Embed Size (px)
Citation preview
2017
Commissioning
guide:
Weight assessment and management
clinics (tier 3) Joint-sponsoring organisations: Associations of British Clinical Diabetologists
Association for Clinical Biochemistry & Laboratory Medicine
Association of Physicians Specialising in Obesity
Association for the Study of Obesity
British Association of Paediatric Surgeons
British Dietetic Association
British Psychological Society
Diabetes UK
Faculty of Public Health
Royal College of Anaesthetists
Royal College of General Practitioners
Royal College of Nursing
Royal College of Obstetrics and Gynaecology
Royal College of Paediatrics and Child Health
Royal College of Physicians (London)
Royal College of Pathologists
Royal College of Psychiatrists
Society for Endocrinology
Society for Obesity and Bariatric Anaesthesia
Weight Loss Surgery Info (WLSInfo)
Commissioning guide 2017 Weight assessment and management clinics
1
Plain English Summary
About two thirds of adults in the UK are overweight, 1 in 4 are obese, and 1 in 3 children aged 10-11 are
overweight or obese. Both conditions predispose to diseases such as type 2 diabetes, high blood pressure,
strokes, heart attacks, cancer, and general ill health. It is urgent that the National Health Service works out
ways to treat patients with severe diseases caused by their obesity. At present, most hospitals do not have
services for these patients. Even if clinics do exist, patients and GPs may not be aware of them and they
are not referred. This document describes the infrastructure needed to set up or commission Weight Assessment and
Management Clinics (referred to as Tier 3 Clinics) in the NHS in England. This includes which staff are
needed in the clinics – for instance specialist nurses and dietitians – to give the best advice to patients. As
the treatment of these patients is often very complex a wide range of professionals, including medical and
surgical doctors, nurses, psychologists and anaesthetists can also be involved. The document is sponsored by and represents the views of 22 professional organisations including 9
medical royal colleges that are directly concerned with patient care. We describe in detail which patients
might benefit from being referred for assessment for surgery (bariatric surgery) if they want to think about
this option. There is also a section on how to set up specialist children’s and adolescent Weight Assessment
and Management Clinics.
Sponsoring Organisation: British Obesity and Metabolic Surgery Society
Date of evidence search: July 2016
Date of publication: March 2017
Date of this Review: March 2017
Date of next Review: March 2020
NICE has accredited the process used by Surgical Speciality Associations and Royal College of Surgeons to produce its Commissioning guidance. Accreditation is valid for 5 years from September 2012. More information on accreditation can be viewed at www.nice.org.uk/accreditation
Commissioning guide 2017 Weight assessment and management clinics
2
Contents
Introduction................................................................................................................................................ 3
1. High Value Care Pathway for weight assessment and management clinics ................................................... 7
2 Procedures explorer for weight assessment and management clinics ....................................................... 18
3 Quality dashboard for weight assessment and management clinics ......................................................... 18
4 Levers for implementation ................................................................................................................... 19
4.1 Audit and peer review measures ....................................................................................................................... 19
4.2 Quality Specification/CQUIN (Commissioning for Quality and Innovation) ...................................................... 20
5 Directory ............................................................................................................................................ 21
5.1 Patient Information for weight assessment and management clinics .......................................................... 21
5.2 Clinician information for weight assessment and management clinics ............................................................ 22
5.3 NHS Evidence Case Studies for Weight Assessment and Management Clinics ................................................. 23
6 Benefits and risks of implementing this guide ........................................................................................ 23
7 Further information ............................................................................................................................. 24
7.1 Research recommendations.......................................................................................................................... 24
7.2 Other recommendations ............................................................................................................................... 25
7.3 Evidence base 27
7.4 Guide development group for weight assessment and management clinics ............................................... 34
7.5 Funding statement 35
7.6 Conflict of Interest Statement ........................................................................................................................... 36
7.7 Addendum 38
The Royal College of Surgeons of England, 35-43 Lincoln’s Inn Fields, London WC2A 3PE
Commissioning guide 2017 Weight assessment and management clinics
3
Introduction
This guidance and recommendations are the revision of existing guidance on Weight Assessment and Management Clinics (WAMCs) published in 2014 on the Royal College of Surgeons and British Obesity and Metabolic Surgery websites. The guidance was also published as a peer-reviewed publication in 2016 in the journal Obesity Surgery 1,
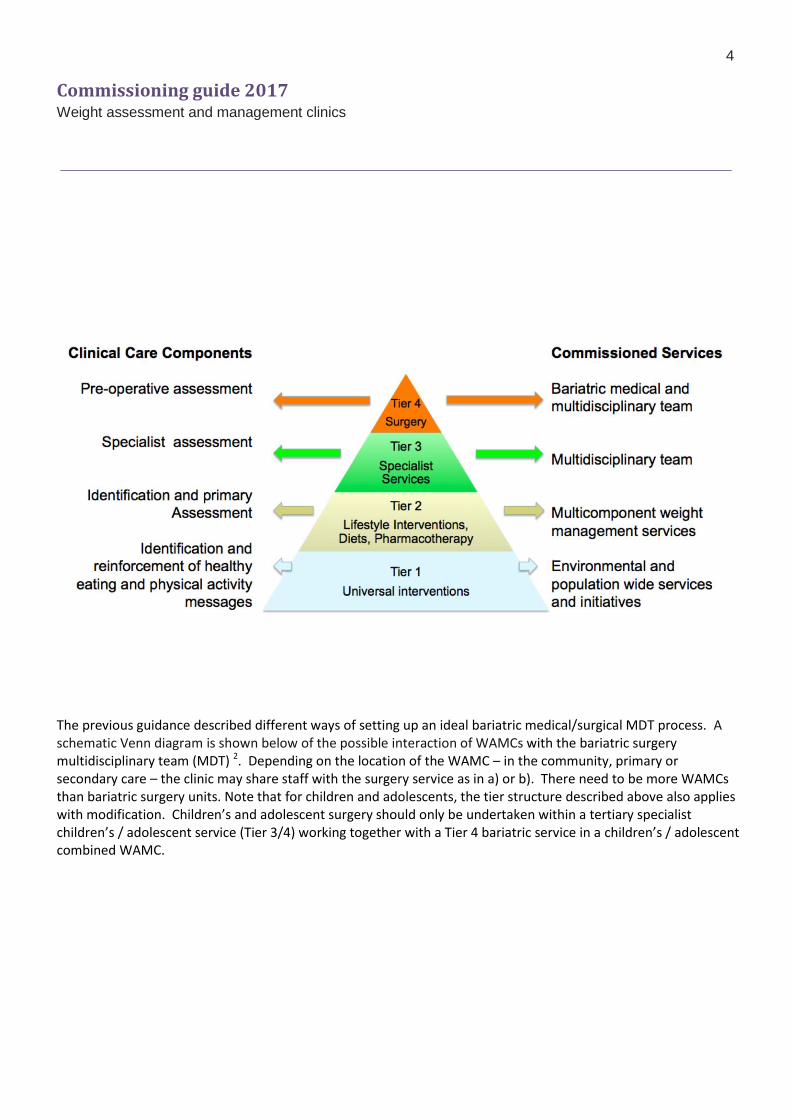
2. Commissioning responsibility for bariatric surgery transfers from specialised commissioning to Clinical Commissioning Groups (CCGs) from April 2017. Although the indicative levels of funding will also be transferred to CCGs there is a need for updated commissioning guidance for several reasons, including a) the availability of new clinical data that alter thresholds for surgical referral; and b) the Clinical Reference Group for Obesity Surgery commissioning was dissolved in April 2016. New guidance will therefore be pertinent to the commissioning process as CCGs (and Local Authorities) determine relative funding levels for the different tiers of the obesity pathway that they are responsible for. The Commissioning Policy (A05 Complex and Specialised Obesity Surgery Services of the NHS Commissioning Board April 2013) is still in current use and therefore this revision should be read in conjunction with that 3. The A05 policy describes the pathway of patients into the multidisciplinary (MDT) bariatric surgical service and later back to primary care as part of a shared care, chronic disease model of care. Despite the large amount of data supporting the use of bariatric surgery, the rate of operations in England fell between 2011-12 and 2014-15 by 31%, from 8,794 to 6,032. In comparison, provision of surgery in other home countries is even worse, with no surgery in N Ireland, and little in Scotland or Wales 4. It is possible that the lack of universal geographical coverage of WAMCs – referred to as Tier 3 weight management services in the English NHS – has contributed to this. It is also very possible that from April 2017 CCGs could disinvest in existing clinics, threatening bariatric surgery services further. In view of the current disinvestment in bariatric surgery and uncertainty surrounding the transfer arrangements to CCGs in 2017, the previous reports ‘Action on Obesity: comprehensive care for all’ of the Royal College of Physicians (Jan 2013) and ‘Measuring up. The medical profession’s prescription for the nation’s obesity crisis’ of the Academy of Medical Royal Colleges (Feb 2013) are still very relevant 5, 6. This updated guidance is therefore again intended for Tier 3 Specialist Services which provide the link between Tier 1/2 Environmental and population-wide services / Lifestyle interventions, and Tier 4 Multidisciplinary Specialist Bariatric Surgical Services, which is covered by NICE and SIGN Guidance and BOMSS standards for clinical services & guidance on commissioning 7-9. The tiers are defined below, as before, according to the terminology from the 2013 DoH Tier 2 guidance 10. In general Tiers 1 and 2 are funded by Local Authorities, and Tiers 3 and 4 by CCGs.
Commissioning guide 2017 Weight assessment and management clinics
4
The previous guidance described different ways of setting up an ideal bariatric medical/surgical MDT process. A schematic Venn diagram is shown below of the possible interaction of WAMCs with the bariatric surgery multidisciplinary team (MDT) 2. Depending on the location of the WAMC – in the community, primary or secondary care – the clinic may share staff with the surgery service as in a) or b). There need to be more WAMCs than bariatric surgery units. Note that for children and adolescents, the tier structure described above also applies with modification. Children’s and adolescent surgery should only be undertaken within a tertiary specialist children’s / adolescent service (Tier 3/4) working together with a Tier 4 bariatric service in a children’s / adolescent combined WAMC.

Commissioning guide 2017 Weight assessment and management clinics
5
The previous guidance also described the role of the referring GP, what should be achieved in the clinics and who should be referred for bariatric surgery. The guidance provided an organised structure and evidence-base for treatment, guidance for referral into and out of the Tier 3 service: either back to primary care or onto specialist or surgical assessment (Tier 4). This revision is also intended to update GPs on the latest evidence, for instance the new NICE Guidance CG189 re type 2 diabetes (2014), a joint statement from international diabetes organisations (2016) and a randomised controlled trial on brief interventions (2016) 7, 11, 12. In view of the scarcity of references revealed by the previous systematic review of the literature a different search question was used for the revision. The main research question was ‘what evidence exists for what should happen in / commissioning of: primary or secondary care weight assessment and management clinics in patients needing specialist care for severe and complex obesity?’. Five hundred and fifty-one references from 2011-2016 were screened systematically by the Guidance Development Group (GDG) and 80 were considered further, with 50 included in the final guidance. As before, the GDG added relevant new evidence when this was missed from the systematic review. Wherever possible meta-analyses, systematic reviews or Randomised Controlled Trial evidence is presented. Observational trial data have also been included where the panel considered that the findings from several studies were consistent and effect sizes large 2. Many people eligible for bariatric surgery may choose not to have it, but still require assessment and discussion about all treatment options and this would require a review at a specialised clinic 2. The clinic could then share a long term treatment plan with the GP. However, it is hoped that in view of the new recommendations relating to

Commissioning guide 2017 Weight assessment and management clinics
6
people with obesity and diabetes GPs will now refer such patients more freely to Tier 3/4 services for a bariatric surgical assessment. There is no evidence base for how long a patient being assessed for surgery should spend in a Tier 3 clinic 7. As before, and contrary to the stipulation in the A05 Policy, patients need not spend a prolonged time in Tier 3 7. Equally, the Tier 3 clinic is not only for assessing patients for surgery. The clinics should also offer specialist diets, pharmacotherapy and psychological treatment. Patients who have persisting needs would be referred back to primary care after assessment, with a new management plan. For such complex patients this process of evaluation and assessment may typically take a period of months. During this time clinically meaningful benefit may be achieved without the need or patient’s wish for referral for surgery. In view of NICE CG189 and the new statement on diabetes recommendations it is important to avoid undue delays in referral for surgery such as repeating failed prior interventions inappropriately due to the high likelihood of recidivism with weight regain and yo-yo dieting 7, 11. This is particularly relevant to patients with BMI > 50 kg/m2 for whom surgery is considered the next option instead of repeating failed lifestyle interventions a. Patients fulfilling the BMI thresholds for surgery ‘should be eligible’ (evidence level 1, grade A recommendation) for a procedure and part of the clinic’s role should be to facilitate this appropriately 13-22. Section 7.7 has a table of the GRADE system of recommendation. Thus overall the pathway is for primary care services that include community-based interventions referring into a specialist multi-disciplinary bariatric service which includes a bariatric physician (the Weight Assessment and Management Service). A proportion of patients would then be considered for bariatric surgery, with the whole team also being involved in the peri-operative care, usually as part of the same team if the surgery service is located in the same hospital. After discharge from the surgical service patients would be managed in a chronic disease model of shared care 5, 23. In this revision the GDG found no evidence to change its view that as the available literature did not distinguish between assessment clinics that either did, or did not contain surgeons (in addition to the rest of the MDT) the organisational recommendations made previously continue to describe overall best practice, avoiding subdividing what should be done in each clinic if the services are run separately. The main changes now are that infrastructure guidance and pathways for assessment of children and adolescents, and guidance for anaesthetic assessment and pathways are added. The guidance also provides updated tools for measuring equity of access into the clinics and referral onwards for surgery. Ample evidence of cost effectiveness already exists for bariatric surgery and NICE has updated its referral guidelines 7. CCGs should be reassured that set-up costs of Tier 3 clinics would be offset by potential savings from reduced medication costs, consultation costs and hospital visits in those having bariatric surgery. CCGs considering disinvesting in Tier 3 or Tier 4 services should also consider the existing potential overlap and sharing of staff between diabetes clinics (with diabetologists/endocrinologists usually the predominant group of bariatric physicians), sleep medicine, dietetics/nutrition, psychology, psychiatry, and physical therapy for instance which would mitigate against new set-up costs.
a Other groups of patients needing expeditious decision-making include severely obese patients needing renal transplants or
presenting to gynaecologists with pelvic cancer.
