Embed Size (px)
Citation preview

2019Course #3
Self-StudyCourse
Contact Us:Phone
614-292-6737
Toll Free1-888-476-7678
Fax614-292-8752
Webdentistry.osu.edu/sms
The Ohio State UniversityCollege of Dentistry305 W. 12th AvenueColumbus, OH 43210
The Ohio State University College of Dentistry is a recognized provider for ADA CERP credit. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to the Commission for Continuing Education Provider Recognition at www.ada.org/cerp.
The Ohio State University College of Dentistry is approved by the Ohio State Dental Board as a permanent sponsor of continuing dental education.This continuing education activity has been planned and implemented in accordance with the standards of the ADA Continuing Education Recognition Program (ADA CERP) through joint efforts between The Ohio State University College of Dentistry Office of Continuing Dental Education and the Sterilization Monitoring Service (SMS).
Course Instructions:
Read and review the course materials.
Complete the 16 question test. A total of 12 questions must be answered correctly for credit.
Submit your answers online at:
http://dentistry.osu.edu/sms-continuing-education
Check your email for your CE certification of completion (please check your junk/spam folder as well).
About SMS CE courses: TWO CREDIT HOURS are issued
for successful completion of this self-study course for the OSDB 2019-2021 biennium totals.
CERTIFICATE of COMPLETIONis used to document your CE credit and is emailed to each course participant.
ALLOW 2 WEEKS for processing of your certificate.
Frequently Asked Questions:
Q: Who can earn FREE CE credits?
A: EVERYONE - All dental professionals in your office may earn free CE credits. Each person must read the course materials and submit an online answer form independently.
Q: Where can I find my SMS number?
A: Your SMS number can be found in the upper right hand corner of your monthly reports, or, imprinted on the back of your test envelopes. The SMS number is the account number for your office only, and is the same for everyone in the office.
Q: How often are these courses available?
A: Four times per year (8 CE credits).

2019 Course
#3
Written by:Christina Zachariadou,
DDS, MS
Edited by:John Kalmar, DMD, PhD
Chris Harrington, DDS, MSSydney Fisher, MPH
Release Date:August 19, 2019
8:30am EST
Last Day to Take Course Free of Charge:
September 19, 20194:30pm EST
Medication-Related Osteonecrosis of the JawThis is an OSDB Category B: Supervised self-instruction course
2
About the AuthorChristina Zachariadou, DDS, MS
Dr. Zachariadou can be reached at [email protected] I nor my immediate family have any financial interests that would create a conflict of interest or restrict my judgement with regard to the content of this course.
Dr. Zachariadou completed her dental education at the Aristotle University of Thessaloniki, Greece where she earned a Doctor of Dental Surgery (DDS) equivalent degree. She worked as a general dentist in Greece from 2014-2015. She completed her residency and Master’s degree in Periodontology at the Ohio State University, USA (2015-2018). She is a diplomate of the American Board of Periodontology. Currently, she is pursuing a PhD degree in Oral Biology at the Ohio State University.
BackgroundIn 2003, Marx first reported an unusual occurrence of
exposed necrotic bone in the jaws.1 Thirty-six patients presented with painful and exposed bone in the mandible, maxilla or both, that would not heal and were recalcitrant to treatment. Although these patients were receiving multiple medications, they all had in common the use of nitrogen – containing bisphosphonates (pamidronate or zoledronate). These antiresorptive drugs were being delivered intravenously for the treatment of cancer-related adverse effects or osteoporosis. As Marx noted, bisphosphonates seem to be the etiologic factor for the necrosis and exposure of jaw bone, a condition that came to be known as “Bisphosphonate - related osteonecrosis of the jaw (BRONJ)”. 1
Since this initial report, the literature has grown to include case reports, retrospective and prospective studies, as well as reviews, systematic reviews and meta-analyses. As the awareness increases, additional drugs have been added to the list of medications that could cause osteonecrosis of the jaw (ONJ). Including denosumab, another antiresorptive drug, and antiangiogenic medications have been added to the list.2-8

Since ONJ can manifest in patients receiving, not only bisphosphonates, but other antiresorptive and antiangiogenic drugs as well, the American Association of Oral and Maxillofacial Surgeons (AAOMS) has recommended the more general and inclusive term “Medication-related osteonecrosis of the jaw (MRONJ).”9 In their 2014 update, MRONJ was defined as “(1) exposed bone or bone that can be probed through an intraoral or extraoralfistula in the maxillofacial region that has persisted for longer than 8 weeks, (2) in a patient with current or previous treatment with antiresorptive or antiangiogenic agents, and (3) no history of radiation therapy to the jaws or obvious metastatic disease to the jaws.” All three conditions are needed to establish a diagnosis of MRONJ.9
Implicated MedicationsBefore providing information on the mechanism of action behind medications
associated with MRONJ, a summary of the bone remodeling cycle is provided for better comprehension of their bone modulatory actions.
Bone remodeling or bone turnoverOur bones and skeleton are active tissues that constantly remodel throughout life to
maintain structural architecture, adjust to mechanical forces, repair microdamage and maintain calcium homeostasis.10 Bone remodeling or bone turnover consists of three consecutive phases and mainly involves two groups of cells: the mesenchymal-origin osteoblasts and the hematopoietic-origin osteoclasts. During resorption, the first phase of bone remodeling, osteoclast precursors are activated, fuse to form multinucleated osteoclasts, attach to bone surfaces and start resorbing bone. During the subsequent reversal phase, bone resorption ceases and mononucleated cells line the bone surface prior to the final bone formation phase. Finally, during the formation phase, mesenchymal cells differentiate into osteoblasts that deposit the non-mineralized part of bone (osteoid) that will later mineralize to form mature bone.11, 12
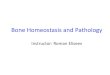
Bone resorption and formation are highly regulated processes. A coupling mechanism between the two assures that bone formation and resorption are balanced to maintain the integrity of our skeletons.10, 12 This communication is achieved through an array of systemic and local factors, such as cytokines, hormones and growth factors. These signals converge on the RANKL/RANK/OPG pathway.11, 12
The receptor activator of nuclear factor kappa-B ligand (RANKL) is expressed on the surface of preosteoblastic cells. It binds to RANK, a receptor on the surface of osteoclast precursors. The binding of RANKL to RANK activates bone resorption by triggering the fusion of preosteoclasts to form functional osteoclasts, by inhibition of osteoclast apoptosis (programmed cell death). In contrast, osteoprotegerin or OPG is a soluble decoy receptor produced by osteoblast lineage cells. It binds to RANKL, inhibits its association with RANK and activation of resorption.11, 12 Proper maintenance of the RANKL/OPG ratio through the systemic and local factors mentioned above ensures proper bone formation/resorption coupling and osseous maintenance. When, RANKL increases or OPG decreases, bone resorption occurs, while bone formation results when OPG increases or RANK decreases.12

