Embed Size (px)
Citation preview

2772 Comparison of Daily Couch Shifts Using MVCT (TomoTherapy) and B-Mode Ultrasound (BAT System)During Prostate Radiotherapy
S. H. Lin, E. Sugar, H. Saleh, T. Teslow, T. McNutt, T. L. DeWeese, J. Wong, D. Song
Department of Radiation Oncology and Molecular Radiation Sciences, The Johns Hopkins University School of Medicine,Baltimore, MD
Purpose/Objective(s): Image-guided radiation therapy with CT- or ultrasound-based systems are commonly used to adjust forsetup error and organ position variability in patients treated for prostate cancer. Despite their widespread use, no directcomparisons have been made to elucidate potential differences between modalities. This study compares the daily patient shiftsfor prostate localization between megavoltage CT (MVCT, Hi-ART TomoTherapy) and b-mode ultrasound (BAT system)performed at a single institution.
Materials/Methods: Twenty-two consecutive patients with prostate cancer treated with TomoTherapy employing daily MVCTfor prostate localization were compared to 23 randomly selected patients treated on a standard linear accelerator using dailyb-mode ultrasound prostate localization with the BAT system. The two groups were not statistically different from each otherwith respect to clinical stage or initial prostate, bladder, or rectal volumes. All patients were initially aligned to isocenter usingskin marks. Couch shifts were made in all three principle axes based on prostate position after comparing daily images to theinitial planning CT images. Negative values were assigned for couch shifts in the left, down, and inferior (out) directions. Themean shift for each axis and the shift variability within individual subjects were calculated using replicate measurements.Pairwise correlations between shifts were calculated for each individual and a Bonferroni correction is used to adjust formultiple comparisons, � � 0.0167.
Results: The table below presents the between subject variability as the mean shifts for each individual of the entire cohort (part1) and the within subject variance as the variability of the repeated daily shift measurements for each individual (part 2). Wefind the variability within replicate measures to be significantly higher for the BAT-localized group compared to theTomoTherapy MVCT-localized group for vertical and SI shifts (p-values: 0.0084 and 0.01037, respectively). For eachindividual, the pairwise correlations between shifts were calculated. Among all the groups and pairings, only the pairing ofVertical and SI adjustments in BAT-localized patients showed significant evidence of correlation (p�0.0006).
Conclusions: Our results likely reflect differences in the ability to precisely align b-mode ultrasound contours to KVCT images,as well as prostate excursion in vertical and SI direction caused by the ultrasound probe. These considerations need to be madewhen defining treatment volumes and argue for incorporation of less disruptive ultrasound-based scanning techniques.
Author Disclosure: S.H. Lin, None; E. Sugar, None; H. Saleh, None; T. Teslow, None; T. McNutt, None; T.L. DeWeese, None;J. Wong, None; D. Song, None.
2773 Setup Errors for Placement of Endorectal Balloon for Prostate Radiotherapy
C. W. Wang, J. K. Wu, J. C. Cheng
Division of Radiation Oncology, Department of Oncology, National Taiwan University Hospital and National TaiwanUniversity College of Medicine, Taipei, Taiwan, Province of China
Purpose/Objective(s): Prostate motion and the effective reduction by endorectal balloon during radiotherapy have been theimportant issues. However, the placement accuracy of endorectal balloon itself has seldom been addressed. This study wasaimed to investigate the setup errors in daily placement of endorectal balloon in prostate radiotherapy.
Materials/Methods: Twelve prostate cancer patients treated with intensity-modulated radiotherapy (78Gy in daily fraction of2Gy) were included in this study. Daily placement of endorectal balloon under uniform instruction was used for prostateimmobilization and rectal sparing in dosimetry. Electronic portal images (EPIs) were collected weekly from anterior-posteriorand lateral opposing views for each patient. The EPIs was compared with digital reconstructed radiographs of computedtomography on pretreatment simulation to obtain the displacements between endorectal balloon, bony landmark, and treatmentisocenter. The systematic and random errors were calculated for the three orthogonal directions separately. The mean systemicerror was defined as the average displacement of measurements in all patients. The random error was defined as the averagedstandard deviation (SD) of displacement for each patient, showing the random fraction-to-fraction variations of balloonplacement. The interfraction deformation of balloon during treatment was estimated by the variations of diameter in 3orthogonal directions.
