Embed Size (px)
Citation preview

Aneurysms and arterial dissections of the Craniocervical Junction
Department of Neurosurgery Kameda Medical Center
Chiba JAPANConflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Michihiro TANAKA,M.D., Ph.D.
2017 ABC/WIN@ Val d'Isère Anatomy-Biology-Clinical correlations -Working group in Interventional Neuroradiology
Menu
1. Anatomical consideration of craniocervical junction
2. Pathology of arterial dissections
3. Imaging modalities and the clinical application
Key words: Dissections, Internal Elastic Lamina,
Segmental vulnerability, Lateral spinal artery , Homology
3Anatomic vulnerability associated with kinematics of craniocervical junction
Various types of vertebral artery (VA) anomalies in cases of congenital atlantoaxial dislocation (CAAD) have been shown in posterior and lateral views.
Salunke et al. Surg Neurol Int. 2014; 5: 82.
Salunke et al. Surg Neurol Int. 2014; 5: 82. Salunke et al. Surg Neurol Int. 2014; 5: 82.
Persistent FIA(first
intersegmental artery)
The causes of vertebral artery dissection can be grouped under two main categories, spontaneous and traumatic.
Spontaneous
Spontaneous cases are considered to be caused by intrinsic factors that weaken the arterial wall. Only a very small proportion (1–4%) have a clear underlying connective tissue disorder, such as Ehlers–Danlos syndrome type 4 and more rarely Marfan's syndrome. Ehlers-Danlos syndrome type 4, caused by mutations of the COL3A gene, leads to defective production of the collagen Marfan's syndrome results from mutations in the FBN1 gene, defective production of the protein fibrillin-1.
Other genetic conditions, such as osteogenesis imperfecta type 1, autosomal dominant polycystic kidney disease and pseudoxanthoma elasticum, α1 antitrypsin deficiency and hereditary hemochromatosis, but evidence for these associations is weaker.
Atherosclerosis does not appear to increase the risk. (Kim et al. Thrombosis research 2009)
There have been numerous reports of associated risk factors for vertebral artery dissection; many of these reports suffer from methodological weaknesses, such as selection bias. Elevated homocysteine levels, often due to mutations in the MTHFR gene, appear to increase the risk of vertebral artery dissection.
People with an aneurysm of the aortic root and people with a history of migraine may be predisposed to vertebral artery dissection.
Table 1 Pathophysiological risk factors for CAD
Risk Factor Basis
Connective TissueAbnormalities52,56
Skin Biopsies of 68% of 25 and 55% of 65 CAD Patients Showed Evidence of IrregularCollagen Fibrils and Fragmentation of Elastic Fibers That Is Thought to Weaken theArterial Wall.
Vascular Type IV Ehlers-Danlos Syndrome52,57,58
and Marfan Syndrome59
These Inherited Connective Tissue Disorders Affect the Skin, Joints, and the Walls ofBlood Vessels. The Incidence of CAD Has Been Reported to Be Higher in Patients WithThese Conditions.
Recent Infection60-62 Case-Control Studies Point to Recent Infection as a Potential Trigger of CAD, PossiblyRelated to Arterial Wall Damage Caused by Proteolytic, Oxidative, or AutoimmuneDefects. Furthermore, the Incidence of CAD Has Been Reported to Be Higher DuringCertain Seasons, Which May Be Related to the Higher Incidence of Upper RespiratoryTract Infections During the Winter.
Hyperhomocysteinemia63-66 Especially Apparent in Patients With Total Plasma Levels That Exceed 12 μmol/L. AssociatedArterial Wall Abnormalities May Increase the Artery's Susceptibility to Mechanical Stress.
FibromuscularDysplasia28,67
Affects the ICA More Commonly Than the VA. Present in Up to 23% of ICA DissectionPatients, Making It the Most Frequently Reported Associated Abnormality. Characterizedby Irregular Segments of Stricture and Dilation in the Vessel.
Cystic Medial Necrosis2 Focal Degeneration of the Elastic Tissue and Muscle of the Tunica Media, With theDevelopment of Mucoid Material. There Is a Breakdown of the Collagen, Elastin, andSmooth Muscle, and an Increase in the Artery's Ground Substance.
Type 1 OsteogenesisImperfecta68
Interferes With the Production of Type 1 Collagen. In Some Cases, Collagen Synthesis IsDecreased, Whereas in Others, Structurally Defective Collagen Is Produced.
AnatomicalAbnormalities12,69-72
May Result in Blood Flow Disturbance Leading to Insufficient Collateral Circulation.The Atlantal Segment of the VA Is Commonly Anomalous. Arterial Redundancies (eg,Coils, Kinks, and Loops) and Increased Diameter of the Common Carotid Artery AreMore Common in Patients With ICA Dissection.
Hypertension14,73-75 Several Studies Have Pointed to Hypertension as a CAD Risk Factor. A Well-DesignedCase-Control Study Reported a Statistically Significant Association in the Subgroup ofVA Dissection Patients, but Not in the Overall CAD Group.
History of Migraine76-78 Robust Odds Ratios Have Been Generated in Several Case-Control Studies Pointing toThis Association—7.41 (95% CI 3.11-17.64) in 1 Study.
Autosomal DominantPolycystic KidneyDisease79,80
Has Been Reported in Association With CAD by Several Authors, Although the Frequencyof This Association and the Mechanism Involved Are Unknown.
AntithyroidAutoimmunity81,82
A Recent Case-Control Study Reported the Presence of Antithyroid Autoimmunity in31.0% of 29 CAD Patients, Compared With 6.9% of 29 Non-CAD Stroke Patients(P = .041). There Have Also Been Recent Case Reports of ICA Dissection in PatientsWith Graves Disease. Immunologic Mechanisms May Contribute to the VascularDamage That Is Thought to Initiate CADs.
EE Genotype of the E469KICAM-1 Polymorphism83
The EE Genotype Gives Rise to a Proinflammatory Tendency in Patients That MayPredispose Them to Developing CAD.
MethylenetetrahydrofolateReductase C677TGenotype63,65,66,84
Mutation of This Genotype Leads to Elevated Serum Levels of Homocysteine. The IssueIs Controversial Because Studies Have Not Been in Agreement.
α-1-AntitrypsinDeficiency85-87
Researchers Have Theorized That This Deficiency May Lead to a Fragile Vessel Wall ThatIs Predisposed to Dissection, but There Is Little Evidence to Support This Relationship. Onlya Few Small Studies Have Reported on This Association, and Their Results Are Conflicting.
Oral ContraceptiveUse60,77,78
Studies That Have Considered This Issue Are in Conflict. Only 1 Small Study ShowedThat Current Use of Oral Contraceptives Was Associated With CAD. The Consensus ofResearchers Is That No Good Evidence Exists Supporting This Association.
Cardiovascular RiskFactors10,14,61,78,88
May Actually Be Protective. Atherosclerotic Changes, Hypercholesterolemia, AdvancedAge, and Diabetes Are Reported to Be Either Not Associated or Significantly LessPrevalent in CAD Patients.
CI indicates confidence interval; ICAM-1, intracellular adhesion molecule 1.
116 M. T. Haneline, A. L. Rosner
There are at least 25 of postulated risk factors.
Why we have to rotate the atlanto-axial joint ? It is necessary to compensate the blind zone.
Modern life is creating stress and stress.
Chiropractics sometimes gives us, not only the relaxation, but also the mechanical stress to VA. Case 1. A 57 year-old-man presented TIA after chiropractic treatment.
Pre
Post Post (High resolution CBCT)
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

High resolution CBCT
Metal artifact reduction
Case 2. A 58 year-old-man, who had a fall accident, presented with TIA.
Transection of IEL (Internal Elastic Lamina)
Lustrin ES et al. Pediatric cervical spine: Normal anatomy, variants, and trauma. Radiographics 2003; 23:539-60.
Note the dislocation of the both foramen transversarium
Golf can be a risk factor for VA dissections.
Nine dissections were found on the right side, 3 on the left side, and 2 were bilateral (P =.046). Choi M et al. AJNR 2014;35:323-326
logic signs and symptoms, treatment, and clinical outcomes. Wealso analyzed radiologic findings such as stroke location (anterioror posterior circulation), side of arterial dissection (right, left, orboth), and anatomic location of the dissection (extracranial orintracranial). Status at symptom onset was classified as duringswing, after golf exercise, and unknown. Clinical outcome wascategorized as returned to normal (mRS ! 0 –1), independent(mRS ! 2–3), dependent (mRS ! 4 –5), and death (mRS ! 6) atdischarge.11 Differences between the stroke location, side of dis-section, and anatomic location of the dissection were analyzed byuse of the !2 test. Statistical significance was considered atP " .05.
RESULTSFourteen male patients were examined. The demographic andclinical-radiologic findings are provided in the On-line Table.The mean age of the patients was 46.9 # 12.8 years, which wasyounger than that of the general stroke population. Seven patientswere right-handed. Of the 7 patients, 2 were professional golferswith 15–17 years of experience, and the remaining patients wereamateur players with playing experience for approximately 7years (range, 0.1–30 years). None of the patients had a history ofhypertension, diabetes, or autoimmune disorder. Symptom onsetoccurred during the golf swing (n ! 9), at an unknown time (n !3), or after golf playing (n ! 2). Twelve patients had posteriorcirculation symptoms such as vertigo, nystagmus, and body tilt-
ing. Eight patients had localized pain at symptom onset. A poten-tial source for vasculopathies and cardioembolic stroke was ex-cluded from laboratory and cardiologic studies.
The location of arterial dissection was confirmed by cerebralangiography (n ! 11), MR angiography (n ! 2), and Dopplerultrasound (n ! 1). The imaging studies revealed that 12 patientshad involvement of the vertebral artery (VA) and 2 patients hadICA involvement (P ! .008). Nine patients had arterial dissec-tions on the right side, of which 2 had ICA involvement; 3 had leftside involvement; and 2 had bilateral lesions (P ! .046). Therewere 12 extracranial and 2 intracranial cases (P ! .008). Normalactivity was possible in 7 patients, but the other cases revealed 5independent patients and 1 death (On-line Table). Radiologicfindings (stroke location and dissection focus) of our 7 cases areshown in Fig 1.
DISCUSSIONOur study illustrates that arterial dissection from golf-relatedstroke was more likely to be on the right side and predominantlyin the extracranial vertebrobasilar system. This preference may beexplained by the anatomic vulnerability of the vertebrobasilar sys-tem and the biomechanics of the golf swing.
