Embed Size (px)
DESCRIPTION
MUSCULOSKELETAL TUMORS AND DISEASESSelf-Scored Self-Assessment Examination2014
Citation preview

MUSCULOSKELETAL TUMORS AND DISEASES
Self-Scored Self-Assessment Examination
2014

Musculoskeletal Tumors and Diseases Self-Scored Self-Assessment Examination 2014
Figure 1a
Figure 1b
Figure 1c
CLINICAL SITUATION FOR QUESTIONS 1 THROUGH 4
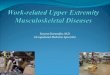
Figures 1a through 1c are the radiograph, CT scan, and bone scan of a 49-year-old woman
admitted to the hospital with right hip pain and an inability to bear weight for 2 days. She
states that the pain began 3 months ago, but suddenly progressed just before her admission.
Question 1 of 143
You decide to obtain further imaging. The best test to order would be
1- ultrasound of the thyroid.
2- MRI scan of the pelvis.
3- CT scan of the chest, abdomen, and pelvis.
4- indium-labeled bone scan.
PREFERRED RESPONSE: 3- CT scan of the chest, abdomen, and pelvis.
Question 2 of 143
Given the scenario, what is the most likely finding on histopathologic review?
1- Metastatic adenocarcinoma
2- Ewing sarcoma
3- Lymphoma of bone
4- Hip joint sepsis
PREFERRED RESPONSE: 1- Metastatic adenocarcinoma
Question 3 of 143
The preferred surgical intervention for this fracture is
1- Radical resection and reconstruction
2- Intramedullary nail fixation

3- Cannulated screw fixation
4- Complex total hip arthroplasty
PREFERRED RESPONSE: 4- Complex total hip arthroplasty
Question 4 of 143
External beam radiotherapy
1- should include the instrumented femur and periacetabular area.
2- should include the femur only.
3- should include the acetabulum only.
4- is contraindicated for this patient.
PREFERRED RESPONSE: 1- should include the instrumented femur and periacetabular
area.
DISCUSSION
The occurrence of a femoral neck fracture in a relatively young patient with no history of
trauma should alert the physician to potential for an underlying pathological process. The
most likely culprit would be metastatic disease, myeloma, or lymphoma. Systemic imaging is
undertaken to determine whether a primary site or site(s) of metastasis can be discovered.
Only after obtaining tissue can the definitive diagnosis be made. Common primary
malignancies that metastasize to bone are breast, lung, prostate, renal, and thyroid
carcinomas. Multiple myeloma and lymphomas may also have a similar appearance in the
bone. In this instance, not only is the femoral neck fractured, but there is a substantial lytic
process in the acetabulum as well as other skeletal sites of involvement. Therefore, complex
hip arthroplasty is the best choice for surgical intervention. Radiotherapy is indicated in the
care of this patient as well. Generally, the radiation field should include the entirety of the
involved implants plus a margin of tissue around them. In this case, this would include the
entire progression of instrumented femur and the periacetabular area. This approach
minimizes risk for local recurrence and transplanted tumor during instrumentation and/or as a
result of postoperative ecchymosis or bleeding. There is no indication for preoperative
radiation in this scenario.
RECOMMENDED READINGS
Buecker PJ, Rothrock CP. Current management of skeletal metastasis. Orthopaedic Knowledge Online Journal. 2010.
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg
Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149. View Abstract at PubMed
Question 5 of 143
Li-Fraumeni syndrome (LFS) is associated with

1- multiple hemangiomas.
2- multiple hereditary osteochondromatosis.
3- soft-tissue sarcomas.
4- neurofibromatosis.
PREFERRED RESPONSE: 3- soft-tissue sarcomas.
DISCUSSION
LFS is a rare genetic condition characterized by an increased risk for developing multiple
types of cancer. The most common types of cancers associated with LFS include soft-tissue
sarcomas (tumors in fat, muscle, nerves, joints, blood vessels, bones, or deep skin), breast
cancer, leukemia, lung cancer, and brain tumors. The cancers that occur in LFS can be
diagnosed during childhood, adolescence, or adulthood. Most people with LFS are found to
have mutations in the TP53 gene. Multiple hemangiomas, osteochondromas, and
neurofibromatosis are not associated with LFS.
RECOMMENDED READINGS
Chompret A. The Li-Fraumeni syndrome. Biochimie. 2002 Jan;84(1):75-82. PubMed PMID: 11900879.
View Abstract at PubMed
Moule RN, Jhavar SG, Eeles RA. Genotype phenotype correlation in Li-Fraumeni syndrome kindreds and its implications for management.
Fam Cancer. 2006;5(2):129-33. Review. PubMed PMID: 16736281.
View Abstract at PubMed
Olivier M, Goldgar DE, Sodha N, Ohgaki H, Kleihues P, Hainaut P, Eeles RA. Li-Fraumeni and related syndromes: correlation between tumor type, family structure, and TP53 genotype. Cancer Res. 2003 Oct 15;63(20):6643-50. PubMed PMID: 14583457.
View Abstract at PubMed
Wong P, Verselis SJ, Garber JE, Schneider K, DiGianni L, Stockwell DH, Li FP, Syngal S. Prevalence of early onset colorectal cancer in
397 patients with classic Li-Fraumeni syndrome. Gastroenterology. 2006 Jan;130(1):73-9. PubMed PMID: 16401470. View Abstract at PubMed
Question 6 of 143
A 60-year-old woman has a proximal femur fracture. A permeative, lytic defect is recognized
at the fracture site. Appropriate imaging studies are performed and show no other lesions.
What is the next treatment step?
1- Cephalomedullary nail
2- Standard antegrade intramedullary nail
3- Resection and arthroplasty reconstruction
4- Open biopsy
PREFERRED RESPONSE: 4- Open biopsy
DISCUSSION
In this patient, tissue diagnosis should be obtained prior to any surgical intervention to avoid
unnecessary contamination in the event the lesion is a sarcoma. Open biopsy will yield the
diagnosis in the majority of cases. The specific choice for surgical treatment of a proximal

femur pathologic fracture is controversial, but it would typically involve either a
cephalomedullary nail or resection/reconstruction. A simple antegrade femoral nail rarely is
sufficient in this setting.
RECOMMENDED READINGS
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg
Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149. View Abstract at PubMed
Pap DP, Mayerson JL, Scharschmidt TJ. Soft tissue tumor recurrence after intramedullary stabilization of impending pathologic fractures. Orthopedics. 2012 Mar 7;35(3):e448-52. doi: 10.3928/01477447-20120222-43. PubMed PMID: 22385463.
View Abstract at PubMed
Figure 7
CLINICAL SITUATION FOR QUESTIONS 7 THROUGH 9
Figure 7 is the MRI scan of a 58-year-old woman who is being evaluated for knee
replacement. Examination reveals a large painless mobile lump on her anterior thigh. The
patient reports the lump has been there for at least 3 years, and she does not know if it is
growing or if it should be removed.
Question 7 of 143
What feature of the lesion most eliminates the need for biopsy prior to resection?
1- Painless nature
2- Location
3- Appearance on MRI scan
4- Rate of growth
PREFERRED RESPONSE: 3- Appearance on MRI scan
Question 8 of 143
Atypical lipomatous lesions often appear as benign lipomas. What study will distinguish an
atypical lipomatous lesion?
1- Cytogenetic testing showing evidence of a ring chromosome (MDM 2)
2- MRI scan showing an entire lesion made up of material isointense to fat on all sequences

3- Hematoxylin and eosin staining showing mature adipocytes
4- Immunohistochemistry staining for BCL-2
PREFERRED RESPONSE: 1- Cytogenetic testing showing evidence of a ring chromosome
(MDM 2)
Question 9 of 143
The pathology is consistent with atypical lipomatous tumor (ALT) well-differentiated
lipoma-like liposarcoma (WDLLS). What is the appropriate treatment and prognosis for this
condition?
1- Wide excision with a high chance of local recurrence and moderate chance of metastasis
2- Marginal excision with a moderate chance of local recurrence and low chance of
metastasis
3- Intralesional excision with a low chance of local recurrence and low chance of metastasis
4- Intralesional excision with a low chance of local recurrence and high chance of metastasis
PREFERRED RESPONSE: 2- Marginal excision with a moderate chance of local recurrence
and low chance of metastasis
DISCUSSION
ALTs are the extremity equivalent to a well-differentiated liposarcoma (WDLS) of the
retroperitoneum and other visceral locations. ALTs can pose a difficult diagnostic dilemma.
They often appear as lipomas, characterized as being made up entirely of fat, isointense to fat
on all MR scan sequences without heterogeneity. Atypical features may be increased
thickened internal septation, large and deep nature, and enhancement on post-gadolinium
studies. With no heterogeneous portions on MRI scan, biopsy is not needed because it is
unlikely to differentiate lipoma from ALT. The painless nature or superficial locations are not
reliable indicators of benign lesions. Concurrent surgery is never an appropriate reason for a
lesion to be removed unless previous imaging shows otherwise.
Benign lipomas and ALT may have some similarities. They both appear on MRI scan to be
made of fat with identical signal characteristics. Routine histology will show mature
adipocytes in both with minimal atypia in the ALTs. Cytogenetic testing, however, will show
a supernumerary ring and/or giant rod chromosomes in ALT, with amplification of the
MDM2 oncogene. BCL-2 is the B-cell lymphoma apoptosis regulator protein, seen in
lymphoma as well as some leukemias and carcinomas.
ALT or WDLLS are lesions with a moderate chance of local recurrence—certainly higher
than for ordinary lipoma, with reported rates of up to 50%. They pose low, if any, distant
metastatic potential. For this reason, marginal excision is recommended. When these lesions
are locally recurrent, they most likely are of the same histology; however, a small percentage
can return as a higher-grade malignancy (with an associated increase in metastatic potential).
The other concern regarding ALTs is the reported up to 10% incidence of dedifferentiation
within them, underscoring the recommendation for excision.

RECOMMENDED READINGS
Conyers R, Young S, Thomas DM. Liposarcoma: molecular genetics and therapeutics. Sarcoma. 2011;2011:483154. doi:
10.1155/2011/483154. Epub 2010 Dec 27. PubMed PMID: 21253554.
View Abstract at PubMed
Hopyans S, Wunder JS, Randall RL. Molecular biology in musculoskeletal neoplasia. In: Schwartz H, ed. Orthopaedic Knowledge Update:
Musculoskeletal Tumors 2. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:383-392.
Gaskin CM, Helms CA. Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): results of MRI evaluations of 126 consecutive fatty masses. AJR Am J Roentgenol. 2004 Mar;182(3):733-9. PubMed PMID: 14975977.
View Abstract at PubMed
Pilotti S, Della Torre G, Mezzelani A, Tamborini E, Azzarelli A, Sozzi G, Pierotti MA. The expression of MDM2/CDK4 gene product in
the differential diagnosis of well differentiated liposarcoma and large deep-seated lipoma. Br J Cancer. 2000 Apr;82(7):1271-5. PubMed
PMID: 10755400. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 12
1- Wide resection alone
2- Amputation
3- Chemotherapy and external beam radiation
4- External beam radiation and surgical resection
Match the preferred treatment option above with the patient description below.
Question 10 of 143
A 70-year-old woman has a 15-cm subfascial soft-tissue sarcoma in her left thigh with no
signs of metastatic disease on staging studies.
1- Wide resection alone
2- Amputation
3- Chemotherapy and external beam radiation
4- External beam radiation and surgical resection
PREFERRED RESPONSE: 4- External beam radiation and surgical resection
Question 11 of 143
A 57-year-old woman has a 3-cm low-grade subcutaneous sarcoma of the upper arm.
1- Wide resection alone
2- Amputation
3- Chemotherapy and external beam radiation
4- External beam radiation and surgical resection
PREFERRED RESPONSE: 1- Wide resection alone

Question 12 of 143
A 33-year-old man has an unplanned resection of a high-grade pleomorphic sarcoma of the
hand with multiple positive microscopic margins on final pathology.
1- Wide resection alone
2- Amputation
3- Chemotherapy and external beam radiation
4- External beam radiation and surgical resection
PREFERRED RESPONSE: 2- Amputation
DISCUSSION
The management of soft-tissue sarcoma can present unique challenges. A systematic
approach is necessary if undue complications and problems are to be avoided. In general,
low-grade lesions smaller than 5 cm that are suprafascial can be excised with appropriate
margins without adjuvant treatment. Lesions that are 5 cm or larger, are high-grade, and deep
to fascia are most often treated with a combination of radiation and surgery. In the event a
sarcoma is removed with inadequate margins (a scenario that is usually preceded by
insufficient imaging before surgery), then the premium is on secondarily obtaining
appropriate margins, most commonly with re-resection. However, in the case of a lesion in
the hand or foot, multiple compartment contamination may require amputation to achieve
adequate local control.
RECOMMENDED READINGS
Cheng EY. Surgical management of sarcomas. Hematol Oncol Clin North Am. 2005 Jun;19(3):451-70, v. Review. PubMed PMID:
15939191. View Abstract at PubMed
Hohenberger P, Wysocki WM. Neoadjuvant treatment of locally advanced soft tissue sarcoma of the limbs: which treatment to choose? Oncologist. 2008 Feb;13(2):175-86. doi: 10.1634/theoncologist.2007-0165. Review. PubMed PMID: 18305063.
View Abstract at PubMed
Hueman MT, Thornton K, Herman JM, Ahuja N. Management of extremity soft tissue sarcomas. Surg Clin North Am. 2008 Jun;88(3):539-
57, vi. doi: 10.1016/j.suc.2008.04.003. Review. PubMed PMID: 18514697.
View Abstract at PubMed
Kaushal A, Citrin D. The role of radiation therapy in the management of sarcomas. Surg Clin North Am. 2008 Jun;88(3):629-46, viii. doi:
10.1016/j.suc.2008.03.005. Review. PubMed PMID: 18514703. View Abstract at PubMed
Figure 13a
Figure 13b
CLINICAL SITUATION FOR QUESTIONS 13 THROUGH 14

Figures 13a and 13b are the MRI scans and biopsy specimen of a 64-year-old man who has
coccygeal pain.
Question 13 of 143
What is the most likely diagnosis?
1- Metastatic carcinoma
2- Giant-cell tumor
3- Chordoma
4- Chondrosarcoma
PREFERRED RESPONSE: 3- Chordoma
Question 14 of 143
Based on the images and histopathology, how is this patient best treated?
1- Chemotherapy and external beam radiotherapy
2- Resection
3- Resection and chemotherapy
4- External beam radiation alone
PREFERRED RESPONSE: 2- Resection
DISCUSSION
The imaging demonstrates a lobular T2 hyperintense sacral lesion, which on biopsy shows
physaliferous cells diagnostic of a sacrococcygeal chordoma. The histology differentiates this
from metastatic carcinoma, giant-cell tumor, or chondrosarcoma. Preferred treatment is en
bloc surgical resection. Although some centers employ adjuvant radiotherapy, this is of
unproven benefit at this time. Evolving data suggest benefits of particle beam therapy (proton
or carbon ion) from phase II studies, but this has not yet proven superior to en bloc surgery.
The lesion shown is surgically accessible.
RECOMMENDED READINGS
DeLaney TF, Liebsch NJ, Pedlow FX, Adams J, Dean S, Yeap BY, McManus P, Rosenberg AE, Nielsen GP, Harmon DC, Spiro IJ, Raskin
KA, Suit HD, Yoon SS, Hornicek FJ. Phase II study of high-dose photon/proton radiotherapy in the management of spine sarcomas. Int J Radiat Oncol Biol Phys. 2009 Jul 1;74(3):732-9. doi: 10.1016/j.ijrobp.2008.08.058. Epub 2008 Dec 25. PubMed PMID: 19095372.
View Abstract at PubMed
Fuchs B, Dickey ID, Yaszemski MJ, Inwards CY, Sim FH. Operative management of sacral chordoma. J Bone Joint Surg Am. 2005
Oct;87(10):2211-6. PubMed PMID: 16203885.
View Abstract at PubMed
Hulen CA, Temple HT, Fox WP, Sama AA, Green BA, Eismont FJ. Oncologic and functional outcome following sacrectomy for sacral
chordoma. J Bone Joint Surg Am. 2006 Jul;88(7):1532-9. PubMed PMID: 16818979. View Abstract at PubMed

Figure 15a
Figure 15b
Figure 15c
Figure 15d
Figure 15e
Figure 15f
Figure 15g
Question 15 of 143
A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an
injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images
are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial
menisectomy, the patient was turned to the prone position and an open posterior arthrotomy
and excision was performed. Low-power and high-power hematoxylin and eosin stained
histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history,
radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
1- Localized pigmented villonodular synovitis (PVNS)
2- Biphasic synovial sarcoma
3- Nodular fasciitis
4- Synovial hemangioma
PREFERRED RESPONSE: 4- Synovial hemangioma
DISCUSSION
The incidental finding in the posterior intercondylar notch of the knee in this patient
represents a benign synovial hemangioma. No intralesional calcifications are shown either on
the plain radiographs or CT scan. The MRI scans reveal a hypervascular lesion with multiple
filling defects, with hyperintensity on T2-weighted images and low to intermediate signal
intensity on T1-weighted images. Histologically, vascular lakes within fine capillaries with a
synovium on the surface of the lesion are characteristic of this condition. Many patients with
synovial hemangioma present with pain, swelling, stiffness, or mechanical symptoms. As
with PVNS, the disease can be localized or diffuse in nature. Surgical excision, either open or
arthroscopic, is the recommended treatment. PVNS is the most common intra-articular tumor,
but hypointensity in either the diffuse or localized type is characteristic on MRI scan in both
T1- and T2-weighted images. Synovial sarcoma, although often found close to a joint, is not
characteristically found within a joint. Nodular fasciitis is not found in intra-articular
locations.
RECOMMENDED READINGS
Adelani MA, Wupperman RM, Holt GE. Benign synovial disorders. J Am Acad Orthop Surg. 2008 May;16(5):268-75. Review. PubMed
PMID: 18460687.
View Abstract at PubMed

Weiss SW, Goldblum JR. Benign tumors and tumor-like lesions of blood vessels. In: Weiss SW, Goldblum JR, eds. Soft Tissue Tumors. 5th
ed. Philadelphia, PA: Mosby Elsevier; 2008:664-665.
Figure 16a
Figure 16b
Figure 16c
CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 19
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe
pain in his right distal thigh and knee with no significant trauma and an inability to bear
weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein
electrophoresis findings are negative, and electrolyte levels are within defined limits.
Question 16 of 143
Based on this patient’s history and imaging, the best next treatment step should include
1- immediate internal fixation of the fracture.
2- a skeletal survey.
3- a dual-energy radiograph absorptiometry (DEXA) scan.
4- a CT scan of the chest, abdomen, and pelvis with a whole-body bone scan.
PREFERRED RESPONSE: 4- a CT scan of the chest, abdomen, and pelvis with a whole-
body bone scan.
Question 17 of 143
No additional bony lesions were noted. What is the most appropriate next step?
1- Bone marrow biopsy
2- Immediate internal fixation of the fracture
3- Biopsy of the fracture site
4- Chemotherapy initiation
PREFERRED RESPONSE: 3- Biopsy of the fracture site

Question 18 of 143
The final results of the patient’s presurgical studies reveal a large solid mass in the right
kidney. He was brought to the operating room and a frozen section of his femur revealed the
findings seen in Figure 16c. What is the best treatment option in this setting?
1- External fixation
2- Retrograde intramedullary rod
3- Distal femoral resection with megaprosthesis
4- Locking plate fixation with allograft of the defect
PREFERRED RESPONSE: 3- Distal femoral resection with megaprosthesis
Question 19 of 143
Approximately what percentage of the time does an unknown primary cancer get identified as
part of a full metastatic work-up that includes radiographs; blood tests; a CT scan of the
chest, abdomen and pelvis; whole-body bone scan; and biopsy of the metastatic focus?
1- 45%
2- 65%
3- 85%
4- 100%
PREFERRED RESPONSE: 3- 85%
DISCUSSION
Metastatic bone cancer is common, affecting nearly 5.3% of the nearly 5 million people with
cancer in the United States each year. This is a typical presentation of a patient with a newly
diagnosed pathologic femur fracture. Without a known history of cancer, this presentation
should initiate a complete metastatic work-up including a radiograph of the pathologic site;
blood tests; whole-body bone scan; and a CT scan of the chest, abdomen, and pelvis.
Additional imaging at the site of concern such as an MRI scan or CT scan may be helpful in
certain cases. The next step is to obtain a biopsy of lesional tissue before proceeding to
immediate fixation. However, it is important to note that this lesion may be a primary cancer
for which case resection or amputation is necessary. A skeletal survey would be helpful in the
setting of multiple myeloma. A DEXA scan has no value in this clinical setting. A bone
marrow biopsy should be considered in the case of myeloma, but not metastatic carcinoma.
Chemotherapy cannot be initiated in any case without a tissue diagnosis. The knowledge that
the patient was found to have a large solid renal mass is highly suspicious for renal cell
carcinoma, which is among the 5 most common primary carcinomas to metastasize to the
bone (breast, lung, thyroid, kidney, and prostate).
Treatment of the femur should focus on a robust repair (whether biologic or not) to outlive
the patient. A distal femoral resection with megaprosthesis is the most durable option for
periarticular renal cell carcinoma metastasis, which is known to respond poorly to
radiotherapy. The pathology shown is classic for a clear cell carcinoma of the kidney. In

current practice, most primary cancers are identified as the result of a metastatic work-up.
Approximately 85% to 90% of primaries are determined from the history, physical, blood
tests, imaging, and biopsy results.
RECOMMENDED READINGS
Rougraff BT. Evaluation of the patient with carcinoma of unknown origin metastatic to bone. Clin Orthop Relat Res. 2003 Oct;(415
Suppl):S105-9. Review. PubMed PMID: 14600599. View Abstract at PubMed
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149.
View Abstract at PubMed
Bickels J, Dadia S, Lidar Z. Surgical management of metastatic bone disease. J Bone Joint Surg Am. 2009 Jun;91(6):1503-16. doi:
10.2106/JBJS.H.00175. Review. PubMed PMID: 19487532.
View Abstract at PubMed
Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint
Surg Am. 2009 Jun;91(6):1518-30. Review. PubMed PMID: 19487533. View Abstract at PubMed
Lin PP, Mirza AN, Lewis VO, Cannon CP, Tu SM, Tannir NM, Yasko AW. Patient survival after surgery for osseous metastases from renal cell carcinoma. J Bone Joint Surg Am. 2007 Aug;89(8):1794-801. PubMed PMID: 17671020.
View Abstract at PubMed
Schulman KL, Kohles J. Economic burden of metastatic bone disease in the U.S. Cancer. 2007 Jun 1;109(11):2334-42. PubMed PMID:
17450591.
View Abstract at PubMed
Figure 20a
Figure 20b
Figure 20c
Figure 20d
Figure 20e
CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 23
Figures 20a and 20b are the radiographs of an 83-year-old active, independent, and healthy
woman who has experienced 2 months of right lower thigh and knee pain. Her pain increased
progressively over the course of several weeks. While exiting a car she “bumped” her knee
against the door, felt a “crack,” and developed excruciating pain. She could no longer
ambulate and was brought to the hospital.
Question 20 of 143
Based on imaging alone, what does this bone lesion most closely resemble?

