Embed Size (px)
Citation preview

ing decreased viscosity and increased flow (p� 0.04 and 0.04, respec-tively), the PI, RI, and CPP were not correlated within the range stud-ied. The degree of change in Hg and Hct after a routine delivery wasnot significantly associated with changes in PSV, MDV, PI, RI, CPP,RAP, or CPP.CONCLUSION: We have established that delivery related blood loss of �1000ml is not likely to be associated with significant cerebrovascularhemodynamic effects. This suggests that normal healthy women willretain functional cerebral autoregulation with this degree of bloodloss. Future studies on the interplay between postpartum hemorrhageand maternal disease states can now be performed focusing on ma-ternal cerebrovascular hemodynamics.
226 Maternal hemodynamic changes in multiplegestation pregnancy: a longitudinal, pilot studyNoor Niyar Ladhani1, Natasha Milligan2, Jose Carvalho3,Prakesh Shah4, Xiang Ye5, Mary-Jean Martin2,Anne Jordan2, Kellie Murphy6
1University of Toronto, Sunnybrook Health Sciences Centre, Department ofObstetrics and Gynaecology, Toronto, ON, Canada, 2Mt Sinai Hospital,Department of Obstetrics and Gynaecology, Toronto, ON, Canada,3University of Toronto, Mt Sinai Hospital, Departments of Anaesthesia and ofObstetrics and Gyanecology, Toronto, ON, Canada, 4University of Toronto,Mt Sinai Hospital, Departments of Paediatrics and of Health Policy,Management, and Evaluation, Toronto, ON, Canada, 5Mt Sinai Hospital,MICare Research Centre, Toronto, ON, Canada, 6University of Toronto, MtSinai Hospital, Departments of Obstetrics and Gynaecology, and of HealthPolicy, Management, and Evaluation, Toronto, ON, CanadaOBJECTIVE: Maternal hemodynamic parameters change significantlyduring pregnancy. These changes are exaggerated in pregnancies in-volving multiple gestations. Cardiac output is thought to increasethrough gestation and return to baseline in the postpartum period.The extent of this change and the timing of return to baseline are notwell characterized. We sought to longitudinally assess the changes inmaternal cardiovascular hemodynamics in women with singletons,twins, and triplets, throughout gestation and in the postpartumperiod.STUDY DESIGN: Women were recruited in the first trimester and he-modynamic variables were measured at four points: 10-14 weeks,24-28 weeks, 32-26 weeks, and 4-8 weeks postpartum. Measurementswere obtained in twenty women using a bioreactance-based non-in-vasive cardiac output monitor, the use of which has been validated inpregnancy.RESULTS: Cardiac output rose during pregnancy, peaking in twinpregnancies (n�5) at the 24-28 week visit, and in singleton (n�10)and triplet (n�5) pregnancies at the 32-36 week visit. The medianpeak cardiac output was highest in the triplet group (8.44 L/min).Postpartum cardiac output remained higher in the triplet group (6.08L/min), than in the twin and singleton groups (4.53 L/min and 5.08L/min). The percent change in cardiac output between the first tri-mester and the postpartum visit was highest in the triplet group(92%), compared to the twin and singleton groups (21% and 53%).CONCLUSION: Cardiac output increased through gestation and peakedin the late second or third trimester. The return to baseline was slowerin the multiple gestation groups. The percent change between the firstvisit and the postpartum visit was highest in the triplet group, showinga slower recovery to maternal baseline. The results of this pilot, pro-spective longitudinal study display the cardiovascular stress imposedon women into the postpartum period and gives insight into the he-modynamic changes that occur in multiple gestation pregnancies.
