Embed Size (px)
Citation preview

Hand Therapy Review CourseWashington UniversitySt. Louis, MOApril 27‐29, 2018
The Brachial Plexus:
Innervation of the Upper Extremity
Lorna C. Kahn, PT, CHT
Spinal accessory nerve injuryMedian nerve injury
Upper trunk injuryUlnar neuropathy
Outline
• Anatomy of the nervous system
• Nerve injuries
• Nerve repair options
• Brachial plexus
• Spinal nerves: pathways, classic lesions, and compression sites
• Anatomy of the nervous system
• Nerve injuries
• Nerve repair options
• Brachial plexus
• Spinal nerves: pathways, classic lesions, and compression sites
Neuroanatomy
• Central Nervous System: inside brain and spinal cord
• Peripheral Nervous System: outside brain and spinal cord
• Connective Tissue: between the nerves-provides nutrition; prevents compression; allows lengthening; speeds conduction

• Unit structure of nervous system is the nerve cell or neuron
• Dendrites conduct impulses toward the cell body
• Axons conduct impulses away from the cell body
• Efferent (motor) fibers conduct away from CNS
• Afferent (sensory) fibers conduct toward the CNS
Peripheral Nerve Anatomy All peripheral nerve fibers have a sheath cell called a Schwann cell or neurolemma
Larger nerve fibers have a fatty (myelin) sheath in addition to the Schwann cell
Presence of myelin speeds conduction
Nodes of Ranvier: constrictions separating successive segments of myelin
Nerve impulses “leap” from node to node
Farther apart = faster conduction
Peripheral Nerve Anatomy: Connective Tissue
• Epineurium-binds fascicles into named nerve
• Perineurium-surrounds fascicles
• Endoneurium-surrounds the axon
• Connective tissue – Protection vs. compression,
traction
– Allows lengthening
Mixed Spinal Nerve
• Anatomy of the nervous system
• Nerve injuries
• Nerve repair options
• Brachial plexus
• Spinal nerves: pathways, classic
lesions, and compressions sites
Nerve Injury
• Agents of nerve injury are mechanical, thermal, chemical, or ischemic
• Motor loss results in venous/lymphatic stasis; muscle atrophy; muscle/joint fibrosis
• Sensory loss results in decreased functional use and increased risk for burn/pressure injury
• Sympathetic loss results in vasomotor, sudomotor, pilomotor, and trophic changes

sympathetic nerve changes with nerve injury
• Vasomotor: changes in skin temperature, color, edema, and cold intolerance
• Sudomotor: changes in sweat patterns (hypo-hidrosis in denervated areas; hyper-hidrosis with partial nerve injury)
• Pilomotor: absence of “goose flesh”
• Trophic: changes in skin texture; atrophy of finger pulps; nail changes; hair growth changes (hyper/hypotrichosis); slowed skin healing
VASOMOTOR CHANGES POST NERVE INJURY
SUDOMOTOR CHANGES POST NERVE INJURYPILOMOTOR CHANGES POST NERVE INJURY
TROPHIC CHANGES POST NERVE INJURY
• SOURCE: Callahan, Anne D. : SensibilityTesting: Clinical Methods Rehab of the Hand ,
ed2, 1984 The CV Mosby Co.
TROPHIC CHANGES POST NERVE INJURY

Connective Tissue
• In vulnerable areas of the body such as anatomic tunnels there are usually more fascicles in the nerves
• Fascicle arrangement more complex proximally
• Jabaley: protection from compression, tensile forces
• More fascicles means more epineurium to protect axons from friction or pressure Sunderland: 21-81% CT, greater % closer to joint
Connective Tissue
Greater number of fasculi: greater connective tissue protection: less deformation with mechanical stress
Connective Tissue
• Undulations of the nerves allow for more nerve gliding without tension “Spiral bands of Fontana” Dellon & Mackinnon: absent in area of compression
• Normal muscle tone helps prevent excessive traction to the nerve
Nerve Traction
• Axon
• Endoneurium
• Perineurium
• Epineurium
Undulation Stretched
Progressive Disruption
Double Crush SyndromeMacKinnon & Novak
• Axoplasmic flow is decreased in chronic compressive injuries – Distal to the compressive force, the nerve becomes
more sensitive to sub-clinical levels of entrapment• Double Crush
– 2 or more levels of compression occur along the same nerve
• Water hose analogy– Less compression required to create symptoms with an
existing compromise in nerve circulation
Observed in approximately 50% of TOS cases
Classification of Nerve Injury
Seddon Sunderland