Recent studies on ethnic differences in spontaneous vertebralartery dissection have shown that intracranial dissection is morecommon than extracranial dissection in East Asian populations.7
Our study of golf-related vertebral artery dissection shows that
FIG 1. Radiologic findings (stroke location, dissection focus, and follow-up) of our 7 cases. Five cases had right-sided involvement: 3 patients(cases 1–3) with extracranial vertebral artery, 1 with intracranial VA (case 4), and 1 with extracranial carotid artery (case 5). One patient (case 6) hada left extracranial VA and 1 patient (case 7) had bilateral intracranial VA involvement. Black arrows indicate the dissection focus or foci. Dottedrectangles indicate follow-up images of dissection focus or foci.
324 Choi Feb 2014 www.ajnr.org
logic signs and symptoms, treatment, and clinical outcomes. Wealso analyzed radiologic findings such as stroke location (anterioror posterior circulation), side of arterial dissection (right, left, orboth), and anatomic location of the dissection (extracranial orintracranial). Status at symptom onset was classified as duringswing, after golf exercise, and unknown. Clinical outcome wascategorized as returned to normal (mRS ! 0 –1), independent(mRS ! 2–3), dependent (mRS ! 4 –5), and death (mRS ! 6) atdischarge.11 Differences between the stroke location, side of dis-section, and anatomic location of the dissection were analyzed byuse of the !2 test. Statistical significance was considered atP " .05.
RESULTSFourteen male patients were examined. The demographic andclinical-radiologic findings are provided in the On-line Table.The mean age of the patients was 46.9 # 12.8 years, which wasyounger than that of the general stroke population. Seven patientswere right-handed. Of the 7 patients, 2 were professional golferswith 15–17 years of experience, and the remaining patients wereamateur players with playing experience for approximately 7years (range, 0.1–30 years). None of the patients had a history ofhypertension, diabetes, or autoimmune disorder. Symptom onsetoccurred during the golf swing (n ! 9), at an unknown time (n !3), or after golf playing (n ! 2). Twelve patients had posteriorcirculation symptoms such as vertigo, nystagmus, and body tilt-
ing. Eight patients had localized pain at symptom onset. A poten-tial source for vasculopathies and cardioembolic stroke was ex-cluded from laboratory and cardiologic studies.
The location of arterial dissection was confirmed by cerebralangiography (n ! 11), MR angiography (n ! 2), and Dopplerultrasound (n ! 1). The imaging studies revealed that 12 patientshad involvement of the vertebral artery (VA) and 2 patients hadICA involvement (P ! .008). Nine patients had arterial dissec-tions on the right side, of which 2 had ICA involvement; 3 had leftside involvement; and 2 had bilateral lesions (P ! .046). Therewere 12 extracranial and 2 intracranial cases (P ! .008). Normalactivity was possible in 7 patients, but the other cases revealed 5independent patients and 1 death (On-line Table). Radiologicfindings (stroke location and dissection focus) of our 7 cases areshown in Fig 1.
DISCUSSIONOur study illustrates that arterial dissection from golf-relatedstroke was more likely to be on the right side and predominantlyin the extracranial vertebrobasilar system. This preference may beexplained by the anatomic vulnerability of the vertebrobasilar sys-tem and the biomechanics of the golf swing.
Recent studies on ethnic differences in spontaneous vertebralartery dissection have shown that intracranial dissection is morecommon than extracranial dissection in East Asian populations.7
Our study of golf-related vertebral artery dissection shows that
FIG 1. Radiologic findings (stroke location, dissection focus, and follow-up) of our 7 cases. Five cases had right-sided involvement: 3 patients(cases 1–3) with extracranial vertebral artery, 1 with intracranial VA (case 4), and 1 with extracranial carotid artery (case 5). One patient (case 6) hada left extracranial VA and 1 patient (case 7) had bilateral intracranial VA involvement. Black arrows indicate the dissection focus or foci. Dottedrectangles indicate follow-up images of dissection focus or foci.
324 Choi Feb 2014 www.ajnr.org
Mechanical explanation for the predominance of the right vertebral artery (VA) dissection during a golf swing.
Choi M et al. AJNR 2014;35:323-326
There are many stress in modern society…Case 3. A 37 year-old-woman wanted to make her car parking in proper position. After few minutes, she presented with severe dizziness, vertigo and right hand ataxia.
NeuroformR 4×30mm
Authentic bow does not compromise the vertebral artery. Functional anatomy of craniocervical junction
ASA and anterior medullary perforators from the union of vertebro-basilar artery. www.centauro.it Interventional Neuroradiology 14: 49-58, 2008
49
teries arise 1,4,5,7-10,12-17. From these arteries alsoemerge the lateral spinal arteries responsiblefor the vascularization of the posterior surfaceof the medulla oblongata 6,11.
This region is increasingly solicited in inter-ventional neuroradiological procedures for em-bolization or arterial aneurysm, dissections, ar-teriovenous malformations, dural fistula or re-pair of an occlusive disease. The proceduressometimes require occlusion of an intraduralsegment of the vertebral artery, occasionally in-cluding the origin of the PICA.
Knowledge of the role of pre- and post-PI-CA segments of the intradural vertebral arteryin pontine vascularization is therefore vital, andthis anatomy should even be envisaged so as toanticipate the risk for lateral ischemia after en-dovascular treatment.
Material and Methods
For the present study, we used 25 brains fromsubjects who had given their bodies to medi-cine. These bodies had been injected with aformaldehyde solution 1-2 weeks before thestudy; the head was then sectioned at the lowercervical level. The vertebral and carotid arterieswere then catheterized and, after washing withsoapy water followed by acetone, neoprene 671A (Safic-Alcan) was injected in 23 cases in acarotid artery until reflux was obtained in the
Summary
This study of 25 brains at the pontomedullaryjunction defined the different possible origins ofthe perforating arteries and lateral spinal arter-ies in relation to the posterior inferior cerebellararteries (PICAs).
- If the PICA emerges from the commontrunk of the AICA-PICA coming from the basi-lar artery, it never gives perforating arteries or alateral spinal artery on the lateral surface of thebrain stem but supplies blood to a part of the ip-silateral cerebellar hemisphere.
- If the PICA arises extradurally at C1, it nev-er gives perforating arteries for the lateral sur-face of the brain stem, but it gives pial branchesfor the posterior surface of the medulla oblon-gata and is always the origin of the lateral spinalartery.
- If the PICA emerges in the intradural verte-bral artery, it is the source of the perforating ar-teries for the lateral surface of the brain stemand of the blood supply of the ipsilateral cere-bellum.
Introduction
The pontomedullary junction is supplied bythe confluence of the vertebral and basilar ar-teries and the posterior inferior cerebellar ar-teries, where a large number of perforating ar-
Vascular Microanatomyof the Pontomedullary Junction,Posterior Inferior Cerebellar Arteries,and the Lateral Spinal Arteries
PH. MERCIER, G. BRASSIER**, H-D FOURNIER, J. PICQUET, X. PAPON,P. LASJAUNIAS*Laboratoire d’Anatomie, Faculté de Médecine, Angers cédex, France* Département de Neuroradiologie, avenue du Gal Leclerc, Hôpital Bicêtre, le Kremlin, France ** Université de Rennes 1, Rennes, France
Key words: medulla oblongata, posterior inferior cerebellar artery (PICA), perforating arteries, lateral spinal artery
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

AICA
PICA
ASA
anterior medullary
perforatorsRight lateral view showing the caudal loop of the PICA. No perforating arteries emerge from the vertebral artery under the PICA’s emergence. Fig.12Mercier P. et al. INR 2008
AICA
PICA
ASA and anterior medullary perforators
AICA
PICA
ASA
anterior medullary
perforators
ASA and anterior medullary perforators originating from the VA distal to the orifice of PICA. Rt.perforators originating relatively lower part of V4 portion that is at least 10mm apart from the union.
Mercier P. et al. INR 2008
Pair of ASAs originate from both fenestrated trunk.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

1. Basilar trunk fenestration: 156 (1.29%)
2. Anterior communicating artery fenestration: 91(0.75%)
3. Persistent primitive trigeminal artery :82 (0.68%)
4. Accessorius or duplication of middle cerebral artery: 69 (0.57%)
5. Azygos A2: 28(0.23%)
6. Primitive dorsal ophthalmic artery: 6 (0.05%)
7. Middle cerebral artery (M1) fenestration: 4 (0.04%)
8. Infraoptic course of anterior cerebral artery: 3 (0.025%)
9. Persistent hypoglossal artery 7 (0.06)
Anatomical variation: Results from 12056 cases of MRA (2004~2006)
2~3/100000 Double fenestrations of basilar trunk Triple fenestrations of basilar trunk
www.centauro.it Interventional Neuroradiology 11 (Suppl 1): 000-000, 2005
1
tration studied by magnetic resonance (MR)angiography are rare 2.The purpose of this studyis to report the incidence of BA fenestration de-lineating its configurations and to investigatethe associated other vascular disease based onlarge series of cranial MR angiography.
Material and MethodsPatients
Between April 2004 and September 2004, atotal of 2280 cranial MR angiographies wereperformed at our institution. These 2280 con-secutive patients consisted from 1013 femalesand 1267 males.
The mean age of the patients at the time ofexamination was 61.8 ± 14.5 (mean ± standarddeviation) years (range 0-95 years). In this se-ries, there were 403 cases of asymptomatic pa-tients for brain check including screening stud-ies, 523 cases presented with headache but noremarkable neuroradiological abnormality, 365cases with vertigo and/or tinnitus without neu-roradiological findings and 859 cases diagnosedas a stroke including asymptomatic lacuna in-farction.
MRI and Radiological FindingsAll patients were studied with two of 1.5 Tes-
la units (SIEMENS, Magnetome VISION andGE,Excite) and one of 1.0 Tesla unit (SIE-
Summary
Basilar artery (BA) fenestrations are the mostfrequently observed variant of the cerebral arter-ies. We examined the magnetic resonance (MR)angiographic incidence, location, characteristicconfiguration of BA fenestration and associatedvascular disease.
From April 2004 to September 2004, a total of2280 cranial MR angiographies were performedat our institution. Twenty-three BA fenestrations(1.0%) were detected on MRA. There were 13males and ten females in this group and meanage was 57.6 years old. Three cases of these fen-estration group are suffered with atherothrombicinfarction in the territory of vertebro-basilar sys-tem. Seven of 23 cases (30%) were associatedwith intracranial aneurysm. Of those four cases,aneurysms were located at anterior circulation.Of those three cases, the aneurysms were associ-ated with BA fenestration. Since saccular aneur-ysms are reported to arise frequently at BA fen-estration, knowledge and recognition of fenestra-tion are useful and important in the interpreta-tion of cerebral MR angiography.
