Embed Size (px)
Citation preview
2/12/2018
1
From Evidence-Based Medicine to Evidence-Based CareHALDEN F. SCOTT, MDSepsis Treatment and Recognition ProgramChildren’s Hospital ColoradoAssociate Professor of Pediatrics and Emergency MedicineUniversity of Colorado School of Medicine
This activity is jointly-provided by SynAptiv and the Colorado Hospital
Association
Conflict of Interest Disclosure Statement
• I have no financial interest or other relationships with the industry relative to the topics being discussed.
2/12/2018
2
A Child Arrives in Triage . . .• 4 year old – language barrier
• Won’t drink and has a fever
• Previously healthy
• Seen 14 days prior with febrile illness: treated with oseltamivir (sibling +Flu A)
• Recovered, was back at school
• Now 4 days of new fever, worsening cough
• No urine output in 12 hours
Triage Exam
• T=100 HR:132 RR:30 SpO2: 86%
• Moaning and grabbing abdomen
• Refuses to walk – carried to stretcher
Triage Exam
What do you notice?What do you do?
• T=100 HR:132 RR:30 SpO2: 86%
• Moaning and grabbing abdomen
• Refuses to walk – carried to stretcher
2/12/2018
3
Pop Quiz!What would you do next?
1. Give acetaminophen
2. Provide supplies for oral rehydration
3. Obtain a full set of vital signs
4. Place oxygen
Pop Quiz!The ED is pretty full. Where would you put this patient?
T=100 HR:132 RR:30 SpO2: 89%
1. A resuscitation/trauma room
2. A regular ED room (telling attending about patient)
3. A regular ED room (no notification)
4. Back to the waiting room (frequent rechecks)
Brought Back to a Regular Room• Placed on 2L nasal cannula
• HR to 160s
• Acetaminophen
• ORT teaching
• Chest x-ray shows pneumonia
• Amoxicillin ordered
2/12/2018
4
Two Hours Later• Did not take ORT. Threw up amoxicillin.
• O2 had been turned up to 4-5L NC
• Sleepy, HR 160s, RR 60-70
• Extremities cool, weak pulses
• Cannot obtain access
• Antibiotics ordered
Uh-Oh• Moved to a front room, higher-level attending
• IV, fluids started
• Hypotensive, dopamine started
• Gas: 7.02/67
Uh-Oh• Moved to a front room, higher-level attending
• IV, fluids started
• Hypotensive, dopamine started
• Gas: 7.02/67
• Ketamine, versed - Intubation
• Desaturation – bradycardia - asystole
• CPR x 8 minutes, pulmonary hemorrhage at time of intubation
2/12/2018
5
Case• ECMO team called
• Ceftriaxone 1 hour post-arrest
• Vancomycin 1 hour post-arrest
• Oseltamivir the next morning
Case• ECMO team called
• Ceftriaxone 1 hour post-arrest
• Vancomycin 1 hour post-arrest
• Oseltamivir the next morning
• Group A Strep grew from pulmonary fluid
• +Influenza
What do you notice about this case?• What were the warning signs?
• What were the reassuring signs?
• What steps could have been better?
2/12/2018
6
