Embed Size (px)
Citation preview
21 The Auditory System
Chadi DarwichApril 15 2009
Outline
• Intro• Sound Processing, Deafness• 3 parts of the Ear• Weber & Rene Tests• Central Auditory pathways & Vas supply• Brainstem Nuclei
– Lateral Lemniscus and Inferior colliculus
• Auditory Cortex
Intro
• The auditory apparatus is adapted for receiving sound waves at the tympanic membrane and transmitting auditory signals to the central nervous system.
• Injury to elements of the peripheral apparatus, such as the ear ossicles, may result in conductive deafness.
• Damage to the cochlea or the cochlear portion of the eighth cranial nerve may result in sensorineural (nerve) deafness.
• Injury to the central auditory pathways cause central deafness which is usually combined with other signs and symptoms. Central lesions seldom result in complete deafness in one ear.

Intro
• The frequency of audible sounds is measured in cycles per second, or hertz (Hz)
• The normal frequency range for human hearing is 50 to 16,000 Hz.
• Most human speech takes place in the range of 100 to 8,000 Hz, and the most sensitive part of the range is between 1,000 and 3,000 Hz
• Intensity of sound is related to the perception of loudness and is usually measured in decibels (dB).
• Intensity is also related to a measure of sound pressure level at the tympanic membrane. A sound that has 10 times the power of a just-audible sound is said to have a 20-dB sound pressure level.
• Normal conversational levels of sound are about 50 dB.
Processing of Sound
• Sound waves are captured by the external ear (pinna) and channeled through the external auditory meatus to the tympanic membrane
• Sounds are transmitted across the middle ear or tympanic cavity from the tympanic membrane to the fluid-filled inner ear by a chain of three bony ossicles: the malleus, incus, and stapes – Diseases such as otosclerosis and otitis media result
in conductive hearing loss by affecting the efficiency of the ossicle movement
Conductive Deafness
• Conductive deafness is a deficit related to an obstructed, or altered, transformation of sound to the tympanic membrane and/or through the ossicle chain of the middle ear. – Damage to the pinna results in a failure of sound waves to be
properly conducted to the auditory meatus. – Infection involving the auditory canal (otitis externa),
inflammation or trauma to the tympanic membrane, or even the excessive accumulation of cerumen (wax) in the auditory canal are other causes of conduction deafness.
• The deficit experienced by the patient may range from decreased hearing to total deafness in the affected ear.
Inner Ear
• The membranous cochlea, the coiled portion of the inner ear, is encased in the osseous cochlea and consists of three spiraling chambers.
• Inner hair cells form a single line spiraling from base to apex, and the outer hair cells form three parallel lines that follow the same course. Once damaged, human hair cells do not regenerate
• The central processes of the spiral ganglion cells form
the cochlear portion of the vestibulocochlear nerve (cranial nerve VIII).
Sensorineural Deafness
• Results from damage to the cochlea or to the cochlear root of the vestibulocochlear nerve.
• The causes of sensorineural deafness may include repeated exposure to loud noises, treatment with certain antibiotics, infections such as rubella, mumps, or bacterial meningitis, and tumors at different levels of the neuraxis.
• Trauma in the form of skull fracture may also result in sensorineural deafness.
• The deficits experienced by the patient are deafness in the ear on the affected side, varying degrees of tinnitus if the cochlea is damaged, and additional signs and symptoms indicative of damage to the adjacent vestibular root.
Weber and Rinne Tests
• Air conduction: a vibrating tuning fork, usually with a 512-Hz frequency, is held about 2.5 cm from the opening of the auditory canal. Normally sound waves generated pass through the external and middle ears – Disease or damage in these areas would
result in decreased or lost hearing in this ear
Weber and Rinne Tests
• Bone conduction: The vibrating tuning fork is placed directly on the skull. Perceiving these vibrations as sounds means that the sound (vibration) is transmitted directly to the cochlea of the inner ear and bypasses the external ear and the middle ear
Weber and Rinne Tests
• Rinne test (bone + air conduction)
• The tuning fork is placed against the mastoid process. – The normal patient perceives the sound in the
ear on that side by bone conduction– after the sound is no longer perceived the
tuning fork is immediately moved to the auditory canal and the sound is again heard by air conduction.
Weber and Rinne Tests
• Negative Rinne test: The sound is perceived by bone conduction but not by air conduction (middle ear disease/deafness)
• Positive Rinne test the sound is perceived by air conduction but not bone conduction (sensorineural deafness cochlea or cochlear nerve damage).
Weber and Rinne Tests
• Weber test
• The tuning fork is placed on the midline of the skull or forehead.
• In a patient with normal hearing the sound (vibration) is perceived about equally in both ears.
Weber and Rinne Tests
• A patient with sensorineural deafness (e.g., cochlear damage) would perceive the sound of the tuning fork in the normal ear
• A patient with conduction deafness (canal middle ear obstruction) would perceive the sound of the tuning fork in the ear on the side of the damage.
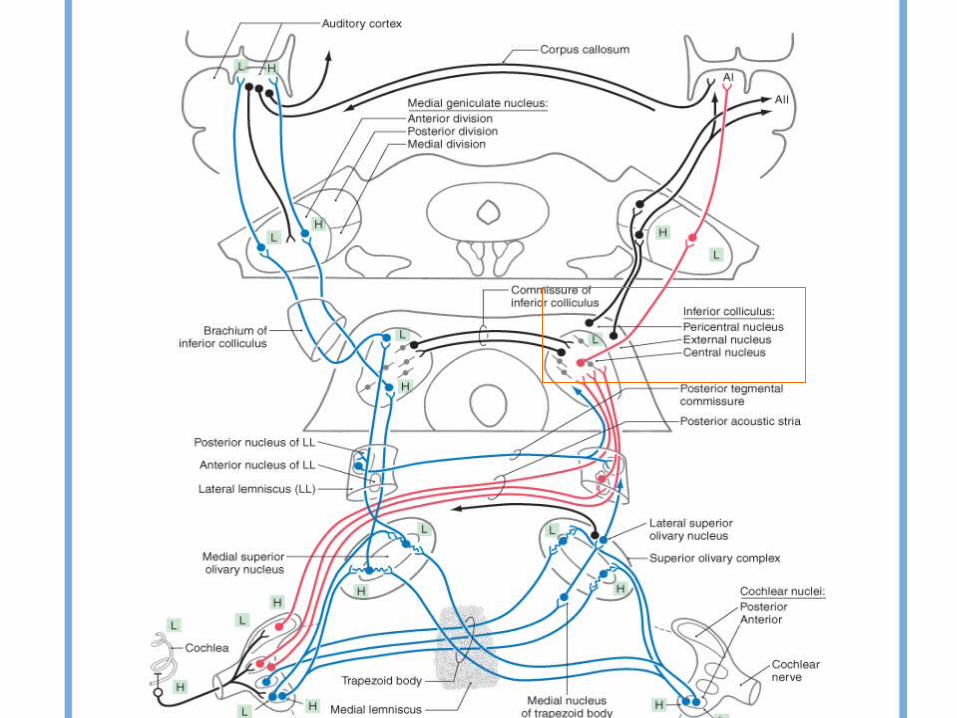
Central Auditory Pathways
• All fibers in the cochlear nerve synapse in the cochlear nuclei and the cochlear info ascends to the auditory cortex
• Information is distributed through multiple parallel pathways that ultimately converge in the inferior colliculus.
