Embed Size (px)
Citation preview
1
The A&M System Annual Enrollment period is taking place from July 1 – July 31, 2014. As an A&M System COBRA Participant, you have the opportunity during this time to make plan changes, enroll in, and/or add dependents to medical, dental, and vision coverage for the upcoming plan year. If you are enrolled in health coverage through Academic HealthPlans, you will get information directly from them regarding your health coverage. Coverage elections or changes will be effective September 1, 2014 and continue for the next year or remainder of your original COBRA eligibility period, whichever period is shorter. No action is required if you do not want to make any changes to the COBRA coverage you currently have; however, please read the benefit changes below for some important information.
Instructions:1. Review the enclosed Personal Benefit Summary.2. Review this brochure for the rates and changes effective September 1, 2014.3. You can make changes to your COBRA coverage on the Personal Benefit Summary.4. If you make changes, return your completed Personal Benefit Summary to the return address on the Personal
Benefits Summary letter no later than July 31st.
Benefit Changes for Plan Year 2014-2015
A&M Care Plan• The coinsurance for the A&M Care Plan is changing from 30% to 20%; the plan will pay 80%, up from
70%.• Office visit copays will be included in the $5,000 annual out-of-pocket maximum.• There will be small changes in the monthly premium costs for members enrolled in the A&M Care Plan in
all categories.
For more information about the plans and provider networks, visit the Benefits Administration webpage at http://www.tamus.edu/benefits/. More Annual Enrollment information is available online at: http://www.tamus.edu/offices/benefits/annual-enrollment/.
2014-2015Annual Enrollment
for COBRA Participants
2
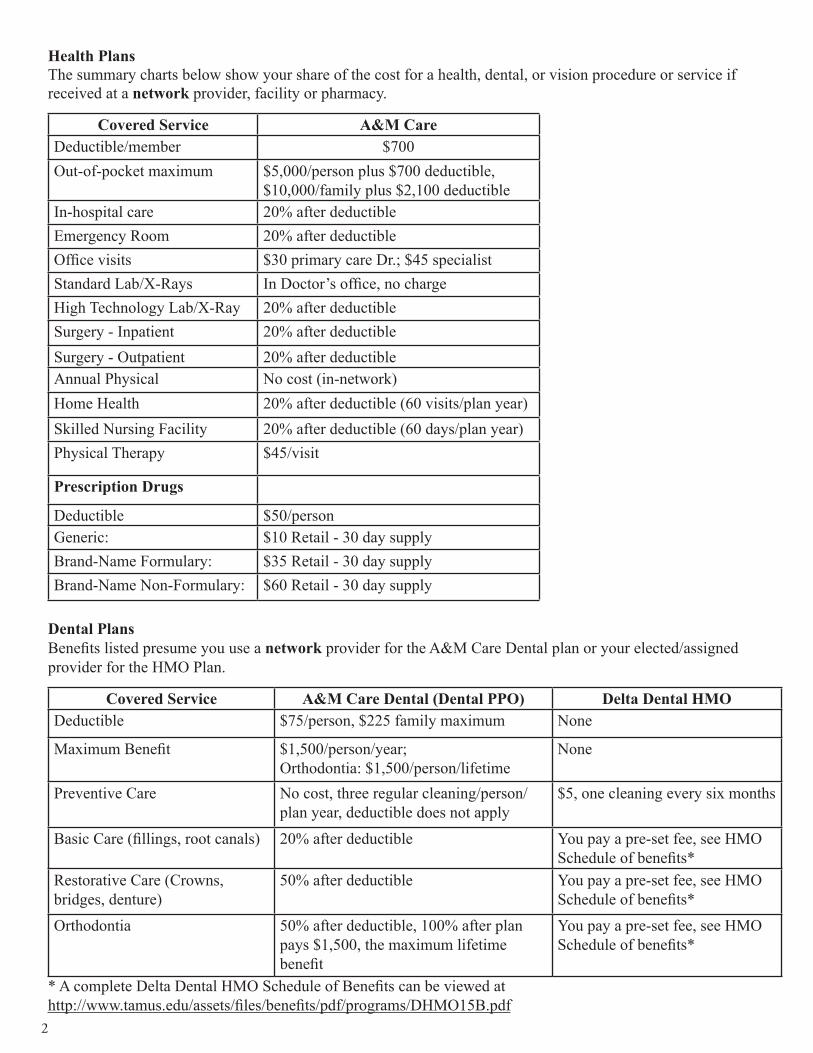
Health Plans The summary charts below show your share of the cost for a health, dental, or vision procedure or service if received at a network provider, facility or pharmacy.
Covered Service A&M CareDeductible/member $700Out-of-pocket maximum $5,000/person plus $700 deductible,
$10,000/family plus $2,100 deductibleIn-hospital care 20% after deductibleEmergency Room 20% after deductibleOffice visits $30 primary care Dr.; $45 specialistStandard Lab/X-Rays In Doctor’s office, no chargeHigh Technology Lab/X-Ray 20% after deductibleSurgery - Inpatient 20% after deductibleSurgery - Outpatient 20% after deductibleAnnual Physical No cost (in-network)Home Health 20% after deductible (60 visits/plan year)Skilled Nursing Facility 20% after deductible (60 days/plan year)Physical Therapy $45/visit
Prescription Drugs
Deductible $50/personGeneric: $10 Retail - 30 day supplyBrand-Name Formulary: $35 Retail - 30 day supplyBrand-Name Non-Formulary: $60 Retail - 30 day supply
Dental PlansBenefits listed presume you use a network provider for the A&M Care Dental plan or your elected/assigned provider for the HMO Plan.
Covered Service A&M Care Dental (Dental PPO) Delta Dental HMODeductible $75/person, $225 family maximum None
Maximum Benefit $1,500/person/year;Orthodontia: $1,500/person/lifetime
None
Preventive Care No cost, three regular cleaning/person/plan year, deductible does not apply
$5, one cleaning every six months
Basic Care (fillings, root canals) 20% after deductible You pay a pre-set fee, see HMO Schedule of benefits*
Restorative Care (Crowns, bridges, denture)
50% after deductible You pay a pre-set fee, see HMO Schedule of benefits*
Orthodontia 50% after deductible, 100% after plan pays $1,500, the maximum lifetime benefit
You pay a pre-set fee, see HMO Schedule of benefits*
* A complete Delta Dental HMO Schedule of Benefits can be viewed athttp://www.tamus.edu/assets/files/benefits/pdf/programs/DHMO15B.pdf

3
COBRA Continuation PremiumsPlan Participant
OnlyParticipant & Spouse
Participant & Child(ren)
Participant & Family
A&M Care * $523.41 $1,036.39 $882.51 $1,241.56Dental PPO $ 30.00 $ 60.00 $ 63.00 $ 95.99DentalCare USA (HMO) $ 21.65 $ 38.52 $ 38.81 $ 60.30EyeMed Vision Care $ 6.45 $ 13.71 $ 10.59 $ 18.87
Covered Service EyeMedEye Exam One per plan year, $10 copaymentMaterials $15 co-pay for frames and lenses, every other plan year for eyeglass lenses, one stan-
dard pair every plan yearFrame Allowance $130 allowance, 20% off balance over $130Contact Lens Fit and follow-up
Once every plan year, in place of eyeglass benefit. Standard Contact Lens - $0 copay, paid in full and two follow up visits. Premium Contact Lens - $0 copay, 10% off retail price, $40 allowance.