Audience PollCould this patient have a similar first several hours of care at your institution?
1. Yes
2. I would like to think no, but maybe… yes
3. No
What Do You Notice About This Case?• Initial vitals not that bad
• Exam findings may be subtle
• Warning signs:o Return of fever after initial febrile prodrome
o Urine output
o Can’t get a blood pressure easily
• No focus on blood pressure, early access, IV fluid, antibiotics in the treatment plan until too late
Objectives1. Review formal pediatric sepsis definitions and formulate a working definition
that facilitates clinical recognition.
2. Understand current guidelines and landmark studies for critical elements of pediatric sepsis care:
• Diagnosis
• Fluid Resuscitation
• Protocolized Treatment
3. Identify practical approaches to improving pediatric sepsis outcomes in your patients.
2/12/2018
7
Objectives1. Review formal pediatric sepsis definitions and formulate a working definition
that facilitates clinical recognition.
2. Understand current guidelines and landmark studies for critical elements of pediatric sepsis care:
• Diagnosis
• Fluid Resuscitation
• Protocolized Treatment
3. Identify practical approaches to improving pediatric sepsis outcomes in your patients.
Pop Quiz!What is sepsis?
1. Systemic Inflammatory Response Syndrome (SIRS) + Infection
2. Life-threatening organ dysfunction caused by a dysregulated host response to infection
3. I know it when I see it
4. qSOFA >= 2
Pediatric Definitions: SIRSSystemic Inflammatory Response Syndrome
(2/4, 1 must be temp or wbc):
• Core Temp > 38.5°C or <36°C
• Tachycardia / Bradycardia if <1 y/o
• Tachypnea
• WBC elevated or depressed
Goldstein PCCM 2005
2/12/2018
8
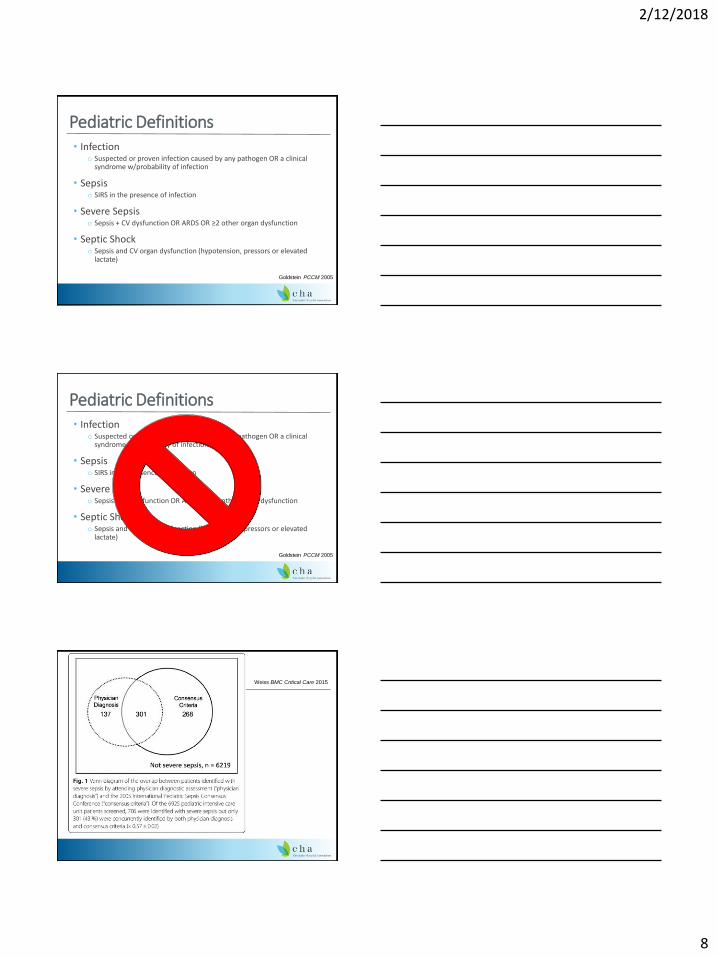
Pediatric Definitions• Infection
o Suspected or proven infection caused by any pathogen OR a clinical syndrome w/probability of infection
• Sepsiso SIRS in the presence of infection
• Severe Sepsiso Sepsis + CV dysfunction OR ARDS OR ≥2 other organ dysfunction
• Septic Shocko Sepsis and CV organ dysfunction (hypotension, pressors or elevated
lactate)
Goldstein PCCM 2005
Pediatric Definitions• Infection
o Suspected or proven infection caused by any pathogen OR a clinical syndrome w/probability of infection
• Sepsiso SIRS in the presence of infection
• Severe Sepsiso Sepsis + CV dysfunction OR ARDS OR ≥2 other organ dysfunction
• Septic Shocko Sepsis and CV organ dysfunction (hypotension, pressors or elevated
lactate)
Goldstein PCCM 2005
Weiss BMC Critical Care 2015
2/12/2018
9
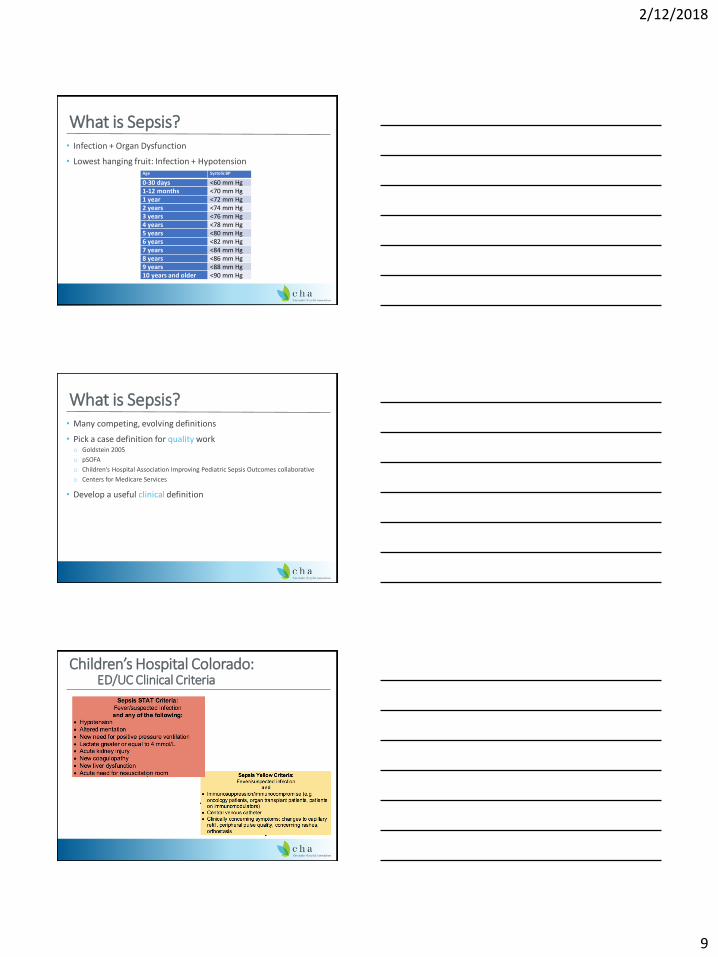
What is Sepsis?• Infection + Organ Dysfunction
• Lowest hanging fruit: Infection + HypotensionAge Systolic BP