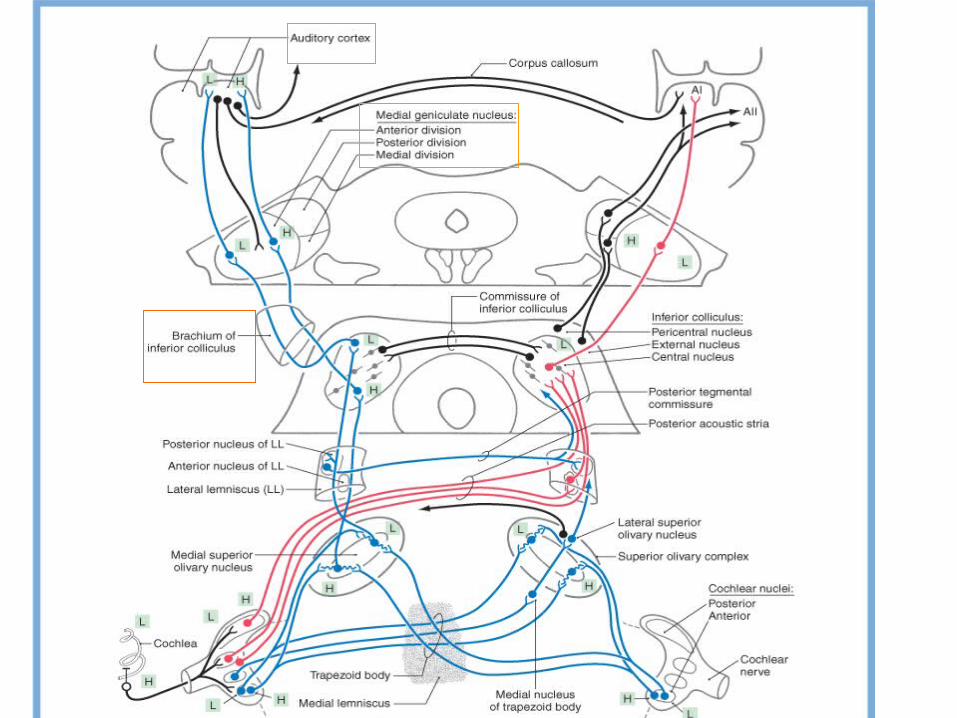
Central Auditory Pathways
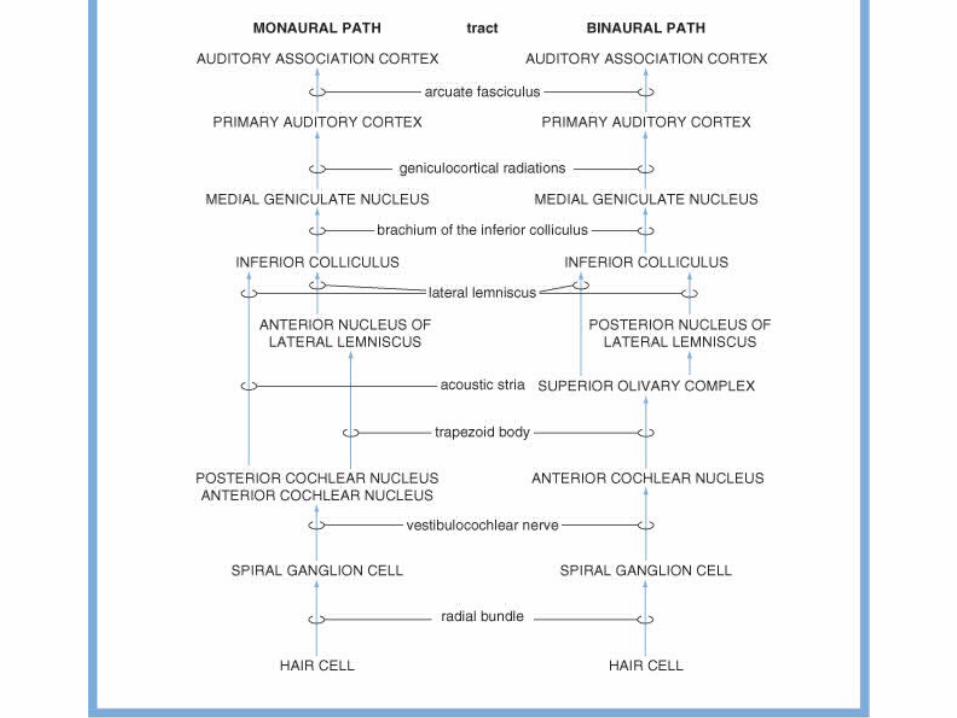
• The hierarchy of auditory nuclei involved in these parallel pathways includes – cochlear nuclei – nuclei of the superior olive and trapezoid body– nuclei of the lateral lemniscus – inferior colliculus.
• Specific fiber bundles that convey this information from one level to the next are – the trapezoid body – acoustic stria– lateral lemniscus.