Seddon’s Neuropraxia = Sunderland 1
A conduction block involving local demyelination
Prognosis is good to excellent
Axon remains intact; NO Wallerian degeneration
Nerve conduction preserved proximal and distal to
the lesion
Complete recovery within 4-12 weeks
“Saturday night palsy”
Seddon’s Axontomesis = Sunderland 2
Axons are damaged
endo/peri neurium are intact
+ Wallerian Degeneration distal to injury
no distal stimulation once WD occurs
typically complete recovery but timing is based on distance to end organ (inch per month)
+ advancing tinel
Seddon’s Axontomesis = Sunderland 3
Axons are damaged
Axons must regenerate but may “get lost”
endoneurium is NOT intact; scarred
perineurium is intact
+ Wallerian Degeneration distal to injury
no distal stimulation once WD occurs
incomplete recovery and timing is based on distance to end organ (inch per month)
+ advancing tinel
Seddon’s Axontomesis = Sunderland 4
Axons are damaged
No regeneration can occur through scar
Endo and perineurium are NOT intact
+ Wallerian Degeneration distal to injury
no distal stimulation once WD occurs; poor recovery
NO advancing tinel
Seddon’s Axontomesis = Sunderland 4
No advancing Tinel’s
Surgery required: resection of neuroma and graft or other procedure
Sequential EMG at 3 mo will confirm failure to improve

Seddon’s Neurotomesis = Sunderland 5
Complete transection of nerve
No advancing Tinel’s
More straight forward diagnostically; early surgical repair may lead to better outcome
summary of outcomes
Grade I: Recovers within 3 months
Grade II: Complete recovery at 1mm/day
Grade III: Incomplete recovery at 1mm/day
Grade IV: No recovery and requires surgery
Grade V: Requires surgery
“Sixth Degree"
Classification added by MacKinnon and Dellon
Combination of I-V degree fascicular injuries within same nerve
Variable recovery and prognosis
Treatment based on pattern and degree of injury
a challenge for the surgeon
33
Anatomy of the nervous system
Nerve injuries
Nerve repair options
Brachial plexus
Spinal nerves: pathways, classic lesions and compressions sites
Nerve repair options
1. direct repair
2. nerve graft:1. autograft= self donor
2. allograft=cadaveric tissue (acellularized matrix); ie Axogen
3. conduit= “bioartificial”
3. nerve transfer
4. (decompression occasionally used with grades 2+3)
Nerve Repair
Microscopic repair- typically epineurial
Grouped fascicular and fascicular: better alignment for fascicular match but extremely
time consuming and technically challenging• nervesurgery.wustl.edu

Nerve Repair/autografts
Potential donors and available lengths
○ Medial antebrachial cutaneous nerve(MABC): < 8cm
○ Sural nerve: up to 30cm
○ Posterior interosseous nerve: distal digital nerve < 2cm
Pros – non-immunogenic, bridge nerve gap
Cons - sensory loss, scarring, neuroma formation, second incision, limited supply, inferior to tension free primary repair
Nerve Repair/allografts
Cadaveric graft (ie: “Axogen”)
Frequently used in sensory repairs
Pros - readily accessible, unlimited supply, bridge nerve gap, avoids donor site morbidity,
Cons – potential side effects of host immunosuppression
Nerve Repair/conduits
biologic or synthetic “tube”
best for sensory repairs and gaps <3cm
Pros - Readily available, avoids donor site morbidity, bridges a nerve gap, barrier to scar tissue infiltration, may allow for accumulation of local neurotrophic factors
Cons - Variable outcomes, lack of scaffold and Schwann cells, limits its use to short nerve gaps
Nerve Repair/nerve transfer
recover motor or sensory function
“rob Peter to pay Paul”
nerve transfers allow a closer proximity of donor to recipient thereby decreasing distance and time for reinnervation and improving functional motor outcomes. (Fu SY, J Neuroscience 1995)
Nerve Repair/recovery
Nerve recovery after surgical repair in an uncomplicated case is
1-3 mm/day or an inch/month
faster proximally
Nerve Repair/post op care
protection after nerve repair 10 days of protection with orthosis following repair with NO tension 3+ weeks following repair under tension
Eur J Hand Surg 2012. A Comparison Between Complete Immobilisation and Protected Active Mobilisation in Sensory Nerve Recovery Following Isolated Nerve Injury Isolated digital nerve repair, n=46 Follow-up 18 mo No difference: RTW, cold intolerance, 2pd, temperature differentiation
prognostics for good result: distal injury age time of repair non smoker
Microsurgery. 2011 Jan;31(1):59-65. doi: 10.1002/micr.20820. Epub 2010 Dec 28. The effect of cigarette smoking on functional recovery followingperipheral nerve ischemia/reperfusion injury.Rinker B1, Fink BF, Barry NG, Fife JA, Milan ME, Stoker AR, Nelson PT