0-30 days <60 mm Hg1-12 months <70 mm Hg1 year <72 mm Hg2 years <74 mm Hg3 years <76 mm Hg4 years <78 mm Hg5 years <80 mm Hg6 years <82 mm Hg7 years <84 mm Hg8 years <86 mm Hg9 years <88 mm Hg10 years and older <90 mm Hg
What is Sepsis?• Many competing, evolving definitions
• Pick a case definition for quality worko Goldstein 2005
o pSOFA
o Children’s Hospital Association Improving Pediatric Sepsis Outcomes collaborative
o Centers for Medicare Services
• Develop a useful clinical definition
Children’s Hospital Colorado: ED/UC Clinical Criteria

2/12/2018
10
Objectives1. Review formal pediatric sepsis definitions and formulate a working definition
that facilitates clinical recognition.
2. Understand current guidelines and landmark studies for critical elements of pediatric sepsis care:
• Diagnosis
• Fluid Resuscitation
• Protocolized Treatment
3. Identify practical approaches to improving pediatric sepsis outcomes in your patients.
Brierley CCM 2009
Capillary Refill Time
2/12/2018
11
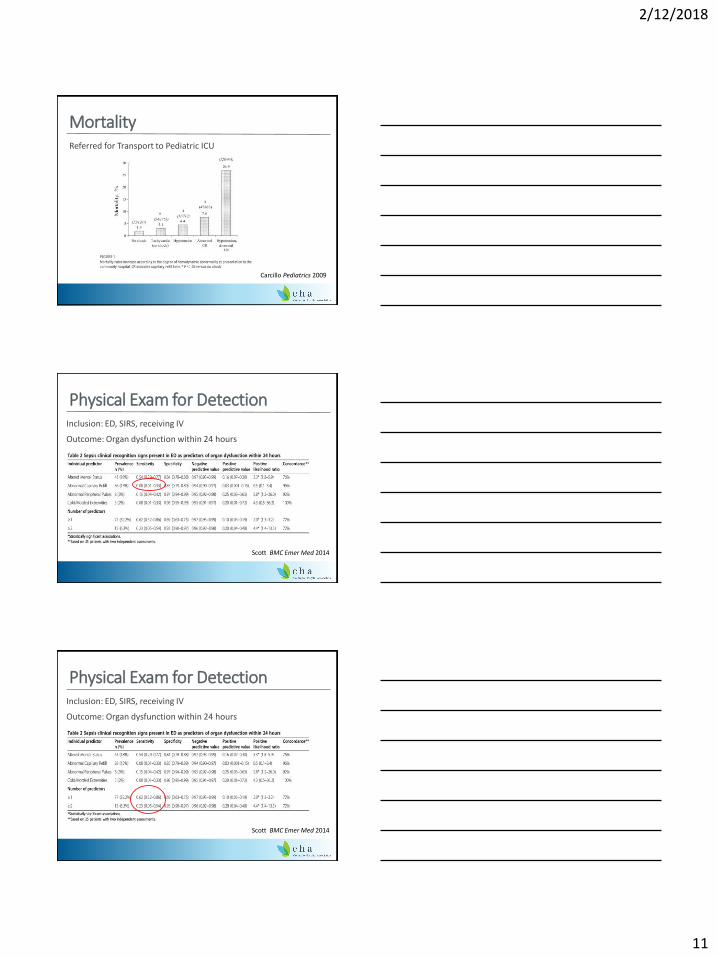
MortalityReferred for Transport to Pediatric ICU
Carcillo Pediatrics 2009
Physical Exam for DetectionInclusion: ED, SIRS, receiving IV
Outcome: Organ dysfunction within 24 hours
Scott BMC Emer Med 2014
Physical Exam for DetectionInclusion: ED, SIRS, receiving IV
Outcome: Organ dysfunction within 24 hours
Scott BMC Emer Med 2014

2/12/2018
12
Physical Exam for Detection• Capillary refill time, peripheral pulse quality, mottled extremitieso Useful in patients already identified as critically ill/septic
o Less useful for triage
• Altered mental statuso Better than the other findings
o Still misses half of severe sepsis patients
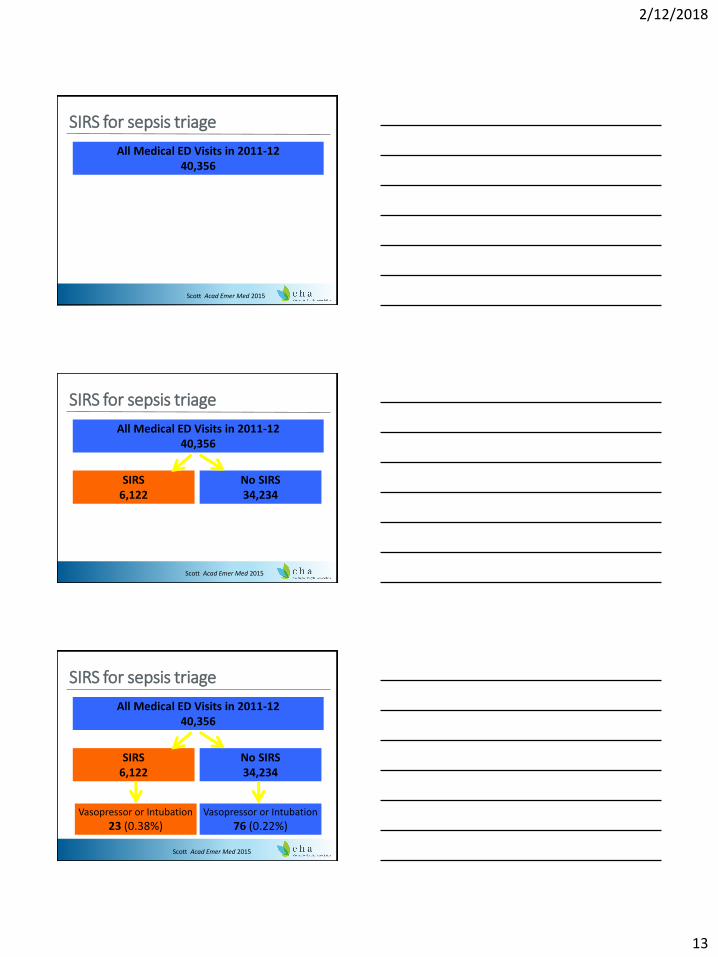
What About SIRS Vital Signs?
Pop Quiz!Of all children who come to the ED and end up intubated or on vasopressors within 24 hours, how many have SIRS? (excluding trauma)
1. 20%
2. 40%
3. 60%
4. 80%
2/12/2018
13
SIRS for sepsis triage
All Medical ED Visits in 2011-1240,356
Scott Acad Emer Med 2015
SIRS for sepsis triage
All Medical ED Visits in 2011-1240,356
Scott Acad Emer Med 2015
SIRS6,122
No SIRS34,234
SIRS for sepsis triage
All Medical ED Visits in 2011-1240,356
Scott Acad Emer Med 2015
SIRS6,122
No SIRS34,234
Vasopressor or Intubation
23 (0.38%)Vasopressor or Intubation
76 (0.22%)
2/12/2018
14
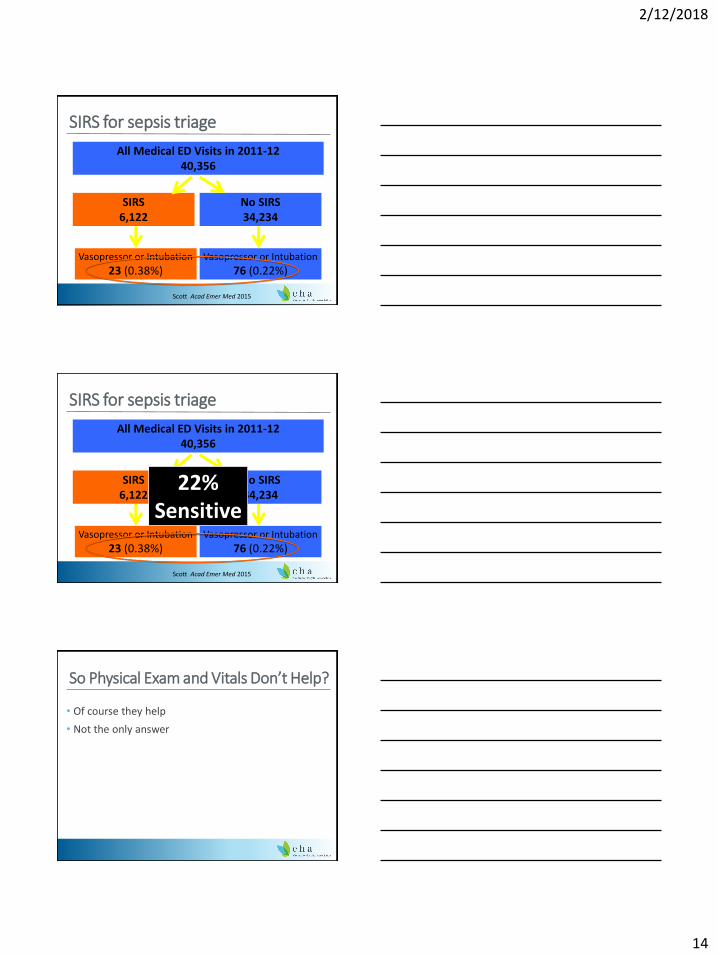
SIRS for sepsis triage
All Medical ED Visits in 2011-1240,356
Scott Acad Emer Med 2015
SIRS6,122
No SIRS34,234
Vasopressor or Intubation
23 (0.38%)Vasopressor or Intubation
76 (0.22%)
SIRS for sepsis triage
All Medical ED Visits in 2011-1240,356
Scott Acad Emer Med 2015
SIRS6,122
No SIRS34,234
Vasopressor or Intubation
23 (0.38%)Vasopressor or Intubation
76 (0.22%)
22% Sensitive
So Physical Exam and Vitals Don’t Help?