Central Auditory Pathways
• From the midbrain, auditory information is conveyed:
inferior colliculus Brachuim
medial geniculate nucleus of the thalamus through the sublenticular limb of the internal capsule
auditory cortex
Vascular Supply
• The internal auditory (labyrinthine) artery, a branch AICA, supplies the inner ear and the cochlear nuclei
• Short circumferential branches of the basilar artery supply the superior olivary complex and lateral lemniscus
• The superior cerebellar and quadrigeminal arteries supply the inferior colliculus
• Thalamogeniculate arteries supply the medial geniculate bodies
• M2 segment of the MCA supply the primary auditory and association cortices
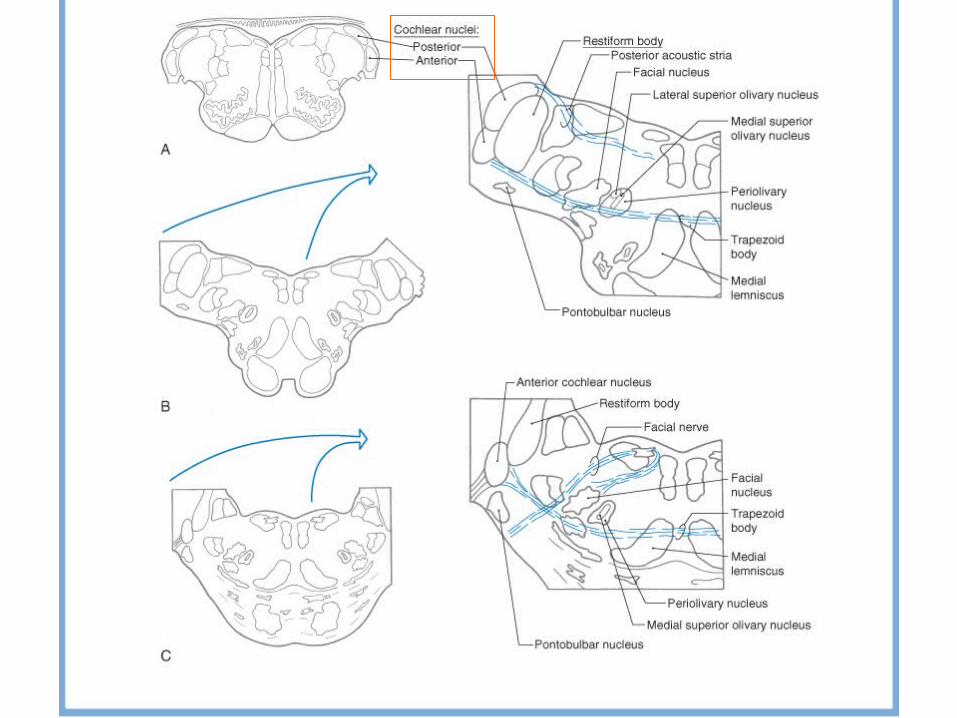
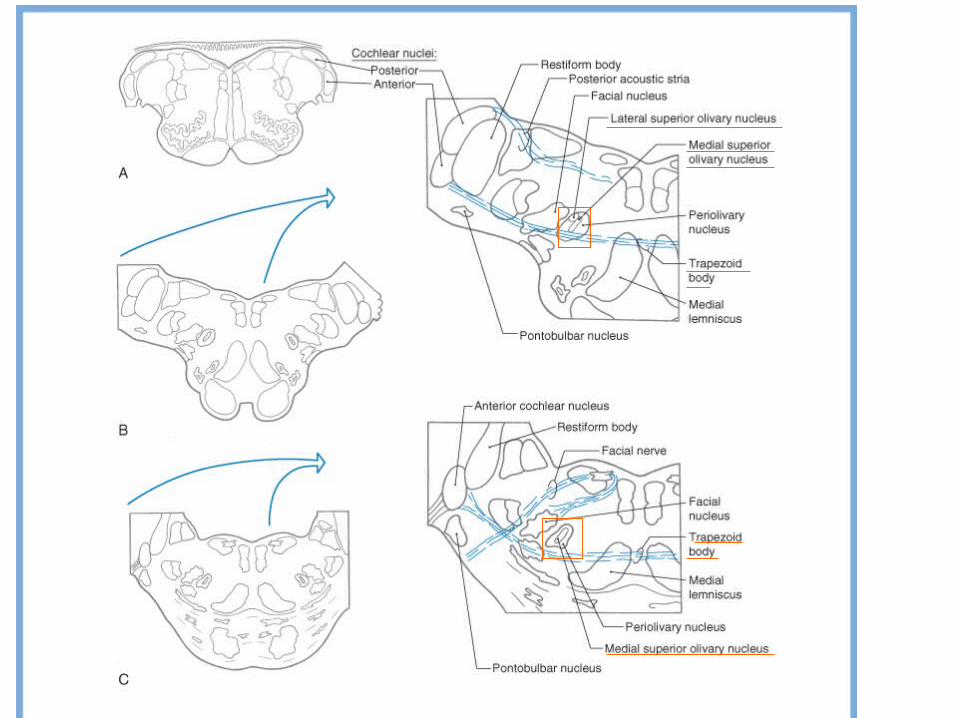
Cochlear Nuclei
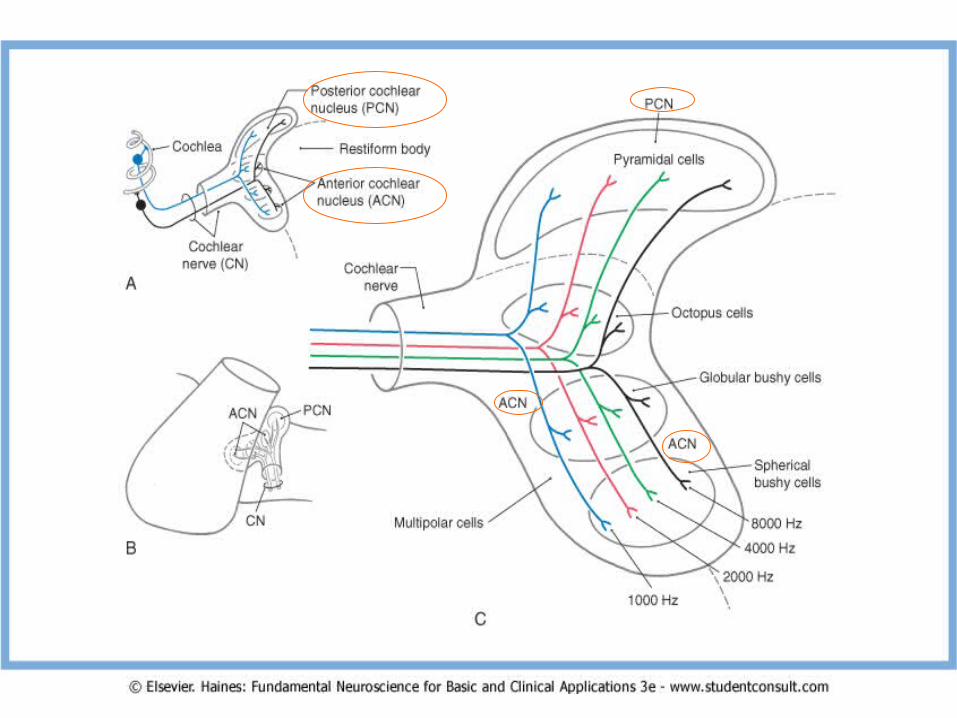
• The posterior cochlear nucleus (dorsal cochlear nucleus) and the anterior cochlear nucleus (ventral cochlear nucleus) are located lateral and posterior to the restiform body and are partially on the surface of the brainstem at the pontomedullary junction.