Introduction
The incidence of basilar artery (BA) fenestra-tion was reported to be 0.6~1.7 % based on an-giography 1,2,3,4. However, reports of BA fenes-
Neuroradiological Analysis of 23 Casesof Basilar Artery Fenestration Basedon 2280 Cases of MR Angiographies
M. TANAKA, Y. KIKUCHI*, T .OUCHI*Department of Neurosurgery and Radiology*, Kameda Medical Center; Chiba, Japan
Key words: basilar artery, fenestration, MR angiographywww.centauro.it Interventional Neuroradiology 11: 000-000, 2005
3
other across the midline. During the secondstage of development, at five weeks’ gestation,fusion of the channels gradually starts to form
the basilar artery. When the paired longitudinalneural arteries fail to fuse, fenestration may oc-cur anywhere along the course of the basilar
Figure 1 Type I: fenestration locating proximal to AICA, Type II: bilateral AICA symmetrically originating from the fen-estrated trunk, Type III: unilateral AICA originating one side of the fenestrated trunk, Type IV: fenestration locating distalto AICA.
A
C
D
B
www.centauro.it Interventional Neuroradiology 11: 000-000, 2005
3
other across the midline. During the secondstage of development, at five weeks’ gestation,fusion of the channels gradually starts to form
the basilar artery. When the paired longitudinalneural arteries fail to fuse, fenestration may oc-cur anywhere along the course of the basilar
Figure 1 Type I: fenestration locating proximal to AICA, Type II: bilateral AICA symmetrically originating from the fen-estrated trunk, Type III: unilateral AICA originating one side of the fenestrated trunk, Type IV: fenestration locating distalto AICA.
A
C
D
B
www.centauro.it Interventional Neuroradiology 11: 000-000, 2005
3
other across the midline. During the secondstage of development, at five weeks’ gestation,fusion of the channels gradually starts to form
the basilar artery. When the paired longitudinalneural arteries fail to fuse, fenestration may oc-cur anywhere along the course of the basilar
Figure 1 Type I: fenestration locating proximal to AICA, Type II: bilateral AICA symmetrically originating from the fen-estrated trunk, Type III: unilateral AICA originating one side of the fenestrated trunk, Type IV: fenestration locating distalto AICA.
A
C
D
B
www.centauro.it Interventional Neuroradiology 11: 000-000, 2005
3
other across the midline. During the secondstage of development, at five weeks’ gestation,fusion of the channels gradually starts to form
the basilar artery. When the paired longitudinalneural arteries fail to fuse, fenestration may oc-cur anywhere along the course of the basilar
Figure 1 Type I: fenestration locating proximal to AICA, Type II: bilateral AICA symmetrically originating from the fen-estrated trunk, Type III: unilateral AICA originating one side of the fenestrated trunk, Type IV: fenestration locating distalto AICA.
A
C
D
B
Tanaka M.et al. Interventional neuroradiology 2006
“Das Arteriensystem der Japaner”
Adachi B. Kyoto University 1928
The patient, who has been suffered from rt. hemifacial spasm for 10 years, presented increasing frequency and deterioration of the spasm. MRA and CT angiography revealed that this aneurysm is originating from proximal part of the fenestration of lower basilar trunk, and it's complex aneurysm invaginates into the brainstem where is adjacent to the rt.REZ of CN Ⅶ-Ⅷ complex.
Case Illustration : A 57y/o female with rt.hemifacial spasm
Multi detector high speed helical CT (64ch.)
Lower BA trunk saccular aneurysm associated with Type I fenestration invaginating into the REZ of CN VII-VII th complex.
CISS: Constructive Interference in Steady State
3DhelicalCTLt.VAG(RAO)
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

IntraaneurysmalflowcondiAon
Pre Post→ Cure of hemifacial spasm
completely Pre Post@6month
MRA 3D TOF
I. Basal Perforation Zones
Fig 138A-C Regular penetrating arteries arising from the most distal vertebral arteries (beyond the anterior spinal arteries) or most proximal basilar artery and entering the brain in the neighborhood of the foramen caecum. A Injected specimen. B Schematic drawing. C Formalin-fixed brain after the reflexion of the vertebro-basilar arteries. Perforators from basilar artery (arrows).
Ant. spin. A
Ic. Pontine Perforation Zone
The pontine perforation zone encompasses the basal surface of the pons. Here, in the surface denuded specimens, a linear array of perforation sites may be appreciated near the midline of the pons on its basal surface. Although generally small, the sites of this medial pontine group are consistently present and are not significantly influ-enced in their distribution by the often deviated course of the basilar artery. Additional perforation sites are seen scattered more laterally over the pons and brachium pontis to form a lateral pontine group (see Fig 124B-C). In latex injected specimens small branches from the undersurface of the basilar artery were seen to enter the medial pontine group while branches of the superior cerebellar and anterior inferior cere-bellar arteries were seen to enter the scattered sites noted more laterally.
Id. Basal Medullary Perforation Zone
Denuded specimens revealed rich arrays of perfo-ration sites on the basal surface of the medulla. One such array, the medial medullary group is evident in the midline extending from the foramen caecum caudally (see Fig 124B-C). The caudal limit of this group is not apparent and it clearly continues to spinal levels in the anterior median fissure. As shown in Figs 138A-C and 139A-C the two pyramids must be retracted laterally to expose two parallel paramedian rows of perforation sites, the largest of which are located rostrally at the foramen caecum. The sites become progressively smaller caudally.
155
AICA
PICA
I. Basal Perforation Zones
Fig 138A-C Regular penetrating arteries arising from the most distal vertebral arteries (beyond the anterior spinal arteries) or most proximal basilar artery and entering the brain in the neighborhood of the foramen caecum. A Injected specimen. B Schematic drawing. C Formalin-fixed brain after the reflexion of the vertebro-basilar arteries. Perforators from basilar artery (arrows).
Ant. spin. A
Ic. Pontine Perforation Zone
The pontine perforation zone encompasses the basal surface of the pons. Here, in the surface denuded specimens, a linear array of perforation sites may be appreciated near the midline of the pons on its basal surface. Although generally small, the sites of this medial pontine group are consistently present and are not significantly influ-enced in their distribution by the often deviated course of the basilar artery. Additional perforation sites are seen scattered more laterally over the pons and brachium pontis to form a lateral pontine group (see Fig 124B-C). In latex injected specimens small branches from the undersurface of the basilar artery were seen to enter the medial pontine group while branches of the superior cerebellar and anterior inferior cere-bellar arteries were seen to enter the scattered sites noted more laterally.
Id. Basal Medullary Perforation Zone
Denuded specimens revealed rich arrays of perfo-ration sites on the basal surface of the medulla. One such array, the medial medullary group is evident in the midline extending from the foramen caecum caudally (see Fig 124B-C). The caudal limit of this group is not apparent and it clearly continues to spinal levels in the anterior median fissure. As shown in Figs 138A-C and 139A-C the two pyramids must be retracted laterally to expose two parallel paramedian rows of perforation sites, the largest of which are located rostrally at the foramen caecum. The sites become progressively smaller caudally.
155
AICA
PICA
Menu
1. Anatomical consideration of craniocervical junction
2. Pathology of arterial dissections
3. Imaging modalities and the clinical application
Several studies have shown that pain is typically the first symptom associated with CAD, and a recent descriptive study involving 245 CAD patients reported that 8% of them presented with head or neck pain as their only symptom.
Several studies have shown that pain is typically the first symptom associated with CAD, and a recent descriptive study involving 245 CAD patients reported that 8% of them presented with head or neck pain as their only symptom.
Cervical artery dissection typically involves an initial tear in the artery lining. It may cause the layers to separate from each other forming a subintimal dissection.
A double lumen is formed when a subintimal hemorrhage ruptures back into the arterial lumen distally.
Subintimal dissection with thrombus formation.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

Emboli may detach from a primary thrombus and travel distally to obstruct progressively smaller vessels in the brain.
Subadventitial dissection occurs when blood penetrates through the tunica media into the subadventitial plane. Blood accumulating between these layers deforms the tunica adventitia outward, producing a pseudoaneurysm. Perrone, R. D. et al. Vascular complications in autosomal
dominant polycystic kidney disease, Nat. Rev. Nephrol. 2015
OBJECTIVE: This was a pathological study to investigate the healing process for cerebral dissecting aneurysms presenting with subarachnoid hemorrhage (SAH).
METHODS: Thirteen dissecting aneurysms that presented with SAH were obtained from 13 patients. Nine aneurysms arose from the vertebral artery, two arose from the anterior cerebral artery, one arose from the internal carotid artery, and one arose from the superior cerebellar artery. Eight aneurysm specimens were collected during autopsy and five were resected during surgery (trapping with or without bypass). The period between the onset of SAH and the time of specimen collection ranged from 6 hours to 35 days. All 13 aneurysms were pathologically examined with immunohistochemical staining, with a focus on the chronological healing process after SAH.
RESULTS: All dissecting aneurysms were generated with sudden widespread disruption of the internal elastic lamina and media. The healing process occurred with neointimal proliferation. The neointima, consisting mainly of newly synthesized smooth muscle cells and collagen fibers, extended from the disrupted ends of the media proper forward to the ruptured portion.
CONCLUSION: It is assumed that the healing process, with neointimal proliferation, begins after 1 week and may not be complete even after 1 month, depending on the extent of the wall injury.
Mizutani T. Neurosurgery 2004
RESULTS
General FindingsAll dissecting aneurysms were generated with sudden
widespread disruption of the internal elastic lamina (IEL) andmedia. The disrupted IEL did not reconnect in any of theaneurysm specimens. Interestingly, in several arteries, thewall of the disrupted IEL, which did not develop an arterialdissection, was silently covered with neointima (Fig. 1A).