1- Multiple myeloma
2- Nonossifying fibroma
3- Metastatic renal cell carcinoma
4- Enchondroma
PREFERRED RESPONSE: 4- Enchondroma
Question 21 of 143
Figures 20c through 20e show the biopsy performed of the above-noted lesion. Based on the
clinical history, radiograph, and biopsy, what diagnosis is most likely?
1- Enchondroma
2- High-grade osteosarcoma
3- Metastatic renal cell carcinoma
4- Dedifferentiated chondrosarcoma
PREFERRED RESPONSE: 4- Dedifferentiated chondrosarcoma
Question 22 of 143
What treatment option carries the lowest risk for local recurrence?
1- Excision of tumor followed by open reduction with internal fixation
2- Megaprosthetic reconstruction of the femur and knee after tumor resection
3- Above-the-knee amputation with wide surgical margin
4- Revision total knee arthroplasty with long-cemented stem after tumor resection
PREFERRED RESPONSE: 3- Above-the-knee amputation with wide surgical margin
Question 23 of 143
What is the most likely site of metastatic disease in patients with this diagnosis?
1- Liver
2- Lungs
3- Brain
4- Kidneys
PREFERRED RESPONSE: 2- Lungs
DISCUSSION

This patient has a pathologic femur fracture. Her history suggests that her pain was
emanating from an impending fracture. The initial radiograph reveals a well-mineralized
lesion within the intramedullary canal with punctate calcifications. This by itself suggests an
enchondroma or low-grade chondroid lesion. It is important to note that enchondromas in the
long bones rarely cause pathologic fracture. That is not the case when they are present in the
hands and feet, where biologically they act more aggressively. Typically, a more aggressive
appearance such as cortical thinning or breach, soft-tissue mass, or periosteal elevation
suggests a chondrosarcoma. Unfortunately, a pathologic fracture makes the images somewhat
more difficult to interpret, which was the case with her MRI and CT scans. There is no
evidence from her radiographs that this is anything but a chondroid tumor. Multiple myeloma
often involves a radiolucent “punched out” lesion. Nonossifying fibromas are seen in children
and are well circumscribed, eccentric radiolucent lesions. Metastatic renal cell carcinoma
rarely demonstrates matrix on a radiograph. The histopathology clearly shows a cartilage-
based tumor. The chondroid tissue appears low grade. However, in an adjacent region there is
a high-grade component seen both on the low power view and the second higher-power
sample that does not resemble cartilage. This is highly suggestive of a dedifferentiated
chondrosarcoma. This signifies that a portion of the original tumor (low-grade
chondrosarcoma), which resembled the tissue of origin, converted into a different cell lineage
with more aggressive properties (nearly any type of high-grade sarcoma). These dangerous
tumors are highly malignant, with average 5-year survivals of about 50%. Local recurrence in
the setting of a pathologic fracture will be high secondary to spillage of tumor into the
fracture hematoma and disturbed compartments. In this case, an above-the-knee amputation
with a wide surgical margin would offer the lowest risk for local recurrence, but at the
expense of the most functional loss, especially in this age group. The most likely site of
metastatic disease from nearly any sarcoma is the lungs. Therefore, patients have their lungs
surveyed with at least a chest radiograph or, in most cases, a CT scan.
RECOMMENDED READINGS
Mavrogenis AF, Gambarotti M, Angelini A, Palmerini E, Staals EL, Ruggieri P, Papagelopoulos PJ. Chondrosarcomas revisited. Orthopedics. 2012 Mar 7;35(3):e379-90. doi: 10.3928/01477447-20120222-30. PubMed PMID: 22385450.
View Abstract at PubMed
Flemming DJ, Murphey MD. Enchondroma and chondrosarcoma. Semin Musculoskelet Radiol. 2000;4(1):59-71. Review. PubMed PMID:
11061692.
View Abstract at PubMed
Figure
24a
Figure
Figure
24c
Figure
24d
Figure
24e
Figure
24f
Figure
24g
Figure
24h
Figure
24i

24b
Question 24 of 143
A 14-year-old boy has had wrist pain for 3 weeks. Radiographs are shown in Figures 24a and
24b. His MRI scans are shown in Figures 24c through 24f. Representative histology is shown
in Figures 24g through 24i. The most likely diagnosis is
1- aneurysmal bone cyst.
2- fibrous dysplasia.
3- giant-cell tumor.
4- osteoblastoma.
PREFERRED RESPONSE: 4- osteoblastoma.
DISCUSSION
The combination of immature woven bone with osteoblastic rimming surrounded by a
vascular fibrous bland stroma seen in Figure 24i and scattered giant cells within the lesion
seen in Figure 24h should arouse the suspicion of osteoblastoma. Osteoblastoma most often is
diagnosed in adolescents and young adults, with 75% of patients younger than 25 years of
age at diagnosis. Within tubular bones, osteoblastoma most often arises in the metadiaphyseal
region, but it is more commonly seen in the spine within the posterior elements. The lesion is
well-defined on radiographs, with lucent to mixed lucent and blastic areas. The MRI scan
findings reveal low to intermediate signal intensity on T1- and intermediate to high signal
intensity on T2-weighted images. Neoplastic woven bone can be seen in Figure 24g, and
osteoclasts are shown in Figures 24h and 24i. Although the bone is expansile in appearance
on radiologic studies, there are no large vascular lakes on histology to support the diagnosis
of aneurysmal bone cyst. Although there are areas of woven bone as in fibrous dysplasia, the
appearance of osteoblastic rimming rules against this diagnosis. The location and histology of
the tumor in this case are inconsistent with giant-cell tumor of bone, the latter being a
metaepiphyseal tumor histologically comprising giant cells within a background of stromal
cells having nuclei identical to those of the giant cells.
RECOMMENDED READINGS
Mirra JB. Bone Tumors. Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA: Lea & Febiger; 1989:391-418.
Nielsen GP, Rosenberg AE. Diagnostic Pathology: Bone. Manitoba, Canada: Amirsys; 2013:1-27.
RESPONSES FOR QUESTIONS 25 THROUGH 29
1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone

7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
Match the condition above with the clinical scenario below.
Question 25 of 143
A 17-year-old girl has knee pain. The imaging shows a distal femur lesion with an adjacent
soft-tissue mass. The cortex is expanded and there is periosteal reaction. There appears to be
a cloud-like density within the lesion.
1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone
7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
PREFERRED RESPONSE: 1- Osteosarcoma
Question 26 of 143
A 44-year-old man has a sacral mass. There is a soft-tissue extension of the mass with bone
involvement centrally within the sacrum. The patient is told that the lesion is radiosensitive.
1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone
7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
PREFERRED RESPONSE: 8- Chordoma

Question 27 of 143
A 13-year-old boy with thigh pain has an enlarging soft-tissue mass. Radiographs show a
mid-diaphyseal lesion with a sunburst pattern of periosteal reaction. A needle biopsy shows
small round blue cells.
1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone
7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
PREFERRED RESPONSE: 2- Ewing sarcoma
Question 28 of 143
An 8-year-old girl has an enlarging mass in her right shoulder. It involves the deltoid and has
a heterogenous pattern on MRI scan. The mass is painless and was noticed when she was
getting bathed 3 months ago. A needle biopsy shows a small round blue-cell tumor.
1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone
7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
PREFERRED RESPONSE: 9- Rhabdomyosarcoma
Question 29 of 143
A 71-year-old man has a history of left hip pain radiating to his knee. The radiographs are
interpreted as osteoarthritis of the hip. He receives a hip injection, but does not experience
relief. A CT scan shows a periacetabular osteolytic lesion with punctuate areas of
calcification and a large soft-tissue mass.

1- Osteosarcoma
2- Ewing sarcoma
3- Aneurysmal bone cyst
4- Giant-cell tumor
5- Dedifferentiated chondrosarcoma
6- Metastatic disease of bone
7- Multiple myeloma
8- Chordoma
9- Rhabdomyosarcoma
10- Desmoid
11- Parosteal osteosarcoma
PREFERRED RESPONSE: 5- Dedifferentiated chondrosarcoma
DISCUSSION
Osteosarcoma is the most common malignant bone tumor and usually involves the
metaphysis of long bones in skeletally immature patients. It is a bone-forming tumor that
often has a cloud-like matrix, which indicates new bone formation. Ewing sarcoma is more
common in the diaphysis. Bone involvement is often accompanied by a soft-tissue mass. It
occurs in a similar age group as osteosarcoma. Ewing sarcoma is radiosensitive; however,
radiation is reserved primarily for nonsurgical anatomic locations. Histologically, it is in the
family of small round blue-cell tumors. Rhabdomyosarcoma is a high-grade soft-tissue
sarcoma most commonly seen in children. Like most soft-tissue sarcomas, it often presents as
an enlarging soft-tissue mass. It is treated with chemotherapy and surgical resection.
Radiation may also be used to reduce risk for local recurrence. Rhabdomyosarcoma is in the
family of small round blue-cell tumors. Chordoma occurs in 2 locations; the central portion
of the lower spine, usually the sacrum, and the base of the skull (the clivus). It is a
radiosensitive tumor; however, resection with a negative margin is the recommended
treatment. Dedifferentiated chondrosarcoma is a high-grade malignant tumor. Histologically,
areas consistent with both chondrosarcoma and osteosarcoma are often found. Other high-
grade tumors have also been described in combination with chondrosarcoma, such as
malignant fibrous histiocytoma of bone. In the pelvis, it can be difficult to see on radiographs,
and the symptoms can be confused with more common entities such as osteoarthritis or Paget
disease. The prognosis for these patients is poor, and chemotherapy use is controversial.
RECOMMENDED READINGS
Lewis VO, Morris CD, Parsons TW. Malignant and benign bone tumors that you are likely to see. Instr Course Lect. 2013;62:535-49. PubMed PMID: 23395056.
View Abstract at PubMed
Schwab JH, Springfield DS, Raskin KA, Mankin HJ, Hornicek FJ. What's new in primary bone tumors. J Bone Joint Surg Am. 2012 Oct
17;94(20):1913-9. doi: 10.2106/JBJS.L.00955. Review. PubMed PMID: 23079883.
View Abstract at PubMed
Peabody TD, Gibbs CP Jr, Simon MA. Evaluation and staging of musculoskeletal neoplasms. J Bone Joint Surg Am. 1998 Aug;80(8):1204-
18. Review. PubMed PMID: 9730132.
View Abstract at PubMed

Figure 30a
Figure 30b
Figure 30c
Question 30 of 143
Figure 30a is the radiograph taken in the emergency department of a 20-year-old man with
pain and swelling in his right-dominant arm. His MRI scan is seen in Figure 30b, and his
histopathology is shown in Figure 30c. What is the most likely diagnosis?
1- Ewing sarcoma
2- Langerhans cell histiocytosis
3- Osteosarcoma
4- Osteomyelitis
PREFERRED RESPONSE: 1- Ewing sarcoma
DISCUSSION
The imaging shows a permeative lytic diaphyseal lesion with malignant periosteal reaction
and a large soft-tissue mass. The histology shows a small round blue-cell tumor consistent
with Ewing sarcoma or lymphoma; genetic or immunohistochemical studies can be used for
the final differentiation. Langerhans cell histiocytosis or osteomyelitis would not present this
histology. Osteosarcoma would more likely be metaphyseal and would show osteoid
production on radiographs and histology.
RECOMMENDED READINGS
Peersman B, Vanhoenacker FM, Heyman S, Van Herendael B, Stam M, Brys P, Verstraete KL, Samson I, Sybers J, Van Dyck P, Parizel PM, De Schepper AM. Ewing's sarcoma: imaging features. JBR-BTR. 2007 Sep-Oct;90(5):368-76. PubMed PMID: 18085191.
View Abstract at PubMed
Bacci G, Balladelli A, Forni C, Longhi A, Serra M, Fabbri N, Alberghini M, Ferrari S, Benassi MS, Picci P. Ewing's sarcoma family
tumours. Differences in clinicopathological characteristics at presentation between localised and metastatic tumours. J Bone Joint Surg Br.
2007 Sep;89(9):1229-33. PubMed PMID: 17905963. View Abstract at PubMed

Arndt CA, Rose PS, Folpe AL, Laack NN. Common musculoskeletal tumors of childhood and adolescence. Mayo Clin Proc. 2012
May;87(5):475-87. doi: 10.1016/j.mayocp.2012.01.015. Review. PubMed PMID: 22560526. View Abstract at PubMed
Figure 31a
Figure 31b
Figure 31c
Figure 31d
Question 31 of 143
An 18-year-old woman has had a right thigh mass for “a long time.” She has found it
increasingly difficult to ambulate. Her medical history is unremarkable, with the exception of
hypertension. On clinical examination, a fullness is appreciated in the popliteal fossa. The
neurovascular status of the distal extremity is intact. Anteroposterior and lateral radiographs
are shown in Figures 31a and 31b. A lateral T2-weighted MRI scan is shown in Figure 31c.
The histology is seen in Figure 31d. What is the most likely diagnosis?
1- Aneurysmal bone cyst
2- Osteosarcoma
3- Periosteal lipoma
4- Parosteal osteosarcoma
PREFERRED RESPONSE: 2- Osteosarcoma
DISCUSSION
The radiographs indicate a bone-forming tumor that has intramedullary and extramedullary
components. The MRI scan confirms the extent of the tumor. Parosteal osteosarcomas are
generally surface tumors sparing the medullary canal, although extension into the canal can
occur. However, the histology is low-grade with a well-differentiated fibrous stroma, unlike
this case. The histology here shows pleomorphic cells, with the haphazard tumor bone
deposition consistent with a high-grade conventional osteosarcoma. Telangiectatic
osteosarcoma is associated with vast lakes of blood, which are usually seen on MRI scan as
fluid-fluid levels. In this patient, there was a single fluid-fluid level on MRI scan, but the
histology provided did not show lakes of blood. Aneurysmal bone cyst and periosteal lipoma
are both benign lesions and not consistent with the histology shown.
RECOMMENDED READINGS
Aboulafia AJ, Malawer MM. Surgical management of pelvic and extremity osteosarcoma. Cancer. 1993 May 15;71(10 Suppl):3358-66. Review. PubMed PMID: 8490883.
View Abstract at PubMed

Messerschmitt PJ, Garcia RM, Abdul-Karim FW, Greenfield EM, Getty PJ. Osteosarcoma. J Am Acad Orthop Surg. 2009 Aug;17(8):515-
27. Review. PubMed PMID: 19652033. View Abstract at PubMed
Figure 32a
Figure 32b
CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 36
A 68-year-old woman is referred for left thigh pain. Her medical history includes
hypertension, diabetes, and adenocarcinoma of the breast treated with surgery, chemotherapy,
and radiation 3 years ago. She currently is on aromatase therapy. She is unable to ambulate
secondary to pain, is limited to a walker, and requires narcotic medications. She has no other
pain but agrees to your recommendation that she urgently be sent to the hospital.
Question 32 of 143
After viewing the radiographs in Figures 32a and 32b, what is the most appropriate next step?
1- Surgical stabilization
2- Biopsy of the lesion
3- Further imaging
4- Immediate administration of bisphosphonates
PREFERRED RESPONSE: 3- Further imaging
Question 33 of 143
The patient is scheduled for surgery to stabilize the bone. According to the Mirels Scoring
System, what is most likely related to risk for pathologic fracture?
1- Pathology of the original tumor
2- Gender
3- Location of the lesion
4- Age of the patient
PREFERRED RESPONSE: 3- Location of the lesion

Question 34 of 143
The surgeon decides to obtain a biopsy before stabilization; new lesions are unrelated to
previous malignancies in what percentage of cases?
1- 5%
2- 15%
3- 25%
4- 35%
PREFERRED RESPONSE: 2- 15%
Question 35 of 143
Chance for fracture healing often is a factor in surgical decision making for reconstruction of
pathologic lesions. Among the diagnoses listed below, which grouping represents fracture
healing likelihood from least likely to most likely?
1- Breast carcinoma, lung carcinoma, multiple myeloma,
2- Multiple myeloma, breast carcinoma, lung carcinoma
3- Lung carcinoma, multiple myeloma, breast carcinoma
4- Lung carcinoma, breast carcinoma, multiple myeloma
PREFERRED RESPONSE: 4- Lung carcinoma, breast carcinoma, multiple myeloma
Question 36 of 143
Which intervention should be added to this patient’s care to best prevent future skeletally
related events (SRE)?
1- Inferior vena cava (IVC) filter placement
2- Bisphosphonates
3- External beam radiation
4- Tc-99 whole-body bone scan at regular intervals
PREFERRED RESPONSE: 2- Bisphosphonates
DISCUSSION
A new lesion in a patient with known carcinoma but without bone disease needs to be
evaluated before stabilization. As shown by Clayer and associates, as many as 15% of new
bone lesions with a history of known carcinoma will be from a different primary and should
be worked up before surgery. Evaluation with appropriate imaging will allow for
identification of other lesions that may be easier to biopsy or require fixation. Mirels
classified the chance that a metastatic lesion in the extremities will go on to pathologic
fracture based on 4 factors: size, site, type of bone reaction, and pain level. Prophylactic

fixation is recommended for scores of 8 or 9 and above, with a 15% to 30% chance of
fracture, respectively. The pathologic diagnosis is not involved with the chance for fracture
based on the Mirels classification.
Pathologic diagnoses, however, are associated with healing likelihood of lesions and the time
at which replacement should be considered over reduction and internal fixation. While not
technically metastatic disease, the systemic nature of multiple myeloma functions like a
widespread disease. Lung carcinoma has a very low healing likelihood, followed by breast
cancer, renal cancer, and myeloma, and should be factored when choosing methods of
surgical stabilization as shown by Gainor and associates.
Finally, because these patients are at significant risk for more lesions and skeletal-related
events, appropriate systemic treatment with bisphosphonates has been shown to help with
hypercalcemia and reduce SREs. IVC filter placement has been advocated to reduce risk for
fatal pulmonary embolism in patients with lower-extremity metastatic disease undergoing
operative intervention. Radiation is indicated for local control, and monitoring with bone
scans will help identify impending lesions sooner than relying on pain symptoms alone.
RECOMMENDED READINGS
Bickels J, Dadia S, Lidar Z. Surgical management of metastatic bone disease. J Bone Joint Surg Am. 2009 Jun;91(6):1503-16. doi:
10.2106/JBJS.H.00175. Review. PubMed PMID: 19487532.
View Abstract at PubMed
Clayer M, Duncan W. Importance of biopsy of new bone lesions in patients with previous carcinoma. Clin Orthop Relat Res. 2006 Oct;451:208-11. PubMed PMID: 16801861.
View Abstract at PubMed
Gainor BJ, Buchert P. Fracture healing in metastatic bone disease. Clin Orthop Relat Res. 1983 Sep;(178):297-302. PubMed PMID:
6883864.
View Abstract at PubMed
Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat
Res. 1989 Dec;(249):256-64. PubMed PMID: 2684463. View Abstract at PubMed
Quinn RH. Surgical management of lower extremity metastatic disease. In: Schwartz H, ed. Orthopaedic Knowledge Update: Musculoskeletal Tumors 2. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:383-392.
Figure 37a
Figure 37b
Figure 37c
Question 37 of 143

Figures 37a and 37b are the lateral and anteroposterior (AP) radiographs of a 60-year-old
man with a remote history of renal cell cancer. A needle biopsy of the lesion is shown in
Figure 37c. The bone destruction that occurs in this process is a result of
1- tumor cells.
2- cytokines secreted by the tumor.
3- host bone osteoblasts.
4- osteoprotegerin.
PREFERRED RESPONSE: 2- cytokines secreted by the tumor.
DISCUSSION
The lateral and AP radiographs of the elbow reveal a lucent lesion consistent with metastatic
disease, and, specifically, metastatic renal cancer. The histology is consistent with clear cell
carcinoma. Tumor cells do not destroy host bone. Rather, cytokines from the tumor stimulate
osteoclasts or osteoblasts to destroy or generate new bone, respectively. Osteoblasts secrete
receptor activator of nuclear factor kappa beta ligand (RANKL), and osteoclasts have
receptors for RANKL. This causes an increase in osteoclast precursors, resulting in increased
bone destruction. Osteoprotegerin is a decoy receptor that binds to RANKL and inhibits an
increase in osteoclasts.
RECOMMENDED READINGS
Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002 Aug;2(8):584-93. Review.
PubMed PMID: 12154351.
View Abstract at PubMed
Roodman GD. Mechanisms of bone metastasis. N Engl J Med. 2004 Apr 15;350(16):1655-64. Review. PubMed PMID: 15084698.
View Abstract at PubMed
Figure 38a
Figure 38b
Question 38 of 143
Figures 38a and 38b are the histopathology of an otherwise healthy 31-year-old man who had
a growing mass excised from his forearm with local anesthetic and no preoperative imaging.
The mass was documented to be subfascial and larger than 5 cm. What is the best local
treatment option?
1- Observation
2- Radiation only
3- Chemotherapy only
4- Re-excision and radiation
PREFERRED RESPONSE: 4- Re-excision and radiation

DISCUSSION
The misdiagnosis of a soft-tissue mass is fairly common. However, in this case the first
indication that the presumed diagnosis is incorrect is supported by significant growth over a
short time period. Generally, lipomas and many other benign soft-tissue masses grow slowly
over years rather than weeks or months. On MRI scan, a lipoma would classically
demonstrate homogenous high-signal intensity on a T1 sequence and fairly low-signal
intensity on a T2 sequence. No imaging was done before surgery, but a high-grade sarcoma
generally shows a heterogenous signal on T1 and T2 sequences that is distinctly different
than the pattern of a lipoma. The histopathology is consistent with a high-grade sarcoma A
spindle-cell tumor with hypercellularity, anaplasia, and pleomorphism. Mitotic figures are
also noted, suggesting rapid turnover and growth. This is a high-grade sarcoma that is treated
with wide surgical excision and observation is not recommended. External beam radiation is
often used as an adjuvant either before or after surgery to help decrease the local recurrence
rate. Radiation alone would not be sufficient treatment. The use of chemotherapy is
controversial. In the setting of a “whoops” or unintended resection of a high-grade soft-tissue
sarcoma, re-excision of the tumor bed with radiation is generally indicated. The radiation is
used to eliminate microscopic contamination. However, there is some evidence to support
surgery alone for superficial (subcutaneous) sarcomas.
RECOMMENDED READINGS
Mankin HJ, Mankin CJ, Simon MA. The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint
Surg Am. 1996 May;78(5):656-63. PubMed PMID: 8642021.
View Abstract at PubMed
Noria S, Davis A, Kandel R, Levesque J, O'Sullivan B, Wunder J, Bell R. Residual disease following unplanned excision of soft-tissue
sarcoma of an extremity. J Bone Joint Surg Am. 1996 May;78(5):650-5. PubMed PMID: 8642020. View Abstract at PubMed
Gibbs CP, Peabody TD, Mundt AJ, Montag AG, Simon MA. Oncological outcomes of operative treatment of subcutaneous soft-tissue sarcomas of the extremities. J Bone Joint Surg Am. 1997 Jun;79(6):888-97. PubMed PMID: 9199387.
View Abstract at PubMed
Figure 39a
Figure 39b
Figure 39c
Figure 39d
Figure 39e
Question 39 of 143
Figure 39a is the anteroposterior radiograph of a 51-year-old man who has had a painless
soft-tissue mass on his left wrist for 2 months. MR sequences are shown in Figures 39b
through 39d. A biopsy was performed and shown in a low-power hematoxylin and eosin
photomicrograph in Figure 39e. The most appropriate treatment for this lesion is

1- a diet that reduces uric acid production.
2- wide local resection followed by radiotherapy.
3- marginal excision.
4- observation until the mineralization matures, and then excision and radiotherapy to prevent
recurrence.
PREFERRED RESPONSE: 3- marginal excision.
DISCUSSION
The tumor seen here is a giant-cell tumor of the tendon sheath. A solid lesion larger than 1.5
cm in the wrist warrants biopsy to exclude malignancy. Synovial sarcoma should be
considered in mineralized periarticular masses; histology does not support this diagnosis. The
3 most common benign tumors of the wrist are ganglion cysts, giant-cell tumors of tendon
sheath, and hemangiomas. Radiographs are nonspecific but may reveal extrinsic erosions of
bone by giant-cell tumor of tendon sheath. MR findings of prominent low-signal intensity
(seen with T2-weighting) and “blooming” artifact from the hemosiderin (seen with gradient-
echo sequences) are nearly pathognomonic of this diagnosis as seen here. Pathology shows
hemosiderin-laden macrophages and giant cells as seen in the histology. Uric acid reduction
would be indicated for gout and wide local excision for a soft-tissue sarcoma. Observation
awaiting mature mineralization would apply to heterotopic ossification.
RECOMMENDED READINGS
Nguyen V, Choi J, Davis KW. Imaging of wrist masses. Curr Probl Diagn Radiol. 2004 Jul-Aug;33(4):147-60. Review. PubMed PMID: 15306759.
View Abstract at PubMed
Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: radiologic-pathologic
correlation. Radiographics. 2008 Sep-Oct;28(5):1493-518. doi: 10.1148/rg.285085134. PubMed PMID: 18794322.
View Abstract at PubMed
Figure 40a
Figure 40b
Figure 40c
CLINICAL SITUATION FOR QUESTIONS 40 THROUGH 43

Figures 40a through 40c are the radiograph, bone scan, and histology of a 68-year-old man
who has had 3 months of pain in his left thigh with weight bearing. He has no history of
cancer and no illnesses.
Question 40 of 143
The lesion seen in Figures 40a and 40b may best be described as
1- malignant.
2- benign latent.
3- benign aggressive.
4- inflammatory.
PREFERRED RESPONSE: 1- malignant.
Question 41 of 143
The origin of the lesion seen in Figures 40a and 40b may best be determined with
1- CT scan of the chest, abdomen and pelvis.
2- CT scan of the lesion.
3- MRI scan.
4- I-131 scan.
PREFERRED RESPONSE: 1- CT scan of the chest, abdomen and pelvis.
Question 42 of 143
The best next diagnostic step after imaging and staging is
1- prophylactic nail with reamings sent for permanent pathology.
2- biopsy.
3- C-reactive protein.
4- MRI scan.
PREFERRED RESPONSE: 2- biopsy.
Question 43 of 143
The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment
should consist of
1- surgical stabilization.
2- surgical stabilization and radiation.