Contact Lens Allowance
Conventional - $0 copay, $150 allowance, 15% off balance over $150 Disposable - $0 copay, $150 allowance
* Remember that the A&M Care plan has an additional monthly charge of $30 for an individual, $30 for a covered spouse, and $30 for one or more covered children who use tobacco products.
Carrier Phone Numbers and Websites
BlueCross BlueShield A&M Care 1-866-295-1212 http://www.bcbstx.com/Delta Dental - A&M Dental 1-800-336-8264 http://www.deltadentalins.com/tamus/
DeltaCare USA Dental HMO 1-800-422-4234 http://www.deltadentalins.com/tamus/
EyeMed Vision Care 1-855-862-4300 http://www.eyemed.com
Express Scripts - A&M Care Drug Program
1-866-544-6970 http://www.express-scripts.com/
Vision PlanBenefits listed presume you use a network provider, however some benefits are available for using non-network providers. If you use a non-network provider, you will need to file a claim to be reimbursed.
For more details on the Vision plan visit: https://www.tamus.edu/offices/benefits/employee-retiree-benefits/vision/.
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
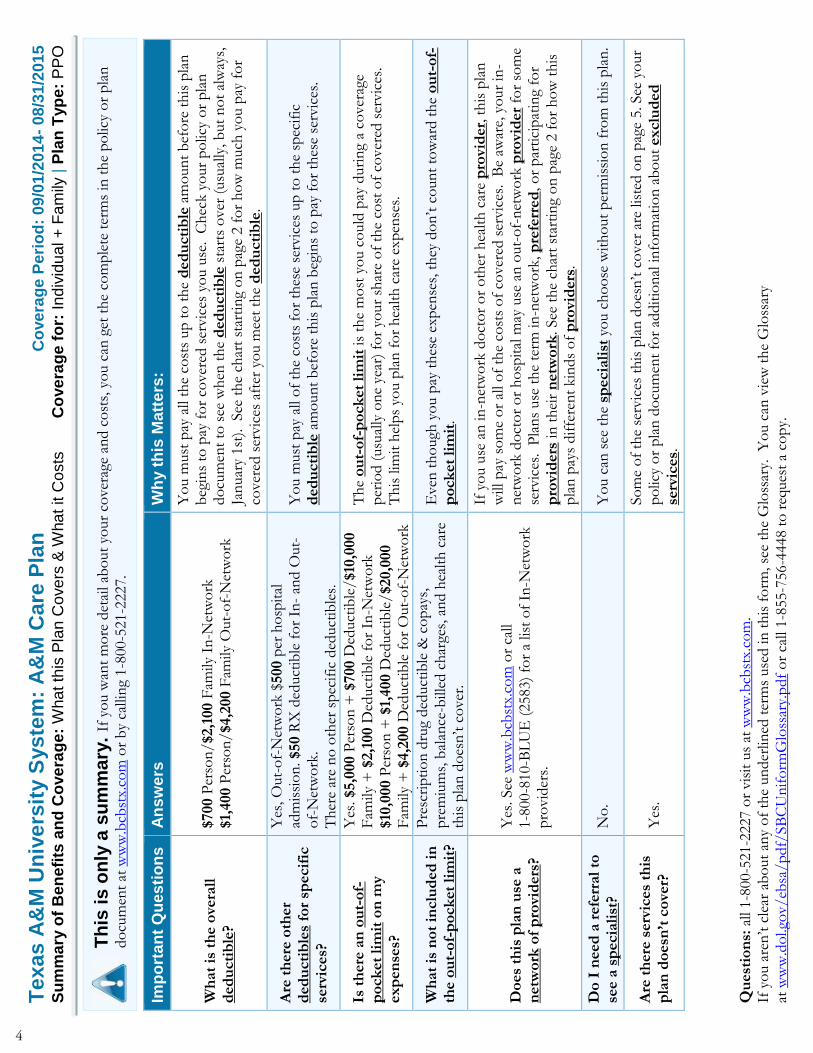
Th
is i
s o
nly
a s
um
ma
ry.
If y
ou w
ant
mo
re d
etai
l ab
out
your
cover
age
and c
ost
s, y
ou c
an g
et t
he
com
ple
te t
erm
s in
th
e p
olic
y o
r p
lan
do
cum
ent
at w
ww
.bcb
stx.
com
or
by
calli
ng
1-8
00-5
21-2
227.
Imp
ort
an
t Q
ues
tio
ns
An
sw
ers
W
hy t
his
Matt
ers
:
Wh
at
is t
he o
vera
ll
ded
ucti
ble
?
$700 P
erso
n/$2,1
00 F
amily
In
-Net
wo
rk
$1,
400 P
erso
n/$4,2
00 F
amily
Out-
of-
Net
wo
rk
Yo
u m
ust
pay
all
the
cost
s up
to
th
e d
ed
ucti
ble
am
oun
t b
efo
re t
his
pla
n
beg
ins
to p
ay f
or
cover
ed s
ervic
es y
ou u
se. C
hec
k y
our
po
licy
or
pla
n
do
cum
ent
to s
ee w
hen
th
e d
ed
ucti
ble
sta
rts
over
(usu
ally
, b
ut
no
t al
way
s,
Jan
uar
y 1st
). See
th
e ch
art
star
tin
g o
n p
age
2 f
or
ho
w m
uch
yo
u p
ay f
or
cover
ed s
ervic
es a
fter
yo
u m
eet
the
ded
ucti
ble
.
Are
th
ere
oth
er
ded
ucti
ble
s fo
r sp
ecif
ic
serv
ices?
Yes
, O
ut-
of-
Net
wo
rk $
500 p
er h
osp
ital
ad
mis
sio
n. $50 R
X d
educt
ible
fo
r In
- an
d O
ut-
of-
Net
wo
rk.
Th
ere
are
no
oth
er s
pec
ific
ded
uct
ible
s.
Yo
u m
ust
pay
all
of
the
cost
s fo
r th
ese
serv
ices
up
to
th
e sp
ecif
ic
ded
ucti
ble
am
oun
t b
efo
re t
his
pla
n b
egin
s to
pay
fo
r th
ese
serv
ices
.
Is t
here
an
ou
t-o
f-p
ock
et
lim
it o
n m
y
exp
en
ses?
Yes
. $5,0
00 P
erso
n +
$700 D
educt
ible
/$10
,000
Fam
ily +
$2,1
00 D
educt
ible
fo
r In
-Net
wo
rk
$10
,000 P
erso
n +
$1,
400 D
educt
ible
/$20,0
00
Fam
ily +
$4,2
00 D
educt
ible
fo
r O
ut-
of-
Net
wo
rk
Th
e o
ut-
of-
po
ck
et
lim
it is
the
mo
st y
ou c
ould
pay
duri
ng
a co
ver
age
per
iod (
usu
ally
on
e ye
ar)
for
your
shar
e o
f th
e co
st o
f co
ver
ed s
ervic
es.
Th
is lim
it h
elp
s yo
u p
lan
fo
r h
ealt
h c
are
expen
ses.
Wh
at
is n
ot
inclu
ded
in
th
e o
ut-
of-
po
ck
et
lim
it?
Pre
scri
pti
on
dru
g ded
uct
ible
& c
op
ays,
p
rem
ium
s, b
alan
ce-b
illed
ch
arge
s, a
nd h
ealt
h c
are
this
pla
n d
oes
n’t
co
ver
.
Even
th
ough
yo
u p
ay t
hes
e ex
pen
ses,
th
ey d
on
’t c
oun
t to
war
d t
he
ou
t-o
f-p
ock
et
lim
it.
Do
es
this
pla
n u
se a
n
etw
ork
of
pro
vid
ers
?