Bisphosphonates (BPs)Although both nitrogen and non-nitrogen containing bisphosphonates are available,
the former are most popular as they are more potent compared to their non-nitrogen counterparts.1,13 Also, they are the ones most associated with MRONJ.1,14 As a result, the following discussion refers to the nitrogen-containing BPs.
Bisphosphonates are antiresorptive drugs that resemble pyrophosphate, a naturally occurring inhibitor of mineralization. However, due to their structure, they are very resistant to degradation, and they bind strongly to hydroxyapatite, the main bone crystal. Once bound, they can become buried in osteoid and remain within the skeleton for years.6 When exposed during resorption, they are internalized by osteoclasts. This leads to inhibition of certain intracellular metabolic pathways (the mevalonate pathway), ultimately causing osteoclast inactivation and apoptosis.14,15
Bisphosphonates are used for the treatment of osteopenia, or metabolic bone diseases such as osteoporosis, and cancer patients with malignancies that affect the skeleton.5, 9
Osteoporosis is a relatively common disease where bone resorption exceeds bone apposition leading to decreased bone mass and altered bone microarchitecture.15,16 These patients present with bone fragility and increased fracture risk.14,15 As bisphosphonates inhibit osteoclast function, and thus bone resorption, they are widely used to maintain bone mineral density and prevent fractures in osteoporosis patients.5,14,15 When bisphosphonates are used in this setting, they are usually given orally in low doses, although intravenous (IV) administration of BPs in low doses is also used.5
Bone is a common site for metastasis of many malignancies, especially breast, prostate and lung cancer.17,18 Multiple myeloma, another form of cancer, commonly causes osseous lesions.5,18 All the above conditions can potentially lead to skeletal-related events, such as pain, fractures and hypercalcemia of malignancy causing high morbidity and low quality of life in patients.5,19 Due to their antiresorptive and antiangiogenic properties, BPs are used intravenously in high doses in cancer patients to prevent these adverse events.17,19
DenosumabDenosumab is a human monoclonal antibody that mimics the action of
osteoprotegerin (OPG). By binding to RANKL and blocking its interaction with RANK on the surface of osteoclast precursors, osteoclasts are not activated, and bone resorption is inhibited.15,16 Due to its antiresorptive functions, it has been used for the treatment of osteoporosis (low doses) and metastatic bone disease (high doses).5,9 It differs from bisphosphonates in the fact that its effects are reversible in a much shorter period of time.16
Studies have shown that subjects receiving denosumab for osteoporosis have decreased risk of vertebral, non-vertebral and hip fractures, higher bone mineral density and lower serum bone turnover markers compared to patients receiving placebo.2-4 It is administered as a subcutaneous injection once every 6 months. It has been shown that serum denosumab concentrations are extremely low at the sixth month after administration, confirming its lack of persistence in the body.4,16
Denosumab is administered in higher doses in patients with malignancies to prevent skeletal-related events with indications similar to those for bisphosphonates5.

Figure 1: Diagram summarizing the mechanism of action of BPs and denosumab. This diagram is taken from a paper written by Wat et al6.
Name Commercial name Route Condition
Alendronate Binosto, Fosamax Oral Osteoporosis
Risedronate Actonel, Atelvia Oral Osteoporosis, Paget’s disease
Ibandronate BonivaOral,
Intravenously
Osteoporosis (low doses),
Malignancies (high doses)
Zoledronate Reclast, Zometa IntravenousOsteoporosis, Paget’s disease (low
doses), Malignancies (high doses)
Pamidronate Aredia Intravenous Malignancies
Denosumab Prolia Subcutaneous Osteoporosis (low doses)
Denosumab Xgeva Subcutaneous Malignancies (high doses)
Table 1: Summary of the most commonly used antiresorptive medications, their commercial name, route of administration and indication of use.

Antiangiogenic agentsAngiogenesis is a detrimental property of tumor cells that allows them to induce
new blood vessel formation to promote tumor growth and spread. Antiangiogenic agentsstrive to decrease this function by specifically targeting and inhibiting growth factors orintracellular pathways of tumor cells that would lead to formation of new vessels.8 One ofthe most common targets of these agents is the vascular endothelial growth factor(VEGF). Beside its function in angiogenesis, VEGF also plays a role in osteoclast functionand survival.6,8
There are two main categories of antiangiogenic drugs:8• Tyrosine kinase inhibitors: these agents are usually given orally.8 Sunitinib and
cabozantanib are examples of this category of medications that have beenassociated with ONJ.6,8
• Monoclonal antibodies: these agents are given either intravenously orsubcutaneously8. Bevacizumab has been associated with ONJ.6,8
Other antiangiogenic medications that have been reported to cause ONJ includefusion proteins, mammalian target of rapamycin (mTOR) inhibitors, radiopharmaceuticals,selective estrogen receptor modulators, BRAF inhibitors and immunosuppressants.7,8
Reports describing associations between those agents and ONJ are rare; however, thismay affect their relatively recent introduction to clinical practice. It is important toremember that except for their antiangiogenic properties, many of these agents haveimmunomodulatory actions as well. Thus, they are also used for treatment of autoimmuneand inflammatory diseases such as rheumatoid arthritis and Crohn disease.8
PathogenesisThe precise pathogenetic mechanism of MRONJ has not yet been fully elucidated. It
is interesting to note that MRONJ presents almost exclusively in the maxillofacial region, afact that has not been fully explained. The most prevalent hypotheses for the manifestationof this condition are presented below. Ultimately, it is believed that MRONJ is a multifactorialcondition that could result from a combination of the following influences:91. Suppressed bone turnover: jaw bones are constantly subjected in mechanical forces
and are characterized by a high rate of bone turnover that assures than anymicrodamage is effectively repaired.21 As antiresorptive medications impede thisphysiologic process, it is believed that osseous damage and microcracks accumulateand finally lead to necrotic bone areas.6,9,22
2. Infection: Studies have shown the presence of a mixed microbial flora on the surfaceof MRONJ lesions.23 Actinomyces species have been well associated with MRONJ, aswell as anaerobic bacteria, such as Porphyromonas, Lactobacillus, Tannerella,Prevotella, Actinomyces, Treponema, Streptococcus, and Fusobacterium.23-25
Additionally, according to the acidification theory, presence of infection lowers the pH,which leads to further release and activation of BPs, and thus greater inhibition of boneresorption and remodeling.13 Yet, it remains uncertain if the bacteria trigger the lesionor colonize the necrotic bone after the lesion has occurred.6,26
3. Direct cellular toxic effects: Toxic effects to epithelial and immune cells can lead todisruption of the oral mucosal coverage and immune dysregulation.6,9,21 Theseabnormalities could further lead to delayed wound healing and necrosis.

4. Inhibition of angiogenesis: Adequate blood supply is pivotal for wound healing. As aresult, inhibition of angiogenesis seen with these medications could lead to necrosis.8,9
Additionally, this theory could explain why MRONJ is more common in the mandible thanin the maxilla. The dense mandibular bone in association with its single vascular supplycould further compromise blood perfusion in the area. Although this theory is relevant inthe case of bisphosphonates and antiangiogenic medications, it does not apply todenosumab treatment, as inhibition of angiogenesis is not a feature of denosumab.9,21
DiagnosisMRONJ is rare. It is estimated that the average general dentist will see 1 new case of
MRONJ for every 62 years in practice.27 However, if and when this happens, dentalprofessionals need to be able to diagnose the condition early to avoid the health burdenassociated with advanced stages of MRONJ.28 Diagnosis is based on review of healthhistory, clinical presentation and radiographic findings.29
• Medical historyA careful review of the patient’s history will reveal any current or past exposure of the
patient to antiresorptive or antiangiogenic drugs. It is important to stress that patients oftenmention their underlying disease, such as osteoporosis, and do not mention their prescribedmedications, as they consider them unrelated to dental treatment. Dental professionalsshould remain vigilant and inquire for prescribed antiresorptive and antiangiogenicmedications, especially in patients reporting related diseases. Communication with thephysician is necessary if there are inconsistencies or questions regarding the patient’smedical history.
• Clinical and radiographic findingsMRONJ is usually seen in older individuals (60-80 years old) and most commonly in
females.30,31 This does not come as a surprise as older women represent the majority ofpatients receiving MRONJ-related medications for treatment of osteoporosis and breastcancer.32 It is most frequently seen in the mandible, as compared to the maxilla andpresentation in both jaws is possible, but rare.9,30,31 It has a predilection for the posteriorareas of the jaws.9,13,31
The most common clinical signs and symptoms of MRONJ include pain and exposedbone.13,23 Exposed bone can involve small areas, such as an extraction socket, or widerareas, sometimes involving the whole jaw.29 Inflammation with redness and swelling(extraoral or intraoral) is also a frequent finding.13,23,29 Other findings include fistulas, pus,disturbances in wound healing, loosening of teeth, sinus pain or sinusitis, altered nervesensation and pathological fractures in advanced cases.9,13,23
Except for a detailed clinical examination, radiographic imaging is also important fordiagnosis of disease. Plain periapical radiographs and orthopantomograms are useful tools.However, if the disease is in its initial stages and bone alterations are not advanced, theseradiographic techniques may not identify pathologic findings.29,33,34 Cone beam computedtomography (CBCT) may be helpful and is highly recommended when plain films arenegative in patients who present with symptoms.29,35 Other advanced radiographictechniques, such as computed tomography (CT), magnetic resonance imaging (MRI) andbone scintigraphy may be useful to allow a more precise identification of the extent of thedefect.29,34-36

