Embed Size (px)
Citation preview


2
Annual Report January – December 2019 Jakarta / Amsterdam, March 2020 SEHATI Programme is implemented by: Simavi Together with: CD-Bethesda YAKKUM Plan International Indonesia Yayasan Rumsram Yayasan Dian Desa Yayasan Masyarakat Peduli In coordination with: Indonesian Ministry of Health Pokja AMPL National, chaired by Bappenas Embassy of the Kingdom of the Netherlands in Indonesia

3
Simavi, a Netherlands based Non-Government Organisation, views that good health is the basis of everyone. Good health enables you to develop yourself socially and economically, take matters into your own hands and pursue your dreams. With good health, you can look after yourself and your family and lift yourself out of poverty. That is why Simavi works towards its mission, a healthy life for all, by ensuring that marginalised people in low and middle income countries practice healthy behaviour based on their own free and informed decisions. To do this, Simavi brings together communities, business and governments in the countries in which Simavi operates and beyond. For more information visit www.simavi.org Materials and documents on the SEHATI programme can be found on https://simavi.org/what-we-do/programmes/sustainable-sanitation-hygiene-eastern-indonesia/ and https://rsr.akvo.org/en/project/5783/
4
Table of Contents
Glossary abbreviations ........................................................................................................ 5
Executive Summary ............................................................................................................ 8
Introduction ....................................................................................................................... 11
General Progress ............................................................................................................... 14 Outcome 1. Capacity, leadership and commitment strengthening of local government (at all levels) to implement and sustain the 5-pillars of STBM ................................................ 19
Outcome 2. Capacity improvement of CSOs on lobbying and advocating local government to lead STBM implementation ....................................................................... 23
Outcome 3. Capacity support to private sector for improved supply of WASH products and services ......................................................................................................................... 24
Outcome 4. The development of a viable implementation model that ensures local government is capable to roll out and sustain a district wide STBM 5 pillars .................... 26
Impact of the SEHATI implementation at community level ........................................... 28
Gender Equality and Social Inclusion (GESI) within the SEHATI Programme ................ 35
Progress at National Level ................................................................................................ 39
Challenges and Lesson Learned ....................................................................................... 41
Financial Overview ............................................................................................................ 43
Future Activities ................................................................................................................ 45
Annex 1 SEHATI Monitoring Framework and Tools ........................................................ 47
Annex 2. EKN Framework – WATER ................................................................................. 52
Annex 3. Financial Overview from 2016 to 2019 .............................................................. 55
5
Glossary abbreviations
ADD (Alokasi Dana Desa) Village Fund Allocation, fund that is allocated by district governments to village governments to support the development at village level
AMPL Drinking Water and Environmental Health
APBD District Annual Plan and Budget
APBDes Village Annual Plan and Budget
Bappeda District Development and Planning Agency
Bappenas National Development and Planning Agency
BOK Health Operational Assistance Fund that allocates mostly to primary health care and district health offices. Provincial and national level have also this fund to monitor the implementation of health programmes at lower level
BUMDes Village-owned Enterprise
Bupati Regent or district head. The regent and the representative council member are elected by popular vote for a term of 5 years
Camat Sub-district head
CD Bethesda Community Development Bethesda YAKKUM, one of Simavi partners implementing SEHATI programme in Sumba Tengah and Sumba Barat Daya, Districts of East Nusa Tenggara. For further information please visit its website http://cdbethesda.org
DD (Dana Desa) Village Fund is allocated directly by national governments to village governments to accelerate the development at village level. BPMPD is responsible to monitor the utilisation of this fund.
Desa Village
Dusun Sub-village or hamlet
FIETS FIETS is sustainability framework based on five sustainability dimensions: Financial, Institutional, Environmental, Technology and Social
IRC A Dutch NGO which provides technical assistance on monitoring and capacity building and knowledge management for SEHATI programme
Kabupaten District
Kecamatan Sub-district
NGO Non-Government Organisation

6
ODF Open Defecation Free
Perbup (Peraturan Bupati) Regent regulation which is issued based on Regent’s authority
Perda (Peraturan Daerah) District Regulation which is issued based on consensus between district governments and council members. This regulation has stronger legitimation than Regent regulation.
Perdes (Peraturan Desa) Village regulation which is issued by head of village
Permenkes (Peraturan Kementerian Kesehatan)
Ministry of Health Regulation
Plan International Indonesia Yayasan Plan International Indonesia, one of Simavi partners implementing SEHATI programme in Lombok Utara and Dompu, District of West Nusa Tenggara. For further information please visit its website: https://plan-international.org/indonesia.
POKJA AMPL Drinking Water and Environmental Health Working Group is an ad hoc working group chaired by Planning and Development Agency to coordinate the development initiatives on Water, Sanitation and Hygiene at all levels
Puskesmas It stands for Pusat Kesehatan Masyarakat in Indonesian or known as Primary Health Care
Roadshow One of STBM core activity to advocate, introduce and raise awareness on STBM and gain commitment from relevant stakeholders
Rumsram Yayasan Rumsram, one of Simavi partners implementing SEHATI programme in Biak Numfor, District of Papua. For further information please visit its website http://www.rumsram.org.
SEHATI Sustainable Sanitation and Hygiene for Eastern Indonesia
SHAW Sanitation, Hygiene and Water
Simavi A Dutch NGO that manages SEHATI; it also plays roles in coordinating SEHATI Programme and conducting advocacy at national level. For further information, please visit its website: website https://simavi.org.
SK Appointment Letter
SPAL It stands for Saluran Pembuangan Air Limbah or known as liquid waste channel
STBM Community Based Total Sanitation approach launched by the Indonesia Ministry of Health since 2008 to improve hygiene practises at community level
WASH Water and Sanitation & Hygiene
YDD Yayasan Dian Desa, one of Simavi partners implementing SEHATI programme in Manggarai Barat, District of East Nusa Tenggara.

7
For further information please visit its website http://www.diandesa.org.
YMP Yayasan Masyarakat Peduli, one of Simavi partners implementing SEHATI programme in Lombok Timur, Districts of West Nusa Tenggara. For further information please visit its website http://ympntb.org.

8

9
Executive Summary In its fourth year of implementation, SEHATI has shown positive results and trends in the 2 key elements of the programme, which are WASH Governance and Service Delivery. Under the WASH Governance element, the leadership, commitment and capacity of stakeholders in general have been continuously improved, evidenced by: (i) existence of supportive regulations at district and village levels, increasing number of governments’ work plans and amount of budget, and (ii) existence and growing capacity of STBM task forces at various levels. These results are contributed by collaborative works of SEHATI partners whose capacities are also increasing, enabling them to advocate, mentor and motivate stakeholders, especially the local governments. Up until 2019, the SEHATI approach has been replicated by the local governments to 161 villages. Under the Service Delivery element, 215 villages with more than 500.000 people have been intervened with STBM 5 pillars; 87 villages have been declared ODF/STBM; a few success of sanitation marketing strategy and financing scheme developed by partners have been acknowledged by the national government of Indonesia. At the national level, collaboration and coordination with the national government of Indonesia and non-government stakeholders are also improving through several learning and sharing sessions facilitated by SEHATI. A significant influence at the national level contributed by SEHATI is the initiation of revising the STBM national monitoring system and tool by the Indonesian Ministry of Health to include 4 other pillars in its existing system and tool. SEHATI has also received a request from the national government to contribute in the processes of policy review and revision in the sector of Water and Sanitation, as well as in Menstrual Health. In May 2019 Simavi co-organised MH Day in Jakarta with various sessions and discussions. By the end of August 2018 three out of five partners finished their activities in four out of seven districts according to plan as they had been intervening in these areas since the implementation of SHAW (2010-2015). By the end of August 2019 Yaysan Plan International Indonesia finished their activities in Dompu district on the island of Sumbawa. As this district showed great progress it was no longer included in the proposal for the SEHATI extension. As Dompu is such a good show case it was chosen to organise the closing ceremony in August 2019 in Dompu. During this closing ceremoy also partners and stakeholders, who finished implementation in 2018, were invited. Since September 2019 Yayasan Plan International Indonesia and Yayasan Dian Desa continued working in the district of Northern Lombok and Western Manggarai. We are grateful to EKN Jakarta that Simavi was given an extension of one year between September 2019 and August 2020. Simavi’s proposal to continue working in Lombok Utara and Manggarai Barat was granted with an additional budget of 450.000 euros. In both districts we kept following the same initial approach. However in the extension we do have and extra focus on private sector collaboration and Menstrual Health. Additionally, since the extension, Simavi incorporated a focus on the provincial level of governance (NTB and NTT), as this level was missing in the initial design of the programme. Year 2019 was also the year for finalising the SEHATI replication model. The implementation of SEHATI in the last 4 years have been providing SEHATI with a thorough flow of process of STBM implementation, all of which has been made in a simple diagram with complete information for easy understanding. In August 2019 Simavi handed over this replication model to the government of Indonesia during the closing ceremony for 5 out of 7 districts of this SEHATI programme.

10
In regards to lobby and advocacy at national level, Simaavi has contributed to the development of national web-based monitoring system of 5-pillars of STBM since the very beginning of SEHATI programme. Simavi supports the Ministry of Health and National Planning Agency, not only in developing the indicators but also providing a practical guideline for sanitarians. In mid 2019, Simavi invited representatives of the district health offices from 7 district to join a training in Surabaya and to test the system within their respective districts by collecting the data at household level. The data analysis of 5 pillars of STBM at national level was supposed to be disseminated by the end of 2019, yet, due to tight schedule of Ministry of Health, the dissemination has been postponed into 2020.
Simavi was also involved in the National Water and Sanitation Conference (KSAN) 2019. Simavi has shared some best practices and approaches in SEHATI programme to various government agencies and non- government stakeholders. This event was responded positively by participants through which SEHATI also gained inputs on our existing approach and strategies. A challenge of 2019 were the ripple effects of the devastating earthquakes of mid 2018 at the island of Lombok. The targets achieved under SEHATI before the earthquakes have decreased in Lombok. However the citizens of Lombok Utara showed a great resilience and an impressing behaviour change. In additions, these earthquakes had limited impact to the general achievement. Our overall target in the 7 districts until the end of the programme remains the same. Other challenges since start from the programme in 2016, remain the same, such as limited clean water resources in some dry areas and tough geographic condition. Apart from continuing to strengthen the capacity of stakeholders as per the workplan, SEHATI gave in 2019 a more focus on the exit strategy for the two partners left (Yayasan Dian Desa and Yayasan Plan International Indonesia). While we are aware that right from its development and design stage SEHATI has included how to do a good exit strategy, in 2019 we also wanted to ensure that dynamics of the situation in the field in the last 3 years, especially due to the mid 2018 earthquakes in Lombok, is incorporated in the exit strategy to make it stronger and more convincing.

11
12
Introduction Funded by the Embassy of the Kingdom of the Netherlands (EKN) for Indonesia, in January 2016 Simavi started implementing a programme, called Sustainable Sanitation and Hygiene for Eastern Indonesia (SEHATI) originally for a period of 2016 to mid 2019, then in June 2019 it granted a year extension until mid 2020. This programme is implemented in collaboration with Indonesian NGOs, aiming at strengthening the capacity of local governments to implement sanitation and hygiene programmes using the national approach of 5 pillars of STBM (Community Led Total Sanitation). As described in the Permenkes No. 3/2014, the pillars of STBM consist of:
• Pillar 1: Open Defecation Free (ODF) • Pillar 2: Hand washing with soap at critical moment • Pillar 3: Household water treatment and safe storage • Pillar 4: Solid waste management • Pillar 5: Household liquid waste management1
The SEHATI programme is basically a continuation of a previous programme, called SHAW (Sanitation, Hygiene and Water), which was implemented between 2010 and 2015. In SHAW, Simavi and its 5 partners promoted the 5 pillars of STBM directly at the grass root level. It resulted in a few successes, such as reaching out to 1.5 million people to practise a healthy behaviour based on the 5 pillars of STBM and declaring 850 STBM villages out of 1.042 triggered villages. Apart from the successes, SHAW also provided partners with a few lessons learned, two of which are: (1) the district governments are the most strategic implementing actors as they have strong power in ensuring the institutionalisation of the STBM approach in the government system; and (2) working at grass root level would take a very long time and cost over 1 billion Euro in order to reach the entire rural population. Using such lessons learned from SHAW and aiming at making the SEHATI programme more efficient and effective in its approaches, SEHATI modified its approach and Theory of Change (ToC). SEHATI views that WASH sector has 2 key elements to be addressed at the same time, which are:
• the WASH Governance element (leadership and commitment, financing, strategy planning and monitoring sector, supportive legislation and enforcement sector) and;
• the Service Delivery element (demand creation, pro-the-poor financing, sanitation marketing, hygiene promotion, monitoring and follow up).
Therefore, programme activities were designed for mobilising and strengthening the capacity of local government actors to address these elements. When the government capacities are enhanced and those key elements are embedded in the government systems and process, Simavi believes that local actors will be able not only to implement sanitation programmes in their areas, but also to replicate and scale up the programmes throughout their districts. Figure 1 below shows the 7 districts on 5 islands in Eastern Indonesia, where the SEHATI Programme is implemented, and the 5 Indonesia NGO partners working for SEHATI (Yayasan Dian Desa, Yayasan Rumsram, Yayasan Plan International Indonesia, CD-Bethesda YAKKUM, and Yayasan Masyarakat Peduli).
1 There is a large overlap with the approach to Community Led Total Sanitation (CLTS), which is known worldwide. However, STBM develops CLTS idea further, towards a clean and healthy living environment by putting hygiene next to sanitation.