3- excision and endoprosthesis.
4- radiation.
PREFERRED RESPONSE: 2- surgical stabilization and radiation.
DISCUSSION
The history and images show a lytic, malignant solitary bone lesion with a pathologic fracture
in an adult patient. In a patient older than age 50 with a lytic bone lesion, metastatic disease is
the most likely diagnosis. Prostate, thyroid, breast, lung, and kidney are the most common
cancer sources for a primary lesion. The most likely test that will identify the primary
malignancy is a CT scan of the chest, abdomen, and pelvis. Because no previous cancer
history exists, a biopsy of the bone lesion is necessary to make a diagnosis and to rule out a
primary bone sarcoma, for which the treatment would vastly differ. In a patient with no
cancer history, the biopsy is obtained to exclude a primary bone malignancy before surgical
intervention. The histology in this case shows nests of cohesive cells mimicking glandular
structures consistent with a carcinoma, so surgical stabilization may be undertaken.
Cementation and curettage alone will not address the mechanical instability, excision and
endoprosthesis would entail a larger surgery than is needed, and radiation alone will not
address the mechanical instability. In the setting of placing an intramedullary nail, the bone
will require radiation to eliminate residual disease within the femur.
RECOMMENDED READINGS
Weber KL. Evaluation of the adult patient (aged >40 years) with a destructive bone lesion. J Am Acad Orthop Surg. 2010 Mar;18(3):169-79. Review. PubMed PMID: 20190107.
View Abstract at PubMed
Cronin CG, Cashell T, Mhuircheartaigh JN, Swords R, Murray M, O'Sullivan GJ, O'Keeffe D. Bone biopsy of new suspicious bone lesions
in patients with primary carcinoma: prevalence and probability of an alternative diagnosis. AJR Am J Roentgenol. 2009 Nov;193(5):W407-
10. doi: 10.2214/AJR.08.1882. PubMed PMID: 19843719. View Abstract at PubMed
Weber KL, Peabody T, Frassica FJ, Mott MP, Parsons TW 3rd. Tumors for the general orthopedist: how to save your patients and practice. Instr Course Lect. 2010;59:579-91. PubMed PMID: 20415407.
View Abstract at PubMed
Figure 44a
Figure 44b
Question 44 of 143

Figures 44a and 44b are the anteroposterior hand and humerus radiographs of a 5-year-old
girl who has painful masses in her hand. Her parents noted concern about her left wrist and
upper arm, which have been sites of occasional pain. Examination reveals obvious deformity
of the left upper arm with shortening, mild bowing, and nonmobile masses within each
finger. No evidence of lesions is seen on her skin or in the soft tissues. What is the
approximate lifetime incidence of malignant degeneration from this condition?
1- 1% to 5%
2- 10% to 25%
3- 50% to 70%
4- 80% to 100%
PREFERRED RESPONSE: 2- 10% to 25%
DISCUSSION
This is a good example of a patient with Ollier disease, or multiple enchondromatosis. The
lack of skin or soft-tissue findings suggests there are no signs of angiomas/hemangiomas that
are required to make the diagnosis of Maffucci syndrome. Ollier disease is associated with
malignant degeneration of benign cartilaginous tumors into chondrosarcomas with variable
reported rates. The reported incidence ranges from 10% to 25%. It is suggested that patients
with Maffucci syndrome have cancer rates approaching 100%; however, in many of these
cases the malignancy is not from sarcomatous transformation of an enchondroma, but rather
other primary sources such as the gastrointestinal tract.
RECOMMENDED READINGS
Ghatan A, Scharschmidt T, Conrad E. Extreme enchondromatosis: a report of two cases and review of the literature. J Bone Joint Surg Am.
2010 Oct 6;92(13):2336-43. doi: 10.2106/JBJS.J.00194. Review. PubMed PMID: 20926729.
View Abstract at PubMed
Pansuriya TC, Kroon HM, Bovée JV. Enchondromatosis: insights on the different subtypes. Int J Clin Exp Pathol. 2010 Jun 26;3(6):557-69.
Review. PubMed PMID: 20661403. View Abstract at PubMed
Figure 45a
Figure 45b
Figure 45c
CLINICAL SITUATION FOR QUESTIONS 45 AND 46
Figures 45a through 45c show the sagittal proton density, T2-weighted, and axial gradient
echo MRI scans of a 34-year-old active woman with knee pain and swelling. Radiographs
show only an effusion.
Question 45 of 143

The most likely diagnosis is
1- synovial sarcoma.
2- synovial chondromatosis.
3- pigmented villonodular synovitis (PVNS).
4- posttraumatic hemarthrosis.
PREFERRED RESPONSE: 3- pigmented villonodular synovitis (PVNS).
Question 46 of 143
First-line treatment recommendations include
1- synovectomy.
2- arthrocentesis, compressive wrap, and rest.
3- en bloc resection.
4- intra-articular radioactive nucleotide injection.
PREFERRED RESPONSE: 1- synovectomy.
DISCUSSION
The MRI scans reveal classic findings of PVNS with low signal on proton density and T2
sequences and evidence of “blooming” on gradient echo sequences. A discrete mass
suggestive of a sarcoma (which would typically appear dark on T1 and bright on T2, but
heterogenous and enhancing) is not seen, and synovial sarcomas rarely arise in an intra-
articular location. Cartilaginous nodules of synovial chondromatosis are not seen, and the
abnormal synovial process indicates that this is more than just a posttraumatic hemarthrosis.
Treatment is synovectomy; radiotherapy is reserved for select recurrent cases. Arthrocentesis
would be used for a simple hemarthrosis, and resection used for a sarcoma.
RECOMMENDED READINGS
Tyler WK, Vidal AF, Williams RJ, Healey JH. Pigmented villonodular synovitis. J Am Acad Orthop Surg. 2006 Jun;14(6):376-85. Review. PubMed PMID: 16757677.
View Abstract at PubMed
Colman MW, Ye J, Weiss KR, Goodman MA, McGough RL 3rd. Does combined open and arthroscopic synovectomy for diffuse PVNS of
the knee improve recurrence rates? Clin Orthop Relat Res. 2013 Mar;471(3):883-90. doi: 10.1007/s11999-012-2589-8. PubMed PMID:
22996360. View Abstract at PubMed
Ogilvie-Harris DJ, McLean J, Zarnett ME. Pigmented villonodular synovitis of the knee. The results of total arthroscopic synovectomy, partial, arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am. 1992 Jan;74(1):119-23. PubMed PMID: 1463472.
View Abstract at PubMed
RESPONSES FOR QUESTIONS 47 THROUGH 52
1- Ultrasound
2- MRI scan of the thigh

3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most
appropriate next evaluation or treatment step listed above.
Question 47 of 143
A 34-year-old man with a large and rapidly enlarging deep mass in his thigh.
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
PREFERRED RESPONSE: 2- MRI scan of the thigh
Question 48 of 143
A 56-year-old woman with a heterogenous retroperitoneal soft-tissue mass larger than 5 cm
(as imaged on MRI scan) that first was noticed after a slip and fall. Staging study findings are
negative.
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy

PREFERRED RESPONSE: 11- Core needle biopsy
Question 49 of 143
A 65-year-old man with an American Joint Committee on Cancer (AJCC) III anterior thigh
sarcoma is considering treatment options. What treatment regimen is associated with a higher
rate of wound healing complications after surgery?
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
PREFERRED RESPONSE: 5- Presurgical radiation therapy
Question 50 of 143
A 44-year-old woman elects surgical treatment of an intramuscular lipoma. What is the
preferred surgical treatment?
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
PREFERRED RESPONSE: 6- Marginal resection
Question 51 of 143

A 29-year-old man with a large and enlarging upper arm deep mass has an inconclusive
needle biopsy.
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
PREFERRED RESPONSE: 9- Incision centered over the mass in line with long axis of limb
Question 52 of 143
A 60-year-old woman with a clear cell sarcoma of the foot has no evidence of disease
elsewhere after standard staging of a soft-tissue sarcoma. What additional evaluation is
recommended?
1- Ultrasound
2- MRI scan of the thigh
3- Chest CT scan and whole-body bone scan
4- Positron emission tomography (PET) scan
5- Presurgical radiation therapy
6- Marginal resection
7- Radical resection and postsurgical radiation
8- Transverse incision centered over the mass
9- Incision centered over the mass in line with long axis of limb
10- Sentinel node biopsy
11- Core needle biopsy
PREFERRED RESPONSE: 10- Sentinel node biopsy
DISCUSSION
In patients with rapidly enlarging painless masses, particularly those that are either large or
deep, the diagnosis of a soft-tissue sarcoma should be entertained. Characteristics that are
concerning are masses larger than 5 cm in largest dimension that are subfascial and
heterogenous on MRI scan. MRI scan is the preferred imaging modality for evaluation of
soft-tissue sarcomas because it can delineate location of the lesion, involvement of
neurovascular structures, intra-articular involvement, and underlying signal alteration in the
osseous structures. Most patients relate the onset of their symptoms to a traumatic event, and
the interpretation of the MRI scan can include a hematoma. Ultrasound is more commonly
used to confirm the clinical impression of a cyst and to distinguish cystic from solid masses.

A core needle biopsy can easily be performed in an outpatient setting or with image guidance
to aid in the diagnosis. Core needle biopsies preserve the architectural relationship of cells,
which is important in the diagnosis of mesenchymal lesions. A fine-needle aspiration allows
cytologic but not histologic analysis, and generally is not favored for the diagnosis of a
sarcoma. If an open biopsy is performed, the incision must be oriented in line with the long
axis of the extremity to minimize contamination of surrounding structures. Meticulous
hemostasis and closure of the tumor pseudocapsule must be achieved to minimize local tissue
contamination. An open biopsy is commonly used if an initial needle biopsy is nondiagnostic.
Transverse biopsy incisions should not be used.
Presurgical radiation for sarcomas is advantageous to decrease the field of radiation and
overall radiation dose, but a significant postsurgical wound-healing complication rate (up to
35%) is associated with presurgical radiation therapy.
Staging of sarcomas is important to predict prognosis. Not all sarcomas are reliably positive
on a PET scan, so the preferred staging studies are CT scan of the chest and whole-body bone
scan. Hematogenous spread of sarcomas is the most common route of metastatic disease,
which speaks to the value of chest CT scans. Clear cell sarcomas (in addition to synovial
sarcoma, angiosarcoma, epitheliod sarcoma, and rhabdomyosarcoma) have a propensity for
lymphatic nodal metastatic disease, so sentinel node biopsy is considered in assessing these
tumors. Recent evidence supports efficacy of sentinel node biopsy for clear cell sarcomas in
particular.
RECOMMENDED READINGS
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer;
2010.
Arbeit JM, Hilaris BS, Brennan MF. Wound complications in the multimodality treatment of extremity and superficial truncal sarcomas. J Clin Oncol. 1987 Mar;5(3):480-8. PubMed PMID: 3819810.
View Abstract at PubMed
Luce EA. The irradiated wound. Surg Clin North Am. 1984 Aug;64(4):821-9. PubMed PMID: 6591499.
View Abstract at PubMed
Cheng EY, Dusenbery KE, Winters MR, Thompson RC. Soft tissue sarcomas: preoperative versus postoperative radiotherapy. J Surg Oncol.
1996 Feb;61(2):90-9. PubMed PMID: 8606553.
View Abstract at PubMed
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg
Am. 1982 Oct;64(8):1121-7. PubMed PMID: 7130225. View Abstract at PubMed
Singer S, Nielsen T, Antonescu CR. Molecular biology of soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1522-1532.
Singer S, Maki RG, O'Sullivan B. Soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice
of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1533-1577.
Malawer MM, Helman LJ, O'Sullivan B. Sarcomas of bone. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and
Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1578-1609.
O'Sullivan B, Davis AM, Turcotte R, Bell R, Catton C, Chabot P, Wunder J, Kandel R, Goddard K, Sadura A, Pater J, Zee B. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002 Jun 29;359(9325):2235-41. PubMed

PMID: 12103287.
View Abstract at PubMed
Andreou D, Boldt H, Werner M, Hamann C, Pink D, Tunn PU. Sentinel node biopsy in soft tissue sarcoma subtypes with a high propensity
for regional lymphatic spread--results of a large prospective trial. Ann Oncol. 2013 May;24(5):1400-5. doi: 10.1093/annonc/mds650. Epub 2013 Jan 31. PubMed PMID: 23372051.
View Abstract at PubMed
Figure 53
Question 53 of 143
Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is
unwilling to use his right arm after a fall on the playground. What is the most appropriate
initial treatment?
1- Nonsurgical treatment of the fracture
2- Aspiration and injection with methylprednisolone
3- Curettage and augmentation with bone cement and internal fixation
4- Further imaging and biopsy
PREFERRED RESPONSE: 1- Nonsurgical treatment of the fracture
DISCUSSION
When a unicameral cyst is present in the setting of a pathological fracture, it is best to allow
the fracture to heal before administering interventions for the cyst. In some cases, waiting
may obviate the need for a procedure to manage the cyst. When indicated, the initial
procedure of choice is aspiration and injection of the cyst. Although many variations of the
procedure exist, current evidence continues to support the role of methylprednisolone in the
injection portion of the procedure. Curettage and packing may sometimes be appropriate for
recalcitrant cysts, but is not indicated for this patient. These cysts are typically solitary and
are not considered at risk for malignant degeneration or systemic involvement; therefore,
further distant imaging and biopsy is unnecessary.
RECOMMENDED READINGS
Baig R, Eady JL. Unicameral (simple) bone cysts. South Med J. 2006 Sep;99(9):966-76. Review. PubMed PMID: 17004531.
View Abstract at PubMed
Donaldson S, Wright JG. Recent developments in treatment for simple bone cysts. Curr Opin Pediatr. 2011 Feb;23(1):73-7. doi:
10.1097/MOP.0b013e3283421111. Review. PubMed PMID: 21191299. View Abstract at PubMed
Lokiec F, Wientroub S. Simple bone cyst: etiology, classification, pathology, and treatment modalities. J Pediatr Orthop B. 1998 Oct;7(4):262-73. Review. PubMed PMID: 9810525.
View Abstract at PubMed

Figure 54
Question 54 of 143
Figure 54 is the CT scan of a 70-year-old man with progressive neck pain; there is no history
of trauma, and examination is notable only for mildly decreased cervical range of motion. He
is neurologically intact. He has monoclonal gammopathy of undetermined significance that
has been stable for many years. Current serum protein electrophoresis is unchanged. History
and examination reveal no other causes for his pain. What is the next step in clinical
management?
1- Corpectomy and anterior fusion
2- Radiation therapy followed by multiple myeloma protocol chemotherapy
3- CT-guided biopsy
4- CT scan of the chest, abdomen, and pelvis
PREFERRED RESPONSE: 4- CT scan of the chest, abdomen, and pelvis
DISCUSSION
The patient has a lytic lesion of unclear etiology. Rougraff and associates demonstrated the
efficacy of a protocol including history and examination, basic laboratory studies, imaging,
and biopsy of the most accessible lesion in identifying the primary site of disease in patients
with skeletal metastases of unknown primary. A CT scan of the chest, abdomen, and pelvis
and bone scan complete the next step of Rougraff’s protocol. Although the history suggests
possible myeloma, the laboratory studies do not support transformation of monoclonal
gammopathy to multiple myeloma. For this patient, CT scan showed a primary lung cancer,
and a biopsy of a rib metastasis (much safer to biopsy than the cervical spine) confirmed
metastatic adenocarcinoma.
Reflexive biopsy of a difficult and risky lesion is incorrect; staging the patient is likely to
identify a safer site to access for biopsy and may identify conditions such as metastatic renal
cell carcinoma that would benefit from embolization before surgery. Corpectomy and anterior
fusion is incorrect because immediate surgery is not needed here (intraosseous lesion causing
pain with a normal neurologic examination and mildly decreased range of motion). Radiation
and chemotherapy should not be administered before a diagnosis is ascertained.
RECOMMENDED READINGS
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg
Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149.
View Abstract at PubMed
Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone
View Abstract at PubMed

Figure 55a
Figure 55b
Figure 55c
Figure 55d
Figure 55e
Question 55 of 143
A 27-year-old incarcerated man was found to have a fungating mass on his anterolateral right
proximal thigh. A clinical photograph is shown in Figure 55a. T1- and T2-weighted coronal
MRI scans are shown in Figures 55b and 55c. The hematoxylin and eosin and CD34 stained
histology are shown in Figures 55d and 55e. What is the most likely diagnosis?
1- Squamous cell carcinoma
2- Melanoma
3- Dermatofibrosarcoma protuberans (DFSP)
4- Desmoid tumor
PREFERRED RESPONSE: 3- Dermatofibrosarcoma protuberans (DFSP)
DISCUSSION
The clinical photograph is characteristic for a large DFSP with lobules of tumor that often
fungate over a long period of time. The tumor has an infiltrative growth pattern and has a
high local recurrence rate if not widely resected. The tumor is characterized by the t(17;22)
translocation with the gene PDGFB to the collagen 1 alpha gene. The gene fusion product is
instrumental in the pathogenesis of the tumor. Histologically, the tumor is composed of
uniform fibroblasts arranged in a storiform pattern. CD34, the human progenitor cell antigen,
is positive. Although squamous cell carcinoma and melanoma can often fungate, the
protruding nodules of tumor clinically are not characteristic of those neoplasms. Aggressive
fibromatosis is much less cellular than DFSP and has less defined margins on MRI scan.
RECOMMENDED READINGS
Cai H, Wang Y, Wu J, Shi Y. Dermatofibrosarcoma protuberans: clinical diagnoses and treatment results of 260 cases in China. J Surg
Oncol. 2012 Feb;105(2):142-8. doi: 10.1002/jso.22000. Epub 2011 Aug 3. PubMed PMID: 21815146.
View Abstract at PubMed
McArthur G. Dermatofibrosarcoma protuberans: recent clinical progress. Ann Surg Oncol. 2007 Oct;14(10):2876-86. Epub 2007 Jul 24.
Review. PubMed PMID: 17647063. View Abstract at PubMed
Weiss SW, Goldblum JR. Fibrohistiocytic tumors of intermediate malignancy. In: Weiss SW, Goldblum JR, eds. Soft Tissue Tumors. 5th ed. Philadelphia, PA: Mosby Elsevier; 2008:371-382.

