Embed Size (px)
Citation preview
TM
8101 West Jefferson Blvd.Fort Wayne, IN 46804
www.phpni.com
2016 Indigo IndividualTM
Purchaser GuideYour guide to buying PHP health plans for individuals and families.
©2015 PHPNI, Inc.October 2015 www.phpni.com

Our commitment to you.
Excellence in customer service and greater freedom are only a few reasons our members are happy with PHP year after year. We are committed to providing you with the best service.
Because we are based right here in Northern Indiana, we offer easy access to the largest local network of healthcare providers, hassle-free claims processing, unmatched personal attention, and helpful resources for the health and well-being of our community.
An ounce of prevention
is worth a pound of cure. All of our plans pay 100% of many important preven-tive services including well-baby care, immunizations, mammograms, pap tests, and annual physical exams when ordered by a participating provider.
Emergency care benefits that
apply anywhere in the world.
While traveling, members are covered should emergency services be needed. Just show your member ID card at the time of service.
Health coverage for
individuals and families.
Indigo IndividualTM
1
PHP Service
AreaApplicants must reside
in one of these counties to be eligible for coverage.
11
Providing you the tools
to manage your healthcare.
You have around-the-clock access to powerful online resources at www.phpni.com. Whether you are look-ing for a physician, researching drug information, or checking your personal account for benefit, claim, deductible, and out-of-pocket information, our Web site allows you to take charge of your health when it’s most convenient for you.
Features of our plans:
• Preventive Services covered at 100% for all plans (Complete list of services found at www.phpni.com)• All plans available as an Individual or Family Policy• Many value-added benefits included automatically: 24-hour nurse line, extensive online health resources, member discounts for health facilities and more• Prescription drug coverage available with all plans• Competitive premium rates • Negotiated provider costs to save you money • Exceptional customer service to help you understand and make the most of your health coverage
The next several pages help you compare the various types of plans we have available:
Traditional Plans Most like traditional employer plans with copays and/or coinsurance for routine medical services.HSA Plans Qualified high-deductible health plans that can be used in conjunction with a Health Savings Account. Catastrophic Plans Basic coverage for accident and illness with the lowest possible premiumChoice Plans Plans that provide you the flexibility to use healthcare providers outside of the network.

2
Phone Numbers
Voice: (260) 432-6690, ext. 810Toll-free: 1-800-982-6257, ext. 810Hearing Impaired: (260) 459-2600
Address
Attn: Individual Product Physicians Health Plan 8101 West Jefferson Blvd.Fort Wayne, IN 46804
[email protected] To help us provide excellent service, be sure to include your name and your daytime phone number.
Web Address
www.phpni.com
Eligibility Requirements
Individuals applying for coverage must be under 65 years old to qualify. Any covered dependent children must be under the age of 26 and either your son, daughter, step-child, or a child subject to legal guardianship, regardless of support level; or a grandchild or other blood relative who is more than 50% dependent on you for total support.
As the primary applicant, you must be a legal Indiana resident residing within our service area (a map of counties in our service area can be found on page 12).
10
Traditional Plans are best suited for:
Anyone wanting the security of a lower deductible plan
Families who regularly schedule doctor’s appointments and well-child visits
Those who prefer to pay less at the time of service
Of all our plans, Traditional Plans are most like group employer plans with copays or coinsurance for routine medical services. Be sure to take advantage of our preventive services benefit, with 100% coverage, to maintain your health. With the Traditional Plans, you may see any provider in our network, and the Choice Plans offer the additional flexibility of seeing out-of-network providers. Just select the deductible and out-of-pocket level that best meet your budget and financial needs.
Traditional Plans
MyNurse 24/7 Health concerns don’t always arise while the doc-tor’s office is open. Our members have access to a toll-free, 24-hour nurse line service for noncriti-cal situations. Members can speak with experi-enced, knowledgeable nurses who answer ques-tions with sound, clinically based information day or night.
MyHealth 24/7 This interactive, online resource acts as a 24-hour medical advisor to help find solutions to common health problems. Evaluate symptoms and overall health, use quizzes and calculators to improve and maintain weight, or search the pharmacy sec-tion to compare drugs and lower expenses.
HealthNEWS Newsletter
Members receive a quarterly newsletter that offers health and wellness information from nutrition and exercise, to seasonal health concerns and medical news. Each issue includes an update of our provider network as well as local events and member discounts.