13
Figure 1. Location of SEHATI programme in Indonesia
As of August 2018, SEHATI has completed the implementation in four districts and as of August 2019 SEHATI has also completed the implmentation in Dompu district on the island of Sumbawa. Since September 2019 until June 2020, SEHATI works in only two districts, namely Lombok Utara on the island of Lombok (NTB) and Manggarai Barat on the island of Flores (NTT). During the extension period, SEHATI focuses on strengthening local capacities and STBM related systems that have been applied since the beginning of the programme, to be able to exit smoothly. Since the extension an extra focus is being put on private sector collaboration, the inclusion of provincial government (NTB and NTT) and integration of Menstrual Health within STBM. This report is the fourth annual report of the SEHATI Programme which covers the period of 1 January to 31 December 20192. For a better flow of reading, this report will first describe the general progress, consisting of (i) progresses on the 4 agreed outcomes of the programme; (ii) progress of implementation at village level; and (iii) progress on Ggender Eequality and Ssocial Iinclusion (GESI) aspects. It will then be followed by a description about progresses at national level and challenges and lessons learned. The two last parts of the report will be the financial overview and future activities.
2 The interested readers can request previous progress reports at [email protected] and [email protected]

14
15
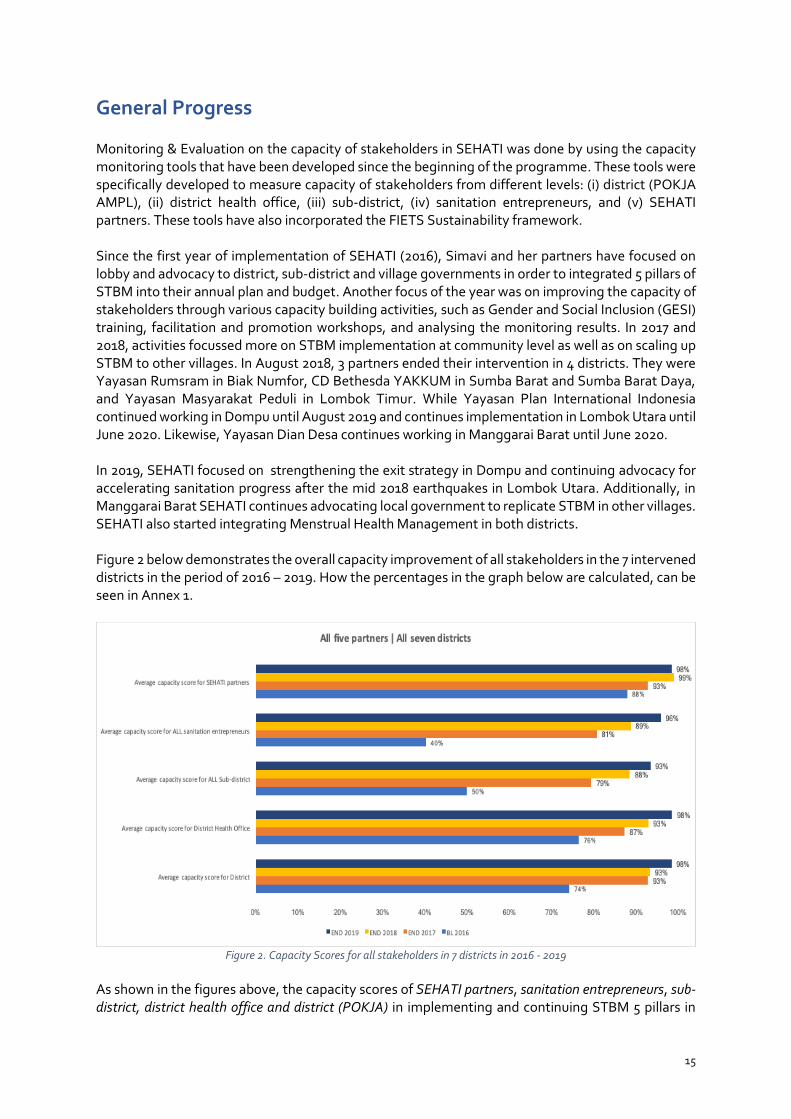
General Progress Monitoring & Evaluation on the capacity of stakeholders in SEHATI was done by using the capacity monitoring tools that have been developed since the beginning of the programme. These tools were specifically developed to measure capacity of stakeholders from different levels: (i) district (POKJA AMPL), (ii) district health office, (iii) sub-district, (iv) sanitation entrepreneurs, and (v) SEHATI partners. These tools have also incorporated the FIETS Sustainability framework. Since the first year of implementation of SEHATI (2016), Simavi and her partners have focused on lobby and advocacy to district, sub-district and village governments in order to integrated 5 pillars of STBM into their annual plan and budget. Another focus of the year was on improving the capacity of stakeholders through various capacity building activities, such as Gender and Social Inclusion (GESI) training, facilitation and promotion workshops, and analysing the monitoring results. In 2017 and 2018, activities focussed more on STBM implementation at community level as well as on scaling up STBM to other villages. In August 2018, 3 partners ended their intervention in 4 districts. They were Yayasan Rumsram in Biak Numfor, CD Bethesda YAKKUM in Sumba Barat and Sumba Barat Daya, and Yayasan Masyarakat Peduli in Lombok Timur. While Yayasan Plan International Indonesia continued working in Dompu until August 2019 and continues implementation in Lombok Utara until June 2020. Likewise, Yayasan Dian Desa continues working in Manggarai Barat until June 2020. In 2019, SEHATI focused on strengthening the exit strategy in Dompu and continuing advocacy for accelerating sanitation progress after the mid 2018 earthquakes in Lombok Utara. Additionally, in Manggarai Barat SEHATI continues advocating local government to replicate STBM in other villages. SEHATI also started integrating Menstrual Health Management in both districts. Figure 2 below demonstrates the overall capacity improvement of all stakeholders in the 7 intervened districts in the period of 2016 – 2019. How the percentages in the graph below are calculated, can be seen in Annex 1.
Figure 2. Capacity Scores for all stakeholders in 7 districts in 2016 - 2019
As shown in the figures above, the capacity scores of SEHATI partners, sanitation entrepreneurs, sub-district, district health office and district (POKJA) in implementing and continuing STBM 5 pillars in
16
their respective areas are consistently improving from 88%, 40%, 50%, 76% and 74% in the beginning of the project in 2016 to 98%, 96%, 93%, 98% and 98% at the end of 2019, respectively. Immense development can be seen in sanitation entrepreneurs and sub-district level that are rising from 40% and 50% in 2016 to 96% to 93%. These two actors are considered as the key of STBM implementation and therefore, besides lobby and advocacy at district level, SEHATI emphasises capacity building on them. Scores at district level which separated into POKJA and District Health Office are also climbing significantly from 74% and 76% respectively in 2016 to 98% for both of them in 2019. Personal and professional approaches conducted by SEHATI partners in lobbying and advocacy are viewed as pivotal measures to this success. In this report, Simavi will highlight the overview in Dompu, Lombok Utara, and Manggarai quantitatively and qualitatively as in these districts, SEHATI continued working in 2019. Nevertheless, Simavi will also elaborate qualitatively on the progress in the other 4 districts where SEHATI ended in 2018. Overview Dompu, Lombok Utara and Manggarai Barat up to 2019
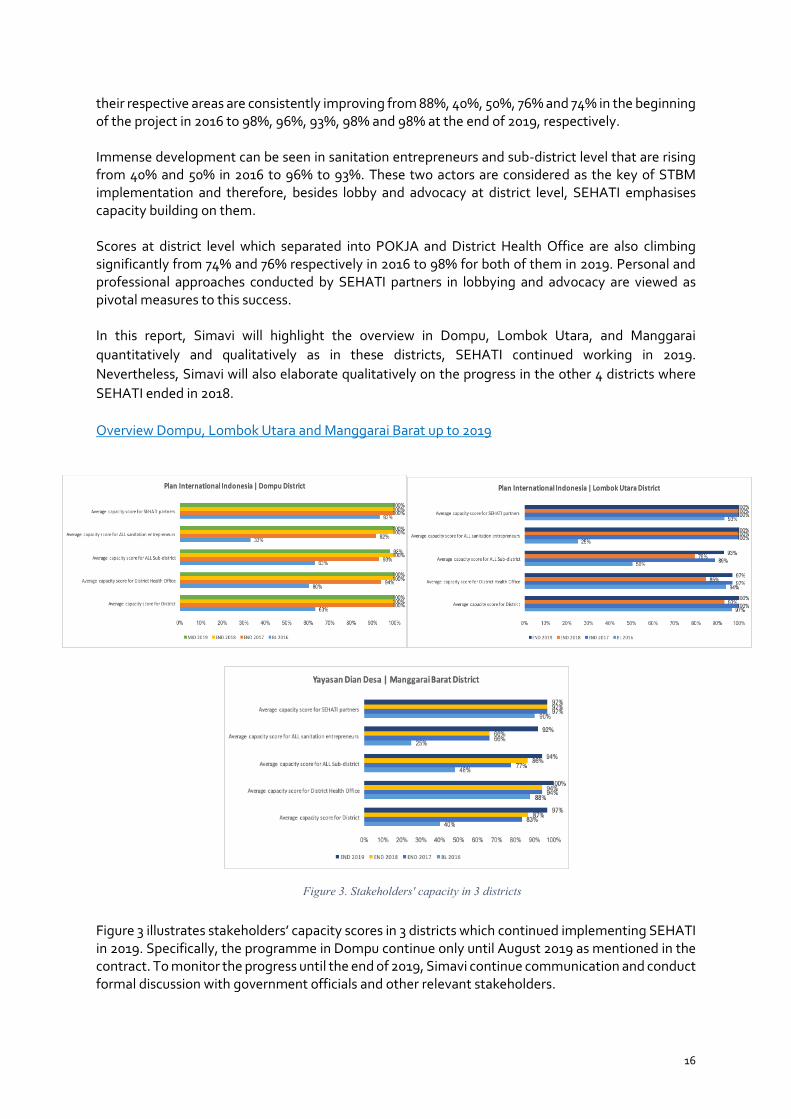
Figure 3 illustrates stakeholders’ capacity scores in 3 districts which continued implementing SEHATI in 2019. Specifically, the programme in Dompu continue only until August 2019 as mentioned in the contract. To monitor the progress until the end of 2019, Simavi continue communication and conduct formal discussion with government officials and other relevant stakeholders.
Figure 3. Stakeholders' capacity in 3 districts
17
Above figure shows positive performance in Dompu since 2016 until 2019 for SEHATI partner, sanitation entrepreneurs, district health office and district government (POKJA AMPL) by reaching 100% in 2019. However, scores for sub-district level slightly decrease from 100% in 2018 to 98% in 2019. It is worth noting that this decrement took place because a few sub-districts allocated smaller funds for STBM in 2019 in their areas, as the villages have gotten Village Fund and support from District Budget in implementing STBM. Given the achievement have made by the Dompu local government, it allows SEHATI to exit from the district in August 2019 as we see that the government is able to continue the implementation throughout the district with their own resources. Similar to Dompu, promising performance is showed by the stakeholders in Manggarai Barat. Theigure above illustrates notable increment of the capacity since 2016 to 2019. Even so, some aspects need to be improved such as execution of budget for STBM, strategic planning at district level and ensuring the quality of scaling up in non SEHATI areas. As Manggarai Barat is now appointed by the President of Indonesia to be one of the 10 premium tourism destinations, there is a challenge within government bodies to prioritise several programmes in 2020. On the contrary, fluctuating performance happened in Lombok Utara. As mentioned in the previous annul report of 2018, Lombok Utara faced severe earthquakes in mid 2018 and it caused devastation in access to water and sanitation as well as planning and budgeting of local government. Figure 3 also shows the decrement of capacity of stakeholders in Lombok Utara in 2018 especially at sub-district, district health office and POKJA AMPL. Within one year, the capacity of those actors escalates remarkably. Progress in Sumba Barat Daya, Sumba Barat, Biak Numfor and Lombok Timur up to 2019 During the closing workshop in Dompu in August 2019, Simavi invited representatives of government from 4 districts in which SEHATI has left in 2018. The discussion focused on sustainability of STBM until 2019 and challenges that might be faced by the government. The progress can be seen below table.
Table 1. Progress of STBM implementation in the district SEHATI ended in 2018
Districts Progress Challenges Sumba Barat Daya - Up to 2019, there are 44 villages
declared 100% STBM 5 pillars. Those are SEHATI and non SEHATI villages. It shows that even after SEHATI left the district, the government continued working on STBM in the whole district. Government provided support by using district annual budget and special fund for sub-districts in implementing STBM (11 sub-districts)
- Even though the Head of District was elected in 2018, the new Bupati continued to enforce STBM related regulation and provide support in ensuring the implementation at lower level.
- Strict culture in Sumba that allow people to live closely with animal husbandry and this challenges government to separate human and animal waste, including to ensure that they practice healthy behaviour.
- Slippage3 might happen due to people’s activities in the field and during take care of their animals.
- District legislation seems to be infirm when it comes to the implementation in most cultural villages.
3 Slippage is the situation when people go back to their previous behaviour, for instance, people have built toilets but as they do not get used to it, they tend to defecate in the open again.

18
Districts Progress Challenges - As mandated by the Ministry of Health,
some villages in Sumba Barat Daya are selected to be pilot project for healthy villages. The government find it very important to sustain 5 pillars of STBM to achieve this target.
Sumba Tengah - New Head of District was selected in 2018 and the implementation of the programme is still being continued. Also, the Head of District has a liveable housing programme for poor families and – unlike the central government programme which usually constructs houses without a toilet - the Bupati directed to allocate budget for constructing toilets in line with the housing programme.
- There are 65 villages that are selected for the housing programme with toilet construction by which each village gets 4,200 EUR to build the toilets in the selected families.
- Similar to Sumba Barat Daya, the district government in Sumba Tengah face the same challenges. This cultural obstacle is contributed by the design of stilt houses in which Sumbanese people live in super-buildings and animals/ livestock stay under it.
- By providing a housing programme, the government tries to re-design the houses in order to separate the human and animal waste.
Biak Numfor - Out of 257 villages in Biak Numfor, 246 villages have been intervened by the government (with support from Yayasan Rumsram in the past) to implement the 5 pillars of STBM.
- Additional 4 villages have declared 100% STBM in 2019. It is important to note that during SHAW, Simavi and her partner contributed to declare 35 villages and during SEHATI, Simavi declared 9 villages. Hence, in total, there are 48 (out of 257) STBM/ODF villages in Biak Numfor.
- Similar to Sumba Tengah and Sumba Barat Daya, Biak Numfor is also run by a new head of district since 2018. Fortunately, the head of district supports the implementation of STBM and sets targets for STBM district in 2023. It means that all villages in the whole district should implement the 5 pillars STBM by 2023.
- The geographical condition in Biak Numfor is dry area and most villages are scattered. This situation affected the availability of adequate human resources in Biak Numfor to implement the 5 pillars of STBM.
- Several changes of team of STBM facilitators took place due to the election of the Bupati. Therefore, the government views that new facilitators need to be trained on technical aspects of the 5 pillars of STBM by higher level, such as provincial or central government.
Lombok Timur - The government is still continuing the cascading monitoring up to village level. Coordination amongst district, sub-district, and village government have been made available up to date.
- The government has replicated the 5 pillars of STBM in 20 villages in 2019.
- Government has a new collaboration with UNICEF and Mercy Corps to continue working on STBM.
- Monitoring and re-verification in the whole villages need to be done to get current figures after earthquakes in 2018.

