Embed Size (px)
Citation preview

Universidade de São Paulo
2014-06
Fluorescence spectroscopy for the detection of
potentially malignant disorders and squamous
cell carcinoma of the oral cavity Photodiagnosis and Photodynamic Therapy, Amsterdam : Elsevier BV, v. 11, n. 2, p. 82-90, June
2014http://www.producao.usp.br/handle/BDPI/50794
Downloaded from: Biblioteca Digital da Produção Intelectual - BDPI, Universidade de São Paulo
Biblioteca Digital da Produção Intelectual - BDPI
Departamento de Física e Ciências Materiais - IFSC/FCM Artigos e Materiais de Revistas Científicas - IFSC/FCM

Photodiagnosis and Photodynamic Therapy (2014) 11, 82—90
Available online at www.sciencedirect.com
ScienceDirect
jo ur nal ho mepage: www.elsev ier .com/ locate /pdpdt
Fluorescence spectroscopy for thedetection of potentially malignant disordersand squamous cell carcinomaof the oral cavity
Ana Lucia Noronha Francisco PhDa, Wagner Rafael Correrb,Luciane Hiramatsu Azevedo PhDc, Vivian Galletta Kern PhDc,Clóvis Antônio Lopes Pinto PhDd, Luiz Paulo Kowalski PhDe,∗,Cristina Kurachi PhDb,∗∗
a Department of Oral Diagnosis, School of Dentistry of Piracicaba, University of Campinas (UNICAMP), Av.Limeira 901, Piracicaba 13414-018, São Paulo, Brazilb Department of Physics and Materials Science, Physics Institute of São Carlos, University of São Paulo(USP), Av. Trabalhador São-Carlense 400, São Carlos 13566-590, São Paulo, Brazilc Special Laboratory of Laser in Dentistry, School of Dentistry of São Paulo, University of São Paulo (USP),Av. Professor Lineu Prestes, Cidade Universitária, São Paulo 05508-000, São Paulo, Brazild Department of Pathology, A.C. Camargo Cancer Center, Rua Prof. Antonio Prudente 211, São Paulo01509-900, São Paulo, Brazile Department of Head and Neck Surgery and Otorhinolaryngology, A.C. Camargo Cancer Center and theNational Institute of Science and Technology in Oncogenomics (INCITO), Rua Prof. Antonio Prudente 211,São Paulo 01509-900, São Paulo, BrazilAvailable online 4 April 2014
KEYWORDSSquamous cellcarcinoma;Fluorescencespectroscopy;Early diagnosis;Potentially malignantdisorders;Oral cavity
Summary Oral cancer is a public health problem with relevant incidence in the world pop-ulation. The affected patient usually presents advanced stage disease and the consequenceof this delay is a reduction in survival rates. Given this, it is essential to detect oral cancerat early stages. Fluorescence spectroscopy is a non-invasive diagnostic tool that can improvecancer detection in real time. It is a fast and accurate technique, relatively simple, whichevaluates the biochemical composition and structure using the tissue fluorescence spectrumas interrogation data. Several studies have positive data regarding the tools for differentiat-ing between normal mucosa and cancer, but the difference between cancer and potentiallymalignant disorders is not clear.
The aim of this study was to evaluate the efficacy of fluorescence spectroscopy in the dis-crimination of normal oral mucosa, oral cancer, and potentially malignant disorders.
∗ Corresponding author.∗∗ Corresponding author at: Physics Institute of São Carlos, University of São Paulo, Avenida Trabalhador São-Carlense 400, São Carlos
13566-590, Brazil. Tel.: +55 16 33739810; fax: +55 16 33739811.E-mail addresses: lp [email protected] (L.P. Kowalski), [email protected] (C. Kurachi).
http://dx.doi.org/10.1016/j.pdpdt.2014.03.0091572-1000/© 2014 Elsevier B.V. All rights reserved.