• Of course they help
• Not the only answer
2/12/2018
15
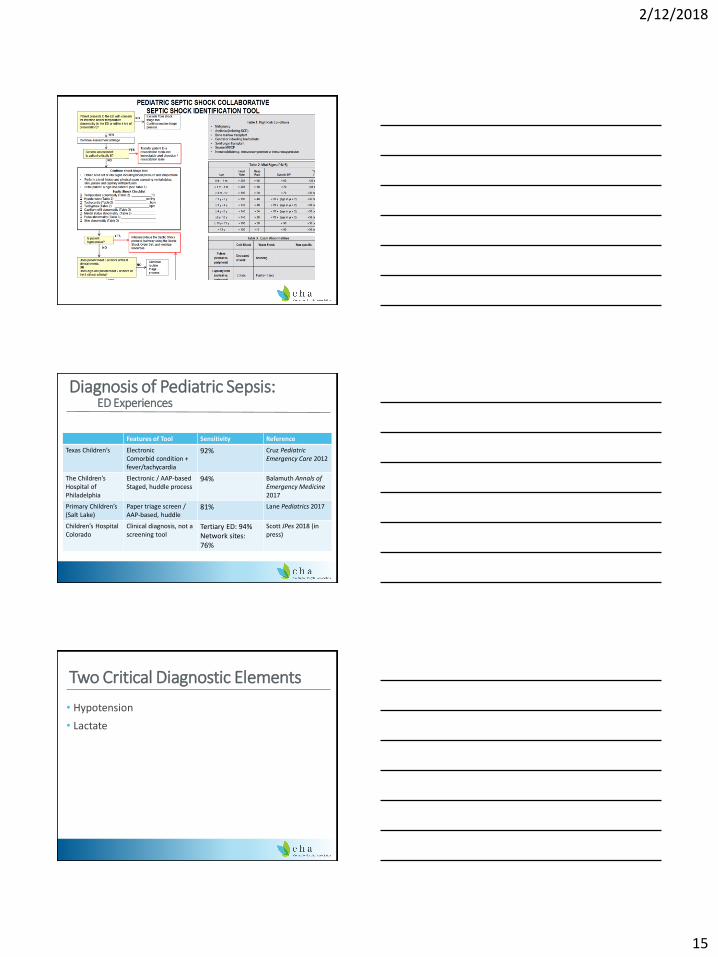
Diagnosis of Pediatric Sepsis: ED Experiences
Features of Tool Sensitivity Reference
Texas Children’s ElectronicComorbid condition + fever/tachycardia
92% Cruz Pediatric Emergency Care 2012
The Children’s Hospital of Philadelphia
Electronic / AAP-basedStaged, huddle process
94% Balamuth Annals of Emergency Medicine 2017
Primary Children’s (Salt Lake)
Paper triage screen / AAP-based, huddle
81% Lane Pediatrics 2017
Children’s Hospital Colorado
Clinical diagnosis, not a screening tool
Tertiary ED: 94%Network sites: 76%
Scott JPes 2018 (in press)
Two Critical Diagnostic Elements
• Hypotension
• Lactate
2/12/2018
16
Lactate in Adult Sepsis
Reprinted from Dellinger RP, Levy MM, Rhodes A, et al: Surviving Sepsis Campaign:
International Guidelines for Management of Severe Sepsis and Septic Shock: 2012. Crit Care
Med 2013; 41:580-637.
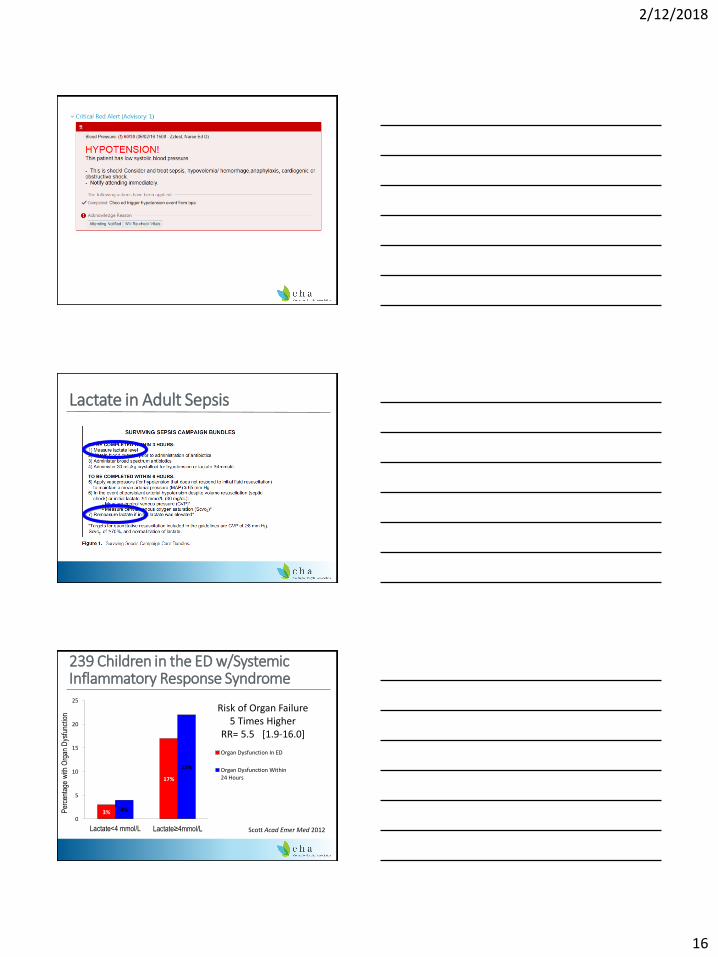
239 Children in the ED w/Systemic Inflammatory Response Syndrome
3%
17%
4%
22%
0
5
10
15
20
25
Lactate<4 mmol/L Lactate≥4mmol/L
Per
cent
age
with
Org
an D
ysfu
nctio
n
Organ Dysfunction In ED
Organ Dysfunction Within24 Hours
Risk of Organ Failure 5 Times Higher
RR= 5.5 [1.9-16.0]
Scott Acad Emer Med 2012
2/12/2018
17
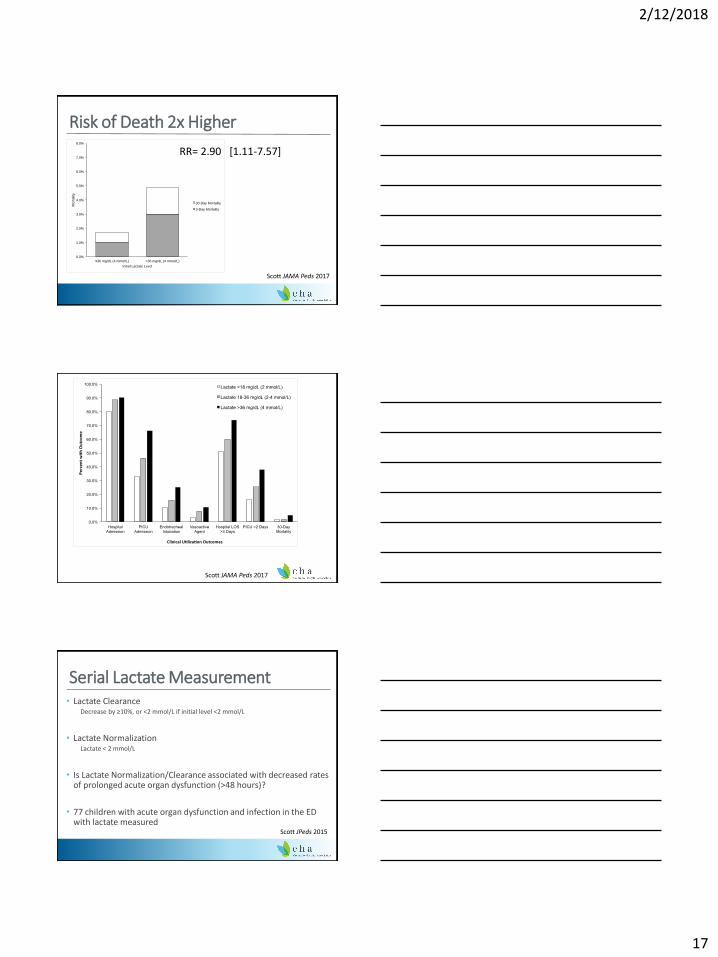
Risk of Death 2x Higher
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
≤36 mg/dL (4 mmol/L) >36 mg/dL (4 mmol/L)
Mo
rta
lity
Initial Lactate Level
30-Day Mortality
3-Day Mortality
Scott JAMA Peds 2017
RR= 2.90 [1.11-7.57]
Scott JAMA Peds 2017
Serial Lactate Measurement• Lactate Clearance
Decrease by ≥10%, or <2 mmol/L if initial level <2 mmol/L
• Lactate NormalizationLactate < 2 mmol/L
• Is Lactate Normalization/Clearance associated with decreased rates of prolonged acute organ dysfunction (>48 hours)?