Commissioning guide 2017 Weight assessment and management clinics
7
Email: [email protected] www.bomss.org.uk
1. High Value Care Pathway for weight assessment and management clinics b
Guidance for General Practitioners (GPs):
Use appropriate opportunities to record current weight and height and calculate body mass index (BMI) to identify overweight and obese patients, including in chronic disease management, opportunistic case finding and routine health checks 12, 24-31.
Discuss with patients with overweight or obesity their understanding of the likely resulting health problems, assess individual health risks and engage with them in a partnership to modify the risks as part of a holistic approach that includes their emotional wellbeing 12
Encourage training for doctors and practice nurses so that they can provide support for patients with overweight and obesity, such as motivational interviewing 32-34
Consider offering patients with overweight or obesity identified as in the pre-diabetes risk group (HBA1c measurement 42-47 mmol/mol) referral to the NHS national diabetes prevention programme if clinically appropriate
Provide a set of scales capable of weighing up to 200kg in every surgery, and offer to refer patients over this weight to a service capable of weighing and monitoring them
Discuss with patients their previous attempts at weight loss and encourage those who have never successfully dieted to participate in a community or commercial Tier 2 weight management plan and share information about national and local lifestyle and behaviour change support c 7, 35, 36
Carefully assess patient engagement with the process before any decision is made about referral to the weight assessment and management clinic 7 26
Recognise patients with a long history of cyclical weight loss and regain (yo-yo dieting) and make a direct referral to a weight assessment and management clinic without requiring further Tier 2 programme management as a qualifying threshold 26.
b In the common Commissioning Guidance specification high value care pathway implies a benefit/cost ratio to providing the
service i.e. high Quality Adjusted Life Year (QALY) value. c Eg The Public Health England ‘One you’ initiative https://www.gov.uk/government/news/phe-launches-one-you .
Commissioning guide 2017 Weight assessment and management clinics
8
Discuss the benefits of weight maintenance if patients are not yet ready to engage with a programme, and encourage them to return at any point if they decide they need help 7, 37
Refer children / adolescents with overweight (BMI > 91st. centile) or obesity (BMI > 98th. centile) to community Tier 2 children's programmes or to specialist children’s / adolescent Weight Assessment and Management Clinics d 7
For GPs discussing with patients with diabetes whether to refer to the Weight Assessment and Management Clinic: e f g
Consider that effective care of overweight and obesity is integral to good diabetes care. Offer weight management to these patients, and refer them appropriately within local services 7, 11, 30. Options for this include:
o Multidisciplinary locally-organised and commissioned services o Management within a diabetes service o Weight Assessment and Management Clinics (Tier 3 obesity services) combining diet, exercise and
healthy nutrition advice aiming at realistic weight reduction goals. Services could be administered on a 1:1 basis or as a structured individual or group programme within a community, primary or secondary care setting
o Bariatric surgery
Expect the doses of hypoglycaemic medications to reduce with weight loss, especially with more restrictive diets that can produce rapid weight loss
Where possible use weight-neutral and/or weight-loss associated hypoglycaemic medications 38-40
Consider appropriate anti-obesity pharmacotherapy according to availability and relevant guidance. While obesity medications may lead to improved glycaemic control, understand that their indication is for weight loss and not glycaemic control 41-45
Refer patients with type 2 diabetes for an assessment for bariatric surgery as long as they are receiving or will receive assessment in a specialist weight management service before referral to a surgical team: 4, 7, 11,
46
o Offer an expedited assessment for people with a BMI ≥ 35 kg/m2 with onset of type 2 diabetes in past 10 years
o Consider an assessment for people with a BMI of 30-34.9 kg/m2 with onset of type 2 diabetes
d The BMI thresholds are based upon NICE guidelines CG189 and expert consensus. Note that for severely obese adolescents
aged ≥ 15 years , adult BMI thresholds can be used as an approximate guide to referral for obesity (BMI ≥ 30kg/m2) and
eligibility for bariatric surgery (BMI 35kg/m2
with significant comorbidity). e The BMI thresholds for surgery were chosen to reflect the quoted literature.
f If a patient is already being treated in secondary care it should be accepted practice to refer to the Weight Assessment and Management Clinic directly if the patient fulfils the criteria. g Diabetes here refers to type 2 diabetes only.

Commissioning guide 2017 Weight assessment and management clinics
9
within 10 years o Consider an assessment for people of Asian origin with onset of type 2 diabetes at a BMI threshold
reduced by 2.5 kg/m2 o Recommend bariatric surgery to patients with a BMI of ≥ 40 kg/m2 or BMI 35.0–39.9kg/m2 when
hyperglycemia is inadequately controlled by lifestyle and optimal medical therapy
Refer children / adolescents with type 2 diabetes to specialist children’s / adolescent diabetes services h
For GPs discussing with adult patients whether to refer to the Weight Assessment and Management Clinic: i j
Consider referring adults with a BMI of 40 or ≥ 35 kg/m2 and other obesity-related comorbidity eg hypertension, obstructive sleep apnoea (OSA), benign intracranial hypertension, functional disability, infertility and depression if specialist advice is needed regarding overall patient management 7, 47
Consider referring patients who have been refused elective (non-bariatric) surgery due to high BMI
Consider that bariatric surgery is the option of choice for adults with BMI >50 when other interventions have not been effective 48
Occasionally patients may be referred whose BMI is below these thresholds, if they have exceeded the thresholds in the past; this may include patients who have already had bariatric surgery presenting with a problem such as weight regain or nutritional deficiency or where revisional surgery might be considered
Consider mental health and psychological issues, and refer patients who have complex issues to a service with appropriate expertise 49
For GPs discussing with children / adolescents and those who care for them whether to refer to a Weight Assessment and Management clinic: 50, 51
Refer those with BMI > 98th. centile and: k o Known comorbidities o Potential red flags for possible secondary causes of obesity, including short stature for parents,
kinky red hair and dysmorphisms o Strong family history of cardiovascular disease or type 2 diabetes o Syndromic obesity if not already under specialist care
Refer those with more extreme obesity, regardless of other factors, generally regarded as BMI ≥ 99.86th. centile 52
h Bariatric surgery is only appropriate through specialist referral.
i The BMI thresholds for surgery were chosen as the quoted literature predominantly refers to patients in these groups. j If patients are already being treated in secondary care it should be accepted practice to refer to the Weight Assessment and Management Clinic directly if the patient fulfils the criteria. k See also later section ‘In the children’s / adolescent Weight Assessment and Management Clinic’.
Commissioning guide 2017 Weight assessment and management clinics
10
The comorbidities of obesity in children and adolescents are largely similar to those in adults, although a range of orthopaedic conditions related to the impact of obesity on growth also occur
o Note that assessment of hypertension, dyslipidaemia and other metabolic comorbidities must be undertaken using age- and sex-appropriate centiles and is therefore unlikely to be undertaken in primary care
o Note that psychological consequences of obesity can present in different ways to adults, and include school refusal and bullying
In the Adult Weight Assessment and Management Clinic:
Organisational recommendations: o The multidisciplinary team (MDT) contains at least a bariatric physician, a dietitian, a specialist
nurse, a clinical psychologist and a liaison psychiatry professional, and a physical therapist l 2, 5, 53, 54
o Ensure adaptations to assessment and interventions are accessible to people with learning disabilities. Adaptations including the use of simple language and individual rather than group sessions can assist comprehension and enable these patients to access weight loss services 7, 30, 55,
56
The BMI is confirmed and the trend in BMI is assessed
A dietary and nutritional assessment is taken to ascertain the patient’s diet and its nutritional adequacy, patient feelings and expectations about potential outcomes and willingness to consider treatment options. Lifestyle advice and education should be provided, including support to stop smoking, so that patients have appropriate understanding of the relationship between eating habits and weight, aiming to: 53, 57
o Improve understanding of necessary changes in eating habits to improve health, and identify risk factors and vulnerabilities so that interventions can be planned to address and improve them
Encourage evidence based weight loss and weight loss maintenance programmes that might contain
structured reduced energy prescription, eating plans, meal replacements and Very Low Energy Diets
Consider screening for rare hormonal or genetic causes for weight gain if there is clinical suspicion, eg very early childhood onset, syndromic or unusual phenotype 58
l No literature was identified that distinguished between care provided by the bariatric physician or by the bariatric surgeon, or regarding the order in which they were seen by the different specialists. See the figure in the introduction for ways in which the various teams can interact. Also the panel recognised there is no literature to identify which professionals are best placed to provide mental health interventions in weight management, and further research is required (section 7.1, page 24). For the purpose of the guidance ‘liaison psychiatry professional’ may include a psychiatrist and a mental health-trained nurse with specialist expertise in weight management. The panel recommends that the ideal service has both a clinical psychologist and a liaison psychiatry professional; however it recognises that this is aspirational and there needs to be local flexibility in commissioning as services develop. Liaison psychiatry refers to a sub-specialty multidisciplinary team that provides an interface between physical and mental health for patients in secondary care. The panel recognised that close working relationships need to be established between the groups described and community mental health teams where available.
Commissioning guide 2017 Weight assessment and management clinics
11
Possible undiagnosed obesity-related diseases are considered, screened for and where appropriate investigated, in particular type 2 diabetes, hypertension, obstructive sleep apnoea (OSA), heart failure, atrial fibrillation, chronic kidney disease, non-alcoholic fatty liver disease, idiopathic intracranial hypertension and depression as well as diseases with markedly increased prevalence such as colon or endometrial cancer
Identified risks are optimised so that those referred for surgery are as fit as possible
o Input from anaesthetists specialising in bariatric care may be valuable to determine peri-operative
risk in complex cases or patients with a history of problems with anaesthesia, to ensure they understand potential risks
o Patients who require non-bariatric surgery but are deemed too obese or unfit and who meet the BMI threshold for bariatric surgery should be referred for a definitive specialist anaesthetic opinion at a bariatric centre or the referral centre for specific advice beforehand
o Cardiologists and respiratory physicians could also be involved by separate referral if patients need
super-specialist care 13, 59
Patients are investigated for vitamin and micronutrient status, and deficiencies corrected, to include recognition of diets deficient in protein in those being referred for bariatric surgery 13, 59
Given the high prevalence of psychiatric comorbidity, patients are assessed for psychological and lifestyle
issues which may interfere with engagement and weight management in the longer term, as well as to provide recommendations to enhance motivation 2, 53
Although NICE estimates that about 80% patients are suitable for bariatric surgery, assessment must identify: 4, 30, 49, 60-65
o Patients with unrealistic expectations of the impact of surgery on weight loss and life change, since these can have a negative impact on psychological health if they are not met 66, 67
o Patients for whom surgery may be inappropriate, eg significant cognitive impairment such as severe learning disability, active uncontrolled psychosis, severe personality disorder
o Patients not presently suitable for surgery, eg untreated or unstable mental health presentation, active alcohol or substance misuse (including cannabis use), active eating disorder such as binge eating without psychological treatment, bulimia nervosa, self-harm and suicidal behaviours in past 12 months, current non-engagement with treatment and recent significant life event, bereavement or relationship breakdown 62, 63, 65, 68, 69
o Patients with weight gain associated with psychotropic medications 70
o Acute and chronic stressors that may affect self-care and engagement with postoperative dietary
and physical activity guidelines 49
o Past stressors including childhood and adult adversity (sexual and physical assault, emotional
neglect) that have been associated with the development of obesity and weight regain 71, 72
o Patients who may after surgery need specific attention and additional long term support or who may be at risk of self-harm
Make recommendations for treatment and offer support within the Weight Assessment and Management
Clinic or refer onward as appropriate before reassessing for the suitability of surgery
Commissioning guide 2017 Weight assessment and management clinics
12
A traffic light system may be useful to identify patients not currently suitable for surgery or who may be
suitable but deemed at higher risk and requiring psychological treatment before being considered 1, 2
o For these patients and for those not wishing surgery the clinic should provide or signpost referral pathways to evidence-based psychological treatments including Cognitive Behavioural Therapy (for binge eating disorder), Mindfulness and Acceptance based interventions 73-75
Consider scores such as the Edmonton Obesity Staging System as a means of assessing individual risk from
obesity-related disease 76
For patients with type 2 diabetes: 46, 77 o The team strives for satisfactory glycaemic control before surgery (HbA1c < 69 mmol/mol) but
inability to achieve this within a reasonable period of time should not be a bar to or delay referral for bariatric surgery
o Macro- and micro-vascular risk is assessed before referral for surgery, including consideration of retinal screening for patients with established retinopathy
o The usual diabetes carer (and GP if not the primary carer) is kept informed of progress through the assessment and treatment pathway
Give appropriate physical activity advice and consider individually tailored programmes to promote health
gains and general fitness 59, 78, 79
Consider appropriate anti-obesity pharmacotherapy according to availability and relevant guidance 41
Give smoking cessation advice and make an appropriate referral for a long term solution 13, 77
In view of most patients having multiple previous episodes of cyclical weight loss/regain, and that absolute weight loss per cycle may be modest, patients should not be made to achieve a set weight loss target before referral to the bariatric surgery service as a means of ‘qualifying’ for surgery; instead they should expect to lose weight during a short, supervised diet in order to make surgery technically feasible, and demonstrate engagement with the process 2, 80
Encourage patients to attend education sessions usually arranged by the bariatric surgery team if referral
for surgery is being considered 81
The MDT meets physically or audio-visually to discuss all patients at least once before deciding on referral back to the GP or for bariatric surgery 53
Provide patient information leaflets written in plain English and other languages as appropriate for all
proposed interventions 53
In the Children’s / Adolescent Weight Assessment and Management Clinic: 82-90
Commissioning guide 2017 Weight assessment and management clinics
13
Organisational recommendations: m
o The MDT contains at least a paediatrician with special interest in obesity, a children’s / adolescent dietitian, a specialist children’s or adolescent nurse, a clinical psychologist with expertise in paediatrics and with access to a social worker, a physical therapist and a liaison child and adolescent psychiatrist 91
o All MDT members should have appropriate training in child safeguarding, have undergone appropriate disclosure and barring assessments ('police checks') and had training in communication skills with children and young people
o At least one Tier 3 specialist children’s / adolescent WAMC should be established in all regional centres serving a population of approximately 1 million children and adolescents, suggesting a need for at least 10-15 such centres across the UK
o Bariatric surgery centres should comprise a children’s / adolescent WAMC working in very close liaison with a bariatric surgery service in the same or an associated hospital. All aspects of the service apart from the surgery itself should primarily be managed from paediatrics, allowing for child-centred care and input from a wider range of paediatric professionals where necessary
o Surgery should be undertaken by an adult bariatric surgeon with experience working with adolescents or alternatively by the combination of a paediatric surgeon with bariatric experience working with an adult bariatric surgeon
o Given the size and population of children and adolescents in the UK (approximately 14 million), and the small number of operations undertaken each year, there should be a maximum of 5 surgery centres including one in Scotland n
Care in the clinic in terms of BMI assessment, dietetic and lifestyle assessments, encouragement of evidence-based weight loss, screening for obesity-related conditions and assessment of surgical risks, is the same as for adults, with the following exceptions:
o A minimum of 6 months comprehensive assessment and management is appropriate for
adolescents before referral for bariatric surgery, which should be considered only when all other appropriate options have been tried o
o Paediatric professionals with knowledge of age- and sex- norms for investigations and trained in working with children and adolescents undertake the assessments and screening
o Very low energy diets are unlikely to be appropriate for adolescents who have not reached full physiological maturity
m
There was very little literature that described the staffing infrastructure of these clinics, or how many there should be for a given population, or how many there should be nationally. There was also little information on how patient care should transfer to adult services in due course. As for adult clinics there was no literature that described which professionals are best placed to provide mental health interventions in children’s / adolescent obesity. n The most recent data suggest that approximately 30 bariatric procedures were undertaken on 13-19 year olds in the NHS in
2009, and the NBSR data suggest there were at least 62 operations in 2011-13 on 18 year olds or younger. Centres should do a minimum of 10 procedures per year to allow the team to develop and maintain appropriate expertise and develop critical mass for research to improve outcomes. o NICE CG 189 states ‘consider referral to an appropriate specialist for children who are overweight or obese and have
significant comorbidities or complex needs (for example, learning disabilities or other additional support needs’.
