Embed Size (px)
DESCRIPTION
patient safety
Citation preview

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 1/28
Top 10Patient Safety
Concerns forHealthcare
Organizations

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 2/28
Publisher: ECRI Institute
EXECUTIVE STAFF
Jeffrey C. Lerner, Ph.D.Presiden and Chief Execuive Officer
Anthony J. Montagnolo, M.S.Execuive Vice Presiden andChief Operaing Officer
Ronni P. Solomon, J.D.Execuive Vice Presiden andGeneral Counsel
Vivian H. Coates, M.B.A.Vice Presiden, Informaion Servicesand Technology Assessmen
Michael Argentieri, M.S., BMEVice Presiden, Marke Developmen
Mark E. Bruley,
CCEVice Presiden, Acciden andForensic Invesigaion
G. Daniel Downing, M.B.A.Vice Presiden, Finance
James P. Keller, Jr., M.S.Vice Presiden, Healh TechnologyEvaluaion and Safey
Jennifer L. Myers
Vice Presiden, SELECT HealhTechnology Services
Thomas E. Skorup, M.B.A., FACHEVice Presiden, Applied Soluions
David W. Watson, Ph.D.
Vice Presiden, Operaions,ECRI Insiue Europe
Jin Lor, MIE (Aus)Regional Direcor, Souheas Asia
MISSION STATEMENT
ECRI Insiue is an independennonprofi organizaion whose missionis o benefi paien care by promoinghe highes sandards of safey, qualiy,and cos-effeciveness in healhcare.We accomplish his hrough ourresearch, publishing, educaion, andconsulaion.
Our goal is o be he world’s mosrused, independen, organizaionproviding healhcare informaion,research, publishing, educaion andconsulaion o organizaions andindividuals in healhcare.
ECRI Insiue, 5200 Buler PikePlymouh Meeing, PA 19462-1298, USATel + 1 (610) 825-6000
Download additional copies of this
report and access more resources at
www.ecri.org/PatientSafetyTop10.

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 3/28
©2015 ECRI Institute.APRIL 2015 3
Top 10 Patient Safety Concerns for Healthcare Organizations
Introduction
NOT JUST A TOP 10 LIST
Wih his repor, ECRI Insiue is releasing is op 10 lis of paien safey concerns for 2015. This is he second year we
have compiled he lis, which is parly based on our review of paien safey even repors, research requess, and roo-
cause analyses submited o ECRI Insiue PSO, one of he firs paien safey organizaions (PSOs) o be federally cerified
under he provisions of he Paien Safey and Qualiy Improvemen Ac (PSQIA).
PSQIA gives healhcare organizaions a unique opporuniy o volunarily share heir safey surveillance daa in a
proeced environmen so PSOs can aggregae and analyze he daa. The law also charges PSOs wih he responsibiliy
o share he findings and lessons learned. The release of our op 10 lis of paien safey concerns is in keeping wih haresponsibiliy.
ECRI Insiue’s Top 10 Paien Safey Concerns for Healhcare Organizaions is more han jus a lis; i’s a reminder ha,
despie he atenion given o paien safey over he las 15 years or so, we can do beter. Since we began collecing paien
safey evens in 2009 as a PSO, we have received nearly 500,000 even repors. Each even ofen describes a sysems-relaed
breakdown, or a near failure, in he care process of he paiens our members are commited o serving. Some of he evens
describe serious, prevenable paien injuries or deahs.
Behind each even here’s a sory abou paiens and heir loved ones who pu hemselves in he hands of heir provid-
ers expecing qualiy care and services. And here’s a separae sory abou he providers whose lives and careers are orn
apar when paiens are harmed because fauly sysems and processes make problems more likely o occur.
Our paien safey analys Sheila Rossi, who shares her own encouner wih a medicaion error in his year’s repor,
reminds us of he sories behind hese evens and he moivaion for our op 10 lis. “When we say ‘he paien’ in healh-care, i someimes becomes impersonal,” Rossi says, urging everyone o pu hemselves in paiens’ shoes and o ask,
“How do I preven his from happening o me?”
Healhcare providers, regardless of wha seting hey pracice in, can sar wih our op 10 lis of paien safey concerns
and use i o guide heir own discussions abou paien safey and improvemen iniiaives.
We will coninue o publish our op 10 lis annually because we are commited o paien safey and o helping you o
deliver he safes care for all of us, your paiens.
Sincerely,
William M. Marella, MBA
Execuive Direcor, Operaions and Analyics
ECRI Insiue’s Paien Safey, Risk, and Qualiy Group

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 4/28
©2015 ECRI Institute. APRIL 20154
Top 10 Patient Safety Concerns for Healthcare Organizations
Top 10 Patient Safety Concerns
for Healthcare Organizations: 2015
ECRI Insiue has released is newes lis of he op 10 paien safey concerns confroning
healhcare organizaions. The lis serves as a “caalys for discussion” among healhcare lead-
ers abou he op paien safey issues faced by heir organizaions, says Caherine Pusey,
RN, MBA, manager, clinical analyss a ECRI Insiue PSO.
ECRI Insiue’s Top 10 Paien Safey Concerns for Healhcare Organizaions for 2015 is compiled
by ECRI Insiue PSO, one of he firs paien safey organizaions (PSOs) o be federally cerified.
“The lis is based on wha we see hroughou he year among he paien safey even repors,
research requess, and roo-cause analyses submited o ECRI Insiue PSO,” says Pusey.
Under he Paien Safey and Qualiy Improvemen Ac, healhcare organizaions canvolunarily submi paien safey repors o PSOs in a proeced environmen for PSOs o
aggregae, analyze, and share findings and lessons learned. ECRI Insiue PSO has been
collecing paien safey daa since 2009 and, by he end of 2014, had received nearly 500,000
even repors.
The lis also draws upon ECRI Insiue saff experise,
including he knowledge gained invesigaing incidens,
observing and assessing hospial pracices, and review-
ing healh-echnology-relaed problem repors submited
o ECRI Insiue’s volunary medical device problem
reporing program. In fac, four of he paien safey con-
cerns idenified for he op 10 lis also rank among ECRIInsiue’s op healh echnology hazards for 2015. Refer o
“ECRI Insiue’s Top 10 Liss” for more informaion on he
healh echnology hazard lis, which is compiled by ECRI
Insiue’s Healh Devices Group.
“Mos organizaions have heir own op 10 lis. They
should review our lis of paien safey concerns o idenify
issues ha should be on heirs,” says Pusey. “We’re no
saying ha every organizaion mus address all 10 opics,
bu hey should deermine where here are similariies and
variaions.”
Using ECRI Insiue’s op 10 lis proacively o improvequaliy of care and paien safey is also in keeping wih
he provisions of he Join Commission’s recenly released
paien safey sysems chaper for is 2015 accredia-
ion manual. The chaper describes he imporance and
srucure of an inegraed approach o paien safey for
healhcare organizaions.
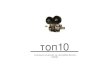
1 Alarm hazards: inadequate alarm configurationpolicies and practices*
2Data integrity: incorrect or missing data in EHRsand other health IT systems
3 Managing patient violence
4Mix-up of IV lines leading tomisadministration of drugs and solutions*
5Care coordination events related to medicationreconciliation
6Failure to conduct independent double checksindependently*
7 Opioid-related events
8Inadequate reprocessing of endoscopes andsurgical instruments
9Inadequate patient handoffs related to patienttransport*
10Medication errors related to pounds andkilograms*
ECRI Institute’s Top 10 Patient Safety Concerns for 2015
*New to the 2015 list.
M S 1 5 1 3 8