19
Figure 4. Closing workshop of SEHATI Programme in 5 districts, conducted in Dompu, August 2019
In early 2019, Simavi organised an external evaluation of the SEHATI programme by hiring an independent consultant. The objective was to evaluate the entire implementation from the beginning of the project up to 2019. The study focused on the evaluation indicators that had been set such as relevance, effectiveness, efficiency, impact and sustainability of SEHATI in the 7 districts. The evaluator team found that lobbying and advocacy since the beginning of the programme is an effective way to encourage local governments to implement and sustain a sanitation programme. Despite positive results and trends, the evaluator team also foundthat SEHATI intervention areas still face some challenges such as inconsistency of local governments in implementing sanitation projects in some districts due to weak leadership and coordination amongst stakeholders. The comprehensive report of the evaluation can be found in this link: https://rsr.akvo.org/media/db/project/5783/document/20191018_Final_feedback_proofread_ismah.pdf. Apart of the evaluation process, Simavi will also elaborate the achievements and challenges that raise up during the reporting period in this document. Outcome 1. Capacity, leadership and commitment strengthening of local government (at all levels) to implement and sustain the 5-pillars of STBM In its Monitoring & Evaluation framework, SEHATI assumes that capacity, leadership and commitment of local governments can be measured from specific aspects, namely the (i) inclusion of STBM in government’s annual work plans and budgets, (ii) availability of STBM related regulation, and (iii) availability of STBM teams formed by local authorities as well as the skills of teams to implement STBM at the lower level and to monitor the progress of STBM. The figures in Table 2 are taken from the annual planning and budget documents in district, sub-district and village governments. The table shows the budget allocation by district, sub-district and village levels for implementing and sustaining STBM, both in SEHATI villages and non SEHATI villages in the 7 districts. While the table above presents the budget on a 6-monthly basis, it is critical to note that the district governments actually prepare budgets on an annual basis with possibility of

20
revision at the second term of the year. As shown by the table, there has been a consistent increment of budget allocations from local governments since SEHATI started in 2016. While SEHATI partners acknowledge that there might be other initiatives contributing to this increment, SEHATI partners believe that this increment, to certain extent, is contributed by the SEHATI programme. Financial allocation to implement STBM
Table 2. Financial allocation at government level from 2016 – 2019
ALL PARTNERS | ALL DISTRICTS | EURO Strong leadership, commitment and improved capacities of the local government (district and sub-district level) to implement and sustain the STBM 5-pillars
2016 MID 2017 END 2017 (REVISION) MID 2018 END 2018
(REVISION) MID 2019 END 2019 (REVISION)
Budget amount allocated for STBM related activities (district government's budget through APBD and ADD) 514.932 941.389 949.053 1.086.210 1.936.307 3,020,587 2,807,233 Total amount released for all SEHATI sub-districts (sub-districts' budget/BOK) 29.000 82.269 133.414 118.282 43.237 38,969 69,930 Total amounts released for all SEHATI villages (village fund through Dana Desa/DD) 354.904 972.649 861.878 725.605 278.323 320,230 846,186 Total amounts released for all non-SEHATI villages (village fund through Dana Desa/DD) - 105.184 288.944 263.059 86.222 182,562 404,371
It is worth nothing that there is a stark decrement of figures in END 2018 and END 2019, in particular in the sub-districts. This decrement is caused by the reduced number of intervened districts from 7 to 3 districts at mid 2018 and from 3 to 2 intervend districts at mid 2019. In contrast, the contribution from district and village governments seem high in 2018 and 2019 because due to the mid 2018 earthquakes, the government of Lombok Utara spent much budget for constructing access to water and sanitation for community and it continues in 2020. In addition, non SEHATI villages which replicate the 5 pillars of STBM contribute to this high figure. SEHATI partners have also engaged local governments to provide smart subsidy for the communities. This subsidy scheme is made as such for constructing toilets, district or village governments will buy products or services from local entrepreneurs (and give them to communities) and ask for contributions from the community in the form of in-kind contributions. Such in-kind contributions have been monetised as shown in the table below.
Table 3. Community Contribution to STBM implementation ALL PARTNERS | ALL DISTRICTS | EURO 2016 2017 2018 2019 Community contribution 44.665 127.724 2.557.588 338,676
The table above demonstrates the increase of community contribution in supply side to fulfil their needs in sanitation and hygiene practices. In 2016, a limited number of people contributed to constructions of toilets (about EUR 45.000), and this figure keeps increasing until at the end of 2018,

21
with more than 2 million Euro was spent by communities to improve their healthy lives, such as constructing toilets, making hand washing facilities and communal rubbish bins, etc. In 2019, SEHATI monitored few contributions from community in providing access to sanitation (around EUR 338,000). This contribution was mostly coming from households that did not construct their access to sanitation in the previous years of the programme. The number dropped because investments were already made in previous years, and it also dropped because in 2019 the SEHATI programme was only still running in 3 districts (and 2 since September 2019), compared to 7 in the previous years. The contribution of the communities along with the budget provided at government level are summarised per year in annex 1 (adjusted with EKN framework). STBM related regulation to support and sustain the implementation of the programme
Table 4. Number of STBM related regulation in the districts
ALL PARTNERS | ALL
DISTRICTS Supportive legislation is in place BASELINE END 2019 STBM related regulation at district level 3 28 STBM related regulation at village level, under the leadership of sub-district authority 0 22
With regards to STBM-related regulation, there was a significant improvement in the period of 2016 to 2019 as a result of SEHATI partners’ advocacy efforts in their respective areas. The forms of regulations resulted at district level were varied, such as Perda (Peraturan Daerah) on AMPL (in Dompu), Perbup (Peraturan Bupati), Instruction of Bupati, SK and STBM related circular letters. In short, 28 STBM-related regulations have been made available at district level by the end of 2019. In 2018, SEHATI reported 27 STBM related regulation at district level were issued. During reporting period 2019, SEHATI succeeded to add one more regulation in Lombok Utara which is an instruction letter signed by the Head of District. This letter instructs all government bodies to accelerate the construction of household toilets post disaster. Though it is issued in 2019, it will be executed effectively during the fiscal year of 2020. The Head of District instructed to construct 5,910 units of household toilets of which separated into two different financial sources, namely District Annual Budget and Village Fund. Equally important, partners have encouraged village governments to issue regulations at village level called Perdes (Peraturan Desa) or village rules (awik – awik). Perdes are issued by heads of villages through which they are allowed to allocate budget and adopt local wisdoms and norms for STBM programmes. Out of 215 target villages in SEHATI, 22 villages have proclaimed Perdes at the end of 2018.
“The involvement of SEHATI in the sanitation programme in Lombok Utara is very helpful for us. Not only do Yayasan Plan International Indonesia and Simavi strengthen our capacity in POKJA AMPL, but also support us with “out of the box” ideas to accelerate the progress in Lombok Utara. We do have a programme and budget in place, but we did business as usual and it which resulted that not everybody was able to get access to sanitation facilities. Through SEHATI, we now really understand how to ensure that no one is being left behind,” said Yuni Kurniati, secretary of Planning and Development Agency of Lombok Utara during SEHATI closing workshop in Dompu, 2019.

22
People trained to implement STBM at all level
Table 5. Number of people trained in SEHATI Programme
ALL PARTNERS | ALL DISTRICT
2016 END 2017 MID 2018
(7 DISTRICTS) END 2018
(3 DISTRICTS) END 2019
(2 DISTRICTS) # of authorities trained in STBM approaches and methodologies, monitoring, verification (all levels)
2.721 3.899 3.280 1.347 905
➔ Number of females trained 1.567 2.142 1.651 691 512
➔ Number of males trained 1.154 1.757 1.629 656 393
Table 5 shows the total number of people trained during the implementation of the SEHATI programme and the division of females and males in the team. The numbers differ per period due to staff rotation at district, sub-district and village levels. A few refreshment trainings for previous and new team members were conducted during the implementation period to fill the gap of capacity when existing team members were rotated to other departments. It is important to note that lesser result in MID 2018, END 2018 and END 2019 were due to lesser districts, from 7 to 3 districts in 2018, and 3 to 2 districts in 2019. Table 6 below is added to inform about the total number of new people trained in STBM institution. The organisations enhanced by SEHATI consist of organisations at district level called POKJA AMPL, technical STBM teams at district, sub-district and village level as well as sanitation entrepreneurship forums. This information has been adjusted with EKN framework and is available on Annex 1.
Table 6. Number of people trained in STBM institution
Baseline 2016 2017 2018 2019 0 2.721 279 280 247
Cumulative result 3.527 people Number of institutions strengthened per period can be seen on below table:
Table 7. Number of WASH organization strengthened Baseline 2016 2017 2018 2019
0 222 42 18 0 Cumulative result 282 organisations
Skill of teams to train the lower level and to monitor the progress of STBM After more than three years of implementation, SEHATI partners view that the capacity of district teams (especially District Health Office) is ample to train the lower levels such as Puskesmas (primary health care) and village cadres. Staff rotation within the team keeps happening due to political situation in the village or even at the district. However, as in the previous year, this situation challenged the programme implementation, at the moment, the knowledge and skills can be somewhat easy to transfer as the old staff are confident enough to train new appointed staff or lower level with less supervision from SEHATI partners. In Manggarai Barat, some refreshment trainings have been conducted in 2019 at village level based

23
on the request of village authorities. For instance, STBM facilitation and data collection training are conducted for village cadres especially in replication areas. Whereas in Lombok Utara, some refreshment trainings are conducted almost at all levels to maintain the capacity and motivation of team members after the natural disaster in 2018. SEHATI implementation partners also conducted MHM training, monitoring data collection and submission to m-water and STBM – GESI facilitation. To improve the capacity of partners and local governments, Simavi views that the topic of Leave No One Behind needed to be shared to them. Therefore, in November 2019, Simavi trained Yayasan Plan International Indonesia, Yayasan Dian Desa, and representatives of POKJA AMPL in regards to social inclusion (especially the term of Leave No One Behind that is mandated by SDGs 2030) to ensure that the government will involve marginalised groups a well in the process of decision making and prioritise their special needs in regards to water and sanitation.
Gabriel Matus, head of Tengku Village in Manggarai Barat has implemented a reward and punishment scheme related to STBM for community members. He also conducts village cleaning activities every Sunday and he asks all community members to clean their houses, toilets, surroundings and streets to ensure that the village is clean. For those who are not actively involving in the Sunday activity, they will not get smart subsidy from the village government.
Outcome 2. Capacity improvement of CSOs on lobbying and advocating local government to lead STBM implementation SEHATI measures the capacity of CSOs on lobbying and advocacy from two aspects, which are (i) skills on Lobby & Advocacy as well as (ii) coaching and mentoring the local government to implement STBM. In general, Simavi is confident to conclude that all SEHATI partners have adequate capacity to lobby and advocate local government to lead the implementation of STBM in their respective districts. It is proven by the increase of capacity of stakeholders from different levels as described in the general overview. SEHATI partners have been engaging and collaborating with several other NGOs. To illustrate, after engaging Yayasan We Care in Dompu in 2018 in providing waste management solution, Yayasan Plan International Indonesia engages FORMASI (a community-based water and sanitation care) in supporting district and village governments to issue STBM related village regulation. Similarly, Yayasan Dian Desa continued engaging a community-based cooperative in supporting a waste bank as one of SEHATI’s effort to tackle the waste issue in Labuan Bajo. Additionally, at national level, Simavi and her partners excellently shared some best practices within Jejaring AMPL (drinking water and health environment network) and other ministries. For example, Simavi and her partners were involved in the National Conference of Water and Sanitation, discussion on the revision of STBM related regulation with the Ministry of Health; and with Menstrual Hygiene Day in which Simavi encouraged stakeholders to consider providing women friendly sanitation facilities in STBM programmes and not only focus on eradicating open defecation. During the closing workshop for 5 out of 7 districts within the SEHATI programme in Dompu in August 2019, Simavi also shared the guideline of the SEHATI approach (replication model) for the local and national governments. General information about this approach had been discussed in the

24
previous annual report 2018 under Outcome 4. This guideline allows local government to continue working on STBM in non SEHATI areas as well as supports national government to scale up the 5 pillars of STBM to other districts. Equally important, it allows the national government to review the role of provincial level on STBM that have not been specified clearly under current regulation. Another best practice that has been done by the SEHATI is programme coordination (PC) meetings which were organised on a regular basis. It allows partners and local governments to learn from each other and to gain more capacity and knowledge. Besides, the participation of national government (Bappenas and MoH) is considered important in the meetings. Not only did they provide SEHATI partners with current policy and input for further implementation, but also attained more insight about current conditions, achievements and progress on the 5 pillars of STBM at district level which enabled them to develop strategic planning at national level. As a result of the successful implementation of SEHATI, Dompu District became a referral area for other districts, especially in Eastern Indonesia, to learn about the 5 pillars of STBM implementation. Study visits have been made available by other programmes in NTB and NTT such as Water for Women project funded by DFAT Australia and Women Disability Inclusive Wash and Nutrition funded by DGIS The Netherlands. This exchange learning is boosting the motivation of the government of Dompu in continuing the implementation even after SEHATI ended in August 2019.
Figure 5. Plastic waste collection in collaboration with Yayasan We Care in Dompu
Outcome 3. Capacity support to private sector for improved supply of WASH products and services Since the beginning of the programme in 2016, SEHATI has been engaging sanitation entrepreneurship and has developed marketing strategies along with potential entrepreneurs and local governments. The capacity of sanitation entrepreneurs in the 7 districts can be seen in the general overview in the previous section. In general, the capacity of sanitation entrepreneurs significantly increased from 40 % in 2016 to 96% in 2019. This increment was contributed by the successful collaboration amongst SEHATI partners, sanitation entrepreneurs and local government. In Manggarai Barat, Yayasan Dian Desa advocates villages authorities to provide some budget (with smart subsidy scheme) from Village Fund to support communities in providing toilets. With this budget, the authority orders a certain amount of toilet construction from local entrepreneurs. Likewise, in Lombok Utara and Dompu, Yayasan International