Value-added services included with every Indigo IndividualTM health plan
Smoking Cessation
In keeping with our mission of encouraging preventive health maintenance, we offer coverage to help you in your goal to quit smoking. Additional information on the Indiana Quitline, tobacco inter-vention programs, community classes, and support groups to quit smoking are also provided.
Member Discounts
Our members are eligible to receive a variety of special discounts at select area health clubs, community classes, and facilities such as:
• Free trial memberships, discounts on enrollment fees, annual memberships, and training packages
• Discounts on medically supervised programs• Discounts on prescription eyewear• Sporting event discounts
A complete listing of member discounts is available online at www.phpni.com.
Open Enrollment for 2016
Generally you and your family can only purchase new coverage during the annual open enrollment period. For 2016, this period is November 1, 2015 through January 31, 2016. Outside of this annual open enrollment period, you may still be eligible to purchase coverage if you experience a qualified special enrollment event, such as a marriage, birth of a child, change in enrollment, etc.

3
Applying for coverage is easy.
Make the choice to protect your family with the security of high-quality health coverage from PHP. Applying is easy. Just go to www.enroll.phpni.com. Apply online and compare the plans that are avail-able. You can also access more information about Indigo IndividualTM plans online at www.phpni.com.
Choose the best payment option for you.
Initial Payments may be made by checking or savings account, credit or debit card, or you mayreceive an invoice to pay by check or money order.
Ongoing Payments can be made several different ways. For your convenience, you may set-up a monthly automatic payment from your checking or savings account. You will receive an email prior to the due date notifying you of the amount that will be deducted from your account if you select this option.
You may also elect to receive a monthly invoice, either by U.S. mail or email. Once you receive the invoice, you may pay by check, money order, or make an online payment using your checking or savings account.
Try us out.
We want you to be satisfied and confident with your Indigo IndividualTM coverage. That’s why you have a “free-look” period to examine your policy when it is received. If for any reason within the free-look period you decide you no longer want the policy, simply return it to us and the policy will be cancelled and your premium refunded.
9
Covered Benefits Traditional Plans
Gold Level Plan Silver Level Plans Bronze Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
$1,250/$6,850$2,500/$13,700
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immu-nizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness $35 pre visit
$30 each for 3 visits per covered person, then 20%*
$30 each for 3 visits per covered person, then 30%*
$50 each for 3 visits per covered person, then 50%*
Other Practitioner Visits10%* 20%* 30%* 50%*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests). 10%* 20%* 30%* 50%*
Outpatient Services10%* 20%* 30%* 50%*
Inpatient Services$500 per visit plus 10%* of
remaining charges$500 per visit plus 20%* of
remaining charges30%* $500 per visit plus 50%* of
remaining charges
Hospital Emergency RoomDiagnosis must be emergent in nature. $300 per visit
plus 10%* of remaining charges$300 per visit plus 20%* of
remaining charges$300 per visit plus 30%* of
remaining charges$300 per visit plus 50%* of
remaining charges
Urgent Care Center
10%* 20%* 30%* 50%*
Ambulance Service
10%* 20%* 30%* 50%*
MaternityBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service setting
Diabetes Services Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Durable Medical Equipment,
Prosthetics, Orthotic Appliances,
and Ostomy Supplies10%* 20%* 30%* 50%*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
Tier 1/Tier 2: $15Tier 3: $45
Tier 4: 10%* Tier 5: 10%*
Tier 1/Tier 2: $15Tier 3: $45
Tier 4: 50%*Tier 5: 50%*
Tier 1/Tier 2: $10Tier 5: $30
Tier 4: 30%* Tier 5: 30%*
Tier 1/Tier 2: $25Tier 3: $60
Tier 4: 25%*Tier 5: 25%*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic sup-plies, per prescription or refill. Six over-the-counter vials of insulin.
Tier 1/Tier 2: $45Tier 3: $135Tier 4: 10%*
Tier 5: Not Covered
Tier 1/Tier 2: $45Tier 3: $135Tier 4: 50%*
Tier 5: Not Covered
Tier 1/Tier 2: $30Tier 3: $90
Tier 4: 30%*Tier 5: Not Covered
Tier 1/Tier 2: $75Tier 3: 50%*Tier 4: 50%*
Tier 5: Not Covered
*Services are subject to the Medical Deductible and apply toward the Medical Out-of-Pocket limit.