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 5/28
©2015 ECRI Institute.APRIL 2015 5
Top 10 Patient Safety Concerns for Healthcare Organizations
Half of he iems on he op 10 lis are new for 2015; he oher half are recurring or varia-
ions of concerns from 2014 when ECRI Insiue firs released is op 10 lis of paien safey
concerns. Refer o “ECRI Insiue’s Top 10 Paien Safey Concerns for 2015” for he full lis.
Iems from he 2014 lis ha do no appear on his year’s lis, such as mislabeled
laboraory specimens and paien falls while oileing, sill remain a concern, says Pusey.
“Bu oher opics have risen o a higher level of atenion.”
APPLICABILITY TO MULTIPLE SETTINGS
Many of he opics on ECRI Insiue’s lis of op 10 paien
safey concerns exend o muliple healhcare setings and
highligh he relevance of hese issues o he coninuum
of care spanning physician pracices and oher oupaien
medical setings, acue care hospials, and aging services
providers in posacue care environmens, nursing homes,
and hospice care.
“While some of hese hazards are mos applicable
o acue care, several are also relevan in ambulaory
setings, and some—especially hose relaed o medicaions
and care coordinaion—span he coninuum of care,” saysWilliam M. Marella, MBA, execuive direcor, operaions
and analyics for ECRI Insiue’s Paien Safey, Risk, and
Qualiy group.
Because he opics on ECRI Insiue’s lis of paien
safey concerns are largely based on repors submited
by hospials, hese issues, while imporan o muliple
healhcare setings, may no always rank among he op
10 concerns for nonhospial setings, such as physician
pracices and aging services providers. For example, appro-
priae managemen of alarms is imporan in long-erm
care setings such as nursing homes where alarms are used
o deec residen wandering and elopemen, falls, and
oher risks, says Vicor Lane Rose, NHA, MBA, CPASRM,
operaions manager of ECRI Insiue’s Aging Services Risk
Managemen program wihin is Paien Safey, Risk, and
Qualiy group. The opic, however, may no rank as aging
services providers’ number one concern, he adds, because
oher issues, such as skin managemen, appropriae saffing
and scheduling, and falls managemen, are ypically
among he highes prioriies for he aging services secor.
Hospital
AgingServices
M S 1 5 1 3 9
AmbulatoryCare
Many of the Top 10 Safety Events Span
Multiple Healthcare Settings

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 6/28
©2015 ECRI Institute. APRIL 20156
Top 10 Patient Safety Concerns for Healthcare Organizations
ECRI Institute’s Top 10 Lists
ECRI Insiue’s op 10 liss of paien safey concerns and healh echnology hazards highligh four overlapping issues ha deservehe atenion of healhcare organizaions. Togeher, hey reflec a unied effor by ECRI Insiue o promoe paien safey in healh-care organizaions.
ECRI Insiue’s Top 10 Health Technology Hazards , released every fall, focuses on echnology, whereas ECRI Insiue’s Top 10Patient Safety Concerns for Healthcare Organizations addresses broader paien safey issues. Like he lis of paien safey concerns, heop 10 lis of healh echnology hazards reflecs ECRI Insiue’s healhcare safey experise. The lis is compiled based on he saff’sexperience invesigaing device-relaed incidens, evaluaing medical devices in ECRI Insiue’s esing laboraory, and reviewingrepors from ECRI Insiue’s and oher organizaions’ daabases for medical device problems and paien safey evens.
ECRI Insiue has published is lis of healh echnology hazards for eigh years and is lis of paien safey concerns for woyears. Boh liss are published annually.
Despie he differen focuses of he wo liss, Caherine Pusey, RN, MBA, manager, clinical analyss a ECRI Insiue PSO, issruck ha wo differen eams idenified four overlapping areas as prioriies for healhcare organizaions in 2015. “Separaely,we are idenifying some of he same issues.” The four overlapping concerns are as follows:
1. Alarm hazards from inadequae alarm configuraion policies and pracices2. Daa inegriy failures from incorrec or missing daa in EHRs and oher healh IT sysems
3. IV line mix-ups leading o misadminisraion of drugs and soluions
4. Inadequae reprocessing of endoscopes and surgical insrumens
In fac, hese four echnology-relaed opics are he op four iems idenified in ECRI Insiue’s Top 10 Health TechnologyHazards for 2015. The overlap of hese four prioriy opics “shows he significance of healhcare echnology as i impacs paiensafey overall,” says James P. Keller, MS, vice presiden, healh echnology evaluaion and safey, ECRI Insiue. “A big reasonwhy echnology shows prominenly on he op 10 lis of paien safey concerns is he growing complexiy of echnology and heincreased reliance on echnology in delivering healhcare,” he says, lising areas such as healh IT and alarm hazards.
The 2015 repor of healh echnology hazards also has some broader opics ha span muliple echnologies. One was insuf-ficien cybersecuriy proecions for medical devices and sysems. “Despie litle evidence o dae of direc harm o paiens,cybersecuriy is neverheless a poenial hrea ha healhcare faciliies mus begin addressing,” says Rob Schluh, senior projec
officer a ECRI Insiue and he lead projec manager for ECRI Insiue’s Top 10 Health Technology Hazards for 2015 projec. “Thevulnerabiliy of medical devices o malware ha could affec device funcionaliy or he inegriy of paien daa is of paricularconcern.” ECRI Insiue predics ha cybersecuriy is a paien safey consideraion ha will require increased atenion in hecoming years.
Anoher broad opic on he 2015 op echnology hazards lis was deficien medical device recall and safey-aler managemenprograms. “We see healhcare organizaions wih aniquaed recall managemen programs,” says Schluh. “One key concern wehave is ha he capabiliies of some hospials’ programs may no be keeping pace wih he growh over he pas decade in henumber of recalls and oher alers ha are issued.”
ECRI Insiue also publishes an annual wach lis of he op 10 echnology and infrasrucure issues ha a hospial C-suieshould carefully examine. The lis draws upon ECRI Insiue’s decades of experience evaluaing he safey, effeciveness, and cos-effeciveness of healh echnologies.
“C-suie leaders need a concise way of seeing where new and emerging healh echnologies fi, if a all, in heir healh sys-ems,” says Diane Roberson, direcor, healh echnology assessmen, ECRI Insiue.
Topics on he 2015 C-suie lis include he following:
Z Disinfecion robos
Z Three-dimensional priners
Z Google Glass
Z Posdischarge clinics
All hree repors are publicly available from ECRI Insiue’s websie. Top 10 Health Technology Hazards for 2015 is publiclyavailable a htps://www.ecri.org/Pages/2015-Hazards.aspx. The 2015 Top 10 Hospital C-Suite Watch List is freely available ahtps://www.ecri.org/Pages/ECRI-Insiue-2015-Top-10-Hospial-C-Suie-Wach-Lis.aspx.
Top 10 Patient Safety Concerns for Healthcare Organizations

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 7/28
©2015 ECRI Institute.APRIL 2015 7
Top 10 Patient Safety Concerns for Healthcare Organizations
ECRI Insiue recommends ha healhcare organizaions
use is op 10 lis of paien safey concerns as a saring
poin for heir paien safey discussions and for se-
ing heir paien safey prioriies. Use he lis o idenify
wheher he organizaion has experienced paien safey
breakdowns in similar areas and wheher he concerns
should be argeed for improvemen. For areas seleced
for improvemen, organizaions can creae risk miiga-
ion sraegies based on he recommendaions providedwih he op 10 lis for each area of concern. Addiional
ECRI Insiue resources, some freely available on ECRI
Insiue’s websie, are highlighed hroughou he repor.
“Our hope is ha healhcare providers use his lis o
reflec on which of hese hazards exis in heir care setings
and on wheher hey have sysems in place o preven or
minimize harm from hose ha are relevan in heir se-
ings,” says Marella.
Rose recommends ha faciliies across he healhcare
specrum use he lis o “undersand he risks ha do exis
a your organizaion, o quanify hem, and o find ouwhere hey’re happening so he organizaion can idenify
pracices o miigae he risks.”
Given ha paien safey improvemens can ofen
require an invesmen in saff ime and he organizaion’s
resources, Pusey recommends ha organizaions presen
he lis o heir senior leaders and members of heir govern
ing boards o gain heir atenion and suppor.
How the List
Was Compiled
To compile is lis of paien safey concerns, ECRI Insiue
PSO reviewed is daabase of paien safey evens, roo-
cause analyses, and cusom research requess submited
hroughou he year by healhcare organizaions and is
parner PSOs, as well as sough guidance from is eam of
expers.
“Our op 10 lis isn’ generaed from a complicaed
algorihm or formula. I’s very much a consensus process
ha atemps o disill he judgmen of ECRI Insiue’spaien safey expers, our advisors, and our members,”
says Marella. “Topics are nominaed based on our analysis
of safey evens repored o ECRI Insiue and our parner
PSOs as well as wha’s happening in he broader paien
safey communiy.”
The final lis reflecs he inpu of ECRI Insiue PSO’s
eam of analyss and oher ECRI Insiue saff, as well as
members of ECRI Insiue PSO’s advisory council.
How to
Use the List