Order of Nerve Recovery; sensory
SENSORY RETURN
pain/temp----------------------
vibration 30 cps--------------
moving touch------------------
constant touch----------------
vibration 256 cps------------
touch localization------------
2 pt. discrimination----------
stereognosis------------------
TEST
sharp/dull, temp
tuning fork 30 cps
moving light touch
Semmes Weinstein
tuning fork 250 cps
touch localization
2 pt. discrimination
stereognosis
Evaluation of nerve recovery/ Motor r FunctionMMT EMG
Anatomy of the nervous system
Nerve injuries
Nerve repair options
Brachial plexus
Spinal nerves: pathways, classic lesions, and compression sites
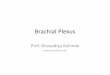
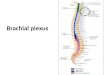
Brachial plexus
Roots
Trunks
Divisions
Cords
Nerves
Brachial plexus/ key surrounding structures

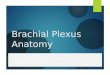
Brachial Plexus: Roots
Location: behind anterior scalene
muscle
Direct Branches Dorsal scapular nerve C5
○ Rhomboid muscles○ Levator scapulae muscle
Long thoracic nerve C5,6,7○ Serratus anterior muscle
Long thoracic nerve
Dorsal scapular nerve
C5
C6
C7
C8
T1
Brachial Plexus: Roots
Dermatome specific skin areas supplied by a specific spinal nerve,
regardless of the cutaneous nerve that supplies that area (relates to sensation)
Typically crosses 2 or more joints
Myotome:represents motor function (weakness) C5- muscles above elbow except triceps C6- elbow region C7- muscles in mid forearm C8, T1- muscles of hand
Brachial Plexus: Roots /test myotomes
C4 resist shoulder shrug
C5 resist shoulder abduction
C6 resist elbow flexion
C7 resist wrist flexion
C8 resist thumb extension
T1 finger abduction & adduction
Dermatomes vs. Cutaneous InnervationSegmental Testing C5
Motor: DeltoidReflex: Biceps
Sensation: Lateral Arm

Segmental Testing C6Motor: biceps, wrist extensorsReflex: brachioradialis
Sensation: thumb (index finger)
Segmental Testing C7Motor: triceps, Wrist Flexors, Finger Ext Reflex: tricepsSensation: index/middle finger
Segmental Testing C8Motor: finger flexorsReflex: noneSensation: ring and small fingers
Segmental Testing T1Motor: InterosseiReflex: None
Sensation: Medial proximal forearm
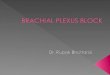
Brachial Plexus: Trunks
SUPRACLAVICULAR: between lateral border of anterior scalene and clavicle
Upper Trunk C5,6
Middle Trunk C7
Lower Trunk C8,T1
Direct branches:
Subclavian nerve C5,6○ Subclavius m.
Suprascapular nerve C5,6○ Supraspinatus muscle○ Infraspinatus muscle
3 TRUNKS
C5
C6
C7
C8
T1
Brachial Plexus: Trunks/ trunk lesion
symptoms-segmental upper trunk lesion: proximal pain paresthesias
in C5,6 dermatome Lower trunk lesion: distal pain, paresthesias
medial arm, hand