Radiographic findings are not specific for MRONJ and should always be interpreted incombination with the clinical findings and the patient’s health history. They can include areasof osteosclerosis (diffuse or local) or osteolysis, sequestrum formation surrounded byradiolucent bone and lack of bone formation in extraction sites.33,37-39 Thickening of thelamina dura, decreased periodontal ligament space or alveolar bone loss, that cannot beattributed to periodontal disease should be examined carefully.9,38 Cortical erosion,enhancement of the inferior alveolar canal or the external oblique ridge, periosteal reaction,cloudiness of the maxillary sinus and fracture can also be seen. The border between necroticand healthy bone is often poorly-defined.9,33,35,38,40
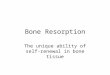
Figure 2: Radiographic findings in patients with MRONJ. The orthopantomogram on the left shows areas of osteolysis and osteosclerosis (white arrow) in a patient with MRONJ (radiograph taken from a paper by Sahin et al.41 ). The orthopantomogram on the right depicts a sequestrum (black arrow) in a patient with MRONJ (radiograph taken from a paper by Wang et al.42)

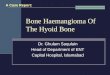
Figure 3: Clinical photo, orthopantomogram and CBCT of MRONJ in a patient receiving Xgevia (denosumab) for treatment of multiple myeloma. MRONJ presented after extraction of two teeth in the posterior right maxillary area. This case would be classified as stage 3 due to presence of oroantral communication (white arrow in the orthopantomogram). Note the difference between right and left maxillary sinuses, as shown in the CBCT image. (Photo and radiographs are courtesy of Dr. Shaun Rotenberg, DMD, MS)
Clinical Findings Radiographic findings
Pain Osteosclerosis / osteolysis
Exposed bone Sequestrum
Redness Thick lamina dura
Swelling Narrow periodontal ligament
Pus Alveolar bone loss
Fistulas Cortical erosion
Delayed or inhibited wound healing Periosteal reaction
Tooth loosening Enhancement of inferior alveolar canal
Sinus alterations Enhancement of external oblique ridge
Sensory alterations Sinus alterations
Fracture Fracture
The following table provides a summary of the most common clinical and radiographic findings in patients with MRONJ.
Table 2: Summary of the most common clinical and radiographic findings in patients with MRONJ

The AAOMS has suggested a staging of the disease to facilitate diagnosis andtreatment strategies of MRONJ (Table 3). The staging system includes 4 disease stages(Stage 0-3), as well as a risk category.9
That includes all patients with a history of antiresorptive or anti-angiogenictreatements.9
Although exposed bone or bone that can be probed through a fistula is thehallmark of MRONJ, a variant of it has recently been described where patients do notpresent with exposed bone, but have other non-specific signs and symptoms that indicateMRONJ.9 These patients can present with odontalgia, jaw pain, sensation alterations,loosening of teeth or periapical and periodontal fistulas. Plain radiographs can revealpathologic findings as described above, but these are contained to the alveolar bone.9,38
If these clinical and radiologic findings cannot be attributed to diseases of dental origin,such as pulpal necrosis or periodontitis, in a patient receiving antiresorptive orantiangiogenic medications, the non-exposed variant or Stage 0 of MRONJ should besuspected. Early recognition is important as some of these patients will progress to moreadvance stages of MRONJ.9
Stage 1 describes cases with exposed bone, but no infection or pain. Stage 2involves cases with infection/inflammation and pain. Pus may or may not be present. Thebone exposure in stages 1 and 2 is contained to the alveolar bone. Stage 3 representsadvanced cases of MRONJ where destruction has progressed beyond the alveolar bone.
To categorize a lesion as stage 3, pain and inflammation need to be presentconcomitantly with one or more of the following: fracture, extraoral fistula, oralcommunication with the nose or maxillary sinus or osteolysis to the inferior border of themandible or the sinus.9
Figure 4: Spontaneous MRONJ in patient receiving zolendronate (Reclast). This case would be considered stage 1, due to the presence of exposed bone without evidence of infection. (Photo is courtesy of Dr. Shaun Rotenberg, DMD, MS)

StageExposed bone or fistula
probing to bonePain Infection Extent
At risk No No No N/A
Stage 0 NoPain or other non-specific
findingsPossibly N/A
Stage 1 Yes No No Alveolar bone
Stage 2 Yes Yes Yes Alveolar bone
Stage 3 Yes Yes Yes Beyond the alveolar bone
Table 3: Main characteristics of MRONJ staging categories.
Figure 5: Left photo shows a case of MRONJ after tooth extraction in a patient receiving Reclast (zolendronate). Note the redness and slight swelling at the margins of the lesion indicating presence of infection and thus classifying the lesion as stage 2. Right photo shows another case of stage 2 spontaneous MRONJ in a patient receiving oral Fosamax (alendronate) for the treatment of osteoporosis. Note the presence of pus next to the area of exposed bone as well as lingual to the premolar. (Photos are courtesy of Dr. Shaun Rotenberg, DMD, MS)
HistologyHistology is not diagnostic of MRONJ and can resemble other inflammatory bone
conditions.29 Having said that, if surgical management of MRONJ lesions is planned, submission of necrotic bone for histologic analysis is deemed necessary to support the clinical diagnosis and rule out the possibility of bone malignancies that have been found concealed in areas of necrotic bone in certain patients.35
Briefly, histology of MRONJ lesions is characterized by necrotic bone devoid of osteocytes and osteoblasts. Inflammatory cells and bacteria are abundant in the specimen.35,43

o Gingivitis and periodontitis o Fibro-osseous lesions
o Peri-implantitis o Malignancies
o Caries o Osteoradionecrosis
o Peri apical pathology o Atypical neuralgia
o Alveolar osteitis or dry socket o TMJ disorders
o Sinusitis o Exposed bone – not related to MRONJ
• Differential DiagnosisConditions that can mimic MRONJ and complicate diagnosis include the following:9,29,44
Although differential diagnosis among these conditions can be difficult, a detailedmedical history and clinical examination can point the dental professional to the rightdirection.
Patients administered MRONJ-related medications are always considered at risk.However, as it will be discussed in the next section, low doses of these medications inosteoporosis patients pose a lower risk of MRONJ compared to higher dosesadministered to cancer patients.31 Furthermore, for the conditions mentioned in the leftcolumn above, duration of the symptoms and response to treatment can guide diagnosis.More specifically, in cases of patients on antiresorptive medications, where routine dentaltreatment was provided, but did not resolve the symptoms, MRONJ should be suspectedand referral to a specialist given.
The conditions in the right column further complicate diagnosis. Most of theseconditions are chronic and require management by a specialist. Additionally,osteoradionecrosis, malignancies and fibro osseous lesions, such as fibrous dysplasia canpresent with clinical and radiographic findings similar to MRONJ.45,46 If a dentalprofessional comes across these findings and cannot attribute them to a known dentalcondition, referral is indicated.
Osteoradionecrosis can resemble MRONJ both clinically and radiographically.Moreover, these conditions have similar risk factors or trigger events, such as dentalextractions.45 Osteoradionecrosis is defined as “an area greater than 1cm of exposedbone in a field of irradiation that has failed to show any evidence of healing for at least 6months.”45 Patients that received radiation for the treatment of malignancies in the headand neck region have a lifelong risk for jaw necrosis and by definition cannot be diagnosedwith MRONJ.45 Medical history will aid the diagnosis in this case.
Finally, some cases of idiopathic bone exposure without any predisposing factorshave been mentioned in the literature. In a case report, bone exposure was noted in thelingual mandible of a patient after tooth extraction.44 The patient had no contributingmedical history. The lesions healed with proper management and the bone exposure wasattributed to trauma and local ischemia due to local anesthesia.44 Medical history andresponse to therapeutic strategies helped with diagnosis.
According to the definition of MRONJ, exposed bone that persists for more than 8weeks is necessary for diagnosis.9 However, it is imperative to note that if a dentalprofessional comes across a situation that resembles MRONJ in a patient withcontributing medical history, prompt referral to an oral and maxillofacial surgeon iswarranted even if exposed bone has been present for less than 8 weeks.