25
Indonesia encouraged district government to involve local entrepreneurs in the programme implementation. To elaborate the output of private sector collaboration during SEHATI implementation until 2019, the table below presents the data per monitoring period.
Table 8. Output for private sector collaboration within SEHATI Private Sector Collaboration | ALL PARTNERS | ALL DISTRICTS Increased private sector collaboration to improve supply of WASH products and services
2016 2017 2018 2019
Cumulative
Average number of customers per sanitation entrepreneur 93 260 193 135 681
# people that accessed or acquired sanitation products or services 1.144 7.090 12.060 8.350 28.644
# of sanitation entrepreneurs that have established viable sanitation businesses 186 628 593 452 1.859
# of sanitation products sold - 21.213 13.794 8.636 43.643 Table 8 shows the output of private sector collaboration with SEHATI in 4 indicators, namely: (i) the average number of customers per sanitation entrepreneurs, (ii) total number of people that accessed or acquired sanitation products or services, (iii) total number of sanitation entrepreneurs that have established viable sanitation businesses, and (iv) total number of sanitation products sold. As seen in the table, the demand for STBM-related products and services are higher in 2017 than in other periods. In 2016, when SEHATI started, only a few villages and communities responded to STBM implementation right away. Local governments provided adequate budgets to construct toilets for the poorer households gradually in 2017, 2018 and 2019. In addition, most villages have been triggered in 2017, hence the demand for products or services was higher in 2017. It is very likely when a village has been declared 5 pillars of STBM, the demand of products and services will be diminished. Therefore, SEHATI is now focusing on a strategy to sustain the sanitation entrepreneurs and improve their various products and services. In 2020 this private collaboration will be scaled up by setting up a production hub of reusable sanitary pads in Labuan Bajo, Manggarai Barat; and by a collaboration between Plan Indonesia, Nazava water filters and the micro-finance facility Komida in Lombok Utara. Up to 2019, several products and services have been made available in the districts, for instance toilet seats, whole packages for toilet construction, herbal soap, water filters (SEHATI collaborates with Nazava, a Bandung based water filter company), locally made rubbish bins, and SPAL construction. In terms of infrastructure such as toilets, Simavi encouraged entrepreneurs to adjust the design to meet the need of women and people with disabilities, children and elderly people. More information about this adjustment will be elaborated under the Gender Equality and Social Inclusion (GESI) section. As mentioned in previous annual report 2018, a collaboration with a private company has occurred. POKJA AMPL in Dompu district has been working together with a mining company, Sumbawa Timur Mining, Ltd, to implement the village participation programme in 8 villages including toilet constructions for poor families in respective villages. SEHATI also encouraged sanitation entrepreneurs to work with Bumdes (village owned enterprises) if available. In Dompu and Lombok Utara where Bumdes have been established, this collaboration works well. However, not every village in other districts have developed Bumdes due to lack of knowledge to run the institution. One challenge that SEHATI found since 2016 regarding the sustainability of sanitation entrepreneurs is capital gain for small-scale entrepreneurs. SEHATI tried to collaborate with financial institutions

26
such as local bank or cooperatives to provide long term loans for the entrepreneurs. However, this partnership mechanism has not established yet. The banks view that this business seems worrisome prospects. Even though SEHATI partners have tried to discuss this with local governments, the banks are not convinced yet.
Yosef Arun, a local mason of Ndoso Sub-district, Manggarai Barat started working as a toilet making entrepreneur since 2018 after joining the sanitation entrepreneurs training conducted by Yayasan Dian Desa. He said that being a sanitation entrepreneur is helping him to gain new income for his family. At the same time, his new skills can contribute to the health environment in his village and it is related to his belief to help people.
In order to support local authorities and stakeholders in replicating the business model of supply side, SEHATI has finalised several education videos in 2019:
a. Toilet seat making process b. Healthy toilet construction c. Herbal soap making process d. Sanitation Microfinance system through BumDes e. Reusable sanitary pad making process
All of videos have been uploaded onto AKVO RSR and can be accessed through this link: https://rsr.akvo.org/en/project/5783/. Outcome 4. The development of a viable implementation model that ensures local government is capable to roll out and sustain a district wide STBM 5 pillars Since 2017, SEHATI partners have been developing a replication model to enable districts and the national government of Indonesia to replicate the SEHATI approach to other areas. This model was also introduced to stakeholders during the Horizontal Learning event in Jakarta which was held by Simavi in July 2018, from which SEHATI gained inputs for an improvement. After several follow-up meetings and discussions, Simavi, in collaboration with IRC, has come up to a final version regarding the SEHATI replication model. The replication model focuses on several aspects, as follows:
a. Relevance of Theory of Change of SEHATI b. Implementation phase of SEHATI c. Replication results during SEHATI implementation
The comprehensive document regarding this model has been finalised and shared to relevant stakeholders at national and local level during the closing workshop for 5 out of 7 disitricts of the SEHATI programme in Dompu in August 2019 and important meetings at the Ministry of Health and Bappenas. Additionally, during World Water Week in Stockholm in August 2019, Simavi had the opportunity to discuss with relevant international stakeholders about the approach and achievements that have been made by local government in Indonesia to tackle sanitation matters. The guideline of SEHATI approach (replication model) can be found in this link:

27
https://rsr.akvo.org/media/db/project/5783/document/FINAL_replication_paper_ENG-compressed-2.pdf Replication Result during SEHATI implementation Local governments have started replicating the SEHATI approach to other villages since 2017. The table below shows the number of villages where the SEHATI approach is replicated and their result towards ODF / STBM declaration.
Table 9. Number of villages that replicate the SEHATI approach ALL PARTNERS | ALL DISTRICTS
Original target of replication areas Current replication areas ODF / STBM verified
villages in replication areas Sumba Barat Daya 6 17 3 Sumba Tengah 0 0 0 Manggarai Barat 30 77 19 Dompu 15 15 9 Lombok Utara 17 15 0 Lombok Timur 21 63 10 Biak Numfor 30 0 0 TOTAL 119 187 41
Table 9 illustrates the number of villages within the 7 districts that have implemented STBM using their own resources. Up to 2019 there are 187 villages outside the SEHATI intervention area that replicated the approach. It is around 157% higher than the original target in each district. In addition, out of 187 villages, 41 villages have been declared ODF/STBM. In total up to 2019, SEHATI has been reaching out to 402 villages (including current intervention villages). As mentioned in the previous annual report 2018, it is crucial to note that there is no replication village in Sumba Tengah as all other villages have been intervened during the SHAW programme (2010 – 2015). While in Biak Numfor, even though the government stated that they have intervened 246 villages with the 5 pillars of STBM as mentioned in General Overview section, Simavi could not get the exact figures of which non SEHATI villages that have been intervened. That is why, in this report we conclude to exclude the figure of replication villages in Biak Numfor.
Hendrikus Medo is the head of Sama Village, Kuwus Sub-district, Manggarai Barat. Sama Village is a replication village that has been declared 5 pillars of STBM in November 2019. With his commitment, he allocated budget from the Village Fund to train cadres, toilet construction training and provide smart subsidy for poor people. One innovation that he and his community members made was constructing septic tanks using plastic drums (containers), as concrete is not available in the village.

28

29
Impact of the SEHATI implementation at community level 5 pillars of STBM at household level The impact of the SEHATI intervention in 215 villages after four-year implementation is described in this section.
Figure 6. Proportion of ODF and STBM verified villages in SEHATI areas
The pie chart on Figure 4 shows that 47 villages have been declared ODF (Open Defecation Free) and 60 villages have been declared STBM. This figure shows an increases 20 villages in 2019 compared to achievement in 2018. It means that by the end of 2019 107 out 215 villages have been declred free from Open Defecation and have been practicing healthy behaviour. Villages that have been declared in Lombok Utara before the earthquakes in mid-2018 are now able to achieve their ODF/STBM status with support from district government and Yayasan Plan International Indonesia.
Table 10. Total villages declared ODF/STBM in 7 districts
ALL PARTNERS | ALL DISTRICTS
SEHATI villages
Declared villages
Replication villages
Declared villages
All villages 215 107 187 41
TOTAL 402 STBM intervened villages
148 declared villages As mentioned in the previous annual report 2018, Simavi and her partners also found that it takes 0.5 to 1.5 years (average) to declare one village for the 5 pillars of STBM in the ideal situation. An ideal situation means that the condition is conducive for a speedy progress and that there are no significant hindering factors. A few factors for conducive conditions are:
a. Higher education levels of the community that might influence awareness b. Higher access to water levels c. Smaller population and area of villages
215
47
60
All partners | All districts
Total villages ODF certified villages STBM 5 pillars verified villages

30
Factors that might impede the progress in the villages are:
a. High staff rotation of STBM teams at all levels that could be related to political issues at district and village level
b. Lack of commitment of team members to allocate time for STBM and team members might have other tasks from their superiors
c. Lack of access to safe water In Biak Numfor, where political issues were quite dominant, it took more than 1.9 years for aone village to declare ODF/STBM. Villages in Lombok Timur took (in average) 1.9 year to declare ODF/STBM due to the high population factor. At SHAW villages in Lombok Timur, Biak Numfor and Sumba Barat Daya4, Simavi and her partners found it somewhat difficult to calculate an average time to declare ODF/STBM as it took more than 7 years to declare. Out of the 56 SHAW villages in those districts, only 7 villages declared ODF/STBM during the SEHATI programme due to reasons or factors mentioned above. Data on behaviour change in each district is shown in below tables.
Table 11. General information at community level Indicators Baseline 2016 END 2019
# of kecamatan 45 53 # of desa 195 215 # of people 468.367 511.631
# of females 238.598 258.332 # of males 229.769 253.299
# of houses 124.772 126.549 Total number of houses with access to toilet 94.089 112.369 a. # of houses with own toilet 81.073 101.884 b. # of houses that do not have toilets but
share a toilet of others 13.015 10.485
Total number of houses without access to toilet
28.319 14.180
# of schools 964 970 # of health facilities 709 780 # of religious places 1.185 1.200
Table 11 presents general information at community level. At the end of 2019, SEHATI has reached out to 53 sub-districts, 215 villages and more than 500.000 people. SEHATI also has reached 970 schools, 780 health facilities and 1.200 religious places. For those facilities, Simavi and her partners only monitor the implementation of pillar 1 (the presence, usage and maintenance of toilets) and pillar 2 (the presence and usage of hand washing facilities). It is worth noting that there is increment of total number of houses that have access to sanitation in 2019 compared to 2016 with around 16% of increment.
4 There are 12, 24 and 20 villages in Lombok Timur, Biak Numfor and Sumba Barat Daya, respectively, that have been intervened STBM since SHAW programme and they were continued in SEHATI programme.
31
Figure 7. Access to sanitation based on JMP definition
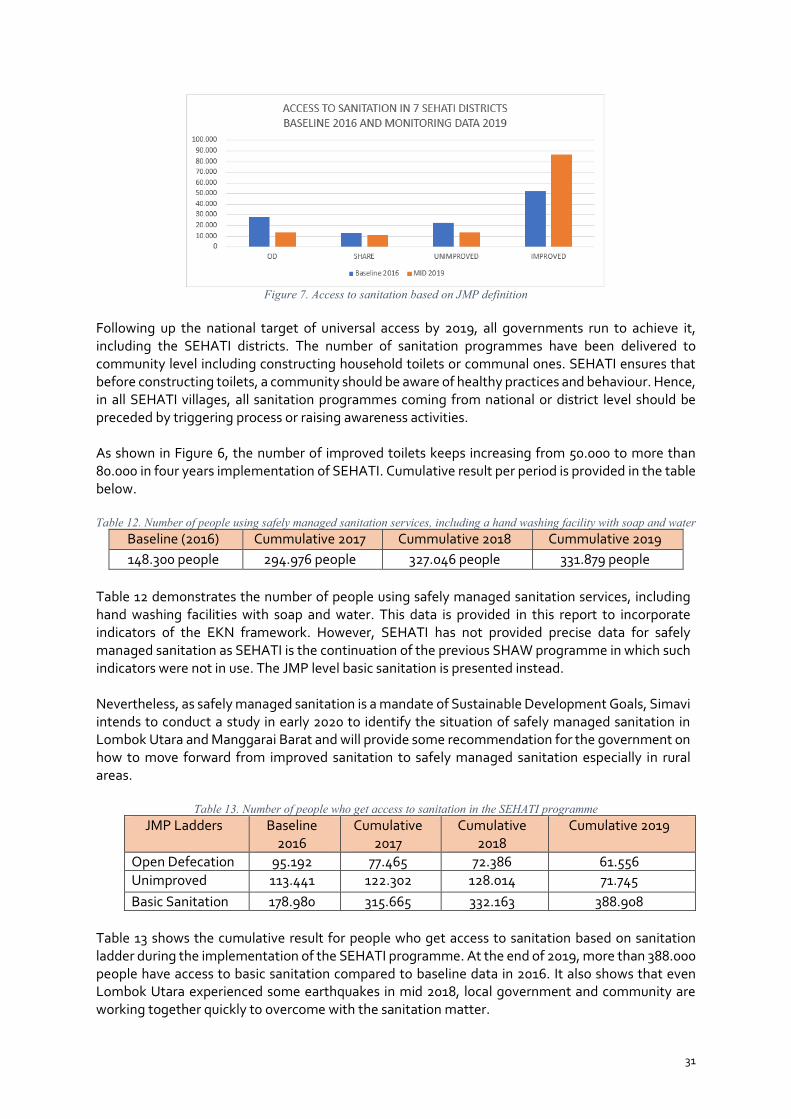
Following up the national target of universal access by 2019, all governments run to achieve it, including the SEHATI districts. The number of sanitation programmes have been delivered to community level including constructing household toilets or communal ones. SEHATI ensures that before constructing toilets, a community should be aware of healthy practices and behaviour. Hence, in all SEHATI villages, all sanitation programmes coming from national or district level should be preceded by triggering process or raising awareness activities. As shown in Figure 6, the number of improved toilets keeps increasing from 50.000 to more than 80.000 in four years implementation of SEHATI. Cumulative result per period is provided in the table below. Table 12. Number of people using safely managed sanitation services, including a hand washing facility with soap and water
Baseline (2016) Cummulative 2017 Cummulative 2018 Cummulative 2019 148.300 people 294.976 people 327.046 people 331.879 people
Table 12 demonstrates the number of people using safely managed sanitation services, including hand washing facilities with soap and water. This data is provided in this report to incorporate indicators of the EKN framework. However, SEHATI has not provided precise data for safely managed sanitation as SEHATI is the continuation of the previous SHAW programme in which such indicators were not in use. The JMP level basic sanitation is presented instead. Nevertheless, as safely managed sanitation is a mandate of Sustainable Development Goals, Simavi intends to conduct a study in early 2020 to identify the situation of safely managed sanitation in Lombok Utara and Manggarai Barat and will provide some recommendation for the government on how to move forward from improved sanitation to safely managed sanitation especially in rural areas.
Table 13. Number of people who get access to sanitation in the SEHATI programme JMP Ladders Baseline
2016 Cumulative
2017 Cumulative
2018 Cumulative 2019
Open Defecation 95.192 77.465 72.386 61.556 Unimproved 113.441 122.302 128.014 71.745 Basic Sanitation 178.980 315.665 332.163 388.908
Table 13 shows the cumulative result for people who get access to sanitation based on sanitation ladder during the implementation of the SEHATI programme. At the end of 2019, more than 388.000 people have access to basic sanitation compared to baseline data in 2016. It also shows that even Lombok Utara experienced some earthquakes in mid 2018, local government and community are working together quickly to overcome with the sanitation matter.