Chronological ChangesIn two VA aneurysms (Cases 1 and 2) that were resected
during surgery (trapping and resection) on Day 0, freshthrombus covered the ruptured portion, with a small numberof neutrophils accumulated around the thrombus. Macro-phages were not observed. In two VA aneurysms (Cases 5 and6) that were treated with parent artery clipping on Day 1 andcollected during autopsy on Day 8 and Day 12, respectively,the healing process, including neutrophil accumulation andthe appearance of macrophages and neointima, was not de-
tected (Fig. 1B). In one VA aneurysm (Case 9) that was treatedconservatively and collected during autopsy on Day 14, neo-intima, consisting mainly of newly synthesized smooth mus-cle cells and collagen fibers, began to extend from the mediaproper to the ruptured portion (Fig. 2, A–C). However, thesynthesized tissue did not entirely cover the ruptured vascular
FIGURE 1. Patient 6, a 67-year-oldmale. The left VA dissecting aneurysmpresented with SAH, was treated withproximal clipping on Day 1, and wascollected during autopsy on Day 12.A, photomicrograph demonstrating si-lent repair of the area of IEL disrup-tion. Localized thickening of the neoin-tima can be observed (*). Arrows,disrupted ends of the IEL (elastica vanGieson stain; original magnification,!40). B, photomicrograph of the an-eurysm at the ruptured portion. Ar-rows, disrupted ends of the IEL. Ar-rowheads, disrupted ends of theadventitia (elastica van Gieson stain;original magnification, !12.5).
TABLE 1. Clinical summarya
Patientno.
Age (yr)/sex Onset Location Collection method Rebleeding Surgery
1 60/M SAH Left VA Surgery on Day 0 Day 0 Trapping " aneurysm resection onDay 0
2 48/M SAH Left VA Surgery on Day 0 Day 0 Trapping " aneurysm resection onDay 0
3 52/M SAH Left A2 Surgery on Day 1 No Trapping " aneurysm resection "A3-A3 bypass on Day 1
4 51/M SAH Left VA Autopsy on Day 2 No No
5 50/M SAH Right VA Autopsy on Day 8 No Proximal clipping on Day 1
6 67/M SAH Left VA Autopsy on Day 12 No Proximal clipping on Day 1
7 56/M SAH Left VA Autopsy on Day 14 Day 2 No
8 43/F SAH Left VA Autopsy on Day 14 Day 7 No
9 41/M SAH Right VA Autopsy on Day 15 Day 0 No
10 70/F SAH Right ICA Autopsy on Day 17 Day 9–11, 5 times No
11 59/M SAH Left A2–A3 Surgery on Day 19 No Trapping " aneurysm resection onDay 19
12 34/F SAH Left SCA Surgery on Day 23 No Trapping " aneurysm resection "STA-SCA bypass on Day 23
13 49/M SAH Right VA Autopsy on Day 35 Day 14 No
a SAH, subarachnoid hemorrhage; VA, vertebral artery; ICA, internal carotid artery; SCA, superior cerebellar artery; STA, superficial temporal artery.
HEALING PROCESS FOR CEREBRAL DISSECTING ANEURYSMS
NEUROSURGERY VOLUME 54 | NUMBER 2 | FEBRUARY 2004 | 343
Mizutani T. Neurosurgery 2004
RESULTS
General FindingsAll dissecting aneurysms were generated with sudden
widespread disruption of the internal elastic lamina (IEL) andmedia. The disrupted IEL did not reconnect in any of theaneurysm specimens. Interestingly, in several arteries, thewall of the disrupted IEL, which did not develop an arterialdissection, was silently covered with neointima (Fig. 1A).
Chronological ChangesIn two VA aneurysms (Cases 1 and 2) that were resected
during surgery (trapping and resection) on Day 0, freshthrombus covered the ruptured portion, with a small numberof neutrophils accumulated around the thrombus. Macro-phages were not observed. In two VA aneurysms (Cases 5 and6) that were treated with parent artery clipping on Day 1 andcollected during autopsy on Day 8 and Day 12, respectively,the healing process, including neutrophil accumulation andthe appearance of macrophages and neointima, was not de-
tected (Fig. 1B). In one VA aneurysm (Case 9) that was treatedconservatively and collected during autopsy on Day 14, neo-intima, consisting mainly of newly synthesized smooth mus-cle cells and collagen fibers, began to extend from the mediaproper to the ruptured portion (Fig. 2, A–C). However, thesynthesized tissue did not entirely cover the ruptured vascular
FIGURE 1. Patient 6, a 67-year-oldmale. The left VA dissecting aneurysmpresented with SAH, was treated withproximal clipping on Day 1, and wascollected during autopsy on Day 12.A, photomicrograph demonstrating si-lent repair of the area of IEL disrup-tion. Localized thickening of the neoin-tima can be observed (*). Arrows,disrupted ends of the IEL (elastica vanGieson stain; original magnification,!40). B, photomicrograph of the an-eurysm at the ruptured portion. Ar-rows, disrupted ends of the IEL. Ar-rowheads, disrupted ends of theadventitia (elastica van Gieson stain;original magnification, !12.5).
TABLE 1. Clinical summarya
Patientno.
Age (yr)/sex Onset Location Collection method Rebleeding Surgery
1 60/M SAH Left VA Surgery on Day 0 Day 0 Trapping " aneurysm resection onDay 0
2 48/M SAH Left VA Surgery on Day 0 Day 0 Trapping " aneurysm resection onDay 0
3 52/M SAH Left A2 Surgery on Day 1 No Trapping " aneurysm resection "A3-A3 bypass on Day 1
4 51/M SAH Left VA Autopsy on Day 2 No No
5 50/M SAH Right VA Autopsy on Day 8 No Proximal clipping on Day 1
6 67/M SAH Left VA Autopsy on Day 12 No Proximal clipping on Day 1
7 56/M SAH Left VA Autopsy on Day 14 Day 2 No
8 43/F SAH Left VA Autopsy on Day 14 Day 7 No
9 41/M SAH Right VA Autopsy on Day 15 Day 0 No
10 70/F SAH Right ICA Autopsy on Day 17 Day 9–11, 5 times No
11 59/M SAH Left A2–A3 Surgery on Day 19 No Trapping " aneurysm resection onDay 19
12 34/F SAH Left SCA Surgery on Day 23 No Trapping " aneurysm resection "STA-SCA bypass on Day 23
13 49/M SAH Right VA Autopsy on Day 35 Day 14 No
a SAH, subarachnoid hemorrhage; VA, vertebral artery; ICA, internal carotid artery; SCA, superior cerebellar artery; STA, superficial temporal artery.
HEALING PROCESS FOR CEREBRAL DISSECTING ANEURYSMS
NEUROSURGERY VOLUME 54 | NUMBER 2 | FEBRUARY 2004 | 343
FIGURE 1. Patient 6, a 67-year-old male. The left VA dissecting aneurysm presented with SAH, was treated with proximal clipping on Day 1, and was collected during autopsy on Day 12. A, photomicrograph demonstrating silent repair of the area of IEL disruption. Localized thickening of the neointima can be observed (*). Arrows, disrupted ends of the IEL (elastica van Gieson stain; original magnification, 40).
B, photomicrograph of the aneurysm at the ruptured portion. Arrows, disrupted ends of the IEL. Arowheads, disrupted ends of the adventitia (elastica van Gieson stain; original magnification, 12.5).
Mizutani T. Neurosurgery 2004
wall (Fig. 2A). The ruptured portion was covered only withthrombus and appeared very fragile (Fig. 2D). In the superiorcerebellar artery aneurysm (Case 13), which was resected dur-ing surgery (trapping and resection) on Day 23, the neointimacompletely covered the vascular wall (Fig. 3A), with endothe-lium covering the entire surface of the neointima. However,the neointima was broken in some of the slices (Fig. 3B),suggesting that this new layer was not strong enough tosustain the hemodynamic stress. One VA aneurysm (Case 14)that was treated conservatively, exhibited rebleeding on Day14, and was collected during autopsy on Day 35 (Fig. 4A)exhibited neointima extending from the media proper but notyet covering the ruptured portion, which was still coveredwith thrombus (Fig. 4B). Endothelium covered the neointimabut did not cover the residual thrombus. Along the luminalmargin of the thrombus, the accumulation of macrophageswas observed (Fig. 4C), suggesting active phagocytosis. Inaneurysms in which the media and IEL complex had com-pletely separated from the adventitia (Cases 7, 8, and 13),neointima formation was minimal even 14 days after the ini-tial SAH (Fig. 5).
DISCUSSION
Saccular aneurysms may have a permanent risk of bleeding.It seems that the healing mechanism is not sufficiently effec-tive, possibly because of the aneurysm structure. We are cur-rently unable to ascertain the age of saccular cerebral aneu-rysms, because they usually present no symptoms at the timeof development. They may gradually enlarge from arterialbifurcations, which lack IEL (15). In contrast, dissecting aneu-rysms are usually generated with sudden widespread disrup-tion of the IEL (6, 14). This type of cerebral arterial trunkaneurysm should be classified as Type 1 (acute cerebral dis-secting aneurysms), according to our clinicopathological clas-sification (7), and should be distinguished from Type 3(chronic enlarging dissecting aneurysms) (4). The time of gen-esis of acute dissecting aneurysms can be clearly determinedon the basis of clinical presentation, including preceding head-aches, SAH, and cerebral infarction. Therefore, specimens ofcerebral dissecting aneurysms collected at different times aftergenesis eloquently demonstrate chronological changes. Thesechanges may represent the healing process after the genesis of
FIGURE 2. Patient 9, a 41-year-old male. The right VA dissecting aneurysmpresented with SAH, was treated conservatively, and was collected duringautopsy on Day 15. A, photomicrograph of an axial slice of the aneurysm.Arrows, disrupted ends of the media and IEL complex. The neointima extendedfrom the disrupted ends of the media (azan stain; original magnification, !20).B, high-magnification view of the slice in A. Arrow, neointima, consisting
mainly of smooth muscle cells and collagen fibers (azan stain; original magni-fication, !100). C, the same slice as in A, stained for collagen Type I (collagenType I stain; original magnification, !100). Arrow, neointima, includingabundant collagen Type I fibers, compared with the media proper. D, photomi-crograph of an axial slice of the ruptured portion, which was still covered withfragile thrombus (arrow) (azan stain; original magnification, !20).
MIZUTANI ET AL.
344 | VOLUME 54 | NUMBER 2 | FEBRUARY 2004 www.neurosurgery-online.com
A 41-year-old male. The right VA dissecting aneurysm presented with SAH, was treated conservatively, and was collected during autopsy on Day 15.
Arrows, disrupted ends of the media and IEL complex. The neointima extended from the disrupted ends of the media (azan stain; original magnification, 20).
Mizutani T. Neurosurgery 2004
B, high-magnification view of the slice Arrow, neointima, consisting mainly of smooth muscle cells and collagen fibers (azan stain; original magnification, 100).