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 8/28

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 9/28
©2015 ECRI Institute.APRIL 2015 9
Top 10 Patient Safety Concerns for Healthcare Organizations
1. Alarm Hazards: Inadequate Alarm
Confguration Policies and Practices
Topping he lis of paien safey concerns is alarm hazards from inadequae alarm configura-
ion policies and pracices, a opic which also ranks as ECRI Insiue’s op healh echnology
hazard for 2015.
Since ECRI Insiue began publishing is lis of op healh echnology hazards in 2007,
“alarm hazards have been a or near he op of he lis,” says Rob Schluh, senior projec offi-
cer a ECRI Insiue and he lead projec manager for he Top 10 Healh Technology Hazards for 2015 projec. The need o address alarm hazards is paricularly imporan wih he Join
Commission’s ongoing Naional Paien Safey Goal for healhcare organizaions o improve
he safey of clinical alarm sysems.
In recen years, much of he lieraure relaed o alarm hazards has focused on alarm
faigue—a condiion ha can lead o alarms missed by providers who are overwhelmed by,
disraced by, or desensiized o he muliple alarms ha acivae.
In is 2015 lis, ECRI Insiue encourages healhcare insiuions o look beyond alarm
faigue. “In addiion o missed alarms ha can resul from excessive alarm acivaions, hospi-
als also have o be concerned abou alarms ha don’ acivae when a paien is in disress,”
says Schluh. “In our experience, alarm-relaed adverse evens—wheher hey resul from
missed alarms or from unrecognized alarm condiions—ofen can be raced o alarm sysemsha were no configured appropriaely.”
To mee he Join Commission’s Naional Paien Safey Goal on clinical alarm safey,
organizaions accredied by he group mus, as of 2016, esablish policies and procedures
o manage alarm signals idenified by he organizaion as essenial for paien safey. ECRI
Insiue recommends ha organizaions examine heir alarm configuraion policies and pro-
cedures o address he full range of facors ha can lead o alarm hazards.
“Our acciden invesigaions have found ha hospials have eiher no had consisen or no
had any pracices o deermine how alarms are se by care area or by paien ype,” says James
P. Keller, MS, vice presiden, healh echnology evaluaion and safey, ECRI Insiue. For
example, “i doesn’ make sense o use he same defaul alarm setings in pediaric inensive
care as in adul inensive care,” he explains, ye ECRI Insiue has found ha many hospials
do no have a policy o adjus he alarm defaul setings by care area. Similarly, hospial
policies ofen fail o specify when and who can make adjusmens o he defaul alarm setings,
says Keller.
In addiion o he recommendaions for addressing alarm hazards conained in he Top 10
Healh Technology Hazards for 2015 , ECRI Insiue has compiled is Alarm Safey Handbook and
Alarm Safey Workbook o help organizaions undersand he breadh of alarm hazards, idenify
alarm safey vulnerabiliies, and develop an effecive program for managing clinical alarms o
improve paien safey. The maerials are provided as a membership benefi for cerain ECRI
Insiue programs and are available o ohers for purchase. See “ECRI Insiue Resources” for
more informaion.
* Some ECRI Insiue resourcesare publicly available. To obainoher ECRI Insiue repors,conac us by elephone a (610)
825-6000, ex. 5891, or by e-maila [email protected].
ECRI INSTITUTE
RESOURCES
HRC
Z Clinical Alarms
Other Memberships
and Sources*
Z The Alarm SafetyHandbook: Strategies,Tools, and Guidance and accompanyingworkbook.
Z Alarm SafeyResource Cener
Z Inerfacing Monior-ing Sysems wihVenilaors: How Well
Do They Communi-cae Alarms? (HealthDevices)
Z Physiologic Monior-ing Sysems: Our
Judgmens on EighSysems (HealthDevices)
Z Top 10 Health Technol-ogy Hazards for 2015

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 10/28
©2015 ECRI Institute. APRIL 201510
Top 10 Patient Safety Concerns for Healthcare Organizations
Healh informaion echnology (IT)–relaed issues have been a recurring heme on ECRI Insiue’s
op 10 liss, appearing on he op 10 healh echnology hazards lis for he las six years and on
he op 10 lis of paien safey concerns since is sar in 2014. For he wo mos recen years, boh
liss have idenified daa inegriy errors as a resul of incorrec or missing daa in elecronic healh
records (EHRs) and oher healh IT sysems.
ECRI Insiue recognizes ha healh IT offers numerous poenial benefis, such as suppor-ing clinical decision making, enhancing provider communicaion, providing access o paien
daa in a secure environmen, engaging paiens, and reducing medical errors. Bu he echnology
can creae new safey risks if i is no designed appropriaely, implemened carefully, and used
houghfully.
In fac, in 2014, ECRI Insiue convened he Parnership for Healh IT Paien Safey , a muli-
sakeholder collaboraive esablished o proacively idenify and address healh IT paien safey
risks in a nonpuniive environmen.
“Wih he inroducion of any new echnology, we need o idenify and respond o novel prob-
lems i presens as well as old problems ha he new echnology doesn’ eliminae,” says Marella.
Daa inegriy issues “exised wih paper medical records as well, bu now as EHRs become more
ineroperable, incorrec informaion is more readily available, more easily shared, and harder oeliminae,” he says. “In order o ge a reurn on he invesmen we’ve made in EHRs and clinical
decision suppor, we now need o ackle he more mundane problem of making sure he daa in he
EHR is accurae.”
“We’ve seen he rapid growh of healh IT sysems, paricularly in he hospial seting,” says
Keller. “Organizaions need o have beter esing of he sysems and checks and balances [afer
implemenaion] o make sure failure poins for missing daa or incorrec daa enries are ideni-
fied and addressed.” As an example, consider he following even repored o ECRI Insiue PSO
and is parner PSOs involving wo separae healh IT sysems—an EHR sysem and a dieary
managemen program:
The paien’s peanu allergy was lised in he EHR bu he informaion did no cross over o he dieary
deparmen’s sysem. The paien quesioned wheher he food allergy informaion had been received by hedieary deparmen afer receiving a food ray ha was no idenified as free of peanu producs.
The near miss highlighed he need for a sofware fix o ensure ha imporan paien daa from
he EHR is ransferred o he organizaion’s dieary IT sysem for paien menu managemen.
2. Data Integrity: Incorrect or
Missing Data in EHRs and OtherHealth IT Systems

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 11/28
©2015 ECRI Institute.APRIL 2015 11
Top 10 Patient Safety Concerns for Healthcare Organizations
Examples of daa inegriy failures, as lised in he Top 10 Healh Technology Hazards for
2015 repor, include he following:
X Appearance of one paien’s daa in anoher paien’s record
X Missing daa or delayed daa delivery
X Clock synchronizaion errors beween medical devices and sysems
X Defaul values being used by misake, or fields being prepopulaed wih
erroneous daa
X Inconsisencies in paien informaion when boh paper and elecronic records
are used
X Oudaed informaion being copied and pased ino a new repor
To correc hese problems, organizaions mus idenify daa inegriy failures as hey
occur in order o apply fixes o preven similar problems from recurring. To do so, hey mus
empower fronline workers and healh IT sysem users o repor all ypes of healh IT-relaed
incidens, including hose ha do no cause any harm as well as near-miss incidens, and
circumsances ha precede an acual even and are caugh before anyhing can happen.
Through is problem and even reporing programs, ECRI Insiue has found ha healh-care saff do no always recognize healh IT’s conribuion o an even. For example, only
afer analysis of an inciden in which a pharmacis placed a medicaion order in he wrong
paien’s record was i recognized ha he error was faciliaed by a medicaion managemen
sysem ha allowed users o have muliple paien records open a he same ime. Reporing
he even as jus a medicaion error overlooks oher conribuing facors, such as he healh
IT sysem’s configuraion o permi muliple paien records o be open on a user’s screen.
“When reporing an adverse even or near miss, saff should consider wheher
some funcion or feaure of a healh IT sysem could have conribued o he problem,” says
Schluh.
Some even reporing programs give reporers he abiliy o idenify he repor as a healh
IT-relaed issue. For example, he Agency for Healhcare Research and Qualiy’s mos recenversion of he Common Formas (version 1.2) includes an even repor for healh IT evens
and unsafe condiions. The Common Formas are used by PSOs and heir paricipaing pro-
viders for even reporing and allow daa aggregaion in a sysemaic manner.
ECRI INSTITUTE
RESOURCES
HRC
Z Elecronic Healh
Records
Other Memberships
and Sources
Z ECRI Institute PSODeep Dive: HealthInformation Technology
Z Healh IT ParnershipProceedings: Parner-ing for Success
Z How o Connecwih he Righ EMRInegraion Vendor (Health Devices)
Z Making Connec-ions: InegraingMedical Devices wihElecronic Medi-cal Records (HealthDevices)
Z Paien Safey aInersecion of Medi-cal and InformaionTechnology (PSONavigator)
Z Top 10 Health Technol-ogy Hazards for 2015

