Embed Size (px)
Citation preview

IFNgIDO1STAT1GZMAGZMKCCR5
CXCL10CXCR3CXCR6CD2
CD3dIL2RA
HLA-DRAPRF1
0 2 4 60
2
4
6
815
20
25
0
100
200
300
0
100
200
300
400
500
0
100
200
300
400
500
0
100
200
300
0
200
400
600
800
1000
1200
0
200
400
600
SITC 2018
#10876
Abstract
Background
Background: Though efficacious, checkpoint inhibitor (CPI) monotherapy
fails to elicit response in the majority of patients. TNBC is one such cancer
type where CPI antibodies (pembrolizumab, avelumab, atezolizumab),
have demonstrated only a ~5-10% response rate, irrespective of PD-L1
expression. We are developing Imprime PGG (Imprime), a novel yeast
derived β-glucan PAMP in combination with pembrolizumab, to enhance
the benefit that TNBC patients derive from CPI-based therapy.
Methods: In this analysis, we present the serum and cellular IPD responses
elicited by Imprime and pembrolizumab in the peripheral blood of 12
TNBC subjects who previously failed front-line chemotherapy, enrolled as
part of a Phase 2 study (NCT02981303). Subjects received Imprime (4
mg/kg qw) + pembro IV (200 mg q3w) in 3 week cycles. Anti-beta glucan
antibodies (ABA), circulating immune complexes (CIC), complement
activation, cytokine production, gene expression changes, and phenotypic
changes on immune cells were evaluated.
Results: As Imprime is known to complex with serum IgG ABA, a drop in
the free ABA levels and a concomitant increase in the CIC was observed at
the end of infusion (EOI) of every Imprime dose. Interestingly, 11 of 12
subjects showed increased ABA levels between cycles 1 and 2, with peak
levels increasing ~1.5 to 35-fold over baseline. In line with this ABA
increase, peak levels in serum CIC levels (range ~3 to 22-fold) and
complement protein SC5b-9 (~1.4 to 41-fold) were also observed at cycle 2
EOI. In a subset of patients, a maximum increase of ~10-1000-fold in
several chemokines was detected at cycle 2 EOI. Gene expression analyses
of whole blood indicated peak activation of several genes at cycle 2
associated with activation of innate immune cells and T-cells. In 8 of 12
subjects, an increased frequency up to 11-fold in the CD16+ monocytes,
cells known for their enhanced cytotoxicity as well as M1-polarizing
functions, was observed between cycles 1 and 2. We also observed an
increase, up to 2-fold, in CD16+ inflammatory DC in 8 of 12 subjects. The
maximal increase (~4 to 20-fold) in newly proliferating (Ki67+), activated
CD8 T cells (PD-1+ CD38+ HLADR+) was observed at cycle 2 in 4 subjects.
Of all these immunological responses, robust cytokine production together
with an increased frequency of activated CD8 T cells, correspond with
objective tumor responses.
Conclusions: These data provide the first evidence in cancer patients that
Imprime can drive the critical IPD changes known to be associated with
efficacy in preclinical cancer models.
Figure 1. Imprime impacts multiple points of the anti-cancer immunity cycle
• Imprime PGG, a yeast-derived pharmaceutical-grade soluble 1,3/1,6 β-
glucan is being developed for the treatment of cancer in conjunction with
tumor targeting and immunomodulatory antibodies (Abs).
-Imprime has shown promising results in multiple Phase 2 clinical trials
in non-small cell lung cancer (NSCLC) and chronic lymphocytic leukemia
(CLL) with additional studies ongoing.
•β-glucans are conserved microbial structures found in the cell wall of
unicellular and multicellular pathogens. They are considered pathogen-
associated molecular patterns (PAMPs) recognized by the pattern
recognition receptors including Dectin-1 and Complement Receptor 3
(CR3). Imprime forms an immune complex with endogenous serum
immunoglobulin IgG anti-beta-glucan antibodies (ABA) before being
recognized by CR3 and FcgRIIA on innate immune cells.