Commissioning guide 2017 Weight assessment and management clinics
14
o A mental health professional with expertise in children and adolescents needs to do a more detailed psychological and social assessment, taking into account the developmental age and capacity to consent, and the support from the family. This will establish whether adolescents have a Child Protection Plan or are a registered Child in Need or have a Statement of Special Educational Need or Education, Health and Care Plan. An assessment from a social worker should be considered when there are concerns about capacity or about the family's ability to provide support
o A history of self-harm is common in adolescents and should not be considered exclusionary in the same way as for adults. Self-harm may represent significant psychological distress as in adults, and also more transient developmental issues
o Obesity staging or scoring systems are unlikely to be appropriate for adolescents o Adolescents are unlikely to have had multiple previous episodes of cyclical weight loss and regain
as in adults. It is appropriate for adolescents to be asked to cease weight gain for a period before surgery (eg 6 months). They should expect to lose weight during a short supervised diet immediately preoperatively to make surgery more feasible and demonstrate engagement, as in adults
o Provide information leaflets on interventions tailored to children and young people and those who care for them
Formulate a clear pathway for handing on children’s / adolescent patients to adult WAMCs at age 18-20 years:
o Follow transition good practice 92 o Tell adolescents and those who care for them of the need for this when they are 14+ years o Transition occurs around the time of completing secondary school (18/19 years) and when young
people have the skills to cope in an adult clinic o The specialist nurse is likely to be the appropriate professional to help ensure a smooth transition;
good communication between the children’s / adolescent and the receiving adult WAMCs is essential
o Consideration should be given to running a joint adolescent and young adult WAMC, potentially up to age 25 years, as many of the issues for young adults are similar to those for adolescents 93
Patients, including children / adolescents, wanting bariatric surgery should be referred if the Weight Assessment and Management Clinics are satisfied that: p
They are adequately engaged with the team, fully understand the surgery, are well-informed and motivated and have realistic expectations 2, 94, 95
All management options have been put to the patient including the characteristics of the various surgical
procedures available and the risks and side effects
They are medically optimised
p The clinic should also be able to refer patients to the bariatric surgery team for ongoing treatment if they have had previous
bariatric surgery elsewhere, or where a surgical complication or revisional surgery is being considered; those patients already known to the bariatric team should also be able to be referred back to the medical clinic in a two-way process

Commissioning guide 2017 Weight assessment and management clinics
15
There is no medical, surgical, anaesthetic, nutritional, psychological, psychiatric or social contraindication
They understand the importance of complying with nutritional requirements before and after surgery and recognise the need for life-long follow up 13
Patients, including children / adolescents, are referred back to the GP when:
They do not engage with the team, for instance if resistant to recommended health and lifestyle changes or repeatedly fail to attend appointments
Obesity-related diseases have been addressed and patients and teams agree that ongoing management can now appropriately be provided by the GP and –
They do not want to be considered or appear inappropriate for bariatric surgery assessment
Patients may remain within the Weight Assessment and Management Clinic if:
They have complex weight-related comorbidity and the MDT agrees to keep them under review on a shared care arrangement with the GP, for instance for early supervision of a Very Low Energy Diet or specific more intensive programme
Pharmacological treatment requires initiation and/or supervision by a specialist
At the point of discharge after surgery the bariatric unit will: q
Provide patients with clear written information on the importance of and reasons for long term follow up, to include advice about what to do if a patient becomes pregnant 96
Ensure that patients are referred to their GPs with an appropriate shared care agreement with a named Tier 3/specialist Weight Assessment and Management Clinic 7, 23, 49
Provide the GP with a discharge letter to include the operation details, nutritional supplements prescribed and details of the necessary long-term supplementation, and detailed guidance on the annual review requirements 23
Consider including the RCGP Top Ten Tips for the management of patients after bariatric surgery in primary care with each discharge letter, or a weblink to this guidance 33
In the period of surgical aftercare the bariatric unit will: r
q This section, while not within the remit of the Weight Assessment And Management Clinic, constitutes best practice for the
bariatric surgical unit r This section is existing guidance for bariatric surgical units
3, 96, 99.
Commissioning guide 2017 Weight assessment and management clinics
16
Follow up patients at regular intervals for a minimum of 2 years s o To include appropriate access to healthcare professionals eg the surgeon, dietitian, specialist nurse,
clinical psychologist/psychiatrist and bariatric physician, ensuring that dietitians have ready access to all MDT members if there are any concerns 7, 23, 97
o Recognising that psychosocial factors affecting adherence to the recommended postoperative dietary and lifestyle regimen may have significant impact on postoperative outcomes 60
Peri-operatively and in the period of surgical aftercare bariatric physicians and surgeons liaise closely with GPs to: 23
Ensure that diabetes management remains optimized 13 o Arrange for patients and GPs to receive a care plan allowing for reduction in hypoglycaemic
medications (as well as other medications e.g. for hypertension) promptly after discharge from hospital
Consider further retinal screening for patients with established retinopathy
Recognise and manage the development of unwanted consequences of bariatric surgery such as post-
prandial hypoglycaemia 98
Ensure that medications for other obesity-related and non-obesity-related diseases are assessed regularly and adjusted eg blood pressure and epilepsy; GPs may best be placed to supervise these with the support of the medical and surgical MDTs 13, 99
Supervise long term assessment of nutritional and trace mineral status and dietary replacement according
to published recommendations, with the help of the dietitian 13, 99
Ensure that patients on treatment for OSA are reviewed appropriately by a sleep clinic to ensure appropriate adjustment or even discontinuation of assisted ventilation
Identify issues that may require referral back to the surgical team and establish local protocols / ‘red flags’
for urgent re-referral of patients with surgical or nutritional complications
Support the patient’s mental health and psychosocial needs as identified before surgery including relapse of existing conditions and the emergence of new psychological disorders in patients without a history
o Accepting that psychological risk factors eg disturbed eating behaviour, binge eating, depression
can lead to an early weight plateau and weight regain 63, 64, 65, 70, 100
Identify patients who become vulnerable after surgery by developing depressive illness, risk of self-harm and suicide, significant eating disturbance or significant body image disturbance
s Note - the surgical aftercare period in the Commissioning Policy A05 is 2 years. The period chosen in NICE CG189 is also 2
years (chosen to fit with the AO5 Policy) 3.
Commissioning guide 2017 Weight assessment and management clinics
17
Identify post-operative alcohol use or other pathological compensatory disorders
Give appropriate contraceptive advice to ensure that the risk of premature and unwanted pregnancy is
minimised 101
After discharge from the bariatric surgery service bariatric physicians and GPs: t
Formulate a shared care model of chronic disease management for lifelong follow up led by the physician that clarifies what is expected of each role and what should be achieved at each review u 23, 102
o Include referral pathways back and access to the WAMC, surgical unit or mental health professional if needed 103
o Include local protocols with the WAMC for appropriate investigation of post-bariatric surgery abnormalities such as anaemia or symptoms such as pain or vomiting, or for weight regain
o Include local protocols with the WAMC for assessment of the psychological difficulties such as depression, disturbed eating behaviours, loss of eating control that can be associated with weight regain after 2 or 3 years v 49, 64, 65, 69, 95, 100, 103-110
Ensure that appropriate computer codes are used to record bariatric procedures and keep a register of patients having bariatric surgery
Arrange for patients to be reviewed at least annually, indefinitely o Include an assessment of nutritional intake, nutritional monitoring and trace mineral status,
weight check, assessment of comorbidities, review of multivitamin and mineral supplements and investigation of abnormal results and appropriate treatment as required, according to the shared care model 13, 99
Arrange at least an Annual Review of diabetes control o Even when patients with type 2 diabetes achieve normoglycaemia without treatment
(‘remission’) they should remain on the diabetes register indefinitely o Consider continuing medications indefinitely for those previously at high cardiovascular risk due
to diabetes, dyslipidaemia and hypertension 13, 111
Continue appropriate physical activity advice 79, 80, 112, 113
Consider referring patients for removal of excess skin according to BAPRAS Commissioning Guidance w 114
t In the context of the tier terminology ‘bariatric physicians and GPs’ implies Tier 3 and primary care services. The panel also recognised that there are existing examples of best practice where in the absence of a bariatric physician or Weight Assessment and Management Clinic surgical teams and GPs have already developed what is in effect a shared model of care. u Examples of models of care are given in the appendices to the O’Kane article
23 and can be downloaded free of charge
http://onlinelibrary.wiley.com/store/10.1111/cob.12145/asset/supinfo/cob12145-sup-0001-AppendixS1-S3.pdf?v=1&s=f327e73b582e90f9d790eba4c2d8beefca5734af . v ASMBS guidelines recommend that even in the absence of severe adverse outcomes, postsurgical psychosocial involvement
may support patients to negotiate the complex and dynamic process of behaviour change following surgery to support sustained adherence to the postoperative regimen in the long term. Long-term psychosocial follow-up is therefore needed.
Commissioning guide 2017 Weight assessment and management clinics
18
Provide data as required to the surgical unit for the National Bariatric Surgery Registry
2 Procedures explorer tool for weight assessment and management clinics
Users can access further procedure information based on the data available in the quality dashboard to see how
individual providers are performing against the indicators. This will enable CCGs to start a conversation with
providers who appear to be ‘outliers’ from the indicators of quality that have been selected.
The Procedures Explorer Tool is available via the Royal College of Surgeons website.
3 Quality dashboard for weight assessment and management clinics
In the guidance development process the quality dashboard potentially provides an overview of activity
commissioned by CCGs from the relevant pathways, and indicators of the quality of care provided by surgical
units. However, the quality dashboard is severely constrained by the lack of national data on provision of non-
surgical services and does not demonstrate all the data required to assess a medical weight management service.
It is suggested that a recognised tool such as the National Obesity Observatory Standard Evaluation Framework is
used to evaluate these services, and that in future consideration is given to collecting these data nationally 51.