Figure 56a
Figure 56b
Figure 56c
Question 56 of 143
Figures 56a and 56b are the axial short tau inversion recovery and T1 with contrast images of
a 7-month-old infant who is found to have a right scapular soft-tissue mass. On examination,
the mass is hard. A biopsy was performed and is shown in Figure 56c (hematoxylin and
eosin, 400x). What is the optimal treatment for this patient?
1- Intralesional excision
2- Marginal excision
3- Wide excision
4- Observation
PREFERRED RESPONSE: 3- Wide excision
DISCUSSION
The lesion seen here is infantile fibromatosis, and advanced imaging (ultrasonography, CT
scan, and MRI scan) reveals lesion extent. Involvement of adjacent structures is common,
reflecting the infiltrative growth pattern often seen in these lesions. MRI scan may show
characteristic features of prominent low- to intermediate-signal intensity and bands of low-
signal intensity representing highly collagenized tissue. However, fibromatoses with less
collagen and more cellularity may have nonspecific high-signal intensity on T2-weighted
images. Local recurrence is frequent after surgical resection because of the aggressive lesion
growth. This tumor is treated with wide excision, and chemotherapy is frequently employed
as an adjunct.
RECOMMENDED READINGS
Robbin MR, Murphey MD, Temple HT, Kransdorf MJ, Choi JJ. Imaging of musculoskeletal fibromatosis. Radiographics. 2001 May-
Jun;21(3):585-600. Review. PubMed PMID: 11353108. View Abstract at PubMed
Santoro A, Pannone G, Errico ME, Bifano D, Lastilla G, Bufo P, Loreto C, Donofrio V. Role of ß-catenin expression in paediatric mesenchymal lesions: a tissue microarray-based immunohistochemical study. Eur J Histochem. 2012 Jul 2;56(3):e25. doi:
10.4081/ejh.2012.e25. PubMed PMID: 23027341.
View Abstract at PubMed

Figure 57a
Figure 57b
Figure 57c
Figure 57d
Figure 57e
Question 57 of 143
Figures 57a through 57d show the radiographs and T1- and T2-weighted MRI scan sequences
of the proximal femur of a 60-year-old man with progressive thigh pain. A review of
radiographs taken 3 years ago reveals that the lesion is new. The biopsy specimen is shown in
Figure 57e; staging studies show no other lesions, and local imaging confirms the process is
confined to bone (no soft-tissue mass). The next treatment step should include
1- hip disarticulation.
2- radiotherapy.
3- ifosfamide-based chemotherapy.
4- wide resection and reconstruction.
PREFERRED RESPONSE: 4- wide resection and reconstruction.
DISCUSSION
The radiographs and MRI scans show a cartilaginous lesion of the proximal femur with
cortical thickening and cortical invasion seen on axial MRI scan. The fact that the lesion is
new proves it is not an enchondroma (which would not be expected to arise de novo in an
adult and would not have such significant cortical changes). Biopsy reveals an intermediate-
grade chondrosarcoma with nuclear atypia in addition to permeation of trabecular bone. The
treatment of choice is surgical resection and reconstruction. Hip disarticulation is not
indicated because the lesion is confined to the bone without involvement of vessels or nerves.
Radiotherapy would be indicated for hematopoietic or radiosensitive malignancies, but
chondrosarcoma does not respond to radiation or chemotherapy. Curettage and bone cement
have been advocated as treatment for low-grade chondrosarcomas. However, the clear
nuclear atypia on the biopsy and the demonstration of intracortical involvement on the axial
MRI scan make this a less optimal treatment choice for this patient.
RECOMMENDED READINGS
Lee FY, Mankin HJ, Fondren G, Gebhardt MC, Springfield DS, Rosenberg AE, Jennings LC. Chondrosarcoma of bone: an assessment of
outcome. J Bone Joint Surg Am. 1999 Mar;81(3):326-38. PubMed PMID: 10199270.
View Abstract at PubMed
Leerapun T, Hugate RR, Inwards CY, Scully SP, Sim FH. Surgical management of conventional grade I chondrosarcoma of long bones.
Clin Orthop Relat Res. 2007 Oct;463:166-72. PubMed PMID: 17632422. View Abstract at PubMed

Donati D, Colangeli S, Colangeli M, Di Bella C, Bertoni F. Surgical treatment of grade I central chondrosarcoma. Clin Orthop Relat Res.
2010 Feb;468(2):581-9. doi: 10.1007/s11999-009-1056-7. Epub 2009 Aug 29. PubMed PMID: 19727994. View Abstract at PubMed
Question 58 of 143
The characteristic translocation and genes involved in extraskeletal myxoid chondrosarcoma
is
1- t(11;12) EWS;FLI1.
2- t(12;16) TLS;CHOP.
3- t(9;22) EWS;CHN.
4- t(9;22) BCR-ABL.
PREFERRED RESPONSE: 3- t(9;22) EWS;CHN.
DISCUSSION
Extraskeletal myxoid chondrosarcoma is characterized by an in-frame fusion of the genes
EWS and TEC (also called CHN) involving chromosomes 9 and 22, respectively. Chronic
myelogenous leukemia is also characterized by a translocation involving chromosomes 9 and
22; however, the fused genes are different. t(11;12) EWS/FLI1 is characteristic of Ewing
sarcoma/t(12;16) TLS; CHOP is characteristic of myxoid liposarcoma.
RECOMMENDED READINGS
Hinrichs SH, Jaramillo MA, Gumerlock PH, Gardner MB, Lewis JP, Freeman AE. Myxoid chondrosarcoma with a translocation involving
chromosomes 9 and 22. Cancer Genet Cytogenet. 1985 Jan 15;14(3-4):219-26. PubMed PMID: 3967207. View Abstract at PubMed
Labelle Y, Bussières J, Courjal F, Goldring MB. The EWS/TEC fusion protein encoded by the t(9;22) chromosomal translocation in human chondrosarcomas is a highly potent transcriptional activator. Oncogene. 1999 May 27;18(21):3303-8. PubMed PMID: 10359536.
View Abstract at PubMed
Figure 59a
Figure 59b
Figure 59c
Question 59 of 143
Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman
who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg.
The histopathology is shown in Figure 59c. A radiograph of her leg showed no
mineralizations or osseous erosions. The chromosomal abnormality that is associated with
this disease is

1- t(11;22).
2- t(2;13).
3- t(X;18).
4- t(12;16).
PREFERRED RESPONSE: 3- t(X;18).
DISCUSSION
The imaging shows a soft-tissue mass with histology showing a synovial sarcoma. This
histology is associated with t(X;18). Ewing sarcoma is associated with t(11;22); alveolar
rhabdomyosarcoma t(2;13); and myxoid liposarcoma t(12;16). Although the presented
monophasic histology could be consistent with other sarcomas, it does not have the
characteristics of Ewing sarcoma (small round blue cells), alveolar rhabdomysarcoma
(alveolar pattern), or myxoid liposarcoma (myxoid stroma and signet ring lipoblasts with a
plexiform capillary network).
RECOMMENDED READINGS
Jones BC, Sundaram M, Kransdorf MJ. Synovial sarcoma: MR imaging findings in 34 patients. AJR Am J Roentgenol. 1993
Oct;161(4):827-30. PubMed PMID: 8396848. View Abstract at PubMed
Sandberg AA. Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet. 2002 Oct 30;115(3):189-93. Review.
PubMed PMID: 12407700.
View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The
patient first noticed it about 6 months after she had a low-impact fall. The general surgeon
evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient
underwent a surgical procedure to remove the mass.
Question 60 of 143
After evaluating the mass with a history and examination, what is the most appropriate next
treatment step?
1- Observation
2- Imaging studies (MRI scan or CT scan)
3- Surgical excision
4- Open biopsy
PREFERRED RESPONSE: 2- Imaging studies (MRI scan or CT scan)
Question 61 of 143

A surgical excision performed on this patient should be done with which principle in mind to
minimize contamination of soft tissues?
1- Meticulous hemostasis and closure
2- Traversing multiple muscle compartments
3- Transverse incision
4- Exposing neurovascular structures
PREFERRED RESPONSE: 1- Meticulous hemostasis and closure
Question 62 of 143
Which description best characterizes an unplanned excision of a soft-tissue sarcoma?
1- The length of the incision is excessive.
2- The incision is oriented transversely on the extremity.
3- No imaging was obtained before surgery.
4- No radiation was given before surgery.
PREFERRED RESPONSE: 3- No imaging was obtained before surgery.
Question 63 of 143
What is the most common detrimental impact of an unplanned excision of a high-grade soft-
tissue sarcoma?
1- Decreased mortality
2- Decreased recurrence
3- Increased wound complications
4- Increased functional outcome
PREFERRED RESPONSE: 3- Increased wound complications
DISCUSSION
This is an example of an unplanned excision. The patient has a history of trauma and a
painless soft-tissue mass. The most common soft-tissue masses are benign; consequently,
nononcologic surgeons may not expect a malignant sarcoma. The patient was taken to
surgery with appropriate imaging and without a biopsy. If the imaging is conclusive a biopsy
is not always indicated, particularly for low-grade lipomatous tumors. The surgical resection
was performed through a transverse incision. It is recommended that the incision be made
longitudinally in the event a wider resection is needed. The grade of the tumor is the most
important aspect. Benign and low-grade tumors may be observed, whereas intermediate and
high-grade tumors require a wide resection and likely perioperative radiation. The appropriate
work-up for a soft-tissue mass is a careful history and examination accompanied by
radiographs and cross-sectional imaging. If a biopsy is needed, it should be performed or

supervised by the surgeon, who would do the final resection if it proves to be a sarcoma. The
most common impact of an unplanned excision is wound complications. This is because of
the need for a wider surgical resection and adjuvant radiation. Mortality and recurrence have
not been shown to be increased with statistical significance. Functional outcome may be
compromised; however, no studies confirm that functional outcome is poorer in patients who
undergo unplanned excision.
RECOMMENDED READINGS
Qureshi YA, Huddy JR, Miller JD, Strauss DC, Thomas JM, Hayes AJ. Unplanned excision of soft tissue sarcoma results in increased rates
of local recurrence despite full further oncological treatment. Ann Surg Oncol. 2012 Mar;19(3):871-7. doi: 10.1245/s10434-011-1876-z. Epub 2011 Jul 27. PubMed PMID: 21792512.
View Abstract at PubMed
Arai E, Nishida Y, Tsukushi S, Wasa J, Ishiguro N. Clinical and treatment outcomes of planned and unplanned excisions of soft tissue
sarcomas. Clin Orthop Relat Res. 2010 Nov;468(11):3028-34. doi: 10.1007/s11999-010-1392-7. PubMed PMID: 20496020.
View Abstract at PubMed
Siegel HJ, Brown O, Lopez-Ben R, Siegal GP. Unplanned surgical excision of extremity soft tissue sarcomas: patient profile and referral
patterns. J Surg Orthop Adv. 2009 Summer;18(2):93-8. PubMed PMID: 19602337. View Abstract at PubMed
Figure 64a
Figure 64b
Figure 64c
CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 66
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man
with medial knee pain and swelling below the knee.
Question 64 of 143
What is the origin of the lesion seen on imaging?
1- A meniscal tear
2- A parameniscal cyst

3- Elastin deficiency
4- Translocation x;18
PREFERRED RESPONSE: 4- Translocation x;18
Question 65 of 143
Arthroscopy is performed, the palpable lesion is aspirated, and no fluid is obtained. What is
the best next treatment step?
1- Marginal resection of the cyst through a transverse incision
2- Marginal resection of the cyst through a longitudinal incision
3- Arthroscopic evaluation of the cyst
4- Biopsy
PREFERRED RESPONSE: 4- Biopsy
Question 66 of 143
Histology of the lesion is shown in Figure 64c. The best next treatment step is
1- radiation.
2- radiation and surgery.
3- chemotherapy.
4- observation.
PREFERRED RESPONSE: 2- radiation and surgery.
DISCUSSION
Parameniscal cysts and soft-tissue sarcomas can easily be confused, especially when there is
an intra-articular abnormality. This patient has a synovial sarcoma, which has an x;18
translocation abnormality. The lack of communication with the joint; no meniscal tear on
MRI scan; a lesion that has signal characteristics that are not the same as muscle, fat, or fluid;
and aspiration that yields no fluid are all characteristics of a soft-tissue sarcoma. A
parameniscal cyst has a signal characteristic that is identical to the joint fluid on MRI scan
and has a visible connection to the joint. When a lesion is encountered that may have
malignant potential, a biopsy is imperative. Principles of an extremity biopsy—longitudinal
incision, strict hemostasis, minimizing tissue plane dissection, and ensuring appropriate
tissue—must be observed. Marginal resection of a soft-tissue sarcoma, especially through a
transverse incision, would not be appropriate care. A soft-tissue sarcoma is treated with
radiation and surgery. Chemotherapy is controversial in this setting with no long-term
benefit.
RECOMMENDED READINGS

Muscolo DL, Ayerza MA, Makino A, Costa-Paz M, Aponte-Tinao LA. Tumors about the knee misdiagnosed as athletic injuries. J Bone
Joint Surg Am. 2003 Jul;85-A(7):1209-14. PubMed PMID: 12851344. View Abstract at PubMed
Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr Course Lect. 2009;58:833-47. PubMed PMID: 19385590.
View Abstract at PubMed
Gilbert NF, Cannon CP, Lin PP, Lewis VO. Soft-tissue sarcoma. J Am Acad Orthop Surg. 2009 Jan;17(1):40-7. Review. PubMed PMID:
19136426.
View Abstract at PubMed
Figure 67a
Figure 67b
Figure 67c
Question 67 of 143
A 26-year-old woman has had a slow-growing and painful mass at the base of her ring finger
for several months. Radiographs of the affected digit show no mineralization or erosions of
the underlying bone. An axial T1 MRI scan is shown in Figure 67a, and a corresponding
short tau inversion recovery image is shown in Figure 67b. A coronal T1 MRI scan with
contrast is shown in Figure 67c. The best next treatment step is
1- referral to a sarcoma center.
2- observation.
3- excisional biopsy.
4- marginal excision.
PREFERRED RESPONSE: 1- referral to a sarcoma center.
DISCUSSION
The lesion seen in the images is larger than 1.5 cm and growing. Therefore, a malignant
growth must be considered. Although malignant tumors of the hand are rare and clear-cell
sarcoma is rarer still, the most common clinical symptom is a small painless mass. Curative
excision or amputation is the treatment of choice. Observation of a malignant lesion is not
acceptable treatment, and neither an excisional biopsy nor marginal excision can achieve the
wide excision necessary for this patient.
RECOMMENDED READINGS
Brien EW, Terek RM, Geer RJ, Caldwell G, Brennan MF, Healey JH. Treatment of soft-tissue sarcomas of the hand. J Bone Joint Surg Am. 1995 Apr;77(4):564-71. PubMed PMID: 7713973.
View Abstract at PubMed

Plate AM, Steiner G, Posner MA. Malignant tumors of the hand and wrist. J Am Acad Orthop Surg. 2006 Nov;14(12):680-92. PubMed
PMID: 17077340. View Abstract at PubMed
Question 68 of 143
What is the most specific immunohistochemistry staining pattern that confirms the diagnosis
of desmoid tumor?
1- Membranous beta-catenin staining
2- Nuclear beta-catenin staining
3- Nuclear SMAD4 staining
4- Vimentin positivity
PREFERRED RESPONSE: 2- Nuclear beta-catenin staining
DISCUSSION
Desmoid tumors are characterized by aberrant activation of Wnt signaling resulting from
mutations in the adenomatous polyposis coli and beta-catenin genes. Although a nuclear beta-
catenin staining pattern can be observed in other tumor types, it is highly specific for desmoid
tumor. Vimentin positivity indicates that a lesion is a mesenchymal neoplasm, but it is not
specific for desmoid tumor.
RECOMMENDED READINGS
Ng TL, Gown AM, Barry TS, Cheang MC, Chan AK, Turbin DA, Hsu FD, West RB, Nielsen TO. Nuclear beta-catenin in mesenchymal
tumors. Mod Pathol. 2005 Jan;18(1):68-74. PubMed PMID: 15375433. View Abstract at PubMed
Tejpar S, Nollet F, Li C, Wunder JS, Michils G, dal Cin P, Van Cutsem E, Bapat B, van Roy F, Cassiman JJ, Alman BA. Predominance of beta-catenin mutations and beta-catenin dysregulation in sporadic aggressive fibromatosis (desmoid tumor). Oncogene. 1999 Nov
11;18(47):6615-20. PubMed PMID: 10597266.
View Abstract at PubMed
Figure 69a
Figure 69b
Figure 69c
Figure 69d
Question 69 of 143

A 30-year-old woman has progressive gait instability, back pain, and urinary retention.
Figures 69a and 69b show the axial T2 and postcontrast MRI scans taken at the level of T11,
and Figure 69c shows the sagittal T1-weighted image. Representative histology is shown in
Figure 69d. The patient remains ambulatory, but symptoms have progressed during the last
week and she is beginning to feel weakness in her legs. Examination is notable for decreased
rectal tone, lower-extremity hyperreflexia and clonus, and 4/5 motor strength throughout the
lower extremities. What is the most appropriate treatment recommendation for this patient?
1- Margin-free en bloc spondylectomy of T11
2- Radiation therapy
3- Radiation therapy followed by anterior corpectomy and fusion
4- Transpedicular decompression and posterior stabilization followed by radiation therapy
PREFERRED RESPONSE: 4- Transpedicular decompression and posterior stabilization
followed by radiation therapy
DISCUSSION
This patient has symptomatic metastatic epidural spinal cord compression from synovial
sarcoma with pathologic fracture and epidural extension of disease. Patchell and associates
demonstrated outcomes with direct decompressive surgery followed by radiation therapy that
were superior to radiation alone for patients presenting in this manner; note that the trial
excluded patients with exquisitely radiosensitive malignancies such as lymphoma and germ-
cell tumors. Ibrahim and associates confirmed these results in a prospective multicenter
observational study. The sagittal T1-weighted image shows other lesions at T1 and T5,
confirming a metastatic process. The histology shows synovial sarcoma and excludes
hematopoietic or germ-cell malignancy (very radiosensitive). Margin-free en bloc
spondylectomy would be difficult to achieve considering extension of tumor into the
posterior elements, degree of epidural compression, and abutment of the aorta. More
important, it is difficult to justify the magnitude and risk associated with this procedure in a
patient with multiple metastatic lesions. Radiation therapy alone and radiation followed by
surgery were shown in Patchell’s study to have inferior outcomes. A patient with a
progressive neurologic deficit should have surgery before radiotherapy.
RECOMMENDED READINGS
Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, Mohiuddin M, Young B. Direct decompressive surgical resection in the
treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005 Aug 20-26;366(9486):643-8. PubMed
PMID: 16112300. View Abstract at PubMed
Ibrahim A, Crockard A, Antonietti P, Boriani S, Bünger C, Gasbarrini A, Grejs A, Harms J, Kawahara N, Mazel C, Melcher R, Tomita K. Does spinal surgery improve the quality of life for those with extradural (spinal) osseous metastases? An international multicenter
prospective observational study of 223 patients. Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral
Nerves, March 2007. J Neurosurg Spine. 2008 Mar;8(3):271-8. doi: 10.3171/SPI/2008/8/3/271. PubMed PMID: 18312079. View Abstract at PubMed
Wang JC, Boland P, Mitra N, Yamada Y, Lis E, Stubblefield M, Bilsky MH. Single-stage posterolateral transpedicular approach for resection of epidural metastatic spine tumors involving the vertebral body with circumferential reconstruction: results in 140 patients.
Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2004. J Neurosurg Spine. 2004
Oct;1(3):287-98. PubMed PMID: 15478367. View Abstract at PubMed

Question 70 of 143
Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most
common type of tumor involving this anatomical location?
1- Conventional chondrosarcoma
2- Aneurysmal bone cyst
3- Chondroblastoma
4- Osteoblastoma
PREFERRED RESPONSE: 3- Chondroblastoma
DISCUSSION
Giant-cell tumor is the most common lesion involving the epiphysis, although its epicenter is
usually in the metaphysis, and in the rare case of giant-cell tumor occurring in a skeletally
immature patient, giant-cell tumor is located in the metaphysis. It also can involve the flat
bone of the pelvis and sacrum. Chondroblastoma exclusively occurs in the epiphysis of
skeletally immature patients. It is more common than the other responses. Although
conventional chondrosarcoma does not involve the epiphysis, clear-cell chondrosarcoma
involves the epiphysis as well; however, it is rare and less common than chondroblastoma.
Aneurysmal bone may occur in the epiphysis; however, it is often seen with other benign
tumors such as chondroblastoma or giant-cell tumor. It is less common in this location than
chondroblastoma. Osteoblastoma does not classically appear at the epiphysis. It is more
commonly seen in the spine or the diaphysis of long bones.
RECOMMENDED READINGS
Sailhan F, Chotel F, Parot R; SOFOP. Chondroblastoma of bone in a pediatric population. J Bone Joint Surg Am. 2009 Sep;91(9):2159-68.
doi: 10.2106/JBJS.H.00657. PubMed PMID: 19723993. View Abstract at PubMed
Ramappa AJ, Lee FY, Tang P, Carlson JR, Gebhardt MC, Mankin HJ. Chondroblastoma of bone. J Bone Joint Surg Am. 2000 Aug;82-A(8):1140-5. PubMed PMID: 10954104.
View Abstract at PubMed
Figure 71a
Figure 71b
Figure 71d
Figure 71e

Figure 71c
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy
who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He
complains of increased pain when he runs and also of pain that wakes him at night. This pain
is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
Question 71 of 143
What is the most likely diagnosis?
1- Stress fracture
2- Osteomyelitis
3- Osteoid osteoma
4- Eosinophilic granuloma
PREFERRED RESPONSE: 3- Osteoid osteoma
Question 72 of 143
Contemporary definitive treatment for this patient is
1- NSAIDs.
2- radiofrequency ablation.
3- intravenous antibiotics.
4- burr-down technique resection.
PREFERRED RESPONSE: 2- radiofrequency ablation.
Question 73 of 143
What is the etiology of the pain associated with this lesion?
1- Prostaglandin production
2- Gram-positive cocci
3- Osteoclast activation
4- Loss of structural integrity of the bone
PREFERRED RESPONSE: 1- Prostaglandin production
DISCUSSION

Osteoid osteomas are most common in adolescent patients and in boys. Although these
tumors can be seen in any bone, almost half are located in the femur and tibia. The significant
inflammatory response to this tumor is presumed to be secondary to high levels of
prostaglandin production. Characteristic pain at night is relieved by aspirin or NSAIDs. Pain
can also be associated with activities and is characterized as being boring and sharp.
Radiographs often show distinctive features of thickened bone surrounding a small central
core of lower density (a nidus). Thin-cut CT scan is the imaging modality of choice for
visualizing the nidus, which typically lies within the cortex of the bone. An MRI scan may be
misleading because of the extensive edema associated with this lesion, bringing other
differential diagnoses into question. A bone scan is also associated with significant uptake but
is nonspecific. Several treatment options are available, including observation and
management with NSAIDs for pain control, with the premise that the lesion will “burn out.”
This may take several years to occur and few patients are content with this treatment regimen.
Surgical resection can be accomplished with en bloc resection, but this approach is fraught
with complications associated with resecting large segments of bone. A fluoroscopically
assisted “burr-down” technique is effective in removing the nidus and minimizing the stress
riser effect to the bone but requires an open surgery. Radiofrequency ablation is the current
first-line treatment modality for osteoid osteoma because of its high efficacy and low
morbidity.
CT-guided radiofrequency ablation removal of the nidus has been successfully used with few
recurrences or complications. This is a lesser procedure, compared to en bloc resection or
intralesional surgery, and may be performed under general anesthesia or a regional block with
sedation. The site of the tumor is identified using fine CT sections, and a radiofrequency
probe is inserted into the tumor. The probe heats the tumor tissues to approximately 90°C,
effectively obliterating the nidus with minimal damage to surrounding tissues. The nidus is
adequately removed in 96% of patients after 1 treatment. The procedure is routinely
performed on an outpatient basis by either an interventional radiologist or an orthopaedic
surgeon. Most procedures take approximately 2 hours, followed by a 2-hour recovery period,
after which the patient may go home with a mild pain reliever. In most cases, the patient may
return to work or school in a few days with some restrictions.
RECOMMENDED READINGS
Rimondi E, Bianchi G, Malaguti MC, Ciminari R, Del Baldo A, Mercuri M, Albisinni U. Radiofrequency thermoablation of primary non-
spinal osteoid osteoma: optimization of the procedure. Eur Radiol. 2005 Jul;15(7):1393-9. Epub 2005 Mar 9. PubMed PMID: 15756555. View Abstract at PubMed
Ward WG, Eckardt JJ, Shayestehfar S, Mirra J, Grogan T, Oppenheim W. Osteoid osteoma diagnosis and management with low morbidity. Clin Orthop Relat Res. 1993 Jun;(291):229-35. PubMed PMID: 8504605.
View Abstract at PubMed
Ilyas I, Younge DA. Medical management of osteoid osteoma. Can J Surg. 2002 Dec;45(6):435-7. PubMed PMID: 12500919.
View Abstract at PubMed