$2,000/$6,850$4,000/$13,700
$2,500/$6,850$5,000/$13,700
$5,000/$6,850$10,000/$13,700
4
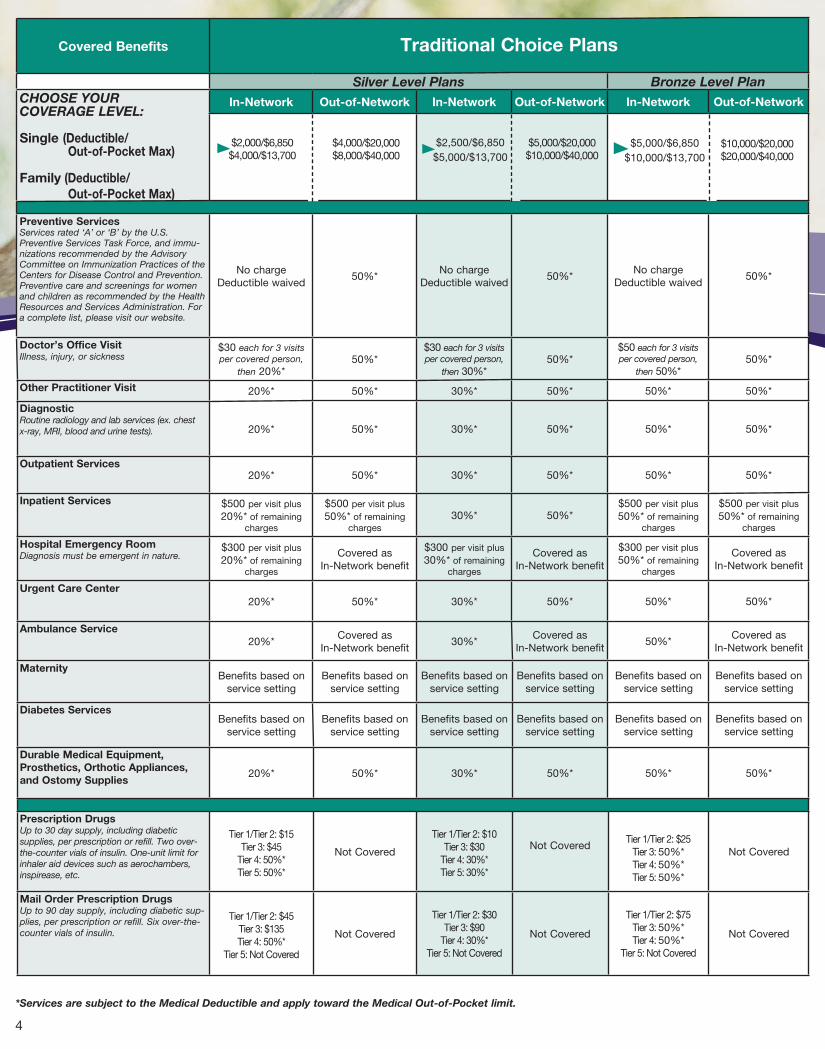
*Services are subject to the Medical Deductible and apply toward the Medical Out-of-Pocket limit.
Covered Benefits Traditional Choice Plans
Silver Level Plans Bronze Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immu-nizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
50%*No charge
Deductible waived50%*
No charge Deductible waived
50%*
Doctor’s Office VisitIllness, injury, or sickness
$30 each for 3 visits per covered person,
then 20%* 50%*
$30 each for 3 visits per covered person,
then 30%* 50%*
$50 each for 3 visits per covered person,
then 50%* 50%*
Other Practitioner Visit 20%* 50%* 30%* 50%* 50%* 50%*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests). 20%* 50%* 30%* 50%* 50%* 50%*
Outpatient Services 20%* 50%* 30%* 50%* 50%* 50%*
Inpatient Services $500 per visit plus 20%* of remaining
charges
$500 per visit plus 50%* of remaining
charges30%* 50%*
$500 per visit plus 50%* of remaining
charges
$500 per visit plus 50%* of remaining
charges
Hospital Emergency Room Diagnosis must be emergent in nature.