A 41-year-old male. The right VA dissecting aneurysm presented with SAH, was treated conservatively, and was collected during autopsy on Day 15.
wall (Fig. 2A). The ruptured portion was covered only withthrombus and appeared very fragile (Fig. 2D). In the superiorcerebellar artery aneurysm (Case 13), which was resected dur-ing surgery (trapping and resection) on Day 23, the neointimacompletely covered the vascular wall (Fig. 3A), with endothe-lium covering the entire surface of the neointima. However,the neointima was broken in some of the slices (Fig. 3B),suggesting that this new layer was not strong enough tosustain the hemodynamic stress. One VA aneurysm (Case 14)that was treated conservatively, exhibited rebleeding on Day14, and was collected during autopsy on Day 35 (Fig. 4A)exhibited neointima extending from the media proper but notyet covering the ruptured portion, which was still coveredwith thrombus (Fig. 4B). Endothelium covered the neointimabut did not cover the residual thrombus. Along the luminalmargin of the thrombus, the accumulation of macrophageswas observed (Fig. 4C), suggesting active phagocytosis. Inaneurysms in which the media and IEL complex had com-pletely separated from the adventitia (Cases 7, 8, and 13),neointima formation was minimal even 14 days after the ini-tial SAH (Fig. 5).
DISCUSSION
Saccular aneurysms may have a permanent risk of bleeding.It seems that the healing mechanism is not sufficiently effec-tive, possibly because of the aneurysm structure. We are cur-rently unable to ascertain the age of saccular cerebral aneu-rysms, because they usually present no symptoms at the timeof development. They may gradually enlarge from arterialbifurcations, which lack IEL (15). In contrast, dissecting aneu-rysms are usually generated with sudden widespread disrup-tion of the IEL (6, 14). This type of cerebral arterial trunkaneurysm should be classified as Type 1 (acute cerebral dis-secting aneurysms), according to our clinicopathological clas-sification (7), and should be distinguished from Type 3(chronic enlarging dissecting aneurysms) (4). The time of gen-esis of acute dissecting aneurysms can be clearly determinedon the basis of clinical presentation, including preceding head-aches, SAH, and cerebral infarction. Therefore, specimens ofcerebral dissecting aneurysms collected at different times aftergenesis eloquently demonstrate chronological changes. Thesechanges may represent the healing process after the genesis of
FIGURE 2. Patient 9, a 41-year-old male. The right VA dissecting aneurysmpresented with SAH, was treated conservatively, and was collected duringautopsy on Day 15. A, photomicrograph of an axial slice of the aneurysm.Arrows, disrupted ends of the media and IEL complex. The neointima extendedfrom the disrupted ends of the media (azan stain; original magnification, !20).B, high-magnification view of the slice in A. Arrow, neointima, consisting
mainly of smooth muscle cells and collagen fibers (azan stain; original magni-fication, !100). C, the same slice as in A, stained for collagen Type I (collagenType I stain; original magnification, !100). Arrow, neointima, includingabundant collagen Type I fibers, compared with the media proper. D, photomi-crograph of an axial slice of the ruptured portion, which was still covered withfragile thrombus (arrow) (azan stain; original magnification, !20).
MIZUTANI ET AL.
344 | VOLUME 54 | NUMBER 2 | FEBRUARY 2004 www.neurosurgery-online.com
Mizutani T. Neurosurgery 2004
C, the same slice as in A, stained for collagen Type I (collagen Type I stain; original magnification, 100). Arrow, neointima, including abundant collagen Type I fibers, compared with the media proper.
wall (Fig. 2A). The ruptured portion was covered only withthrombus and appeared very fragile (Fig. 2D). In the superiorcerebellar artery aneurysm (Case 13), which was resected dur-ing surgery (trapping and resection) on Day 23, the neointimacompletely covered the vascular wall (Fig. 3A), with endothe-lium covering the entire surface of the neointima. However,the neointima was broken in some of the slices (Fig. 3B),suggesting that this new layer was not strong enough tosustain the hemodynamic stress. One VA aneurysm (Case 14)that was treated conservatively, exhibited rebleeding on Day14, and was collected during autopsy on Day 35 (Fig. 4A)exhibited neointima extending from the media proper but notyet covering the ruptured portion, which was still coveredwith thrombus (Fig. 4B). Endothelium covered the neointimabut did not cover the residual thrombus. Along the luminalmargin of the thrombus, the accumulation of macrophageswas observed (Fig. 4C), suggesting active phagocytosis. Inaneurysms in which the media and IEL complex had com-pletely separated from the adventitia (Cases 7, 8, and 13),neointima formation was minimal even 14 days after the ini-tial SAH (Fig. 5).
DISCUSSION
Saccular aneurysms may have a permanent risk of bleeding.It seems that the healing mechanism is not sufficiently effec-tive, possibly because of the aneurysm structure. We are cur-rently unable to ascertain the age of saccular cerebral aneu-rysms, because they usually present no symptoms at the timeof development. They may gradually enlarge from arterialbifurcations, which lack IEL (15). In contrast, dissecting aneu-rysms are usually generated with sudden widespread disrup-tion of the IEL (6, 14). This type of cerebral arterial trunkaneurysm should be classified as Type 1 (acute cerebral dis-secting aneurysms), according to our clinicopathological clas-sification (7), and should be distinguished from Type 3(chronic enlarging dissecting aneurysms) (4). The time of gen-esis of acute dissecting aneurysms can be clearly determinedon the basis of clinical presentation, including preceding head-aches, SAH, and cerebral infarction. Therefore, specimens ofcerebral dissecting aneurysms collected at different times aftergenesis eloquently demonstrate chronological changes. Thesechanges may represent the healing process after the genesis of
FIGURE 2. Patient 9, a 41-year-old male. The right VA dissecting aneurysmpresented with SAH, was treated conservatively, and was collected duringautopsy on Day 15. A, photomicrograph of an axial slice of the aneurysm.Arrows, disrupted ends of the media and IEL complex. The neointima extendedfrom the disrupted ends of the media (azan stain; original magnification, !20).B, high-magnification view of the slice in A. Arrow, neointima, consisting
mainly of smooth muscle cells and collagen fibers (azan stain; original magni-fication, !100). C, the same slice as in A, stained for collagen Type I (collagenType I stain; original magnification, !100). Arrow, neointima, includingabundant collagen Type I fibers, compared with the media proper. D, photomi-crograph of an axial slice of the ruptured portion, which was still covered withfragile thrombus (arrow) (azan stain; original magnification, !20).
MIZUTANI ET AL.
344 | VOLUME 54 | NUMBER 2 | FEBRUARY 2004 www.neurosurgery-online.com
wall (Fig. 2A). The ruptured portion was covered only withthrombus and appeared very fragile (Fig. 2D). In the superiorcerebellar artery aneurysm (Case 13), which was resected dur-ing surgery (trapping and resection) on Day 23, the neointimacompletely covered the vascular wall (Fig. 3A), with endothe-lium covering the entire surface of the neointima. However,the neointima was broken in some of the slices (Fig. 3B),suggesting that this new layer was not strong enough tosustain the hemodynamic stress. One VA aneurysm (Case 14)that was treated conservatively, exhibited rebleeding on Day14, and was collected during autopsy on Day 35 (Fig. 4A)exhibited neointima extending from the media proper but notyet covering the ruptured portion, which was still coveredwith thrombus (Fig. 4B). Endothelium covered the neointimabut did not cover the residual thrombus. Along the luminalmargin of the thrombus, the accumulation of macrophageswas observed (Fig. 4C), suggesting active phagocytosis. Inaneurysms in which the media and IEL complex had com-pletely separated from the adventitia (Cases 7, 8, and 13),neointima formation was minimal even 14 days after the ini-tial SAH (Fig. 5).
DISCUSSION
Saccular aneurysms may have a permanent risk of bleeding.It seems that the healing mechanism is not sufficiently effec-tive, possibly because of the aneurysm structure. We are cur-rently unable to ascertain the age of saccular cerebral aneu-rysms, because they usually present no symptoms at the timeof development. They may gradually enlarge from arterialbifurcations, which lack IEL (15). In contrast, dissecting aneu-rysms are usually generated with sudden widespread disrup-tion of the IEL (6, 14). This type of cerebral arterial trunkaneurysm should be classified as Type 1 (acute cerebral dis-secting aneurysms), according to our clinicopathological clas-sification (7), and should be distinguished from Type 3(chronic enlarging dissecting aneurysms) (4). The time of gen-esis of acute dissecting aneurysms can be clearly determinedon the basis of clinical presentation, including preceding head-aches, SAH, and cerebral infarction. Therefore, specimens ofcerebral dissecting aneurysms collected at different times aftergenesis eloquently demonstrate chronological changes. Thesechanges may represent the healing process after the genesis of
FIGURE 2. Patient 9, a 41-year-old male. The right VA dissecting aneurysmpresented with SAH, was treated conservatively, and was collected duringautopsy on Day 15. A, photomicrograph of an axial slice of the aneurysm.Arrows, disrupted ends of the media and IEL complex. The neointima extendedfrom the disrupted ends of the media (azan stain; original magnification, !20).B, high-magnification view of the slice in A. Arrow, neointima, consisting
mainly of smooth muscle cells and collagen fibers (azan stain; original magni-fication, !100). C, the same slice as in A, stained for collagen Type I (collagenType I stain; original magnification, !100). Arrow, neointima, includingabundant collagen Type I fibers, compared with the media proper. D, photomi-crograph of an axial slice of the ruptured portion, which was still covered withfragile thrombus (arrow) (azan stain; original magnification, !20).
MIZUTANI ET AL.
344 | VOLUME 54 | NUMBER 2 | FEBRUARY 2004 www.neurosurgery-online.com
D, photomicrograph of an axial slice of the ruptured portion, which was still covered with fragile thrombus (arrow) (azan stain; original magnification, 20).
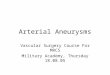
Type 1 aneurysm (classic dissecting aneurysm). A. At the peripheral portion of the aneurysm, the continuity of the IEL is preserved and the pseudolumen is detected. B. Widespread disruption of the IEL is observed at the midportion of the aneurysm
Mizutani T. Neurosurgery. 45(2):253, 1999
Left vertebral arteriogram showing a Type 1 aneurysm. Stenotic portion indicated by an arrow corresponds with Slice D in b. b, postmortem photographs of the aneurysm arising from the left vertebral artery. c, photomicrographs of the serial axial slices of the aneurysm (Slices A-D) (elastica van Gieson; original magnification, x4).
Slices A-D correspond with the slices shown in b. Widespread disruption of the IEL is shown in Slices A-C. P, pseudolumen.
Slice E was obtained from the opposite normal vertebral artery.