Yes
. See
ww
w.b
cbst
x.co
m o
r ca
ll 1-8
00-8
10-B
LU
E (
2583)
for
a lis
t o
f In
-Net
wo
rk
pro
vid
ers.
If y
ou u
se a
n in
-net
wo
rk d
oct
or
or
oth
er h
ealt
h c
are
pro
vid
er,
th
is p
lan
w
ill p
ay s
om
e o
r al
l o
f th
e co
sts
of
cover
ed s
ervic
es. B
e aw
are,
yo
ur
in-
net
wo
rk d
oct
or
or
ho
spit
al m
ay u
se a
n o
ut-
of-
net
wo
rk p
rovi
der
for
som
e se
rvic
es. P
lan
s use
th
e te
rm in
-net
wo
rk, p
refe
rred
, o
r p
arti
cip
atin
g fo
r p
rovi
ders
in
th
eir
netw
ork
. See
th
e ch
art
star
tin
g o
n p
age
2 f
or
ho
w t
his
p
lan
pay
s dif
fere
nt
kin
ds
of
pro
vid
ers
.
Do
I n
eed
a r
efe
rral
to
see a
sp
ecia
list
? N
o.
Yo
u c
an s
ee t
he
specia
list
yo
u c
ho
ose
wit
ho
ut
per
mis
sio
n f
rom
th
is p
lan
.
Are
th
ere
serv
ices
this
p
lan
do
esn
’t c
ove
r?
Yes
. So
me
of
the
serv
ices
th
is p
lan
do
esn
’t c
over
are
lis
ted o
n p
age
5. See
yo
ur
po
licy
or
pla
n d
ocu
men
t fo
r ad
dit
ion
al in
form
atio
n a
bo
ut
exclu
ded
se
rvic
es.
4
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
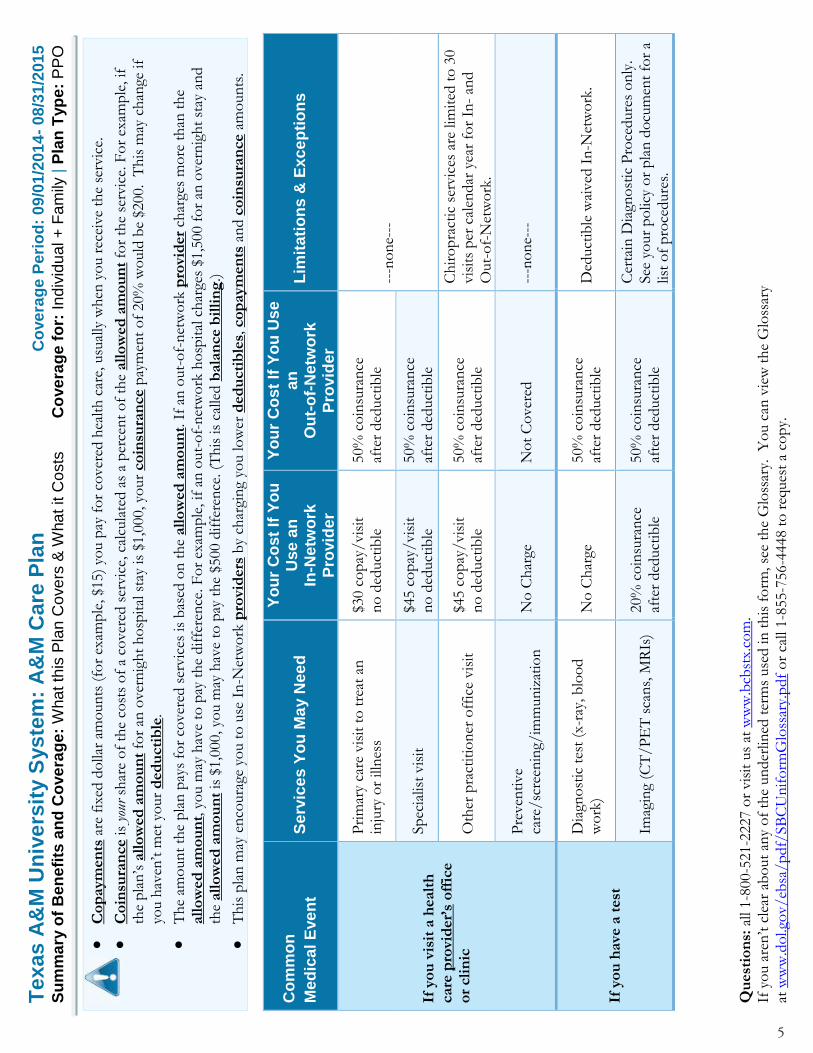
Co
paym
en
ts a
re f
ixed
do
llar
amo
un
ts (
for
exam
ple
, $1
5)
you p
ay f
or
cover
ed h
ealt
h c
are,
usu
ally
when
yo
u r
ecei
ve
the
serv
ice.
Co
insu
ran
ce is
your
sh
are
of
the
cost
s o
f a
cover
ed s
ervic
e, c
alcu
late
d a
s a
per
cen
t o
f th
e all
ow
ed
am
ou
nt
for
the
serv
ice.
Fo
r ex
amp
le, if
th
e p
lan
’s a
llo
wed
am
ou
nt
for
an o
ver
nig
ht
ho
spit
al s
tay
is $
1,0
00, yo
ur
co
insu
ran
ce p
aym
ent
of
20%
wo
uld
be
$200. T
his
may
ch
ange
if
you h
aven
’t m
et y
our
ded
ucti
ble
.
Th
e am
oun
t th
e p
lan
pay
s fo
r co
ver
ed s
ervic
es is
bas
ed o
n t
he
all
ow
ed
am
ou
nt.
If
an o
ut-
of-
net
wo
rk p
rovi
der
char
ges
mo
re t
han
th
e all
ow
ed
am
ou
nt,
yo
u m
ay h
ave
to p
ay t
he
dif
fere
nce
. F
or
exam
ple
, if
an
ou
t-o
f-n
etw
ork
ho
spit
al c
har
ges
$1,5
00 f
or
an o
ver
nig
ht
stay
an
d
the
all
ow
ed
am
ou
nt
is $
1,0
00, yo
u m
ay h
ave
to p
ay t
he
$500 d
iffe
ren
ce. (T
his
is
calle
d b
ala
nce b
illi
ng
.)
Th
is p
lan
may
en
coura
ge y
ou t
o u
se I
n-N
etw
ork
pro
vid
ers
by
char
gin
g yo
u lo
wer
ded
ucti
ble
s, c
op
aym
en
ts a
nd c
oin
sura
nce a
mo
un
ts.
Co
mm
on
Me
dic
al E
ve
nt
Se
rvic
es
Yo
u M
ay N
ee
d
Yo
ur
Co
st
If Y
ou
U
se
an
In
-Netw
ork
P
rovid
er
Yo
ur
Co
st
If Y
ou
Us
e
an
O
ut-
of-
Ne
two
rk
Pro
vid
er
Lim
itati
on
s &
Exc
ep
tio
ns
If y
ou
vis
it a
healt
h
care
pro
vid
er’
s o
ffic
e
or
cli
nic
Pri
mar
y ca
re v
isit
to
tre
at a
n
inju
ry o
r ill
nes
s $3
0 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Sp
ecia
list
vis
it
$45 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
Oth
er p
ract
itio
ner
off
ice
vis
it
$45 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
Ch
iro
pra
ctic
ser
vic
es a
re lim
ited
to
30
vis
its
per
cal
endar
yea
r fo
r In
- an
d
Out-
of-
Net
wo
rk.