Existing definitions of bariatric surgery according to HES are an estimate and open to interpretation but standard
metrics could be presented against these, populated from Hospital Episode Statistics (HES) and Office for National
Statistics (ONS) data. Although the following mostly relate to bariatric surgery and not Weight Assessment and
Management clinics, the metrics could include:
Rates of referral to Weight Assessment and Management clinics, as presented in a quality dashboard,
according to:
o Gender and ethnicity
o Reported population prevalence of obesity (Standardised / 100,000) (Quality Outcomes
Framework (QOF) / ONS)
o Reported population prevalence of diabetes (Standardised / 100,000) (QOF / ONS)
o Reported population prevalence of cardiovascular disease (Standardised / 100,000) (QOF / ONS)
Rates of referral for surgery
o For each of the above metrics
w
NHS England advises that this can only be undertaken in line with the local Effective Use of Resources policies of each CCG.
Commissioning guide 2017 Weight assessment and management clinics
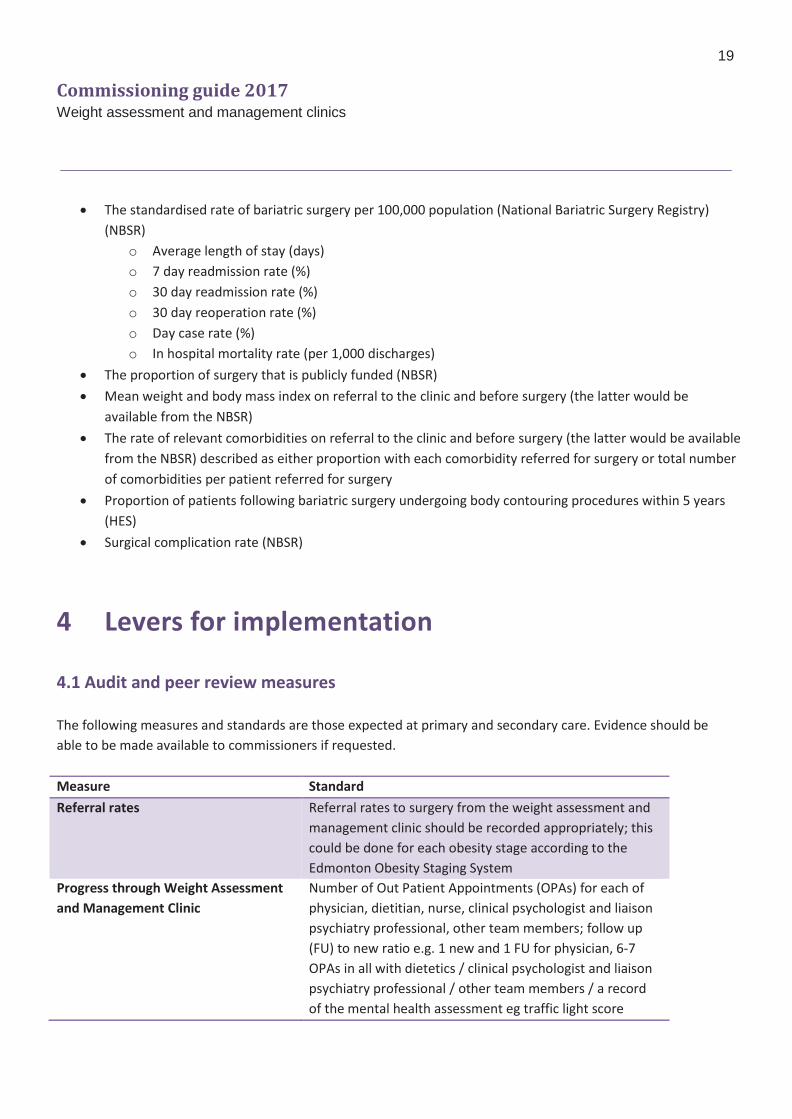
19
The standardised rate of bariatric surgery per 100,000 population (National Bariatric Surgery Registry)
(NBSR)
o Average length of stay (days)
o 7 day readmission rate (%)
o 30 day readmission rate (%)
o 30 day reoperation rate (%)
o Day case rate (%)
o In hospital mortality rate (per 1,000 discharges)
The proportion of surgery that is publicly funded (NBSR)
Mean weight and body mass index on referral to the clinic and before surgery (the latter would be
available from the NBSR)
The rate of relevant comorbidities on referral to the clinic and before surgery (the latter would be available
from the NBSR) described as either proportion with each comorbidity referred for surgery or total number
of comorbidities per patient referred for surgery
Proportion of patients following bariatric surgery undergoing body contouring procedures within 5 years
(HES)
Surgical complication rate (NBSR)
4 Levers for implementation
4.1 Audit and peer review measures
The following measures and standards are those expected at primary and secondary care. Evidence should be
able to be made available to commissioners if requested.
Measure Standard
Referral rates Referral rates to surgery from the weight assessment and
management clinic should be recorded appropriately; this
could be done for each obesity stage according to the
Edmonton Obesity Staging System
Progress through Weight Assessment
and Management Clinic
Number of Out Patient Appointments (OPAs) for each of
physician, dietitian, nurse, clinical psychologist and liaison
psychiatry professional, other team members; follow up
(FU) to new ratio e.g. 1 new and 1 FU for physician, 6-7
OPAs in all with dietetics / clinical psychologist and liaison
psychiatry professional / other team members / a record
of the mental health assessment eg traffic light score

Commissioning guide 2017 Weight assessment and management clinics
20
National Obesity Standard Evaluation
Framework
The provider should arrange for on-going population and
submission of this comprehensive national specified data
collection tool
Documentation of MDT process Record each patient discussed, frequency of meetings,
who attends, quoracy
National Bariatric Surgery Registry Provider should arrange for on-going annual submission
of data to the NSBR for operated patients according to
the current dataset requirements
4.2 Quality Specification/CQUIN (Commissioning for Quality and Innovation) Measure Description Data specification
(if required)
Patient satisfaction rates with the
complex obesity service
The provider demonstrates
service user experience
satisfaction with its service
Local patient survey data
Patient quality of life following
service use
Use of a validated tool such as
SF36 or EQ5D to demonstrate
impact on quality of life
Local data collection
Mean weight loss (kg or % or
both) and/or excess BMI loss
and/or % excess weight loss post
engagement with the service at
12 months
Would capture effect on weight
at one year of any intervention
provided in the clinic
Partial data are available
in the NBSR (for surgical
patients) but additional
follow up data are
required from non-
surgical and non-
specialist services which
could come from a
registry set up for the
purpose
Measures of patient engagement Measure ‘opt-in’ rates; Did Not
Attend (DNA) rates including
DNA even once; stratified by
gender and ethnic origin, to
assess equality of access
E.g. discharge if >2 DNAs
Length of stay, improvement in
HbA1c for surgical patients (more
likely a component of a surgical
CQUIN)
Provider demonstrates a mean
length of stay of number more
than x days
Data available from
NBSR/HES
Commissioning guide 2017 Weight assessment and management clinics
21
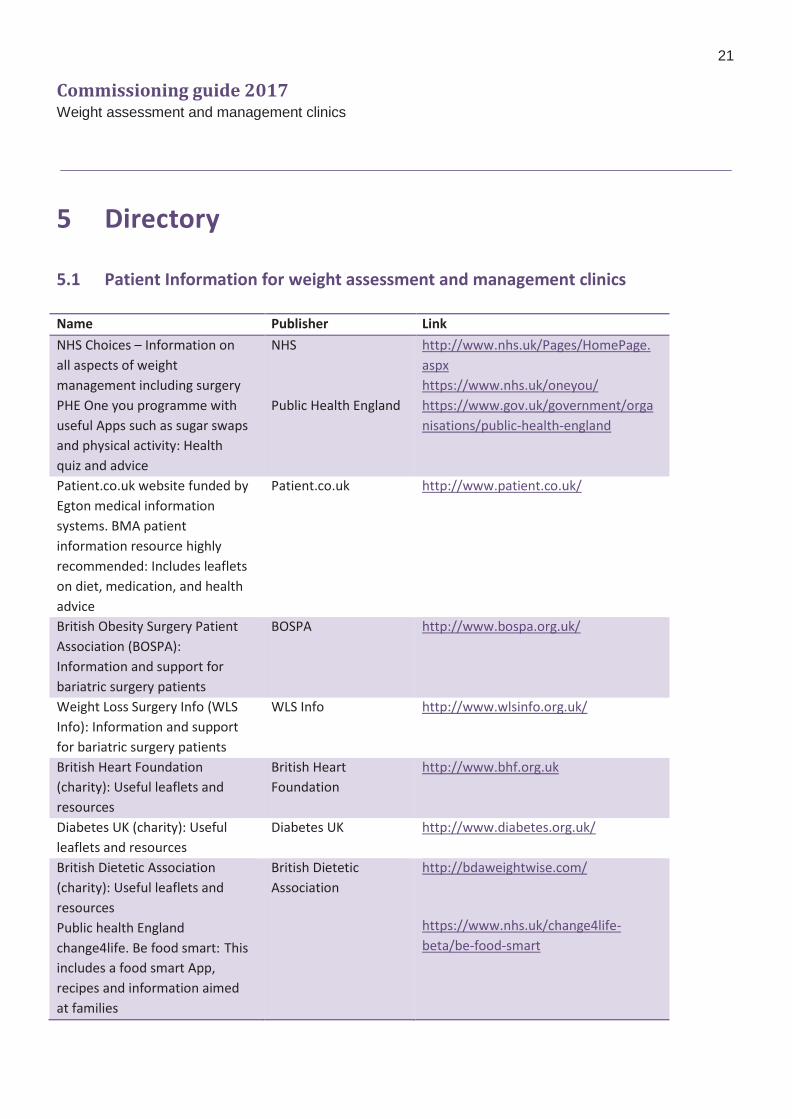
5 Directory
5.1 Patient Information for weight assessment and management clinics
Name Publisher Link
NHS Choices – Information on
all aspects of weight
management including surgery
PHE One you programme with
useful Apps such as sugar swaps
and physical activity: Health
quiz and advice
NHS
Public Health England
http://www.nhs.uk/Pages/HomePage.
aspx
https://www.nhs.uk/oneyou/
https://www.gov.uk/government/orga
nisations/public-health-england
Patient.co.uk website funded by
Egton medical information
systems. BMA patient
information resource highly
recommended: Includes leaflets
on diet, medication, and health
advice
Patient.co.uk http://www.patient.co.uk/
British Obesity Surgery Patient
Association (BOSPA):
Information and support for
bariatric surgery patients
BOSPA http://www.bospa.org.uk/
Weight Loss Surgery Info (WLS
Info): Information and support
for bariatric surgery patients
WLS Info http://www.wlsinfo.org.uk/
British Heart Foundation
(charity): Useful leaflets and
resources
British Heart
Foundation
http://www.bhf.org.uk
Diabetes UK (charity): Useful
leaflets and resources
Diabetes UK http://www.diabetes.org.uk/
British Dietetic Association
(charity): Useful leaflets and
resources
Public health England
change4life. Be food smart: This
includes a food smart App,
recipes and information aimed
at families
British Dietetic
Association
http://bdaweightwise.com/
https://www.nhs.uk/change4life-
beta/be-food-smart
Commissioning guide 2017 Weight assessment and management clinics
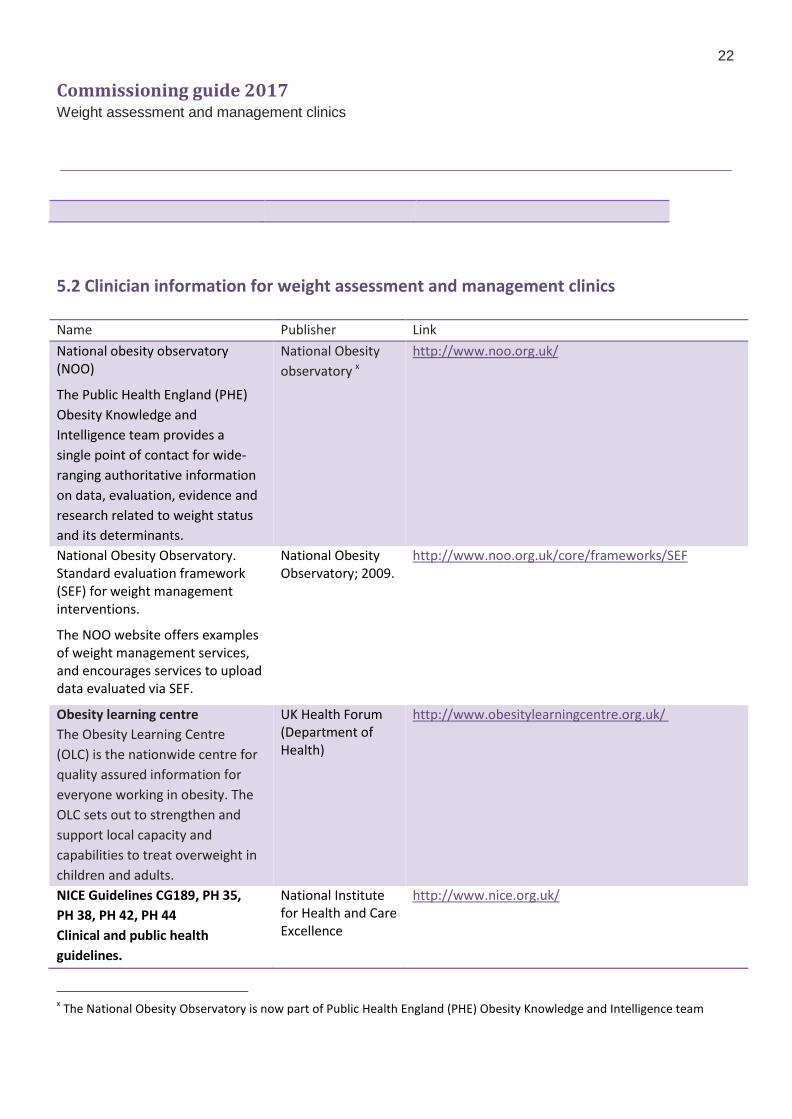
22
5.2 Clinician information for weight assessment and management clinics Name Publisher Link
National obesity observatory (NOO)
The Public Health England (PHE)
Obesity Knowledge and
Intelligence team provides a
single point of contact for wide-
ranging authoritative information
on data, evaluation, evidence and
research related to weight status
and its determinants.