Mizutani T. Neurosurgery. 45(2):253, 1999
Type 2 aneurysm (segmental ectasia). Slice A, normal artery, shows intact IEL. The Type 2 aneurysm has stretched (Slice B) or fragmented (Slice C) IEL with adaptive intimal thickening. The luminal surface of the intimal thickening is smooth. Thrombus formation does not occur in Type 2 aneurysms. Mizutani T. Neurosurgery. 45(2):253, 1999
Type 3 aneurysm (dolichoectatic dissecting aneurysm). The Type 3 aneurysm has a fragmented IEL with intimal thickening. Multiple dissections occur in the thickened intima (Slices A and B). Thrombus is formed in and around the dissected intima (Slices A-C).
Type 4 aneurysm (saccular aneurysm or blister like aneurysm arising from arterial trunk). The Type 4 aneurysm arises from the portion of minimally disrupted IEL without intimal thickening. The dome comprises fragile adventitia or connective tissue.
gen fibers (1). According to the original “response-to-injury”hypothesis of atherogenesis (10, 11), the appearance and pro-liferation of smooth muscle cells in the intima after endothelialinjury are the initial cellular reactions after vascular wall in-jury. Normal endothelial cells regulate vascular tone and con-traction (12, 16). When endothelial cells are injured, macro-phages, T cells, and platelets are activated and releasecytokines and growth factors. These cytokines and growthfactors may contribute to the migration and proliferation ofsmooth muscle cells. They transform contractile smooth mus-cle cells into synthetic smooth muscle cells. The syntheticsmooth muscle cells then produce the extracellular matrix,including collagen fibers (9–11). There have been two hypoth-eses regarding the origin of smooth muscle cells in the neoin-tima; one suggests migration of medial smooth muscle cellsinto the intima and the other proposes intramural division ofcells (12). In this study, vascular wall repair via neointimaformation occurred from the disrupted ends of the mediaproper toward the ruptured portion. This finding stronglysupports the former hypothesis. Proper functioning of thishealing mechanism may be delayed under several conditions.One such condition involves aneurysms with large defects ofthe aneurysmal wall in the ruptured portion. Most large an-eurysms may be included in this group. It can be easilyassumed that a longer time is required for repair tissue tocover the entire circumference of an area with a larger diam-eter. Therefore, large aneurysms may carry the risk of rebleed-ing for a longer period. The second condition involves aneu-rysms with abundant thrombus in the ruptured portion,because neointima may appear in accordance with retractionof the thrombus. The third condition may involve aneurysmsin which the media and IEL complex are completely separatedfrom the adventitia, as noted in Cases 7 and 8 in this study. It
can be easily assumed that wall repair is completed after theneointima covers the entire area of the arterial wall. In thisstudy, with specimens of dissecting aneurysms obtained aslate as 35 days after the first SAH episode, the neointima didnot reach the ruptured portion of the aneurysm in most cases.Therefore, pathological confirmation of safety from the risk ofrebleeding was not obtained. Clinical data suggest that therate of rebleeding of ruptured dissecting aneurysms decreases1 week after SAH. This period of 1 week may correspond to astandard time for the appearance of the neointima in animalmodels (3, 8). However, nearly 10% of the rebleeding occurredafter 1 month (5). The longest interval in our previous reportwas 41 days.
REFERENCES1. Glagov S, Zarins CK, Masawa N, Xu CP, Bassiouny H, Giddens DP: Me-
chanical functional role of non-atherosclerotic intimal thickening. FrontMed Biol Eng 5:37–43, 1993.
2. Glynn LE: Medial defects in the circle of Willis and their relation to aneu-rysm formation. J Pathol Bacteriol 51:213–222, 1940.
3. Mitchell GM, McCann JJ, Rogers IW, Hickey MJ, Morrison WA, O’Brien BM:A morphological study of the long-term repair process in experimentallystretched but unruptured arteries and veins. Br J Plast Surg 49:34–40, 1996.
4. Mizutani T: A fatal, chronically growing basilar artery: A new type ofdissecting aneurysms. J Neurosurg 84:962–971, 1996.
5. Mizutani T, Aruga T, Kirino T, Miki Y, Saito I, Tsuchida T: Recurrentsubarachnoid hemorrhage from untreated ruptured vertebrobasilar dissect-ing aneurysms. Neurosurgery 36:905–913, 1995.
6. Mizutani T, Kojima H, Asamoto S, Miki Y: Pathological mechanism andthree dimensional mechanism of cerebral dissecting aneurysms.J Neurosurg 94:712–717, 2001.
7. Mizutani T, Miki Y, Kojima H, Suzuki H: Proposed classification of nonatherosclerotic cerebral fusiform and dissecting aneurysms. Neurosurgery45:253–260, 1999.
8. Poole JFC, Cromwell SB, Benditt BS, Benditt EP: Behavior of smooth musclecells and formation of extracellular structures in the reaction of arterial wallsto injury. Am J Pathol 62:391–414, 1971.
9. Ross R: The pathogenesis of atherosclerosis: A perspective for the 1990s.Nature 362:801–809, 1993.
FIGURE 5. Patient 8, a 43-year-old female. The dissecting aneurysm aris-ing from the left VA presented with SAH, was conservatively treated, andwas collected during autopsy on Day 14. The photomicrograph of the rup-tured portion of the aneurysm demonstrates that the ruptured portion wasstill covered with dense thrombus. Neointima formation was not observed(azan stain; original magnification, !20).
FIGURE 6. Genesis and healing of cerebral dissecting aneurysms.
MIZUTANI ET AL.
346 | VOLUME 54 | NUMBER 2 | FEBRUARY 2004 www.neurosurgery-online.com
Genesis and healing of cerebral dissecting aneurysms. Mizutani T. Neurosurgery 2004
Dissection with aneurysm. focal narrowing (arrow) of the right vertebral artery indicating the site of intimal disruption, and a distal dilatation (arrowheads).
b | Photomicrograph (10× magnification; hematoxylin and eosin stain) demonstrates complete disruption of the intima and media, and a dissection plane (thrombus) that propagated superficial to the media.
c | Photomicrograph (10× magnification; Movat's pentachrome stain) demonstrates an intact internal elastic lamina (arrows) away from the site of intimal disruption.
Abbreviations: M, media; T, thrombus.
Krings T. et al. Nature reviews. Neurology 2011
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

http://neuroangio.org/
Segmental susceptibility to dissection
http://neuroangio.org/
Segmental susceptibility to dissection
the craniocervical junction with perimedullary venous drainage. AJNR 17, 1137-1141, 19967. Mitsuhashi Y, Aurboonyawat T, Pereira VM, Geibprasert S, Toulgoat F, Ozanne A, Lasjaunias P. Dural arteriovenous fistulas draining into the petrosal vein or bridging vein of the medulla: pos-sible homologs of spinal dural arteriovenous fistulas. J Neurosurg 111, 889-899, 2009
8. Onda K, Yoshida Y, Arai H, Terada T. Complex arteriovenous fistulas at C1 causing hemato-myelia through aneurysmal rupture of a feeder from the anterior spinal artery. Acta Neurochir 154, 471-475, 2012
9. Rhoton AL Jr. The foramen magnum. Neurosurgery 47, S155 - S193, 200010. Sato K, Endo T, Niizuma K, Fujimura M, Inoue T, Shimizu H, Tominaga T. Concurrent dural and perimedullary arteriovenous fistulas at the craniocervical junction: case series with special reference to angioarchitecture. J Neurosurg 118, 451-459, 2013
Niche Neuro-Angiology Conference 2013!
Sato K
Sato K,et al Concurrent dural and perimedullary arteriovenous fistulas at the craniocervical junction . J Neurosurg 118, 451-459, 2013
Mizutani K. et al. BJR Case Rep 2016;2:
Segmental susceptibility to dissection
J. gabrieli et al.
J neurosurg April 1, 20162
multidisciplinary discussion, endovascular treatment was considered to be the most suitable treatment option.
Under general anesthesia, via a 6-F guiding catheter positioned at the distal aspect of the V2 segment of the left vertebral artery, n-butyl cyanoacrylate (Glubran 2, GEM Srl) diluted at 30% in Lipiodol (Guerbet) was selectively delivered through a flow-dependent microcatheter (1.2-F Magic, Balt Extrusion). Distal navigation was obtained with the help of a 0.007-inch micro guidewire (Hybrid, Balt Extrusion) to reach the farthest position. Glue injec-tion was satisfactory, resulting in complete exclusion of the bleeding source with neither proximal nor distal mi-gration of the liquid embolic agent (Fig. 1D). Control angi-ography revealed patency of all regional vessels except for the embolized segment and mild retrograde flow toward the glue cast (Fig. 1E).
Postprocedure clinical evaluation showed a left Wal-lenberg syndrome characterized by left Horner’s syn-
drome with neither diplopia nor nystagmus swallowing difficulty related to a left ninth cranial nerve palsy, hoarse-ness and severe hiccups, ipsilateral reduction of pain and temperature sensation of the face, and contralateral loss of pain and temperature sensation of the body. Diffusion-weighted MR images confirmed the presence of a left bul-bar stroke (Fig. 1F). The patient was subsequently referred for functional and speech reeducation.
Follow-up at 4 months revealed a general improvement with residual deficit; the main complaint concerned body pain and temperature sensation. The patient was unable to continue his previous occupation and was referred to pro-fessional rehabilitation; his modified Rankin Scale score at discharge was evaluated at 2.
DiscussionThe PICA is a highly variable artery at the craniocervi-
Fig. 1. a: Pretreatment left vertebral artery DSA in lateral projection showing the bulbar artery origin (single black arrow), the ASA origin (double black arrows), the aneurysm at the posterior medullary segment (white arrowhead), and the junction between the LSA and the PICA proper (white arrow). b: Superselective injection at the origin of the ASA (double arrows). A hypertrophic vaso-corona originates from the ASA. Coronary vessels (dotted black arrow), LSA (double black arrowheads), LSA-PICA junction (white arrow). c: Superselective injection distally into the bulbar artery just before the glue injection, further navigation was not possible; only partial opacification of the aneurysm is seen on DSA due to intrasaccular recumbent stagnating contrast media. Bulbar artery origin (black arrow), aneurysm (white arrowhead), LSA-PICA junction (white arrow), and microcatheter tip (black arrowhead) are shown. D: Glue cast after glue injection under blank road map. The removed microcatheter tip (black arrowhead) and excluded aneurysm (white arrowhead) are seen. Note that also the faded white area is part of the glue cast since also the roadmap was affected by the recumbent stagnating contrast media. e: Posttreatment left vertebral artery DSA in lateral projection showing the complete occlusion of the aneurysm, a mild spasm at the origin of the bulbar artery (black arrow), and reversed flow toward the glue cast through small anastomotic branches (dotted white arrows). F: Postembolization axial diffusion-weighted MR image (3 T) showing hyperintensity of the left dorsal medulla oblongata is seen (dotted white arrow), consistent with an acute ischemic stroke.
anterior spinal and bulbar artery supply to the pica
J neurosurg April 1, 2016 3
cal junction and usually originates from the vertebral ar-tery. It is considered to be the result of the embryological dominance of a posterior radiculopial artery.1
The PICA usually arises from the dominance of a sin-gle pial vessel at the level of the hypoglossal nerve. How-ever, several variations have been reported in the litera-ture, notably a cranial anterior inferior cerebellar artery (AICA)–PICA variant or caudal proatlantal C-1 and C-2 origins characterized by dominance of nearby segmental levels; such cases are usually associated with a hypertro-phic bulbar perforator arising at the usual hypoglossal segmental level.