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 12/28
©2015 ECRI Institute. APRIL 201512
Top 10 Patient Safety Concerns for Healthcare Organizations
Every day, U.S. hospials deal wih violen paien incidens and hreaening behaviors ha
affec he safey and well-being of saff, paiens, and visiors. According o curren lieraure
on he opic, violence is occurring in all care setings, even in oncology and maerniy unis,
and no jus in he emergency deparmen (ED).
Clinical saff in acue care unis ypically lack raining in behavioral healh and may dis-
miss or poorly handle behavioral cues ha signal imminen violence, says Ruh Ison, MDiv,STM, paien safey analys/consulan a ECRI Insiue PSO. Ison noes ha repors submi-
ed o ECRI Insiue PSO and is parner PSOs show ha docors, nurses, ancillary saff, and
even securiy officers working in emergency and acue care setings are grealy challenged
in managing paiens who become violen or hreaen violence. In 2014, failure o adequaely
manage hreaening or violen behavior of paiens in acue care setings was among ECRI
Insiue’s op 10 paien safey concerns.
The range and impac of paien violence across he hospial is no limied o incidens
ha make he headlines. Clinical saff may feel abandoned and lef wihou he resources o
do heir jobs safely, given he frequency wih which hey mus manage violen behavior in
paiens—a leas 15 incidens a day, according o one PSO member hospial.
The firs hing ha hospial leadership mus do is acknowledge ha violence is occurringwihin he faciliy’s walls, says Judy Gushue, RN, BS, MJ, CEN, CPHQ, paien safey analys,
ECRI Insiue PSO. When healhcare workers perceive assauls and hreas as a workplace
hazard ha mus be oleraed, hey underrepor—resuling in lack of awareness and inac-
ion by hospial leadership. “Lack of psychiaric services and inervenions pus pressure on
nurses and oher fronline saff o be rained in violence de-escalaion echniques,” she poins
ou.
Ison believes ha raining saff in de-escalaion sraegies is a smar invesmen ha can
improve paien and worker safey on many levels, reducing coercion and empowering saff
o engage, raher han avoid, paiens wih agiaion or hreaening behavior while promo-
ing safe condiions. The effor may prove o be more cos-effecive han use of unrained
“siters,” who have been menioned in PSO even repors as he arges of atacks by paiens,
Ison says. The siter’s presence or behavior may be perceived by he paien as provoca-
ive, as he siter is placed in he posiion of prevening he paien from engaging in cerain
unsafe behaviors, she noes. Unrained siters may no be sensiive o he paien’s clinical
siuaion, may no fully undersand he recommended safey precauions, or may argue wih
he paien. Oher siter behaviors (e.g., exing, chating, playing games on a smarphone)
migh resul in siter inatenion or even provoke a violen response from he paien.
3. Managing Patient Violence

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 13/28
©2015 ECRI Institute.APRIL 2015 13
Top 10 Patient Safety Concerns for Healthcare Organizations
Gushue adds ha in addiion o requiring reporing and providing saff raining in de-
escalaion sraegies and skills, he hospial should have a faciliy-wide safey plan ha
considers all levels of risk, from he single acue episode of hreaening behavior o an acive
shooer siuaion anywhere in he faciliy or on campus. “Know he risks posed by your
paien populaion—local police saisics may help idenify areas of risk or peak periods
when risk may be greaer.” The program should address physical securiy and response(e.g., use of hidden alarms, cameras, elecronic saff locaor services, increased sraegic secu-
riy presence, limiing sies of enrance and egress a nigh), implemening and monioring
compliance wih policies and procedures for inspecing belongings of visiors and paiens
for weapons, reconfiguring ED waiing areas, invoking emergency legal processes for com-
mimen or reamen (when appropriae), and esablishing a rained rapid response eam o
assess poenial violen behavior and inervene when summoned.
Ison agrees: he acue sympoms ha demonsrae a paien’s behavioral or medical
inabiliy o cooperae wih care inervenions should no be misinerpreed by healhcare
workers as unwillingness; however, “aggressive or agiaed behavior signals a high-risk,
high-acuiy siuaion ha needs immediae clinical atenion comparable o a sroke, cardiac,
or respiraory even.” Ison has idenified he following paien facors from ECRI Insiue
PSO even repors involving violen paien behavior: acue subsance abuse or addicion,acue wihdrawal, drug-seeking behavior, psychosis, possurgical saus, and various medi-
cal and menal healh comorbidiies (e.g., neurologic disorders, infecions, delirium, adverse
prescripion drug reacions, developmenal disabiliies) combined wih behavioral healh
sympoms (e.g., paranoia, moor agiaion, emoional volailiy) and social dislocaion.
Clinical managemen sraegies can include sanding orders and medicaion order ses
ha can be acivaed immediaely by he saff on duy, as well as securiy measures. And
while acuely agiaed or hreaening, violen paiens should never be handed off, as hese
are emergency siuaions. Subsequen handoff communicaion of he paien’s medical saus
should include idenificaion of acue socioemoional or behavioral healh issues ha are
adversely affecing he paien, Ison says. These migh be addressed by social workers or
behavioral healh saff.Diminishing he risks involved wih paien violence sars wih acceping is realiy
across healhcare setings, Gushue says. The experise of leadership, managemen, and
clinical saff a all levels is needed o develop a comprehensive response ha mees hese
vulnerable paiens’ medical needs and keeps all healhcare saff safe in he process.
ECRI INSTITUTE
RESOURCES
HRC
Z Paien Violence Z Workplace Violence
Prevenion Plan
Z Violence Risk Assess-men Tool for HomeCare
Other Memberships
and Sources
Z Residen Aggres-sion and Violence (Continuing Care Risk
Management)
Z Residen Aggression/Violence AssessmenTool (Continuing CareRisk Management)

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 14/28
©2015 ECRI Institute. APRIL 201514
Top 10 Patient Safety Concerns for Healthcare Organizations
4. Mix-Up of IV Lines Leading to
Misadministration of Drugs andSolutions
Inravenous (IV) line mix-ups can lead o medicaion errors, resuling in wrong-drug,
wrong-rae, wrong-dose, or wrong-sie infusions, some wih serious consequences. Paiens,
paricularly hose in criical care setings, can have muliple IV infusions, increasing he risk
of connecing he line o he wrong infusion pump, wrong fluid conainer, or wrong adminis-
raion roue.
Paiens may have oher inerfering facors, such as leads and cables for physiologic moni-ors, increasing he risk of misakes wih IV line mix-ups, says Keller. Someimes described
as “spagheti syndrome” or he angle of ubes, caheers, and cables ha engulf paiens, he
muliple lines “make i harder o rack he source of an IV line as i leads from he paien’s
inserion sie o he original source,” he says.
In he following even repored o ECRI Insiue PSO and is parner PSOs, an older
paien received oo much heparin because he IV lines for heparin and saline were
misconneced:
The ED paien was suspeced of having a hear atack and was sared on a high-risk proocol for
IV heparin. Afer he paien was ransferred o he uni, he nurse noiced ha he heparin bag was
almos empy. The nurse checked he pump and saw ha i was running a he faser rae inended for
he saline soluion. The ubing lines were mixed up, and he heparin ran for four hours a he faserrae, resuling in he paien receiving seven imes as many unis of heparin as inended. The paien
was reaed for a heparin overdose and ransferred o he criical care uni.
Alhough he risk of IV line mix-ups is pronounced in he criical care seting, he risk also
exiss in oher acue care setings, as he above even illusraes, and in nonhospial setings,
such as a nursing home, where residens may require, for example, boh an IV anibioic and
pain medicaion. Alhough paiens in hese setings may have fewer lines, misakes can sill
occur, paricularly if he provider does no have he same advanced raining as a criical care
nurse o ensure safey, says Keller.