National Obesity
observatory x
http://www.noo.org.uk/
National Obesity Observatory. Standard evaluation framework (SEF) for weight management interventions.
The NOO website offers examples of weight management services, and encourages services to upload data evaluated via SEF.
National Obesity Observatory; 2009.
http://www.noo.org.uk/core/frameworks/SEF
Obesity learning centre
The Obesity Learning Centre
(OLC) is the nationwide centre for
quality assured information for
everyone working in obesity. The
OLC sets out to strengthen and
support local capacity and
capabilities to treat overweight in
children and adults.
UK Health Forum (Department of Health)
http://www.obesitylearningcentre.org.uk/
NICE Guidelines CG189, PH 35,
PH 38, PH 42, PH 44
Clinical and public health
guidelines.
National Institute for Health and Care Excellence
http://www.nice.org.uk/
x The National Obesity Observatory is now part of Public Health England (PHE) Obesity Knowledge and Intelligence team
Commissioning guide 2017 Weight assessment and management clinics
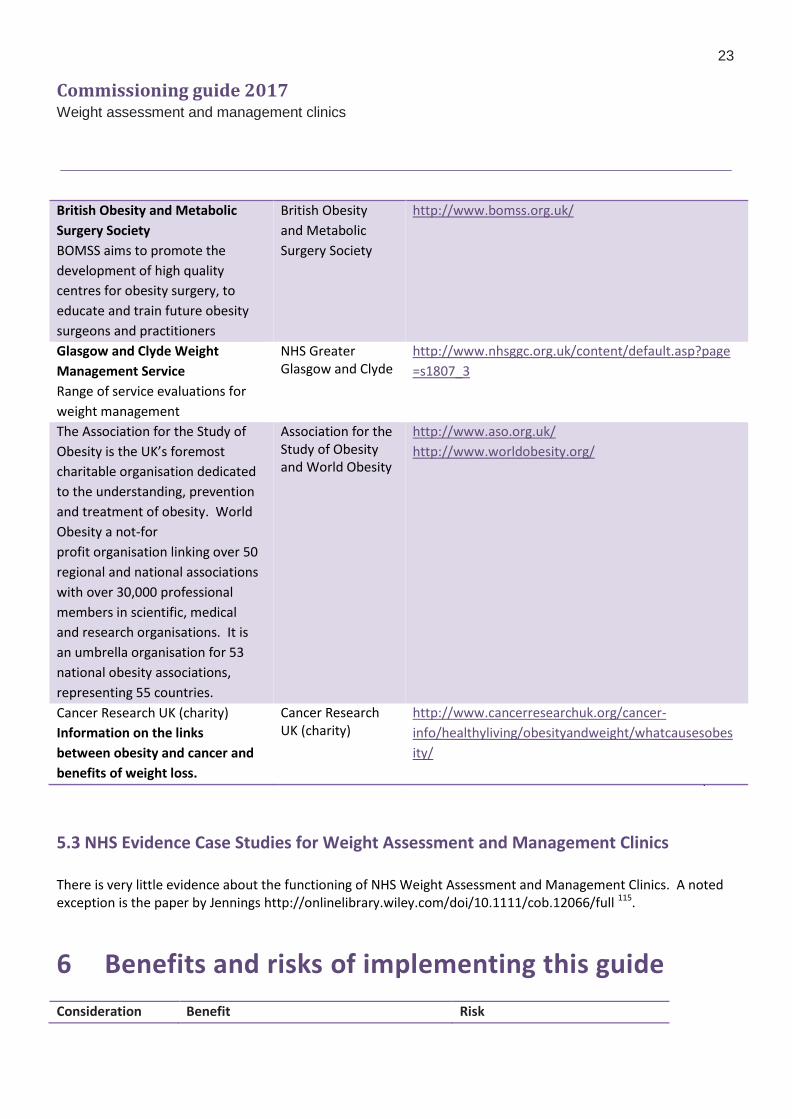
23
British Obesity and Metabolic
Surgery Society
BOMSS aims to promote the
development of high quality
centres for obesity surgery, to
educate and train future obesity
surgeons and practitioners
British Obesity
and Metabolic
Surgery Society
http://www.bomss.org.uk/
Glasgow and Clyde Weight
Management Service
Range of service evaluations for
weight management
NHS Greater Glasgow and Clyde
http://www.nhsggc.org.uk/content/default.asp?page
=s1807_3
The Association for the Study of
Obesity is the UK’s foremost
charitable organisation dedicated
to the understanding, prevention
and treatment of obesity. World
Obesity a not-for
profit organisation linking over 50
regional and national associations
with over 30,000 professional
members in scientific, medical
and research organisations. It is
an umbrella organisation for 53
national obesity associations,
representing 55 countries.
Association for the Study of Obesity and World Obesity
http://www.aso.org.uk/
http://www.worldobesity.org/
Cancer Research UK (charity)
Information on the links
between obesity and cancer and
benefits of weight loss.
Cancer Research UK (charity)
http://www.cancerresearchuk.org/cancer-
info/healthyliving/obesityandweight/whatcausesobes
ity/
5.3 NHS Evidence Case Studies for Weight Assessment and Management Clinics There is very little evidence about the functioning of NHS Weight Assessment and Management Clinics. A noted exception is the paper by Jennings http://onlinelibrary.wiley.com/doi/10.1111/cob.12066/full 115.
6 Benefits and risks of implementing this guide
Consideration Benefit Risk
Commissioning guide 2017 Weight assessment and management clinics
24
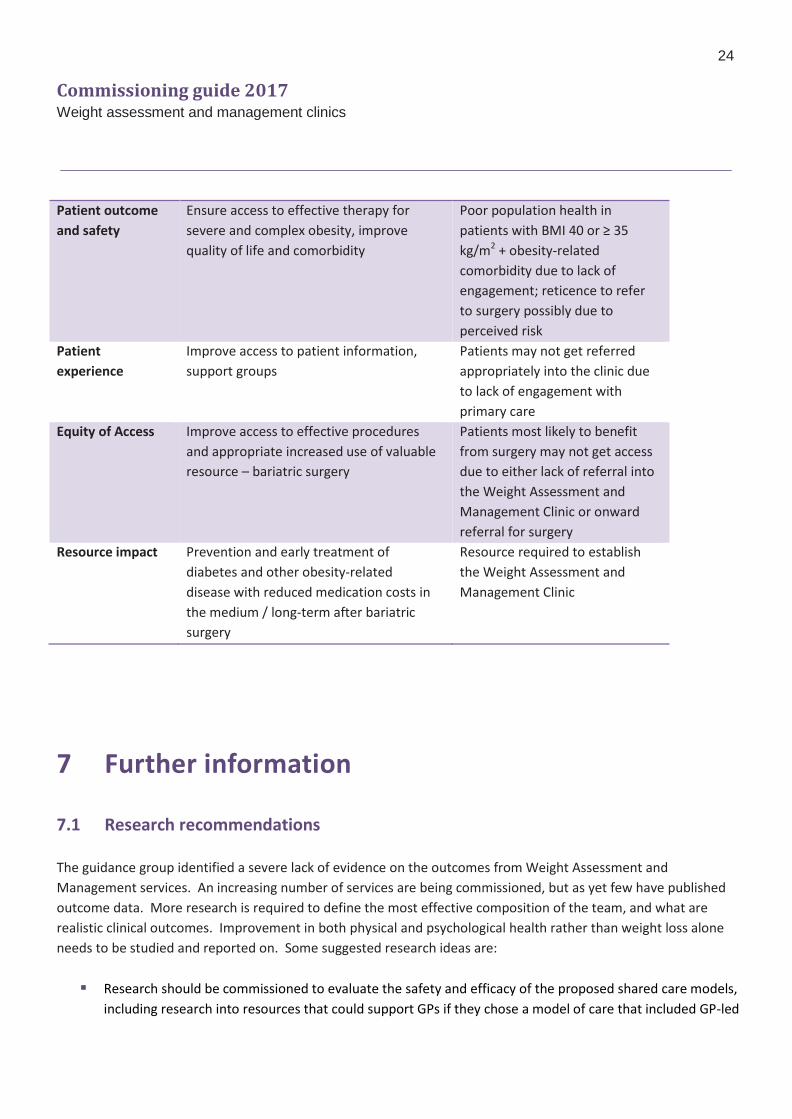
Patient outcome
and safety
Ensure access to effective therapy for
severe and complex obesity, improve
quality of life and comorbidity
Poor population health in
patients with BMI 40 or ≥ 35
kg/m2 + obesity-related
comorbidity due to lack of
engagement; reticence to refer
to surgery possibly due to
perceived risk
Patient
experience
Improve access to patient information,
support groups
Patients may not get referred
appropriately into the clinic due
to lack of engagement with
primary care
Equity of Access Improve access to effective procedures
and appropriate increased use of valuable
resource – bariatric surgery
Patients most likely to benefit
from surgery may not get access
due to either lack of referral into
the Weight Assessment and
Management Clinic or onward
referral for surgery
Resource impact Prevention and early treatment of
diabetes and other obesity-related
disease with reduced medication costs in
the medium / long-term after bariatric
surgery
Resource required to establish
the Weight Assessment and
Management Clinic
7 Further information
7.1 Research recommendations
The guidance group identified a severe lack of evidence on the outcomes from Weight Assessment and
Management services. An increasing number of services are being commissioned, but as yet few have published
outcome data. More research is required to define the most effective composition of the team, and what are
realistic clinical outcomes. Improvement in both physical and psychological health rather than weight loss alone
needs to be studied and reported on. Some suggested research ideas are:
Research should be commissioned to evaluate the safety and efficacy of the proposed shared care models,
including research into resources that could support GPs if they chose a model of care that included GP-led
Commissioning guide 2017 Weight assessment and management clinics
25
annual review
Research is needed on which of the proposed shared care models is most acceptable to patients and cost-
effective
Studies should be done to identify the current knowledge among GPs, dietitians and primary care staff
about the management of post bariatric patients, and if educational needs are identified appropriate
training should be developed
Training needs have been identified among healthcare professionals obstetricians, including midwives,
dietitians and emergency department staff and educational resources including e learning should be
developed, evaluated and disseminated
Alternative ways of collecting long-term data for NBSR should be explored
Research into the ideal make-up of the MDT in the children’s / adolescent WAMC
Research into the ideal age at which to perform bariatric surgery in children / adolescents
Research will be needed to consider the clinician experience and competencies of the mental health
professionals described in the American Society for Metabolic and Bariatric Surgery (ASMBS) article by
Sogg in relation to UK clinicians 49
Studies to test the hypothesis that: nurse specialists with prescribing rights can be just as effective as
bariatric physicians as members of multidisciplinary teams in Tier 3
Studies considering the impact of appropriately trained dietitians and specialist nurses providing
psychosocial screening assessments in Tier 3 services
Studies considering what issues raised in psychological/psychosocial screening need further intervention
from within the MDT and which issues are referred to other services
Studies looking at outcomes for patients who have accessed a clinical psychologist and a liaison psychiatry
professional in Tier 3 vs those who have not
Evidence is lacking on what stops patients ‘opting in’ to weight management programmes. A multi-
component qualitative study including telephone interviews, focus groups etc. including MDT experience
might discover barriers to engagement and generate hypotheses on how to engage hard to reach groups
A multidisciplinary group should be set up to look at relevant research questions, perhaps involving the Society
for Endocrinology Obesity bariatric physician group.
7.2 Other recommendations
There is an urgent need for a national registry of Tier 3 / Weight Assessment and Management Clinics. It is
important for a relevant clear outcomes dataset to be identified to evaluate the work up for surgery and
for surgery itself, and key stakeholders (patients, surgeons, endocrinologists, nurses, dietitians, clinical
psychologists and liaison psychiatry professionals) should select these outcomes. A core set of outcomes
could then be measured and reported in all studies of medical work-up for severe and complex obesity
There is an urgent need to commission and implement children’s / adolescent obesity clinics
All children’s / adolescent patients should be entered into the NBSR
It would be important to add in a measure of co-morbidities such as the Edmonton Obesity Staging System
Commissioning guide 2017 Weight assessment and management clinics
26
(EOSS) score to the baseline data, and to recognise that valid comparison between services should reflect
the population recruited
A multidisciplinary group could look at these ideas and the possibility of working with the PHE Obesity
Knowledge and Intelligence Team should be explored.