Brachial Plexus: Trunks/ trunk lesion
Upper Trunk
Erb’s Palsy: “waiter’s tip posture”—IR, elbow extension, wrist/finger flexion
Lower Trunk
Klumpke’s Palsy: may imitate ulnar nerve lesion
Cervical Rib Syndrome
Thoracic Outlet Syndrome
Brachial Plexus: Trunks/ trunk lesion
Hint: wasting of Supraspinatus, Infraspinatus
Which nerve innervates SS, IS?
Where does it come off BP?
Also wasting of Deltoid (and TM)
Which nerve innervates deltoid & teres minor?
Where does this nerve come off the BP?
Where is this lesion occurring?
Brachial Plexus/ trunks/supraclavicularThoracic Outlet Syndrome
NEUROGENIC SYMPTOMS (95%):
Motor: weakness
Sensory: paresthesiasand numbness
Autonomic: hyperhidrosis, discoloration, burning pain
VASCULAR SYMPTOMS (5%):
Venous: distal edema, dull pain with a nonspecific distribution, sensation of heaviness, cyanosis
Arterial: fatigue; ischemia; coldness of distal extremity; Raynaud’s
Brachial Plexus/ trunks/supraclavicularThoracic Outlet Syndrome
Potential compression sites:1. Interscalene triangle: between
anterior and middle scalenes
2. Costoclavicular space: between 1st rib and clavicle
3. Subcoracoid space:
retro pectoralis minor
Brachial Plexus/ trunks/supraclavicularThoracic Outlet Syndrome
Differential diagnoses Cervical Radiculopathy Cubital Tunnel Syndrome, Carpal
Tunnel Syndrome Shoulder disorders i.e. Impingement or
rotator cuff tear Pancoast Tumor Brachial Neuritis Complex regional pain syndrome
Brachial Plexus: Divisions
Location: behind clavicleCause of lesion: clavicle fx
Anterior division:innervates volar structures
Posterior division:innervates dorsal structures
Direct branches: Lateral anterior thoracic nerve
C5,6,7 Pectoralis
DIVISIONS

Brachial Plexus/ Cords
Location Below clavicle, behind
pectoralis minor Named relative to axillary artery Lesions at cord level do not
cause segmental symptoms Motor and sensory deficits
follow the distribution of the affected peripheral nerve
LATERAL POSTERIOR MEDIAL
CORDS
Anatomy of the nervous systemNerve injuriesNerve repair optionsBrachial plexusSpinal nerves: pathways, classic lesions, and compression sites
lateral cord: c5,6,7 upper/mid trunks, anterior division
Musculocutaneous nerve C5,6,7
Biceps
Brachialis (along with radial nerve)
Corocobrachialis
Lateral root of Median nerve C5,6,7
Motor to all median nerve muscles except the intrinsics
The Lateral Cord gives rise to 2 nerves
Lateral portion of Median Nerve:� PT, FCR, PL, FDS(weak)
MusculocutaneousNerve:� Coracobrachialis
� Biceps
� Brachialis
lateral cord: musculocutaneous nerve C5,6
LABC innervation
Arises from lateral cord
Innervates biceps, brachialis(with radial) and corocobrachialis
Sensory branches to lateral forearm
Functional deficitBiceps atrophyWeak elbow flex in supDecreased sensation along
radial and volar aspects of forearm
Dermatomes vs. Cutaneous Innervation

Posterior Cord: all trunks, posterior division Posterior Cord
Posterior Cord
Upper subscapular nerve C5,6 Subscapularis muscle
Lower subscapular nerve C5,6 Teres major muscle
Axillary nerve C5,6○ Deltoid muscle, teres minor
Thoracodorsal nerve C6,7,8 Latissimus dorsi muscle
Radial nerve C5,6,7,8,T1 Triceps, BR, Anconeus, ECRL/B, Supinator, ECU, EDC,
EDM, APL, EPL, EPB, EIP
Posterior Cord: 5 nerves
Radial Nerve:Triceps, BR, Anconeus, ECRL/B,Supinator, ECU, EDC, EDM, APL, EPL, EPB, EIPAxillary Nerve:
Deltoid Teres minor
Thoracodorsal Nerve: Lattisimus Dorsi
Upper/Lower Subscapular Nerve: SubscapularisTeres Major
Posterior Cord: Axillary nerve Posterior Cord: Axillary nerve C5,6
Originates in ventral aspect of subscapularis
Passes laterally toward inferior shoulder joint just inferior to humeral head
Through quadrangular space Medial: humerus Lateral: long head of triceps Superior: teres minor Inferior: teres major
Wraps horizontally around post surgical neck of humerus
Enters deltoid