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 15/28
©2015 ECRI Institute.APRIL 2015 15
Top 10 Patient Safety Concerns for Healthcare Organizations
Among ECRI Insiue’s recommendaions o preven IV infusion-line confusion are he
following:
X Trace all lines back o heir origin before making connecions. Doing so verifies ha
he correc lines will be joined. Lines should be rechecked upon he paien’s arrival
in a new seting or service and a shif changes as par of he handoff process.
X Develop a policy of posiioning differen lines on differen sides of he paien. Con-sisenly puting lines in he same place migh make i easier for clinicians o correcly
idenify hem and connec hem appropriaely.
X Label each infusion line wih he name of he drug or soluion being infused.
X Do no force connecions. If a connecion is difficul o make—ha is, if i requires a
lo of effor—chances are i should no be made.
Separaely, misconnecions can also occur when ubing from one delivery sysem is
misconneced o a sysem inended for a differen purpose (e.g., an eneral feeding pump
being conneced o an IV line). New connecor sandards are being developed o reduce his
risk; however, he sandards will no preven all line misconnecions. Once he new design
sandards for connecors are fully in place, IV lines will coninue o use he same ype of con-
necor, making i possible o sill have IV infusion mix-ups.
ECRI Insiue recommends using posers o remind saff abou sraegies o preven ub-
ing misconnecions. For example, ips for clinical saff are summarized in a poser developed
by ECRI Insiue summarizing is TRACER™ program o preven ubing misconnecions.
Informaion for obaining he poser from ECRI Insiue, as well as oher resources, is pro-
vided in “ECRI Insiue Resources.”
ECRI INSTITUTE
RESOURCES
HRC
Z Prevening Miscon-
necions of Lines andCables
Z Invasive Lines
Other Memberships
and Sources
Z Be a T.R.A.C.E.R. noa RACER! (poser)
Z Choosing a SyringeInfusion Pump (Health Devices)
Z Fixing Bad Linkso Preven TubingMisconnecions (PSO
Navigator) Z Infusion Pump Ine-
graion: Why Is INeeded and WhaAre he Challenges? (Health Devices)
Z Paien-ConrolledAnalgesic InfusionPumps: Making aPainless Purchase (Health Devices)
Z Top 10 Health Technol-ogy Hazards for 2015
Z Which Smar PumpsAre Smares? Raings for Six Large-VolumeInfusion Pumps (Health Devices)

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 16/28
©2015 ECRI Institute. APRIL 201516
Top 10 Patient Safety Concerns for Healthcare Organizations
A every care ransiion, such as admissions, ransfers, and discharges, “he paien’s medi-
caions should be reconciled o ensure he paien is on he correc medicaions for he nex
phase of care,” says Mary Beh Michell, MSN, RN, CPHQ, CCM, SSBB, paien safey analys
and consulan a ECRI Insiue PSO. Inadequae medicaion reconciliaion pus paiens a
risk for medicaion errors, inadequae follow-up care, and hospial readmissions.
On admission, medicaion reconciliaion is challenging o conduc effecively unless hepaien or family members have kep accurae records of he paien’s medicaions, says
Michell. To ensure he lis’s accuracy, she recommends verifying he paien’s medicaion
lis wih anoher source, such as he paien’s primary care physician and/or pharmacy. The
backup approach is no fail-safe, however, if he paien goes o muliple pharmacies or is
seen by muliple specialiss, “all of whom may order prescripions for he paien,” she says.
Providers should also ask abou any over-he-couner and herbal medicaions ha he paien
may be aking, as well as any ransdermal paches ha are in place.
A faciliy migh also refer o he paien’s las medical record from a previous say o
idenify he paien’s lis of medicaions a discharge. “Bu ha may no be a good source forinformaion if i’s been a long ime since he paien’s las hospializaion or if he paien has
had medicaion changes by heir primary care physician and/or specialiss,” says Michell.
The paien’s medicaions may have changed if he previous hospializaion was no recen, asin he following even repored o ECRI Insiue PSO and is parner PSOs:
The paien was admited hrough he ED. The paien brough a lis of curren medicaions. The lis
was compared o he paien’s medicaion lis from a previous say. Two oher medicaions, an anipsy-
choic drug and a diabees medicine, from he previous say were no on he paien’s medicaion lis
and were ordered. No one wen over he paien’s curren medicaion lis wih he paien. During he
paien’s say, he paien’s wife repored he paien was having hallucinaions and seemed coninually
drowsy when ha wasn’ he paien’s norm. I was deermined ha he paien had no aken he wo
addiional medicaions for a year, so hey were disconinued.
When a paien is admited for care, providers may decide o disconinue some or all of
he paien’s medicaions aken before he admission in order o address he paien’s acue
needs. They may also inroduce new medicaions o rea he acue condiion. As he paien’scondiion improves or changes and when he paien is ransferred o anoher level of care,
clinicians mus coninue o evaluae he paien’s medicaion needs, deciding wheher o dis-
coninue he medicaions for he acue condiion, inroduce any new drugs, or resume any of
he medicaions ha he paien ook before admission.
“By he ime he paien is ready for discharge, hey should no be receiving new medica-
ions ha hey did no receive while in he hospial,” says Michell. “The poin of conducing
medicaion reconciliaion every sep along he way of he hospializaion is ha by he ime
he paien is ready for discharge, hey should be on he righ medicaions and he healhcare
providers should know ha he paien can olerae he medicaions when aken ogeher.”
5. Care Coordination Events
Related to MedicationReconciliation

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 17/28
©2015 ECRI Institute.APRIL 2015 17
Top 10 Patient Safety Concerns for Healthcare Organizations
While EHRs can improve communicaion among providers abou paiens’ medicaions,
Michell warns o use he echnology cauiously. For example, a discharge, don’ simply
prin he paien’s lis of medicaions wihou assigning someone o go hrough he lis o look
for errors, such as dosing errors and duplicae orders for similar drugs wih differen names,
she recommends. In addiion, some EHRs allow only one person o reconcile he medicaions,
which means ha ha physician mus be sure of all of he medicaions and recommended
doses from he specialis physicians.
If he paien is being discharged o anoher healhcare seting, medicaion reconciliaion
can only be achieved by effecively managing he paien’s discharge from he hospial and
he admission o he oher faciliy, such as a nursing home or subacue care faciliy, says Rose.
“Boh pieces need o be managed . . . for medicaion reconciliaion o work well,” he says.
If he discharge and admission process from one faciliy o anoher is poorly managed,
paien care can suffer. “Medicaions ha were disconinued a he hospial may no be
resared when he person comes back o an aging services provider or reurns home,” says
Rose. The aging services provider mus hen coordinae wih he hospial and physicianwho was overseeing he paien’s care or he paien’s primary care physician o idenify
he paien’s medicaions. “I’s no an easy process and can lead o delays in resuming he
paien’s care,” Rose says.
Typically, aging services providers conduc char checks wihin 24 hours of a residen’s
reurn o he faciliy afer a hospial discharge o review he residen’s medicaions, o see
if anyhing was sopped or added, and o deermine if here’s a reason for he change, says
Rose. If he residen is new o he faciliy, he organizaion will verify ha informaion wih
he individual’s primary care physician.
There are many ways o manage medicaion reconciliaion. Some publicly available
resources for medicaion reconciliaion recommend pharmacis-led inervenions, bu here
are oher approaches as well. A good mechanism o ensure ha he medicaion reconciliaion
process works well is o proacively evaluae he process using a failure mode and effecs
analysis (FMEA) o idenify gaps in ha process. Consider involving he pharmaciss, case
managers, nursing, and oher FMEA eam members in idenifying soluions o close he gaps,says Michell. “Pharmaciss don’ necessarily need o lead he inervenions, bu hey need o
be involved wih he mulidisciplinary eam in closing he gap,” she says.
Rose, who also recommends ha aging services providers conduc a similar proacive
analysis of heir medicaion reconciliaion processes, encourages hospials and aging services
providers o engage each oher in he medicaion reconciliaion assessmen. “Find ou where
he risks exis and have inelligen conversaions wih your care parners in he communiy o
pu pracices in place o miigae hem,” he says. Refer o “ECRI Insiue Resources” for addi-
ional informaion.
ECRI INSTITUTE
RESOURCES
HRC
Z Discharge Planning
Z Medicaion Safey Z Subacue Care in
Long-Term CareSetings