Commissioning guide 2017 Weight assessment and management clinics
27
7.3 Evidence base
1. Welbourn R, Wass J, Barth J, Clare K, Dixon J, Finer N, Hughes C, Jolly A, Sawyer S, McClelland L, McMillan I,
O’Kane, Pinnock G, le Roux C, Sedman P, Snowdon-Carr V. British Obesity and Metabolic Surgery Society /
Royal College of Surgeons Commissioning guide: Weight Assessment and Management Clinics (tier 3).
https://www.rcseng.ac.uk/healthcare-bodies/docs/weight-assessment-and-management-tier-3-services
(2014) and http://www.bomss.org.uk/wp-content/uploads/2014/04/Commissioning-guide-weight-
assessment-and-management-clinics-published.pdf (2014)
2. Welbourn R, Dixon J, Barth JH, Finer N, Hughes CA, le Roux CW, Wass J on behalf of the Guidance
Development Group. NICE-Accredited Commissioning Guidance for Weight Assessment and Management
Clinics: a Model for a Specialist Multidisciplinary Team Approach for People with Severe Obesity. Obesity
Surgery 2016; 26: DOI 10.1007/s11695-015-2041-8.
3. Clinical Commissioning Policy: Complex and Specialised Obesity Surgery. April 2013. Reference
NHSCB/A05/P/a. http://www.england.nhs.uk/wp-content/uploads/2013/04/a05-p-a.pdf
4. Welbourn R, le Roux C, Owen-Smith A, Wordsworth S, Blazeby JM. Why the NHS should do more bariatric
surgery; how much should we do? BMJ 2016; 353 doi: http://dx.doi.org/10.1136/bmj.i1472
5. Royal College of Physicians. Action on obesity: comprehensive care for all. Report of a working party.
London: RCP, 2013. http://www.rcplondon.ac.uk/sites/default/files/action-on-obesity.pdf
6. Academy of Medical Royal Colleges. Measuring up. The medical profession’s prescription for the nation’s
obesity crisis. London 2013. http://www.aomrc.org.uk/about-us/news/item/doctors-unite-to-deliver-
prescription-for-uk-obesity-epidemic.html
7. NICE. Obesity: identification, assessment and management. Clinical guideline [CG189]. November 2014.
https://www.nice.org.uk/guidance/cg189
8. SIGN. Management of obesity. 115. Edinburgh: Scottish Intercollegiate Guidelines Network; 2010.
Available from: www.sign.ac.uk/pdf/sign115.pdf
9. BOMSS. Providing bariatric surgery: BOMSS standards for clinical services & guidance on commissioning.
London: British Obesity & Metabolic Surgery Society; 2012. Available from:
http://www.bomss.org.uk/pdf/clinical_services_standards/Service_std-2012.pdf
10. Developing a specification for lifestyle weight management services. Best practice guidance for tier 2
services. Department of Health, Obesity and Food Policy Branch, PHD. March 2013.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/142723/Weight_Manag
ement_Service_Spec_FINAL_with_IRB.pdf
11. Rubino F, Nathan DM, Eckel RH, Schauer PR, Alberti KGMM, Zimmet PZ et al. Metabolic Surgery in the Treatment Algorithm for Type 2 Diabetes: A Joint Statement by International Diabetes Organizations. Diabetes Care 2016;39:861–877 | DOI: 10.2337/dc16-0236.
12. Aveyard P, Lewis A, Tearne S, Hood K, Christian-Brown A, Adab P et al. Screening and brief intervention for obesity in primary care: a parallel, two-arm, randomised trial. Lancet 2016; 388: 2472-2500. Published Online October 24, 2016 http://dx.doi.org/10.1016/ S0140-6736(16)31893-1.
13. Mechanick JI, Youdim A, Jones DB, Garvey WT, Hurley DL, McMahon MM et al. Clinical practice guidelines
Commissioning guide 2017 Weight assessment and management clinics
28
for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013
update: Co-sponsored by American Association of Clinical Endocrinologists, The Obesity Society, and
American Society for Metabolic & Bariatric Surgery. Obesity 2013; 21: S1-S27.
http://www.ncbi.nlm.nih.gov/pubmed/23529939 or
http://www.seen.es/docs/apartados/485/ASPEN%20BARIATRIC%20SURGERY.pdf (2008 Clinical practice
guidelines)
14. Colquitt JL et al. Surgery for weight loss in adults. Cochrane Database of Systematic Reviews 2014 (8). 15. Gloy, V. L., et al. Bariatric surgery versus non-surgical treatment for obesity: a systematic review and meta-
analysis of randomised controlled trials. BMJ 2013; 347: f5934. 16. Courcoulas AP et al. Surgical vs medical treatments for type 2 diabetes mellitus: a randomized clinical trial.
JAMA Surgery 2014; 149(7): 707-715. 17. Liang, Z., et al. Effect of laparoscopic Roux-en-Y gastric bypass surgery on type 2 diabetes mellitus with
hypertension: a randomized controlled trial. Diabetes Res Clin Pract 2013; 101(1): 50-56. 18. Ikramuddin, S., et al. Roux-en-Y gastric bypass vs intensive medical management for the control of type 2
diabetes, hypertension, and hyperlipidemia: the Diabetes Surgery Study randomized clinical trial. JAMA 2013; 309(21): 2240-2249.
19. Schauer, P. R., et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Eng J Med 2012; 366(17): 1567-1576.
20. Paluszkiewicz, R., et al. Prospective randomized clinical trial of laparoscopic sleeve gastrectomy versus open Roux-en-Y gastric bypass for the management of patients with morbid obesity. Wideochirurgia I Inne Techniki Maloinwazyjne 2012; 7(4): 225-232.
21. Mingrone, G., et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Eng J Med 2012; 366(17): 1577-1585.
22. Woelnerhanssen, B., et al. Effects of postbariatric surgery weight loss on adipokines and metabolic parameters: comparison of laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy--a prospective randomized trial. Surg Obes Relat Dis 2011; 7(5): 561-568.
23. O’Kane M, Parretti HM, Hughes CA, Sharma M , Woodcock S, Puplampu T et al. Guidelines for the follow-up of patients undergoing bariatric surgery. Clin Obesity 2016; 6, 210–224.
24. Brauer P, Connor Gorber S, Shaw E, Singh H, Bell N, Shane AR, Jaramillo A, Tonelli M, Canadian Task Force on Preventive Health Care. Recommendations for prevention of weight gain and use of behavioural and pharmacologic interventions to manage overweight and obesity in adults in primary care. CMAJ. 2015 Feb 17;187(3):184-95. https://www.guideline.gov/summaries/summary/49013/recommendations-for-prevention-of-weight-gain-and-use-of-behavioural-and-pharmacological-interventions-to-manage-overweight-and-obesity-in-adults-in-primary-care
25. Management of Overweight and Obesity Working Group. VA/DoD clinical practice guideline for screening and management of overweight and obesity. Washington (DC): Department of Veterans Affairs, Department of Defense; 2014. 178 p.
26. Wadden TA et al. Behavioral treatment of obesity in patients encountered in primary care settings: a systematic review. JAMA 2014; 312(17): 1779-1791.
27. Kushner RF, DH Ryan. Assessment and lifestyle management of patients with obesity: clinical recommendations from systematic reviews. JAMA 2014; 312(9): 943-952.
28. Fitch A, Fox C, Bauerly K, Gross A, Heim C, Judge-Dietz J, Kaufman T, Krych E, Kumar S, Landin D, Larson J, Leslie D, Martens N, Monaghan-Beery N, Newell T, O'Connor P, Spaniol A, Thomas A, Webb B. Prevention and management of obesity for children and adolescents. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); 2013 Jul. 94 p.
Commissioning guide 2017 Weight assessment and management clinics
29
https://www.guideline.gov/summaries/summary/47102/prevention-and-management-of-obesity-for-children-and-adolescents
29. Swinburn B, Arroll B. Rethinking primary care systems for obesity. Lancet October 24, 2016 http://dx.doi.org/10.1016/ S0140-6736(16)31913-4.
30. Public Health England (2016). Making reasonable adjustments to obesity and weight management services for people with learning disabilities. http://www.improvinghealthandlives.org.uk/gsf.php5?f=314268&fv=22261
31. Hassan Y, Head V , Jacob D, Bachmann MO, Diu S, Ford J. Lifestyle interventions for weight loss in adults with severe obesity: a systematic review.
32. Rollnick S, Heather N, Bell A. Negotiating behaviour change in medical settings: The development of brief motivational interviewing. J Mental Health 1992: 1: 25-37. http://phe512.files.wordpress.com/2011/03/04-rollnick.pdf
33. Ten top tips for the management of patients post bariatric surgery in primary care. RCGP 2014. http://www.rcgp.org.uk/clinical-and-research/clinical-resources/nutrition/~/media/Files/CIRC/Nutrition/Obesity/RCGP-Top-ten-tips-for-post-bariatric-surgery-patients-in-primary-care-Nov-2014.ashx
34. Simpson SA et al. A feasibility randomised controlled trial of a motivational interviewing-based intervention for weight loss maintenance in adults. Health Technology Assessment (Winchester, England) 19(50): v-vi, xix-xxv, 1-378.
35. National Institute for Health and Care Excellence - NICE (2014). Weight management: lifestyle services for overweight or obese adults : guidance (PH53). https://www.nice.org.uk/guidance/ph53
36. Jebb SA, Ahern AL, Olson AD, et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: a randomised controlled trial. Lancet. 2011;378(9801):1485-92.
37. GP Ten Top Tips: Raising the Topic of Weight. RCGP 2013. http://www.rcgp.org.uk/clinical-and-research/clinical-resources/nutrition/~/media/Files/CIRC/Clinical%20News/Top-Ten-Tips-Leaflet-2013.ashx
38. Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JFE, Nauck MA et al for the LEADER Steering Committee on behalf of the LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2016; 375:311-322July 28, 2016DOI: 10.1056/NEJMoa1603827
39. Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S et al for the EMPA-REG OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015; 373:2117-2128November 26, 2015DOI: 10.1056/NEJMoa1504720
40. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998 Sep 12;352(9131):854-65.
41. Pi-Sunyer X, Astrup A, Fujioka K, et al. SCALE Obesity and Prediabetes NN8022-1839 Study Group. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N Engl J Med 2015; 373:11-22. doi:10.1056/NEJMoa1411892 pmid:26132939.
42. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA 2014; 311(1): 74-86.
43. Gray LJ et al. A systematic review and mixed treatment comparison of pharmacological interventions for the treatment of obesity. Obesity Reviews 2012; 13(6): 483-498.
44. Davies, M. J., et al. Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial. JAMA 2015; 314(7): 687-699.
45. Rubin RR et al. Impact of intensive lifestyle intervention on depression and health-related quality of life in type 2 diabetes: the Look AHEAD Trial. Diabetes Care 2014; 37(6): 1544-1553.
Commissioning guide 2017 Weight assessment and management clinics
30
46. Dixon JB, Zimmet P, Alberti KG. Rubino F, on behalf of the International Diabetes Federation Taskforce on Epidemiology and Prevention. Bariatric surgery: an IDF statement for obese Type 2 diabetes. Diabet Med 2011; 28: 628-642. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3123702/
47. Burguera, B., et al. (2015). An Intensive Lifestyle Intervention Is an Effective Treatment of Morbid Obesity: The TRAMOMTANA Study-A Two-Year Randomized Controlled Clinical Trial. International Journal of Endocrinology 2015 (no pagination)(194696).
48. NICE. Obesity: clinical assessment and management. Quality standard [QS127]. August 2016. https://www.nice.org.uk/guidance/QS127/
49. Sogg S, Lauretti J, West-Smith L. Recommendations for the presurgical psychosocial evaluation of bariatric surgery patients. Surgery for Obesity and Related Diseases 2016; 12: 731–749. http://dx.doi.org/10.1016/j.soard.2016.02.008
50. Bocca, G., et al. Results of a multidisciplinary treatment program in 3-year-old to 5-year-old overweight or obese children: a randomized controlled clinical trial. Arch Pediatrics Adolesc Med 2012; 166(12): 1109-1115.
51. Banks, J., et al. Evaluating the transferability of a hospital-based childhood obesity clinic to primary care: a randomised controlled trial. Br J Gen Pract 2012; 62(594): e6-12.
52. Ells LJ, Hancock C, Copley VR, et al. Prevalence of severe childhood obesity in England: 2006-2013. Archives of Disease in Childhood 2015;100(7):631-36. doi: 10.1136/archdischild-2014-307036
53. Academy of Nutrition and Dietetics (2014). Adult weight management evidence-based nutrition practice guideline. http://www.andeal.org/topic.cfm?menu=5276&cat=4688
54. Halperin F et al. Roux-en-Y gastric bypass surgery or lifestyle with intensive medical management in patients with type 2 diabetes: feasibility and 1-year results of a randomized clinical trial. JAMA Surgery 2014; 149(7): 716-726.
55. Biswas A, Vahabzadeh A, Hobbs T and Healy J. Obesity in people with learning disabilities: possible causes and reduction interventions. Nursing Times; 106: 31:16-8.
56. Spanos, D. Melville, C. & Hanky, C. Weight management interventions in adults with intellectual disabilities and obesity: a systematic review of the evidence Nutrition Journal 201312: 132 DOI: 10.1186/1475-2891-12-132.
57. Myers K, Hajek P, Hinds C, McRobbie H. Stopping Smoking Shortly Before Surgery and Postoperative Complications. A Systematic Review and Meta-analysis. Ann Int Med 2011; 171: 983-989. http://archinte.jamanetwork.com/article.aspx?articleid=227487
58. Goldstone AP, Beales PL. Genetic obesity syndromes. Front Horm Res. 2008;36:37-60. doi: 10.1159/0000115336.
59. Apovian CM, Cummings S, Anderson W, Borud L, Boyer K, Day K et al. Best Practice Updates for
Multidisciplinary Care in Weight Loss Surgery. Obesity 2009; 17: 871-89. Doi:10.1038/oby.2008.580.
http://onlinelibrary.wiley.com/store/10.1038/oby.2008.580/asset/oby.2008.580.pdf?v=1&t=hkcj74du&s=
ec124201a65701c9436948e1323b4c95f10f76e3
60. Malik S, Mitchell JE, Engel S, Crosby R, Wonderlich S. Psychopathology in bariatric surgery candidates: a
review of studies using structured diagnostic interviews. Compr Psychiatry 2014; 55(2): 248-59. doi:
10.1016/j.comppsych.2013.08.02. 61. Backman O, Stockeld D, Rasmussen F, Näslund E, Marsk R. Alcohol and substance abuse, depression and
suicide attempts after Roux-en-Y gastric bypass surgery. Br J Surg 2016; 103(10): 1336-42. doi: 10.1002/bjs.10258.