Predisposing Factors and Incidence/Prevalence
In the following section, the terms “incidence” and “prevalence” will be mentioned. Itis considered prudent to define these terms for better comprehension. Incidence of acondition is defined as the number of new cases in a population in a specific unit of time.Prevalence is the number of cases in a population at a given time point.27
MRONJ can occur spontaneously in patients receiving antiresorptive orantiangiogenic drugs.23,30,35 However, there are certain predisposing factors that increasethe risk. These can be divided in the following categories:91. Medication – related factors2. Local factors3. Other factors
1. Medication - related factorsMedication-related factors refer to type of medication given, route of administration,
dosage, frequency and duration. All of these constitute the cumulative dosage that affectsthe occurrence of MRONJ.13,19
Nitrogen – containing bisphosphonates (BPs) bind tightly to the skeleton and canremain incorporated for years.15 This means that even following drug cessation, theirpresence in the bones can lead to MRONJ. Binding ability differs among the various BPs:zolendronic acid has the highest binding affinity, followed in decreasing order byalendronate, ibandronate and risedronate.47
Oral or intravenous (IV) administration of bisphosphonates also affects theirpotency. Bisphosphonates are not well absorbed by the oral route, and when administeredorally the majority of the drug is excreted.14,48 Instead IV administration leads toaccumulation of higher doses of the medication in the skeleton with higher possibility ofadverse effects.32,48,49
Dosage, frequency and duration are also important factors because they relate tothe amount of drug affecting the skeleton. Looking at oral bisphosphonates given forosteoporosis, studies have shown that 4 years is the cut-off time point where risk ofMRONJ increases.9 Regarding denosumab given for osteoporosis, a 10 year-long studyconcluded that there was no clear relationship between MRONJ risk and durationexposure, probably reflecting the non-binding quality of denosumab. On the other hand,MRONJ can occur in denosumab-treated patients as early as after the first dose.50,51
As the dose and frequency of these drugs increase, so does the risk of MRONJ.More specifically, a study by Aljohani et al. looked at a group of patients presenting withMRONJ and treated with denosumab.31 Patients receiving 60mg of denosumab every 6months for treatment of osteoporosis comprised only 16% of this group, in contrast topatients receiving 120mg every 4 weeks (cancer treatment) which comprised 78%.31
Another study tried to define the mean cumulative dosages that would result to MRONJ.That dose was 4503 mg for oral alendronate and 150mg for IV zolendronic acid.52
Finally, the risk of MRONJ increases when a cancer patient receives a combinationof antiresorptive and antiangiogenic drugs at the same time. For example, patients treatedconcomitantly with an antiresorptive agent and a VEGF-receptor tyrosine kinase inhibitorhave a five to ten times higher risk of developing MRONJ as compared to patientsreceiving only the antiresorptive agent.53

Given the issues in the cancer patient population, and knowing that patients treatedfor osteoporosis receive relatively low doses of antiresorptive medications, it is easy tounderstand why the risk of ONJ in this group is approximately 100 times smaller thancancer patients.9 More specifically, the risk of developing MRONJ in patients receiving oralbisphosphonates is less than 0.1%, but can rise to 0.21% in patients in treatment for morethan 4 years.9,27 The risk for patients on IV bisphosphonates or subcutaneous denosumabfor treatment of osteoporosis is also low (0.017 to 0.2%) and remains similar to the risk ofpatients receiving placebo9. In contrast, patients receiving IV zolendronate or denosumabfor cancer treatment have a risk of 1-2%, which is 50-100 times higher than in patientswith cancer receiving placebo.9,27
1. Local factorsAlthough MRONJ can occur spontaneously, multiple local factors have been implicated
as triggering events. These factors can be divided into operative and anatomic.23,30,35
a) Operative local factorsThe most well-documented triggering event for MRONJ is dental extractions.
According to the 2014 update of AAOMS, the risk of MRONJ after dental extraction for oralBP users is 0.5%. The percentage rises to 1.6-14.8% in cancer patients receiving IV BPs.9Dental extractions have been shown to be a precedent in 45 - 69.6 % of MRONJ caseswith a mean period between the extraction and MRONJ development of 3months.23,30,31,54-56
Dentoalveolar surgical procedures, including implant placement and periodontal andendodontic surgeries that require manipulation of bone have also been implicated in theoccurrence of MRONJ, but their documentation is less complete compared to toothextractions. More specifically, dentoalveolar surgery has been considered the triggeringevent in 7.2-21% of MRONJ cases and implant placement in 3.9 – 10.7 of thecases.23,30,54,56 Recognizing the absence of data, the AAOMS considers the risk to besimilar to that following tooth extractions.9
More information on the risk of MRONJ as it relates to implants is considerednecessary. According to a systematic review, implants in patients receiving intraoralbisphosphonates seem to have similar survival rates as the ones in patients not receivingantiresorptive medications (98.8 vs 97%).57 The survival rate drops in patients receiving IVbisphosphonates and implant placement is not considered safe in these patients.57
MRONJ after implant placement has been reported in patients receiving oral BPs, and therisk increases in the posterior areas of the jaw, when BP treatment is longer than 3 yearsand if the patient is also receiving corticosteroids.49,58 Additionally, except for cases ofMRONJ arising after implant surgery, necrosis can also occur around implants that havebeen placed and are functional for years before commencement of antiresorptivemedications.58,59 In this case, MRONJ can occur either spontaneously around well-osseointegrated implants or in a background of peri-implantitis.60 This has been reported inpatients receiving either BPs or denosumab.61 Dental professionals should be aware ofthis phenomenon and advise patients accordingly.
Other factors that have been associated with MRONJ occurrence include poor oralhygiene, presence of inflammation, periodontal disease and trauma from ill-fittingprostheses.9,13,23,54-56

b) Anatomic factorsAreas of thin mucosa overlying bone prominences, such as tori and the
myelohyoid ridge in the posterior mandible are anatomical factors that facilitate MRONJdevelopment after minor trauma.29 Apart from the dense bone and limited vasculature ofthe mandible, such anatomy is an additional factor that can explain the higher prevalenceof MRONJ in the mandible and especially the posterior areas.9,13,30,31
3. Other factors• Presence of systemic comorbidities and immunosuppressive drugs increase the risk
of MRONJ. Hyperthyroidism, hypothyroidism, diabetes, autoimmune disease andanemia, as well as treatment with corticosteroids or other immunosuppressants havebeen associated with increased risk of MRONJ in patients receivingantiresorptive/antiangiogenic medications.9,13,19,22,30,35 For patients with diabetes, theglycemic control is very important, as hyperglycemia exacerbates inflammation,vascular defects and negative effects on bone.62
• Although incompletely understood, genetics can also affect the risk of a patientdeveloping MRONJ.27,63
PreventionAlthough MRONJ is rare, it can be difficult to treat when it occurs.64 As a result,
prevention is of outmost importance in patients receiving MRONJ-related medications.Studies have shown that preventive actions reduce occurrence of MRONJ with a recentmeta-analysis reporting a decrease in the risk of 77.3%.9,19,65
Prevention against MRONJ relates to either one of the following categories ofpatients:• A patient not currently receiving MRONJ-related medications, but referred from his
physician for a dental check-up before initiation of such treatment.• A patient currently receiving MRONJ-related medications.
In both cases, dental professionals need to evaluate the risk of MRONJ, as it relatesto each patient taking into consideration the underlying disease, dosage and duration ofmedication.18,66 More specifically, the following categories of patients should beconsidered:9• Patients on antiresorptive medications for the treatment of osteoporosis, receiving this
medication for less than 4 years (for oral bisphosphonates) without any other riskfactors: generally considered at low risk.
• Patients on antiresorptive medications for the treatment of osteoporosis, receiving thismedication for less than 4 years (for oral bisphosphonates) and presenting with otherconcomitant risk factors, such as corticosteroids or antiangiogenic medication:considered at high risk.
• Patients on antiresorptive medications for the treatment of osteoporosis, receiving thismedication for more than 4 years (for oral bisphosphonates) and presenting with orwithout other concomitant risk factors, such as corticosteroids or antiangiogenicmedication: considered at high risk.
• Patient on antiresorptive or antiangiogenic medications for the treatment ofmalignancies: considered at the highest risk of all.