While dominance is certainly the most common ana-tomical form, up to 2%4 of cases may exhibit an unusual codominance, also called a double PICA origin,3 charac-terized by 2 separate segments supplying the PICA proper. This condition, often underreported, is associated with higher aneurysm prevalence, possibly due to a regional vascular developmental disorganization.3
The PICA is related to the lateral spinal artery (LSA) as much as the posterior radiculomedullary arteries are re-lated to the posterior spinal artery, and this relationship is confirmed by the fact that in most instances (73%) an LSA is visible originating from the PICA itself.1 Thus, if the PICA proximal to the restiform body (junction of the LSA and PICA)5 fails to develop or sufficiently enlarge, usu-ally the LSA becomes the dominant/codominant channel and is supplied either cranially by an anastomotic channel from the AICA or caudally from a segmental branch orig-inating from the extraspinal longitudinal arteries (most commonly the vertebral artery). Interestingly, the location of the PICA’s origin seems not only to be related to the LSA but also to affect the origin of the ventral spinal ar-tery.5
Indeed, the well-known scheme proposed by Lasjau-nias et al.2 allows the theoretical possibility for the ASA also to be the origin or co-origin of the PICA, just as the basilar artery regularly gives origin to the AICA.
As demonstrated by this case, the codominant LSA cranially directed to supply the PICA may be supplied by the ASA through the anastomotic network of the coronary vessels. This codominant ASA supply could be either a primitive variant or the result of a postdevelopmental oc-clusion of a proatlantal feeder followed by hypertrophy of the existing coronary network; the latter seems more likely to explain the features observed in our case (Fig. 3). Indeed, the collateral circulation often develops from embryonic arterial systems, but acquired vascular patterns do not reproduce embryonic stages.1 In this case, a post-developmental arrangement is more likely since multiple irregular tortuous feeders point to the overuse of the adult network rather than the persistence and development of embryonic vessels that usually regress. Nevertheless, this configuration somehow completes the aforementioned scheme and, to our knowledge, has not been previously reported in the literature.
Unfortunately, treatment is still a challenge, since the vessels involved may vascularize eloquent regions of the brainstem and the treatment consists of a selective vascu-lar sacrifice. It is a common opinion that such selective segmental occlusion is usually well tolerated, even if per-forators arise next to or from the trapped segment;7 never-theless, the risk is present and should be balanced with the expected benefits.
Alternatively, selective exclusion of the aneurysm(s) plus a vascular PICA-PICA bypass distal to the origin of the aneurysm to protect the medulla via retrograde flow in case of feeder sacrifice has previously been reported at least once.6 In our case, this option did not seem to add sufficient benefit since the ASA-PICA network already constitutes a natural bypass, as demonstrated by the post-operative patency of all vessels including a retrograde flow toward the glue cast. A distal bypass nevertheless could have a hemodynamic impact reducing the flow through the proximal network and the shear stress on the wall of its arteries.
Fig. 2. left: Illustration summarizing the anatomical configuration observed in our case. right: DSA fusion image obtained by the overlap of 2 separate superselective injections at the level of the ASA and of the bulbar artery. The PICA is supplied by the LSA (double arrowheads) fed by the ASA (double arrows) through the hypertrophic coronary vessels (dotted arrow) and by the bulbar artery (arrow), which harbors a small aneurysm (arrowhead). Only partial filling of the aneurysm is visible. Mild retrograde opacification of the vertebral artery (asterisk) is observed. Figure is available in color online only.
J. gabrieli et al.
J neurosurg April 1, 20164
This case highlights a particular anatomical arrange-ment, its associated aneurysmal lesion, and once again7 stresses the importance of the medullary perforating ves-sels, especially in cases of variations of the PICA origin.
references 1. Lasjaunias P, Berenstein A, terBrugge KG: Clinical Vascu-
lar Anatomy and Variations. Berlin: Springer, 2001 2. Lasjaunias P, Vallee B, Person H, terBrugge K, Chiu M:
The lateral spinal artery of the upper cervical spinal cord. Anatomy, normal variations, and angiographic aspects. J Neurosurg 63:235–241, 1985
3. Lesley WS, Rajab MH, Case RS: Double origin of the poste-rior inferior cerebellar artery: association with intracranial aneurysm on catheter angiography. AJR Am J Roentgenol 189:893–897, 2007
4. Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Micro-surgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982
5. Mercier P, Brassier G, Fournier D, Hentati N, Pasco-Papon A, Papon X: Predictibility of the cervical origin of the ante-rior spinal artery. Interv Neuroradiol 3:283–288, 1997
6. Mortazavi MM, Frerich JM, Sekhar LN: Multiple aneurysms
on inter-PICA communicating collaterals: case report on a rare entity. Cureus 6:e181, 2014
7. Pasco A, Thouveny F, Papon X, Tanguy JY, Mercier P, Caron-Poitreau C, et al: Ruptured aneurysm on a double ori-gin of the posterior inferior cerebellar artery: a pathological entity in an anatomical variation. Report of two cases and review of the literature. J Neurosurg 96:127–131, 2002
DisclosuresDr. Sourour reports that he is a consultant and proctor for Covi-dien and Stryker.
author contributionsConception and design: Gabrieli. Acquisition of data: Sourour. Analysis and interpretation of data: Gabrieli, Clarençon. Criti-cally revising the article: all authors. Reviewed submitted version of manuscript: all authors.
correspondenceJoseph Gabrieli, Department of Neuroradiology, Pitié-Salpêtrière Hospital, 47 Bd de l’Hôpital, Paris 75013, France. email: [email protected].
Fig. 3. Schematic of the developmental pathways allowed at the craniocervical junction, depicted in the style shown in Lasjaunias et al.: J Neurosurg 63:235–241, 1985. left: A hypothetical insult (X) at the level of a low PICA origin. right: Postdevelopmental hypertrophy of the ASA (double arrows), vasocorona (arrowhead), and bulbar artery (arrow). VERT = vertebral artery. Figure is available in color online only.
anterior spinal and bulbar artery supply to the pica
J neurosurg April 1, 2016 3
cal junction and usually originates from the vertebral ar-tery. It is considered to be the result of the embryological dominance of a posterior radiculopial artery.1
The PICA usually arises from the dominance of a sin-gle pial vessel at the level of the hypoglossal nerve. How-ever, several variations have been reported in the litera-ture, notably a cranial anterior inferior cerebellar artery (AICA)–PICA variant or caudal proatlantal C-1 and C-2 origins characterized by dominance of nearby segmental levels; such cases are usually associated with a hypertro-phic bulbar perforator arising at the usual hypoglossal segmental level.
While dominance is certainly the most common ana-tomical form, up to 2%4 of cases may exhibit an unusual codominance, also called a double PICA origin,3 charac-terized by 2 separate segments supplying the PICA proper. This condition, often underreported, is associated with higher aneurysm prevalence, possibly due to a regional vascular developmental disorganization.3
The PICA is related to the lateral spinal artery (LSA) as much as the posterior radiculomedullary arteries are re-lated to the posterior spinal artery, and this relationship is confirmed by the fact that in most instances (73%) an LSA is visible originating from the PICA itself.1 Thus, if the PICA proximal to the restiform body (junction of the LSA and PICA)5 fails to develop or sufficiently enlarge, usu-ally the LSA becomes the dominant/codominant channel and is supplied either cranially by an anastomotic channel from the AICA or caudally from a segmental branch orig-inating from the extraspinal longitudinal arteries (most commonly the vertebral artery). Interestingly, the location of the PICA’s origin seems not only to be related to the LSA but also to affect the origin of the ventral spinal ar-tery.5
Indeed, the well-known scheme proposed by Lasjau-nias et al.2 allows the theoretical possibility for the ASA also to be the origin or co-origin of the PICA, just as the basilar artery regularly gives origin to the AICA.
As demonstrated by this case, the codominant LSA cranially directed to supply the PICA may be supplied by the ASA through the anastomotic network of the coronary vessels. This codominant ASA supply could be either a primitive variant or the result of a postdevelopmental oc-clusion of a proatlantal feeder followed by hypertrophy of the existing coronary network; the latter seems more likely to explain the features observed in our case (Fig. 3). Indeed, the collateral circulation often develops from embryonic arterial systems, but acquired vascular patterns do not reproduce embryonic stages.1 In this case, a post-developmental arrangement is more likely since multiple irregular tortuous feeders point to the overuse of the adult network rather than the persistence and development of embryonic vessels that usually regress. Nevertheless, this configuration somehow completes the aforementioned scheme and, to our knowledge, has not been previously reported in the literature.
Unfortunately, treatment is still a challenge, since the vessels involved may vascularize eloquent regions of the brainstem and the treatment consists of a selective vascu-lar sacrifice. It is a common opinion that such selective segmental occlusion is usually well tolerated, even if per-forators arise next to or from the trapped segment;7 never-theless, the risk is present and should be balanced with the expected benefits.
Alternatively, selective exclusion of the aneurysm(s) plus a vascular PICA-PICA bypass distal to the origin of the aneurysm to protect the medulla via retrograde flow in case of feeder sacrifice has previously been reported at least once.6 In our case, this option did not seem to add sufficient benefit since the ASA-PICA network already constitutes a natural bypass, as demonstrated by the post-operative patency of all vessels including a retrograde flow toward the glue cast. A distal bypass nevertheless could have a hemodynamic impact reducing the flow through the proximal network and the shear stress on the wall of its arteries.