Pre
ven
tive
care
/sc
reen
ing/
imm
un
izat
ion
N
o C
har
ge
No
t C
over
ed
---n
on
e---
If y
ou
have
a t
est
Dia
gno
stic
tes
t (x
-ray
, b
loo
d
wo
rk)
No
Ch
arge
50%
co
insu
ran
ce
afte
r ded
uct
ible
D
educt
ible
wai
ved
In
-Net
wo
rk.
Imag
ing
(CT
/P
ET
sca
ns,
MR
Is)
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
Cer
tain
Dia
gno
stic
Pro
cedure
s o
nly
. See
yo
ur
po
licy
or
pla
n d
ocu
men
t fo
r a
list
of
pro
cedure
s.
5

Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
Co
mm
on
Me
dic
al E
ve
nt
Se
rvic
es
Yo
u M
ay N
ee
d
Yo
ur
Co
st
If Y
ou
U
se
an
In
-Netw
ork
P
rovid
er
Yo
ur
Co
st
If Y
ou
Us
e
an
O
ut-
of-
Ne
two
rk
Pro
vid
er
Lim
itati
on
s &
Exc
ep
tio
ns
If y
ou
need
dru
gs
to
treat
yo
ur
illn
ess
or
co
nd
itio
n
Mo
re in
form
atio
n a
bo
ut
pre
scri
pti
on
dru
g
co
vera
ge is
avai
lab
le a
t w
ww
.exp
ress
scri
pts
.co
m
Gen
eric
dru
gs
Ret
ail:
$10 c
op
ay/
p
resc
rip
tio
n a
fter
$50
ded
uct
ible
M
ail:
$20 c
op
ay/
p
resc
rip
tio
n a
fter
$50
ded
uct
ible
To
tal co
st o
f p
resc
rip
tio
n
at t
he
tim
e o
f se
rvic
e. 7
5%
o
f al
low
able
,ch
arge
s ar
e re
imb
urs
ed a
fter
ap
plic
able
co
pay
men
t
Ret
ail:
one
cop
ay p
er 3
0 d
ay s
up
ply
M
ail:
two
co
pay
s up
to
90 d
ay s
up
ply
Pre
ferr
ed b
ran
d d
rugs
Ret
ail:
$35 c
op
ay/
p
resc
rip
tio
n a
fter
$50
ded
uct
ible
M
ail:
$70 c
op
ay/
p
resc
rip
tio
n a
fter
$50
ded
uct
ible
To
tal co
st o
f p
resc
rip
tio
n
at t
he
tim
e o
f se
rvic
e. 7
5%
o
f al
low
able
,ch
arge
s ar
e re
imb
urs
ed a
fter
ap
plic
able
co
pay
men
t
Ret
ail:
one
cop
ay p
er 3
0 d
ay s
up
ply
M
ail:
two
co
pay
s up
to
90 d
ay s
up
ply
No
n-p
refe
rred
bra
nd d
rugs
Ret
ail:
$60 c
op
ay/
p
resc
rip
tio
n a
fter
$50
ded
uct
ible
M
ail:
$120 c
opay
/
pre
scri
pti
on
aft
er $
50
ded
uct
ible
To
tal co
st o
f p
resc
rip
tio
n
at t
he
tim
e o
f se
rvic
e. 7
5%
o
f al
low
able
,ch
arge
s ar
e re
imb
urs
ed a
fter
ap
plic
able
co
pay
men
t
Ret
ail:
one
cop
ay p
er 3
0 d
ay s
up
ply
M
ail:
two
co
pay
s up
to
90 d
ay s
up
ply
Sp
ecia
lty
dru
gs
Gen
eric
$10 c
opay
P
refe
rred
$35 c
op
ay
No
n-p
refe
rred
$60
cop
ay/
afte
r $5
0 d
educt
ible
To
tal co
st o
f p
resc
rip
tio
n
at t
he
tim
e o
f se
rvic
e. 7
5%
o
f al
low
able
,ch
arge
s ar
e re
imb
urs
ed a
fter
ap
plic
able
co
pay
men
t
Beg
inn
ing
wit
h s
eco
nd f
ill s
pec
ialt
y m
edic
atio
n m
ust
be
fille
d t
hro
ugh
Sp
ecia
lty
Ph
arm
acy:
on
e co
pay
men
t p
er 3
0 d
ay s
up
ply
If y
ou
have
ou
tpati
en
t su
rgery
Fac
ilit
y fe
e (e
.g.,
amb
ula
tory
su
rger
y ce
nte
r)
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Ph
ysic
ian
/su
rgeo
n f
ees
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
6
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
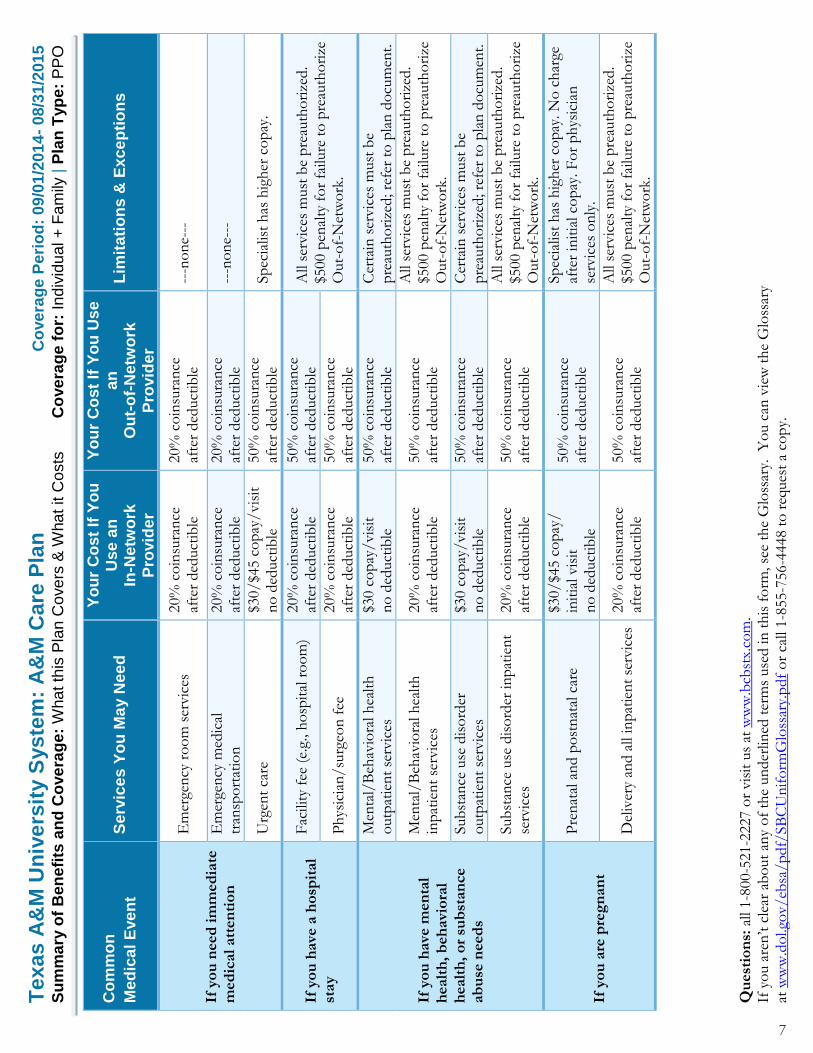
Co
mm
on
Me
dic
al E
ve
nt
Se
rvic
es
Yo
u M
ay N
ee
d
Yo
ur
Co
st
If Y
ou
U
se
an
In
-Netw
ork
P
rovid
er
Yo
ur
Co
st
If Y
ou
Us
e
an
O
ut-
of-
Ne
two
rk
Pro
vid
er
Lim
itati
on
s &
Exc
ep
tio
ns
If y
ou
need
im
med
iate
m
ed
ical
att
en
tio
n
Em
erge
ncy
ro
om
ser
vic
es
20%
co
insu
ran
ce
afte
r ded
uct
ible
20%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Em
erge
ncy
med
ical
tr
ansp
ort
atio
n
20%
co
insu
ran
ce
afte
r ded
uct
ible
20%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Urg
ent
care
$3
0/$4
5 c
opay
/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
Sp
ecia
list
has
hig
her
co
pay
.