62. Chao AM, Wadden TA, Faulconbridge LF, Sarwer DB, Webb VL, Shaw JA, Thomas JG, Hopkins CM, Bakizada ZM, Alamuddin N, Williams NN. Binge-eating disorder and the outcome of bariatric surgery in a
Commissioning guide 2017 Weight assessment and management clinics
31
prospective, observational study: Two-year results. Obesity (Silver Spring). 2016; 24(11): 2327-2333. doi: 10.1002/oby.21648.
63. Devlin MJ, King WC, Kalarchian MA, White, GE, Marcus, MD, Garcia L, Yanovski SZ, Mitchell JE. Eating pathology and experience and weight loss in a prospective study of bariatric surgery patients: 3‐year follow‐up. Int J Eating Disorders. 2016; 49(12): 1058-1067.
64. Mitchell J, De Zwaan M. Psychopathology and bariatric surgery. In: Still C, Sarwer D, Blankenship J, eds. The ASMBS textbook of bariatric surgery, 2nd vol. NewYork: Springer; 2014.p.11–7.
65. Kalarchian M, King W, Devlin M, Marcus MD, Chen JY, Garcia L, Yanovski S, Mitchell J. Psychiatric Disorders
and weight Change in a Prospective Study of Bariatric Surgery Patients: A 3-Year Follow-Up. Surg Obes
Relat Dis 2015; 11(6): S47.
66. Fischer L, Nickel F, Sander J, Ernst A, Bruckner T, Herbig B, Büchler MW, Müller-Stich, BP, Sandbu R. Patient
expectations of bariatric surgery are gender specific—a prospective, multicenter cohort study. Surgery for
Obesity and Related Diseases 2014; 10(3): 516-523.
67. Kubik JF, Gill RS, Laffin M, Karmali S. The impact of bariatric surgery on psychological health. J Obes
2013;2013:837989.
68. Dawes AJ, Maggard-Gibbons M, Maher AR, Booth MJ, Miake-Lye I, Beroes JM Shekelle PG. Mental health conditions among patients seeking and undergoing bariatric surgery: a meta-analysis. JAMA 2016; 315(2): 150-163.
69. Sheets C, Peat C, Berg K et al. Post-operative psychosocial predictors of outcome in bariatric surgery. Obes Surg 2015; 25(2): 330–45.
70. Rummell CM, Heinberg LJ. Assessing marijuana use in bariatric surgery candidates: should it be a contraindication? Obes Surg 2014;24:1764-70. doi: 10.1007/s11695-014-1315-x.
71. Hemmingsson E, Johansson K, Reynisdottir S. Effects of childhood abuse on adult obesity: a systematic review and meta-analysis. Obes Rev. 2014; 15 :882-93. doi: 10.1111/obr.12216.
72. Brewerton TD, ONeil PM, Dansky BS, Kilpatrick DG. Extreme Obesity and its Associations with Victimization, PTSD, Major Depression and Eating Disorders in a National Sample of Women. J Obes Eating Disorders 2015; 1 No. 2: 6: 1-9 http://obesity.imedpub.com/.
73. Brownley KA, Berkman ND, Peat, CM, Lohr KN, Cullen KE, Bann CM, Bulik CM. Binge-Eating Disorder in Adults. A Systematic Review and Meta-analysis. Ann Int Med 2016; 165(6): 409-420.
74. Mantzios M, Wilson J. Mindfulness, Eating Behaviours, and Obesity: A Review and Reflection on Current
Findings. Current Obesity Reports 2015; 4:(1): 141–146. 75. O'Reilly G, Cook L, Spruijt-Metz D, Black, S. Mindfulness-based interventions for obesity-related eating
behaviours: a literature review. Obes Rev. 2014; 15(6): 453–461. 76. Padwal RJ, Pajewski NM, Allison DB, Sharma AM. Using the Edmonton obesity staging system to predict
mortality in a population-representative cohort of people. CMAJ 2011; 83: 1-8.
http://www.cmaj.ca/content/183/14/E1059.full.pdf+html or
http://www.slideshare.net/DrAMSharma/edmonton-obesity-staging-system 77. NHS Diabetes. Joint British Diabetes Societies Inpatient Care Group. Management of adults with diabetes
undergoing surgery and elective procedures: improving standards. April 2011.
http://www.diabetes.nhs.uk/document.php?o=224 78. Baillot A et al. Effects of lifestyle interventions that include a physical activity component in class II and III obese
individuals: a systematic review and meta-analysis. PLoS ONE [Electronic Resource] 2015; 10(4): e0119017. 79. Shah M et al. High-volume exercise program in obese bariatric surgery patients: a randomized, controlled
trial. Obesity 2011; 19(9): 1826-1834. 80. Kim JJ, Rogers AM, Ballem N, Schirmer B on behalf of the American Society for Metabolic and Bariatric
Commissioning guide 2017 Weight assessment and management clinics
32
Surgery Clinical Issues Committee. ASMBS Guidelines/Statements ASMBS updated position statement on
insurance mandated preoperative weight loss requirements. Surgery for Obesity and Related Diseases
2016; 12: 955–959.
81. Wee CC, Pratt JS, Fanelli R, Samour PQ, Trainor LS, Paasche-Orlow MK. Best Practice Updates for Informed
Consent and Patient Education in Weight Loss Surgery. Obesity 2009; 17: 885-888.
Doi:10.1038/oby.2008.567.
http://onlinelibrary.wiley.com/store/10.1038/oby.2008.567/asset/oby.2008.567.pdf?v=1&t=hkcjikxt&s=f6
eb2cead109ff74692d54fe2ae7d6157b4a65c3
82. Academy of Nutrition and Dietetics (2015). 2015 Pediatric weight management evidence-based nutrition
practice guidelines. http://www.andeal.org/topic.cfm?menu=5296&cat=5632
83. Ells LJ et al. Surgery for the treatment of obesity in children and adolescents. Cochrane Database of
Systematic Reviews(6). 2015. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011740/abstract
84. Brei, M. N. and S. Mudd. Current guidelines for weight loss surgery in adolescents: a review of the
literature. J Pediat Health Care 2014; 28(4): 288-294.
85. Black JA et al. Bariatric surgery for obese children and adolescents: a systematic review and meta-analysis.
Obesity Reviews 2013; 14(8): 634-644. 86. Paulus GF, de Vaan LEG, Verdam FJ et al. Obes Surg 2015; 25: 860–878. doi:10.1007/s11695-015-1581-2. 87. Taylor RW et al. A Tailored Family-Based Obesity Intervention: A Randomized Trial. Pediatrics 2015; 136(2):
281-289. 88. Harder-Lauridsen NM et al. A randomized controlled trial on a multicomponent intervention for
overweight school-aged children - Copenhagen, Denmark. BMC Pediatrics 2014; 14: 273. 89. Wright N, Wales J. Assessment and management of severely obese children and adolescents. Arch Dis
Child 2016; 101: 1161–1167. doi:10.1136/archdischild-2015-309103 90. Viner RM, White B, Barrett T, Candy DCA, Gibson P, Gregory JW et al. Assessment of childhood obesity in
secondary care: OSCA consensus statement. Arch Dis Child Educ Pract Ed 2012; 97: 98–105. doi:10.1136/edpract-2011-301426
91. Wake, M., et al. Shared care obesity management in 3-10 year old children: 12 month outcomes of HopSCOTCH randomised trial. BMJ 2013; 346: f3092.
92. Christie D, Viner R. Chronic illness and transition: time for action. Adolesc Med State Art Rev. 2009; 20(3):
981-7.
93. Patton GC et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016 Jun
11; 387(10036): 2423-78.
94. Wadden TA, Sarwer DB. Behavioral Assessment of Candidates for Bariatric Surgery: A Patient-Oriented Approach. Obesity 2006; 14: 53S-62S. http://onlinelibrary.wiley.com/doi/10.1038/oby.2006.283/full
95. Karmali S, Brar B, Shi X, Sharma AM, de Gara C, Birch DW. Weight recidivism post-bariatric surgery: a
systematic review. Obesity Surgery 2013; 23(11): 1922-1933.
96. Too Lean a Service? A review of the care of patients who underwent bariatric surgery. A report by the National Confidential Enquiry into Patient Outcome and Death (2012)
97. Sarwer DB, Dilks RJ, West-Smith L. Dietary intake and eating behavior after bariatric surgery: threats to weight loss maintenance and strategies for success. Surg Obes Relat Dis 2011; 7: 644–651.
98. Shantavasinkul PC, Torquati A, Corsino L. Post-gastric bypass hypoglycaemia: a review. Clin Endocrinol (Oxf). 2016 Jul; 85(1): 3-9. doi: 10.1111/cen.13033. PMID: 26840207
99. BOMSS Guidelines on perioperative and postoperative biochemical monitoring and micronutrient
Commissioning guide 2017 Weight assessment and management clinics
33
replacement for patients undergoing bariatric surgery. 2014. http://www.bomss.org.uk/wp-content/uploads/2014/09/BOMSS-guidelines-Final-version1Oct14.pdf
100. Ogden J et al. The impact of psychological support on weight loss post weight loss surgery: a randomised control trial. Obesity Surgery 2015; 25(3): 500-505.
101. Mengesha B, Griffin L, Nagle A, Kiley J. Assessment of contraceptive needs in women undergoing bariatric surgery. Contraception. 2016 Jul;94(1):74-7. doi: 10.1016/j.contraception.2016.02.027
102. Richman RM, Webster P, Salgo AR, Mira M, Stenbeck KS, Caterson ID. A shared care approach in
obesity management: the general practitioner and a hospital based service. Int J Obes Relat Metab Disord
1996; 20: 413-9. http://www.ncbi.nlm.nih.gov/pubmed/8696419
103. Rudolph A, Hilbert A. Post‐operative behavioural management in bariatric surgery: a systematic
review and meta‐analysis of randomized controlled trials. Obes Reviews 2013; 14(4): 292-302.
104. Biörserud C, Olbers T, Fagevik Olsén M. Patients’ experience of surplus skin after laparoscopic
gastric bypass. Obes Surg 2011; 21(3): 273–7.
105. Rutledge T, Adler S, Friedman R. A prospective assessment of psychosocial factors among bariatric
versus non-bariatric surgery candidates. Obes Surg 2011; 21(10): 1570–9.
106. Kruseman M, Leimgruber A, Zumbach F, Golay A. Dietary, weight, and psychological changes
among patients with obesity, 8 years after gastric bypass. J Am Diet Assoc 2010; 110(4): 527–34.
107. Kubik JF, Gill RS, Laffin M, Karmali S. The impact of bariatric surgery on psychological health. J Obes
2013; 2013: 837989.
108. de Zwaan M, Enderle J, Wagner S, Mühlhans B, Ditzen B, Gefeller O, Mitchell JE, Müller A. Anxiety
and depression in bariatric surgery patients: a prospective, follow-up study using structured clinical
interviews. J Affective Disorders 2011;133(1): 61-68.
109. King WC, Chen JY, Mitchell JE, Kalarchian MA, Steffen KJ, Engel SG, Courcoulas AP, Pories WJ and
Yanovski SZ.. Prevalence of alcohol use disorders before and after bariatric surgery. JAMA 2012; 307(23):
2516-2525.
110. Lent MR, Napolitano MA, Wood GC, Argyropoulos G, Gerhard GS, Hayes S, Foster GD, Collins CA,
Still CD. Internalized weight bias in weight-loss surgery patients: psychosocial correlates and weight loss
outcomes. Obesity Surgery 2014; 24(12): 2195-2199.
111. Moore M, Hopkins J, Wainwright P. Primary care management of patients after weight loss
surgery. BMJ 2016; 352 352: i945. doi: https://doi.org/10.1136/bmj.i945
112. Woodlief TL et al. Dose response of exercise training following roux-en-Y gastric bypass surgery: A randomized trial. Obesity 2015; 23(12): 2454-2461.
113. Coen PM et al. Clinical trial demonstrates exercise following bariatric surgery improves insulin sensitivity. Journal of Clinical Investigation 2015; 125(1): 248-257
114. BAPRAS/RCS NICE-Approved Commissioning Guidance on Body Contouring Surgery. 2014.
http://www.rcseng.ac.uk/healthcare-bodies/docs/published-guides/body-contouring-surgery
115. Jennings A, Hughes C A, Kumaravel B, Bachmann M, Steel N, Capehorn M and Cheema K.
Evaluation of a multidisciplinary Tier 3 weight management service for adults with morbid obesity, or
obesity and comorbidities, based in primary care. Clinical Obesity, 4: 254–266. doi: 10.1111/cob.12066.
Commissioning guide 2017 Weight assessment and management clinics
34
7.4 Guide development group for weight assessment and management clinics
A commissioning guide development group was established to review and advise on the content of the
commissioning guide. This group met twice, with additional interaction taking place via email.