• The posterior cochlear nucleus drapes over the restiform body just inferior to the pontomedullary junction.
• The anterior cochlear nucleus extends rostral to the posterior cochlear nucleus, where it may be covered by the flocculus and by caudal fascicles of the middle cerebellar peduncle.
Cochlear Nuclei
• Cochlear nerve fibers end in the cochlear nuclei on the ipsilateral side
• They enter the brainstem at the CPA angle, they divide into ascending and descending bundles.
• Ascending bundle fibers synapse in the anterior part of the anterior cochlear nucleus
• Descending bundle fibers synapse in the posterior part of the anterior cochlear nucleus and in the posterior cochlear nucleus
Cochlear Nuclei
• In the cochlear nuclei, each afferent nerve fiber makes specialized synaptic contacts with several different cell types so that the resulting order produces distinct tonotopic maps in each division
• The frequency-related lines are organized so that low frequencies are represented laterally and high frequencies medially
Cochlear Nuclei
• Specific cell types of the cochlear nuclei, in turn, give rise to parallel but separate ascending pathways in the auditory system
• Monaural information is conveyed to the inferior colliculus
• Binaural processing is conveyed to the superior olivary complex.
Posterior cochlear nucleus
• Many of the cells in the posterior cochlear nucleus contribute to complex local circuits and are not easily correlated with distinct ascending channels.
• A major output of the posterior cochlear nucleus is via a direct pyramidal cell projection to the contralateral inferior colliculus
Anterior cochlear nucleus
• Anterior cochlear nucleus is distinguished by the presence of anatomically and physiologically distinct output cell types:
– Bushy cells: binaural information – Multipolar cells: direct monaural pathway – Octopus cells: indirect monaural pathway
Anterior cochlear nucleus
• Bushy cells: Their axons travel in the trapezoid body. They are the central origin of ascending channels and are useful for sound localization
• Multipolar cells are sensitive to changes in sound pressure levelthey convey information to the contralateral inferior colliculus about the intensity of the sound
• Octopus cells: Their axons synapse mainly in the contralateral anterior nucleus of the lateral lemniscus. They convey information that is useful in analyzing brief components of speech sounds
Superior Olivary Complex
• Located near the facial motor nucleus in the caudal pons
• It is the first site in the brainstem where information from both ears converges.
• It is a binaural processing.
• It is essential for accurate sound localization and the formation of a neural map of the contralateral auditory hemifield.
Superior Olivary Complex
• Components– The medial superior olivary nucleus (MSO), the principal nucleus
in the human superior olivary complex
– The lateral superior olivary nucleus (LSO), is not distinct and contains fewer cells. Summation of excitatory and inhibitory inputs to LSO neurons causes detection of interaural intensity differences, which provide spatial cues caused by shadowing of sounds by the path from the contralateral side of the head
– The trapezoid body is a bundle of myelinated fibers passing anterior to the superior olivary complex
Superior Olivary Complex
• Axons in the trapezoid body arising from ipsilateral spherical bushy cells make excitatory synapses with the laterally directed dendrites.
• Axons in the trapezoid body from the contralateral spherical bushy cells make excitatory synapses with the medially directed dendrites
• The excitatory neurotransmitter is probably gluglu or or aspasp. Local inhibitory circuits use glycineglycine as a neurotransmitter.
Superior Olivary Complex
• The MSO projections from the travel largely in the ipsilateral side in the lateral lemniscus and synapse in the central nucleus of the inferior colliculus
• The LSO projections always end in the posterior nucleus of the lateral lemniscus that projects to the contralateral inferior colliculus– This constitutes the indirect binaural pathway from the
superior olive to the inferior colliculus
Lateral Lemniscus
• The lateral lemniscus contains axons from– Second-order neurons in the cochlear nuclei, – Third-order neurons in the superior olive, – Fourth-order neurons in the adjacent nuclei of the lateral
lemniscus.
• This heterogeneous collection prevents a simple correlation of nuclei or tracts with specific wave components of the auditory evoked responses used to assess clinically the level of brainstem function.
• The interposition of synaptic delays in each of these components contribute to at least the second, third, and fourth wave components of the evoked responses.