$300 per visit plus 20%* of remaining
charges
Covered as In-Network benefit
$300 per visit plus 30%* of remaining
charges
Covered as In-Network benefit
$300 per visit plus 50%* of remaining
charges
Covered as In-Network benefit
Urgent Care Center
20%* 50%* 30%* 50%* 50%* 50%*
Ambulance Service
20%*Covered as
In-Network benefit30%*
Covered as In-Network benefit
50%*Covered as
In-Network benefit
MaternityBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service setting
Diabetes Services Benefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service setting
Durable Medical Equipment,
Prosthetics, Orthotic Appliances,
and Ostomy Supplies20%* 50%* 30%* 50%* 50%* 50%*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
Tier 1/Tier 2: $15Tier 3: $45
Tier 4: 50%*Tier 5: 50%*
Not Covered
Tier 1/Tier 2: $10Tier 3: $30
Tier 4: 30%* Tier 5: 30%*
Not CoveredTier 1/Tier 2: $25
Tier 3: 50%* Tier 4: 50%*Tier 5: 50%*
Not Covered
Mail Order Prescription DrugsUp to 90 day supply, including diabetic sup-plies, per prescription or refill. Six over-the-counter vials of insulin.
Tier 1/Tier 2: $45Tier 3: $135Tier 4: 50%*
Tier 5: Not Covered
Not Covered
Tier 1/Tier 2: $30Tier 3: $90
Tier 4: 30%*Tier 5: Not Covered
Not Covered
Tier 1/Tier 2: $75Tier 3: 50%*Tier 4: 50%*
Tier 5: Not Covered
Not Covered
$2,500/$6,850$5,000/$13,700
$5,000/$20,000$10,000/$40,000
$5,000/$6,850$10,000/$13,700
$10,000/$20,000$20,000/$40,000
$4,000/$20,000$8,000/$40,000
$2,000/$6,850$4,000/$13,700

5
HSA Plans are best suited for:
People looking to build a savings account for future qualified medical expenses
Those wanting more control of how their healthcare dollars are spent
Anyone willing to trade a higher deductible for lower premiums while
maintaining basic coverage for accident and illness Many of our Bronze Plans are qualified high-deductible health plans that can be used in conjunction with a Health Savings Account (HSA). An HSA can be obtained from the bank of your choice, and funds in your HSA grow tax-free. Also, there is not a requirement to use the funds within a specified timeframe so you can save for future healthcare expenses.
Like our other plans, when you purchase a qualified high-deductible health plan you can see any provider in our network. The Marquee plans that are qualified high-deductible health plans are: Marquee Silver 3500, Marquee Bronze 3750, and Marquee Bronze 6000.
HSA Plans
9
*Services are subject to the Medical Deductible and apply toward the Medical Out-of-Pocket limit.
**Catastrophic Plans have eligibility restrictions. Contact PHP for more details.
Covered BenefitsCatastrophic
Plan**
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness
No Coinsurance*Deductible waived for first
3 primary care visits only.
Other Practitioner Visits No Coinsurance*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests).
No Coinsurance*
Outpatient ServicesNo Coinsurance*
Inpatient ServicesNo Coinsurance*
Hospital Emergency RoomDiagnosis must be emergent in nature. No Coinsurance*
Urgent Care CenterNo Coinsurance*
Ambulance ServiceNo Coinsurance*
Maternity Benefits based on service setting
Dibetes Services Benefits based on service setting
Durable Medical Equipment,
Prosthetics, Orthotic
Appliances, and
Ostomy Supplies
No Coinsurance*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aero-chambers, inspirease, etc.
No Coinsurance*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic supplies, per prescription or refill. Six over-the-counter vials of insulin.
No Coinsurance*Tier 5: Not Covered
$6,850/$6,850$13,700/$13,700

8
Catastrophic Plan is best suited for:
Anyone looking for the lowest possible
premium while maintaining basic
coverage for accident and illness
Young adults rolling off of their parent’s
health plan
Those who are willing to exchange limited
benefits for lower premiums
Our Catastrophic Plan is designed to be the most afford-able option for those seeking low premiums. With higher deductibles and limited benefits, you may select either in-network or in and out-of-network coverage, allowing you the freedom to see healthcare providers outside of the network if you choose. Eligibility restrictions apply for Catastrophic Plans.