227 Maternal hemodynamics by impedance cardiographyfor normal pregnancy before and after vaginal or cesareandeliveryRachael Morris1, Laura Rush1, Pamela Blake1, Belinda Ellis1,Imran Sunesara2, Marie Darby1, Justin Brewer1, James Martin1
1University of Mississippi Medical Center, Obstetrics and Gynecology,Jackson, MS, 2University of Mississippi Medical Center, Biostatistics,Jackson, MSOBJECTIVE: Impedance cardiography (ICG) is a non-invasive, vali-dated method to accurately assess maternal hemodynamics. We de-sired to establish normative values for pregnancy during the secondand third trimester and 24 to 48 hours postpartum; these data providea basis to compare values obtained in hypertensive/cardiac pregnantpatients.STUDY DESIGN: Prospective observational study of normotensivepregnant patients (n�168) using Cardiodynamics/Sonosite imped-ance cardiography performed at specific times during gestation. An-tepartum testing was done at (a) 20-27 weeks, (b) 28-33 weeks, and (c)34-40 weeks. Postpartum testing was done in four groups of patients:(e) 6-23 hours after vaginal delivery; (f) 24-48 hours after vaginaldelivery; (g) 6-23 hours postcesarean; and (h) 24-48 hours postcesar-ean; 25 patients were recruited for each of the 7 groups. Hemody-namic as well as demographic and obstetric/neonatal data were re-corded for all patients. Data analysis performed using STATAsoftware package.RESULTS: Maternal cardiac output (CO) and heart rate (HR) are notedto increase with advancing gestation; both decrease during the first 48hours postpartum (see table). Maternal mean arterial pressure (MAP)and the systemic vascular resistance index (SVRI) both increased overthe course of gestation and were sustained for 48 hours postpartum inthese normotensive parturients. Thoracic fluid content (TFC) in-creased immediately postpartum in normotensive patients followingvaginal and cesarean delivery.CONCLUSION: These ICG data from normotensive pregnant patientsbefore and immediately following vaginal or cesarean delivery pro-vide normative baseline information for comparing data obtained inhypertensive or otherwise complicated pregnant patients during thesecond half of pregnancy and immediately postpartum (48 hours).
228 Micro PET imaging in pregnancy: acute andchronic maternal nutrient availability altersin vivo fetal and tissue glucose uptakeScarlett Karakash1, Hye Heo1, Wade Koba2, Yongmei Zhao1,Allison Berdichevsky1, Eugene Fine2, Francine Einstein1
1Montefiore Medical Center/Albert Einstein College of Medicine, Obstetrics& Gynecology and Women’s Health, Bronx, NY, 2Montefiore MedicalCenter/Albert Einstein College of Medicine, Nuclear Medicine, Bronx, NYOBJECTIVE: Micro Positron Emission Tomography (mPET) is a non-invasive,functional imaging tool used to quantify in vivo tissue glu-cose uptake (GU). Our goal was to measure the effect of chronic ma-ternal diets and acute lipid load on fetal-placental GU and maternalcardiac GU in pregnant dams using mPET.STUDY DESIGN: Four groups of age-matched, female SD rats were stud-ied:1)CON(n�6)standard chow ad libitum, 2) CR(n�9)Calorie Re-striction,pair-fed 60%CON kcal/d of standard chow from D11 of ges-tation, 3) WD(n�7)Western Diet from 3 weeks through gestation,and 4) ALL(n�7) Acute Lipid Load,normal dams fed an oral lipid
Maternal hemodynamics
Poster Session I Clinical Obstetrics, Epidemiology, Fetus, Medical-Surgical Complications, Neonatology, Physiology/Endocrinology, Prematurity www.AJOG.org
S104 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2013
load 4 hours prior to study. On D19 of gestation, dams were given IVradiolabeled 18F-fluorodeoxyglucose to measure tissue GU andmPET was performed. ASIPRO (Siemens) software was used to local-ize regions of interest (ROI), defined as 5 image slices representingmaximum concentration of fetus/placenta. For each animal’s ROI,the mean GU was calculated in SUVs (standard uptake value). A3-point scale quantified maternal cardiac GU (0�none, 1�minimal,2�maximal).RESULTS: CON weighed more than CR (302�8g vs 268�14g,p�0.01)and WD more than Con and ALL(384�9.6g vs 302�8g, 297�18gp�0.01). Pup weight and litter size were similar between groups. CRand WD dams demonstrated increased fetal-placental GU and de-creased maternal cardiac GU compared to CON [Figure]. Similarly, inresponse to acute lipid load, ALL dams had increased fetal-placentalGU with a decrease in maternal cardiac GU [Table].CONCLUSION: Similar to acute lipid load, chronic maternal CR andWD results in increased fetal-placental GU and decreased maternalcardiac GU. These findings suggest that both calorie restriction andchronic high fat feeding in pregnancy induces greater maternal reli-ance on lipid oxidation, therefore making more glucose available fortransport to the fetus. In pregnant models, mPET may be a valuabletool not only to measure in vivo glucose transport, but also transportof other nutrients, such as lipids.