32
Regarding number of people living in Open Defecation communities until 2019, SEHATI monitored the progress only in the ODF/STBM declared villages. The result is presented in Table 14 below.
Baseline (2016) Intervention (2016)
2017 2018 2019
30.214people (15.500 females)
220 people (115 females)
35,512 people (17,554 females)
127,749 people (65,559 females)
13.145 people (7.314 females)
Table 14. Number of people living in open defecation free communities (ODF / STBM villages) Regarding the achievement in other pillars, Simavi measured the progress based on STBM criteria that have been set up since the beginning of the SEHATI programme.
Figure 8. Progress of 5 pillars of STBM
Figure 7 illustrates that the achievement for all pillars up to 2019 rose significantly compared to the baseline in 2016. However, only pillar 1 increased almost to 70% at the end 2019 while pillar 2 increased to 50% and other pillars are still below 50%. As mentioned in the previous section, it takes around 0.5 – 1.5 year to declare a village ODF/STBM, and therefore it is understandable that behaviour change at community level moves with leaden steps especially on pillar 3 - 5. In addition, Simavi monitored the access to safe water as it is the basic criteria when selecting the intervened villages. However, SEHATI decided to include villages that have limited access to safe water due to request of local governments for SEHATI to support certain villages. Hence, this monitoring result will help them to improve the access to safe water in respective areas. Based on figure 7, a little progress has been made to increase the access to safe water in the villages. STBM at schools and other facilities Simavi has also been monitoring the implementation of STBM in several facilities such as schools, health care centres, religious places and public facilities. The general information for these facilities has been made available in Table 9 while Table 13 provides the progress in each facility.
0102030405060708090
100
PILAR 1 -IMPROVED
TOILET
PILAR 2 - HANDWASHING
PILAR 3 -DRINKING
WATER ANDFOOD STORAGE
PILAR 4 - SOLIDWASTE
MANAGEMENT
PILAR 5 - LIQUIDWASTE
MANAGEMENT
ACCESS TO SAFEWATER
5 Pillars of STBM in 7 Districts
BASELINE 2016 END 2019
33
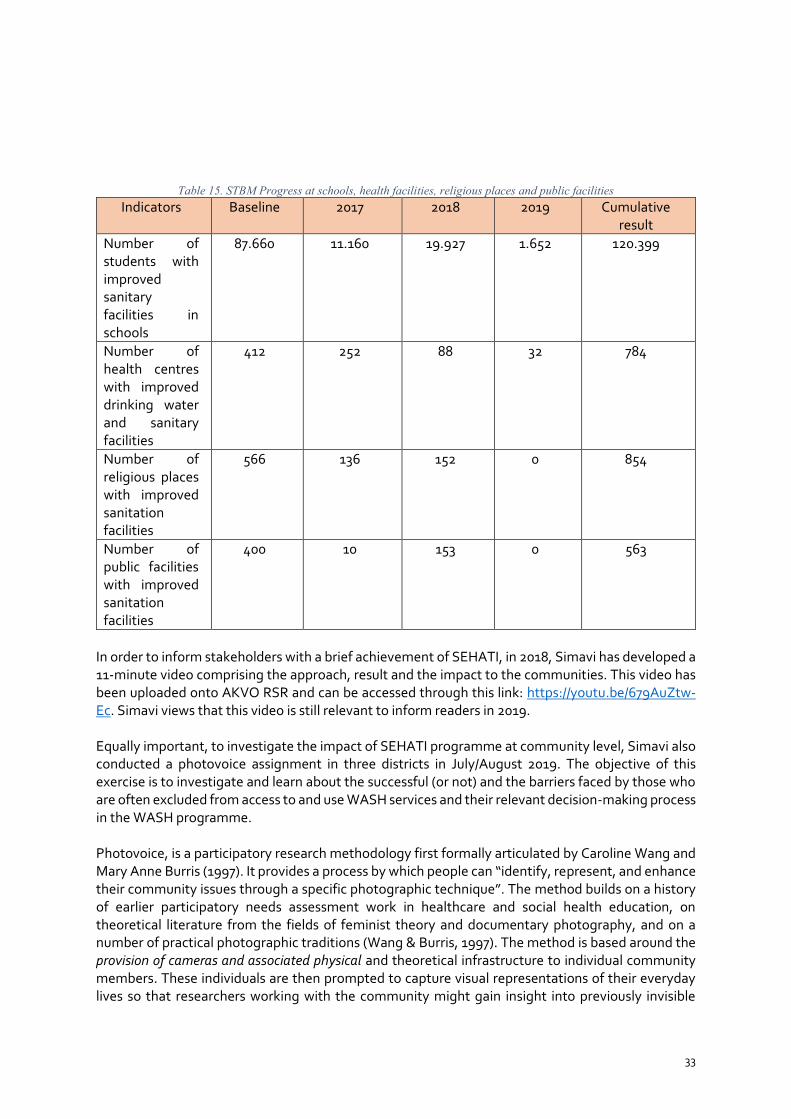
Table 15. STBM Progress at schools, health facilities, religious places and public facilities Indicators Baseline 2017 2018 2019 Cumulative
result Number of students with improved sanitary facilities in schools
87.660 11.160 19.927 1.652 120.399
Number of health centres with improved drinking water and sanitary facilities
412 252 88 32 784
Number of religious places with improved sanitation facilities
566 136 152 0 854
Number of public facilities with improved sanitation facilities
400 10 153 0 563
In order to inform stakeholders with a brief achievement of SEHATI, in 2018, Simavi has developed a 11-minute video comprising the approach, result and the impact to the communities. This video has been uploaded onto AKVO RSR and can be accessed through this link: https://youtu.be/679AuZtw-Ec. Simavi views that this video is still relevant to inform readers in 2019. Equally important, to investigate the impact of SEHATI programme at community level, Simavi also conducted a photovoice assignment in three districts in July/August 2019. The objective of this exercise is to investigate and learn about the successful (or not) and the barriers faced by those who are often excluded from access to and use WASH services and their relevant decision-making process in the WASH programme. Photovoice, is a participatory research methodology first formally articulated by Caroline Wang and Mary Anne Burris (1997). It provides a process by which people can “identify, represent, and enhance their community issues through a specific photographic technique”. The method builds on a history of earlier participatory needs assessment work in healthcare and social health education, on theoretical literature from the fields of feminist theory and documentary photography, and on a number of practical photographic traditions (Wang & Burris, 1997). The method is based around the provision of cameras and associated physical and theoretical infrastructure to individual community members. These individuals are then prompted to capture visual representations of their everyday lives so that researchers working with the community might gain insight into previously invisible
34
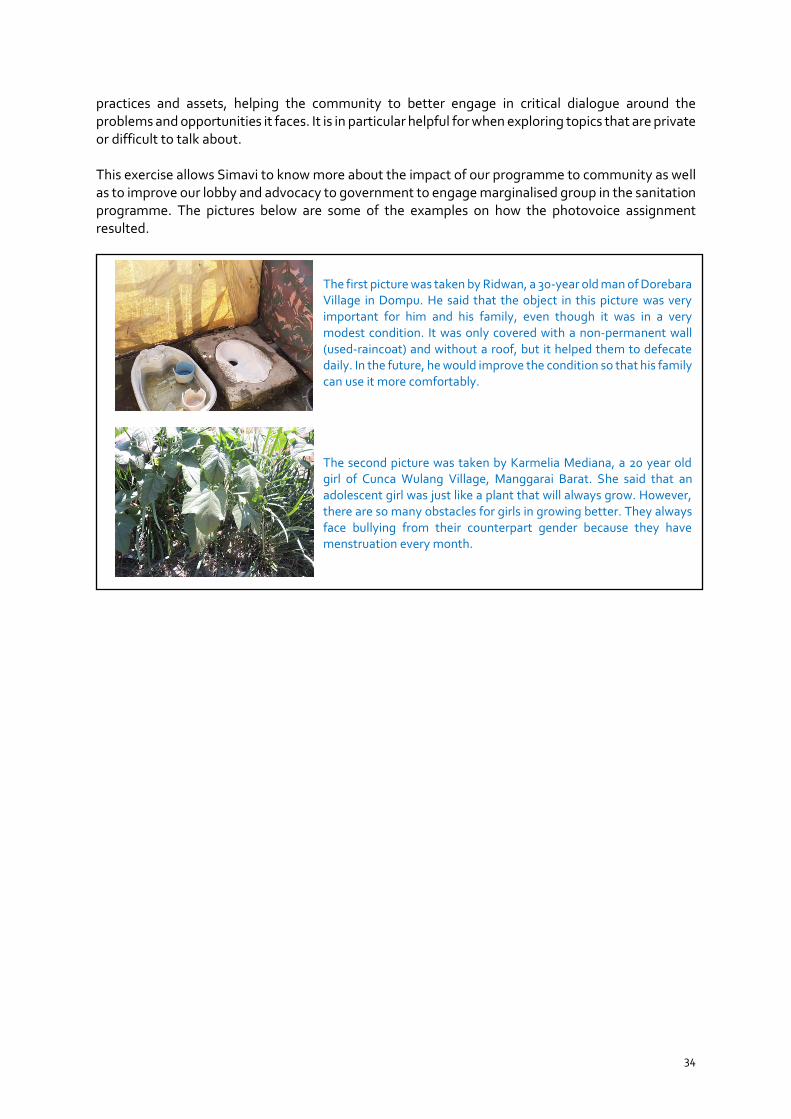
practices and assets, helping the community to better engage in critical dialogue around the problems and opportunities it faces. It is in particular helpful for when exploring topics that are private or difficult to talk about. This exercise allows Simavi to know more about the impact of our programme to community as well as to improve our lobby and advocacy to government to engage marginalised group in the sanitation programme. The pictures below are some of the examples on how the photovoice assignment resulted.
The first picture was taken by Ridwan, a 30-year old man of Dorebara Village in Dompu. He said that the object in this picture was very important for him and his family, even though it was in a very modest condition. It was only covered with a non-permanent wall (used-raincoat) and without a roof, but it helped them to defecate daily. In the future, he would improve the condition so that his family can use it more comfortably. The second picture was taken by Karmelia Mediana, a 20 year old girl of Cunca Wulang Village, Manggarai Barat. She said that an adolescent girl was just like a plant that will always grow. However, there are so many obstacles for girls in growing better. They always face bullying from their counterpart gender because they have menstruation every month.

35

36
Gender Equality and Social Inclusion (GESI) within the SEHATI Programme The integration of Gender Equality and Social Inclusion (GESI), including Menstrual Health, in this SEHATI programme has been done since the beginning of the implementation in 2016. SEHATI partners have been trained by Simavi for GESI for the STBM Programme in 2016. This training was conducted in order to facilitate the local governments in planning and implementing water and sanitation programmes which are responsive to Gender Equality and Social Inclusion. In the view of GESI, SEHATI partners also figured out the composition of their staff working for the SEHATI programme. The composition for Yayasan Dian Desa and Yayasan Plan International Indonesia in 2019 was 30 males and 23 females.
In early 2018, Simavi has produced a learning brief of Gender Equality and Social Inclusion in which we describe the integration of Gender Equality and Social Inclusion within the STBM approach. Containing SEHATI’s best practices in integrating Gender Equality and Social Inclusion in the programme, this learning brief has been circulated to national and local stakeholders. This knowledge has been uploaded onto AKVO RSR: https://rsr.akvo.org/en/project/5783/
At national level, Simavi works together with other organisations such as SNV, UNICEF, GIZ to advocate the Ministry of Health in including gender perspectives and social inclusion on the regulation of STBM. At the moment, the Ministry of Health is revising the STBM regulation to be more applicable at village level. Moreover, Simavi is also involved in Menstrual Hygiene Day since 2018 and collaborated with several local NGOs to raise awareness of adolescents in urban areas in 2019. In addition, during the National Water and Sanitation Conference in Jakarta in November 2019 (KSAN 2019), Simavi had the opportunity to discuss with UNICEF Global, University of Indonesia and also a local female entrepreneur of Lombok Timur about Women in the WASH Sector. This session talks about how to narrow the gender gap in the WASH sector, in particular the capacity of WASH practitioners. The discussion was in line with the SEHATI approach in which SEHATI tries to empower more women working in the WASH sector, not only in a promotion activity as cadres, but also participating in decision making and working towards supply chain as a female local entrepreneur, for instance. Additionally, Simavi also had opportunity to invite Head of Dompu District to exchange the knowledge on integrating GESI in sanitation sector together with Mayor of Surakarta and Bandar Bandar Lampung. In separate session, Simavi shared best practices of integrating MHM in 5 pillars of STBM in Dompu, facilitated by the champion of MHM.