If y
ou
have
a h
osp
ital
stay
Fac
ilit
y fe
e (e
.g.,
ho
spit
al r
oo
m)
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
A
ll se
rvic
es m
ust
be
pre
auth
ori
zed.
$500 p
enal
ty f
or
failu
re t
o p
reau
tho
rize
O
ut-
of-
Net
wo
rk.
Ph
ysic
ian
/su
rgeo
n f
ee
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
If y
ou
have
men
tal
healt
h,
beh
avi
ora
l h
ealt
h,
or
sub
stan
ce
ab
use
need
s
Men
tal/
Beh
avio
ral h
ealt
h
outp
atie
nt
serv
ices
$3
0 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
C
erta
in s
ervic
es m
ust
be
pre
auth
ori
zed; re
fer
to p
lan
do
cum
ent.
Men
tal/
Beh
avio
ral h
ealt
h
inp
atie
nt
serv
ices
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
All
serv
ices
must
be
pre
auth
ori
zed.
$500 p
enal
ty f
or
failu
re t
o p
reau
tho
rize
O
ut-
of-
Net
wo
rk.
Sub
stan
ce u
se d
iso
rder
o
utp
atie
nt
serv
ices
$3
0 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
C
erta
in s
ervic
es m
ust
be
pre
auth
ori
zed; re
fer
to p
lan
do
cum
ent.
Sub
stan
ce u
se d
iso
rder
in
pat
ien
t se
rvic
es
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
All
serv
ices
must
be
pre
auth
ori
zed.
$500 p
enal
ty f
or
failu
re t
o p
reau
tho
rize
O
ut-
of-
Net
wo
rk.
If y
ou
are
pre
gn
an
t
Pre
nat
al a
nd p
ost
nat
al c
are
$30/$4
5 c
opay
/
init
ial vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
Sp
ecia
list
has
hig
her
co
pay
. N
o c
har
ge
afte
r in
itia
l co
pay
. F
or
ph
ysic
ian
se
rvic
es o
nly
.
Del
iver
y an
d a
ll in
pat
ien
t se
rvic
es
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
All
serv
ices
must
be
pre
auth
ori
zed.
$500 p
enal
ty f
or
failu
re t
o p
reau
tho
rize
O
ut-
of-
Net
wo
rk.
7
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
Co
mm
on
Me
dic
al E
ve
nt
Se
rvic
es
Yo
u M
ay N
ee
d
Yo
ur
Co
st
If Y
ou
U
se
an
In
-Netw
ork
P
rovid
er
Yo
ur
Co
st
If Y
ou
Us
e
an
O
ut-
of-
Ne
two
rk
Pro
vid
er
Lim
itati
on
s &
Exc
ep
tio
ns
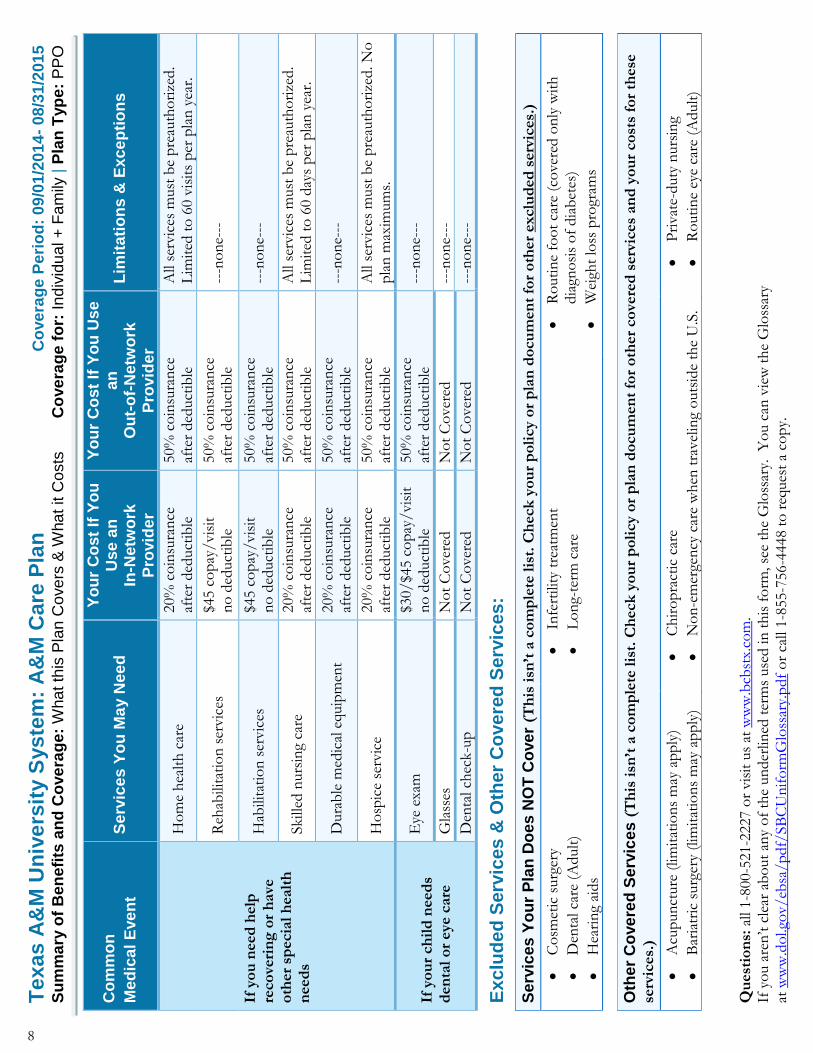
If y
ou
need
help
re
co
veri
ng
or
have
o
ther
specia
l h
ealt
h
need
s
Ho
me
hea
lth
car
e 20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
A
ll se
rvic
es m
ust
be
pre
auth
ori
zed.
Lim
ited
to
60 v
isit
s p
er p
lan
yea
r.
Reh
abili
tati
on
ser
vic
es
$45 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Hab
ilita
tio
n s
ervic
es
$45 c
op
ay/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Skille
d n
urs
ing
care
20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
A
ll se
rvic
es m
ust
be
pre
auth
ori
zed.
Lim
ited
to
60 d
ays
per
pla
n y
ear.
Dura
ble
med
ical
equip
men
t 20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Ho
spic
e se
rvic
e 20%
co
insu
ran
ce
afte
r ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
A
ll se
rvic
es m
ust
be
pre
auth
ori
zed. N
o
pla
n m
axim
um
s.