Posterior Cord: Axillary nerve C5,6
Innervates: deltoid and teres min
Sensation: lateral aspect of the upper arm/deltoid tuberosity area
Functional loss-shoulder Abd/ER/elevation, numbness of lateral upper arm
Possible causes of lesions: Shoulder dislocation Humeral neck fracture Serum/vaccine induced Brachial neuritis
Posterior Cord: Axillary nerve C5,6/injury
deltoid atrophy
Posterior Cord:Radial Nerve
Posterior Cord: Radial Nerve
Emerges between long and medial heads of triceps
Crosses under lateral head of triceps, pierces lateral intermuscularseptum, enters anterior compartment of arm
Diverges anterior to radial head in forearm
Posterior Cord: Radial Nerve
Cutaneous branches:
Posterior cutaneous of arm
Lower lateral cutaneous of arm
Posterior cutaneous of forearm
Motor innervation in upper arm:
Triceps
Anconeus
BR
ECRL
Brachialis (musculocutaneous)
Posterior Cord: Radial Nerve Bifurcates at anterior radial head
Superficial branch:Superficial Radial Sensory N. Descends forearm just medial to BR Cutaneous supply to dorsoradial hand
Deep branch: Posterior InterosseousNerve Supinator ECRB EDC EDM ECU EPL, EPB, APL EIP

Dermatomes vs. Cutaneous InnervationSuperficial RADIAL NERVE Sensory Innervation
Posterior cord/RADIAL NERVEPotential Sites of Compression
Radial Groove of Humerus
Lateral Intermuscular Septum
Fibrous Band betweenBR and Brachialis/ECRB
Leash of Henry
Arcade of Frohse
Supinator
Distal BR
Medial Cord: lower trunk, anterior division
Medial Cord
Medial anterior thoracic nerve C8,T1 Pectoralis minor muscle Pectoralis major muscle
Medial cutaneous nerve of arm C8,T1
Medial cutaneous nerve of forearm C8,T1
Ulnar nerve C8,T1
Medial root of median nerve C8,T1 Median intrinsics and cutaneous in the hand
Medial Cord
The Medial Cord gives rise to
three motor nerves
Medial Ant. Thoracic N.: Pectoralis Major/ Minor
Ulnar Nerve:FCU, FDP ¾, AddP, FPB,Lumbrical ¾Interossei, ADM,ODM,FDM
Medial Portion of the Median N.: FDS, FDP 1,2, FPL, PQ, APB, FPB, OP, Lumbricals 1,2

Medial and Lateral Cords c5,6,7,8/median nerve
Lateral root of median nerve from lateral cord
Medial root of median nerve from medial cord
Medial and Lateral Cords c5,6,7,8/median n
Arises from medial andlateral cords
Descends arm in medial neurovascular bundle withulnar nerve and brachial artery
Moves laterally to enter cubitalfossa and passes deep tobicipital aponeurosis
Exits cubital fossa between 2 heads of PT and fibrous FDSarch in forearm
Median nerve in the forearm Medial and Lateral Cords c5,6,7,8/median n
AIN (anterior interosseous n) branches off median nerve at approximately level of PT or FDS arch
Median nerve continues in deep position down forearm between FDS and FDP
MPC (median palmar cutaneous) branches from median at distal 1/3 of FA.
Median curves laterally at proximal wrist to be volar to FDS to cross into hand under TCL
Medial and Lateral Cords c5,6,7,8,T1 median n Median motor innervation:
PT FCR PL FDS FPB (superficial head) APB OP Lumbricals 1 + 2
AIN motor innervation: FPL PQ FDP to IF (MF)
Medial and Lateral Cords c5,6,7,8, T1 median n