• 77 children with acute organ dysfunction and infection in the ED with lactate measured
Scott JPeds 2015
2/12/2018
18
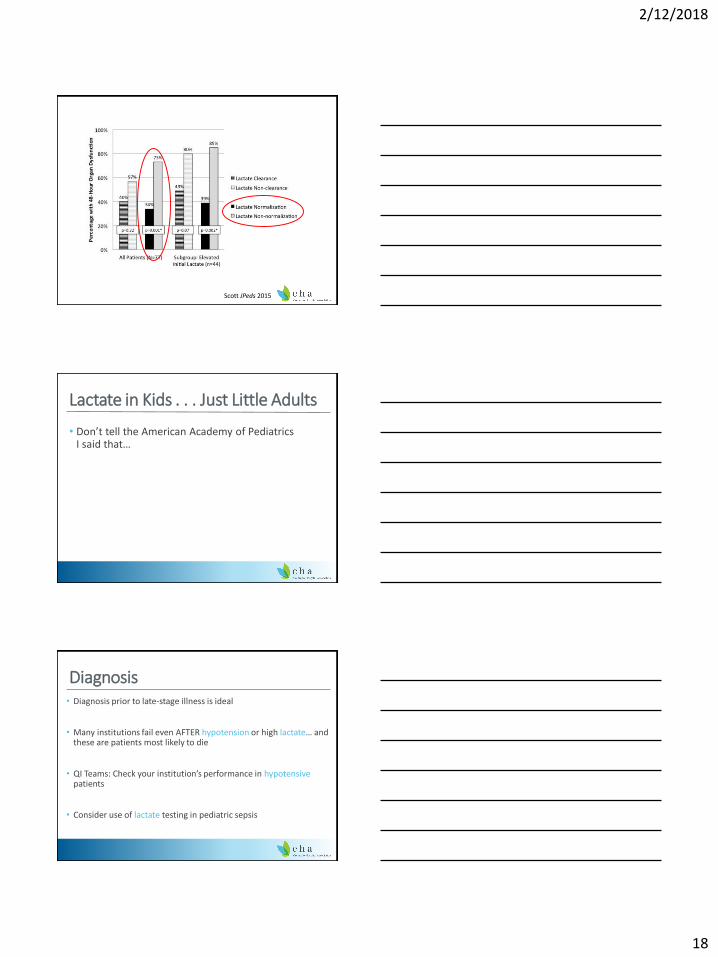
Scott JPeds 2015
Lactate in Kids . . . Just Little Adults
• Don’t tell the American Academy of Pediatrics I said that…
Diagnosis• Diagnosis prior to late-stage illness is ideal
• Many institutions fail even AFTER hypotension or high lactate… and these are patients most likely to die
• QI Teams: Check your institution’s performance in hypotensivepatients
• Consider use of lactate testing in pediatric sepsis
2/12/2018
19
Objectives1. Review formal pediatric sepsis definitions and formulate a working definition
that facilitates clinical recognition.
2. Understand current guidelines and landmark studies for critical elements of pediatric sepsis care:
• Diagnosis
• Fluid Resuscitation
• Protocolized Treatment
3. Identify practical approaches to improving pediatric sepsis outcomes in your patients.
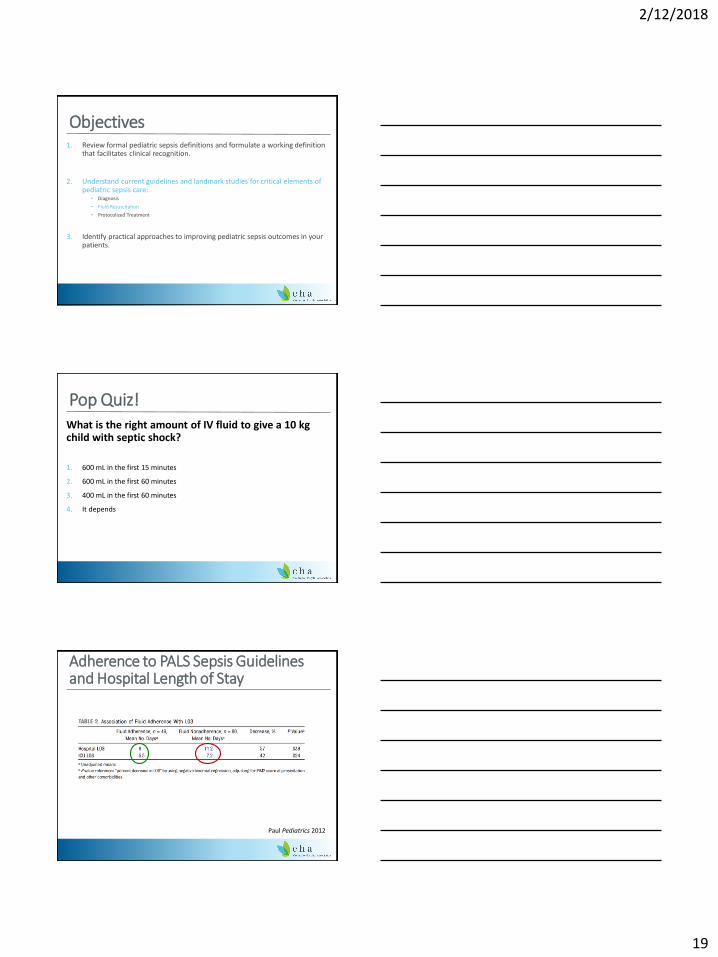
Pop Quiz!What is the right amount of IV fluid to give a 10 kg child with septic shock?