S642 I. J. Radiation Oncology ● Biology ● Physics Volume 66, Number 3, Supplement, 2006
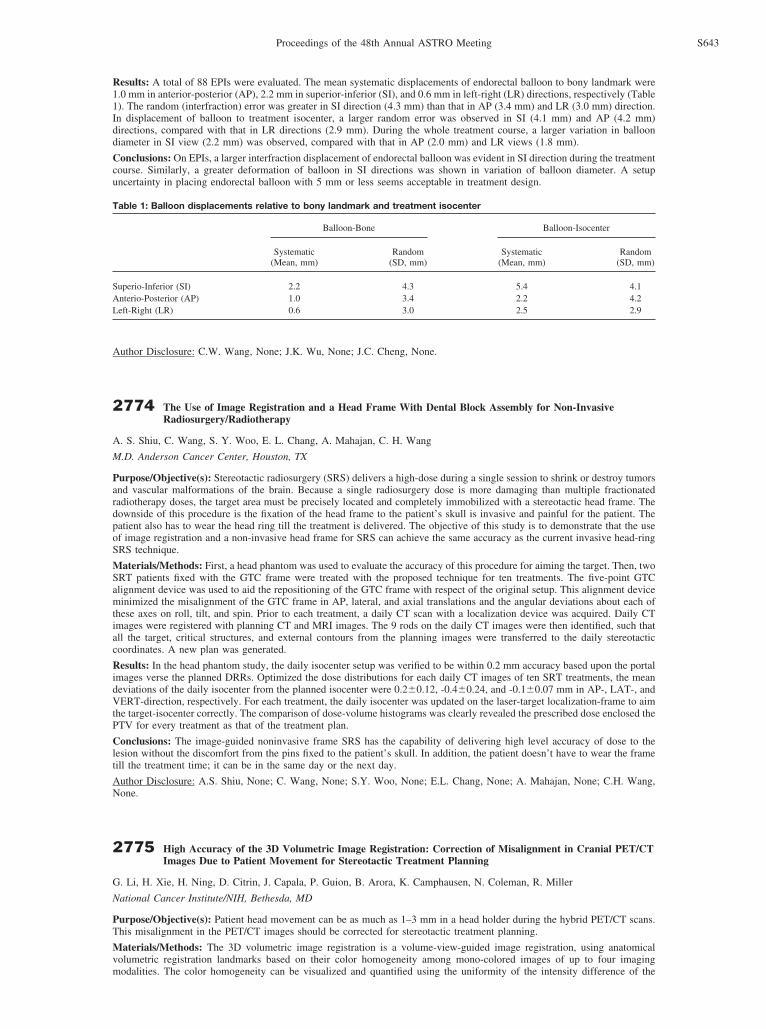
Results: A total of 88 EPIs were evaluated. The mean systematic displacements of endorectal balloon to bony landmark were1.0 mm in anterior-posterior (AP), 2.2 mm in superior-inferior (SI), and 0.6 mm in left-right (LR) directions, respectively (Table1). The random (interfraction) error was greater in SI direction (4.3 mm) than that in AP (3.4 mm) and LR (3.0 mm) direction.In displacement of balloon to treatment isocenter, a larger random error was observed in SI (4.1 mm) and AP (4.2 mm)directions, compared with that in LR directions (2.9 mm). During the whole treatment course, a larger variation in balloondiameter in SI view (2.2 mm) was observed, compared with that in AP (2.0 mm) and LR views (1.8 mm).
Conclusions: On EPIs, a larger interfraction displacement of endorectal balloon was evident in SI direction during the treatmentcourse. Similarly, a greater deformation of balloon in SI directions was shown in variation of balloon diameter. A setupuncertainty in placing endorectal balloon with 5 mm or less seems acceptable in treatment design.
Author Disclosure: C.W. Wang, None; J.K. Wu, None; J.C. Cheng, None.