Medial Cord/ MEDIAN NERVE Sensory Innervation
AREA OF SENSORY CHANGE DUE TO COMPRESSION AT THE CARPAL TUNNEL
AREA OF SENSORY CHANGE DUE TO COMPRESSION PROXIMAL TO THE CARPAL TUNNEL
Median Palmar Cutaneous (superficial palmar nerve)supplies skin of lateral hand and base of thenar eminence
Cutaneous branch supplies skin of lateral thumb, 2 1/2 digits volarlyand distal to the DIP joints dorsally
Dermatomes vs. Cutaneous Innervation
Medial and Lateral Cords c5,6,7,8, T1 median n
Causes of injury:
Lacerations of the arm, forearm, wrist, or hand
Prolonged compression
Ulnar dislocation
Fracture of elbow joint or distal radius
Toxic or infectious neuritis
MEDIAN NERVE/ Potential Sites of Compression
Ligament of Struthers (1% of population)
Lacertus Fibrosis/BicipitalAponeurosis
Pronator Teres
Flexor DigitorumSuperficialis
Transverse Carpal Ligament
Medial Cord/ Ulnar Nerve Medial Cord/ Ulnar Nerve Medial Cord/ Ulnar Nerve
Descends arm in medial neurovascular bundle with median nerve, brachial artery
At distal 1/3 of arm, passes through medial intermuscular septum into posterior compartment
Descends supracondylar area in fascial groove, crosses elbow posteriorly in condylar groove
Enters FA passing between medial epicondyle and olecranon then deep to FCU

Medial Cord/ Ulnar Nerve
Passes through entire FA deep to FCU
DCU,UPC branch off ulnar nerve about distal third of FA
At FCU attachment to pisiform, ulnar nerve passes lateral to pisiform and medial to hook of hamate
Ulnar nerve branches superficial (cutaneous) and deep (motor)within this canal (Guyon’s)
Medial Cord c8, T1 Ulnar Nerve
Motor innervation in FA: FCU FDP to RF/SF
Motor innervation in hand: ADM FDM ODM Palmar and Dorsal Interossei
(8) Lumbricals 3 & 4 Deep head of FPB ADd Pollicis
Medial Cord c8, T1 Ulnar Nerve
Cutaneous branch supplies skin of ulnar 1 1/2 digits volarly and distal to the PIP joints dorsally
Palmar Cutaneous Ulnar supplies skin of ulnar volar palm
Dorsal Cutaneous Ulnar supplies the skin of the dorso-medial hand
Medial Cord c8, T1/ Ulnar Nerve
AREA OF SENSORY CHANGE FROM LESION OF THE ULNAR NERVE DISTAL TO THE DORSAL CUTANEOUS BRANCH
AREA OF SENSORY CHANGE FROM LESION OF THE ULNAR NERVE DISTAL TO PALMAR CUTANEOUS BRANCH
Dermatomes vs. Cutaneous Innervation Ulnar Nerve/ Potential Sites of Compression
Arcade of Struthers
Medial Intermuscular Septum
Subluxing Medial Head Triceps
Cubital Tunnel
Osbourne’s band
Flexor Carpi Ulnaris
Guyon’s Canal

109
Ulnar Neuropathy SIGNS Ulnar nerve/Duchenne Sign
• RF/SF MCP hyperextension due to unchecked pull of extrinsic extensors and absence/weakness of intrinsic extension (lumbricals and interossei)
• IP joints flexion due to unopposed extrinsic flexors• FDP weakness with high ulnar nerve palsy diminishes
this posture
Claw deformity of thering and small finger
Low ulnar nerve palsy
Ulnar nerve/Andre Thomas Sign
Exaggeration of the claw deformity The unconscious attempt straighten fingers by flexing the wrist which results in the tenodesis effect on the extensors and thereby the increases claw deformity.
Ulnar nerve/Crossed Finger Sign
Weakness of the interossei limiting ability of the middle finger to fully cross the index finger
Compare with uninvolved side
Ulnar nerve/Egawa Sign
MF unable to ab/adduct when flexed at IP joints (hook fist position)
IP joint flexion limits ability of extrinsic extensors to aid ab/adduction
Ulnar nerve/Froment Sign
Pt asked to pull/resist piece of paper held between thumb and radial index finger
*With loss/weakness of Adductor Pollicis, Flexor DigitorumProfundus overcompensates with thumb IP joint flexion