1. 600 mL in the first 15 minutes
2. 600 mL in the first 60 minutes
3. 400 mL in the first 60 minutes
4. It depends
Adherence to PALS Sepsis Guidelines and Hospital Length of Stay
Paul Pediatrics 2012
2/12/2018
20
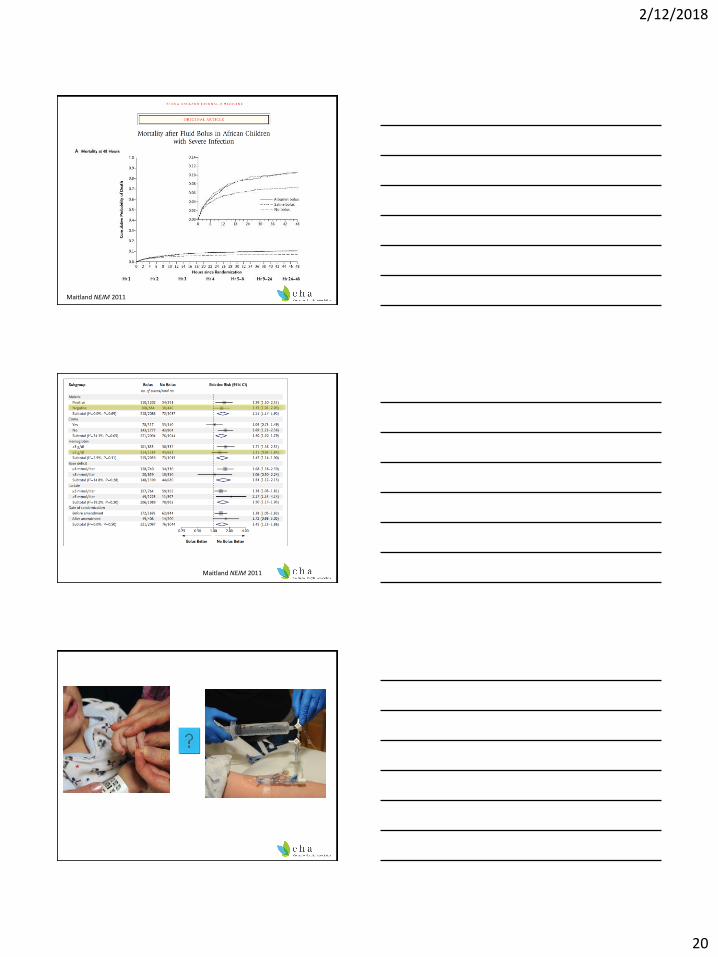
Maitland NEJM 2011
Maitland NEJM 2011
2/12/2018
21
PALS Fluid Recommendations• Administration of an initial fluid bolus… in shock is reasonable (Class IIa, LOE
C-LD)
• When caring for children with severe febrile illness in settings with limited access to critical care resources… administration of bolus intravenous fluids should be undertaken with extreme caution (Class IIb, LOE B-R)
• Continued emphasis on fluid resuscitation for shock
• Fluid not safe for all patients in all settings
• Increased emphasis on
◦ Individual patient assessment and reassessment
◦ Consideration of vulnerabilities to fluidde Caen Circulation 2015
A Trial to Determine Whether Septic Shock Reversal is Quicker in Pediatric Patients Randomized to an EGD Fluid-Sparing Strategy vs. Usual Care
Melissa Parker, McMaster University
Objectives1. Review formal pediatric sepsis definitions and formulate a working definition
that facilitates clinical recognition.
2. Understand current guidelines and landmark studies for critical elements of pediatric sepsis care:
• Diagnosis
• Fluid Resuscitation
• Protocolized Treatment
3. Identify practical approaches to improving pediatric sepsis outcomes in your patients.
2/12/2018
22
Pediatric Sepsis Teaching Points
Standardized, Expedited Processes Save Lives in Pediatric Sepsis
An Emergency Department Septic Shock Protocol and Care Guidelines for Children Initiated at Triage
2/12/2018
23
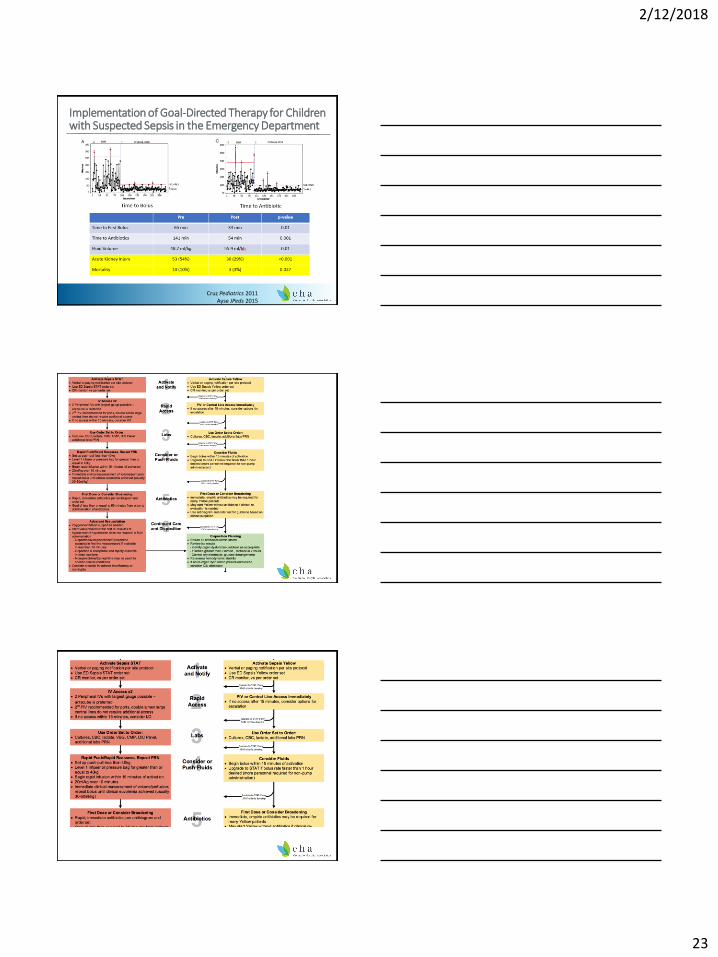
Implementation of Goal-Directed Therapy for Children with Suspected Sepsis in the Emergency Department
Cruz Pediatrics 2011Ayse JPeds 2015
2/12/2018
24
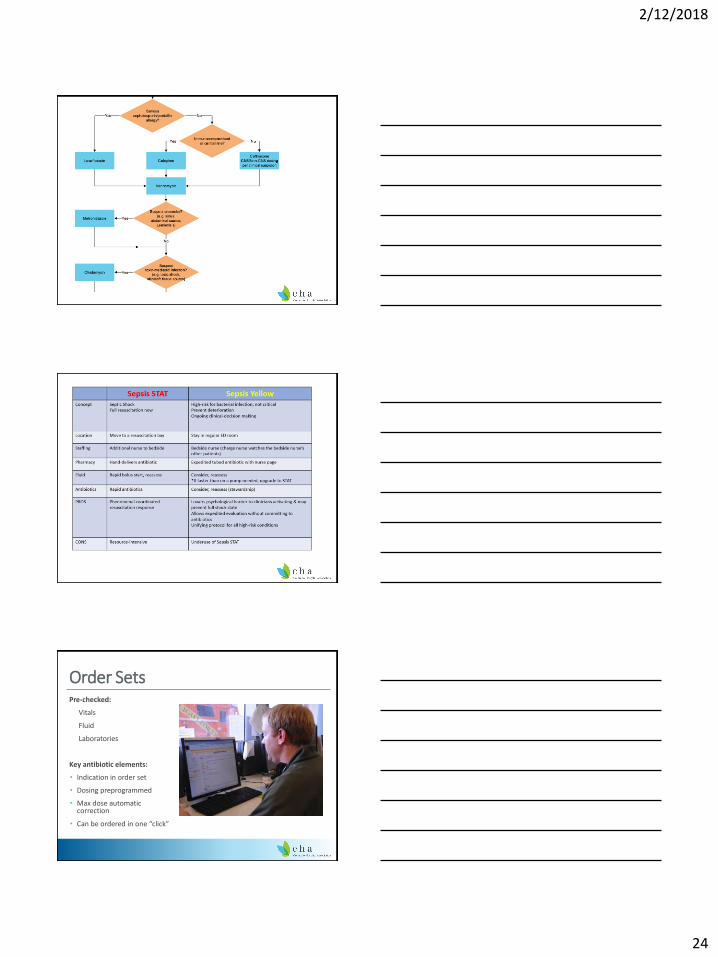
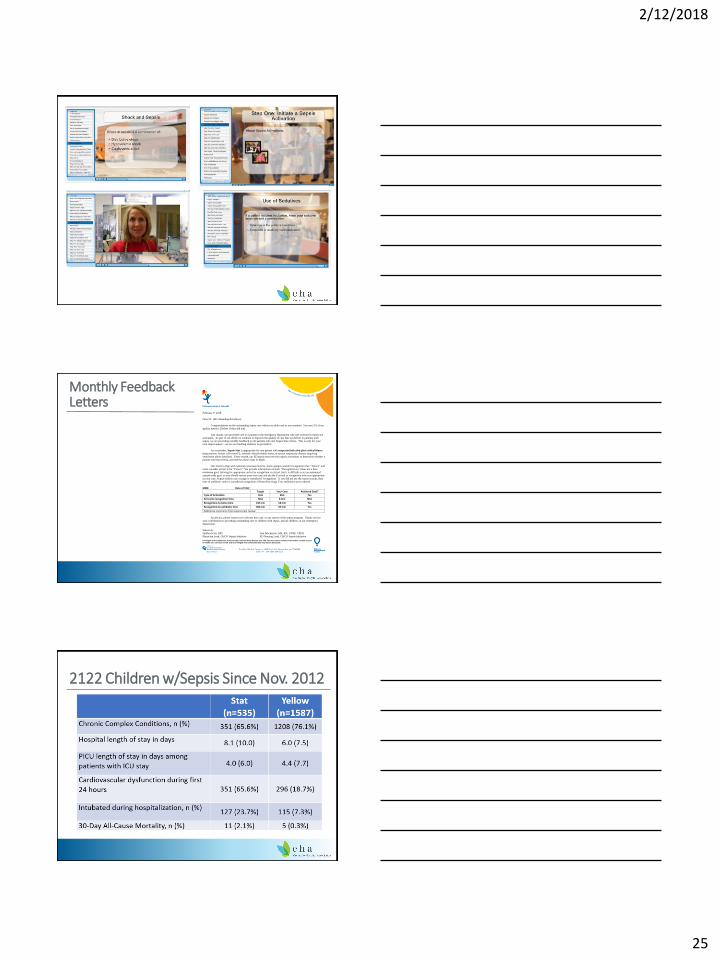
Order SetsPre-checked:
Vitals
Fluid
Laboratories
Key antibiotic elements:
• Indication in order set
• Dosing preprogrammed
• Max dose automatic correction
• Can be ordered in one “click”
2/12/2018
25
Monthly Feedback Letters