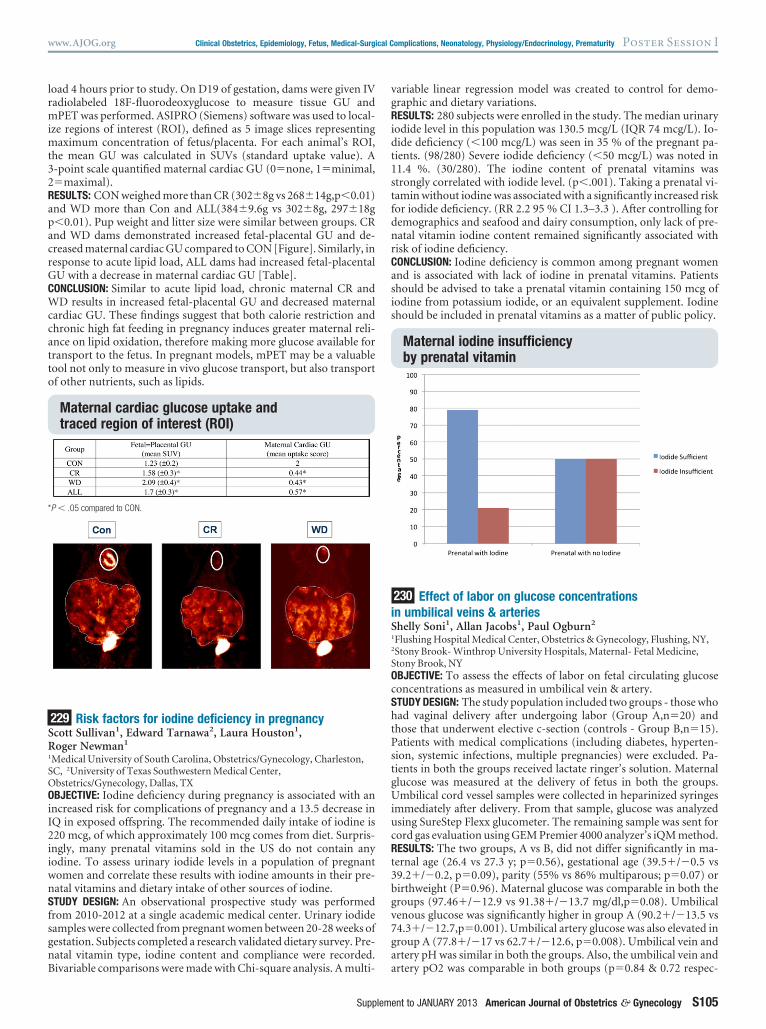
229 Risk factors for iodine deficiency in pregnancyScott Sullivan1, Edward Tarnawa2, Laura Houston1,Roger Newman1
1Medical University of South Carolina, Obstetrics/Gynecology, Charleston,SC, 2University of Texas Southwestern Medical Center,Obstetrics/Gynecology, Dallas, TXOBJECTIVE: Iodine deficiency during pregnancy is associated with anincreased risk for complications of pregnancy and a 13.5 decrease inIQ in exposed offspring. The recommended daily intake of iodine is220 mcg, of which approximately 100 mcg comes from diet. Surpris-ingly, many prenatal vitamins sold in the US do not contain anyiodine. To assess urinary iodide levels in a population of pregnantwomen and correlate these results with iodine amounts in their pre-natal vitamins and dietary intake of other sources of iodine.STUDY DESIGN: An observational prospective study was performedfrom 2010-2012 at a single academic medical center. Urinary iodidesamples were collected from pregnant women between 20-28 weeks ofgestation. Subjects completed a research validated dietary survey. Pre-natal vitamin type, iodine content and compliance were recorded.Bivariable comparisons were made with Chi-square analysis. A multi-
variable linear regression model was created to control for demo-graphic and dietary variations.RESULTS: 280 subjects were enrolled in the study. The median urinaryiodide level in this population was 130.5 mcg/L (IQR 74 mcg/L). Io-dide deficiency (�100 mcg/L) was seen in 35 % of the pregnant pa-tients. (98/280) Severe iodide deficiency (�50 mcg/L) was noted in11.4 %. (30/280). The iodine content of prenatal vitamins wasstrongly correlated with iodide level. (p�.001). Taking a prenatal vi-tamin without iodine was associated with a significantly increased riskfor iodide deficiency. (RR 2.2 95 % CI 1.3–3.3 ). After controlling fordemographics and seafood and dairy consumption, only lack of pre-natal vitamin iodine content remained significantly associated withrisk of iodine deficiency.CONCLUSION: Iodine deficiency is common among pregnant womenand is associated with lack of iodine in prenatal vitamins. Patientsshould be advised to take a prenatal vitamin containing 150 mcg ofiodine from potassium iodide, or an equivalent supplement. Iodineshould be included in prenatal vitamins as a matter of public policy.