1. Prevention strategies for a patient not currently receiving MRONJ-relatedmedications, but referred from his physician for a dental check-up beforeinitiation of such treatment.
This initial screening should include a careful clinical and radiographicexamination.9,18
First of all, prevention starts with good patient education.9,18 It is important toexplain well and make sure that the patient comprehends the risk of MRONJ. His/heroral hygiene, motivation and compliance with future regular dental check-ups should beevaluated and improved, if deemed inadequate at this initial appointment. Additionally,patients should be instructed to promptly report any MRONJ-related symptoms thatmay arise, such as pain, swelling, pus or exposed bone.9,67 Although there areconflicting findings on the association between smoking and MRONJ, consider advisingpatients on smoking cessation.9,55,67
Areas of infection or inflammation should be identified and treated. Dentalprophylaxis, periodontal treatment, caries management and periapical pathologyshould be addressed at this time. Consider fluoride application. Non-restorable teeth orteeth with poor prognosis should be extracted and other necessary dentoalveolarprocedures should be performed. It is advised to allow sufficient time for mucosalcoverage (14-21 days) or osseous healing before initiation ofantiresorptive/antiangiogenic medication (as long as systemic condition permits).9,18
Removable restorations should be evaluated to assure that they are not causingtrauma to the underlying tissues.9,18,50 It is prudent to advise patients not to wear theirdentures for some hours of the day, and soft liners could be considered.1,66 Regardingfixed tooth-supported restorations, assure that the margins are not impinging into thebiologic width of abutment teeth.66 Finally, since MRONJ has been reported aroundimplants placed before initiation of such medications, nit is wise to advise patients withimplant-supported prostheses about this risk.59,61
For patients that will receive antiresorptive drugs in high doses for treatment ofmalignancies, dental professionals should strive to complete all the above actionsbefore initiation of treatment, as long as the systemic condition permits.9 On the otherhand, patients that will receive oral bisphosphonates for the treatment of osteoporosisare considered of low risk. Ideally, dental health should be restored before initiation ofsystemic treatment, but can also be completed within the first 6 months in thesepatients.66
2. Patients currently receiving MRONJ-related medications.For these patients, dental professionals should strive to maintain oral health, as
areas of infection could trigger MRONJ.9,18,30,54,56 Regular dental prophylaxis isconsidered safe and highly indicated.18 Endodontic treatment should be preferred todental extractions and instrumentation beyond the apex should be avoided.9,66
For patients receiving oral bisphosphonates for less than 4 years, extractions,elective dentoalveolar surgeries and implant placement are not contraindicated.However, patients need to be informed about the low risk of MRONJ and provideappropriate consent.9

The risk of MRONJ increases if the patients above have other concomitant riskfactors or are receiving oral bisphosphonates for more than 4 years. Extractions andelective dentoalveolar procedures are still not contraindicated in these patients, but theAAOMS advises to consider a drug holiday.9 Drug holiday involves the cessation of theantiresorptive medication for a time period before and after the dental procedure.Bisphosphonates bind to and reside within the skeleton for multiple years.15 As a result,the benefit of such a drug holiday is not well established. However, it seems that a drugholiday starting 2 months before the surgery and continuing until 3 months later (or untilosseous healing occurs) could be beneficial.9 Evidence on a denosumab drug holiday isnot well-established either. However, since this medication does not bind to the skeleton,it is possible that temporal cessation could have some positive effect.31 In any case, ifdrug holiday is considered, it should be done only after communication with theprescribing provider to ascertain that the patient’s systemic condition will not beaggravated.9,64
Finally, for patients receiving antiresorptive medications in high doses for treatment ofcancer, the risk of MRONJ is high. Thus, extractions and all surgical procedures thatinvolve manipulation of bone should be avoided.9 In case of non-restorable teeth, analternative to extraction would be removal of crown and endodontic therapy of the root.9Some studies have considered forced eruption to achieve atraumatic removal of thetooth.18
In cases where extractions cannot be avoided in this group of patients, the followinginstructions can help decrease the risk of MRONJ:• Extract the tooth as atraumatically as possible.• Smoothen all sharp bony edges that may remain after tooth extraction.68-70
• Consider raising a flap to achieve primary closure and isolate the extraction area ofpotential bacterial contamination. However, extensive surgical manipulations andexposure of a large osseous area in an effort to achieve primary closure should beavoided.18
• Have the patient use a chlorhexidine rinse 2-3 times / day before and after theextraction until the area heals.18,66
• Consider prescribing antibiotics. No specific antibiotic regimen has been decided inthe literature with studies reporting use of antibiotics before and after surgicalprocedures for various time periods.65,66,71 The AAOMS suggests the penicillingroup of antibiotics. For patients allergic to penicillins, quinolones, metronidazole,clindamycine, doxycycline, erythromycin, and azythromycin have been used.9,69,71
• Advise patients not to wear their prostheses until the surgical area heals.69
• In case where multiple extractions are needed, consider a staged approach.50
As mentioned above, patients receiving low doses of MRONJ-related medicationshave lower risk of developing osteonecrosis as compared to cancer patients. However,the above guidelines should be considered in the former group of patients as well.

There is no consensus on provision of orthodontic treatment to patients onantiresorptive/antiangiogenic therapy. Tooth movement requires bone formation andbone resorption, processes that are inhibited by these medications. For patients on IVantiresorptive treatment, orthodontic movement should be avoided.48 For patients onoral agents, it could be considered.48 However, slower and more limited movement ofteeth has been reported. Patients should be monitored for inhibition of tooth movementand MRONJ development.48,72
It is imperative to emphasize that if a dental professional does not feelcomfortable performing an extraction or surgical procedure on a patient receivingMRONJ-related medications, referral to an oral and maxillofacial surgeon is considerednecessary. Additionally, patients with past (and not current) exposure to antiresorptiveagents should always be treated cautiously at the dental office, as the antiresorptiveeffects of such medications linger after treatment cessation.15
TreatmentTreatment of established MRONJ may not be within the scope of the general
dentist. If MRONJ is suspected, the patient might need to be referred to an oral andmaxillofacial surgeon or other specialist with experience in the management of theselesions. Thus, the following section is not intended to be inclusive of all availabletreatment options. Rather, it aims to provide an overview of the most commontreatments, which are divided in two broad categories: non-surgical and surgical.36
Non-surgical treatment appropriate for general dentists includes the applicationof topical and/or systemic antimicrobials.36 This involves chlorhexidine, an antimicrobialknown to decrease bacterial plaque and inflammation, and systemic antibiotics. Oralantibiotics are usually the first treatment option, but intravenous alternatives can beconsidered in extensive or refractory cases.36,73
Surgical treatment includes debridement and resection.36 Debridement is moreconservative aiming to remove some necrotic bone, but not necessarily all of it, whileresection involves the removal of all necrotic bone until healthy vital bone is seen.36,74,75
Segmental resection is the most extensive form of resection where necrotic bone isremoved en bloc, frequently resulting in discontinuity defects that requirereconstruction. Removed bone should be submitted for histology to exclude thepresence of malignancy.36
Current studies show very good outcomes with surgical treatment.26,32,76 Toachieve success, it is important to remove all necrotic bone.35,36,74,75 This can beaccomplished with detailed analysis of pre-operative CT and CBCT scan and othertechniques, such as fluorescent-guided surgery.34 Additionally, failure to achieve softtissue closure and operator’s skills may affect the outcome.35,36,64
Currently, there is no agreement on which treatment is the most appropriate forthe management of MRONJ. The position paper of the AAOMS, as well as otherauthors suggest following a stage-guided treatment decision.9,36,64 Initial stages shouldbe treated with conservative treatment and surgical approaches should be implementedonly when the non-surgical ones have failed. An additional benefit of conservativetreatment, even if it does not lead to the resolution of the condition, could be thedecrease of the extent of the wound and infection, thus potentially making the surgicalapproach more well-managed64. Surgical techniques are indicated in advanced MRONJstages, such as patients with Stage 3 disease.9