37
Figure 9. Panel session on Women in WASH during KSAN 2019
Up to 2019, Simavi has capacitated 3.527 people, of which 2.351 are women, including local sanitation entrepreneurs in 7 districts within the SEHATI programme. At implementation level, Simavi wants to engage other marginalised groups in the community as well. Simavi believes that leaving no one behind is a must to ensure that everyone is able to fully participate in society and enjoy basic health regardless of their ethno-racial background, financial status, education level, physical or mental ability, religious and faith-based beliefs, gender, marital status, geographical location, sexual orientation, age and other socio-economic circumstances. Therefore, in November 2019, Simavi trained her local partners Yayasan Dian Desa and Yayasan Plan International Indonesia and government officials from Lombok Utara and Manggarai Barat on the topic of Leave No One Behind so that local governments can provide access to sanitation based on the needs of marginalised groups and include them in decision making processes. Simavi understands that SEHATI has integrated GESI since the beginning of the programme and this training will benefit partners and government with the concept of Leave No One Behind so they know how to implement it properly. In 2020, Simavi will monitor the implementation of this integration within SEHATI programme. Additionally, to ensure all women and girls get access to private and comfortable sanitation facilities, Simavi initiates to include Menstrual Health (MH) since late 2018. This activity is intended to increase the awareness of women needs, including women friendly toilets. In 2019 alone, Simavi has trained Yayasan Plan International Indonesia and local government on MH and how to integrate it with 5 pillars of STBM. In Lombok Utara, there are 6 villages in 2019 that integrated STBM programme and MH. While in Manggarai Barat, a MH training has been done in December 2018. Yayasan Dian Desa, in collaboration with AYO Indonesia (a local NGO based in Ruteng), implemented MH in 4 STBM declared villages between January and June 2019. After six months, Yayasan Dian Desa replicated the MH integration to 6 other villages, making a total of 10 intervened villages in Manggarai Barat. Equally important, in January 2020 SEHATI will start to collaborate with Yayasan Kopernik (a 501 registered organisation in the US based in Bali) which works on The Perfect Fit, a project to improve awareness on menstrual health (MH) and sexual reproductive health and rights (SRHR) to girls and women in Indonesia. Simavi and Kopernik will train local women to manufacture reusable menstrual

38
pads using locally-sourced materials and recruit menstrual health agents from local communities (e.g health workers, cadres, and teachers) to provide education on MH/SRHR issues, using the pad as an entry point. The collaboration between Kopernik and Simavi has started since was established in 2018 for an 18-month pilot project in Ruteng, Manggarai District, financed by Grand Challenges Canada (GCC). This pilot showed a 10% increase in MH knowledge and a 7.8% increase in health-seeking behaviours change related to Menstrual Health problem for girls and women involved in the project. Simavi aims for similar results in Labuan Bajo, Manggarai Barat. At the same time Simavi aims to increase private sector collaboration with this initiative to support outcome 3 of the SEHATI programme. The composition of the tailors will include gender-based violence survivals, woman with disabilities, and low-income housewives. The activities regarding this collaboration will be started in January 2020.
Simavi ensure that people with disabilities can also experience the access to improved sanitation by taking any measures. In Teniga village, Lombok Utara, a 14 year old boy, who stopped from his school due to his impairment (cannot walk at all), is now able to get access to his own toilet. The family worked together with cadres to construct handrails fitted in his bedroom all the way to the toilet. This eases him to do bathing and defecating.

39
Progress at National Level
SEHATI, through Simavi, has series of programme activities to support lobby and advocacy at the national level in Indonesia. In 2019, Simavi focused on providing enhancement support on 5 pillars of STBM related regulation and monitoring, strengthening the capacity of Pokja AMPL and Menstural Health (MH) as well as Gender Equality and Social Inclusion (GESI) campaigns within the WASH sector. Practically, Simavi coordinated and communicated with the central government, especially Bappenas and the Ministry of Health. Simavi was also involved in various meetings conducted by relevant government agencies when it was in line with SEHATI’s objectives.
In regards to the development of national web-based monitoring system of 5-pillars of STBM, Simavi supports the Ministry of Health, not only in developing the indicators but also providing a practical guideline for sanitarians. In mid 2019, Simavi invited representatives of the district health offices from 7 district to join a training in Surabaya and to test the system within their respective districts by collecting the data at household level. The data analysis of 5 pillars of STBM at national level was supposed to be disseminated by the end of 2019, yet, due to tight schedule of Ministry of Health, the dissemination has been postponed into 2020.
Figure 10. Household monitoring visit conducted by sanitarian in Sumba Barat Daya, August 2019, using national
monitoring indicators.
Equally important, MH and GESI perspective has been integrated into STBM implementation. The Ministry of Health and other NGOs are now working on providing women and/or people with disability friendly toilets. Additionally, starting 2019, the Ministry of Health has a special fund to support the poorest in constructing toilets. In May 2019 Simavi co-organised MH Day in Jakarta.
Simavi was also involved in the National Water and Sanitation Conference (KSAN) 2019. Simavi has shared some best practices and approaches in SEHATI programme to various government agencies and non- government stakeholders. This event was responded positively by participants through which SEHATI also gained inputs on our existing approach and strategies. During the meeting, Simavi shared best practices regarding integrating GESI in the sanitation sector. Head of Dompu district had session of knowledge exchange together with Mayor of Surakarta and Bandar Lampung. In addition, Simavi facilitated Women in WASH session to discuss about the increasing role of women in WASH sector and the challenge to empower more women in the sector. Also, in separate session, the implementation of MHM in 5 pillars of STBM was shared by SEHATI champion in Dompu, Ibu Ratu.

40
In 2019 Simavi actively participated at national level meetings in various topics, such as:
STBM - Supported the Ministry of Health on the set of regulation of implementation of the 5 Pillar STBM
- Review of the STBM Permenkes No.3 2014 - Improvement of the 5 Pillar STBM indicator which is adjusted to the SDG indicator - Review of STBM 5 Pillars implementation and triggering guidelines
- Assisted facilitating the 5 Pillar STBM training managed by the Ministry of Health together with SEHATI partners in Jakarta
- Participated in the evaluation of the 5 Pillar STBM implementation - Contributed in the 2019 STBM Award - Workshop the 5 Pillar STBM in Indonesia implementation - And trial the new format 5 Pillar STBM monitoring and evaluation system
Drinking Water and Environment Health - Joined and was involved in various AMPL network meetings to discuss water and sanitation
development in Indonesia - Coordinated with Bappenas through the National AMPL Working Group to strengthen AMPL
institutions at the provincial (NTB and NTT) and district levels where the SEHATI programme was running
- Contributed to the implementation of the 2019 KSAN activities
MH
- Increased MH knowledge capacity for adolescents - Participated in MHD Day series in April – May 2019 - MH knowledge books development - MH integration campaign in the 5 Pillar STBM activities in Manggarai Barat and Lombok
Utara

41
Challenges and Lesson Learned Challenges Simavi and her partners experienced several challenges over the programme implementation period. The challenges described in this chapter will cover those at the national and district levels. Challenges at the national level During 2019, Simavi and her partners did not find any new significant challenge apart from those which have been anticipated and identified in the proposal, such as the lack of supporting or conducive environment from national level (gap between STBM approach and implementation; unsupportive monitoring and evaluation system, tools and guidelines, etc.). As mentioned in the previous section, Simavi did several meetings and lobby activities to ensure that the Ministry of Health adapts 5 pillars of STBM indicators into their web-based monitoring system and guidelines. However, due to internal challenges within the Ministry of Health, this outcome is still a long way to go. The obstables are: - The STBM indicators are still debatable amongst national stakeholders especially in relation with
SDGs indicators - No functioning STBM secretariat at the moment - Uneven distribution of information regarding new indicators and guideline to lower levels
To cope with these obstacles, Simavi will keep supporting the Ministry of Health, together with other NGOs, in delivering the web-based monitoring system and national practical guidelines of the 5 pillars of STBM. Challenges at provincial level Even though Indonesia’s government implements a bottom – up scheme for planning and budgeting, capacity building and monitoring activities are conducted using a top – down approach. Provincial governments have the responsibility to ensure that STBM is executed at a lower level properly, after they were capacitated by the national government. However, Simavi and her partners found that there is a gap between national and district level which are overlooked at provincial level in particular in the capacity building and monitoring of STBM. Insufficient capacity building and monitoring activities from provincial governmenst leads to the lack of capacity at district level to implement STBM at community level. Therefore, since September 2019 (SEHATI extension) Simavi focussed as well on engaging the provincial governments of NTB and NTT in executing an exit strategy in the future period. Also, the engagement with provincial governments will encourage them to replicate the SEHATI approach to other districts in the region. Challenges at the district level Similar like the challenges at national level, most of the challenges in 2019 remained the same with those anticipated and identified during the project design stage of SEHATI in 2016. • In Lombok Utara, SEHATI found that a small percentage of families tend to construct their
houses as main priority and put the construction of toilet as a second priority. This makes the number of people practice open defecation and/or share toilets decrease slowly, even though the

42
government has allocated some funds for sanitation. In addition, some village governments are still inconsistent in utilising the Village Fund for sanitation programming.
• As mentioned in previous report, Simavi viewed that the geographical condition of Manggarai Barat and lack of clean water in certain villages hinder the implementation of the sanitation programme at household level. By using biannual monitoring data from SEHATI, Yayasan Dian Desa keeps advocating local governments to pay more attention to those challenges in their future planning, for instance providing more water supply programme in the fiscal year and capacitate local facilitator to reach remote villages.
• The village governments have low attention for inclusion sanitation for persons with disabilities, the poor, women and children. It needs to deliver a message in a local format towards Gender Equality and Social Inclusion.
Lessons Learned
Several lessons learned gained from 2019 are as follows:
1. Securing support from the provincial governments is really important. This is why SEHATI proposed to work with the provincial government in the extension period (NTT and NTB government provinces are expected to follow the progress up in all the districts they cover).
2. While the ToC of SEHATI in principle is still valid, the way SEHATI presents it at the beginning is not always easy to understand by readers or observers. Revising it after testing and learning from it together with stakeholders throughout the time is seen useful and even critical.
3. Even though SEHATI has contributed to the improvement of access to sanitation and hygiene facilities at district level as well as the capacity of local government to lead the implementation of STBM, some challenges remain to exist to achieve the Sustainable Development Goal (SDG) 6, especially when discussing about Safely Managed Sanitation. This issue was not the main focus of SEHATI when the programme was implemented in 2016. Therefore, introducing and incorporating it with an exit strategy before SEHATI ends is important. Simavi will conduct a study on Safely Managed Sanitation in 2020 to identify the current conditions in Lombok Utara and Manggarai Barat. This study intends to come up with some relevant recommendations for both district governments in order to support strategic planning on Safely Managed Sanitation in 2030.
4. Integrating a few other health issues into STBM programme is possible and could be more effective and efficient as STBM’s approach and concerns are overlapped with them. This can be seen from initiatives of SEHATI in integrating Menstrual Health (MH) in schools. MH touches upon 3 pillars of STBM. Based on this practice, there has been a thought about integrating MH at community level as this integration could result in positive outputs such as construction of MH-supportive toilets.

43
Financial Overview
A. EKN Contribution
Table 16 below shows financial overview of 2019 only, while the comprehensive overview from 2016 to 2019 is provided in Annex 3 A.
Table 16. Overview of the SEHATI expenditure in 2019
Activities
2019
Initial Budget (Jan – Aug 2019)
Total Approved Budget
(Jan – Aug 2019)
Expenditure (Jan – Dec 2019)
Variance (%)
Outcome 1
Strong leadership, commitment and improved capacities of the local government (district and sub-district level) to implement and sustain the 5-pillars STBM
9,394
77,340 64,377 83%
Outcome 2
Strengthened capacity of CSOs on lobbying and advocating local government to lead STBM implementation
-
4,880 5,366 110%
Outcome 3 Strong private sector for Improved supply of WASH products and services
- 8,264 6,838 83%
Outcome 4
A viable implementation model that ensures the local government is capable to roll out and sustain a district-wide STBM 5 pillar
36,337
31,958 45,396 142%
Outcome 5 Programme Management and Coordination
42,408 64,696 105,437 163%
Outcome 6 Communication / knowledge management / production of materials
2,771
37,858 12,604 33%
Outcome 7 Human Resources 159,241
212,142 221,662 104%
Outcome 8 Operational Costs 53,105
51,437 53,599 104%
Outcome 9 Admin Cost 7% 13,400
21,540 11,310 53%
Grand Total 316,656
510,115 526,588 103%
Grand Total with extension (1/3 of 450.000 euro)*
660,115 526,588 80%
Note: The above table consists of audited figures from all local partners (Simavi Local Office and 2 local partners) and non-audited figures from Simavi Head Office in Amsterdam. The audit report for Simavi Head Office will be submitted latest by 30 June 2020, therefore, the figures on above table might change based on the audit result. • In this initial budget overview the amount of the extension is not integrated yet. Taking
1/3 of 450.000 euro we can include 150.000 euro to the initial budget. The 1/3 is calculated based on 4 months (September – December 2019) out of 12 months (September 2019 – August 2020).

44
B. Partners and Local Government Contribution
Regarding partners and local government contribution, they are elaborated on financial statement that is submitted along with this narrative report. Partner expenses are also included in the financial report but local governments are not. SEHATI did have figures of local governments’ expenditure based on unaudited information and document, and they are all recorded in SEHATI monitoring capacity tools which has been elaborated under section 1 (general progress) of this report. Yet, those figures are not presented in the financial statement because they are not auditable by SEHATI auditor. SEHATI tried to get state audited figures but failed to do so due to restricted access to government expenditure documents. This difficulty of access has happened since 2017, 2018 and therefore it has not been recorded in financial statements of 2019.

45
Future Activities To address some of the challenges that exist in the implementation of the SEHATI Programme, the following activities will be done between January and June 2020:
· In Lombok Utara and Manggarai Barat districts, SEHATI will continue to strengthen the capacity, skills and knowledge of the STBM team members by conducting activities agreed in the work plan, including making sense that replication villages will have the same quality with the intervened ones.
· Conduct a study on Safely Managed Sanitation to provide a diagnostic analysis and recommendation for local and national government to achieve the target of SDG 6.
· At the national level, SEHATI will continue to provide support to the Ministry of Health collaboration with national stakeholders on review the Permenkes no.3 2014 about STBM and encourage the finalisation of the 5 Pillar STBM monitoring evaluation system that adjusted to the SDG indicators complete with field technical guidance.
· Simavi will coordinate with the Government of Indonesia, especially with Bappenas and the Ministry of Health to strengthen the institutional capacity of the Provincial (NTB and NTT) and District AMPL Working Groups where the SEHATI programme is implementing.
· A production hub for reusable pads will be set up by Kopernik in Labuan Bajo, Manggarai Barat in order to support private sector collaboration, increase Menstrual Health, empower women economically, and to decrease solid waste (pillar 4 of STBM).
· In Lombok Utara Yayasan Plan International Indonesia will collaborate with Nazava and Komida for access to alternative micro-finance in relation to safe drinking water (pillar 3 of STBM).

