every treatment as that of the treatment plan.
Conclusions: The image-guided noninvasive frame SRS has the capability of delivering high level accuracy of dose to thelesion without the discomfort from the pins fixed to the patient’s skull. In addition, the patient doesn’t have to wear the frametill the treatment time; it can be in the same day or the next day.
Author Disclosure: A.S. Shiu, None; C. Wang, None; S.Y. Woo, None; E.L. Chang, None; A. Mahajan, None; C.H. Wang,None.
2775 High Accuracy of the 3D Volumetric Image Registration: Correction of Misalignment in Cranial PET/CTImages Due to Patient Movement for Stereotactic Treatment Planning
G. Li, H. Xie, H. Ning, D. Citrin, J. Capala, P. Guion, B. Arora, K. Camphausen, N. Coleman, R. Miller
National Cancer Institute/NIH, Bethesda, MD
Purpose/Objective(s): Patient head movement can be as much as 1–3 mm in a head holder during the hybrid PET/CT scans.This misalignment in the PET/CT images should be corrected for stereotactic treatment planning.
Materials/Methods: The 3D volumetric image registration is a volume-view-guided image registration, using anatomicalvolumetric registration landmarks based on their color homogeneity among mono-colored images of up to four imagingmodalities. The color homogeneity can be visualized and quantified using the uniformity of the intensity difference of the
Table 1: Balloon displacements relative to bony landmark and treatment isocenter
Balloon-Bone Balloon-Isocenter
Systematic(Mean, mm)
Random(SD, mm)
Systematic(Mean, mm)
Random(SD, mm)
Superio-Inferior (SI) 2.2 4.3 5.4 4.1Anterio-Posterior (AP) 1.0 3.4 2.2 4.2Left-Right (LR) 0.6 3.0 2.5 2.9
S643Proceedings of the 48th Annual ASTRO Meeting

viewing voxels as the cost function. As a comparison, mutual information is applied for patient image registration. To test theaccuracy of the 3D volumetric image registration technique, three head phantoms were used to acquire CT, MR and PET/CTimages with lateral shifts of 0.0, 5.0, 10.0 and 15.0 mm on the scanner couches and compared with the image registration shifts.For patient head movement studies, 14 patient cranial MR (T1/T2/FLAIR) images acquired from the same scanner and 18patient cranial PET/CT images acquired in the hybrid scanner were used and compared with the 3D volumetric registrationresults.
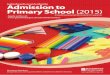
Results: Based on the head phantom studies, 0.1 mm accuracy is achieved for anatomic (CT/CT and MR/MR) images and 0.5mm accuracy is achieved for PET/CT images. Based on the 14 patient MR/MR image registration results, the average patientmovements during two consecutive scans are 0.4�0.4 mm in translation and 0.2°�0.4° in rotation. Based on the 18 patientPET/CT image registration results, the average patient movements are 0.7�0.4 mm in translation and 0.4°�0.5° in rotation.One patient example is shown in Figure 1. In the patient studies, the largest misalignment observed is 1.6 mm in translationand 1.5° in rotation, which is similar to the setup error in stereotactic radiotherapy/radiosurgery.
Conclusions: The 3D volumetric image registration method is useful in detecting and correcting small misalignment error incranial PET/CT images, and should be used for quality assurance, especially for stereotactic radiation treatment.
Figure 1: The color homogeneity of PET/CT cranial images is improved from (A) to (B) and (C), where the PET image isin red, and CT image is in green, light blue and yellow, respectively. (A) The original PET/CT images, (B) the registered imagesusing mutual information and (C) the registered images using 3D volumetric views. The color inhomogeneity in the orbital/noseregion is due to the low-resolution artifact at high curvature area of the PET image. Also, some bone facial bone structures areshown where little PET signal is available.
Author Disclosure: G. Li, None; H. Xie, None; H. Ning, None; D. Citrin, None; J. Capala, None; P. Guion, None; B. Arora,None; K. Camphausen, None; N. Coleman, None; R. Miller, None.
2776 Automated Registration and Correction of Patient Positioning for IGRT and Body Radiosurgery Usingthe Novalis “ExacTrac” System
R. M. Macklis, C. Robinson, T. Djemil
Cleveland Clinic Foundation, Cleveland, OH
Purpose/Objective(s): Radiation Medicine is now incorporating more sophisticated degrees of automation in its technologicprogression towards an Image-Guided Radiation Therapy (IGRT) treatment paradigm. This is especially true for stereotacticbody radiosurgery (SBR) and similar focal approaches to beam targeting. As the IGRT/SBR paradigm evolves, we are relyingless on skin marks in daily patient set-up. Instead, internal fiducials such as radioopaque anatomic structures or implantedmarkers are used as proxies for positional target registration. Phantom studies have shown that the combination of trackable skinmarkers and internal fiducials produce targeting accuracies on the order of �/- 1 mm. However, real-world usability data forsuch systems are sparse.
We are currently utilizing the BrainLab “ExacTrac” IGRT system for SBR and extracranial stereotactic radiotherapy. Patientsare set up in treatment position based on traditional skin marks correlated to a planning CT. These skin mark positions aretracked daily using 5–7 removable infrared reflector markers affixed to the most informative and stable skin sites. The initialset-up is made using these reflector markers followed by correction to a final position based on orthogonal high resolution X-rayimages of internal fiducials or bony anatomy acquired prior to treatment and used to validate final treatment coordinates. Finaltargeting coordinates are based on near-real-time X-ray images of informative markers. We have analyzed a representativeclinical dataset indicating the magnitude of the positional discordances between original skin mark target position vs. the finalinternal fiducial position and analyzed patterns seen in a representative set of over 100 measurements obtained in 13 extracranialIGRT patients. These data are of interest because they give some indication of daily radiotherapy set-up reproducibility and thedegree of positional modification necessary when final treatment coordinates are corrected based on internal markers in areal-world situation.
Materials/Methods: Patients were divided into tumor groups: Head/Neck (N � 4) Lung (N � 3) Trunk (N � 3) and Spine(N � 3). H/N immobilization was accomplished using an ORFIT mask, while body immobilization was accomplished usingthe BODYFIX system. The center of mass was calculated for each target prior to treatment based on the x,y,z positionalinformation obtained from the internal markers. The ExacTrac system was used to calculate and automatically adjust patientpositioning. Data presented here represent the absolute magnitude of the shifts (mean �/- SD) for the center of mass for thetarget.
Results: For H/N sites, correction shifts were within 1–2 (�/- 1) mm of original skin mark set-up. For Spine sites, shifts weremuch larger (approx. 2–9 (�/- 8) mm. For Trunk and Lung cases, shifts were intermediate (in the range of 2–7 (�/- 2) mm.The automated system typically added less than 5 minutes to daily clinical treatment times.
Conclusions: This real-world usability analysis confirmed the utility and applicability of the ExacTrac IGRT positioningsystem for extracranial SBR cases for a broad range of target sites. The combination of trackable infrared skin markers andin-room high-resolution orthogonal X-ray imagers represents a facile and robust automated solution to set-up challenges inclinical IGRT and body radiosurgery.
Author Disclosure: R.M. Macklis, Brainlab, D. Speakers Bureau/Honoraria; C. Robinson, None; T. Djemil, None.
S644 I. J. Radiation Oncology ● Biology ● Physics Volume 66, Number 3, Supplement, 2006