6
Covered Benefits HSA Plans
Bronze Level Plans Silver Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screen-ings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness 40%* No Coinsurance* No Coinsurance*
Other Practitioner Visits 40%* No Coinsurance* No Coinsurance*DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests)
40%* No Coinsurance* No Coinsurance*
Outpatient Services 40%* No Coinsurance* No Coinsurance*
Inpatient Services40%* No Coinsurance* No Coinsurance*
Hospital Emergency RoomDiagnosis must be emergent in nature) $300 per visit plus 40%* of
remaining charges
$300 Copay per visit, remain-ing charges apply toward
deductible*
$300 Copay per visit, remaining charges apply toward
deductible*Urgent Care Center
40%* No Coinsurance* No Coinsurance*
Ambulance Service40%*
Covered as In-Network benefit
No Coinsurance*
Maternity
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Diabetes Services
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Durable Medical Equipment, Prostetics, Orthotic
Appliances,
and Ostomy Supplies 40% No Coinsurance* No Coinsurance*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per pre-scription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
40%* No Coinsurance* No Coinsurance*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic supplies, per pre-scription or refill. Six over-the-counter vials of insulin. 40%*
Tier 5: Not CoveredNo Coinsurance*
Tier 5: Not CoveredNo Coinsurance*
Tier 5: Not Covered
$6,000/$6,550$12,000/$13,100
$3,750/$6,550$7,500/$13,100
$3,500/$4,500$7,000/$9,000
*Services are subject to the Medical Deductible
and apply toward the Medical Out-of-Pocket limit.
*HSA Choice Plans continued on next page.
*Services are subject to the Medical Deductible and apply toward
the Medical Out-of-Pocket limit.
**Catastrophic Plans have eligibility restrictions. Contact PHP for
more details.
Covered BenefitsCatastrophic
Plan**
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness
No Coinsurance*Deductible waived for first
3 primary care visits only.
Other Practitioner Visits No Coinsurance*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests).
No Coinsurance*
Outpatient ServicesNo Coinsurance*
Inpatient ServicesNo Coinsurance*
Hospital Emergency RoomDiagnosis must be emergent in nature. No Coinsurance*
Urgent Care CenterNo Coinsurance*
Ambulance ServiceNo Coinsurance*
Maternity Benefits based on service setting
Dibetes Services Benefits based on service setting
Durable Medical Equipment,
Prosthetics, Orthotic
Appliances, and
Ostomy Supplies
No Coinsurance*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aero-chambers, inspirease, etc.
No Coinsurance*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic supplies, per prescription or refill. Six over-the-counter vials of insulin.
No Coinsurance*Tier 5: Not Covered
$6,850/$6,850$13,700/$13,700
Catastrophic Plan

6
HSA Choice PlansCovered Benefits HSA Choice Plans
Bronze Level Plans Silver Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
In-Network Out-of-Network In-Network Out-of-Network In-Network Out-of-Network
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
50%*No charge
Deductible waived50%*
No charge Deductible waived
50%*
Doctor’s Office VisitIllness, injury, or sickness 40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Other Practitioner Visits40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests). 40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Outpatient Services 40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Inpatient Services40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Hospital Emergency Room$300 per visit plus 40%* of remaining
charges
Covered as In-Network benefit
$300 Copay pervisit, remainging charges
apply toward deductible*
Covered as In-Network benefit
$300 Copay per visit, remaining charges
apply toward deductible*
Covered as In-Network benefit
Urgent Care Center
40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Ambulance Service
40%*Covered as
In-Network benefitNo Coinsurance*
Covered as In-Network benefit
No Coinsurance*Covered as
In-Network benefit
MaternityBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service setting
Diabetes Services
Benefits based onservice setting
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Durable Medical Equipment,
Prostetics, Orthotic
Appliances,
and Ostomy Supplies
40%* 50%* No Coinsurance* 50%* No Coinsurance* 50%*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
40%*Not Covered No Coinsurance* Not Covered No Coinsurance* Not Covered
Mail Order Prescription DrugsUp to 90 day supply, including diabet-ic supplies, per prescription or refill. Six over-the-counter vials of insulin.
40%* Not CoveredNo Coinsurance*
Tier 5: Not CoveredNot Covered
No Coinsurance*Tier 5: Not Covered
Not Covered
$6,000/$6,550$12,000/$13,100
$3,750/$6,550$7,500/$13,100
$7,500/$20,000$15,000/$40,000
$12,000/$20,000$24,000/$40,000
*Services are subject to the Medical Deductible and apply toward the Medical Out-of-Pocket limit. 7
$7,000/$20,000$14,000/$40,000
$3,500$4,500$7,000/$9,000

8
Catastrophic Plan is best suited for:
Anyone looking for the lowest possible
premium while maintaining basic
coverage for accident and illness
Young adults rolling off of their parent’s
health plan
Those who are willing to exchange limited
benefits for lower premiums
Our Catastrophic Plan is designed to be the most afford-able option for those seeking low premiums. With higher deductibles and limited benefits, you may select either in-network or in and out-of-network coverage, allowing you the freedom to see healthcare providers outside of the network if you choose. Eligibility restrictions apply for Catastrophic Plans.