Privileged and Confidential; Protected by Colorado State Statute 25-3-109. This document contains information created as part of health care services review and is privileged and confidential and may not be disclosed.
February 9, 2018
Dear Dr. [ED Attending & Fellow]:
Congratulations on the outstanding sepsis care which you delivered to your patient! You met 3/3 of our
quality metrics. [Delete if they did not]
Last month, you provided care to a patient in the emergency department who met criteria for sepsis stat
activation. As part of our efforts to continue to improve the quality of care that we deliver to patients with
sepsis, we are providing monthly feedback on all patients who met Sepsis Stat criteria. This is only for your
own improvement – we are not tracking statistics on providers!
As a reminder, Sepsis Stat is appropriate for any patient with suspected infection plus critical illness
(hypotension, lactate ≥4.0 mmol/L, severely altered mental status, or severe respiratory distress requiring
ventilation above baseline). Every month, our ED sepsis team reviews sepsis activations to determine whether a
patient met Stat criteria, and reviews these cases in depth.
Our metrics align with national consensus metrics. Some groups consider recognition time “Time 0” and
some consider arrival to be “Time 0.” We provide information on both. “Recognition-to” times are a bare
minimum goal. Striving for appropriate arrival to recognition is critical, but it is difficult to set an automated
system-wide goal, so you should review your own case and decide if arrival to recognition time was appropriate
in your case. Sepsis orderset use or page is considered “recognition,” if you did not use the sepsis system, then
time of antibiotic order is considered recognition, followed by triage if no antibiotics were ordered.
MRN: Date of Visit:
Target Your Case Achieved Goal?
Type of Activation Stat Stat Yes
Arrival to recognition time N/A 8 min N/A
Recognition-to-bolus time ≤30 min 18 min Yes
Recognition-to-antibiotic time ≤60 min 37 min Yes
Additional comments from sepsis team review:
As always, please contact us to discuss this case, or any aspect of the sepsis program. Thank you for
your contribution to providing outstanding care to children with sepsis, and all children, in our emergency
department.