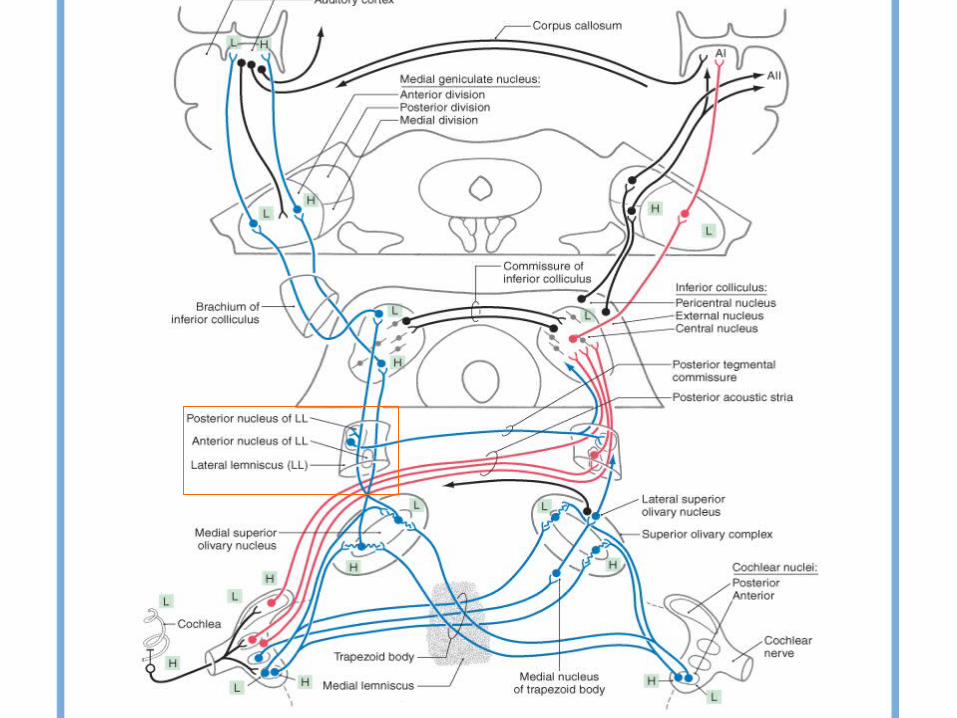
Anterior Lateral Lemniscus Nuclei
• The anterior (ventral, larger) nucleus of the lateral lemniscus consists of cells scattered among the ascending fibers of the lateral lemniscus.
• It extends from the rostral limit of the superior olive to just below the inferior colliculus.
• These cells project to the inferior colliculus, completing an indirect monaural pathway
Posterior LateralLemniscus Nuclei
• The posterior (dorsal, smaller) nucleus of the lateral lemniscus is intercalated in the ascending fiber bundles of the lateral lemniscus
• It is caudal to the inferior colliculus.• Its ascending projections decussate in the posterior
tegmental commissure and terminate in the contralateral inferior colliculus and in the contralateral posterior nucleus of the lateral lemniscus
• This pathway is largely inhibitory, using GABA as the neurotransmitter.
• It conveys binaural information and inhibits activity from the opposite hemifield.
Inferior Colliculus
• All ascending auditory pathways terminate in the inferior colliculus
• The egg-shaped central nucleus, is formed by fibers (major source of input) of the lateral lemniscus.
• Paracentral nuclei are in a shell around the central nucleus
– the pericentral nucleus, which lies posterior and is traversed by fibers from the commissure of the inferior colliculus
– the external (lateral) nucleus, which lies lateral and is intersected by fibers that form the brachium of the inferior colliculus.
Inferior Colliculus
• Many cells in the inferior colliculus respond to input from either ear
• Binaural responses of inferior collicular neurons resemble those of the superior olivary neurons, from which they receive a dominant binaural input
• Other cells in the fibrodendritic laminae of the central nucleus are monaural and are mainly excited only by the contralateral ear
Inf Coll. Central Nucleus
• The central nucleus integrates info from hindbrain auditory sources and projects it to the anterior division of the medial geniculate nucleus.
• The central nucleus consists of parallel layers of cells with disc-shaped dendritic fields. Afferents from the lateral lemniscus (fibrodendritic laminae) course parallel to these dendritic fields.
Inf Coll. Central Nucleus
• Ascending projections diverge and converge in a point-to-plane order in the central nucleus
each point along the cochlear spiral is
represented in an isofrequency lamina.
• Functionally, cells in the central nucleus are narrowly tuned, with the lowest frequencies represented posterolaterally and higher frequencies anteromedially.
Inf Coll. Paracentral Nucleus
• Cells in the paracentral nuclei are broadly tuned to frequency, and they habituate rapidly to repetitive stimuli.
• They receive input from the central nucleus and the cerebral cortex and
• They receive nonauditory input from the spinal cord, posterior column nuclei, and superior colliculus.
• These nuclei project to the medial geniculate nucleus superior colliculus, reticular formation, and precerebellar nuclei.
• Thus, the paracentral nuclei are probably involved in functions related to attention, multisensory integration, and auditory-motor reflexes.
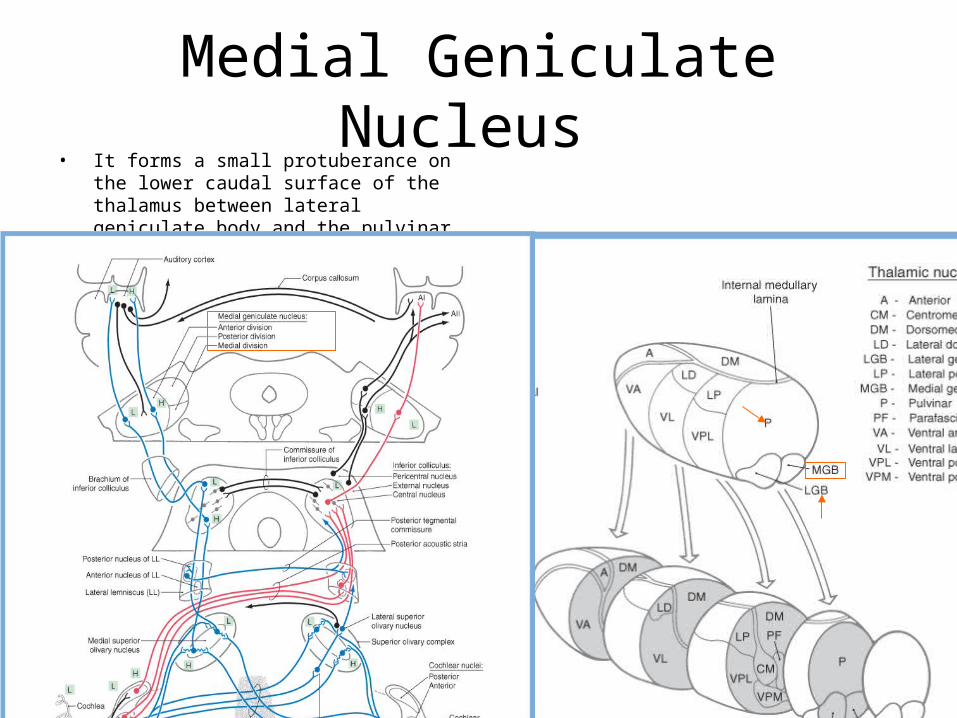
Medial Geniculate Nucleus • It forms a small protuberance on the lower
caudal surface of the thalamus between lateral geniculate body and the pulvinar
Medial Geniculate Nucleus
• The anterior division receives afferents from the central nucleus of the inferior colliculus and projects to the primary auditory cortex
• Isofrequency contours in the anterior division are arranged so that low frequencies are represented laterally and higher frequencies are represented medially
• As a result of collicular and thalamic integration most cells are not reliably excited by simple tones and are probably involved in complex feature detection
Medial Geniculate Nucleus
• The posterior division receives input from the pericentral nucleus of the inferior colliculus and projects to secondary auditory cortex
• Also tonotopically arranged
• This pathway is more broadly tuned and sensitive to habituation,it convey information about moving or novel stimuli that direct auditory attention.