All experiments funded by Biothera
Pharmaceuticals Inc. No external funding was
received to support the work.
Effective antigen presentation• Active, mature
dendritic cells• M1-state macrophages
T-Cell based anti-cancer immunity• CD8, CD4 T cell infiltration• PD-L1 + Tumor, myeloid cells• Adaptive immune signature
Sufficient antigen debris field
• Sufficiently foreign• Presentable
Proposed Mechanism: Imprime triggers a series of innate immune activation eventsthat culminate in enhanced T cell based anti-cancer immunity
Hypothesis: Imprime in combination with pembrolizumab will enhance sensitivityto checkpoint inhibitors (CPI) by stimulation of the patient’s innate andadaptive immune systems in those patients who have failed prior therapy (CPI-naive)
Repolarizes the immune microenvironment
Activates antigen presentationActivates tumor cell killing
Permissive immune microenvironment• M1>>> M2 polarized macrophages• Reduced/differentiated MDSCs
The Imprime Immune Complex
IgG ABA Complement opsoniniC3b
iC3b
Figure 3. Imprime administration resulted in drop of free IgG ABA concentrations and increase in CIC levels. Shown here
are serological changes in (A) IgG ABA and, (B) CIC levels tested at pre-dose, and ~EOI of Imprime and pembro for 3 cycles
using an ELISA method.
Figure 4. Imprime and pembrolizumab dosing resulted in several innate and adaptive immune activatingpharmacodynamic changes that generally peaked between cycle 1 and cycle 2. We explored peripheral blood changes at
pre-dose and EOI of Cycles 1, 2, 3, 4, 5, 6, and beyond. The peak IPD responses are observed between cycles 1 and 2.
(A) Maximum fold-increase in serum levels of free ABA, CIC, and complement-activation product SC5b-9 measured at cycle
2 EOI by ELISA, (B) Fold increase over C1 in cytokine levels measured at cycles 1-3 EOI by Luminex in a representative
subject (103102), and (C) Representative plot from a patient showing the appearance of CD16+ intermediate/ non-classical
monocytes (107107) and inflammatory DC (104104) in the peripheral whole blood at cycle 2 (pre-dose) as measured by flow
cytometry. Changes in the frequencies of CD16+ monocytes and inflammatory DC from cycle 1 to cycle 2 (pre-dose) in all 12
subjects are also shown, (D) A representative plot from a patient (109128) showing the appearance of of Ki67+ PD-1+
responding CD8 T cells in whole blood as measured by flow cytometry. The responding Ki67+ PD-1+ population is activated
(CD38+ HLA-DR+) and is largely contained within the memory CD8 T cells. Changes in the frequency of Ki67+ PD-1+ CD8 T cells
from cycle 1 to cycle 2 (pre-dose) in all 12 subjects are also shown.
Acknowledgements
Immunopharmacodynamic (IPD) responses of Imprime PGG combined with pembrolizumab in chemotherapy-resistant, metastatic triple negative breast cancer (TNBC) subjects in a Phase 2 trial: Analyses of stage 1 patients
Nadine R. Ottoson1, Adria B. Jonas1, Anissa SH Chan1, Xiaohong Qiu1, Blaine T. Rathmann1, Richard M. Walsh1, Ben Harrison1, Mike Danielson1, Kyle Michel1, Michaela Finley1, Mark Uhlik1, Jamie Lowe1, Paulette Mattson1, Michele Gargano1, Michael Chisamore2, Joanna Cox1, Bruno Osterwalder3, Jeremy R. Graff1, and Nandita Bose1
1Biothera Pharmaceuticals, Inc., Eagan MN, 55121. 2Merck & Co. Inc., Kenilworth, NJ. 3B.O. Consulting GmbH, Riehen, Switzerland
Fold
In
cre
ase
Ove
r P
re-d
ose
Cyc
le 1
Evidence of Imprime-ABA Immune Complex Formation In Vivo
Pre-dose EOI
Cycle 1 Cycle 2 Cycle 3
**p=0.004 **p=0.003 **p=0.0051
IgG
AB
A (µg
/mL)
Pre-dose EOI Pre-dose EOI
A. B.Cycle 1 Cycle 2 Cycle 3
*p=0.0218 ***p=0.0001 ***p=0.0008
Pre-dose EOI Pre-dose EOI Pre-dose EOI
CIC
(µg
Eq
/mL)
Peak Immunopharmacodynamic Responses Measured in Serum/Plasma and at Cellular Levels (cycle 2)
Fold
in
cre
ase
ove
r b
ase
lin
e
Figure 2. Study Schema
Peripheral Immunological Responses Associated with Clinical Response
B.