46

Annex 1 SEHATI Monitoring Framework and Tools
To measure outcomes and outputs of SEHATI, a number of indicators have been set up for district, sub-district, village, sanitation-entrepreneurs and partners levels. Since outcomes and outputs also involve qualitative data, the data needed to be quantified and which was done by using scorecards. Scoring or rating was done by using a continuum (no-limited-good-completed) to show different levels of progress.
A typical score card can be seen in below table.
Levels or scores for capacity outcomes
COMPLETE GOOD LIMITED NO
Fully present Strong In between None / Absent
All conditions or criteria are met
Almost all the conditions or criteria are met
Some of the conditions or criteria are met
None of the conditions or criteria are met
Indicators of outcomes
The following tables contain indicators for capacity outcomes that need to be measured at different levels in each district and how to measure them.
Scoring is made by selecting the appropriate box under SCORE column. Once it is selected the percentage will automatically appear (COMPLETE: 100%; GOOD: 66%; LIMITED: 33%; and NO: 0%)
A. District level (POKJA AMPL)
CATATAN:�INFORMASI�TENTANG�KABUPATEN�HARUS�DIPEROLEH�PADA�WAKTU�PERTEMUAN�DENGAN�POKJA�AMPL.�
KODE OC FIETS INDICATORS COMPLETE GOOD LIMITED NO IN�%
#1_KAB01 1 F
>> >> >> >> >>
>> >> >> >> >>
>> >> >> >> >>
#1_KAB05 1 I
#1_KAB06 1 I
#1_KAB07 1 I
#1_KAB08 1 I
#_1KAB09 1 I
#1_KAB10 1 I
Overall�score�>>�
SCOREOUTCOME�INDICATORS
Clear�division�of�roles�and�responsibilities�to�implement�STBM�
STBM�supportive�legislation�in�the�form�of�Bupati�instruction�or�Perda�is�in�place
District�STBM�team�is�formed�under�district�authority�and�functioning�
A�monitoring�system�is�in�place�that�measures�progress�on�STBM�at�village,�sub-district�and�district�level�
Adequate�funds�are�released�to�support�SEHATI�programme�activities
Actual�amount�released�this�year�to�support�SEHATI�programme�activities
Actual�amount�released�this�year�to�replicate�or�scale�up�STBM�in�non-SEHATI�target�areas
F
#1_KAB04 1 F
#1_KAB02 1 F
#1_KAB03 1
Information�from��regular�monitoring�is�shared,�analysed�and�discussed�with�relevant�district�level�stakeholders
Regular�coordination�meetings�organised�with�all�relevant�district�level�stakeholders
Adequate�funds�are�made�available�to�replicate�or�scale�up�STBM�in�non-SEHATI�target�areas
STBM�is�included�in�RPJMD
STBM�is�included�in�annual�plans�and�budgets
Adequate�funds�are�released�to�support�SEHATI�programme�activities

48
B. District Health Office level
C. Sub-district level
CATATAN:�INFORMASI�TENTANG�KABUPATEN�HARUS�DIPEROLEH�PADA�WAKTU�PERTEMUAN�DENGAN�KEPALA�DINAS�KESEHATAN�/�TIM�STBM�KABUPATEN
KODE OC FIETS INDICATORS COMPLETED GOOD LIMITED NO IN�%
#1_DIN01 1 F
>> >> >> >> >>
#1_DIN03 1 I
#1_DIN04 1 I
#1_DIN05 1 I
#1_DIN06 1 I
#1_DIN07 1 I
#1_DIN08 1 I
#1_DIN09 1 I
#1_DIN10 1 I
#1_DIN11 1 I
Overall�Score
OUTCOME�INDICATORS
A�detailed�work�plan�is�in�place�to�implement�STBM�in�the�district
Adequate�financial�resources�are�available�to�implement�the�plans
SCORE
#1_DIN02 1 F
Actual�funds�released�to�implement�the�plan�
Capacity�exists�to�provide�training�to�sub-district�STBM�teams�in�proven�demand�creation�methodologies
Capacity�exists�to�provide�training�to�sub-district�STBM�teams�in�proven�hygiene�promotion�methodologies
Capacity�exists�to�provide�training�to�sub-district�STBM�teams�in�STBM�monitoring
Capacity�to�provide�follow-up�to�the�sub-district�STBM�teams�after�training�in�the�form�of�guidance,�coaching,�motivation�and/or�support�during�implementation�
Capacity�exists�to�analyse�monitoring�data�submitted�by�Kecamatan�STBM�teams
Regularly�assesses�the�performance�of�sub-district�STBM�teams�responsible�for�demand�creation�and�follow-up
Regularly�organises�coordination�meetings�with�sub-district�STBM�teams�to�discuss�progress�and�challenges
The�information�from�monitoring,�experiences�and�lessons�learned�are�used�to�adjust�or�improve�implementation�plans�when�relevant
Capacity�to�verify�and�validate�village�level�and�Kecamatan�level�STBM�verification�and�declaration
CATATAN:�INFORMASI�TENTANG�KECAMATAN�HARUS�DIPEROLEH�PADA�WAKTU�PERTEMUAN�DENGAN�TIM�STBM�KECAMATAN
KODE OC FIETS INDICATORS COMPLETED GOOD LIMITED NO IN�%
#1_KEC01 1 F
>> >> >> >> >>
#1_KEC03 1 I
#1_KEC04 1 I
#1_KEC05 1 I
#1_KEC06 1 I
#1_KEC07 1 I
#1_KEC08 1 I
#1_KEC09 1 I
#1_KEC10 1 I
#1_KEC11 1 I
#1_KEC12 1 I
Overall�Score
The�information�from�monitoring,�experiences�and�lessons�learned�are�used�to�adjust�or�improve�implementation�plans�when�relevant
Capacity�to�organise�and�conduct�village�level�STBM�verification�and�declaration
Capacity�exists�to�provide�training�to�village�STBM�teams�in�proven�hygiene�promotion�methodologies
Capacity�exists�to�provide�training�to�village�STBM�teams�in�STBM�monitoring
Capacity�exists�to�provide�follow-up�to�the�village�STBM�teams�after�training�in�the�form�of�guidance,�coaching,�motivation�and/or�support�during�implementation�
Capacity�exists�to�analyse�monitoring�data�submitted�by�village�STBM�teams
Regularly�assesses�the�performance�of�village�STBM�teams�responsible�for�demand�creation�and�follow-up
Regularly�organises�coordination�meetings�with�village�STBM�teams�or�village�authorities�to�discuss�progress�and�challenges
SCORE
#1_KEC02 1 F
Actual�fund�realised�to�implement�the�plans�
Capacity�exists�to�provide�training�to�village�STBM�teams�in�proven�demand�creation�methodologies
INDICATORS�OUTCOME
A�detailed�work�plan�is�in�place�to�implement�STBM�in�the�sub-district
Adequate�financial�resources�are�available�to�implement�the�plans
STBM�team�at�sub-district�level�is�formed�under�district�authorities�and�functioning
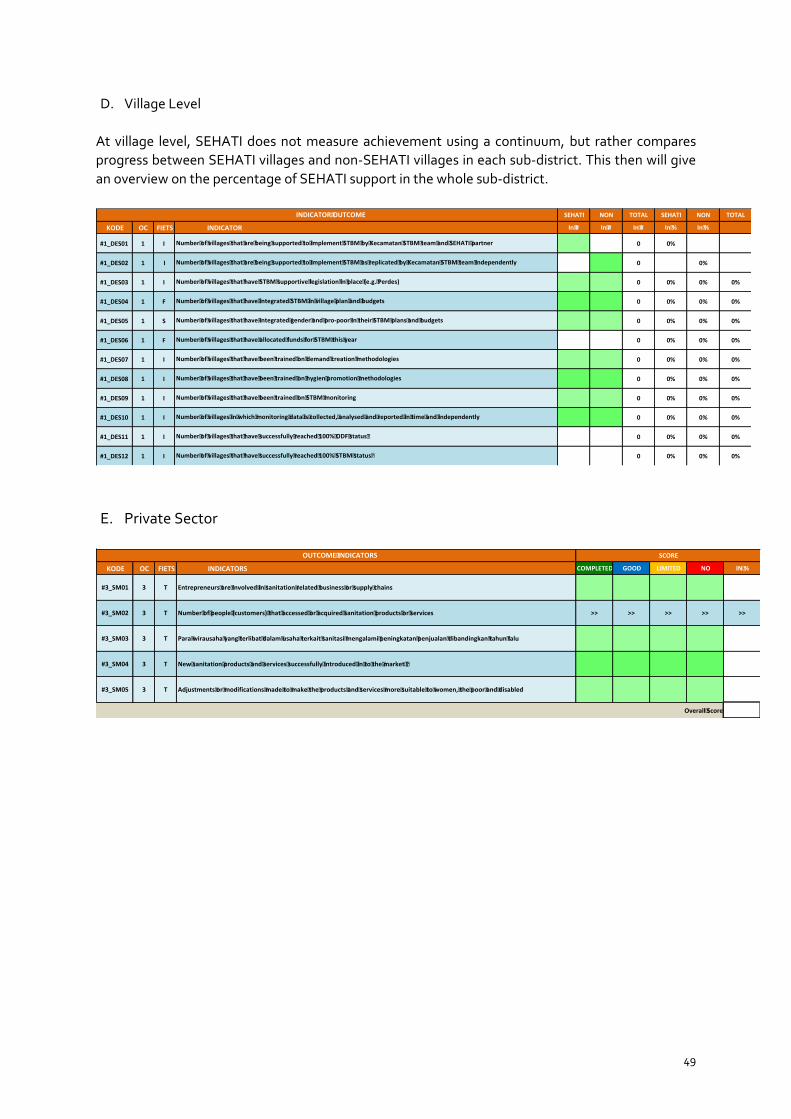
49
D. Village Level
At village level, SEHATI does not measure achievement using a continuum, but rather compares progress between SEHATI villages and non-SEHATI villages in each sub-district. This then will give an overview on the percentage of SEHATI support in the whole sub-district.
E. Private Sector
CATATAN:�INFORMASI�TENTANG�DESA�HARUS�DIDAPAT�PADA�WAKTU�PERTEMUAN�DENGAN�TIM�STBM�KECAMATAN
SEHATI NON TOTAL SEHATI NON TOTAL
KODE OC FIETS INDICATOR In�# In�# In�# In�% In�%
#1_DES01 1 I 0 0%
#1_DES02 1 I 0 0%
#1_DES03 1 I 0 0% 0% 0%
#1_DES04 1 F 0 0% 0% 0%
#1_DES05 1 S 0 0% 0% 0%
#1_DES06 1 F 0 0% 0% 0%
#1_DES07 1 I 0 0% 0% 0%
#1_DES08 1 I 0 0% 0% 0%
#1_DES09 1 I 0 0% 0% 0%
#1_DES10 1 I 0 0% 0% 0%
#1_DES11 1 I 0 0% 0% 0%
#1_DES12 1 I 0 0% 0% 0%
INDICATOR�OUTCOME
Number�of�villages�that�have�been�trained�on�demand�creation�methodologies
Number�of�villages�that�have�been�trained�on�hygien�promotion�methodologies
Number�of�villages�that�have�been�trained�on�STBM�monitoring
Number�of�villages�in�which�monitoring�data�is�collected,�analysed�and�reported�in�time�and�independently
Number�of�villages�that�have�integrated�STBM�in�village�plan�and�budgets
Number�of�villages�that�have�integrated�gender�and�pro-poor�in�their�STBM�plans�and�budgets
Number�of�villages�that�have�allocated�funds�for�STBM�this�year
Number�of�villages�that�are�being�supported�to�implement�STBM�by�Kecamatan�STBM�team�and�SEHATI�partner
Number�of�villages�that�are�being�supported�to�implement�STBM�as�replicated�by�Kecamatan�STBM�team�independently
Number�of�villages�that�have�STBM�supportive�legislation�in�place�(e.g.�Perdes)
Number�of�villages�that�have�successfully�reached�100%�STBM�status�
Number�of�villages�that�have�successfully�reached�100%�ODF�status�
CATATAN�:�INFORMASI�TENTANG�KINERJA�PENGUSAHA�SANITASI�DIDAPAT�SELAMA�INTERVENSI�PROGRAM
KODE OC FIETS INDICATORS COMPLETED GOOD LIMITED NO IN�%
#3_SM01 3 T
#3_SM02 3 T >> >> >> >> >>
#3_SM03 3 T
#3_SM04 3 T
#3_SM05 3 T
Overall�Score
Para�wirausaha�yang�terlibat�dalam�usaha�terkait�sanitasi�mengalami�peningkatan�penjualan�dibandingkan�tahun�lalu
New�sanitation�products�and�services�successfully�introduced�in�to�the�market��
Adjustments�or�modifications�made�to�make�the�products�and�services�more�suitable�to�women,�the�poor�and�disabled
OUTCOME�INDICATORS
Entrepreneurs�are�involved�in�sanitation�related�business�or�supply�chains
Number�of�people�(customers)�that�accessed�or�acquired�sanitation�products�or�services
SCORE