Detection of potentially malignant disorders 83
The fluorescence spectroscopy was evaluated in 115 individuals, of whom 55 patients presentedoral squamous cell carcinoma, 30 volunteers showing normal oral mucosa, and 30 patients havingpotentially malignant disorders. The spectra were classified and compared to histopathology toevaluate the efficiency in diagnostic discrimination employing fluorescence. In order to classifythe spectra, a decision tree algorithm (C4.5) was applied. Despite of the high variance observedin spectral data, the specificity and sensitivity obtained were 93.8% and 88.5%, respectively at406 nm excitation. These results point to the potential use of fluorescence spectroscopy as animportant tool for oral cancer diagnosis and potentially malignant disorders.© 2014 Elsevier B.V. All rights reserved.
Introduction
Annually, about 10 million malignant tumors are diagnosedworldwide, and cancer of the oral cavity represents 6% ofall cases [1,2]. Different tumors may affect the oral cav-ity, and oral squamous cell carcinoma (OSCC) is the mostfrequent one, representing 90% of all cases [2—5]. Unfor-tunately, in most cases, the patients present for treatmentwith advanced stage disease, with consequent decrease insurvival rates [1,6]. The treatment of these patients is usu-ally aggressive and may be mutilating [7]. Despite the recentadvances in the treatment of OSCC, there has been only asmall increase in the survival rate [8].
Disease local and regional control and rehabilitation ofpatients with advanced oral carcinoma are extremely dif-ficult. On the other hand, initial lesions are more easilyremoved with less patient mutilation and better prognosis[9,10].
Some OSCC lesions come from pre-existing potentiallymalignant disorders [6,11] with the annual malignant trans-formation rate of approximately 1% [11,12]. Patients withprevious history of oral cancer, especially those that hadbeen heavy smokers, present an altered oral mucosa (can-cerization field). Although oral lesions are common, topredict the biological behavior of them remains a chal-lenge. The standard methodology for the diagnosis ofthese lesions is clinical examination and histopatholog-ical analysis. Most oral potentially malignant disorders(PMD) are clinically present as leukoplakia or erythro-plakia, but histologically they can show a wide varietyof phenotypes, such as hyperkeratosis, dysplasia or evencarcinoma [13].
Currently, there is great interest in optical techniquesthat use fluorescence to evaluate lesions using a non-invasive procedure. Based on the tissue optical propertiesand diagnostic sensitivity to capture the fluorescence emit-ted by native fluorophores, these optical techniques havebeen indicated to differentiate endogenous tissue varia-tions [14—16]. The fluorescence spectroscopy has become animportant tool in detecting potentially malignant and malig-nant lesions in the oral mucosa [17,18]. The biochemicalcomposition and tissue architecture can be assessed by theemitted fluorescence spectrum, which will be modified inthe presence of tissue alterations [19]. Mathematical algo-rithms can then be developed and optimized to classify therespective tissues in histological categories based on theirspectral characteristics [20—23].
The aim of this study was to determine the ability of fluo-rescence spectroscopy to discriminate normal and abnormal
oral mucosa, potentially malignant and/or malignant orallesions.
Patients and methods
This prospective study was performed at the Departmentof Head and Neck Surgery and Otorhinolaryngology, A.C.Camargo Cancer Center and LELO-USP (Special Laboratory ofLaser Dentistry), São Paulo, Brazil. The clinical research pro-tocol was approved by the Ethical Committee of the partic-ipant institutions, and all recruited patients that agreed toparticipate as volunteers signed an informed consent form.
The fluorescence spectroscopy system is composed of anexcitation light source, an interrogation probe, a portablespectrophotometer USB 2000 (Ocean Optics, USA) and a lap-top. Two solid state lasers, a diode emitting at 406 nm and adoubled-frequency neodymium: YAG at 532 nm, were used asexcitation light sources. The interrogation probe is a Y-typefiberoptic probe, where one tip is connected to the spec-trophotometer and the other one to the excitation laser.Two optical fibers of 600 �m in diameter are positioned sideby side. One conducts the excitation light and the other col-lects the re-emitted light by the tissue. The outer diameterof the interrogation tip is 1.6 mm and the total diameter ofthe area that is placed in contact with the tissue surfaceis 3.2 mm. The spectroscopic data was acquired using thesoftware OOIBase32 (Ocean Optics, USA).
All subjects were interviewed and the data filledin a standardized interview form containing informationregarding the habits (including tobacco and alcohol con-sumption), family history, etc. Clinical examination wasperformed and examiner clinical impression was recorded.In patients with cancer (C) and PMD, clinical characteristics,including lesion dimensions, color, and site were evaluated.In vivo fluorescence spectroscopy measurements were per-formed under both excitation wavelengths, collecting asmany points needed to cover the whole lesion surface, atleast one hour after the last meal. In the case of identifica-tion of superficial clinical heterogeneities, as leukoplakia orerythroplakia, fluorescence spectra were taken and iden-tified to correlate with distinct clinical patterns. Tissueresearch was not taken from area of necrosis, usuallypresent at the center of ulcerated lesions. In each chosenarea, five spectroscopic measurements under each wave-length were taken. The patient evaluation was performed atthe surgical theater at A.C. Camargo Hospital, after induc-tion of general anesthesia, and at outpatient clinics at LELO,before the biopsy procedure or surgical resection of thelesions.