If y
ou
r ch
ild
need
s d
en
tal
or
eye c
are
Eye
exa
m
$30/$4
5 c
opay
/vis
it
no
ded
uct
ible
50%
co
insu
ran
ce
afte
r ded
uct
ible
--
-no
ne-
--
Gla
sses
N
ot
Co
ver
ed
No
t C
over
ed
---n
on
e---
Den
tal ch
eck-u
p
No
t C
over
ed
No
t C
over
ed
---n
on
e---
Ex
clu
de
d S
erv
ices
& O
ther
Co
ve
red
Se
rvic
es
:
Se
rvic
es
Yo
ur
Pla
n D
oes
NO
T C
ove
r (T
his
isn
’t a
co
mp
lete
lis
t. C
heck
yo
ur
po
licy o
r p
lan
do
cu
men
t fo
r o
ther
exclu
ded
serv
ices.
)
Co
smet
ic s
urg
ery
Den
tal ca
re (
Adult
)
Hea
rin
g ai
ds
Infe
rtili
ty t
reat
men
t
Lo
ng-
term
car
e
Ro
uti
ne
foo
t ca
re (
cover
ed o
nly
wit
h
dia
gno
sis
of
dia
bet
es)
Wei
ght
loss
pro
gram
s
Oth
er
Co
ve
red
Se
rvic
es
(T
his
isn
’t a
co
mp
lete
lis
t. C
heck
yo
ur
po
licy o
r p
lan
do
cu
men
t fo
r o
ther
co
vere
d s
erv
ices
an
d y
ou
r co
sts
for
these
se
rvic
es.
)
Acu
pun
cture
(lim
itat
ion
s m
ay a
pp
ly)
Bar
iatr
ic s
urg
ery
(lim
itat
ion
s m
ay a
pp
ly)
Ch
iro
pra
ctic
car
e
No
n-e
mer
gen
cy c
are
wh
en t
ravel
ing
outs
ide
the
U.S
.
Pri
vat
e-duty
nurs
ing
Ro
uti
ne
eye
care
(A
dult
)
8
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Su
mm
ary
of
Ben
efi
ts a
nd
Co
ve
rag
e:
Wha
t th
is P
lan C
ove
rs &
Wha
t it C
osts
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
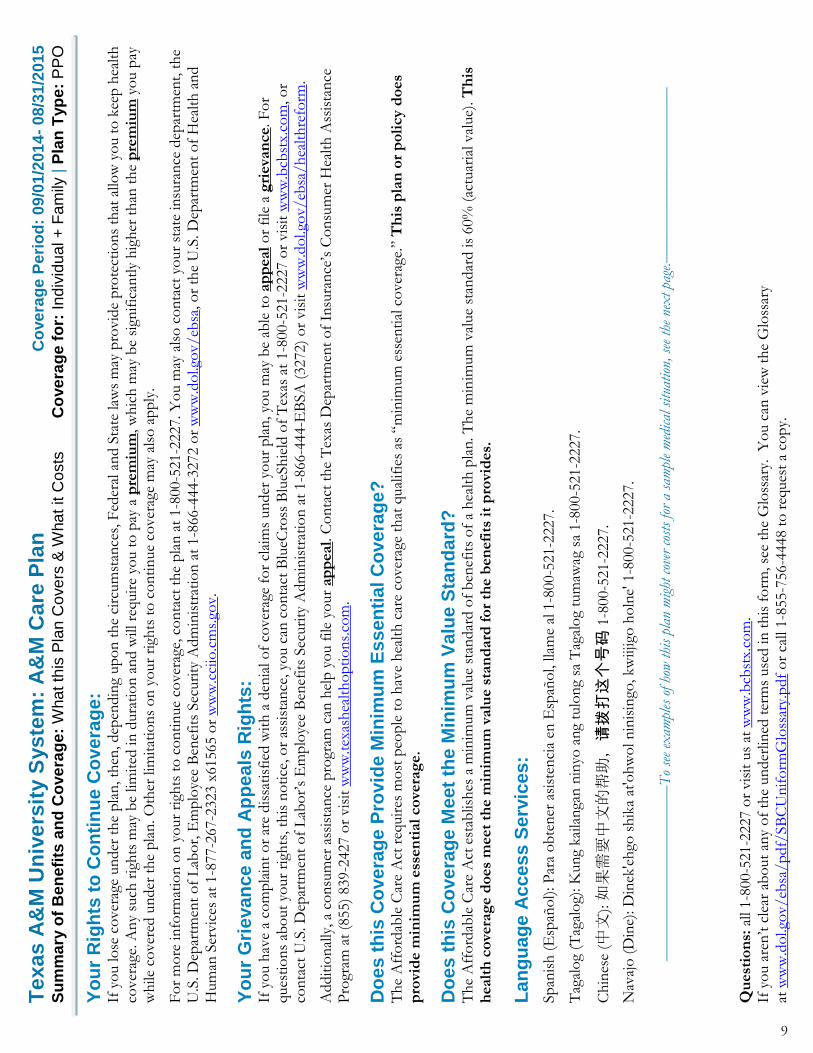
Yo
ur
Rig
hts
to
Co
nti
nu
e C
ove
rag
e:
If y
ou lo
se c
over
age
un
der
th
e p
lan
, th
en, dep
endin
g up
on
th
e ci
rcum
stan
ces,
Fed
eral
an
d S
tate
law
s m
ay p
rovid
e p
rote
ctio
ns
that
allo
w y
ou t
o k
eep
hea
lth
co
ver
age.
An
y su
ch r
igh
ts m
ay b
e lim
ited
in
dura
tio
n a
nd w
ill re
quir
e yo
u t
o p
ay a
pre
miu
m, w
hic
h m
ay b
e si
gnif
ican
tly
hig
her
th
an t
he
pre
miu
m y
ou p
ay
wh
ile c
over
ed u
nder
th
e pla
n. O
ther
lim
itat
ion
s o
n y
our
righ
ts t
o c
on
tin
ue
cover
age
may
als
o a
pp
ly.
Fo
r m
ore
in
form
atio
n o
n y
our
righ
ts t
o c
on
tin
ue
cover
age,
co
nta
ct t
he
pla
n a
t 1-8
00-5
21-2
227. Y
ou m
ay a
lso
co
nta
ct y
our
stat
e in
sura
nce
dep
artm
ent,
th
e U
.S. D
epar
tmen
t o
f L
abo
r, E
mp
loye
e B
enef
its
Sec
uri
ty A
dm
inis
trat
ion
at
1-8
66-4
44-3
272 o
r w
ww
.do
l.go
v/eb
sa, o
r th
e U
.S. D
epar
tmen
t o
f H
ealt
h a
nd
Hum
an S
ervic
es a
t 1-8
77-2
67-2
323 x
61565 o
r w
ww
.cci
io.c
ms.
gov.
Yo
ur
Gri
eva
nc
e a
nd
Ap
pe
als
Rig
hts
: If
yo
u h
ave
a co
mp
lain
t o
r ar
e dis
sati
sfie
d w
ith
a d
enia
l o
f co
ver
age
for
clai
ms
un
der
yo
ur
pla
n, yo
u m
ay b
e ab
le t
o a
pp
eal
or
file
a g
rieva
nce. F
or
ques
tio
ns
abo
ut
your
righ
ts, th
is n
oti
ce, o
r as
sist
ance
, yo
u c
an c
on
tact
Blu
eCro
ss B
lueS
hie
ld o
f T
exas
at
1-8
00-5
21-2
227 o
r vis
it w
ww
.bcb
stx.
com
, o
r co
nta
ct U
.S. D
epar
tmen
t o
f L
abo
r’s
Em
plo
yee
Ben
efit
s Sec
uri
ty A
dm
inis
trat
ion
at
1-8
66-4
44-E
BSA
(3272)
or
vis
it w
ww
.do
l.go
v/eb
sa/h
ealt
hre
form
.