2774 The Use of Image Registration and a Head Frame With Dental Block Assembly for Non-InvasiveRadiosurgery/Radiotherapy
A. S. Shiu, C. Wang, S. Y. Woo, E. L. Chang, A. Mahajan, C. H. Wang
M.D. Anderson Cancer Center, Houston, TX
Purpose/Objective(s): Stereotactic radiosurgery (SRS) delivers a high-dose during a single session to shrink or destroy tumorsand vascular malformations of the brain. Because a single radiosurgery dose is more damaging than multiple fractionatedradiotherapy doses, the target area must be precisely located and completely immobilized with a stereotactic head frame. Thedownside of this procedure is the fixation of the head frame to the patient’s skull is invasive and painful for the patient. Thepatient also has to wear the head ring till the treatment is delivered. The objective of this study is to demonstrate that the useof image registration and a non-invasive head frame for SRS can achieve the same accuracy as the current invasive head-ringSRS technique.
Materials/Methods: First, a head phantom was used to evaluate the accuracy of this procedure for aiming the target. Then, twoSRT patients fixed with the GTC frame were treated with the proposed technique for ten treatments. The five-point GTCalignment device was used to aid the repositioning of the GTC frame with respect of the original setup. This alignment deviceminimized the misalignment of the GTC frame in AP, lateral, and axial translations and the angular deviations about each ofthese axes on roll, tilt, and spin. Prior to each treatment, a daily CT scan with a localization device was acquired. Daily CTimages were registered with planning CT and MRI images. The 9 rods on the daily CT images were then identified, such thatall the target, critical structures, and external contours from the planning images were transferred to the daily stereotacticcoordinates. A new plan was generated.
Results: In the head phantom study, the daily isocenter setup was verified to be within 0.2 mm accuracy based upon the portalimages verse the planned DRRs. Optimized the dose distributions for each daily CT images of ten SRT treatments, the meandeviations of the daily isocenter from the planned isocenter were 0.2�0.12, -0.4�0.24, and -0.1�0.07 mm in AP-, LAT-, andVERT-direction, respectively. For each treatment, the daily isocenter was updated on the laser-target localization-frame to aimthe target-isocenter correctly. The comparison of dose-volume histograms was clearly revealed the prescribed dose enclosed thePTV for every treatment as that of the treatment plan.
Conclusions: The image-guided noninvasive frame SRS has the capability of delivering high level accuracy of dose to thelesion without the discomfort from the pins fixed to the patient’s skull. In addition, the patient doesn’t have to wear the frametill the treatment time; it can be in the same day or the next day.
Author Disclosure: A.S. Shiu, None; C. Wang, None; S.Y. Woo, None; E.L. Chang, None; A. Mahajan, None; C.H. Wang,None.
2775 High Accuracy of the 3D Volumetric Image Registration: Correction of Misalignment in Cranial PET/CTImages Due to Patient Movement for Stereotactic Treatment Planning
G. Li, H. Xie, H. Ning, D. Citrin, J. Capala, P. Guion, B. Arora, K. Camphausen, N. Coleman, R. Miller
National Cancer Institute/NIH, Bethesda, MD
Purpose/Objective(s): Patient head movement can be as much as 1–3 mm in a head holder during the hybrid PET/CT scans.This misalignment in the PET/CT images should be corrected for stereotactic treatment planning.
Materials/Methods: The 3D volumetric image registration is a volume-view-guided image registration, using anatomicalvolumetric registration landmarks based on their color homogeneity among mono-colored images of up to four imagingmodalities. The color homogeneity can be visualized and quantified using the uniformity of the intensity difference of the
Table 1: Balloon displacements relative to bony landmark and treatment isocenter
Balloon-Bone Balloon-Isocenter
Systematic(Mean, mm)
Random(SD, mm)
Systematic(Mean, mm)
Random(SD, mm)
Superio-Inferior (SI) 2.2 4.3 5.4 4.1Anterio-Posterior (AP) 1.0 3.4 2.2 4.2Left-Right (LR) 0.6 3.0 2.5 2.9
S643Proceedings of the 48th Annual ASTRO Meeting





