Figure 74
Question 74 of 143
Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most
influenced by
1- stage at presentation.
2- grade at presentation.
3- response to neoadjuvant chemotherapy.
4- histologic subtype.
PREFERRED RESPONSE: 1- stage at presentation.
DISCUSSION
The imaging is characteristic for high-grade osteosarcoma. In patients with osteosarcoma,
stage at presentation has the most prognostic impact; clinically detectable mestastases at
presentation has a very poor prognosis. The other factors all influence prognosis in patients
without metastatic disease. Low-grade nonmetastatic tumors have the best prognosis and are
treated with surgery alone. In high-grade tumors, histologic response to neoadjuvant
chemotherapy is predictive of survival. Response to chemotherapy, distal appendicular sites,
and female gender were associated with improved survival in the study by Whelan and
associates of 1067 patients with localized extremity osteosarcoma. Increased tumor volume
after chemotherapy had an adverse effect on survival independent of histologic response to
chemotherapy. Age, high levels of alkaline phosphatase, tumor volume, 2-drug regimen,
surgical margins, and histologic response to chemotherapy were important prognostic factors.
RECOMMENDED READINGS
Whelan JS, Jinks RC, McTiernan A, Sydes MR, Hook JM, Trani L, Uscinska B, Bramwell V, Lewis IJ, Nooij MA, van Glabbeke M,
Grimer RJ, Hogendoorn PC, Taminiau AH, Gelderblom H. Survival from high-grade localised extremity osteosarcoma: combined results
and prognostic factors from three European Osteosarcoma Intergroup randomised controlled trials. Ann Oncol. 2012 Jun;23(6):1607-16. doi: 10.1093/annonc/mdr491. Epub 2011 Oct 19. PubMed PMID: 22015453.
View Abstract at PubMed
Kim MS, Lee SY, Cho WH, Song WS, Koh JS, Lee JA, Yoo JY, Jung ST, Jeon DG. Effect of increases in tumor volume after neoadjuvant
chemotherapy on the outcome of stage II osteosarcoma regardless of histological response. J Orthop Sci. 2009 May;14(3):292-7. doi:
10.1007/s00776-009-1334-y. Epub 2009 Jun 5. PubMed PMID: 19499296. View Abstract at PubMed
Bacci G, Longhi A, Versari M, Mercuri M, Briccoli A, Picci P. Prognostic factors for osteosarcoma of the extremity treated with neoadjuvant chemotherapy: 15-year experience in 789 patients treated at a single institution. Cancer. 2006 Mar 1;106(5):1154-61. PubMed
PMID: 16421923.
View Abstract at PubMed

Figure 75a
Figure 75b
Figure 75c
Figure 75d
Question 75 of 143
Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old
man who has had a several-month history of progressive pain in his right hip and groin
region. Based on these images and histology, what is the most appropriate treatment?
1- Wide resection
2- Curetting and bone grafting
3- Percutaneous cementation and radiotherapy
4- Chemotherapy and radiotherapy
PREFERRED RESPONSE: 1- Wide resection
DISCUSSION
The imaging (which includes a clear chest CT scan) demonstrates a lytic periacetabular lesion
with internal matrix production and a cellular cartilage lesion on histology, diagnostic for a
chondrosarcoma with negative staging. Wide excision with limb salvage is appropriate for a
lesion without evidence of neurovascular encasement. Although used for select low-grade
cartilage lesions in the extremity, curettage is not indicated for pelvic chondrosarcomas.
Radiation and chemotherapy are not used in the treatment of conventional chondrosarcoma.
RECOMMENDED READINGS
Han I, Lee YM, Cho HS, Oh JH, Lee SH, Kim HS. Outcome after surgical treatment of pelvic sarcomas. Clin Orthop Surg. 2010 Sep;2(3):160-6. doi: 10.4055/cios.2010.2.3.160. Epub 2010 Aug 3. PubMed PMID: 20808587.
View Abstract at PubMed
Deloin X, Dumaine V, Biau D, Karoubi M, Babinet A, Tomeno B, Anract P. Pelvic chondrosarcomas: surgical treatment options. Orthop
Traumatol Surg Res. 2009 Oct;95(6):393-401. doi: 10.1016/j.otsr.2009.05.004. Epub 2009 Oct 3. PubMed PMID: 19801212.
View Abstract at PubMed

Figure 76
Question 76 of 143
Figure 76 is the radiograph of a 77-year-old patient with a history of myeloma who has had
severe arm pain after opening a jar. Pain was present for 3 months prior to injury. The most
biomechanically stable construct for this fracture is
1- intramedullary nailing (IMN).
2- IMN and cement.
3- plate.
4- plate and cement.
PREFERRED RESPONSE: 4- plate and cement.
DISCUSSION
Although intramedullary nails or plates with screws, either of which may be combined with
cement, may be used as internal fixation for a displaced humeral diaphyseal pathologic
fracture, torsional performance is best biomechanically when the canal is filled with cement
and fixed with a plate. In the largest comparative biomechanical study to date, 40 artificial
humeri were divided into 5 different constructs and tested in torsion. The construct that
resisted the largest load to failure was the construct at which the canal and tumor defect were
filled with bone cement and the screws were inserted into dry cement. That being said, the
weaknesses of the plate and cement technique include the potential for poor quality bone
adjacent to and extending away from the fracture site and difficulty in protecting the entire
bone from progression of local disease. Numerous factors beyond just the biomechanics,
including the patient’s disease load and comorbidities, the underlying primary disease and
responsiveness to radiotherapy and other adjuvant treatments, and the location and local
extent of disease, must be considered when determining the best operative technique to
employ in each patient with a pathologic fracture.
RECOMMENDED READINGS
Al-Jahwari A, Schemitsch EH, Wunder JS, Ferguson PC, Zdero R. The biomechanical effect of torsion on humeral shaft repair techniques
for completed pathological fractures. J Biomech Eng. 2012 Feb;134(2):024501. doi: 10.1115/1.4005696. PubMed PMID: 22482676. View Abstract at PubMed
Weiss KR, Bhumbra R, Biau DJ, Griffin AM, Deheshi B, Wunder JS, Ferguson PC. Fixation of pathological humeral fractures by the cemented plate technique. J Bone Joint Surg Br. 2011 Aug;93(8):1093-7. doi: 10.1302/0301-620X.93B8.26194. PubMed PMID: 21768635.
View Abstract at PubMed

Figure 77a
Figure 77b
Figure 77c
CLINICAL SITUATION FOR QUESTIONS 77 THROUGH 79
Figures 77a through 77c are the radiograph and MRI scans of a 45-year-old woman who
enjoys dancing and has had left ankle pain for approximately 1 month with minimal trauma.
She has slightly limited ankle dorsiflexion with a mechanical block with pain.
Question 77 of 143
What process most likely led to the pathology?
1- Synovial metaplasia
2- Posttraumatic heterotopic ossification
3- Malignant chondroid development
4- Neoplastic proliferation of a mixed epithelial and spindle-cell lesion
PREFERRED RESPONSE: 1- Synovial metaplasia
Question 78 of 143
An anterior approach to the ankle is chosen to resect this lesion. From medial to lateral, what
are the structures just below the level of the ankle joint?
1- Extensor hallucis longus (EHL) tendon, tibialis anterior (TA) tendon, deep peroneal nerve,
anterior tibial artery, extensor digitorum longus (EDL) tendon
2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL
3- TA, EHL, EDL, deep peroneal nerve, anterior tibial artery
4- TA, deep peroneal nerve, anterior tibial artery, EHL, EDL
PREFERRED RESPONSE: 2- TA, EHL, anterior tibial artery, deep peroneal nerve, EDL
Question 79 of 143

The patient undergoes recommended surgery and minimal joint damage is found. How
should she be counseled regarding her future prognosis?
1- High risk for local recurrence, moderate risk for metastases
2- High risk for local recurrence, no risk for metastases
3- Low risk for local recurrence, moderate risk for metastases
4- Low risk for local recurrence, no risk for metastases
PREFERRED RESPONSE: 4- Low risk for local recurrence, no risk for metastases
DISCUSSION
This patient has history and imaging consistent with synovial chondromatosis (synovial
osteochondromatosis). This condition most often is seen in larger joints, particularly the knee,
but has been well described in the ankle. The most common cause is primary synovial
chondromatosis, which is a benign proliferative chondroid metaplasia of the synovium. These
can exist in various states of calcification. In this patient, the radiographs and MRI scan
reveal multiple well-calcified lesions in the anterior portion of the joint with an effusion.
Secondary synovial chondromatosis can occur after trauma in the joint but is most likely
related to degenerative changes in the articular cartilage or meniscus/labral tissue.
Heterotopic ossification is rarely intra-articular, and would more likely have only 1 mass.
Neoplastic chondroid development would be a chondrosarcoma, which is exceedingly rare in
an intra-articular location, and, even with calcification, would be a solitary mass. Synovial
sarcoma is often seen in the foot and ankle, but is usually extra-articular nonsynovial with a
mixed epithelial and spindle-cell morphology.
Treatment of synovial chondromatosis is resection of the lesions and synovectomy.
Combined anterior and posterior approaches often can be used, and arthroscopy often is
helpful. Without significant removal of joint structures, there should be minimal instability
after surgery. A single surgery should handle the problem, but there is a small chance of local
recurrence. As a benign process, synovial chondromatosis does not metastasize.
RECOMMENDED READINGS
Holm CL. Primary synovial chondromatosis of the ankle. A case report. J Bone Joint Surg Am. 1976 Sep;58(6):878-80. PubMed PMID: 956234.
View Abstract at PubMed
Bojanic I, Bergovec M, Smoljanovic T. Combined anterior and posterior arthroscopic portals for loose body removal and synovectomy for
synovial chondromatosis. Foot Ankle Int. 2009 Nov;30(11):1120-3. doi: 10.3113/FAI.2009.1120. PubMed PMID: 19912726.
View Abstract at PubMed

Figure 80a
Figure 80b
Figure 80c
Figure 80d
Question 80 of 143
Figures 80a through 80d are the radiographs and MRI scans of a 16-year-old girl who
requires crutches because she is unable to bear weight on her right lower extremity. The pain
has progressed over 2 months despite nonsurgical treatment. Treatment at this point should
include
1- continued observation.
2- aspiration and injection with methylprednisolone.
3- curettage and grafting.
4- wide margin resection.
PREFERRED RESPONSE: 3- curettage and grafting.
DISCUSSION
This lesion represents a nonossifying fibroma (NOF). In general, NOFs are found incidentally
and require no treatment other than serial follow up for a period of time to document stability.
However, when they are painful, particularly with weight bearing, the likelihood of
impending or evolving pathological fracture must be considered. In this patient, curettage and
grafting with or without internal fixation is the surgical treatment of choice. Although
aspiration and injection with methylprednisolone is appropriate for unicameral bone cysts, it
has little role in the management of NOF. Wide margin resection is reserved for malignancy,
which is not evident in this clinical scenario.
RECOMMENDED READINGS
Moretti VM, Slotcavage RL, Crawford EA, Lackman RD, Ogilvie CM. Curettage and graft alleviates athletic-limiting pain in benign lytic
bone lesions. Clin Orthop Relat Res. 2011 Jan;469(1):283-8. doi: 10.1007/s11999-010-1374-9. Epub 2010 May 12. PubMed PMID: 20461483.
View Abstract at PubMed
Vanel D, Ruggieri P, Ferrari S, Picci P, Gambarotti M, Staals E, Alberghini M. The incidental skeletal lesion: ignore or explore? Cancer
Imaging. 2009 Oct 2;9 Spec No A:S38-43. doi: 10.1102/1470-7330.2009.9009. Review. PubMed PMID: 19965292.
View Abstract at PubMed
Vlychou M, Athanasou NA. Radiological and pathological diagnosis of paediatric bone tumours and tumour-like lesions. Pathology. 2008
Feb;40(2):196-216. doi: 10.1080/00313020701813784. Review. PubMed PMID: 18203042. View Abstract at PubMed

Question 81 of 143
A previously healthy 60-year-old woman has a T5 pathologic compression fracture secondary
to metastatic renal cell carcinoma. She has myelopathy with severe pain upon sitting from a
supine position. The adjacent thoracic levels are unaffected. On MRI scan, there is minimal
space available for the cord because of epidural involvement. What is the optimal treatment
method at this time?
1- Surgical decompression and instrumented fusion
2- Surgical decompression without fusion
3- Image-guided intensity-modulated radiation therapy
4- Chemotherapy
PREFERRED RESPONSE: 1- Surgical decompression and instrumented fusion
DISCUSSION
Data strongly support surgical treatment for spinal metastases when neurologic compromise
and/or mechanical instability are present. In this patient, pain upon sitting from a supine
position is a sign of mechanical instability. Although radiation therapy and chemotherapy are
appropriate for the treatment of spinal metastases in other circumstances, the optimal
treatment method in this case is to surgically decompress the affected level and restore
mechanical stability by fusing the motion segment.
RECOMMENDED READINGS
Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, Mohiuddin M, Young B. Direct decompressive surgical resection in the
treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005 Aug 20-26;366(9486):643-8. PubMed PMID: 16112300.
View Abstract at PubMed
Furlan JC, Chan KK, Sandoval GA, Lam KC, Klinger CA, Patchell RA, Laporte A, Fehlings MG. The combined use of surgery and
radiotherapy to treat patients with epidural cord compression due to metastatic disease: a cost-utility analysis. Neuro Oncol. 2012
May;14(5):631-40. doi: 10.1093/neuonc/nos062. Epub 2012 Apr 14. PubMed PMID: 22505658. View Abstract at PubMed
Figure 82a
Figure 82b
Figure 82c
Figure 82d
Question 82 of 143

Figures 82a and 82b are the MRI scans consisting of a T2 coronal sequence and axial T1
pulse sequence of a 38-year-old man who has had right thigh pain and a mass for 4 months
since he pulled his hamstring. The presumed diagnosis considering his clinical history and
evaluation of the MRI scan was hematoma and the mass was evacuated. The histology is
shown in Figures 82c and 82d. Next treatment steps should include
1- physical therapy to accelerate healing and improve function.
2- a complete hematologic work-up to evaluate a bleeding disorder.
3- tumor bed excision and radiation to reduce local recurrence.
4- radiotherapy to complete definitive treatment of this problem.
PREFERRED RESPONSE: 3- tumor bed excision and radiation to reduce local recurrence.
DISCUSSION
Unplanned excisions of soft-tissue sarcomas occur with alarming frequency and result in high
rates of residual disease, potentially affecting local control and local morbidity. Patients with
unplanned excisions who undergo limb-salvage procedures require more extensive surgical
procedures involving free flaps and skin grafting and more adjuvant radiotherapy; amputation
also may be required. Unplanned excisions of high-grade soft-tissue sarcomas result in
increased rates of local recurrence but do not diminish disease-specific survival. Patients with
unplanned excisions of high-grade sarcomas require adequate surgical excision and radiation.
Radiation alone or physical therapy is incomplete treatment in this setting. Soft-tissue
sarcomas are often mistaken for spontaneous hematomas because of central tumor necrosis
and intratumoral bleeding, but a hematologic evaluation in a patient with a soft-tissue
sarcoma is not warranted.
RECOMMENDED READINGS
Potter BK, Adams SC, Pitcher JD Jr, Temple HT. Local recurrence of disease after unplanned excisions of high-grade soft tissue sarcomas.
Clin Orthop Relat Res. 2008 Dec;466(12):3093-100. doi: 10.1007/s11999-008-0529-4. Epub 2008 Sep 26. PubMed PMID: 18818981.
View Abstract at PubMed
Temple HT, Worman DS, Mnaymneh WA. Unplanned surgical excision of tumors of the foot and ankle. Cancer Control. 2001 May-
Jun;8(3):262-8. PubMed PMID: 11378652. View Abstract at PubMed
Figure 83a
Figure 83b
Figure 83c
Question 83 of 143
Figures 83a through 83c are the radiograph and MRI scans of a 16-year-old girl who had
posterior knee pain after a dance recital 3 weeks ago; the pain resolved 1 week ago with
ibuprofen use. What is the appropriate treatment for this patient?

1- Biopsy and resection of lesion
2- Observation and serial radiographs
3- Tc-99 whole-body bone scan and fine-cut CT scan
4- Evaluation by a pediatric oncologist
PREFERRED RESPONSE: 2- Observation and serial radiographs
DISCUSSION
The images reveal a small reactive-type lesion in the posteromedial aspect of the distal femur
consistent with an avulsive cortical irregularity. Also referred to as a cortical desmoid,
periosteal desmoid, or “tug lesion,” it is seen most commonly in young adolescents, with a
slight preponderance in boys, with one-third occurring bilaterally. It is thought to be related
to repeated microtrauma with pulling of the adductor magnus or medial gastrocnemius head.
Proper treatment involves recognition of this benign disorder without further work-up. Often
best seen on an oblique radiograph, the lack of soft-tissue mass or bone destruction leads to
the benign diagnosis. Serial radiographs may show complete resolution by age 20.
RECOMMENDED READINGS
Gould CF, Ly JQ, Lattin GE Jr, Beall DP, Sutcliffe JB 3rd. Bone tumor mimics: avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007
May-Jun;36(3):124-41. Review. PubMed PMID: 17484955. View Abstract at PubMed
Yamazaki T, Maruoka S, Takahashi S, Saito H, Takase K, Nakamura M, Sakamoto K. MR findings of avulsive cortical irregularity of the distal femur. Skeletal Radiol. 1995 Jan;24(1):43-6. PubMed PMID: 7709251.
View Abstract at PubMed
Damron TA, Morris C, Rougraff B, Tamurian R. Diagnosis and treatment of joint-related tumors that mimic sports-related injuries. Instr
Course Lect. 2009;58:833-47. PubMed PMID: 19385590. View Abstract at PubMed
Figure 84a
Figure 84b
CLINICAL SITUATION FOR QUESTIONS 84 THROUGH 86
Figures 84a and 84b are the CT and MRI scans of a 17-year-old girl with a painful
lumbosacral scoliosis that has been present for 12 months. Examination is notable only for
pain over the left sacral region and a postural scoliosis leaning away from this side.
Question 84 of 143
The girl’s parents should be advised that their daughter’s condition
1- will respond to bracing and require treatment if curve magnitude exceeds 45 degrees at
skeletal maturity.
2- results from a genetic mutation.

3- requires prolonged antibiotic treatment.
4- is likely to respond to percutaneous intervention.
PREFERRED RESPONSE: 4- is likely to respond to percutaneous intervention.
Question 85 of 143
Medical treatment for this condition
1- uses nonsteroidal anti-inflammatory or aspirin medications.
2- uses radioactive iodine as first-line treatment.
3- centers on antimicrobial susceptibilities.
4- requires autologous stem cell transplantation.
PREFERRED RESPONSE: 1- uses nonsteroidal anti-inflammatory or aspirin medications.
Question 86 of 143
With treatment, the spinal deformity is expected to
1- spontaneously resolve.
2- remain stable and nonprogressive.
3- respond in proportion to the family’s compliance with brace treatment.
4- resolve in the coronal plane and progress in the sagittal plane.
PREFERRED RESPONSE: 1- spontaneously resolve.
DISCUSSION
This young woman has classic imaging features of a sacral ala osteoid osteoma. Preferred
treatment is removal or ablation of the nidus by surgery or percutaneous techniques. Bracing
may be used for adolescent idiopathic scoliosis, but plays no role in the treatment of scoliosis
secondary to osteoid osteoma. Antibiotics would be used for osteomyelitis. There is no
known genetic predisposition to osteoid osteoma.
Nonsteroidal medications or aspirin will alleviate symptoms in the short term. Antibiotics,
radioactive iodine, and stem cell transplantation play no role in treatment for osteoid
osteoma.
The “scoliosis” is expected to resolve following treatment. Bracing is not needed. No lasting
spinal deformity is expected.
RECOMMENDED READINGS
Atesok KI, Alman BA, Schemitsch EH, Peyser A, Mankin H. Osteoid osteoma and osteoblastoma. J Am Acad Orthop Surg. 2011 Nov;19(11):678-89. Review. PubMed PMID: 22052644.
View Abstract at PubMed

Kelly CM. Benign tumors of bone. In: Damron TA, ed. Orthopedic Surgery Essentials: Oncology and Basic Science. Philadelphia, PA:
Lippincott Williams and Wilkins; 2008:54-60.
Figure 87a
Figure 87b
Figure 87c
Figure 87d
Figure 87e
Question 87 of 143
Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-
old woman who is experiencing pain in her distal thigh with activity and at night. She has
undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
1- external beam radiation.
2- curetting and cementation.
3- radiofrequency ablation.
4- wide local resection.
PREFERRED RESPONSE: 4- wide local resection.
DISCUSSION
The imaging shows a cartilaginous lesion with destruction and a malignant extraosseous mass
most consistent with a dedifferentiated chondrosarcoma. The histology demonstrates a high-
grade spindle-cell sarcoma abutting a cartilaginous tumor, confirming this diagnosis.
Treatment in this patient would be wide resection. The role of chemotherapy in this tumor is
unproven, and an 85-year-old patient is an unlikely candidate for such treatment.
Radiofrequency ablation, curettage, and radiation do not play a role in the treatment of this
tumor.
RECOMMENDED READINGS
Mavrogenis AF, Ruggieri P, Mercuri M, Papagelopoulos PJ. Dedifferentiated chondrosarcoma revisited. J Surg Orthop Adv. 2011
Summer;20(2):106-11. Review. PubMed PMID: 21838071.
View Abstract at PubMed
Dickey ID, Rose PS, Fuchs B, Wold LE, Okuno SH, Sim FH, Scully SP. Dedifferentiated chondrosarcoma: the role of chemotherapy with
updated outcomes. J Bone Joint Surg Am. 2004 Nov;86-A(11):2412-8. PubMed PMID: 15523011. View Abstract at PubMed

Figure 88a
Figure 88b
Figure 88c
CLINICAL SITUATION FOR QUESTIONS 88 through 92
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of
localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens
with any activity and at night. She appears otherwise healthy.
Question 88 of 143
The next treatment step is
1- radiotherapy.
2- CT scan of the chest, abdomen, and pelvis.
3- bone marrow biopsy.
4- surgical stabilization.
PREFERRED RESPONSE: 2- CT scan of the chest, abdomen, and pelvis.
Question 89 of 143
What is the role of presurgical lesional biopsy for this patient?
1- Unnecessary, considering the known history of renal cell carcinoma
2- Should be performed before any surgical treatment
3- Should be performed if the lesion is solitary, but not necessarily if multifocal
4- Should always be accompanied by bone marrow biopsy
PREFERRED RESPONSE: 3- Should be performed if the lesion is solitary, but not
necessarily if multifocal
Question 90 of 143
Representative histology is shown in Figure 88c. Advanced imaging shows mild extraosseous
extent of disease, nondisplaced pathologic fracture, and no neurovascular encasement. The
humerus is best managed with

1- radiotherapy.
2- closed intramedullary rodding.
3- curettage, cancellous allograft, and plate fixation.
4- resection and reconstruction.
PREFERRED RESPONSE: 4- resection and reconstruction.
Question 91 of 143
Chemotherapeutic treatment for this patient
1- centers on bone marrow transplantation.
2- has severe myelosuppressive effects.
3- inhibits vascular endothelial growth factor (VEGF) pathways.
4- is given as a radiation sensitizer.
PREFERRED RESPONSE: 3- inhibits vascular endothelial growth factor (VEGF) pathways.
Question 92 of 143
Oncologic outcome for this patient
1- is influenced by extraosseous tumor extension.
2- is more favorable if the lesion is solitary.
3- involves a predictable rapid demise.
4- hinges on the presence or absence of gene amplification.
PREFERRED RESPONSE: 2- is more favorable if the lesion is solitary.
DISCUSSION
This patient has a lytic lesion filling the proximal humerus with a history of renal cell
carcinoma. In a patient with a history of localized cancer with a bone lesion, staging with CT
scan of the chest, abdomen, and pelvis (and a bone scan, as well) is indicated to define the
extent of disease. A positron emission tomography scan, not given as an option, would be a
reasonable substitute for a CT and bone scan. The most likely clinical scenario is the
development of metastatic renal cell carcinoma, and these tests will define the extent of
disease. Immediate radiotherapy would not be indicated without a diagnosis; as well, renal
cell carcinoma’s response to radiotherapy is unpredictable, and the extent of bony destruction
implies a degree of mechanical insufficiency that would benefit from surgical treatment.
Bone marrow biopsy would be indicated for hematopoietic tumors such as myeloma or
lymphoma. Reflexive surgery should be avoided until a diagnosis is obtained or a widespread
metastatic process is identified to avoid inadvertently mistreating a new sarcoma. As well,
curettage procedures near joints are not very durable in renal cell carcinoma because of its
aggressive behavior and radioresistance.