6
Covered Benefits HSA Plans
Bronze Level Plans Silver Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screen-ings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness 40%* No Coinsurance* No Coinsurance*
Other Practitioner Visits 40%* No Coinsurance* No Coinsurance*DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests)
40%* No Coinsurance* No Coinsurance*
Outpatient Services 40%* No Coinsurance* No Coinsurance*
Inpatient Services40%* No Coinsurance* No Coinsurance*
Hospital Emergency RoomDiagnosis must be emergent in nature) $300 per visit plus 40%* of
remaining charges
$300 Copay per visit, remain-ing charges apply toward
deductible*
$300 Copay per visit, remaining charges apply toward
deductible*Urgent Care Center
40%* No Coinsurance* No Coinsurance*
Ambulance Service40%*
Covered as In-Network benefit
No Coinsurance*
Maternity
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Diabetes Services
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Durable Medical Equipment, Prostetics, Orthotic
Appliances,
and Ostomy Supplies 40% No Coinsurance* No Coinsurance*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per pre-scription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
40%* No Coinsurance* No Coinsurance*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic supplies, per pre-scription or refill. Six over-the-counter vials of insulin. 40%*
Tier 5: Not CoveredNo Coinsurance*
Tier 5: Not CoveredNo Coinsurance*
Tier 5: Not Covered
$6,000/$6,550$12,000/$13,100
$3,750/$6,550$7,500/$13,100
$3,500/$4,500$7,000/$9,000
*Services are subject to the Medical Deductible
and apply toward the Medical Out-of-Pocket limit.
*HSA Choice Plans continued on next page.
*Services are subject to the Medical Deductible and apply toward
the Medical Out-of-Pocket limit.
**Catastrophic Plans have eligibility restrictions. Contact PHP for
more details.
Covered BenefitsCatastrophic
Plan**
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immunizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness
No Coinsurance*Deductible waived for first
3 primary care visits only.
Other Practitioner Visits No Coinsurance*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests).
No Coinsurance*
Outpatient ServicesNo Coinsurance*
Inpatient ServicesNo Coinsurance*
Hospital Emergency RoomDiagnosis must be emergent in nature. No Coinsurance*
Urgent Care CenterNo Coinsurance*
Ambulance ServiceNo Coinsurance*
Maternity Benefits based on service setting
Dibetes Services Benefits based on service setting
Durable Medical Equipment,
Prosthetics, Orthotic
Appliances, and
Ostomy Supplies
No Coinsurance*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aero-chambers, inspirease, etc.
No Coinsurance*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic supplies, per prescription or refill. Six over-the-counter vials of insulin.
No Coinsurance*Tier 5: Not Covered
$6,850/$6,850$13,700/$13,700
Catastrophic Plan

3
Applying for coverage is easy.
Make the choice to protect your family with the security of high-quality health coverage from PHP. Applying is easy. Just go to www.enroll.phpni.com. Apply online and compare the plans that are avail-able. You can also access more information about Indigo IndividualTM plans online at www.phpni.com.
Choose the best payment option for you.
Initial Payments may be made by checking or savings account, credit or debit card, or you mayreceive an invoice to pay by check or money order.
Ongoing Payments can be made several different ways. For your convenience, you may set-up a monthly automatic payment from your checking or savings account. You will receive an email prior to the due date notifying you of the amount that will be deducted from your account if you select this option.
You may also elect to receive a monthly invoice, either by U.S. mail or email. Once you receive the invoice, you may pay by check, money order, or make an online payment using your checking or savings account.
Try us out.
We want you to be satisfied and confident with your Indigo IndividualTM coverage. That’s why you have a “free-look” period to examine your policy when it is received. If for any reason within the free-look period you decide you no longer want the policy, simply return it to us and the policy will be cancelled and your premium refunded.