Addit
ion
ally
, a
con
sum
er a
ssis
tan
ce p
rogr
am c
an h
elp
yo
u f
ile y
our
ap
peal. C
on
tact
th
e T
exas
Dep
artm
ent
of
Insu
ran
ce’s
Co
nsu
mer
Hea
lth
Ass
ista
nce
P
rogr
am a
t (8
55)
839-2
427 o
r vis
it w
ww
.tex
ash
ealt
ho
pti
on
s.co
m.
Do
es
th
is C
ove
rag
e P
rovid
e M
inim
um
Es
se
nti
al C
ov
era
ge
?
Th
e A
ffo
rdab
le C
are
Act
req
uir
es m
ost
peo
ple
to
hav
e h
ealt
h c
are
cover
age
that
qual
ifie
s as
“m
inim
um
ess
enti
al c
over
age.
” T
his
pla
n o
r p
oli
cy d
oes
pro
vid
e m
inim
um
ess
en
tial
co
vera
ge
.
Do
es
th
is C
ove
rag
e M
eet
the M
inim
um
Va
lue S
tan
da
rd?
T
he
Aff
ord
able
Car
e A
ct e
stab
lish
es a
min
imum
val
ue
stan
dar
d o
f b
enef
its
of
a h
ealt
h p
lan. T
he
min
imum
val
ue
stan
dar
d is
60%
(ac
tuar
ial val
ue)
. T
his
h
ealt
h c
ove
rag
e d
oes
meet
the m
inim
um
valu
e s
tan
dard
fo
r th
e b
en
efi
ts i
t p
rovi
des.
La
ng
ua
ge
Ac
ce
ss
Se
rvic
es
:
Sp
anis
h (
Esp
año
l): P
ara
ob
ten
er a
sist
enci
a en
Esp
año
l, llam
e al
1-8
00-5
21-2
227.
Tag
alo
g (T
agal
og)
: K
ung
kai
lan
gan
nin
yo a
ng
tulo
ng
sa T
agal
og
tum
awag
sa
1-8
00-5
21-2
227.
Ch
ines
e (中文
): 如果需要中文的帮助,请拨打这个号码
1-8
00-5
21-2
227.
Nav
ajo
(D
ine)
: D
inek
'eh
go s
hik
a at
'oh
wo
l n
inis
ingo
, kw
iijig
o h
oln
e' 1
-800-5
21-2
227.
––––––––––––––––––––––
To
see
exam
ples
of ho
w thi
s pl
an m
ight
cov
er c
osts
for
a s
ampl
e m
edical
situa
tion
, se
e th
e ne
xt
page
.––––––––––––––––––––––
9
Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Co
ve
rag
e E
xam
ple
s
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
Ha
vin
g a
ba
by
(n
orm
al d
eliv
ery)
Ma
na
gin
g t
yp
e 2
dia
be
tes
(r
outi
ne
mai
nte
nan
ce o
f
a w
ell-
con
tro
lled c
on
dit
ion
)
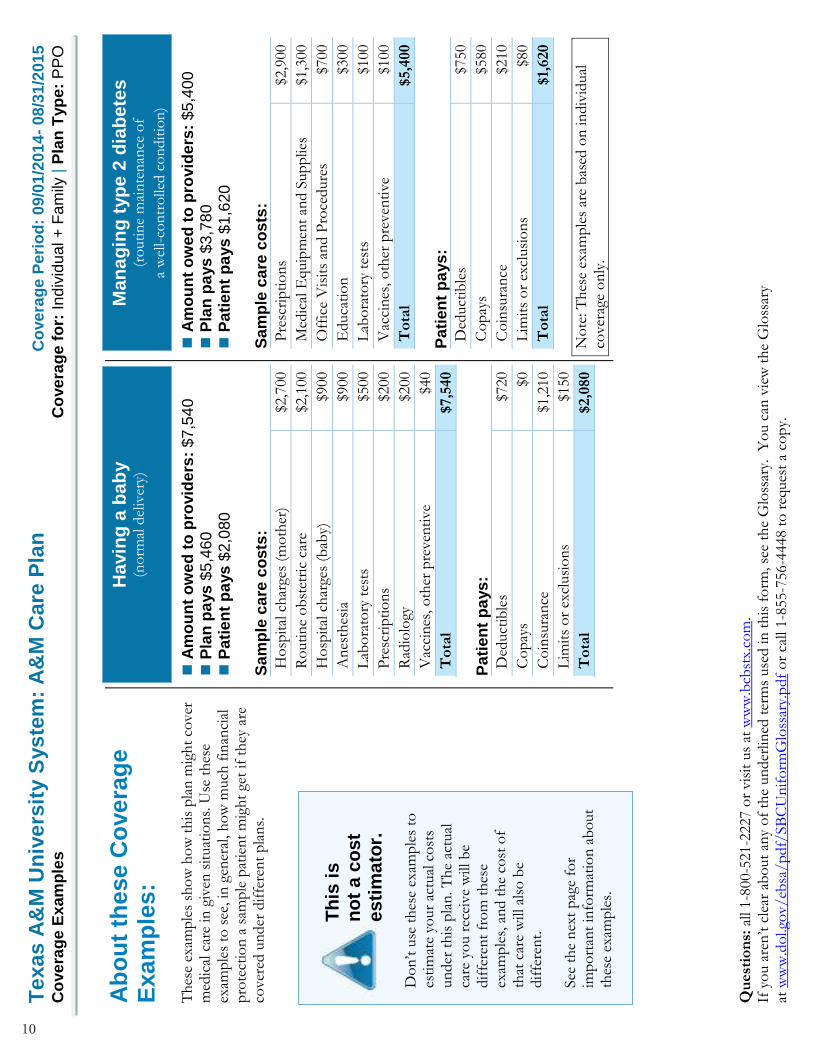
Ab
ou
t th
ese C
ove
rag
e
Exa
mp
les:
Th
ese
exam
ple
s sh
ow
ho
w t
his
pla
n m
igh
t co
ver
m
edic
al c
are
in g
iven
sit
uat
ion
s. U
se t
hes
e ex
amp
les
to s
ee, in
gen
eral
, h
ow
much
fin
anci
al
pro
tect
ion
a s
amp
le p
atie
nt
mig
ht
get
if t
hey
are
co
ver
ed u
nder
dif
fere
nt
pla
ns.
A
mo
un
t o
we
d t
o p
rovid
ers
: $
7,5
40
P
lan
pa
ys
$5
,46
0
P
ati
en
t p
ays
$2
,080
S
am
ple
ca
re c
os
ts:
Ho
spit
al c
har
ges
(mo
ther
) $2
,700
Ro
uti
ne
ob
stet
ric
care
$2
,100
Ho
spit
al c
har
ges
(bab
y)
$900
An
esth
esia
$9
00
Lab
ora
tory
tes
ts
$500
Pre
scri
pti
on
s $2
00
Rad
iolo
gy
$200
Vac
cin
es, o
ther
pre
ven
tive
$40
To
tal
$7,5
40
Pa
tien
t p
ays
:
Ded
uct
ible
s $7
20
Co
pay
s $0
Co
insu
ran
ce
$1,2
10
Lim
its
or
excl
usi
on
s $1
50
To
tal
$2,0
80
A
mo
un
t o
we
d t
o p
rovid
ers
: $
5,4
00
P
lan
pa
ys
$3
,78
0
P
ati
en
t p
ays
$1
,620
S
am
ple
ca
re c
os
ts:
Pre
scri
pti
on
s $2
,900
Med
ical
Equip
men
t an
d S
up
plie
s $1
,300
Off
ice
Vis
its
and P
roce
dure
s $7
00
Educa
tio
n
$300
Lab
ora
tory
tes
ts
$100
Vac
cin
es, o
ther
pre
ven
tive
$100
To
tal
$5,4
00
Pa
tien
t p
ays
:
Ded
uct
ible
s $7
50
Co
pay
s $5
80
Co
insu
ran
ce
$210
Lim
its
or
excl
usi
on
s $8
0
To
tal
$1,
620
No
te: T
hes
e ex
amp
les
are
bas
ed o
n in
div
idual
co
ver
age
on
ly.