Medial Geniculate Nucleus
• The medial (magnocellular) division receives afferents from the external nucleus of the inferior colliculus and projects to association areas of auditory cortex
• It contains cells that are broadly tuned to auditory and other sensory stimuli (vestibular & somesthetic inputs).
• It projects to temporal and parietal association areas and
to the amygdala, putamen, and pallidum.
• In view of the multisensory convergence that occurs in this pathway, it may be a part of the reticular activating system.
Clinical / Central Deafness
• Central deafness results from damage to the cochlear nuclei and/or the central pathways that relay auditory information to the auditory cortex.
• Damage to the cochlear nuclei may cause
deafness in the ear on the affected side.
• Central lesions within the brainstem, diencephalon, or auditory cortices may alter the perception of sound but infrequently result in deafness in one ear.
Clinical / Central Deafness
• Pontine lesions may result in pontine auditory hallucinosis, such as an orchestra out of tune, buzzing insects, or strands of music.
• These perceived auditory events are accompanied by more typical symptoms of pontine lesions, such as cranial nerve deficits and/or long tract signs.
• A perception of noise or sounds may also be experienced by patients with temporal lobe seizures or a temporal lobe lesion that damages auditory cortices.
Auditory Cortex
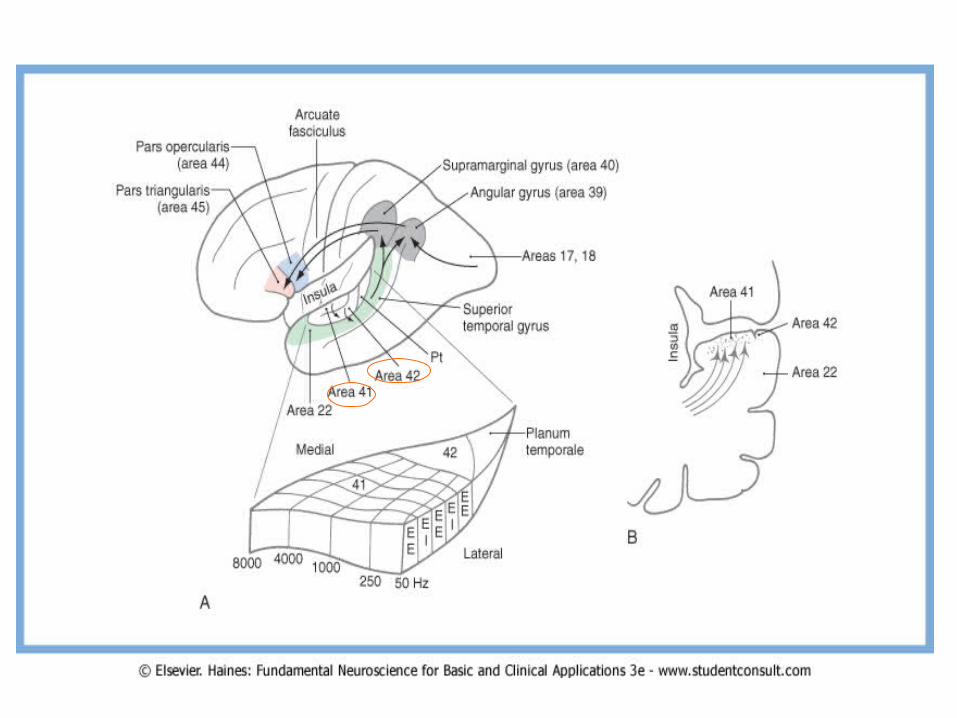
• The primary auditory cortex (AI, Brodmann area 41) is located in the transverse gyri of Heschl
• It is located in the first (anterior) transverse temporal gyrus but may extend into the second (posterior) gyrus
• Cytoarchitecturally, area 41 encompasses the granular cortex, with its well-developed layer IV containing small granule cells and densely packed small pyramidal cells in layer VI
• The secondary auditory cortex (AII, area 42) is adjacent to the granular cortex in the second transverse gyrus and planum temporale
Auditory Cortex
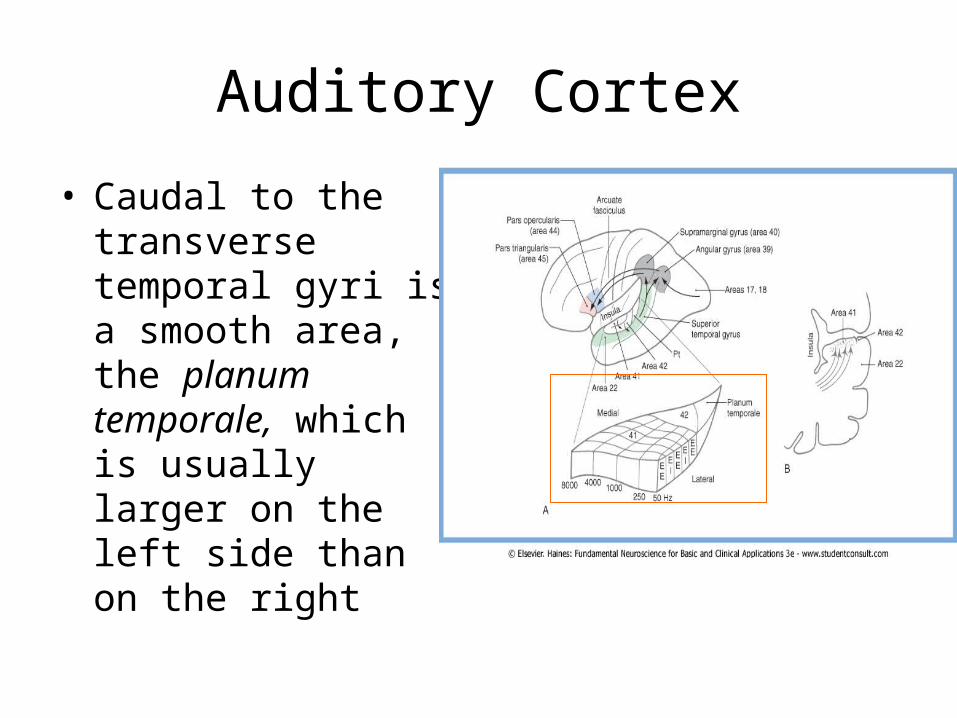
• Caudal to the transverse temporal gyri is a smooth area, the planum temporale, which is usually larger on the left side than on the right
Auditory Cortex
• Area 41 is connected with the anterior division of the medial geniculate body
• Area 42 is connected with the posterior division, of the medial geniculate body.