Fig. 2. left: Illustration summarizing the anatomical configuration observed in our case. right: DSA fusion image obtained by the overlap of 2 separate superselective injections at the level of the ASA and of the bulbar artery. The PICA is supplied by the LSA (double arrowheads) fed by the ASA (double arrows) through the hypertrophic coronary vessels (dotted arrow) and by the bulbar artery (arrow), which harbors a small aneurysm (arrowhead). Only partial filling of the aneurysm is visible. Mild retrograde opacification of the vertebral artery (asterisk) is observed. Figure is available in color online only.
Menu
1. Anatomical consideration of craniocervical junction
2. Pathology of arterial dissections
3. Imaging modalities and the clinical application
Key words: Dissections, Internal Elastic Lamina,
Segmental vulnerability, Lateral spinal artery , Homology
106 T Okudera et al. In vivo microneuroangiographyAutoradiogram
High resolution CBCT
Mercier P. et al. INR 2008 High resolution CBCT
Organization of the Cerebral Microcirculation 325
References p. 396
Fig 7.23C Perforating arteries to the brain stem and the
corpus callosum.
Organization of the Cerebral Microcirculation 325
References p. 396
Fig 7.23C Perforating arteries to the brain stem and the
corpus callosum.
Case 4 A 76 year-old-man presented with sudden onset of headache and loss of consciousness. H&H grade 2, WFNS grade 2, Fisher group 3
IEL
Type 4
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

Type 4
K. Arimura et al.518
Neurol Med Chir (Tokyo) 56, September, 2016
trapping (surgical or endovascular) with or without extracranial-intracranial (EC-IC) bypass, clipping or wrapping of the aneurysm sac,19,20) stent-assisted coil embolization of the aneurysm sac,21) and stent monotherapy including the use of flow diverters22,23) (Fig. 1). Therapeutic safety and efficacy of endovas-cular and surgical treatment have not been tested in a randomized trial. Recently, endovascular (internal) trapping is undertaken more frequently than surgical treatment for ruptured intracranial VA dissection.24) Although internal trapping is effective to avoid rebleeding and less invasive, postoperative medul-lary infarctions remains unresolved.25)
Recent nationwide study of vertebrobasilar artery dissections in Japan demonstrated that craniotomy accounted for 20% of all intervention (including surgical and endovascular treatment), and trap-ping was the most frequent (62.5%) procedures in the craniotomy.26) Since proximal occlusion cannot completely block the retrograde flow from the contralateral VA, trapping will be most effective to prevent rebleeding.27) However, it was reported that higher incidence of ischemic complication was observed in trapping than proximal occlusion.26)
treatment. Mizutani demonstrated that most IAD causing SAH bled within a few days after onset of dissection indicated by preceding headache.15) Since it was reported that serial angiographic change was seen in 88.2% of unruptured vertebral artery (VA) dissection and it may be amenable for surgical treatment,16) a follow-up angiography should be recommended during the early stage (within approximately 3 weeks after onset).16,17) Moreover, another paper reported that unruptured VA dissec-tion had bled 4 months after onset.18) Consequently, even unruptured IAD should be followed carefully at least a few months by neuroimaging, and surgical treatment may be considered if the formation or enlargement of the aneurysmal dilatation has been confirmed.
Surgical Strategy
1. Vertebral arteryVA is the most frequently affected site in IAD.
In the nationwide study of IAD in Japan, 82% of IAD is located in VA.3) There are several treatment strategies for VA dissection; proximal occlusion,
Fig. 1 Treatment strategies for vertebral artery dissecting aneurysms. An: aneurysm, EC-IC: extracranial-intracranial.
Arimura K. et al. Neurologia medico-chirurgica 2016
Semi jail technique with Headway 21, LVIS 4.5×23mm, Target Nano 1.5mm×2cm, Deltaplush 1.5mm×2cm
Pre Post
High resolution cone beam CT He could return to his home @15th post onset. mRS 0
Case 5. A 37 year-old-man presented with suboccipial and nuchal pain.
Onset @1week @3 weeks
VasoCT (coronal)
High resolution CBCT
Onset @1week @3 weeks
Type 1 Classic dissection
K. Arimura et al.518
Neurol Med Chir (Tokyo) 56, September, 2016
trapping (surgical or endovascular) with or without extracranial-intracranial (EC-IC) bypass, clipping or wrapping of the aneurysm sac,19,20) stent-assisted coil embolization of the aneurysm sac,21) and stent monotherapy including the use of flow diverters22,23) (Fig. 1). Therapeutic safety and efficacy of endovas-cular and surgical treatment have not been tested in a randomized trial. Recently, endovascular (internal) trapping is undertaken more frequently than surgical treatment for ruptured intracranial VA dissection.24) Although internal trapping is effective to avoid rebleeding and less invasive, postoperative medul-lary infarctions remains unresolved.25)
Recent nationwide study of vertebrobasilar artery dissections in Japan demonstrated that craniotomy accounted for 20% of all intervention (including surgical and endovascular treatment), and trap-ping was the most frequent (62.5%) procedures in the craniotomy.26) Since proximal occlusion cannot completely block the retrograde flow from the contralateral VA, trapping will be most effective to prevent rebleeding.27) However, it was reported that higher incidence of ischemic complication was observed in trapping than proximal occlusion.26)
treatment. Mizutani demonstrated that most IAD causing SAH bled within a few days after onset of dissection indicated by preceding headache.15) Since it was reported that serial angiographic change was seen in 88.2% of unruptured vertebral artery (VA) dissection and it may be amenable for surgical treatment,16) a follow-up angiography should be recommended during the early stage (within approximately 3 weeks after onset).16,17) Moreover, another paper reported that unruptured VA dissec-tion had bled 4 months after onset.18) Consequently, even unruptured IAD should be followed carefully at least a few months by neuroimaging, and surgical treatment may be considered if the formation or enlargement of the aneurysmal dilatation has been confirmed.
Surgical Strategy
1. Vertebral arteryVA is the most frequently affected site in IAD.
In the nationwide study of IAD in Japan, 82% of IAD is located in VA.3) There are several treatment strategies for VA dissection; proximal occlusion,
Fig. 1 Treatment strategies for vertebral artery dissecting aneurysms. An: aneurysm, EC-IC: extracranial-intracranial.
Arimura K. et al. Neurologia medico-chirurgica 2016
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

Pre Post
Metal artifact reduction mode
CT on admission
K. Arimura et al.518
Neurol Med Chir (Tokyo) 56, September, 2016
trapping (surgical or endovascular) with or without extracranial-intracranial (EC-IC) bypass, clipping or wrapping of the aneurysm sac,19,20) stent-assisted coil embolization of the aneurysm sac,21) and stent monotherapy including the use of flow diverters22,23) (Fig. 1). Therapeutic safety and efficacy of endovas-cular and surgical treatment have not been tested in a randomized trial. Recently, endovascular (internal) trapping is undertaken more frequently than surgical treatment for ruptured intracranial VA dissection.24) Although internal trapping is effective to avoid rebleeding and less invasive, postoperative medul-lary infarctions remains unresolved.25)
Recent nationwide study of vertebrobasilar artery dissections in Japan demonstrated that craniotomy accounted for 20% of all intervention (including surgical and endovascular treatment), and trap-ping was the most frequent (62.5%) procedures in the craniotomy.26) Since proximal occlusion cannot completely block the retrograde flow from the contralateral VA, trapping will be most effective to prevent rebleeding.27) However, it was reported that higher incidence of ischemic complication was observed in trapping than proximal occlusion.26)
treatment. Mizutani demonstrated that most IAD causing SAH bled within a few days after onset of dissection indicated by preceding headache.15) Since it was reported that serial angiographic change was seen in 88.2% of unruptured vertebral artery (VA) dissection and it may be amenable for surgical treatment,16) a follow-up angiography should be recommended during the early stage (within approximately 3 weeks after onset).16,17) Moreover, another paper reported that unruptured VA dissec-tion had bled 4 months after onset.18) Consequently, even unruptured IAD should be followed carefully at least a few months by neuroimaging, and surgical treatment may be considered if the formation or enlargement of the aneurysmal dilatation has been confirmed.
Surgical Strategy
1. Vertebral arteryVA is the most frequently affected site in IAD.
In the nationwide study of IAD in Japan, 82% of IAD is located in VA.3) There are several treatment strategies for VA dissection; proximal occlusion,
Fig. 1 Treatment strategies for vertebral artery dissecting aneurysms. An: aneurysm, EC-IC: extracranial-intracranial.
Arimura K. et al. Neurologia medico-chirurgica 2016Rt.PICA extracranial origin, Lt.PICA-AICA
AICA
PICA
PICA
mRS 0@30day post op.
Case 6. A 60 y/o female has presented her nuchal and occipital headache for a couple of days. She consulted a neurologist in regional hospital, but was not diagnosed as a SAH. Afterwards, she presented with more severe headache and vomiting. An emergency CT showed a massive SAH mainly distributed at the level of cerebello-medullary and prepontine cistern.
CT on admission (H&K grade IV,WFNS grade 4)
CT on admission H&K grade IV
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .

145
Rt.VA
Lt.PICARt.PICA
ASA
Rt.V4 trunk is indeed hypoplastic but bilateral PICA originate symmetrically. →ASA and medullary perforators come from symmetrically. 2794488
Final View
Frontal Lateral
Although left VA is hypoplastic, dominant ASA and anterior medullary perforators are originating from left side. Note the dominancy of PICA
When something is small, it doesn’t have to mean that it is not important.
Mercier P. et al. INR 2008 Left VAG (post embolization)Frontal
Rt.AICA-PICA
Cortical territory of cerebellar hemisphere
Infratentorial arterial system
2010/10/02 2010/11/29mRS 0H&H grade IV
@1 year post Op.
The Galerie de paléontologie et d'anatomie comparée in Paris
More you see in detail, more you are fascinated.
Summary
1. There are two major factors as the susceptibility to dissection of VA. ・Kinetic motion factor at the level of atlantoaxial joint. ・Anatomical fragility of the intracranial V4 portion and PICA corresponding to the vasa corona as the homology of lateral spinal artery.
2. Functional vascular anatomy is the key to indicate the proper management and decision making.
→ Anatomical disposition is the message to predict the important perforators.
3. Sophisticated imaging technologies (e.g.high resolution CBCT) can provide in vivo microneuroangiography.
Thank you…
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC - W
IN S
emina
r. All r
ights
rese
rved -
Any
repr
oduc
tion e
ven i
n par
t is pr
ohibi
ted.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
.
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .
2017
© A
BC-WIN
Sem
inar. A
ll righ
ts re
serve
d - A
ny re
prod
uctio
n eve
n in p
art is
proh
ibited
] .