Biopsy generally is not necessary for patients with established metastatic disease and typical
presentations prior to surgical management. Additionally, if a patient has new metastatic
disease and multiple lesions, biopsy is not needed before surgery because histologic
confirmation can be obtained at surgery. However, for a patient with a solitary lesion and no
history of metastatic disease, biopsy is indicated to exclude a new primary tumor before
surgical treatment is undertaken.
The histology reveals clear-cell carcinoma consistent with a renal primary. Radiotherapy
alone is a poor option considering the unpredictable response of renal cell carcinoma to
radiation and the presence of a pathologic fracture. Closed intramedullary rodding would
provide little proximal fixation. Both this option and curettage are not optimal because of
significant bleeding and lack of durability in this situation. Amputation is seldom indicated
for metastatic disease (even if the neurovascular bundle is encased, which it is not). Formal
resection and reconstruction provides the most durable functional outcome. For a solitary
lesion, resection of the entire lesion would be preferable, although in other situations,
intralesional resection and prosthetic reconstruction may be applicable. If an intralesional
procedure is planned, embolization should be considered before surgery.
Recent understanding of the role of the VEGF pathway in renal cell carcinoma has led to the
use of tyrosine kinase inhibitors and related agents for chemotherapy. These can have wound-
healing effects (critical for surgeons to recognize and understand), but generally are not
myelosuppressive. Objective response rates approach 30%. Bone marrow transplantation and
radiosensitizing chemotherapy are not used in this situation.
Patients with metastatic renal cell carcinoma to bone have a median survival of 11.5 months
in the largest study, and this likely improves with newer adjuvant therapies. Patients with
solitary lesions have longer survival, but the likelihood of true cure is low even with en bloc
resection. There is no known prognostic significance of extraosseous extension or gene
amplification in renal carcinoma.
RECOMMENDED READINGS
Lin PP, Mirza AN, Lewis VO, Cannon CP, Tu SM, Tannir NM, Yasko AW. Patient survival after surgery for osseous metastases from renal cell carcinoma. J Bone Joint Surg Am. 2007 Aug;89(8):1794-801. PubMed PMID: 17671020.
View Abstract at PubMed
Posadas EM, Figlin RA. Systemic therapy in renal cell carcinoma: advancing paradigms. Oncology (Williston Park). 2012 Mar;26(3):290-
301. Review. PubMed PMID: 22545314.
View Abstract at PubMed
Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint
Surg Am. 2009 Jun;91(6):1518-30. Review. PubMed PMID: 19487533. View Abstract at PubMed
Figure 93a
Figure 93b

Question 93 of 143
Figures 93a and 93b are the MRI scans of a 24-year-old man with painless, persistent
swelling in his left knee without any trauma. What is the best next treatment step?
1- Arthroscopic anterior synovectomy and posterior open resection
2- Arthroscopic anterior synovectomy only
3- Radiation therapy and wide excision
4- Observation
PREFERRED RESPONSE: 3- Radiation therapy and wide excision
DISCUSSION
The lesion seen in the figures is pigmented villonodular synovitis (PVNS), as shown by the
dark areas on MRI scan attributable to chronic hemosiderin deposition. The age of the
patient, symptom of persistent swelling, and lack of trauma are all consistent with a synovial
proliferative disorder. The fronds arising from the synovium make PVNS the most likely of
the synovial proliferative diseases, which include PVNS, synovial chondromatosis, lipoma
arborescens, and synovial hemangioma. The imaging shows diffuse disease throughout the
knee in the anterior compartment and extra-articular disease extending from the posterior
compartment. The current accepted standard of care for initial presentation and treatment is
an anterior synovectomy and an open posterior approach to resect the extra-articular disease.
Recurrence rates for diffuse disease are higher with arthroscopic compared to open
synovectomy, although morbidity is lower with arthroscopic treatment. Radiation therapy and
wide excision would be reserved for a soft-tissue sarcoma, and, in the setting of a chronic
effusion, observation would not suffice because the joint is at risk for degradation from the
chronic hemosiderin and inflammatory reaction in the intra-articular space.
RECOMMENDED READINGS
van der Heijden L, Gibbons CL, Dijkstra PD, Kroep JR, van Rijswijk CS, Nout RA, Bradley KM, Athanasou NA, Hogendoorn PC, van de
Sande MA. The management of diffuse-type giant cell tumour (pigmented villonodular synovitis) and giant cell tumour of tendon sheath (nodular tenosynovitis). J Bone Joint Surg Br. 2012 Jul;94(7):882-8. doi: 10.1302/0301-620X.94B7.28927. Review. PubMed PMID:
22733940.
View Abstract at PubMed
Masih S, Antebi A. Imaging of pigmented villonodular synovitis. Semin Musculoskelet Radiol. 2003 Sep;7(3):205-16. Review. PubMed
PMID: 14593562. View Abstract at PubMed
Question 94 of 143
What biopsy technique for a posterior thigh sarcoma is associated with the highest risk for
adverse outcome?
1- Transverse incision open biopsy
2- Core needle biopsy
3- Fine-needle aspirate
4- Longitudinal incision open biopsy

PREFERRED RESPONSE: 1- Transverse incision open biopsy
DISCUSSION
Fundamental planning and execution of a biopsy are imperative to maximize a surgeon’s
technical ability to perform limb-salvage surgery and preclude risk for amputation as a result
of a poorly executed biopsy. An incorrectly performed biopsy can place a patient who is a
limb-salvage candidate into a non-limb-salvage category. Transverse incisions for a sarcoma
on an extremity are absolutely contraindicated. A transverse incision increases the extent of
dissection necessary to achieve an appropriate radical resection, contaminates more anatomic
planes, and places neurovascular structures at higher risk for contamination. In many
instances, a free vascularized muscle flap and/or skin grafting is needed to close the defect
created by an incorrectly performed biopsy. Meticulous hemostasis at the time of biopsy is
also essential to avoid contamination of additional tissue, thus expanding the extent of
dissection.
For open biopsies, incisions in line with the long axis of a limb are mandatory. Many tumors
are amenable to core needle biopsy. Placement of the needle or incision must be carefully
thought out to ensure that the biopsy tract may be excised in continuity with the mass at the
time of definitive resection surgery. In an ideal situation, the biopsy should be performed by
the surgeon, who will perform the definitive procedure. This obviates the need to speculate
about needle tracts and biopsy techniques. Fine-needle aspirate biopsies are generally safe,
but likely have lower diagnostic yield.
RECOMMENDED READINGS
Enneking WF. Musculoskeletal Tumor Surgery. Vol 1. Philadelphia, PA: Churchill-Livingstone; 1983: Chapters 1-3, 7.
Enneking WF, Maale GE. The effect of inadvertent tumor contamination of wounds during the surgical resection of musculoskeletal neoplasms. Cancer. 1988 Oct 1;62(7):1251-6. PubMed PMID: 3416267.
View Abstract at PubMed
Heslin MJ, Lewis JJ, Woodruff JM, Brennan MF. Core needle biopsy for diagnosis of extremity soft tissue sarcoma. Ann Surg Oncol. 1997
Jul-Aug;4(5):425-31. PubMed PMID: 9259971.
View Abstract at PubMed
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg
Am. 1982 Oct;64(8):1121-7. PubMed PMID: 7130225. View Abstract at PubMed
Shiu MH, Brennan MF. Surgical Management of Soft Tissue Sarcoma. Philadelphia, PA: Lea and Febiger; 1989:Chapter 6; 58-64.
Question 95 of 143
A 60-year-old woman with a history of breast cancer has a rapidly enlarging arm mass. The
lesion is situated outside of the prior irradiation field, but within an area of heavy
lymphedema involvement. Needle biopsy reveals a high-grade sarcoma. What is the most
likely diagnosis?
1- Lymphangiosarcoma
2- Acral myxoinflammatory fibroblastic sarcoma

3- Hemangioendothelioma
4- Hemangiopericytoma
PREFERRED RESPONSE: 1- Lymphangiosarcoma
DISCUSSION
Lymphangiosarcomas that arise in pre-existing lymphedema are aggressive malignancies (ie,
Stewart-Treves syndrome) that require resection or amputation. Acral myxoinflammatory
fibroblastic sarcoma is a low-grade sarcoma. Hemangioendothelioma and
hemangiopericytoma are not typically associated with chronic lymphedema.
RECOMMENDED READINGS
Hellman S, DeVita VT, Rosenberg S, eds. Cancer: Principles and Practice of Oncology. Philadelphia, PA: Lippincott-Raven; 2001:1853.
Chung KC, Kim HJ, Jeffers LL. Lymphangiosarcoma (Stewart-Treves syndrome) in postmastectomy patients. J Hand Surg Am. 2000
Nov;25(6):1163-8. Review. PubMed PMID: 11119680. View Abstract at PubMed
Figure 96a
Figure 96b
Figure 96c
Figure 96d
RESPONSES FOR QUESTIONS 96 THROUGH 100
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
Match the condition above to the patient description below.
Question 96 of 143
10-year-old girl with sickle cell anemia and a swollen, erythematous, and painful elbow
(Figures 96a through 96d)

1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
PREFERRED RESPONSE: 4- Osteomyelitis
Figure 97a
Figure 97b
Figure 97c
Figure 97d
Figure 97e
Figure 97f
RESPONSES FOR QUESTIONS 96 THROUGH 100
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
Match the condition above to the patient description below.
Question 97 of 143
12-year-old girl with knee and lower leg pain and swelling for 2 months after minor trauma
(Figures 97a through 97f)
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
PREFERRED RESPONSE: 1- Osteosarcoma

Figure 98a
Figure 98b
Figure 98c
Figure 98d
Figure 98e
RESPONSES FOR QUESTIONS 96 THROUGH 100
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
Match the condition above to the patient description below.
Question 98 of 143
11-year-old boy with severe pain in the lower back and pelvic region, particularly with
activity and at night; CD99 immunostaining positive (Figures 98a through 98e)
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
PREFERRED RESPONSE: 2- Ewing sarcoma
Figure 99a
Figure 99b
Figure 99c
Figure 99d
Figure 99e
Figure 99f
RESPONSES FOR QUESTIONS 96 THROUGH 100

1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
Match the condition above to the patient description below.
Question 99 of 143
4-year-old boy who began limping after having increasing pain in his lower thigh and knee
for 3 months (Figures 99a through 99f)
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
PREFERRED RESPONSE: 3- Langerhans cell histiocytosis (LCH)
Figure 100a
Figure 100b
Figure 100c
Figure 100d
Figure 100e
Figure 100f
RESPONSES FOR QUESTIONS 96 THROUGH 100
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
Match the condition above to the patient description below.

Question 100 of 143
22-year-old man with rapidly growing mass and severe swelling in the knee; CD20-positive
on immunostaining (Figures 100a through 100f)
1- Osteosarcoma
2- Ewing sarcoma
3- Langerhans cell histiocytosis (LCH)
4- Osteomyelitis
5- Primary lymphoma of bone
PREFERRED RESPONSE: 5- Primary lymphoma of bone
DISCUSSION
Osteomyelitis in the pediatric population occurs in approximately 1 in 5000 children.
Staphylococcus aureus accounts for approximately 80% of all infections. Staphylococcus
remains the most common organism in patients with sickle cell anemia; however, an unusual
culprit in these patients can be salmonella. Imaging studies may not be specific but often
show periosteal reaction, variable bone loss and production, and significant inflammation on
MRI scan. The classic sign on radiograph is “bone-in-bone” for subacute and chronic cases.
This often signifies new bone (involucrum) surrounding the necrotic “trapped” sequestrum.
The histopathology varies depending on the acuity of disease. A variety of inflammatory cells
often will be seen. Typically, more neutrophils are seen in acute disease, and lymphocytes
and macrophages in chronic disease. Chronic cases normally show focal areas of bone
necrosis with empty lacunae.
Osteosarcoma is the most common primary cancer of bone excluding multiple myeloma. It
most often occurs during the first 2 decades of life. The imaging studies show an aggressive
bone loss and new bone formation process in addition to a soft-tissue mass on MRI scan. In
this case, the radiograph shows an excellent example of a “sunburst” or “hair-on-end” pattern
signifying the rapid growth of the tumor and subsequent periosteal reaction. The
histopathology varies by subtype; however, the most common variety (classic, high grade) as
in this scenario demonstrates hypercellular round or spindle cells with atypia, pleomorphism,
atypical mitoses, and osteoid production. Ewing sarcoma is the second-most-common bone
sarcoma in children. It will demonstrate aggressive changes on radiograph, but, unlike
osteosarcoma, it frequently does not produce new bone within the matrix of the tumor.
However, periosteal elevation and bone reaction are often seen. This case shows subtle
changes on radiograph but impressive changes on MRI scan with a soft-tissue mass and
extensive bone marrow involvement. This is fairly common for small round blue-cell tumors
such as Ewing sarcoma/primitive neuroectodermal tumor, lymphoma, multiple myeloma, and
others. The histopathology often shows hypercellularity with sheets of small round blue cells.
In most cases, CD99 is positive and a characteristic 11:22 translocation is seen, making the
diagnosis definitive.
LCH is a rare condition with an uncertain pathogenesis. It is generally seen in patients
younger than 20 years of age and often can mimic other conditions such as infection or
cancer. The imaging studies can range from benign-looking with a focal, well-circumscribed
lesion to more common aggressive lesions with less-defined borders, periosteal reaction,
associated edema, and, in some cases, pathologic fracture. The histopathology in this case is

critical to the diagnosis. The presence of Langerhans cells in a granulomatous-like setting
with a reactive background of macrophages, eosinophils, multinucleate giant cells, and T
cells is important to identify. The Langerhans cell is a large, ovoid, mononuclear cell with a
folded nucleus, a discrete nucleolus, and moderate amounts of slightly eosinophilic
homogeneous cytoplasm. On electron microscopy, Birbeck granules with their tennis racquet
form can be seen in Langerhans cells. Primary lymphoma of bone is rare. It accounts for
approximately 1% of all lymphoma cases. As with other small round blue-cell tumors, the
imaging may vary. Osteolytic and osteoblastic findings may be present on radiograph, but
often the MRI scan reveals a larger-than-expected soft-tissue component. The histopathology
shows sheets of small round blue cells. These can be differentiated from others in this
category by flow cytometry and also by using specialized surface markers like CD20, as in
this case.
RECOMMENDED READINGS
Thomsen I, Creech CB. Advances in the diagnosis and management of pediatric osteomyelitis. Curr Infect Dis Rep. 2011 Oct;13(5):451-60.
doi: 10.1007/s11908-011-0202-z. PubMed PMID: 21789499. View Abstract at PubMed
Hatzenbuehler J, Pulling TJ. Diagnosis and management of osteomyelitis. Am Fam Physician. 2011 Nov 1;84(9):1027-33. Review. PubMed PMID: 22046943.
View Abstract at PubMed
Ejindu VC, Hine AL, Mashayekhi M, Shorvon PJ, Misra RR. Musculoskeletal manifestations of sickle cell disease. Radiographics. 2007
Jul-Aug;27(4):1005-21. Review. PubMed PMID: 17620464. View Abstract at PubMed
Jaffe N. Osteosarcoma: review of the past, impact on the future. The American experience. Cancer Treat Res. 2009;152:239-62. doi: 10.1007/978-1-4419-0284-9_12. Review. PubMed PMID: 20213394.
View Abstract at PubMed
Messerschmitt PJ, Garcia RM, Abdul-Karim FW, Greenfield EM, Getty PJ. Osteosarcoma. J Am Acad Orthop Surg. 2009 Aug;17(8):515-
27. Review. PubMed PMID: 19652033.
View Abstract at PubMed
Maheshwari AV, Cheng EY. Ewing sarcoma family of tumors. J Am Acad Orthop Surg. 2010 Feb;18(2):94-107. Review. PubMed PMID:
20118326. View Abstract at PubMed
Abla O, Egeler RM, Weitzman S. Langerhans cell histiocytosis: Current concepts and treatments. Cancer Treat Rev. 2010 Jun;36(4):354-9. doi: 10.1016/j.ctrv.2010.02.012. Epub 2010 Feb 25. Review. PubMed PMID: 20188480.
View Abstract at PubMed
Mikhaeel NG. Primary bone lymphoma. Clin Oncol (R Coll Radiol). 2012 Jun;24(5):366-70. doi: 10.1016/j.clon.2012.02.006. Epub 2012
Mar 6. Review. PubMed PMID: 22402011.
View Abstract at PubMed
Figure
101a
Figure
101b
Figure
102a
Figure
102b
Figure
103a
Figure
103b
Figure
104a
Figure
104b
RESPONSES FOR QUESTIONS 101 THROUGH 104

1- Clear cell renal carcinoma
2- Squamous carcinoma of the lung
3- Multiple myeloma
4- Metastatic adenocarcinoma
Match each set of photomicrographs with the correct diagnosis.
Question 101 of 143
Figures 101a and 101b
1- Clear cell renal carcinoma
2- Squamous carcinoma of the lung
3- Multiple myeloma
4- Metastatic adenocarcinoma
PREFERRED RESPONSE: 1- Clear cell renal carcinoma
Question 102 of 143
Figures 102a and 102b
1- Clear cell renal carcinoma
2- Squamous carcinoma of the lung
3- Multiple myeloma
4- Metastatic adenocarcinoma
PREFERRED RESPONSE: 4- Metastatic adenocarcinoma
Question 103 of 143
Figures 103a and 103b
1- Clear cell renal carcinoma
2- Squamous carcinoma of the lung
3- Multiple myeloma
4- Metastatic adenocarcinoma
PREFERRED RESPONSE: 2- Squamous carcinoma of the lung
Question 104 of 143
Figures 104a and 104b

1- Clear cell renal carcinoma
2- Squamous carcinoma of the lung
3- Multiple myeloma
4- Metastatic adenocarcinoma
PREFERRED RESPONSE: 3- Multiple myeloma
DISCUSSION
These photomicrographs represent metastatic entities commonly found in the bone. Renal
carcinoma is distinguished by large cells with vacuolated cytoplasm that warrant the term
"clear cell" carcinoma. Squamous carcinomas are characterized by nests of epithelial cells
that are relatively monotonous and form layers or sheets of cells. Myeloma is a plasma cell
proliferative disorder, and the cells are classified by the "clock-face" nuclei and basophilic
cytoplasm. Adenocarcinomas are noted to have the appearance of malignant cells forming
gland-like structures in the invaded tissue. The more well-differentiated the tumor, the more
prominent and distinctive are the glands. These representations are relatively classic for
lesions such as prostate and breast adenocarcinoma.
RECOMMENDED READINGS
Layfield LJ. Cytopathology of Bone and Soft Tissue Tumors. Oxford, England: Oxford University Press; 2002.
Unni KK, Inwards CY. Dahlin's Bone Tumors. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009.
Figure 105a
Figure 105b
Figure 105c
Figure 105d
Figure 105e
Figure 105f
Question 105 of 143
A 22-year-old mother noticed left leg pain while lifting her only child. A previous biopsy of
her left tibia 7 years ago had been interpreted as osteofibrous dysplasia. She has no other
medical history. Her current anteroposterior and lateral radiographs are shown in Figures
105a and 105b. Her comparative T2-weighted axial MRI scan from a similar area of the
diaphyseal tibia is shown in Figure 105c. The histologic specimens are shown in Figures
105d and 105e. A cytokeratin stain is shown in Figure 105f. The diagnosis is
1- osteofibrous dysplasia.
2- osteofibrous dysplasia-like adamantinoma.
3- low-grade osteosarcoma.
4- metastatic adenocarcinoma.