Ulnar nerve/Jeanne’s Sign
Thumb MCP hyperextension in addition to IP joint
flexion
Observed during evaluation of Adductor Pollicis (paper
pull/resist test or resisted lateral pinch)
Ulnar nerve/Wartenberg Sign
Small finger posturing in abduction
Inability/weakness limiting SF adduction to RF
Ulnar nerve/Masse Sign
Intrinsic muscle wasting causing flattening of the hypothenar eminence and metacarpal arch
case
17 yr old cello player with right thumb pain
7 year hx of pain
R hand holds the bow
Pain increases with length of play
ReferencesBell Krotoski JA. Sensibility Testing: History, Instrumentation, and Clinical
Procedures in Rehabilitation of the Hand and Upper Extremity, 6th Edition. Skirven, Osterman, Fedorczyk, Amadio. Elsevier/Mosby: Philadelphia, PA 2011.
Boyd KU, Nimigan AS & MacKinnon SE. Nerve Reconstruction in the Hand and Upper Extremity. Clin Plast Surg. 2011 Oct; 38(4):643-60.
Callahan A. Sensibility Assessment For Nerve Lesions-In-Continuity and Nerve Lacerations in Rehabilitation of the Hand and Upper Extremity, 5th Edition. Hunter, Mackin, Callahan. Mosby: St. Louis, MO 2002.
Fox IK & MacKinnon SE. Adult Peripheral Nerve Disorders- Nerve Entrapment, Repair, Transfer and Brachial Plexus Disorders. Plast Reconstr Surg 2011 May; 127(5).
Giuffre JL, Kakar S, Bishop AT, Spinner RJ & Shin AY. Current Concepts of the Treatment of Adult Brachial Plexus Injuries. JHS 2010; 35A:678-688.
Henry FP, Farkhad RI, O’Shaughnessy M & O’Sullivan ST. A Comparison Between Complete Immobilisation an Protected Active Mobilization in Sensory Nerve Recovery Following Isolated Digital Nerve Injury. J Hand Surg Eur 2012 Jun; 37(5):422-6.
120

References (cont) Hooper TL, Denton J, McGalliard MK, Brismee JM & Sizer PS. Thoracic Outlet Syndrome: a
controversial clinical condition. Part I: anatomy, and clinical examination/diagnosis. J Manual & Manipulative Therapy 2010 Jun; 18(2):74-83.
Kattan AE & Borschel GH. Anatomy of the Brachial Plexus. J Ped Rehab Med: An Interdisciplinary Approach 2011; 4:107-111.
Limthongthang R, Bachoura A, Songcharoen P & Osterman AL. Adult Brachial Plexus Injury Evaluation and Management. Orthop Clin N Am 2013; 44:591-603.
Novak CB & Mackinnon SE. Outcomes Following Conservative Management of Thoracic Outlet Syndrome. JHS 1995; 20(4):542-548.
Osterman AL & Lincoski C. Thoracic Outlet Syndrome in Rehabilitation of the Hand and Upper Extremity, 6th Edition. Skirven, Osterman, Fedorczyk, Amadio. Elsevier/Mosby: Philadelphia, PA 2011.
Pratt N. Anatomy of Nerve Entrapment Sites in the Upper Quarter. J Hand Ther 2005; 18:216-229.
Ray WZ, Mackinnon SE. Management of nerve gaps: Autografts, allografts, nerve transfers, and end-to-side neurorrhaphy. Experimental neurology. 2010;223(1):77-85. doi:10.1016/j.expneurol.2009.03.031.
Sheth RN & Campbell JN. Surgical Treatment of Thoracic Outlet Syndrome: A Randomized Trial Comparing Two Operations. J Neurosurg Spine 2005; 3(5):355-363.
121