Keeping in mind the above, the AAOMS position paper suggests painmanagement, antibiotics and observation for patients with Stage 0 disease.9 Stage 1management should include antibacterial mouth rinses and consideration of a drugholiday. Mouth rinses, antibiotics, pain control and debridement are considerations forStage 2 and Stage 3 disease. Stage 3 patients are also candidates for resectionsurgeries.9
Regardless of the staging of the disease, there are some guidelines that shouldbe considered in all patients with MRONJ. Dentoalveolar surgeries should be avoided inall such patients.9 However, teeth in the necrotic bone areas should be extracted toeliminate a source of infection, especially since it is not believed that extraction of theseteeth will result in extension of necrosis.9 Loose sequestra that create soft tissueirritation should be removed.9 Finally, conservative treatment is always the treatmentoption for patients who deny surgery or the ones whose systemic condition does notallow surgery.75
Antibiotics are frequently mentioned in the management of MRONJ. Most studiessuggest penicillin-based antibiotics with or without β-lactamase inhibitor.71 For patientswith allergy to penicillin, clindamycin is the alternative most commonly used in studies,but other options include quinolones, metronidazole, azithromycin, doxycycline, anderythromycin.9,36,71 The duration of treatment has not been decided and in studies itranges between 1-7 days pre-operative and 5 days – 6 weeks post-operatively.71
Another controversial issue is whether cessation of theantiresorptive/antiangionenic agent (drug holiday) will aid with treatment. There arestudies that report better treatment outcomes in patients who followed a drugholiday.64,77 However, since bisphosphonates remain in the skeleton even aftercessation of the medication, other studies report that there is no evidence to support theusefulness of a drug holiday with these medications.54 Instead, denosumab cessationwould be more reasonable.26,54 In any case, it is important to remember that thedecision on a drug holiday is dependent on the patient’s systemic condition and shouldonly be implemented after communication with the physician.64
Other treatments that have been used in combination with conservative orsurgical treatment include platelet-rich plasma, laser, parathyroid hormone (PTH), bonemorphogenic proteins and pentoxifylline and vitamin E. Further research is required toestablish the predictability of these treatments.9,36,54
Serological Markers
Finally, a brief discussion on serological markers will conclude this course. Someauthors have supported the measurement of markers of bone turnover in the serum inan effort to identify patients that are at risk of developing MRONJ after extractions andother surgical procedures.78,79 These molecules are by-products of bone formation orbone resorption and include the c-terminal telopeptide cross-link of type I collagen(CTX), osteocalcin (OC), parathyroid hormone (PTH) and bone-specific alkalinephosphatase (BAP).78

The most well-known of these markers is the CTX. It is a degradation product thatarises when osteoclasts resorb bone and collagen I (the major organic component ofbone) is cleaved.79 It has been suggested that patients who are at risk of MRONJ willpresent with great inhibition of bone turnover due to their antiresorptive medications,and thus low CTX values. CTX values less than 100 pg/mL, 100-150 pg/mL andabove 150 pg/mL have been suggested to identify high, moderate and low riskpatients respectively.79
Although this concept sounds promising, other studies have found nocorrelation between CTX values and MRONJ development.80 According to the 2014update of the AAOMS, the use of these markers has not been validated.9

References
1. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. JOral Maxillofac Surg 2003;61(9):1115-7.
2. Papapoulos S, Chapurlat R, Libanati C, et al. Five years of denosumab exposure in women with postmenopausalosteoporosis: results from the first two years of the FREEDOM extension. J Bone Miner Res 2012;27(3):694-701.
3. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women withosteoporosis. N Engl J Med 2009;361(8):756-65.
4. Bone HG, Wagman RB, Brandi ML, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis:results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol 2017;5(7):513-23.
5. Nicolatou-Galitis O, Schiodt M, Mendes RA, et al. Medication-related osteonecrosis of the jaw: definition and best practicefor prevention, diagnosis, and treatment. Oral Surg Oral Med Oral Pathol Oral Radiol 2019;127(2):117-35.
6. Wat WZM. Current Controversies on the Pathogenesis of Medication-Related Osteonecrosis of the Jaw. Dent J (Basel)2016;4(4).
7. Nicolatou-Galitis O, Kouri M, Papadopoulou E, et al. Osteonecrosis of the jaw related to non-antiresorptive medications: asystematic review. Support Care Cancer 2019;27(2):383-94.
8. King R, Tanna N, Patel V. Medication-related osteonecrosis of the jaw unrelated to bisphosphonates and denosumab-areview. Oral Surg Oral Med Oral Pathol Oral Radiol 2019;127(4):289-99.
9. Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper onmedication-related osteonecrosis of the jaw--2014 update. J Oral Maxillofac Surg 2014;72(10):1938-56.
10. Frost HM. Skeletal structural adaptations to mechanical usage (SATMU): 1. Redefining Wolff's law: the bone modelingproblem. Anat Rec 1990;226(4):403-13.
11. Raisz LG. Physiology and pathophysiology of bone remodeling. Clin Chem 1999;45(8 Pt 2):1353-8.12. Hadjidakis DJ, Androulakis, II. Bone remodeling. Ann N Y Acad Sci 2006;1092:385-96.13. Otto S, Schreyer C, Hafner S, et al. Bisphosphonate-related osteonecrosis of the jaws - characteristics, risk factors, clinical
features, localization and impact on oncological treatment. J Craniomaxillofac Surg 2012;40(4):303-9.14. Pavone V, Testa G, Giardina SMC, et al. Pharmacological Therapy of Osteoporosis: A Systematic Current Review of
Literature. Front Pharmacol 2017;8:803.15. Anastasilakis AD, Polyzos SA, Makras P. THERAPY OF ENDOCRINE DISEASE: Denosumab vs bisphosphonates for the
treatment of postmenopausal osteoporosis. Eur J Endocrinol 2018;179(1):R31-R45.16. Deeks ED. Denosumab: A Review in Postmenopausal Osteoporosis. Drugs Aging 2018;35(2):163-73.17. Wu S, Dahut WL, Gulley JL. The use of bisphosphonates in cancer patients. Acta Oncol 2007;46(5):581-91.18. Goodday RH. Preventive Strategies for Patients at Risk of Medication-related Osteonecrosis of the Jaw. Oral Maxillofac
Surg Clin North Am 2015;27(4):527-36.19. Kajizono M, Sada H, Sugiura Y, et al. Incidence and Risk Factors of Osteonecrosis of the Jaw in Advanced Cancer Patients
after Treatment with Zoledronic Acid or Denosumab: A Retrospective Cohort Study. Biol Pharm Bull 2015;38(12):1850-5.20. Friedrich RE, Scheuer HA, Holtje W. The effect of bisphosphonate medication on orthodontics and orthognathic surgery in
patients with osteogenesis imperfecta. GMS Interdiscip Plast Reconstr Surg DGPW 2019;8:Doc06.21. Katsarelis H, Shah NP, Dhariwal DK, Pazianas M. Infection and medication-related osteonecrosis of the jaw. J Dent Res
2015;94(4):534-9.22. Kim KM, Rhee Y, Kwon YD, et al. Medication Related Osteonecrosis of the Jaw: 2015 Position Statement of the Korean
Society for Bone and Mineral Research and the Korean Association of Oral and Maxillofacial Surgeons. J Bone Metab2015;22(4):151-65.
23. Panya S, Fliefel R, Probst F, et al. Role of microbiological culture and polymerase chain reaction (PCR) of actinomyces inmedication-related osteonecrosis of the jaw (MRONJ). J Craniomaxillofac Surg 2017;45(3):357-63.
24. Russmueller G, Seemann R, Weiss K, et al. The association of medication-related osteonecrosis of the jaw withActinomyces spp. infection. Sci Rep 2016;6:31604.
25. Hallmer F, Bjornland T, Andersson G, et al. Bacterial diversity in medication-related osteonecrosis of the jaw. Oral Surg OralMed Oral Pathol Oral Radiol 2017;123(4):436-44.
26. Ruggiero S, Saxena D, Tetradis S, Aghaloo T, Ioannidou E. Task Force on Design and Analysis in Oral Health Research:Medication-Related Osteonecrosis of the Jaw. JDR Clin Trans Res 2018;3(3):222-25.
27. Dodson TB. The Frequency of Medication-related Osteonecrosis of the Jaw and its Associated Risk Factors. Oral MaxillofacSurg Clin North Am 2015;27(4):509-16.
28. Capocci M, Romeo U, Guerra F, et al. Medication-related osteonecrosis of the jaws (MRONJ) and quality of life evaluation: apilot study. Clin Ter 2017;168(4):e253-e57.
29. Ruggiero SL. Diagnosis and Staging of Medication-Related Osteonecrosis of the Jaw. Oral Maxillofac Surg Clin North Am2015;27(4):479-87.
30. Aljohani S, Fliefel R, Ihbe J, et al. What is the effect of anti-resorptive drugs (ARDs) on the development of medication-related osteonecrosis of the jaw (MRONJ) in osteoporosis patients: A systematic review. J Craniomaxillofac Surg2017;45(9):1493-502.
31. Aljohani S, Gaudin R, Weiser J, et al. Osteonecrosis of the jaw in patients treated with denosumab: A multicenter caseseries. J Craniomaxillofac Surg 2018;46(9):1515-25.
32. Ruggiero SL, Kohn N. Disease Stage and Mode of Therapy Are Important Determinants of Treatment Outcomes forMedication-Related Osteonecrosis of the Jaw. J Oral Maxillofac Surg 2015;73(12 Suppl):S94-S100.
33. Manea HC, Urechescu HC, Balica NC, et al. Bisphosphonates-induced osteonecrosis of the jaw - epidemiological, clinicaland histopathological aspects. Rom J Morphol Embryol 2018;59(3):825-31.
34. Tsuchimochi M, Kurabayashi T. Symposium: Imaging modalities for drug-related osteonecrosis of the jaw (1), role of imagingin drug-related osteonecrosis of the jaw: An up-to-date review (secondary publication). Jpn Dent Sci Rev 2019;55(1):1-4.
35.