PREFERRED RESPONSE: 2- osteofibrous dysplasia-like adamantinoma.
DISCUSSION
An insidious onset of pain is a characteristic symptom in patients with adamantinoma. The
characteristic radiographic finding is a “soap-bubble” osteolytic lesion of the tibia with
surrounding sclerosis. A soft-tissue mass also is characteristic. Few keratin-positive cells are
seen in osteofibrous dysplasia. The characteristic fibrous stroma with spicules of bone with
basophilic epithelioid cells is diagnostic of adamantinoma. The other diagnoses mentioned do
not have these characteristics.
RECOMMENDED READINGS
Qureshi AA, Shott S, Mallin BA, Gitelis S. Current trends in the management of adamantinoma of long bones. An international study. J
Bone Joint Surg Am. 2000 Aug;82-A(8):1122-31. PubMed PMID: 10954102.
View Abstract at PubMed
Most MJ, Sim FH, Inwards CY. Osteofibrous dysplasia and adamantinoma. J Am Acad Orthop Surg. 2010 Jun;18(6):358-66. Review.
PubMed PMID: 20511441. View Abstract at PubMed
Figure 106a
Figure 106b
Figure 106c
Question 106 of 143
Figures 106a and 106b are the T1 sagittal and T2 coronal images of a 41-year-old woman
who has been experiencing electric shock-type radiating pain over her right ankle for 4½
years. Her biopsy specimen is shown in Figure 106c. What is the best next treatment step?
1- Marginal excision
2- Wide excision
3- Wide excision and radiation
4- Observation
PREFERRED RESPONSE: 1- Marginal excision
DISCUSSION
The lesion seen here is a benign nerve sheath tumor—specifically, a schwannoma. The
diagnosis of neurogenic tumors can be suggested from their imaging appearance, including
lesion shape and intrinsic imaging characteristics such as target and string signs. The
histology shows benign nerve elements including verocay bodies with Antoni A (more
cellular) and Antoni B (less cellular) areas. Most patients with benign nerve sheath tumors

present with a painful mass, paresthesias, or numbness without significant weakness.
Marginal excision with preservation of the associated nerve fibers is the optimal treatment for
symptomatic schwannomas. Wide excision eliminates symptoms successfully with minimal
concern for recurrence, but should be avoided to preserve nerve function. Wide excision with
or without radiation is not warranted in this benign condition, and, although observation is
acceptable for difficult locations or asymptomatic Schwannomas, the persistent symptoms
experienced by this patient preclude observation as the best option.
RECOMMENDED READINGS
Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic
tumors: radiologic-pathologic correlation. Radiographics. 1999 Sep-Oct;19(5):1253-80. PubMed PMID: 10489179.
View Abstract at PubMed
Levi AD, Ross AL, Cuartas E, Qadir R, Temple HT. The surgical management of symptomatic peripheral nerve sheath tumors. Neurosurgery. 2010 Apr;66(4):833-40. doi: 10.1227/01.NEU.0000367636.91555.70. PubMed PMID: 20190660.
View Abstract at PubMed
Figure 107a
Figure 107b
Figure 107c
Question 107 of 143
Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man.
While walking, he collapsed and was unable to ambulate because of pain and deformity in his
right leg. What is the most appropriate next step?
1- Staging studies to assess the extent of disease
2- Immediate stabilization of the fracture with an intramedullary nail

3- Curetting and bone culture
4- Segmental resection of the tibia and allograft reconstruction
PREFERRED RESPONSE: 1- Staging studies to assess the extent of disease
DISCUSSION
This patient has a pathologic fracture; in patients older than age 50, the most likely diagnosis
is metastatic carcinoma or hematopoietic malignancy. A systemic work-up with staging
imaging studies and laboratory tests as outlined by Rougraff and associates will identify the
primary site of disease in approximately 90% of patients. A biopsy may not be necessary, and
this protocol will also effectively exclude a primary sarcoma in the vast majority of patients.
The other options all initiate treatment without first evaluating for extent of disease and
diagnosis. If this turns out to be a sarcoma, stabilization or curetting the lesion might make
subsequent limb salvage difficult or impossible. Segmental resection adds unnecessary
morbidity to the surgical procedure in the more common circumstance that this is revealed to
be metastatic carcinoma.
RECOMMENDED READINGS
Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint
Surg Am. 2009 Jun;91(6):1518-30. Review. PubMed PMID: 19487533. View Abstract at PubMed
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149.
View Abstract at PubMed
RESPONSES FOR QUESTIONS 108 THROUGH 111
1- Glomus tumor
2- Diffuse pigmented villonodular synovitis (PVNS)
3- Extra-abdominal fibromatosis
4- Schwannoma
5- Hemangioma
Please match the characteristics below to the condition listed above.
Question 108 of 143
Painful lesion that frequently is triggered by cold and has characteristics of vascular origin
1- Glomus tumor
2- Diffuse pigmented villonodular synovitis (PVNS)
3- Extra-abdominal fibromatosis
4- Schwannoma
5- Hemangioma
PREFERRED RESPONSE: 1- Glomus tumor

Question 109 of 143
High local recurrence rate despite surgical excision and controversial to treat with
chemotherapy and/or external beam radiation; may have similar appearance as a soft-tissue
sarcoma.
1- Glomus tumor
2- Diffuse pigmented villonodular synovitis (PVNS)
3- Extra-abdominal fibromatosis
4- Schwannoma
5- Hemangioma
PREFERRED RESPONSE: 3- Extra-abdominal fibromatosis
Question 110 of 143
S-100-positive and low recurrence rate after surgical excision
1- Glomus tumor
2- Diffuse pigmented villonodular synovitis (PVNS)
3- Extra-abdominal fibromatosis
4- Schwannoma
5- Hemangioma
PREFERRED RESPONSE: 4- Schwannoma
Question 111 of 143
Most common soft-tissue tumor in childhood and infancy; may fluctuate in size with activity
1- Glomus tumor
2- Diffuse pigmented villonodular synovitis (PVNS)
3- Extra-abdominal fibromatosis
4- Schwannoma
5- Hemangioma
PREFERRED RESPONSE: 5- Hemangioma
DISCUSSION
Hemangiomas are common soft-tissue tumors that resemble the architecture of normal blood
vessels. They are the most common tumors seen during infancy and childhood and they can
be found in any tissue type. Larger, deep hemangiomas commonly cause pain with activity.
They may fluctuate in size and, if superficial enough, skin color changes may be noted.

PVNS is a locally aggressive proliferative disorder of the synovium. It can be found in the
joint, tendon sheath, or synovial bursa. It generally is found in 2 forms: localized or nodular
diffuse or villonodular. The diffuse form has a high local recurrence rate between 33% and
50%. The peak incidence is noted in people who are 20 to 50 years of age and it is more
common in women. Treatment is generally surgical, although radiation implants have been
used for recalcitrant cases.
A schwannoma (neurilemoma) is a common encapsulated nerve sheath tumor. Histologically,
it has 2 components: Antoni A (cellular regions) and Antoni B (loose myxoid regions). Like
most neural tumors, S-100 immunostain is strongly positive. As opposed to neurofibromas,
which are intraneural and seen commonly in patients with neurofibromatosis type I, these
lesions are located within the nerve sheath, more commonly occur as a solitary tumor, and are
generally easier to remove than neurofibromas. However, there is risk for nerve damage with
excision of any nerve sheath tumor, and for difficult locations or asymptomatic
Schwannomas, observation may be appropriate. The local recurrence rate is low with
marginal excision.
Extra-abdominal fibromatosis (desmoid tumor) is locally aggressive and can be found
superficially or deep. The deep variant tends to grow larger and faster. Local recurrence rates
can be high, but vary greatly on location, size, and histology, among other factors. Surgical
excision is the treatment of choice. External beam radiation and chemotherapy have been
used in recurrent disease or to treat regions that are unresectable. In some cases, fibromatoses
can mimic sarcomas, but these tumors do not have metastatic potential.
Glomus tumors are small, painful soft-tissue masses of smooth muscle origin typically in a
subungual location. They often cause moderate to severe pain from touch or cold.
RECOMMENDED READINGS
Bruder E, Alaggio R, Kozakewich HP, Jundt G, Dehner LP, Coffin CM. Vascular and perivascular lesions of skin and soft tissues in children and adolescents. Pediatr Dev Pathol. 2012;15(1 Suppl):26-61. doi: 10.2350/11-11-1119-PB.1. Review. PubMed PMID: 22420724.
View Abstract at PubMed
Coffin CM, Dehner LP. Pathologic evaluation of pediatric soft tissue tumors. Am J Clin Pathol. 1998 Apr;109(4 Suppl 1):S38-52. Review.
PubMed PMID: 9533748.
View Abstract at PubMed
Sheth S, Lai CK, Dry S, Binder S, Fishbein MC. Benign vascular tumors and tumor-like proliferations. Semin Diagn Pathol. 2008
Feb;25(1):1-16. Review. PubMed PMID: 18350917. View Abstract at PubMed
Mendenhall WM, Mendenhall CM, Reith JD, Scarborough MT, Gibbs CP, Mendenhall NP. Pigmented villonodular synovitis. Am J Clin Oncol. 2006 Dec;29(6):548-50. Review. PubMed PMID: 17148989.
View Abstract at PubMed
Molloy AP, Hutchinson B, O'Toole GC. Extra-abdominal desmoid tumours: a review of the literature. Sarcoma. 2012;2012:578052. doi:
10.1155/2012/578052. Epub 2012 Aug 16. PubMed PMID: 22966217.
View Abstract at PubMed
Rutenberg MS, Indelicato DJ, Knapik JA, Lagmay JP, Morris C, Zlotecki RA, Scarborough MT, Gibbs CP, Marcus RB. External-beam
radiotherapy for pediatric and young adult desmoid tumors. Pediatr Blood Cancer. 2011 Sep;57(3):435-42. doi: 10.1002/pbc.22916. Epub
2010 Dec 15. PubMed PMID: 21744472.
View Abstract at PubMed
Gombos Z, Zhang PJ. Glomus tumor. Arch Pathol Lab Med. 2008 Sep;132(9):1448-52. doi: 10.1043/1543-
2165(2008)132[1448:GT]2.0.CO;2. Review. PubMed PMID: 18788860.
View Abstract at PubMed

Figure 112a
Figure 112b
Figure 112c
Figure 112d
Figure 112e
Figure 112f
Question 112 of 143
Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man
who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial
and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in
Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
1- Secondary sarcoma in a pre-existing condition
2- Angiosarcoma
3- Metastatic lung carcinoma
4- Fibrous dysplasia
PREFERRED RESPONSE: 1- Secondary sarcoma in a pre-existing condition
DISCUSSION
The figures show an aggressive destructive lesion in a bone that is already involved with
Paget disease, and the pathology shows highly malignant cells. This represents a secondary
sarcoma arising in Pagetoid bone. Secondary sarcomas occurring in Pagetic bone include
malignant fibrous histiocytoma and chondrosarcomas, but osteosarcomas are the most
common malignancy in these patients. Most patients are older than age 60 and have new pain
in the setting of known Paget disease. The prognosis is generally poor because this is a very
aggressive sarcoma that is difficult to treat in an older population. Wide surgical removal and
chemotherapy are most commonly employed. The pathology does not show rudimentary
vessels or channels which are expected with angiosarcoma, effectively excluding that
diagnosis. A lack of nests or gland formation excludes metastatic lung carcinoma, and the
absence of fibrous stroma intermixed with bone islands or “Chinese characters” excludes
fibrous dysplasia.
RECOMMENDED READINGS
Deyrup AT, Montag AG, Inwards CY, Xu Z, Swee RG, Krishnan Unni K. Sarcomas arising in Paget disease of bone: a clinicopathologic
analysis of 70 cases. Arch Pathol Lab Med. 2007 Jun;131(6):942-6. PubMed PMID: 17550323.
View Abstract at PubMed
Mangham DC, Davie MW, Grimer RJ. Sarcoma arising in Paget's disease of bone: declining incidence and increasing age at presentation.
Bone. 2009 Mar;44(3):431-6. doi: 10.1016/j.bone.2008.11.002. Epub 2008 Nov 19. PubMed PMID: 19064007. View Abstract at PubMed

Figure 113a
Figure 113b
CLINICAL SITUATION FOR QUESTIONS 113 THROUGH 116
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in
his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a
lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was
made 1 year before this presentation. His lung cancer treatment consisted of partial
lobectomy and postsurgical radiation therapy.
Question 113 of 143
What is the preferred study to stage his disease at this time?
1- Whole-body bone scan
2- Chest/abdomen/pelvis CT scan
3- Bronchoscopy
4- Positron emission tomography (PET) scan
PREFERRED RESPONSE: 4- Positron emission tomography (PET) scan
Question 114 of 143
If this is a solitary metastasis, what is the preferred treatment?
1- Radiation therapy
2- Chemotherapy
3- Curettage, cementation, and internal fixation
4- Resection and prosthetic reconstruction
PREFERRED RESPONSE: 3- Curettage, cementation, and internal fixation
Question 115 of 143
Before receiving treatment, the patient falls and sustains a fracture through the base of the
femoral neck region; the best treatment now is

1- radiation therapy.
2- chemotherapy.
3- curettage, cementation, and internal fixation.
4- resection and prosthetic reconstruction.
PREFERRED RESPONSE: 4- resection and prosthetic reconstruction.
Question 116 of 143
Staging studies show no other lesions and surgical treatment is planned; when should a
biopsy be performed?
1- Before surgery
2- Intraoperatively after instrumentation
3- After surgery (reamings/curettings sent)
4- No biopsy is needed
PREFERRED RESPONSE: 1- Before surgery
DISCUSSION
Patients with a metastatic lung carcinoma are best staged and imaged with a PET scan.
Although many tumors are clinically evaluated with PET scans, metastatic lung cancer is one
of the few “approved” indications for PET imaging. This imaging modality is sensitive for
delineating the extent of disease and helpful for identifying areas that may also be at risk for
pathologic fracture. Stabilization of painful, lytic lesions in weight-bearing bones is
recommended to prevent pathologic fracture. Stabilization of an impending pathologic
fracture is generally easier than stabilization of a pathologic fracture; once the patient in this
vignette sustains a fracture, resection and reconstruction is indicated because stabilization
alone is unlikely to heal and poses high risk for failure. In cases of extreme bone loss,
especially in the epiphyseal region, reconstruction with tumor megaprostheses is desirable to
avoid mechanical failure of additional internal fixation. Patients with widely metastatic
disease may not be able to use ambulatory assistance aids effectively, placing traditional
internal fixation at risk for failure. Use of megaprostheses obviates the need for adjuvant
therapies to correct the loss of bone stock.
Radiation therapy alone to lesions that are radiosensitive is effective but does not alleviate the
risk for pathologic fracture. Chemotherapy alone is insufficient treatment for bone
metastases. Hormonal therapy is acceptable for treatment of hormone-sensitive tumors;
however, is not sufficient treatment for an impending pathologic fracture.
For patients with remote diagnoses of carcinoma, biopsy of new-onset presumed metastases
is mandatory to avoid an incorrect treatment regimen being employed. Patients can develop a
secondary malignancy or infection, both of which will require a different treatment regimen.
Biopsy should be done and diagnosis established either preoperatively or intraoperatively
prior to instrumentation (with frozen section analysis) to avoid contamination of the femoral
canal and soft-tissue envelope. Sending a specimen after instrumenting the femur or after

surgery contaminates the femur if a sarcoma is diagnosed and lessens the likelihood of limb
salvage.
RECOMMENDED READINGS
Clayer M, Duncan W. Importance of biopsy of new bone lesions in patients with previous carcinoma. Clin Orthop Relat Res. 2006
Oct;451:208-11. PubMed PMID: 16801861. View Abstract at PubMed
Damron TA, Sim FH. Surgical treatment for metastatic disease of the pelvis and the proximal end of the femur. Instr Course Lect. 2000;49:461-70. Review. PubMed PMID: 10829199.
View Abstract at PubMed
Capanna R, Campanacci DA. The treatment of metastases in the appendicular skeleton. J Bone Joint Surg Br. 2001 May;83(4):471-81.
Review. PubMed PMID: 11380113.
View Abstract at PubMed
Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat
Res. 1989 Dec;(249):256-64. PubMed PMID: 2684463. View Abstract at PubMed
Figure 117a
Figure 117b
Figure 117c
CLINICAL SITUATION FOR QUESTIONS 117 THROUGH 120
Figures 117a through 117c are the radiographs and MRI scan of a 16-year-old boy who has
had a persistent fullness in his thigh since being kicked while playing soccer 4 weeks ago. He
states that initially the area was painful, but now all symptoms other than the mass have
resolved.
Question 117 of 143
What is the most likely diagnosis?
1- Myositis ossificans
2- Juxtacortical osteogenic sarcoma

3- Osteochondroma
4- Cortical desmoid
PREFERRED RESPONSE: 3- Osteochondroma
Question 118 of 143
You explain to the patient and his parents that the lesion is
1- benign and simply can be observed with serial radiographs.
2- posttraumatic and should be allowed to mature prior to excision.
3- premalignant and should be immediately excised.
4- malignant and should be resected following neoadjuvant chemotherapy.
PREFERRED RESPONSE: 1- benign and simply can be observed with serial radiographs.
Question 119 of 143
A reliable indicator for the presence of malignancy in this scenario would be
1- loss of heterozygosity of the EXT-1 gene.
2- occurrence in a skeletally immature individual.
3- a cartilage cap of 1 cm.
4- growth beyond skeletal maturity.
PREFERRED RESPONSE: 4- growth beyond skeletal maturity.
Question 120 of 143
Findings of multiple lesions in multiple skeletal sites may be associated with
1- decreased risk for malignancy.
2- a characteristic chromosomal translocation.
3- soft-tissue hemangiomas.
4- limb deformity and short stature.
PREFERRED RESPONSE: 4- limb deformity and short stature.
DISCUSSION
This lesion is an osteochondroma. The finding on MRI scan or CT scan of a shared cortex
between the lesion and the host bone is pathognomonic. These lesions are benign and most
often can be followed with serial radiographs. Reasons to excise would be pain, unacceptable
cosmetic deformity, or growth, particularly if the patient is beyond skeletal maturity, which

can be a sign of malignancy. Loss of heterozygosity of either the EXT-1 locus or EXT-2
locus is associated with hereditary multiple exostoses (HME), which increases the risk for
malignant degeneration of 1 or more lesions throughout a patient’s life but does not always
lead to malignancy. Because HME affects all growth plates to some degree, short stature and
limb deformity may occur. A cartilage cap of up to 2 cm can be acceptable, particularly
during youth. If, however, this condition persists or enlarges beyond skeletal maturity,
excision should be entertained.
RECOMMENDED READINGS
Horvai A, Unni KK. Premalignant conditions of bone. J Orthop Sci. 2006 Jul;11(4):412-23. Review. PubMed PMID: 16897210.
View Abstract at PubMed
van der Eijken JW. Strategy in the treatment of benign bone tumors: an overview. J Pediatr Orthop B. 1998 Oct;7(4):249-52. Review.
PubMed PMID: 9810522. View Abstract at PubMed
Vlychou M, Athanasou NA. Radiological and pathological diagnosis of paediatric bone tumours and tumour-like lesions. Pathology. 2008 Feb;40(2):196-216. doi: 10.1080/00313020701813784. Review. PubMed PMID: 18203042.
View Abstract at PubMed
Figure 121a
Figure 121b
Figure 121c
Question 121 of 143
Figure 121a is the axial T1 MRI scan and Figure 121b is the coronal T1 MRI scan of an 85-
year-old man who has a mass in his medial thigh. The mass was present for years and
recently grew. His biopsy specimen is shown in Figure 121c. What is the best treatment for
this patient?
1- Chemotherapy and wide local resection
2- Wide local resection and radiotherapy
3- Marginal excision
4- Observation and reimaging in 6 months
PREFERRED RESPONSE: 2- Wide local resection and radiotherapy
DISCUSSION
The history of a long-standing mass with sudden growth suggests transformation of an
existing tumor. The imaging features of a fatty lesion with internal complexity suggest an
atypical lipomatous tumor (formerly called a well-differentiated liposarcoma). Juxtaposed to
this on imaging is a solid tumor. Histology reveals a high-grade spindle-cell sarcoma adjacent

to a fatty tumor. This clinical presentation is most consistent with a long-standing atypical
lipomatous tumor that has undergone dedifferentiation. The role of chemotherapy for soft-
tissue sarcomas is controversial and unlikely to be applicable in an 85-year-old man.
However, wide local excision with adjuvant radiation therapy is the best option for durable
local control. Marginal excision would be appropriate for an atypical lipomatous tumor that
has not undergone dedifferentiation. Observation of a high-grade sarcoma is not appropriate.
RECOMMENDED READINGS
Nascimento AG. Dedifferentiated liposarcoma. Semin Diagn Pathol. 2001 Nov;18(4):263-6. Review. PubMed PMID: 11757866
View Abstract at PubMed
Murphey MD, Arcara LK, Fanburg-Smith J. From the archives of the AFIP: imaging of musculoskeletal liposarcoma with radiologic-
pathologic correlation. Radiographics. 2005 Sep-Oct;25(5):1371-95. Review. PubMed PMID: 16160117. View Abstract at PubMed
Question 122 of 143
What tumor commonly metastasizes to regional lymph nodes?
1- Fibromyxoid sarcoma
2- Epithelioid sarcoma
3- Leiomyosarcoma
4- Liposarcoma
PREFERRED RESPONSE: 2- Epithelioid sarcoma
DISCUSSION
The common sarcomas that metastasize to regional lymph nodes are epithelioid sarcoma,
synovial sarcoma, angiosarcoma, rhabdomyosarcoma, and clear cell sarcoma. Metastasis to
the lungs remains the most common location for all sarcoma metastases. Daigeler and
associates evaluated regional lymph node metastasis (RLNM) and reported that the condition
was seen in 21.4% of patients with epithelioid sarcoma and 17.6% of patients with clear cell
sarcoma. Other sarcomas had RLNM rates below 10%.
RECOMMENDED READINGS
Daigeler A, Kuhnen C, Moritz R, Stricker I, Goertz O, Tilkorn D, Steinstraesser L, Steinau HU, Lehnhardt M. Lymph node metastases in
soft tissue sarcomas: a single center analysis of 1,597 patients. Langenbecks Arch Surg. 2009 Mar;394(2):321-9. doi: 10.1007/s00423-008-0371-x. Epub 2008 Jul 2. PubMed PMID: 18594854.
View Abstract at PubMed
Maduekwe UN, Hornicek FJ, Springfield DS, Raskin KA, Harmon DC, Choy E, Rosenberg AE, Nielsen GP, DeLaney TF, Chen YL, Ott
MJ, Yoon SS. Role of sentinel lymph node biopsy in the staging of synovial, epithelioid, and clear cell sarcomas. Ann Surg Oncol. 2009
May;16(5):1356-63. doi: 10.1245/s10434-009-0393-9. Epub 2009 Mar 4. PubMed PMID: 19259743. View Abstract at PubMed
Question 123 of 143
A 64-year-old woman has significant right arm pain associated with a destructive proximal
humeral bone lesion with an associated soft-tissue mass. Her medical history includes

carcinoma of the breast treated 8 years ago with modified radical mastectomy, hormone
receptor-based chemotherapy, and 45 Gy of radiation with 8 subsequent disease-free years.
Biopsy reveals a high-grade osteogenic sarcoma. What factor is most likely related to her
current disease?
1- Presence of metastatic disease
2- Dosage of radiation treatment
3- Type of prior surgical procedure
4- Type of chemotherapy given
PREFERRED RESPONSE: 2- Dosage of radiation treatment
DISCUSSION
Postradiation sarcomas are a rare subset of sarcomas (approximately 3% of all sarcomas),
with an incidence lower than 1% in patients receiving high-dose radiation. Diagnosis is
usually based on the following: differing histologic diagnoses between original and
secondary lesion, location within the field of radiation, latent period of more than 4 years, and
radiation doses higher than 40 Gy (although this level is controversial and no true threshold
exists). Chemotherapy is not related to postradiation sarcoma because the ionizing effect of
the radiation causes irreparable cell damage, leading to possible transformation in the future
to malignancies. Five-year survival from postradiation sarcoma is approximately 33%.
Complete surgical resection is the mainstay of treatment, with adjunctive chemotherapy used
in bone sarcomas or metastatic disease. Neither type of surgical procedure nor chemotherapy
has an impact on the development of postradiation sarcoma
RECOMMENDED READINGS
Inoue YZ, Frassica FJ, Sim FH, Unni KK, Petersen IA, McLeod RA. Clinicopathologic features and treatment of postirradiation sarcoma of
bone and soft tissue. J Surg Oncol. 2000 Sep;75(1):42-50. PubMed PMID: 11025461.
View Abstract at PubMed
Kalra S, Grimer RJ, Spooner D, Carter SR, Tillman RM, Abudu A. Radiation-induced sarcomas of bone: factors that affect outcome. J Bone
Joint Surg Br. 2007 Jun;89(6):808-13. PubMed PMID: 17613509. View Abstract at PubMed
Figure 124a
Figure 124b
Figure 124c
Question 124 of 143
Figures 124a and 124b are the MRI scans of a 25-year-old woman who has a painful mass in
her left gluteal and thigh region. Her biopsy specimen is seen in Figure 124c. What is the
most likely diagnosis?