9
Covered Benefits Traditional Plans
Gold Level Plan Silver Level Plans Bronze Level Plan
CHOOSE YOUR COVERAGE LEVEL:
Single (Deductible/ Out-of-Pocket Max)
Family (Deductible/
Out-of-Pocket Max)
$1,250/$6,850$2,500/$13,700
Preventive ServicesServices rated ‘A’ or ‘B’ by the U.S. Preventive Services Task Force, and immu-nizations recommended by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention. Preventive care and screenings for women and children as recommended by the Health Resources and Services Administration. For a complete list, please visit our website.
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
No charge Deductible waived
Doctor’s Office VisitIllness, injury, or sickness $35 pre visit
$30 each for 3 visits per covered person, then 20%*
$30 each for 3 visits per covered person, then 30%*
$50 each for 3 visits per covered person, then 50%*
Other Practitioner Visits10%* 20%* 30%* 50%*
DiagnosticRoutine radiology and lab services (ex. chest x-ray, MRI, blood and urine tests). 10%* 20%* 30%* 50%*
Outpatient Services10%* 20%* 30%* 50%*
Inpatient Services$500 per visit plus 10%* of
remaining charges$500 per visit plus 20%* of
remaining charges30%* $500 per visit plus 50%* of
remaining charges
Hospital Emergency RoomDiagnosis must be emergent in nature. $300 per visit
plus 10%* of remaining charges$300 per visit plus 20%* of
remaining charges$300 per visit plus 30%* of
remaining charges$300 per visit plus 50%* of
remaining charges
Urgent Care Center
10%* 20%* 30%* 50%*
Ambulance Service
10%* 20%* 30%* 50%*
MaternityBenefits based on
service settingBenefits based on
service settingBenefits based on
service settingBenefits based on
service setting
Diabetes Services Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Benefits based on service setting
Durable Medical Equipment,
Prosthetics, Orthotic Appliances,
and Ostomy Supplies10%* 20%* 30%* 50%*
Prescription DrugsUp to 30 day supply, including diabetic supplies, per prescription or refill. Two over-the-counter vials of insulin. One-unit limit for inhaler aid devices such as aerochambers, inspirease, etc.
Tier 1/Tier 2: $15Tier 3: $45
Tier 4: 10%* Tier 5: 10%*
Tier 1/Tier 2: $15Tier 3: $45
Tier 4: 50%*Tier 5: 50%*
Tier 1/Tier 2: $10Tier 5: $30
Tier 4: 30%* Tier 5: 30%*
Tier 1/Tier 2: $25Tier 3: $60
Tier 4: 25%*Tier 5: 25%*
Mail Order Prescription DrugsUp to 90 day supply, including diabetic sup-plies, per prescription or refill. Six over-the-counter vials of insulin.
Tier 1/Tier 2: $45Tier 3: $135Tier 4: 10%*
Tier 5: Not Covered
Tier 1/Tier 2: $45Tier 3: $135Tier 4: 50%*
Tier 5: Not Covered
Tier 1/Tier 2: $30Tier 3: $90
Tier 4: 30%*Tier 5: Not Covered
Tier 1/Tier 2: $75Tier 3: 50%*Tier 4: 50%*
Tier 5: Not Covered
*Services are subject to the Medical Deductible and apply toward the Medical Out-of-Pocket limit.
$2,000/$6,850$4,000/$13,700
$2,500/$6,850$5,000/$13,700
$5,000/$6,850$10,000/$13,700

2
Phone Numbers
Voice: (260) 432-6690, ext. 810Toll-free: 1-800-982-6257, ext. 810Hearing Impaired: (260) 459-2600
Address
Attn: Individual Product Physicians Health Plan 8101 West Jefferson Blvd.Fort Wayne, IN 46804
[email protected] To help us provide excellent service, be sure to include your name and your daytime phone number.
Web Address
www.phpni.com
Eligibility Requirements
Individuals applying for coverage must be under 65 years old to qualify. Any covered dependent children must be under the age of 26 and either your son, daughter, step-child, or a child subject to legal guardianship, regardless of support level; or a grandchild or other blood relative who is more than 50% dependent on you for total support.
As the primary applicant, you must be a legal Indiana resident residing within our service area (a map of counties in our service area can be found on page 12).