35. Mucke T, Krestan CR, Mitchell DA, Kirschke JS, Wutzl A. Bisphosphonate and Medication-Related Osteonecrosis of theJaw: A Review. Semin Musculoskelet Radiol 2016;20(3):305-14.
36. Williams WB, O'Ryan F. Management of Medication-Related Osteonecrosis of the Jaw. Oral Maxillofac Surg Clin North Am2015;27(4):517-25.
37. Bagan J, Peydro A, Calvo J, et al. Medication-related osteonecrosis of the jaw associated with bisphosphonates anddenosumab in osteoporosis. Oral Dis 2016;22(4):324-9.
38. Sahin O, Odabasi O, Demiralp KO, Kursun-Cakmak ES, Aliyev T. Comparison of findings of radiographic and fractaldimension analyses on panoramic radiographs of patients with early-stage and advanced-stage medication-relatedosteonecrosis of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128(1):78-86.
39. Cardoso CL, Barros CA, Curra C, et al. Radiographic Findings in Patients with Medication-Related Osteonecrosis of theJaw. Int J Dent 2017;2017:3190301.
40. Klingelhoffer C, Klingelhoffer M, Muller S, Ettl T, Wahlmann U. Can dental panoramic radiographic findings serve asindicators for the development of medication-related osteonecrosis of the jaw? Dentomaxillofac Radiol2016;45(5):20160065.
41. Sahin O, Odabasi O, Aliyev T, Tatar B. Risk factors of medication-related osteonecrosis of the jaw: a retrospective study ina Turkish subpopulation. J Korean Assoc Oral Maxillofac Surg 2019;45(2):108-15.
42. Wang Q, Liu J, Qi S, et al. Clinical analysis of medication related osteonecrosis of the jaws: A growing severe complicationin China. J Dent Sci 2018;13(3):190-97.
43. Favia G, Pilolli GP, Maiorano E. Histologic and histomorphometric features of bisphosphonate-related osteonecrosis of thejaws: an analysis of 31 cases with confocal laser scanning microscopy. Bone 2009;45(3):406-13.
44. Bozana LB, Vanja VB, Ana KK, et al. Idiopathic Exposed Bone Lesions of the Jaw. Dent J (Basel) 2019;7(2).45. Grisar K, Schol M, Schoenaers J, et al. Osteoradionecrosis and medication-related osteonecrosis of the jaw: similarities and
differences. Int J Oral Maxillofac Surg 2016;45(12):1592-99.46. Pereira T, Gomes CC, Brennan PA, Fonseca FP, Gomez RS. Fibrous dysplasia of the jaws: Integrating molecular
pathogenesis with clinical, radiological, and histopathological features. J Oral Pathol Med 2019;48(1):3-9.47. Brown JP, Morin S, Leslie W, et al. Bisphosphonates for treatment of osteoporosis: expected benefits, potential harms, and
drug holidays. Can Fam Physician 2014;60(4):324-33.48. Zahrowski JJ. Bisphosphonate treatment: an orthodontic concern calling for a proactive approach. Am J Orthod Dentofacial
Orthop 2007;131(3):311-20.49. Granate-Marques A, Polis-Yanes C, Seminario-Amez M, Jane-Salas E, Lopez-Lopez J. Medication-related osteonecrosis of
the jaw associated with implant and regenerative treatments: Systematic review. Med Oral Patol Oral Cir Bucal2019;24(2):e195-e203.
50. Watts NB, Grbic JT, Binkley N, et al. Invasive Oral Procedures and Events in Postmenopausal Women With OsteoporosisTreated With Denosumab for Up to 10 Years. J Clin Endocrinol Metab 2019;104(6):2443-52.
51. Diniz-Freitas M, Fernandez-Feijoo J, Diz Dios P, Pousa X, Limeres J. Denosumab-related osteonecrosis of the jaw followingnon-surgical periodontal therapy: A case report. J Clin Periodontol 2018;45(5):570-77.
52. Hallmer F, Andersson G, Gotrick B, et al. Prevalence, initiating factor, and treatment outcome of medication-relatedosteonecrosis of the jaw-a 4-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 2018;126(6):477-85.
53. van Cann T, Loyson T, Verbiest A, et al. Incidence of medication-related osteonecrosis of the jaw in patients treated withboth bone resorption inhibitors and vascular endothelial growth factor receptor tyrosine kinase inhibitors. Support CareCancer 2018;26(3):869-78.
54. Kuroshima S, Sasaki M, Sawase T. Medication-related osteonecrosis of the jaw: A literature review. J Oral Biosci2019;61(2):99-104.
55. McGowan K, McGowan T, Ivanovski S. Risk factors for medication-related osteonecrosis of the jaws: A systematic review.Oral Dis 2018;24(4):527-36.
56. Kang MH, Lee DK, Kim CW, Song IS, Jun SH. Clinical characteristics and recurrence-related factors of medication-relatedosteonecrosis of the jaw. J Korean Assoc Oral Maxillofac Surg 2018;44(5):225-31.
57. Gelazius R, Poskevicius L, Sakavicius D, Grimuta V, Juodzbalys G. Dental Implant Placement in Patients onBisphosphonate Therapy: a Systematic Review. J Oral Maxillofac Res 2018;9(3):e2.
58. Giovannacci I, Meleti M, Manfredi M, et al. Medication-Related Osteonecrosis of the Jaw Around Dental Implants: ImplantSurgery-Triggered or Implant Presence-Triggered Osteonecrosis? J Craniofac Surg 2016;27(3):697-701.
59. Holzinger D, Seemann R, Matoni N, et al. Effect of dental implants on bisphosphonate-related osteonecrosis of the jaws. JOral Maxillofac Surg 2014;72(10):1937 e1-8.
60. Troeltzsch M, Cagna D, Stahler P, et al. Clinical features of peri-implant medication-related osteonecrosis of the jaw: Isthere an association to peri-implantitis? J Craniomaxillofac Surg 2016;44(12):1945-51.
61. Pogrel MA, Ruggiero SL. Previously successful dental implants can fail when patients commence anti-resorptive therapy-acase series. Int J Oral Maxillofac Surg 2018;47(2):220-22.
62. Rahimi-Nedjat RK, Sagheb K, Pabst A, Olk L, Walter C. Diabetes Mellitus and Its Association to the Occurrence ofMedication-Related Osteonecrosis of the Jaw. Dent J (Basel) 2016;4(2).
63. Sandro Pereira da Silva J, Pullano E, Raje NS, Troulis MJ, August M. Genetic predisposition for medication-relatedosteonecrosis of the jaws: a systematic review. Int J Oral Maxillofac Surg 2019.
64. Ramaglia L, Guida A, Iorio-Siciliano V, et al. Stage-specific therapeutic strategies of medication-related osteonecrosis of thejaws: a systematic review and meta-analysis of the drug suspension protocol. Clin Oral Investig 2018;22(2):597-615.
65. Karna H, Gonzalez J, Radia HS, Sedghizadeh PP, Enciso R. Risk-reductive dental strategies for medication relatedosteonecrosis of the jaw among cancer patients: A systematic review with meta-analyses. Oral Oncol 2018;85:15-23.
66. Di Fede O, Panzarella V, Mauceri R, et al. The Dental Management of Patients at Risk of Medication-Related Osteonecrosisof the Jaw: New Paradigm of Primary Prevention. Biomed Res Int 2018;2018:2684924.
67. Zebic L, Patel V. Preventing medication-related osteonecrosis of the jaw. BMJ 2019;365:l1733.68. Topaloglu G, Koseoglu OT, Karaca C, Kosemehmetoglu K. The effect of chronic dental inflammation on development of
Stage 0 medication-related osteonecrosis of the jaw. J Craniomaxillofac Surg 2017;45(8):1158-64.69. Heufelder MJ, Hendricks J, Remmerbach T, et al. Principles of oral surgery for prevention of bisphosphonate-related
osteonecrosis of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol 2014;117(6):e429-35.70.