1- Desmoid fibromatosis
2- Extraskeletal Ewing sarcoma
3- Metastatic breast cancer
4- Lymphoma
PREFERRED RESPONSE: 1- Desmoid fibromatosis
DISCUSSION
The imaging shows an infiltrative soft-tissue mass; histology demonstrates a bland spindle-
cell lesion without nuclear atypia consistent with desmoid tumor. Extraskeletal Ewing
sarcoma would be expected to have more surrounding edema and small round blue cells on
histology. Metastatic breast cancer and lymphoma can have similar appearances on MRI scan
but different characteristic histologies, the former with nests of malignant cells, and the latter
with small round blue cells.
RECOMMENDED READINGS
Robbin MR, Murphey MD, Temple HT, Kransdorf MJ, Choi JJ. Imaging of musculoskeletal fibromatosis. Radiographics. 2001 May-
Jun;21(3):585-600. Review. PubMed PMID: 11353108. View Abstract at PubMed
Molloy AP, Hutchinson B, O'Toole GC. Extra-abdominal desmoid tumours: a review of the literature. Sarcoma. 2012;2012:578052. doi: 10.1155/2012/578052. Epub 2012 Aug 16. PubMed PMID: 22966217.
View Abstract at PubMed
Figure 125a
Figure 125b
Figure 125c
CLINICAL SITUATION FOR QUESTIONS 125 THROUGH 128
A 45-year-old woman has increasing knee pain with activity and at rest. Her radiograph, MRI
scan, and histology are shown in Figures 125a through 125c.
Question 125 of 143
The best descriptor for the lesion seen in Figures 125a and 125b is

1- malignant.
2- benign.
3- benign aggressive.
4- inflammatory.
PREFERRED RESPONSE: 3- benign aggressive.
Question 126 of 143
The next appropriate step in staging is
1- biopsy.
2- skeletal survey.
3- whole-body bone scan
4- chest radiograph.
PREFERRED RESPONSE: 4- chest radiograph.
Question 127 of 143
Biopsy results are shown in Figure 125c. Treatment should consist of
1- extended intralesional curettage.
2- chemotherapy and intralesional resection.
3- chemotherapy and complete resection.
4- radiation and complete resection.
PREFERRED RESPONSE: 1- extended intralesional curettage.
Question 128 of 143
The cell that directly causes osteolysis in this lesion is
1- giant cell.
2- stromal cell.
3- osteoblast.
4- fibroblast.
PREFERRED RESPONSE: 1- giant cell.
DISCUSSION
This patient has a giant-cell tumor (GCT) of bone, a benign aggressive lesion. The lesion is
locally aggressive and destroys bone, but metastasizes rarely enough to be considered benign.

The metastatic rate of GCT is 5% or lower, and the metastatic disease most commonly
deposits in the lung, leading to the necessity for systemic staging of the chest. The histology
of a GCT shows large, multinucleated giant cells in a field of smaller stromal cells similar to
the nuclei of the giant cells. The osteoclast-like giant cells are directed through the receptor
activator of nuclear factor kappa-beta ligand pathway to induce lytic bone destruction seen in
this tumor, but the stromal cells are the neoplastic component. The preferred treatment is
complete extended intralesional curettage with high-speed burring and bone grafting or
cementation and fixation as individualized by patient and lesion.
RECOMMENDED READINGS
Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006 Jan;37(1):35-51. Review. PubMed PMID: 16311110.
View Abstract at PubMed
Kim Y, Nizami S, Goto H, Lee FY. Modern interpretation of giant cell tumor of bone: predominantly osteoclastogenic stromal tumor. Clin
Orthop Surg. 2012 Jun;4(2):107-16. doi: 10.4055/cios.2012.4.2.107. Epub 2012 May 17. Review. PubMed PMID: 22662295. View Abstract at PubMed
Thomas DM. RANKL, denosumab, and giant cell tumor of bone. Curr Opin Oncol. 2012 Jul;24(4):397-403. doi: 10.1097/CCO.0b013e328354c129. Review. PubMed PMID: 22581354.
View Abstract at PubMed
Figure 129a
Figure 129b
Figure 129c
Question 129 of 143
Figures 129a through 129c are the lateral radiograph of the sacrum, axial CT scan, and a
high-power view of a fine-needle biopsy of a 47-year-old man who has buttock pain and
constipation. A large mass is palpable on rectal examination. The tumor cell that is the
signature of this tumor is known as a(n)
1- giant cell.
2- physaliferous cell.
3- chondroblast.
4- adipocyte.
PREFERRED RESPONSE: 2- physaliferous cell.
DISCUSSION
The lateral radiograph and axial CT scan image of the sacrum reveal a destructive lesion in
S4 with a large soft-tissue mass. The differential includes chordoma, giant-cell tumor, and
sacral schwannoma. The images and histology are consistent with chordoma, a tumor usually
diagnosed during the fourth to eighth decades of life. The signature cell of the chordoma is

the physaliphorous cell, although these cells are not pathognomonic of chordoma. Other types
of tumors may have similar-appearing cells, and some chordomas may lack them.
Physaliphorous cells have a large single cytoplasmic vacuole that causes them to appear like
adipocytes. The extracellular stroma is myxoid, resembling chondrosarcoma.
RECOMMENDED READINGS
Nielsen GP, Rosenberg AE. Diagnostic Pathology: Bone. Manitoba, Canada: Amirsys; 2013:8.9-15.
Weber K. Malignant bone tumors. In: Lieberman JR, ed. AAOS Comprehensive Orthopaedic Review. Vol 1. Rosemont, IL: American
Academy of Orthopaedic Surgeons; 2009:417-442.
Figure 130a
Figure 130b
Figure 130c
Figure 130d
Question 130 of 143
Figures 130a through 130c show the CT scan and T1- and T2-weighted MRI scan sequences
of an otherwise healthy 67-year-old woman with progressive left groin pain. Her biopsy
specimen is shown in Figure 130d. Staging studies reveal no other lesions. Treatment should
include
1- radiotherapy.
2- chemotherapy followed by surgical resection.
3- curettage with adjuvant treatment and grafting.
4- en bloc resection.
PREFERRED RESPONSE: 4- en bloc resection.
DISCUSSION
The imaging studies reveal a pelvic chondrosarcoma with extraosseous extension, which is
confirmed by the biopsy specimen. En bloc resection is the treatment of choice for pelvic
chondrosarcomas. Although curettage may be used for select low-grade extremity lesions, it
is not recommended for pelvic lesions. As well, the imaging shows extraosseous extension
and the histology shows a higher-grade lesion (characteristics that make curettage unsuitable
in any skeletal location). Radiotherapy and chemotherapy do not play a role in nonmetastatic
chondrosarcoma.
RECOMMENDED READINGS
Hickey M, Farrokhyar F, Deheshi B, Turcotte R, Ghert M. A systematic review and meta-analysis of intralesional versus wide resection for
intramedullary grade I chondrosarcoma of the extremities. Ann Surg Oncol. 2011 Jun;18(6):1705-9. doi: 10.1245/s10434-010-1532-z. Epub 2011 Jan 22. Review. PubMed PMID: 21258968.
View Abstract at PubMed

Normand AN, Cannon CP, Lewis VO, Lin PP, Yasko AW. Curettage of biopsy-diagnosed grade 1 periacetabular chondrosarcoma. Clin
Orthop Relat Res. 2007 Jun;459:146-9. PubMed PMID: 17452919. View Abstract at PubMed
Figure 131a
Figure 131b
Figure 131c
Question 131 of 143
A lateral radiograph (Figure 131a), sagittal short tau inversion recovery MRI scan (Figure
131b), and an axial T1 contrast MRI scan (Figure 131c) were performed on a 15-year-old boy
who has injured his right knee twice during the last 5 months. He has a reduced range of
motion of the knee and posterior thigh tenderness. A biopsy showed bland spindle cells, giant
cells, and blood-filled spaces without endothelial lining. What is the most appropriate
treatment?
1- Chemotherapy and wide local excision
2- Chemotherapy and radiotherapy
3- Marginal excision
4- Extended intralesional curettage
PREFERRED RESPONSE: 4- Extended intralesional curettage
DISCUSSION
The imaging shows an aneurysmal bone cyst with a destructive, eccentric metaphyseal lesion
with fluid-fluid levels on MR imaging. The described histology confirms this. The
differential diagnosis would include telangiectactic osteosarcoma, although there is no
associated soft-tissue mass on imaging and no malignant stroma described on histology.
Treatment is extended intralesional curettage. Serial embolization is used in surgically
inaccessible spaces. Chemotherapy and/or radiotherapy are not indicated for this benign
lesion. Intralesional treatment rather than excision is the appropriate surgical option.
RECOMMENDED READINGS
Murphey MD, wan Jaovisidha S, Temple HT, Gannon FH, Jelinek JS, Malawer MM. Telangiectatic osteosarcoma: radiologic-pathologic
comparison. Radiology. 2003 Nov;229(2):545-53. Epub 2003 Sep 25. PubMed PMID: 14512511. View Abstract at PubMed
Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg. 2012 Apr;20(4):233-41. doi: 10.5435/JAAOS-20-04-233. Review. PubMed PMID: 22474093.
View Abstract at PubMed

Figure 132
CLINICAL SITUATION FOR QUESTIONS 132 THROUGH 134
Figure 132 is the bone scan of a 73-year-old man who is referred from his family doctor with
diffuse bone pain, fatigue, and right knee pain. Examination is notable for pain with motion
about the right knee and mild hyporeflexia.
Question 132 of 143
The most appropriate next step is
1- total spine MRI scan.
2- needle biopsy of the osseous lesion.
3- bone marrow biopsy.
4- CT scan of the chest, abdomen, and pelvis and laboratory studies.
PREFERRED RESPONSE: 4- CT scan of the chest, abdomen, and pelvis and laboratory
studies.
Question 133 of 143
During the course of evaluation, the patient develops a worsening mental status bordering on
stupor. His serum calcium level is 15.8 mg/dL (reference range, 8.5-10.1mg/dL). Treatment
should include

1- initiation of outpatient hemodialysis.
2- cardiac monitoring and fluid restriction.
3- intravenous bisphosphonate treatment.
4- intravenous vitamin D therapy.
PREFERRED RESPONSE: 3- intravenous bisphosphonate treatment.
Question 134 of 143
Further imaging shows pulmonary metastases without an obvious primary tumor of origin
and an incomplete fracture of the right distal femur. A decision is made to surgically treat his
distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for
this patient?
1- The distal femoral lesion should undergo needle biopsy first.
2- Bone marrow biopsy should be done first.
3- Preoperative biopsy is not necessary because a metastatic process is present.
4- Biopsy is not necessary if the lesion demonstrates a standardized uptake value (SUV)
greater than 3 on fluorodeoxyglucose positron emission tomography (PET) imaging.
PREFERRED RESPONSE: 3- Preoperative biopsy is not necessary because a metastatic
process is present.
DISCUSSION
This patient has widespread metastatic disease based on bone scan findings. According to a
study by Rougraff and associates, CT scan of the chest, abdomen, and pelvis and laboratory
studies will identify the primary site of disease in more than 85% of cases. When signs or
symptoms of spinal cord compression are absent, total spine MR imaging probably is not
needed. Biopsy alone is less accurate than staging in establishing a diagnosis. Bone marrow
biopsy is used only if a hematopoietic tumor (myeloma, lymphoma) is diagnosed.
Patients who develop hypercalcemia need hydration (with supplemental furosemide),
bisphosphonates, and evaluation for cardiac arrhythmia. Hemodialysis and vitamin D therapy
are not indicated, and fluid restriction would be contraindicated.
Biopsy before intervention for pathologic lower-extremity fracture likely is not needed in a
scenario with numerous bone lesions and pulmonary metastases. The absence of a clear
primary tumor of origin suggests this is unlikely to be a renal cell carcinoma for which
preoperative embolization would be considered before an intralesional procedure. Tissue
should be obtained at the time of surgery. Although an SUV greater than 3 is suspicious for
malignancy, activity on PET scan should not influence the need for biopsy in this scenario.
RECOMMENDED READINGS
Rougraff BT, Kneisl JS, Simon MA. Skeletal metastases of unknown origin. A prospective study of a diagnostic strategy. J Bone Joint Surg
Am. 1993 Sep;75(9):1276-81. PubMed PMID: 8408149.
View Abstract at PubMed

Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint
Surg Am. 2009 Jun;91(6):1518-30. Review. PubMed PMID: 19487533. View Abstract at PubMed
Figure 135a
Figure 135b
Figure 135c
Figure 135d
Figure 135e
Figure 135f
Question 135 of 143
Figures 135a through 135d are the radiographs, sagittal T1-, and coronal T2-weighted MRI
scans of a 22-year-old woman who has had pain in her right ankle for 6 months. Figures 135e
and 135f show a gross photograph of an amputated specimen and a biopsy specimen,
respectively. In this tumor, cytogenetics reveals which translocation?
1- t(12;22)(q13;q12-3)
2- t(X;18)(p11.2;q11.2)
3- t(11;22)(q24;q12)
4- t(1;3)(p36.3;q25)
PREFERRED RESPONSE: 4- t(1;3)(p36.3;q25)
DISCUSSION
The radiographs and MRI scans reveal a multicentric destructive process. Multicentric lesions
in adjacent bones suggest a vascular malignancy such as epithelioid hemangioendothelioma,
which is now included under the category of solitary fibrous tumors. Here, the tumor cells are
in cords within a myxoid stroma that resembles cartilaginous matrix. The translocation that
occurs in epithelioid hemangioendothelioma is t(1;3)(p36.3;q25). Clear cell sarcoma has been
shown to harbor t(12;22)(q13;q12-3), synovial sarcoma t(X;18)(p11.2;q11.2), and Ewing
sarcoma t(11;22)(q24;q12).
RECOMMENDED READINGS
Nielsen GP, Rosenberg AE. Diagnostic Pathology: Bone. Manitoba, Canada: Amirsys; 2013:11.17-21.
Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 5th ed. Philadelphia, PA: Elsevier; 2008:681-702, 945-988, 1161-1220.

Question 136 of 143
The optimal method to treat a recurrent presentation of pigmented villonodular synovitis
(PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic
effusions is
1- 700 cGy of radiation therapy.
2- open arthrotomy with synovectomy.
3- imatinib therapy.
4- observation.
PREFERRED RESPONSE: 2- open arthrotomy with synovectomy.
DISCUSSION
Local control of recurrent diffuse PVNS is best accomplished with open arthrotomy and
complete synovectomy. Arthroscopic methods in the setting of persistent diffuse PVNS are
associated with an unacceptably high rate of recurrence. Radiation therapy (700 cGy) is the
typical dose administered for heterotopic ossification prophylaxis, but this dose is not high
enough to achieve local control in PVNS. Imatinib, a colony-stimulating factor inhibitor, has
been described for recurrent/refractory disease, but is not considered as effective as open
surgical treatment.
RECOMMENDED READINGS
Tyler WK, Vidal AF, Williams RJ, Healey JH. Pigmented villonodular synovitis. J Am Acad Orthop Surg. 2006 Jun;14(6):376-85. Review.
PubMed PMID: 16757677.
View Abstract at PubMed
Heyd R, Micke O, Berger B, Eich HT, Ackermann H, Seegenschmiedt MH; German Cooperative Group on Radiotherapy for Benign
Diseases. Radiation therapy for treatment of pigmented villonodular synovitis: results of a national patterns of care study. Int J Radiat Oncol Biol Phys. 2010 Sep 1;78(1):199-204. doi: 10.1016/j.ijrobp.2009.07.1747. Epub 2010 May 18. PubMed PMID: 20488628.
View Abstract at PubMed
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E,
Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell
tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110.
View Abstract at PubMed

Figure 137a
Figure 137b
Question 137 of 143
The radiographs of a 63-year-old man with knee and proximal tibia discomfort are shown in
Figures 137a and 137b. What genetic abnormality is associated with this condition?
1- Fibrillin mutation
2- EXT 1 gene
3- p53 mutation
4- t(x;18)
PREFERRED RESPONSE: 2- EXT 1 gene
DISCUSSION
The radiographs reveal multiple osteochondromas consistent with multiple hereditary
exostoses. The EXT 1 and EXT 2 genes have been associated with this condition. The EXT 1
gene is located at 8q24 and the EXT 2 gene at 11 p11-p12, but additional linkage to
chromosomal locus 19p has suggested the existence of an as of yet unidentified EXT 3 gene.
Fibrillin mutations are associated with Marfan syndrome, p53 mutations with a variety of
malignancies, and t(x;18) with synovial sarcoma.
RECOMMENDED READINGS
Congenital and inherited bone conditions. In: Damron TA, ed. Orthopedic Surgery Essentials: Oncology and Basic Science. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:212-228.
Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis. 2008 Feb 13;3:3. doi: 10.1186/1750-1172-3-3. Review. PubMed PMID:
18271966.
View Abstract at PubMed
Bridge JA, Nelson M, Orndal C, Bhatia P, Neff JR. Clonal karyotypic abnormalities of the hereditary multiple exostoses chromosomal loci
8q24.1 (EXT1) and 11p11-12 (EXT2) in patients with sporadic and hereditary osteochondromas. Cancer. 1998 May 1;82(9):1657-63.
PubMed PMID: 9576285.
View Abstract at PubMed
RESPONSES FOR QUESTIONS 138 THROUGH 143

1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
Match the descriptions below to the conditions listed above.
Question 138 of 143
Often associated with the shortest mean survival once it is metastatic to bone and solid organs
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
PREFERRED RESPONSE: 4- Adenocarcinoma of the lung
Question 139 of 143
Advanced disease including bone metastases is treated with vascular endothelial growth
factor (VEGF) inhibitors (ie, sunitinib) and, typically, the lesions are radioresistant.
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
PREFERRED RESPONSE: 6- Renal cell carcinoma
Question 140 of 143
Often treated with bisphosphonates and radioiodine in the setting of metastatic bone disease
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma

PREFERRED RESPONSE: 5- Thyroid cancer
Question 141 of 143
Frequently involves mixed osteolytic and osteoblastic metastatic bone disease that typically is
less responsive to treatment if the patient is human epidermal growth factor receptor 2 (HER-
2)-positive
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
PREFERRED RESPONSE: 3- Adenocarcinoma of the breast
Question 142 of 143
Classically known for predominantly osteoblastic metastatic bone disease in male patients
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
PREFERRED RESPONSE: 2- Prostate cancer
RESPONSES FOR QUESTIONS 138 THROUGH 143
1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
Match the descriptions below to the conditions listed above.
Question 143 of 143
A small round blue-cell neoplasm of plasma cells responsive to chemotherapy and radiation

1- Multiple myeloma
2- Prostate cancer
3- Adenocarcinoma of the breast
4- Adenocarcinoma of the lung
5- Thyroid cancer
6- Renal cell carcinoma
PREFERRED RESPONSE: 1- Multiple myeloma
DISCUSSION
Metastatic bone disease is a common phenomenon. The 5 most common primary cancers that
spread to bone are breast, lung, thyroid, kidney, and prostate (commonly remembered with
the easy pneumonic BLT with a Kosher Pickle). Radiologically, lung, thyroid, and kidney
cancers are mostly radiolucent, prostate cancer classically shows osteoblastic changes, and
breast cancer demonstrates a mix. Lung cancer in general is associated with the shortest mean
survival among the primary carcinomas listed once the disease is metastatic to multiple
locations including bone. Patients generally survive less than 1 year after diagnosis.
Metastatic renal cell carcinoma has a poor prognosis, but a small subset of patients can
survive for years. Newer drugs such as VEGF inhibitors have shown in select cases to be
effective, presumably by diminishing blood supply to these vascular tumors. These tumors
are often radioresistant, making them difficult to control with nonsurgical measures. Thyroid
cancer that has spread to bone is treated like most metastatic bone cancer. Bisphosphonates
are used to help reduce bone pain and decrease risk for pathologic fracture. However,
radioiodine is often used as targeted therapy. Prostate cancer that metastasizes to bone is best
known for its classic osteoblastic lesions. However, it is important to note that this is not
always the case. Whole-body bone scans often show intense uptake at the site of the
metastatic lesions in patients with prostate cancer, as opposed to those with renal cell
carcinoma or multiple myeloma, who often demonstrate little bony reaction and have a
“cold” scan. Multiple myeloma is a primary cancer of the bone marrow. It is classified as a
small round blue-cell tumor histopathologically and is generally responsive to chemotherapy
and radiation. Metastatic breast cancer often features lesions that are mixed radiolucent and
osteoblastic. The response to treatment is often dictated by tumor cell surface markers.
Typically, the most responsive tumors are estrogen and progesterone receptor positive and
HER-2 negative. HER-2-positive tumors denote a more aggressive and difficult to treat
subset of cancer.
RECOMMENDED READINGS
Biermann JS, Holt GE, Lewis VO, Schwartz HS, Yaszemski MJ. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint Surg Am. 2009 Jun;91(6):1518-30. Review. PubMed PMID: 19487533.
View Abstract at PubMed
Lewis VO. What's new in musculoskeletal oncology. J Bone Joint Surg Am. 2009 Jun;91(6):1546-56. doi: 10.2106/JBJS.I.00375. Review.
PubMed PMID: 19487537.
View Abstract at PubMed
Schmidinger M, Larkin J, Ravaud A. Experience with sunitinib in the treatment of metastatic renal cell carcinoma. Ther Adv Urol. 2012
Oct;4(5):253-65. PubMed PMID: 23024706. View Abstract at PubMed
Rossi A, Gridelli C, Ricciardi S, de Marinis F. Bone metastases and non-small cell lung cancer: from bisphosfonates to targeted therapy. Curr Med Chem. 2012 Nov 1;19(32):5524-35. PubMed PMID: 22963665.
View Abstract at PubMed

Lopez-Olivo MA, Shah NA, Pratt G, Risser JM, Symanski E, Suarez-Almazor ME. Bisphosphonates in the treatment of patients with lung
cancer and metastatic bone disease: a systematic review and meta-analysis. Support Care Cancer. 2012 Nov;20(11):2985-98. doi: 10.1007/s00520-012-1563-z. Epub 2012 Sep 7. PubMed PMID: 22956190.
View Abstract at PubMed
This is the last question of the exam.