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 18/28
©2015 ECRI Institute. APRIL 201518
Top 10 Patient Safety Concerns for Healthcare Organizations
In blood banking, having wo praciioners perform an independen double check of he
blood group before ransfusion is a long-sanding requiremen. “Nobody in he universe
would hink of doing a blood ransfusion wihou doing an independen double check firs
because you could kill he paien prety quickly,” saes Elizabeh Drozd, MS, MT(ASCP)
SBB, CPPS, paien safey analys, ECRI Insiue PSO. “Bu for high-aler medicaions, we’ve
seen a lo of conroversy abou doing independen double checks and have seen a lo of fail-ures in ha process.”
The following wo evens repored o ECRI Insiue PSO and is parner PSOs illusrae
how failures in independen double checks can affec paiens:
Paien was receiving a heparin drip, which required a double check per policy. The dosing nomo-
gram and rae were double-checked appropriaely, bu here was no double check when he nurse
changed he rae on he infusion pump. The drip rae was changed o 18 mL/hr insead of 15 mL/hr,
resuling in an elevaed parial hromboplasin ime wih bleeding from he IV sie.
An independen double check was no compleed when a paien-conrolled analgesia (PCA) pump
was se, resuling in a 10-fold opioid overdose. Naloxone was adminisered, and he paien was rans-
ferred o he inensive care uni (ICU).
When double checks are used, one major issue is he failure o conduc hem in a way hais ruly independen. As he second provider, “I wan o check your work oally indepen-
denly of wha you’re elling me,” says Drozd. “I wan o look a everyhing,” such as paien
ideniy, indicaion and appropriaeness, drug or blood ype, dose, programmed infusion rae,
and roue.
To achieve ruly independen double checks, he organizaion needs saff buy-in. “They
have o undersand why independen double checks are done independenly,” Drozd
emphasizes. Imporanly, he process mus be free of he poenial for confirmaion bias. For
example, if he firs provider asks he second provider, “I go 5,000 unis of heparin. Wha do
you ge?” he second provider is already biased oward a specific dose and drug. A provider
may overly rely on he second provider’s check, possibly skipping seps, if he or she expecs
ha simply doing a double check will cach any errors or believes ha he second provider“doesn’ make misakes.”
6. Failure to Conduct Independent
Double Checks Independently

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 19/28
©2015 ECRI Institute.APRIL 2015 19
Top 10 Patient Safety Concerns for Healthcare Organizations
In addiion, he organizaion mus be judicious when deciding which processes require
an independen double check. A common misake is o “add a double check as a soluion o
everyhing,” says Drozd, poenially leading o double check faigue. Insead, “use indepen-
den double checks wih a lo of cauion and only for processes ha could harm he paien
very, very quickly.”
Sysems issues should also be invesigaed. For example, if policies and proceduresrequire an independen double check in a paricular siuaion bu a second provider is ofen
unavailable, saff may use workarounds or even skip he double check.
How can organizaions invesigae wheher hey are performing independen double
checks in a way ha is ruly independen? “The only way, really, is o begin o audi and
observe he acual process,” says Drozd. “You have o be ou here in he paien care areas
and observe,” using a checklis of wha o look for. This approach is labor-inensive, bu
“i’s also your opporuniy o link wih he individuals o explain he imporance of doing i
properly.”
Alhough here are many poenial barriers o ruly independen double checks, he
Insiue for Safe Medicaion Pracices (ISMP) calculaes ha hey can deec up o 95% of
errors. “When done properly, hey do deec a significan amoun of errors,” says Drozd.
ECRI INSTITUTE
RESOURCES
HRC
Z Ask HRC: Conduc-
ing and DocumeningDouble-Checks forMedicaion Safey
Z High-AlerMedicaions
Z Blood Transfusions

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 20/28
©2015 ECRI Institute. APRIL 201520
Top 10 Patient Safety Concerns for Healthcare Organizations
7. Opioid-Related Events
“The use and he prescribing of opioids has significanly increased in recen years,” says
Sephanie Uses, PharmD, MJ, JD, paien safey analys, ECRI Insiue PSO, and “ha’s one
of he reasons opioid safey has become more of an issue.” According o he U.S. Deparmen
of Healh and Human Services’ Naional Acion Plan for Adverse Drug Even Prevenion , he
number of prescripion opioids dispensed doubled beween 1999 and 2010, and by he end of
ha period, he number of relaed deahs exceeded he number of overdose deahs involvingheroin and cocaine combined. The number of ED visis relaed o opioid misuse and abuse
oaled more han 420,000 in 2011—double he number of visis in 2004.
Problems relaed o opioid overdose, such as over-sedaion and respiraory depression,
are a major paien safey concern, bu hey are no he only ones. Oher issues include gas-
roinesinal adverse evens (e.g., nausea, vomiing, consipaion), hyperalgesia, prurius, and
immunologic or hormonal dysfuncion.
Among evens in ECRI Insiue’s PSO daabase, he problem is “no specific o any one
opioid,” says Uses. However, hose commonly involved in evens are hydromorphone, oxy-
codone, opioids used in PCA, and fenanyl paches.
Two issues are especially concerning. Firs, “some of he more common errors wih hydro-
morphone are due o is poency,” says Uses. Hydromorphone is abou seven imes as poenas morphine, bu physicians someimes prescribe he same amoun of hydromorphone
as hey would morphine, leading o overdose, as in he following even repored o ECRI
Insiue PSO and is parner PSOs:
Paien presens o ED wih abdominal pain. The paien’s pain is poorly relieved wih morphine
4 mg; atending physician changes pain orders o hydromorphone 4 mg inravenously every 4 hours
as needed. The paien’s nurse adminisers a dose of hydromorphone. Shorly afer he dose is given,
he nurse noices decreased responsiveness, he paien becomes apneic, and code blue is called. Two
doses of naloxone are given. Paien becomes responsive and is ransferred o he inensive care uni for
monioring.
Second, prescribers someimes fail o disinguish paiens who are opioid-oleran (hose
who have been aking an opioid of a leas a cerain hreshold dosage for a leas a week) fromhose who are opioid-naïve (hose who have no). For example, opioid-naïve paiens should
no be prescribed fenanyl paches, and hese paiens should receive only very low doses of
susained-release oxycodone, if he drug is used a all. They should no receive coninuous
infusion when PCA herapy is iniiaed; raher, bolus-only herapy should be used.