50
F. Partner Performance
CATATAN�:�INFORMASI�MENGENAI�MITRA�HARUS�DIPEROLEH�PADA�WAKTU�PERTEMUAN�DENGAN�MANAJER�PROGRAM�SEHATI
CODE OC FIETS INDICATORS COMPLETED GOOD LIMITED NO IN�%
#DIV/0!
#2_PAR01 2
#2_PAR02 2
#2_PAR03 2
#2_PAR04
#2_PAR05
#2_PAR06
#DIV/0!
#2_PAR07
#2_PAR08
#2_PAR09
#2_PAR10
Overall�score�>>� #DIV/0!
OUTCOME�INDICATORS SCORE
Programmatic�Issue
Partners�have�an�advocacy�strategy�suitable�for�their�location�/�local�context
Partners�have�MOUs�or�commitment�letters�signed�with�districts�and�sub-districts�for�the�local�authorities�to�take�the�lead�and�full�responsibilities�for�STBM
Partners�have�transfered�their�knowledge�and�skills�to�other�CSOs
Capacity�to�build�capacity�of�local�actors
Actual�achievements�in�capacity�building�and�realisation�of�exit�strategy�conditions
Actual�achievements�in�realising�annual�targets
Programme�management�issue
Quality�and�timeliness�of�planning�and�reporting�
Quality�and�timeliness�of�financial�reporting�and�budget�realisation
Quality�and�timeliness�of�monitoring�data
Partners�implement�programme�efficiently�and�effectively�(results�versus�costs)
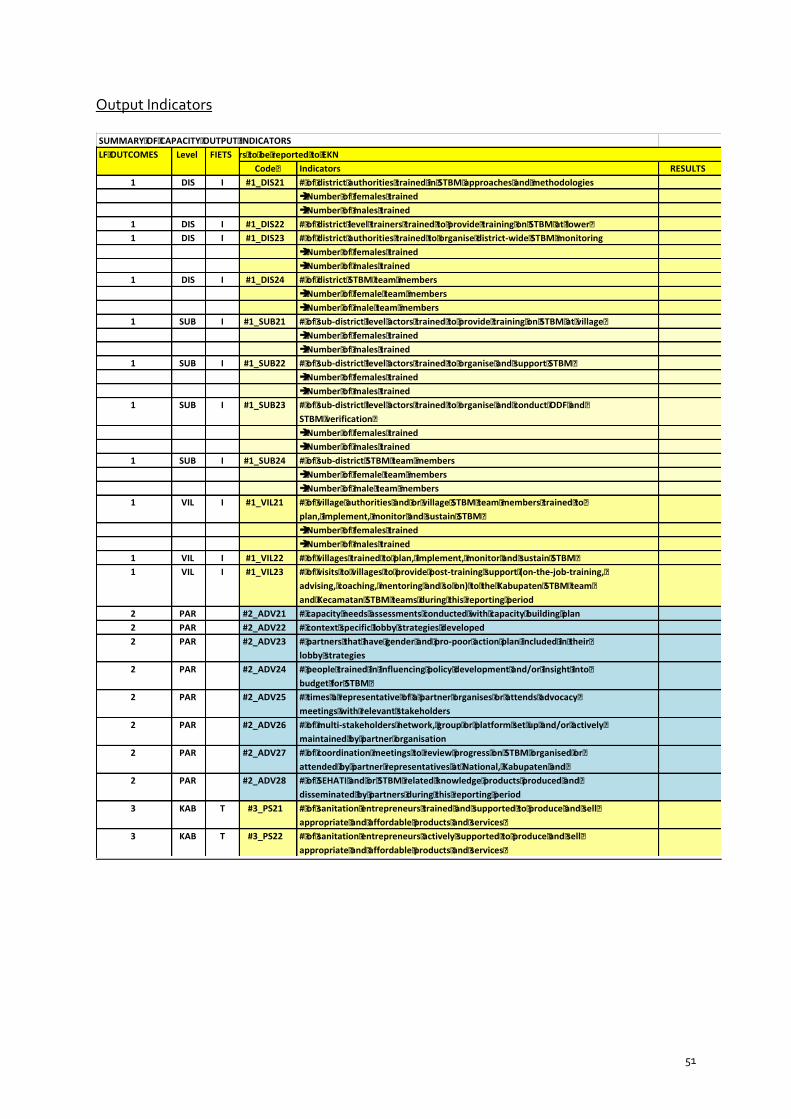
51
Output Indicators
SUMMARY�OF�CAPACITY�OUTPUT�INDICATORSLF�OUTCOMES Level FIETSOUTPUT�indicators�to�be�reported�to�EKN
Code� Indicators RESULTS1 DIS I #1_DIS21 #�of�district�authorities�trained�in�STBM�approaches�and�methodologies
è�Number�of�females�trainedè�Number�of�males�trained
1 DIS I #1_DIS22 #�of�district�level�trainers�trained�to�provide�training�on�STBM�at�lower�1 DIS I #1_DIS23 #�of�district�authorities�trained�to�organise�district-wide�STBM�monitoring
è�Number�of�females�trainedè�Number�of�males�trained
1 DIS I #1_DIS24 #�of�district�STBM�team�membersè�Number�of�female�team�membersè�Number�of�male�team�members
1 SUB I #1_SUB21 #�of�sub-district�level�actors�trained�to�provide�training�on�STBM�at�village�è�Number�of�females�trainedè�Number�of�males�trained
1 SUB I #1_SUB22 #�of�sub-district�level�actors�trained�to�organise�and�support�STBM�è�Number�of�females�trainedè�Number�of�males�trained
1 SUB I #1_SUB23 #�of�sub-district�level�actors�trained�to�organise�and�conduct�ODF�and�STBM�verification�è�Number�of�females�trainedè�Number�of�males�trained
1 SUB I #1_SUB24 #�of�sub-district�STBM�team�membersè�Number�of�female�team�membersè�Number�of�male�team�members
1 VIL I #1_VIL21 #�of�village�authorities�and�or�village�STBM�team�members�trained�to�plan,�implement,�monitor�and�sustain�STBM�è�Number�of�females�trainedè�Number�of�males�trained
1 VIL I #1_VIL22 #�of�villages�trained�to�plan,�implement,�monitor�and�sustain�STBM�1 VIL I #1_VIL23 #�of�visits�to�villages�to�provide�post-training�support�(on-the-job-training,�
advising,�coaching,�mentoring�and�so�on)�to�the�Kabupaten�STBM�team�and�Kecamatan�STBM�teams�during�this�reporting�period
2 PAR #2_ADV21 #�capacity�needs�assessments�conducted�with�capacity�building�plan2 PAR #2_ADV22 #�context�specific�lobby�strategies�developed2 PAR #2_ADV23 #�partners�that�have�gender�and�pro-poor�action�plan�included�in�their�
lobby�strategies2 PAR #2_ADV24 #�people�trained�in�influencing�policy�development�and/or�insight�into�
budget�for�STBM�2 PAR #2_ADV25 #�times�a�representative�of�a�partner�organises�or�attends�advocacy�
meetings�with�relevant�stakeholders2 PAR #2_ADV26 #�of�multi-stakeholders�network,�group�or�platform�set�up�and/or�actively�
maintained�by�partner�organisation2 PAR #2_ADV27 #�of�coordination�meetings�to�review�progress�on�STBM�organised�or�
attended�by�partner�representatives�at�National,�Kabupaten�and�2 PAR #2_ADV28 #�of�SEHATI�and�or�STBM�related�knowledge�products�produced�and�
disseminated�by�partners�during�this�reporting�period3 KAB T #3_PS21 #�of�sanitation�entrepreneurs�trained�and�supported�to�produce�and�sell�
appropriate�and�affordable�products�and�services�3 KAB T #3_PS22 #�of�sanitation�entrepreneurs�actively�supported�to�produce�and�sell�
appropriate�and�affordable�products�and�services�

Annex 2. EK
N Fram
ework – W
ATER
Impact
Water security and w
ater safety for people and ecosystems
Outcom
es W
ater, Sanitation and Hygiene
Indicators P
eople use safe drinking water and adequate sanitary facilities
a.
Num
ber of people using safely managed drinking w
ater services (SDG
6.1.1) SEH
ATI has not included drinking w
ater services in the intervention.
b. N
umber of people using safely m
anaged sanitation services, including a hand washing facility w
ith soap and water
Baseline (2016)
Cumulative 2017
Cumulative 2018
Cumulative 2019
148.300 people 294.976 people
327.046 people 331.879 people
Target: NA
A
dditional Information:
Simavi has not provided baselines/targets for safely m
anaged sanitation as SEHA
TI is the continuation of the previous SHA
W
programm
e in which that indicator w
as not in use. The JMP level basic sanitation is presented instead.
JMP Ladders
Baseline (2016)
Cumulative 2017
Cumulative 2018
Cumulative 2019
OD
95.192
77.465 72.386
61.556 U
nimproved
113.441 122.302
128.014 71.745
Basic
178.980 315.665
332.163 388.908
Target : NA
c. N
umber of people living in O
pen Defecation Free com
munities
Baseline (2016)
Intervention (2016) 2017
2018 2019
30.214 people
(15.500 females)
220 people
(115 fem
ales) 35,512
people (17,554 fem
ales) 127,749 people (65,559 fem
ales) 13.145
people (7.314 fem
ales) Cum
ulative result : 206.840 people (106.042 females)
Target : NA

53
d. N
umber of village declared O
pen Defecation Free / 5 pillars of STB
M
B
aseline (2016) 2017
2018 2019
18 villages 18 villages
51 villages 20 villages
Cumulative: 107 villages
Target: 131
Total number of people w
ho benefitted from the SEH
ATI program
me : 511.631 people.
Institutions Finances
Facilities O
utputs Institutions
are able
to carry
out their
functions with respect to drinking w
ater and sanitation
Local financing
mechanism
s for
drinking w
ater and
sanitation developed
WA
SH facilities are functional for at
least 15 years
a.
Num
ber of
WA
SH
organisations strengthened B
aseline : 0 Progress 2016: 222 organisations Progress 2017: 42 organisations Progress 2018 : 18 organisations Progress 2019 : 0 Cum
ulative result:
282 organisations;
consists of
277 governm
ent ad
hoc organisations
(POK
JA
AM
PL and
/ or
districts, sub-districts and village STBM
teams) and 5 sanitation entrepreneurship
forums.
Target: NA
a. N
umber
of dom
estic financing
mechanism
B
aseline : NA
Progress 2016 : 4 Progress 2017 : 4 Progress 2018 : 4 Progress 2019: 0 Cum
ulative result: 12 Target : N
A
a. N
umber
of clim
ate resilient
sanitary facilities constructed B
aseline 2016 : NA
Progress 2017 : 21.213 Progress 2018 : 13.794 Progress 2019: 4.059 Cum
ulative result : 39.066 Target : N
A
b.
Num
ber of
people trained
in W
ASH
institutions B
aseline : 0 Progress by 2016 : 2.721 people Progress by 2017 : 279 people
b. Total am
ount of funds leveraged third parties (regional budget at governm
ent level, B
OK
, village fund, and comm
unity contribution)
b. N
umber of students/pupils w
ith im
proved sanitary
facilities in
schools B
aseline 2016: 87.660 Progress 2017: 11.160

54
Progress by 2018 : 280 people Progress by 2019: 247 people Cum
ulative result : 3.527 people Target : N
A
c.
Does this project use the D
GIS – IG
G
sustainability tools
(clause, check,
compact)?
No.
Baseline : -
Progress 2016 : € 795.552 Progress by 2017 : € 3.697.177 Progress by 2018: € 5.564.546 Progress by 2019: € 2.072.597 Cum
ulative result : € 12.174.528 Those budget are consists of regional budgets
(ABPD
at
district level),
village fund at village level, BO
K at
sub-district level that intended for physical
construction and
non-physical im
plementation.
Target : NA
c. N
umber of people w
ith access to m
icrofinance for WA
SH (B
umD
es) B
aseline 2016: 0 Progress 2017 : 85 people Progress 2018 : 0 Progress 2019: 0 Cum
ulative result : 85 people Target : N
A
Progress 2018 : 19.927 Progress 2019: 1652 Cum
ulative result : 120.399 Target: N
A
c.
Num
ber of
health centres
with
improved
drinking w
ater and
sanitary facilities B
aseline 2016 : 412 Progress 2017 : 252 Progress 2018 : 88 Progress 2019: 32 Cum
ulative result : 784 Target : N
A
d. N
umber
of religius
places w
ith im
proved sanitation facilities B
aseline 2016 : 566 Progress 2017 : 136 Progress 2018 : 152 Progress 2019: 0 Cum
ulative result : 854 Target : N
A
e. N
umber of public facilities w
ith im
proved sanitation facilities B
aseline 2016 : 400 Progress 2017 : 10 Progress 2018 : 153 Progress 2019: 0 Cum
ulative result : 563 Target : N
A
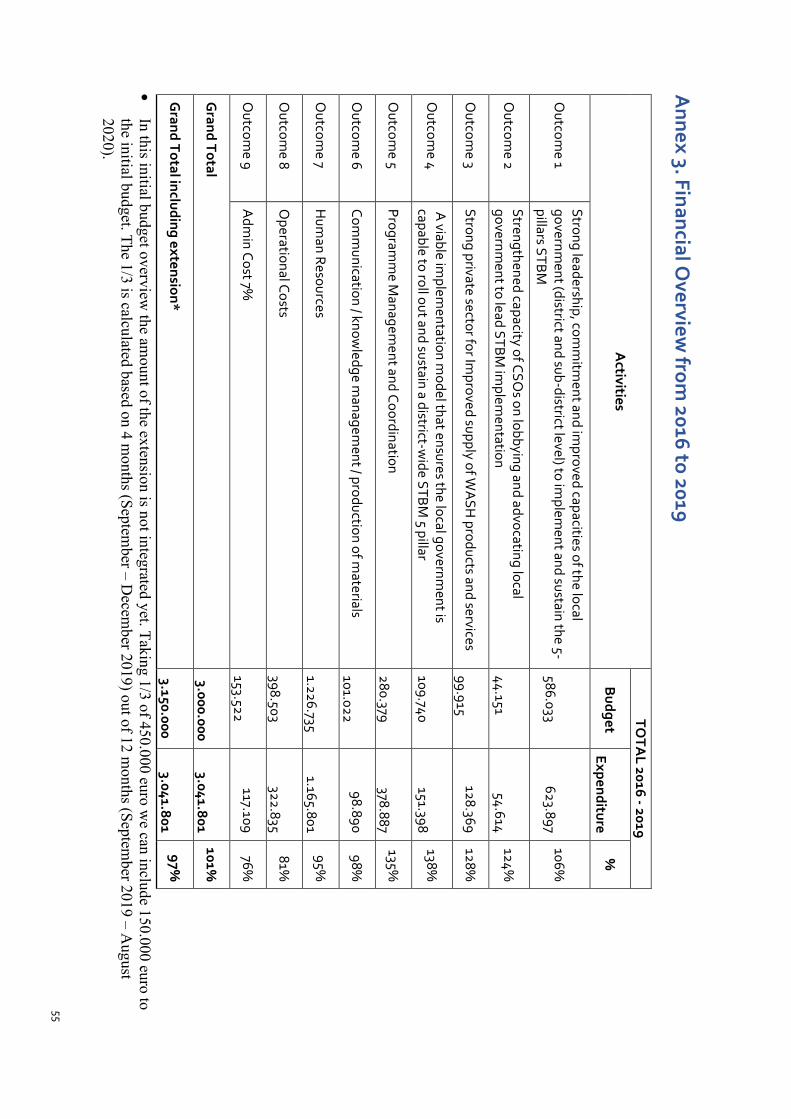
55
Annex 3. Financial O
verview from
2016 to 2019
Activities
TOTA
L 2016 - 2019
Budget
Expenditure %
Outcom
e 1 Strong leadership, com
mitm
ent and improved capacities of the local
government (district and sub-district level) to im
plement and sustain the 5-
pillars STBM
586.033
623.897
106%
Outcom
e 2 Strengthened capacity of CSO
s on lobbying and advocating local governm
ent to lead STBM im
plementation
44.151
54.614
124%
Outcom
e 3 Strong private sector for Im
proved supply of WA
SH products and services
99.915
128.369 128%
Outcom
e 4 A
viable implem
entation model that ensures the local governm
ent is capable to roll out and sustain a district-w
ide STBM
5 pillar 109.740
151.398
138%
Outcom
e 5 Program
me M
anagement and Coordination
280.379
378.887
135%
Outcom
e 6 Com
munication / know
ledge managem
ent / production of materials
101.022
98.890 98%
Outcom
e 7 H
uman Resources
1.226.735
1.165.801 95%
Outcom
e 8 O
perational Costs 398.503
322.835
81%
Outcom
e 9 A
dmin Cost 7%
153.522
117.109 76%
Grand Total
3.000.000
3.041.801
101%
Grand Total including extension*
3.150.000
3.041.801
97%
• In this initial budget overview
the amount of the extension is not integrated yet. Taking 1/3 of 450.000 euro w
e can include 150.000 euro to the initial budget. The 1/3 is calculated based on 4 m
onths (September – D
ecember 2019) out of 12 m
onths (September 2019 – A
ugust 2020).

56