Sincerely,
Halden Scott, MD Joni Mackenzie, MS, RN, CPNP, CPEN
Physician Lead, CHCO Sepsis Initiative ED Nursing Lead, CHCO Sepsis Initiative
2122 Children w/Sepsis Since Nov. 2012
2/12/2018
26
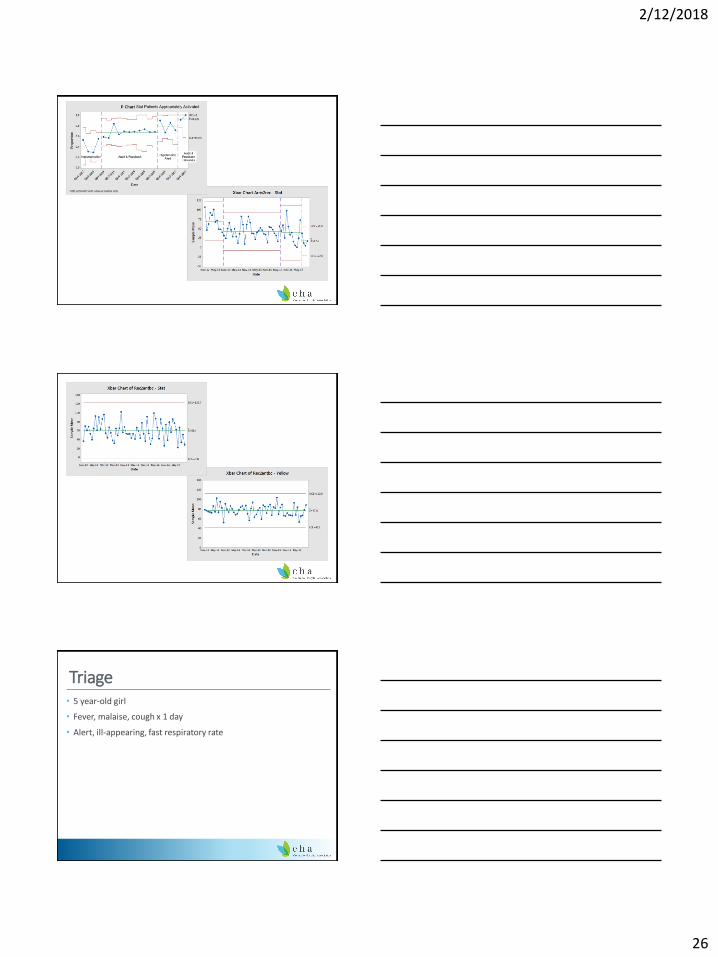
Triage• 5 year-old girl
• Fever, malaise, cough x 1 day
• Alert, ill-appearing, fast respiratory rate
2/12/2018
27
Triage• 5 year-old girl
• Fever, malaise, cough x 1 day
• Alert, ill-appearing, fast respiratory rate
• T=37.9 HR=146 RR=40 Sat 82% BP = 86/55
• Diminished L-sided breath sounds
• 4s capillary refill
To Resuscitation Room• IV placed, bolus started with a push-pull
• RR=70 BP=84/40
Sepsis Stat Activated
• Spitting up blood
• Monitor: PVCs bigeminy
Bedside Results• Lactate=6 mmol/dL
• Bedside CXR: L-sided pna
• Cefepime (65 min after arrival)/Vanc
• Oseltamivir in ED
2/12/2018
28
First Hour• Fluids: 60 ml/kg
• Dopamine started: SBP now >90
• High-flow NC 70% FiO2 on nasal CPAP
• Intubation – frank blood below cords
• Cardiology consulted
• Admitted to ICU
Outcome• Influenza B positive
• Group A Strep positive blood culture
• 25-day hospital course
• Discharged free of sequelae
So What Should We Do?1. Create an ordering system / order set for pediatric sepsis
2. Work on antibiotic delivery processes
3. Don’t miss hypotension
4. Measure performance
5. Enhance diagnosis
Further questions: [email protected]
2/12/2018
29
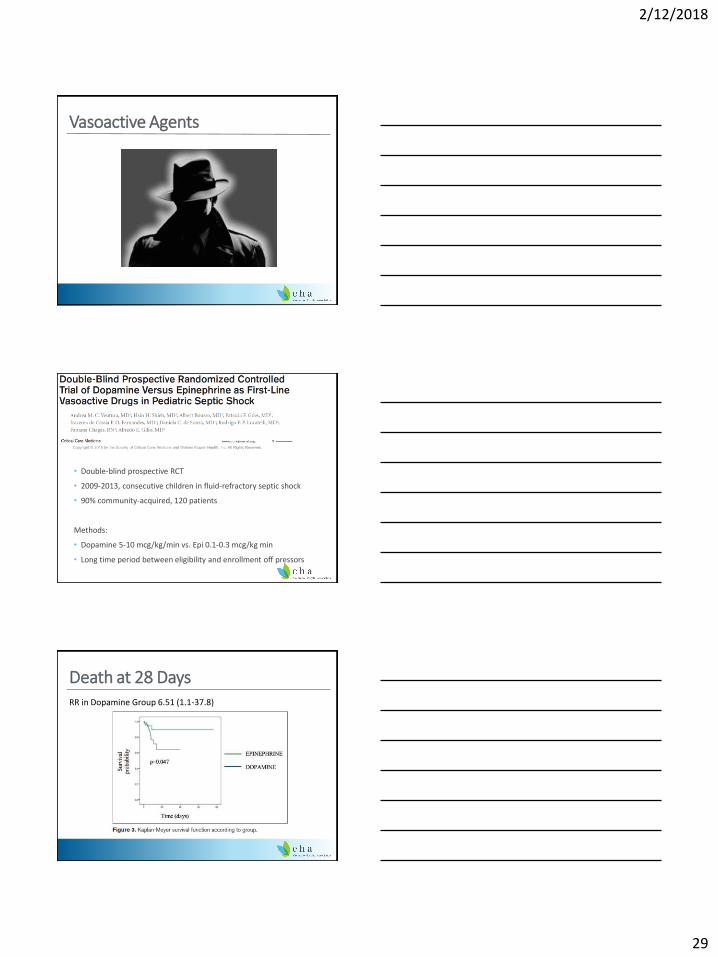
Vasoactive Agents
• Double-blind prospective RCT
• 2009-2013, consecutive children in fluid-refractory septic shock
• 90% community-acquired, 120 patients
Methods:
• Dopamine 5-10 mcg/kg/min vs. Epi 0.1-0.3 mcg/kg min
• Long time period between eligibility and enrollment off pressors
Death at 28 DaysRR in Dopamine Group 6.51 (1.1-37.8)