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 21/28
©2015 ECRI Institute.APRIL 2015 21
Top 10 Patient Safety Concerns for Healthcare Organizations
Opioid-relaed evens are no resriced o he hospial. For example, oxycodone and
fenanyl paches may be used in long-erm and ambulaory care setings and a home. In
addiion, family members or friends may inappropriaely ake he paien’s medicaions o
self-rea heir pain, or he drugs may be oherwise misused or abused by he paien or oh-
ers. ISMP has also repored on incidens, including deahs, in children and older aduls wih
cogniive impairmen who have suck fenanyl paches on heir bodies or ingesed hem.“Fenanyl is so poen,” says Uses, “a young child will sop breahing righ away” afer
ingesing or applying a fenanyl pach.
Alhough many sraegies should be employed o promoe safey hroughou he medica-
ion-use process, Uses highlighs a few key inervenions o preven and miigae he kinds of
evens ECRI Insiue PSO is seeing.
Prescribers should be educaed abou opioid safey and he evens ha can resul. One
cenral issue is appropriae prescribing. “Does he paien really require an opioid?” says
Uses. “Someimes ha’s no he firs choice ha we need o go o.” Order ses—wih differ-
en drug forms and dosages for opioid-naïve and opioid-oleran paiens, for example—may
help guide clinicians as well.
In hospials, saff should be rained o monior for sedaion. “A lo of imes, people don’monior for sedaion and don’ recognize sedaion as a problem unil he paien is already
experiencing respiraory depression,” Uses cauions. The Pasero Opioid Sedaion Scale is one
ool ha saff can use o monior for opioid-induced sedaion.
A home and in oher nonhospial setings, paiens and caregivers mus know how o
appropriaely sore and dispose of opioids. These drugs should no be kep in easy view and
reach of ohers, and disposal opions include ake-back days, locked drop boxes, and appro-
priae disposal a home.
To invesigae opioid-relaed evens hey are experiencing, healhcare organizaions can
no only look a heir adverse even daabase bu also use rigger ools—for example, by
running daily repors o idenify when naloxone, a reversal agen, is dispensed. Faser noi-
ficaion allows for easier invesigaion of evens, and “you can rack and rend and see whayour problems are,” Uses noes.
ECRI INSTITUTE
RESOURCES
HRC
Z High-Aler
Medicaions Z Pain Medicaion and
PRN Orders
Z Paien-ConrolledAnalgesia
Z Infusion Pumps
Other Memberships and
Sources
Z ECRI Institute PSODeep Dive: MedicationSafety
Z Pain Relief: How oKeep Opioid Admin-israion Safe (PSONavigator)
Z Pasero Opioid Seda-ion Scale (POSS)wih Inervenions
Z Prevening Opioid-Induced RespiraoryDepression (webinarfor ECRI InsiuePSO)

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 22/28
©2015 ECRI Institute. APRIL 201522
Top 10 Patient Safety Concerns for Healthcare Organizations
Reprocessing of endoscopes and surgical insrumens, a op 10 paien safey concern and
healh echnology hazard for 2014, reurns o boh op 10 liss for 2015. In fac, reprocessing
has been raised as a op 10 healh echnology hazard for six years in a row.
“We coninue o see reprocessing issues in our acciden invesigaions” and in media repors,
says Schluh. Addiionally, as ECRI Insiue was preparing Top 10 Healh Technology Hazards for
2015 , he Ebola virus had become fron-page news, furher “highlighing he criical imporanceof he reprocessing funcion,” says Schluh.
The poenial harm o paiens from he ransmission of infecious agens remaining on
reusable devices can be severe. More han half of he “immediae hrea o life” findings from
Join Commission surveys conduced in 2013 were direcly relaed o improper equipmen
reprocessing, Schluh noes.
Healhcare faciliies reprocess housands of reusable surgical insrumens and devices
every day for subsequen use. No only are he devices difficul o clean, bu “muliple seps
are required o ge i righ,” says Keller. Each sep mus be properly performed from sar
o finish. For example, if he devices are no horoughly cleaned, organisms may remain on
he devices, unaffeced by disinfecion or serilizaion. Similarly, if he devices are no hor-
oughly dried in he final reprocessing sep, “hey are a breeding ground for organisms ogrow posprocessing,” says Keller.
8. Inadequate Reprocessing
of Endoscopes and SurgicalInstruments

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 23/28
©2015 ECRI Institute.APRIL 2015 23
Top 10 Patient Safety Concerns for Healthcare Organizations
ECRI INSTITUTE
RESOURCES
HRC
Z Reprocessing of
Flexible Endoscopes Z Reprocessing in
Cenral Service
Z Endoscope Reprocess-ing: The Imporanceof Being Proacive
Other Memberships
and Sources
Z CRE and Duodeno-scope ResourceCener
Z Clear Channels:Ensuring Effecive
Endoscope Repro-cessing (HealthDevices)
Z Inadequaely Repro-cessed Insrumens:If I’s Diry, How CanI Be Clean? (PSO
Monthly Brief )
Z Serile ProcessingDeparmen’s Role inPaien Safey (PSONavigator)
Z Top 10 Health Technol-
ogy Hazards for 2015
Furher complicaing he reprocessing funcion are he muliple ypes of devices, each
wih heir own cleaning and disinfecion or serilizaion insrucions, says Keller. If auo-
maed reprocessing sysems are used for endoscope disinfecion, each device model will
likely require unique model-specific channel adapers o properly flush each channel of he
device, he adds.
Any ime a change is inroduced o reprocessing, such as a new disinfecan, cleaningagen, or channel cleaning brushes, he impac of he change needs o be evaluaed for any
ripple effec on he qualiy of he process. For example, afer being asked o invesigae
an infecion oubreak in an endoscopy clinic, ECRI Insiue discovered ha he clinic had
swiched o a new cleaning soluion ha required a longer soak ime for insrumens han
required wih he previously used cleaning soluion. The clinic’s reprocessing procedures
were no longer effecive, because he clinic had no adjused he insrumen soak ime
required wih he new soluion.
In addiion o he recommendaions for ensuring adequae device reprocessing lised
in Top 10 Healh Technology Hazards for 2015 , oher guidance from ECRI Insiue is lised in
“ECRI Insiue Resources.”

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 24/28
©2015 ECRI Institute. APRIL 201524
Top 10 Patient Safety Concerns for Healthcare Organizations
“Transporing a paien wihin he hospial o anoher clinical seting or beween unis
wihin he faciliy presens risk of harm o he paien and, depending on he needs of he
paien, can be an unsetling experience for nurses charged wih caring for he paien, and
for he ransporer,” says Kelly Graham, BS, RN, paien safey analys a ECRI Insiue PSO.
Safe ranspor involves idenifying and providing appropriae resources and requiremens
for each paien during ranspor and includes proper handoff communicaion o and fromappropriaely rained ransporers. Paiens may be ranspored o he wrong deparmen,
he wrong paien may be ranspored, or paiens may be lef unmoniored a he receiving
sie. A sandardized process for paien ranspor and handoff communicaion can reduce risk
during ranspor and a he sending and receiving ends of he process, Graham says.
Risks of ranspor vary wih paien acuiy. “Ideally, he level of care provided dur-
ing ranspor pairs wih he care he paien receives in he uni,” Graham adds. Criically
ill paiens, for example, are exposed o periods of poenial insabiliy during ranspor.
Mainaining oxygenaion during ranspor and acivaing a code when a paien’s condiion
rapidly deerioraes during ranspor are bu a few examples of poenial risk.
To enhance safey, criically ill paiens are ypically ranspored by eams of qualified crii-
cal care providers wih defined roles for monioring and ensuring venilaor suppor. Theranspor process and relaed communicaion is guided by formal policy reflecing guidelines
from he Sociey of Criical Care Medicine and he American College of Criical Care Medicine
for ransporing criically ill paiens. Bu because danger is inheren in he ranspor process of
all paiens, faciliy ranspor policy and procedures should guide handoff communicaion for
he safe ranspor of he non-ICU paien.
The Join Commission requires ha each paien handoff communicaion include a
sandardized and ineracive approach for he safe ransfer of a paien from one care area o
anoher. Handoffs are an inegral par of safe ranspor, and wihou careful atenion o hand-
off communicaion and ranspor safey a each poin in he ranspor process, errors can occur,
Graham says.
Noably, of 2,390 paien-ranspor-relaed repors submited o he Pennsylvania PaienSafey Auhoriy from May 2004 hrough Sepember 2008, 41% involved communicaion
issues, according o an aricle in he March 2009 Pennsylvania Paien Safey Advisory. ECRI
Insiue PSO and is parner PSOs have received repors involving ineffecive handoffs in
he paien ranspor process ha have conribued o paien harm in a variey of care se-
ings. The following repor provides an example of inadequae handoff communicaion
during ranspor of an infan wihin a hospial:
Immediaely afer undergoing a surgical procedure, he infan was ranspored o he neonaal
inensive care uni (NICU) in an open crib. Saff in he uni had no been informed ha he infan’s
9. Inadequate Patient Handoffs
Related to Patient Transport