230 Effect of labor on glucose concentrationsin umbilical veins & arteriesShelly Soni1, Allan Jacobs1, Paul Ogburn2
1Flushing Hospital Medical Center, Obstetrics & Gynecology, Flushing, NY,2Stony Brook- Winthrop University Hospitals, Maternal- Fetal Medicine,Stony Brook, NYOBJECTIVE: To assess the effects of labor on fetal circulating glucoseconcentrations as measured in umbilical vein & artery.STUDY DESIGN: The study population included two groups - those whohad vaginal delivery after undergoing labor (Group A,n�20) andthose that underwent elective c-section (controls - Group B,n�15).Patients with medical complications (including diabetes, hyperten-sion, systemic infections, multiple pregnancies) were excluded. Pa-tients in both the groups received lactate ringer’s solution. Maternalglucose was measured at the delivery of fetus in both the groups.Umbilical cord vessel samples were collected in heparinized syringesimmediately after delivery. From that sample, glucose was analyzedusing SureStep Flexx glucometer. The remaining sample was sent forcord gas evaluation using GEM Premier 4000 analyzer’s iQM method.RESULTS: The two groups, A vs B, did not differ significantly in ma-ternal age (26.4 vs 27.3 y; p�0.56), gestational age (39.5�/�0.5 vs39.2�/�0.2, p�0.09), parity (55% vs 86% multiparous; p�0.07) orbirthweight (P�0.96). Maternal glucose was comparable in both thegroups (97.46�/�12.9 vs 91.38�/�13.7 mg/dl,p�0.08). Umbilicalvenous glucose was significantly higher in group A (90.2�/�13.5 vs74.3�/�12.7,p�0.001). Umbilical artery glucose was also elevated ingroup A (77.8�/�17 vs 62.7�/�12.6, p�0.008). Umbilical vein andartery pH was similar in both the groups. Also, the umbilical vein andartery pO2 was comparable in both groups (p�0.84 & 0.72 respec-
Maternal cardiac glucose uptake andtraced region of interest (ROI)
*P � .05 compared to CON.
Maternal iodine insufficiencyby prenatal vitamin
www.AJOG.org Clinical Obstetrics, Epidemiology, Fetus, Medical-Surgical Complications, Neonatology, Physiology/Endocrinology, Prematurity Poster Session I
Supplement to JANUARY 2013 American Journal of Obstetrics & Gynecology S105





