Name Job Title/Role Affiliation
Mr Richard Welbourn Consultant Surgeon (Co-Chair) Past-President, British Obesity
and Metabolic Surgery Society,
RCS
Prof John Wass Professor of Endocrinology
(Co-Chair)
Past Academic Vice-President,
Royal College of Physicians
Dr Julian Barth Consultant Chemical
Pathologist
Association for Clinical
Biochemistry & Laboratory
Medicine
Mr Ken Clare Patient representative British Obesity and Metabolic
Surgery Society Council
member, WLSInfo patient
support group
Dr John Cousins Consultant Anaesthetist Royal College of Anaesthetists,
Society of Obesity and
Bariatric Anaesthesia
Mr Ashish Desai Consultant Paediatric Surgeon British Association of Paediatric Surgeons
Ms Alison Diamond Metabolic Dietitian - Ante-
natal Clinic
Royal College of Obstetrics and Gynaecology
Prof John Dixon Professor of Metabolic
Medicine
Baker IDI Heart and Diabetes
Institute, Melbourne,
Australia, invited international
expert member
Prof Nick Finer Hon Professor Association of Physicians
Specialising in Obesity-UK
Dr Rob Gregory Consultant Endocrinologist Association of British Clinical
Diabetologists
Mr James Hopkins Consultant Surgeon BOMSS, RCS
Dr Carly Hughes General Practitioner, Bariatric
Physician, Hon Lecturer,
Medical School, University of
East Anglia
Royal College of General
Practitioners, Association for
the Study of Obesity
Dr Nick Kennedy Consultant Anaesthetist Royal College of Anaesthetists,
Society of Obesity and
Commissioning guide 2017 Weight assessment and management clinics
35
Bariatric Anaesthesia
Prof David Kerrigan Consultant Surgeon BOMSS, RCS
Prof Carel le Roux Professor of Metabolic
Medicine
Royal College of Pathologists
Dr Lisa McClelland Consultant Psychiatrist Royal College of Psychiatrists
Dr Barbara McGowan Consultant Endocrinologist
and Honorary Senior Lecturer
at Guys & St Thomas's
Hospital, London
Metabolic and Obesity
Network Lead and Treasurer
for Society for Endocrinology,
Trustee of ASO
Ms Iris McMillan Patient representative Royal College of Surgeons
Patient Liaison Group, Obesity
Empowerment UK
Ms Mary O’Kane Consultant Dietitian British Obesity and Metabolic
Surgery Society Council
member, British Dietetic
Association
Dr Vicci Owen-Smith Clinical Director of Public
Health
Faculty of Public Health
Ms Gail Pinnock Dietitian British Obesity and Metabolic
Surgery Society Council
member, British Dietetic
Association
Ms Lisa Rickers Specialist Bariatric Nurse Royal College of Nursing
Ms Sue Sawyer Specialist Commissioner NHS England
Dr Vanessa Snowdon-Carr Lead Clinical Psychologist British Obesity and Metabolic
Surgery Society, British
Psychological Society
Douglas Twenefour Deputy Head of Care,
Diabetes UK
Diabetes UK
Prof Russell Viner Consultant Paediatrician Royal College of Paediatrics
and Child Health
Ms Claire Woods Specialist Bariatric Nurse Royal College of Nursing
7.5 Funding statement
The development of this commissioning guidance has been funded by the following sources:
Department of Health Right Care funded the costs of the guide development group, literature searches
and contributed towards administrative costs.
The Royal College of Physicians provided premises to support the guideline development.
Commissioning guide 2017 Weight assessment and management clinics
36
7.6 Conflict of Interest Statement
Individuals involved in the development and formal peer review of commissioning guides are asked to complete a
conflict of interest declaration. It is noted that declaring a conflict of interest does not imply that the individual
has been influenced by his or her secondary interest. It is intended to make interests (financial or otherwise)
more transparent and to allow others to have knowledge of the interest.
Name Position Declared Interest
Dr Julian Barth Consultant in Chemical Pathology & Metabolic Medicine
None
Mr Ken Clare Chair of Trustees WLSInfo NovoNordisk consultancy fees, speaker fees as key opinion leader
Sponsorship fees for attending conference Dr John Cousins Consultant Anaesthetist Fees for consultancy MSD – Sugammadex
advisory board
Fees for speaking at meeting/symposium – MSD, Medtronic
Mr Ashish Desai Consultant Paediatric
Surgeon
None
Ms Alison Diamond Metabolic Dietitian - Ante-
natal Clinic
None
Prof John Dixon Professor, NHMRC Senior Research Fellow, Head Clinical Obesity
Research, Baker Heart and
Diabetes Institute
Melbourne, Australia
Consultancy fees NovoNordisk, Apollo EndoSurgery, Medtronics, Bariatric Advantage, Nestlé Health Science
Advisory Board and Speaker fees iNova, Novartis
Prof Nick Finer Hon Consultant, Senior
Principal Clinical Scientist,
Global Medical Affairs,
Novo Nordisk A/G
Currently employed by Novo Nordisk – manufacturer of pharmacological treatments for obesity
Speaker fees and sponsorship for conference attendance Novo Nordisk
Dr Rob Gregory Consultant Endocrinologist None
Mr James Hopkins Consultant Surgeon None
Dr Carly Hughes Bariatric Physician
Fakenham weight
management service,
Associate Tutor and Hon
Lecturer at University of
East Anglia
Consultancy fees Orexigen, Mundipharma, Oviva, Nutricia, ActiveNorfolk
Speaker fees from academic conferences on obesity and diabetes Ethicon, Novo Nordisk
Clinical advisor Kastech (unpaid)
Dr Nick Kennedy Consultant Anaesthetist Secondary Care Clinician on Governing Body of South Gloucestershire CCG
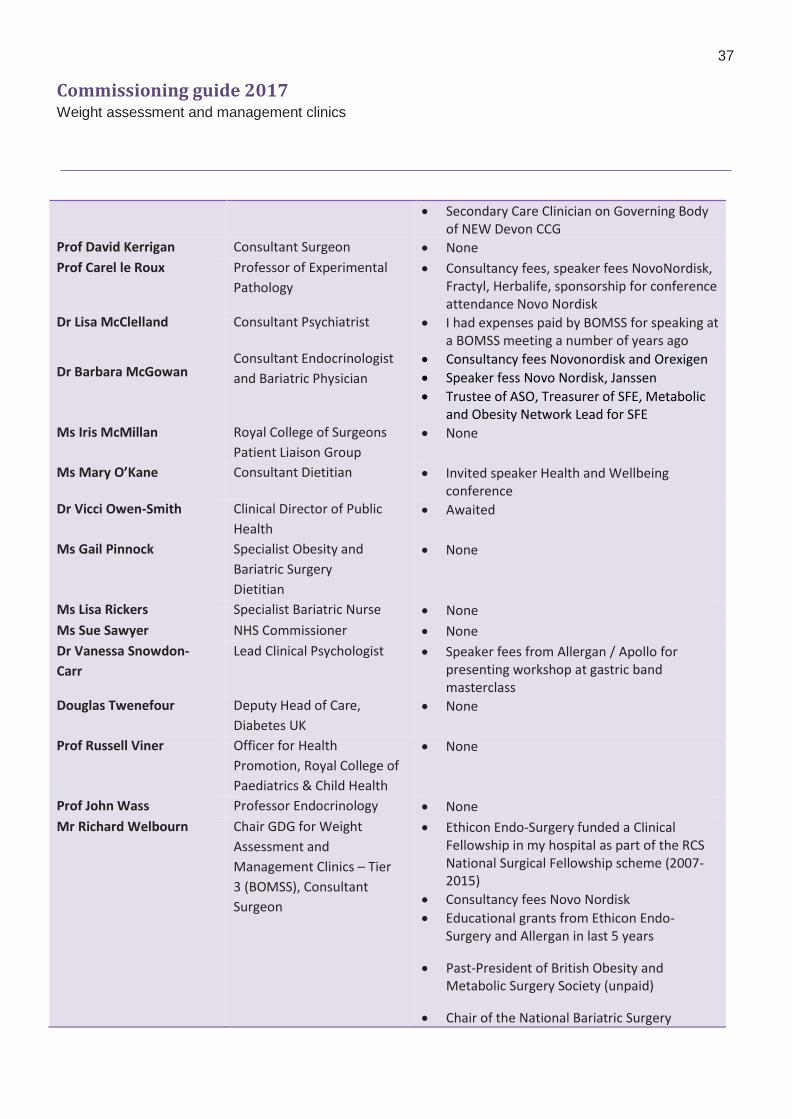
Commissioning guide 2017 Weight assessment and management clinics
37
Secondary Care Clinician on Governing Body of NEW Devon CCG
Prof David Kerrigan Consultant Surgeon None
Prof Carel le Roux Professor of Experimental
Pathology
Consultancy fees, speaker fees NovoNordisk, Fractyl, Herbalife, sponsorship for conference attendance Novo Nordisk
Dr Lisa McClelland Consultant Psychiatrist I had expenses paid by BOMSS for speaking at a BOMSS meeting a number of years ago
Dr Barbara McGowan Consultant Endocrinologist
and Bariatric Physician
Consultancy fees Novonordisk and Orexigen
Speaker fess Novo Nordisk, Janssen
Trustee of ASO, Treasurer of SFE, Metabolic and Obesity Network Lead for SFE
Ms Iris McMillan Royal College of Surgeons
Patient Liaison Group
None
Ms Mary O’Kane Consultant Dietitian Invited speaker Health and Wellbeing conference
Dr Vicci Owen-Smith Clinical Director of Public
Health
Awaited
Ms Gail Pinnock Specialist Obesity and
Bariatric Surgery
Dietitian
None
Ms Lisa Rickers Specialist Bariatric Nurse None
Ms Sue Sawyer NHS Commissioner None
Dr Vanessa Snowdon-
Carr
Lead Clinical Psychologist Speaker fees from Allergan / Apollo for presenting workshop at gastric band masterclass
Douglas Twenefour Deputy Head of Care,
Diabetes UK
None
Prof Russell Viner Officer for Health
Promotion, Royal College of
Paediatrics & Child Health
None
Prof John Wass Professor Endocrinology None
Mr Richard Welbourn Chair GDG for Weight
Assessment and
Management Clinics – Tier
3 (BOMSS), Consultant
Surgeon
Ethicon Endo-Surgery funded a Clinical Fellowship in my hospital as part of the RCS National Surgical Fellowship scheme (2007-2015)
Consultancy fees Novo Nordisk
Educational grants from Ethicon Endo-Surgery and Allergan in last 5 years
Past-President of British Obesity and Metabolic Surgery Society (unpaid)
Chair of the National Bariatric Surgery
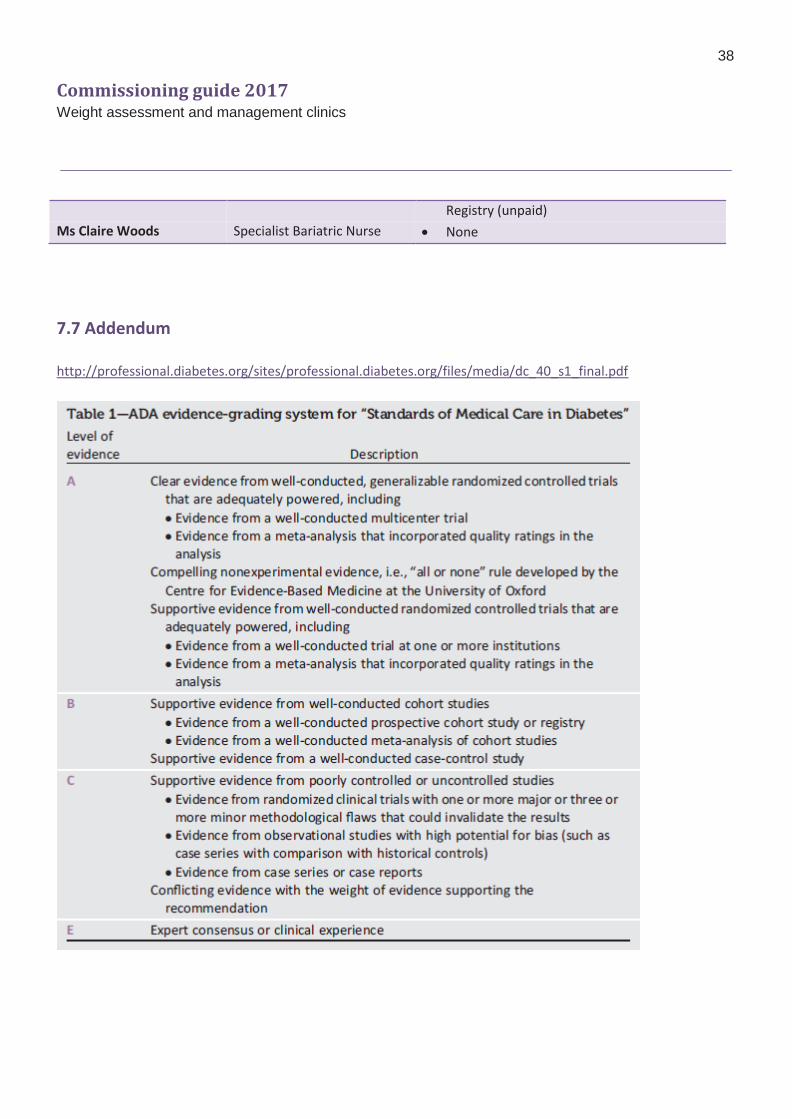
Commissioning guide 2017 Weight assessment and management clinics
38
Registry (unpaid)
Ms Claire Woods Specialist Bariatric Nurse None
7.7 Addendum
http://professional.diabetes.org/sites/professional.diabetes.org/files/media/dc_40_s1_final.pdf