70. Gaudin E, Seidel L, Bacevic M, Rompen E, Lambert F. Occurrence and risk indicators of medication-related osteonecrosisof the jaw after dental extraction: a systematic review and meta-analysis. J Clin Periodontol 2015;42(10):922-32.
71. Akashi M, Kusumoto J, Takeda D, et al. A literature review of perioperative antibiotic administration in surgery formedication-related osteonecrosis of the jaw. Oral Maxillofac Surg 2018;22(4):369-78.
72. Leung FY, Rabie AB, Wong RW. Osteoporosis, osteonecrosis, and orthodontics. World J Orthod 2009;10(3):261-71.73. Goutham BS, Manchanda K, Sarkar AD, et al. Efficacy of two commercially available Oral Rinses - Chlorohexidine and
Listrine on Plaque and Gingivitis - A Comparative Study. J Int Oral Health 2013;5(4):56-61.74. Spanou A, Lyritis GP, Chronopoulos E, Tournis S. Management of bisphosphonate-related osteonecrosis of the jaw: a
literature review. Oral Dis 2015;21(8):927-36.75. Ristow O, Otto S, Troeltzsch M, Hohlweg-Majert B, Pautke C. Treatment perspectives for medication-related
osteonecrosis of the jaw (MRONJ). J Craniomaxillofac Surg 2015;43(2):290-3.76. El-Rabbany M, Sgro A, Lam DK, Shah PS, Azarpazhooh A. Effectiveness of treatments for medication-related
osteonecrosis of the jaw: A systematic review and meta-analysis. J Am Dent Assoc 2017;148(8):584-94 e2.77. Hinson AM, Siegel ER, Stack BC, Jr. Temporal correlation between bisphosphonate termination and symptom resolution
in osteonecrosis of the jaw: a pooled case report analysis. J Oral Maxillofac Surg 2015;73(1):53-62.78. Peisker A, Raschke GF, Fahmy MD, et al. Cross-Sectional Study of four Serological Bone Turnover Markers for the Risk
Assessment of Medication-Related Osteonecrosis of the Jaw. J Craniofac Surg 2018;29(2):e137-e40.79. Marx RE, Cillo JE, Jr., Ulloa JJ. Oral bisphosphonate-induced osteonecrosis: risk factors, prediction of risk using serum
CTX testing, prevention, and treatment. J Oral Maxillofac Surg 2007;65(12):2397-410.80. Awad ME, Sun C, Jernigan J, Elsalanty M. Serum C-terminal cross-linking telopeptide level as a predictive biomarker of
osteonecrosis after dentoalveolar surgery in patients receiving bisphosphonate therapy: Systematic review and meta-analysis. J Am Dent Assoc 2019.

Post-Course Questionnaire• Answer each question ONLINE (link provided on SMS website)• Answer 12 of 16 questions correctly to pass• Answer post-course survey questions and click “Finish”• Deadline is September 19, 2019 4:30pm
1. A patient is diagnosed with MRONJ, if he/she is receiving antiresorptive/antiangiogenic medication, does not have a history of radiation therapy or metastatic disease to the jaws and presents with exposed bone or bone that can be probed through a fistula for at least:
a. 2 weeksb. 4 weeksc. 6 weeksd. 8 weeks
2. MRONJ presents only in patients with current or past exposure to bisphosphonates.a. TRUEb. FALSE
3. Which of the following categories of patients has the highest risk of developing MRONJ?
a. Patients receiving high doses of IV or subcutaneous antiresorptive medications for the treatment of cancer-related events.
b. Patients receiving low doses of IV antiresorptive medications for the treatment of osteoporosis.
c. Patients receiving oral bisphosphonates for treatment of osteoporosis for more than 4 years.
d. Patients receiving oral bisphosphonates for treatment of osteoporosis for less than 4 years.
4. Medical history is an important component of proper diagnosis and prevention of MRONJ.
a. TRUEb. FALSE

5. MRONJ presenting with exposed bone and absence of pain and infection is classified as:
a. Stage 0b. Stage 1c. Stage 2d. Stage 3
6. MRONJ presenting with exposed bone and presence of pain and infection with or without pus is classified as:
a. Stage 0b. Stage 1c. Stage 2d. Stage 3
7. Dental extractions are a common triggering event of MRONJ.a. TRUEb. FALSE
8. If a dental extraction is necessary on patients receiving antiresorptive/ antiangiogenic medications:
a. The tooth should be extracted in a traumatic manner.b. The tooth should be extracted as atraumatically as possible, and all sharp
bony edges should be smoothened.c. Sharp bony edges should be left intact, even if they traumatize the soft tissues
in the area.
9. If a dental infection is present in a patient receiving antiresorptive/ antiangiogenic medications:
a. It should be treated as soon as possible, as infection could be a trigger factor for MRONJ.
b. It should be left untreated, because any therapeutic manipulations in such patients could cause MRONJ.
10. A meticulous dental check-up should be performed on all patients planned to receive antiresorptive/ antiangiogenic medications, before initiation of such medication.
a. TRUEb. FALSE
11. After how many years of medication intake, does the risk of MRONJ increase inpatients on oral bisphosphonates?
a. 1 yearb. 2 yearsc. 4 years

13. Dental prophylaxis should be provided regularly on patients receiving antiangiogenic/antiresorptive medications.
a. TRUEb. FALSE
14. If a patient presents with established or suspected MRONJ:a. The general dentist should try to treat the MRONJ even if he/she does not
feel comfortable with such treatment.b. The general dentist should ignore the condition, as it will heal on its own.c. The general dentist should refer the patient to an oral and maxillofacial
surgeon or other specialist experienced on treatment of MRONJ.
15. Regardless of the MRONJ staging, loose bone sequestra:a. Should be left in place, because their removal could exacerbate the
lesion.b. Should be promptly removed, because they could create trauma to the
soft tissues.
16. The most well-known serological marker in patients at risk of developing MRONJ is:
a. Osteocalcin (OC)b. Parathyroid hormone (PTH)c. Bone-specific alkaline phosphatase (BAP)d. C-terminal telopeptide cross-link of type I collagen (CTX)
12. MRONJ can present at any time around a well-osseointegrated and functioningimplant and does not necessarily relate to the surgical procedure of implantplacement.
a. TRUEb. FALSE
End of Test