Th
is i
s
no
t a c
os
t e
sti
ma
tor.
Do
n’t
use
th
ese
exam
ple
s to
es
tim
ate
your
actu
al c
ost
s un
der
th
is p
lan
. T
he
actu
al
care
yo
u r
ecei
ve
will
be
dif
fere
nt
fro
m t
hes
e ex
amp
les,
an
d t
he
cost
of
that
car
e w
ill a
lso
be
dif
fere
nt.
See
th
e n
ext
pag
e fo
r im
po
rtan
t in
form
atio
n a
bo
ut
thes
e ex
amp
les.
10

Texas A
&M
Un
ive
rsit
y S
ys
tem
: A
&M
Care
Pla
n
Co
ve
rag
e P
eri
od
: 0
9/0
1/2
01
4-
08
/31
/201
5
Co
ve
rag
e E
xam
ple
s
C
ove
rag
e f
or:
In
div
idu
al +
Fa
mily
| P
lan
Typ
e:
PP
O
Qu
est
ion
s: a
ll 1-8
00-5
21-2
227 o
r vis
it u
s at
ww
w.b
cbst
x.co
m.
If
yo
u a
ren
’t c
lear
ab
out
any
of
the
un
der
lined
ter
ms
use
d in
th
is f
orm
, se
e th
e G
loss
ary.
Y
ou c
an v
iew
th
e G
loss
ary
at w
ww
.do
l.go
v/eb
sa/p
df/
SB
CU
nif
orm
Glo
ssar
y.p
df
or
call
1-8
55-7
56-4
448 t
o r
eques
t a
cop
y.
Qu
esti
on
s a
nd
an
sw
ers
ab
ou
t th
e C
ove
rag
e E
xam
ple
s:
Wh
at
are
so
me o
f th
e
as
su
mp
tio
ns
be
hin
d t
he
C
ove
rag
e E
xa
mp
les
?
Co
sts
do
n’t
in
clude
pre
miu
ms.
Sam
ple
car
e co
sts
are
bas
ed o
n n
atio
nal
av
erag
es s
up
plie
d b
y th
e U
.S.
Dep
artm
ent
of
Hea
lth
an
d H
um
an
Se r
vic
es, an
d a
ren
’t s
pec
ific
to
a
par
ticu
lar
geo
grap
hic
are
a o
r h
ealt
h p
lan
.
Th
e p
atie
nt’
s co
ndit
ion
was
no
t an
ex
cluded
or
pre
exis
tin
g co
ndit
ion
.
All
serv
ices
an
d t
reat
men
ts s
tart
ed a
nd
ended
in
th
e sa
me
cover
age
per
iod.
Th
ere
are
no
oth
er m
edic
al e
xpen
ses
for
any
mem
ber
co
ver
ed u
nder
th
is p
lan
.
Out-
of-
po
cket
exp
ense
s ar
e b
ased
on
ly
on
tre
atin
g th
e co
ndit
ion
in
th
e ex
amp
le.
Th
e p
atie
nt
rece
ived
all
care
fro
m in
-n
etw
ork
pro
vid
ers
. I
f th
e p
atie
nt
had
re
ceiv
ed c
are
fro
m o
ut-
of-
net
wo
rk
pro
vid
ers
, co
sts
wo
uld
hav
e b
een
hig
her
.
Wh
at
do
es
a C
ove
rag
e E
xa
mp
le
sh
ow
?
Fo
r ea
ch t
reat
men
t si
tuat
ion
, th
e C
over
age
Exa
mp
le h
elp
s yo
u s
ee h
ow
ded
ucti
ble
s,
co
paym
en
ts, an
d c
oin
sura
nce c
an a
dd u
p. It
al
so h
elp
s yo
u s
ee w
hat
exp
ense
s m
igh
t b
e le
ft
up
to
yo
u t
o p
ay b
ecau
se t
he
serv
ice
or
trea
tmen
t is
n’t
co
ver
ed o
r p
aym
ent
is lim
ited
.
Do
es
th
e C
ove
rag
e E
xa
mp
le
pre
dic
t m
y o
wn
care
ne
ed
s?
N
o.
Tre
atm
ents
sh
ow
n a
re just
exam
ple
s.
Th
e ca
re y
ou w
ould
rec
eive
for
this
co
ndit
ion
co
uld
be
dif
fere
nt
bas
ed o
n y
our
do
cto
r’s
advic
e, y
our
age,
ho
w s
erio
us
your
con
dit
ion
is,
an
d m
any
oth
er f
acto
rs.
Do
es
th
e C
ove
rag
e E
xa
mp
le
pre
dic
t m
y f
utu
re e
xp
en
se
s?
N
o.
Co
ver
age
Exam
ple
s ar
e n
ot
cost
esti
mat
ors
. Y
ou c
an’t
use
th
e ex
amp
les
to
esti
mat
e co
sts
for
an a
ctual
co
ndit
ion
. T
hey
ar
e fo
r co
mp
arat
ive
purp
ose
s o
nly
. Y
our
ow
n c
ost
s w
ill b
e dif
fere
nt
dep
endin
g o
n
the
care
yo
u r
ecei
ve,
th
e p
rice
s yo
ur
pro
vid
ers
ch
arge
, an
d t
he
reim
burs
emen
t yo
ur
hea
lth
pla
n a
llow
s.
Ca
n I
us
e C
ove
rag
e E
xa
mp
les
to
co
mp
are
pla
ns?
Y
es.
When
yo
u lo
ok a
t th
e Sum
mar
y o
f
Ben
efit
s an
d C
over
age
for
oth
er p
lan
s,
you’ll
fin
d t
he
sam
e C
over
age
Exa
mp
les.
W
hen
yo
u c
om
par
e p
lan
s, c
hec
k t
he
“Pat
ien
t P
ays”
bo
x in
eac
h e
xam
ple
. T
he
smal
ler
that
num
ber
, th
e m
ore
co
ver
age
the
pla
n p
rovid
es.
Are
th
ere
oth
er
co
sts
I s
ho
uld
c
on
sid
er
wh
en
co
mp
ari
ng
p
lan
s?
Y
es.
An
im
po
rtan
t co
st is
the
pre
miu
m
you p
ay. G
ener
ally
, th
e lo
wer
yo
ur
pre
miu
m, th
e m
ore
yo
u’ll
pay
in
out-
of-
po
cket
co
sts,
such
as
co
paym
en
ts,
ded
ucti
ble
s, a
nd c
oin
sura
nce. Y
ou
sho
uld
als
o c
on
sider
co
ntr
ibuti
on
s to
ac
coun
ts s
uch
as
hea
lth
sav
ings
acc
oun
ts
(HSA
s), fl
exib
le s
pen
din
g ar
ran
gem
ents
(F
SA
s) o
r h
ealt
h r
eim
burs
emen
t ac
coun
ts
(HR
As)
th
at h
elp
yo
u p
ay o
ut-
of-
po
cket
ex
pen
ses.
11