10
Traditional Plans are best suited for:
Anyone wanting the security of a lower deductible plan
Families who regularly schedule doctor’s appointments and well-child visits
Those who prefer to pay less at the time of service
Of all our plans, Traditional Plans are most like group employer plans with copays or coinsurance for routine medical services. Be sure to take advantage of our preventive services benefit, with 100% coverage, to maintain your health. With the Traditional Plans, you may see any provider in our network, and the Choice Plans offer the additional flexibility of seeing out-of-network providers. Just select the deductible and out-of-pocket level that best meet your budget and financial needs.
Traditional Plans
MyNurse 24/7 Health concerns don’t always arise while the doc-tor’s office is open. Our members have access to a toll-free, 24-hour nurse line service for noncriti-cal situations. Members can speak with experi-enced, knowledgeable nurses who answer ques-tions with sound, clinically based information day or night.
MyHealth 24/7 This interactive, online resource acts as a 24-hour medical advisor to help find solutions to common health problems. Evaluate symptoms and overall health, use quizzes and calculators to improve and maintain weight, or search the pharmacy sec-tion to compare drugs and lower expenses.
HealthNEWS Newsletter
Members receive a quarterly newsletter that offers health and wellness information from nutrition and exercise, to seasonal health concerns and medical news. Each issue includes an update of our provider network as well as local events and member discounts.
Value-added services included with every Indigo IndividualTM health plan
Smoking Cessation
In keeping with our mission of encouraging preventive health maintenance, we offer coverage to help you in your goal to quit smoking. Additional information on the Indiana Quitline, tobacco inter-vention programs, community classes, and support groups to quit smoking are also provided.
Member Discounts
Our members are eligible to receive a variety of special discounts at select area health clubs, community classes, and facilities such as:
• Free trial memberships, discounts on enrollment fees, annual memberships, and training packages
• Discounts on medically supervised programs• Discounts on prescription eyewear• Sporting event discounts
A complete listing of member discounts is available online at www.phpni.com.
Open Enrollment for 2016
Generally you and your family can only purchase new coverage during the annual open enrollment period. For 2016, this period is November 1, 2015 through January 31, 2016. Outside of this annual open enrollment period, you may still be eligible to purchase coverage if you experience a qualified special enrollment event, such as a marriage, birth of a child, change in enrollment, etc.

Our commitment to you.
Excellence in customer service and greater freedom are only a few reasons our members are happy with PHP year after year. We are committed to providing you with the best service.
Because we are based right here in Northern Indiana, we offer easy access to the largest local network of healthcare providers, hassle-free claims processing, unmatched personal attention, and helpful resources for the health and well-being of our community.
An ounce of prevention
is worth a pound of cure. All of our plans pay 100% of many important preven-tive services including well-baby care, immunizations, mammograms, pap tests, and annual physical exams when ordered by a participating provider.
Emergency care benefits that
apply anywhere in the world.
While traveling, members are covered should emergency services be needed. Just show your member ID card at the time of service.
Health coverage for
individuals and families.
Indigo IndividualTM
1
PHP Service
AreaApplicants must reside
in one of these counties to be eligible for coverage.
11
Providing you the tools
to manage your healthcare.
You have around-the-clock access to powerful online resources at www.phpni.com. Whether you are look-ing for a physician, researching drug information, or checking your personal account for benefit, claim, deductible, and out-of-pocket information, our Web site allows you to take charge of your health when it’s most convenient for you.
Features of our plans:
• Preventive Services covered at 100% for all plans (Complete list of services found at www.phpni.com)• All plans available as an Individual or Family Policy• Many value-added benefits included automatically: 24-hour nurse line, extensive online health resources, member discounts for health facilities and more• Prescription drug coverage available with all plans• Competitive premium rates • Negotiated provider costs to save you money • Exceptional customer service to help you understand and make the most of your health coverage
The next several pages help you compare the various types of plans we have available:
Traditional Plans Most like traditional employer plans with copays and/or coinsurance for routine medical services.HSA Plans Qualified high-deductible health plans that can be used in conjunction with a Health Savings Account. Catastrophic Plans Basic coverage for accident and illness with the lowest possible premiumChoice Plans Plans that provide you the flexibility to use healthcare providers outside of the network.

TM
8101 West Jefferson Blvd.Fort Wayne, IN 46804
www.phpni.com
2016 Indigo IndividualTM
Purchaser GuideYour guide to buying PHP health plans for individuals and families.
©2015 PHPNI, Inc.October 2015 www.phpni.com