• Through the corpus callosum, each auditory
cortical area is connected with the reciprocal areas in the other cerebral hemisphere.
Auditory Cortex
• The tonotopic organization of constituent cells of the cortical layers and incoming afferent fibers form a series of orderly isofrequency columns that extend through the primary auditory cortex as long stripes.
• High frequencies are represented medially and low frequencies laterally.
• The series of stripes so formed have one subcomponent composed of cells excited by stimulation of both ears (EE) alternating with a subcomponent composed of cells excited by the contralateral ear and inhibited by the ipsilateral ear (EI).
Auditory Cortex
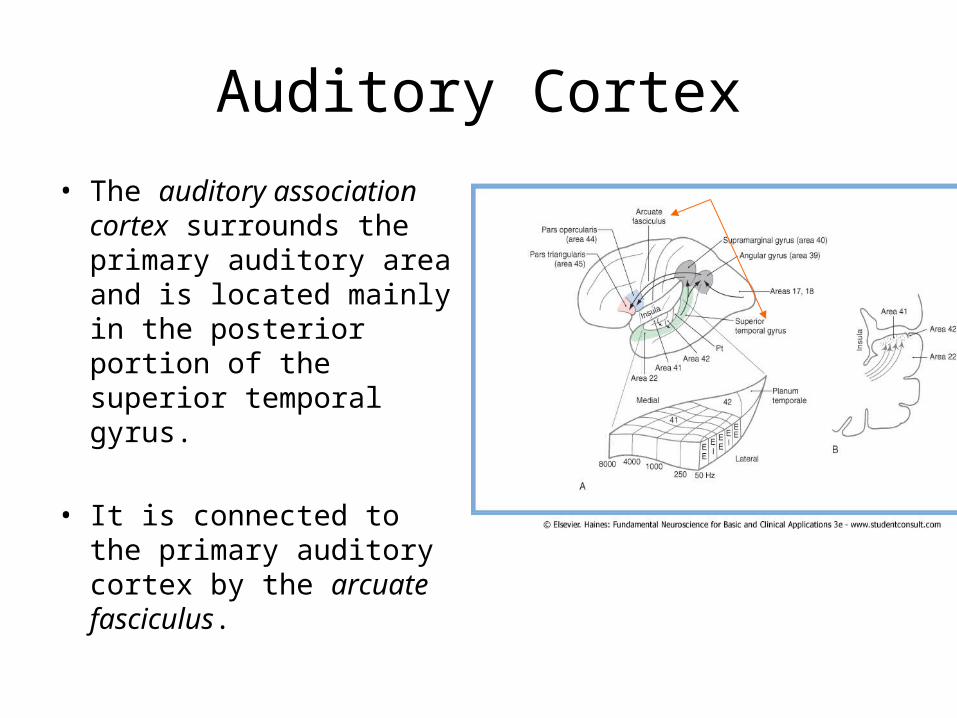
• The auditory association cortex surrounds the primary auditory area and is located mainly in the posterior portion of the superior temporal gyrus.
• It is connected to the primary auditory cortex by the arcuate fasciculus.
Auditory Cortex
• Area 22 includes a part of the planum temporale and the posterior portion of the superior temporal gyrus. It receives connections from the primary auditory cortex, as well as visual and somesthetic information.
• This speech receptive area, known as the Wernicke area, may be as much as seven times larger on the left side than on the right.
• When this area is damaged by occlusion of branches of the MCA, an auditory aphasia (Wernicke aphasia) results where comprehension of speech sounds is impaired but discrimination of nonverbal sounds is largely unaffected.
Auditory Cortex
• Brodmann areas 44 and 45 are known as the Broca area for expressive speech and language.
• They are located in the pars opercularis and pars triangularis of the inferior frontal gyrus.
• The major pathway connecting these areas with the primary and association auditory cortex is the arcuate fasciculus.
• If areas 44 and 45 are damaged along with other motor cortices on the left side by a stroke involving branches of the middle cerebral artery, the result is Broca aphasia where the speech is nonfluent, but comprehension of verbal and nonverbal sounds is largely unimpaired.