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 25/28
©2015 ECRI Institute.APRIL 2015 25
Top 10 Patient Safety Concerns for Healthcare Organizations
ECRI INSTITUTE
RESOURCES
HRC
Z Communicaion
Z Safe Paien MobiliyPolicy andProcedure
Other Memberships
and Sources
Z Handoffs: Oppor-uniy for Safe Care (PSO Navigator)
body emperaure dropped in he operaing room (OR), or ha he infan was ranspored direcly
from he OR o he uni, and ha he infan had no been moniored in a recovery uni. A nurse pre-
paring he infan for he NICU say expressed concern abou he infan’s pale coloring and slowed
respiraion. The baby was given vigorous spinal simulaion in an effor o resore breahing and
reurn body emperaure o normal, and required inubaion when breahing did no fully respond o
he spinal simulaion.Graham recommends ha faciliies’ even and near-miss reporing sysems capure
ranspor-relaed incidens and near misses ha occur “off uni” and during ranspor. Such
repors can idenify gaps in policies, procedures, or raining; he need for improved com-
municaion processes and oversigh for follow-up and monioring of handoff proocols; and
oher problems ha may require reassessmen of ranspor policies and procedures.
Graham suggess ha ranspor policies and procedures be based on consideraion of
numerous issues, he following among hem:
X Idenifying unis are mos ofen involved in ranspor and safey hazards paricular o
he unis
X Developing crieria for deermining he level of ranspor eam needed (depending on
paien assessmen and he level of care required)X Ensuring availabiliy of equipmen, assigning responsibiliy for mainenance of hera-
pies during ranspor, and roubleshooing equipmen during ranspor
X Deermining raining, experience, and compeency required of ranspor personnel
in ligh of expeced levels of inervenion ha may be required during ranspor
X Developing and implemening ools and checkliss o suppor handoff communicaion
among he care eam, ranspor personnel, and saff a he receiving sie
Policies and procedures migh incorporae use of a ranspor form, ofen referred o as
a “Ticke o Ride” form, ha helps convey essenial informaion from he sending uni,
provides a checklis o be addressed by ranspor saff and by he receiving uni, and incor-
poraes a siuaion-background-assessmen-recommendaion (SBAR) forma o enhance
communicaion a each end of he process. ECRI Insiue has also developed handoff com-municaion sraegies ha address ranspor. For addiional informaion, see “ECRI Insiue
Resources.”

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 26/28
©2015 ECRI Institute. APRIL 201526
Top 10 Patient Safety Concerns for Healthcare Organizations
The paien safey evens presened in his repor are no jus saisics, as he issue of pound-
kilogram mix-ups illusraes. “We definiely see hese evens in he PSO daa,” says Sheila
Rossi, MHA, paien safey analys/consulan, ECRI Insiue PSO. Bu she gained a firs-
hand undersanding of he issue hrough her own personal experience.
On a visi o a local ED, Rossi’s wo-year-old son was weighed in he riage room. Laer,
he physician deermined ha he needed wo oral medicaions, o be given by Rossi and herhusband. “Having previously given him wo similar medicaions a home, we had some
idea of he dosing based on his age and weigh,” Rossi says. When he nurse brough in wo
big syringes, Rossi and her husband said, “Wow, ha looks like a lo of medicaion,” and
quesioned he amoun. “Almos in unison, he nurse and he docor said, ‘I’s weigh-based
dosing.’” Sill rusing heir insinc ha somehing wasn’ righ, Rossi and her husband gave
heir son a porion of each dose, disposing of he excess in a napkin, afer he providers lef
he room.
The nex morning, he physician called and apologized, informing Rossi ha here had
been a mix-up in he weigh-based calculaion. Their son had been weighed in pounds, bu
his 30-pound weigh had been enered ino he EHR as 30 kilograms (equivalen o abou 66
pounds). The oral syringes had each conained roughly wice he amoun of medicaion heshould have received; forunaely, neiher was a high-aler medicaion. Bu, says Rossi, “My
concern wasn’ so much for my child; my concern was for he nex child ha comes along
and wha sysem fixes hey were going o make so ha his would no occur again.”
Mix-ups beween pounds and kilograms are no limied o EDs and hospials; hey can
happen “anyplace ha has a scale,” says Rossi. And alhough he problem poses “a huge
poenial for error wih aduls,” children and older aduls may be even more sensiive o
medicaion dosing errors. Similarly, overdoses involving high-aler medicaions pose a par-
icular paien safey concern. Consider he following even repored o ECRI Insiue PSO
and is parner PSOs, which involved an older adul:
Weigh was enered in he EHR incorrecly. The employee used pounds for kilograms. A low-molec-
ular-weigh heparin was dosed for more han double he paien’s weigh. The pharmacy discovered heerror, and he order was disconinued. The anicoagulaion saus of he paien was moniored.
10. Medication Errors Related to
Pounds and Kilograms

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 27/28
©2015 ECRI Institute.APRIL 2015 27
Top 10 Patient Safety Concerns for Healthcare Organizations
ECRI INSTITUTE
RESOURCES
HRC
Z Medicaion Safey:
Inaccurae PaienWeigh Can CauseDosing Errors
Z Medicaion Safey
Other Memberships
and Sources
Z Medicaion Safey:Inaccurae PaienWeigh Can CauseDosing Errors (PSONavigator)
One of he mos effecive sraegies o reduce he risk of such errors is o “ge rid of scales ha
measure in pounds,” says Rossi. There are many barriers o employing his sraegy. For exam-
ple, i requires subsanial capial, and parens ofen wan o know heir child’s weigh in pounds.
Alernaives may include adjusing elecronic scales so ha hey display only in kilograms and
giving parens weigh conversion chars. “If you can ge rid of ha mix-up a he very firs sep in
he process, pounds are never inroduced ino he equaion,” says Rossi.Oher high-impac sraegies include he following:
X Ensuring ready availabiliy of pediaric scales (e.g., o reduce reliance on parenal
esimaes, which are likely o be in pounds)
X Recording and displaying weigh only in kilograms in he EHR
X Inegraing digial scales wih he EHR o eliminae or reduce he need for daa enry
X Using clinical decision suppor funcions ha compare enered weigh wih expeced
weigh (e.g., based on growh chars)
X Purchasing infusion pumps wih dose error reducion feaures
X No soring in clinical areas any high-aler drugs or oher medicaions ha have he
poenial o cause paien harm if weigh-based doses are miscalculaedTo invesigae his issue, organizaions may sar by reviewing heir even-reporing sys-
ems. Bu ha may yield limied informaion because “i assumes ha people are acually
reporing hese evens as weigh-based errors,” Rossi noes. Char audis and observaion
can help he organizaion explore furher. “How are paiens being weighed, wha scales are
used, how is he weigh enered ino he EHR, where are he chances for error?” says Rossi.
Rossi’s encouner offers some moivaion and perspecive for all paien safey evens.
“When we say ‘he paien’ in healhcare, i someimes becomes impersonal, and we see he
paien as someone else, a body or objec o which care is delivered and in some cases bad
evens or oucomes occur. We have all been or will become ‘paiens’ a some poin in our
lives,” says Rossi. “How are we going o improve paien safey for ourselves? How do we pu
ourselves in he paien’s shoes and say, ‘How do I preven his from happening o me?’”

7/21/2019 2015 Patient Safety Top10
http://slidepdf.com/reader/full/2015-patient-safety-top10 28/28
Z UNITED STATES
5200 Butler Pike,
Plymouth Meeting, PA
19462-1298, USA
Telephone +1 (610) 825-6000
Z EUROPE
Suite 104, 29 Broadwater Road
Welwyn Garden City,
Hertfordshire, AL7 3BQ, UK
Telephone +44 (1707) 871 511
Z ASIA PACIFIC
11-3-10, Jalan 3/109F,
Danau Business Centre,
Taman Danau Desa,
58100 Kuala Lumpur, Malaysia
Z MIDDLE EAST
Ofce No. 1101, 11th Floor,
Al Shafar Tower 1, TECOM
P.O. Box 128740
Dubai, United Arab Emirates