Fre
qu
en
cy o
f C
D1
6+
mo
no
Ki67+ PD-1+
A.
C.
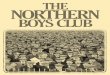
Figure 5. Association between peripheral immunological responses and objective clinical response. Shown here are trends
in association of some of the select immunological changes to the objective clinical responses, including (A) more robust
cytokine/chemokine profile regulating both innate and adaptive immunity observed in all the responders (B) T-cell
activation gene expression profile using RNA from whole blood, and (C) higher magnitude of increase in the frequency of
Ki67+ PD-1+ CD8 T cells in all the responders. Fold maximal change between C2 and C6 over pre-dose C1 is shown.
Results
Responder (confirmed)Responder (unconfirmed)
Summary•For the first time, this study provides evidence for Imprime-ABA immune complex formation and the
downstream peripheral innate and adaptive immune activation responses in cancer subjects.
•For the first time in TNBC patients, treatment with Imprime (in combination with Pembrolizumab)
elicits peripheral innate immune-activating immunopharmacodynamic changes including complement
activity, select chemokine production, and phenotypic activation of monocytes and DC. These
activities have been previously evident in pre-clinical efficacy models as well as healthy volunteers.
•The strong association between the clinical responses and the innate/adaptive immune responses are
suggestive of interplay between the therapeutic mechanisms of Imprime and pembrolizumab.
•The correlative work between the peripheral immunological responses and the tumor
microenvironmental changes are ongoing.
118102
103102
109128
107107
111101
104104
115107
109116
110130
112103
107113
Stable DiseaseProgressive Disease
*OR=overall response
Stage 1 = 12 pts
Imprime PGG 4 mg/kg QW
Pembro 200 mg Q3W
NO
YES
Repeat Stage 1 with
Imprime PGG 2
mg/kg QW
NO STOP
N = 41 TNBC patients
≤4 Gr 3/4 toxicities
in each tumor type
≥1 OR in TNBC*
Success: ≥5 OR
Stage 2 = 29 pts
Note: Subject 109112 was excluded from exploratory analyses due to discontinuation of treatment prior to C2
ABA CIC
SC5b-9
0
10
20
30
40
50
A.
C.
Cycle1 Cycle20
20
40
60
8017.8%
CD16+ DC14.9%
3.2%
Nonclassical
IntermediateCycle 1
Pre-dose
Cycle 2
Pre-dose
23.4%
5.5%
CD
16
29.3%
Monocytes Dendritic Cells
CD1cCD14
Monocytes Dendritic Cells
Cycle1 Cycle20
10
20
30
40F
req
ue
ncy
of
CD
16
+D
C
CYCLE 1 CYCLE 2 CYCLE 3
Cycle1 Cycle20
5
10
15
Fre
qu
en
cy o
f K
i67
+P
D-1
+
Cycle 6
pre-dose
D.
Ki67- PD-1-
Cycle 1
Pre-dose
Cycle 2
pre-dose
Ki6
7
PD-1
CD
27
CD45RA
Ki67+ PD-1+
CD
38
HLA-DR
CD8+ T cells
B.
Fre
qu
en
cy o
f C
D1
6+
mo
no