Descending Auditory Pathways
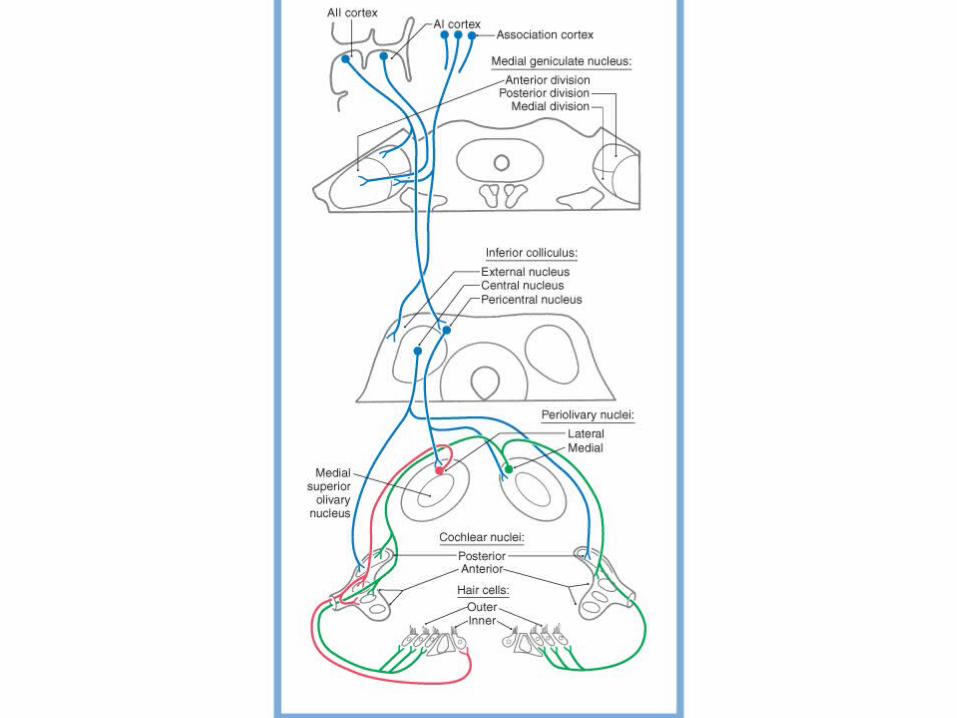
• Descending projections make reciprocal connections throughout the auditory pathway.
• They form feedback loops that provide circuits to modulate information processing from the peripheral level to the cortex.
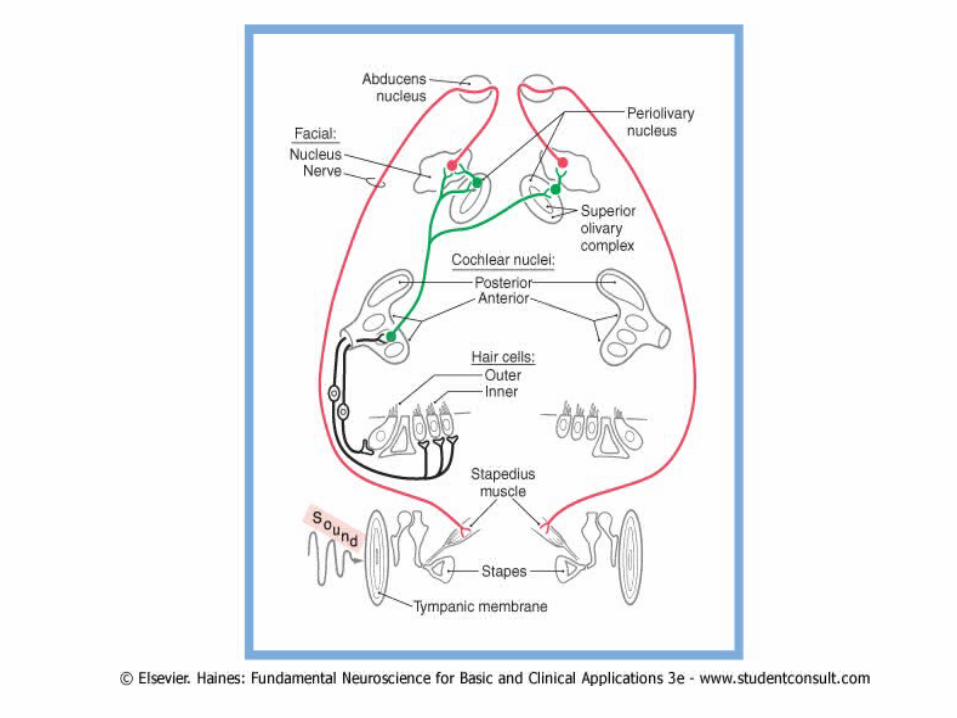
• For example, the auditory cortex projects to the medial geniculate nucleus and nuclei of the inferior colliculus. The inferior colliculus projects to the periolivary nuclei, which, in turn, send olivocochlear efferents to the cochlea.
The Olivocochlear Bundle
• The olivocochlear efferent system arises from groups of cells in the periolivary nuclei of the superior olivary complex.
• They travel as the olivocochlear bundle in the vestibular part of the vestibulocochlear nerve.
• Lateral olivocochlear efferent cells project to the ipsilateral inner hair cells, where they make axoaxonic synapses with type I spiral ganglion afferent fibers.
• Medial olivocochlear efferent cells have bilateral projections that terminate directly on outer hair cells
Cochlear Mechanics
• Direct efferent feedback to outer hair cells may influence cochlear mechanics and the sensitivity and frequency selectivity of the cochlea.
• Efferent-induced changes in outer hair cell membrane potentials result in changes in the height of the cells and the stiffness of their stereocilia.
• These changes modulate basilar membrane motion and thereby influence cochlear function.
Cochlear Mechanics
• The tight coupling of the basilar membrane to the tectorial membrane by the outer hair cells enables this efferent mechanism to feed energy back to the cochlea to amplify responses to specific tones.
• The cochlear amplifier effect is important in selectively tuning the cochlea to important sounds.
Middle Ear Reflex
• The middle ear reflex activate the small striated muscles:– The stapedius muscle is innervated by facial
motor neurons (associated with the caudal end of the superior olivary complex)
– The tensor tympani muscle is innervated by trigeminal motor neurons (associated with the rostral end of the superior olivary complex).
Middle Ear Reflex
• Auditory input via axons of neurons in the cochlear nuclei or the superior olivary complex provides the sensory limb of the reflex.
• The sensory pathways are bilateral, so that stimuli may be presented by earphones to one ear while the device to measure impedance is placed in the ear canal on the other side.
Thanks