84 A.L.N. Francisco et al.
A 3 mm punch biopsy was taken at patients with cancerat the time of surgery. Biopsy sites were matching with spe-cific spectroscopic measurement sites, and were performedaccording to heterogenicity of the lesion defined by thephysician based on clinical judgment. Tissue specimens werestored in plastic vials containing 10% formalin solution forhistology processing.
In volunteers with normal mucosa, and no history ofcancer, fluorescence measurements were taken from theborder of the tongue (BOT), dorsum of the tongue (DOT),floor of the mouth (FOM), lower labial mucosa (LB), buccalmucosa (BM), gingiva or alveolar ridge, hard palate andlip, with at least 5 spectroscopy measurements for eachexcitation wavelength. From each area, an exfoliativecytology was performed.
The spectra were analyzed according to the differentanatomical sites and amended by tissue injury com-pared to normal tissue. The results were correlated withthe histopathological diagnosis. Different types of com-putational processing were conducted to evaluate thediscrimination among normal mucosa (NM), PMD, and cancer(C).
Initially, all spectra were analyzed based on classificationand independent of anatomical site. In a second analysis,principal component analysis (PCA) was performed, classi-fying the spectra also according to the anatomical site. PCAwas applied using three types of spectrum preprocessing:normalization by maximum intensity, standardization andanalysis of the first derivative and the second derivative.
Classification using spectral indices (SI) based on qualita-tive analysis of the spectra was also performed. The SI wasdefined comparing emission intensities at wavelengths mod-ified in the PMD and OSCC groups, when compared to the NM.The index used to classify the spectra can be expressed bythe following equation:
R =∫ 643.2
623.1I d�
∫ 506.6
485.4I d�
where I is emission intensity, in arbitrary units, and � is theemission wavelength.
Finally, computational classifiers were also used toachieve a more robust system for spectra classification. Inone analysis, the classifiers were applied to the databasewithout any spectral normalization and a second analy-sis with the spectra normalized by its maximum emission.This approach could lead to a better comprehension aboutthe role of spectrum intensity in the quality of classifica-tion. Three different classifiers were used: Naïve Bayes,k-nearest neighbor (kNN) and a decision tree C4.5 (J48), allof them implemented on open source software WEKA [44].All classifiers were tested for both excitation wavelengthsin the exact same conditions. Moreover, the excess of vari-ables (wavelengths) may contain unnecessary and redundantinformation, which can compromise the classifier perfor-mance. Thus, variables selection methods were appliedprior to computational classifiers in order to keep only therelevant ones. The selection methods used were ReliefF andCFS (correlation-feature selection), both present in WEKAsoftware.
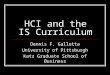
Fig. 1 Erythroleukoplakia lesion in the region of the oralmucosa (A) and histopathological diagnosis corresponding tomoderate dysplasia with hyperkeratosis (B).
Results
One hundred and fifteen subjects over 18 years old, bothgenders, smokers and nonsmokers were investigated in thisstudy. The subjects were enrolled in the study as 55 OSCCpatients, 30 patients with PMD, and 30 volunteers with nor-mal oral mucosa, without history of malignancy in airwaydigestive tract. Of the total of 115 subjects, 54 (47%) werewomen and 61 (53%) men. The mean age was 58.59 years old,while among women was 54.5 years and for men was 62.69.Each biopsy was analyzed by a certified oral pathologistblind to the fluorescence results, describing the diagnosisand histopathological characteristics (Figs. 1 and 2). Fivepatients presented more than one lesion, resulting in 99interrogated lesions. Classification was based on histopatho-logical diagnosis as gold standard. Fluorescence patternswere determined, identifying spectroscopic features foreach type of mucosa evaluated. The sample distributionbased on the histopathological analysis and site location ispresented at Table 1.
Among 85 individuals with lesions in the oral mucosa, 56were OSCC patients and underwent surgery for resection ofthe lesion with tridimensional surgical margins. The mostaffected anatomical site was the BOT (25 lesions, 44.5%),followed by the BM (11 lesions, 19.5%), FOM and LM, 5

Detection of potentially malignant disorders 85
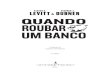
Fig. 2 Ulcerated lesion in the region of the lower alveolarridge (A) and the corresponding histopathological diagnosis ofOSCC well differentiated (B).
lesions each, and alveolar ridge (retromolar region) with4 lesions.
The qualitative comparison between the effectivenessof violet and green light excitation for fluorescence in thedetection of oral cancer was performed. The oral mucosashowed distinct fluorescence features in distinct interro-gated sites.
Variation at fluorescence intensity was observed depend-ing on oral site, and inter- and intra-patient measurements.Due to the fact that these differences may result from probe
positioning, and pressure, the intensity emission raw val-ues were not used for diagnostic. As overall analysis of thefluorescence spectral behavior, the higher emission intensi-ties were present at palate and alveolar ridge, for 406 nmexcitation. The tongue and the FOM are highly vascular-ized tissues, and hemoglobin is the main biological absorberresulting in the low intensity of the spectra collected classi-fication (Figs. 3 and 4). We observed that the center of thecancer lesion emits very low fluorescence signal, while theborders emit distinct fluorescence emissions depending onthe heterogeneity of the lesion and site location.
The BOT site showed the major spectral differences inthe shape and intensity of the fluorescence emission. Thissite is a transition region of dorsal and ventral tongue. Thedorsum of the tongue shows a unique mucosa with the pres-ence of large papillae and high bacteria colonization thatproduces porphyrin compounds, which emits a high intensityred fluorescence. Analyzing the fluorescence from erythro-plakia lesions, a lower intensity is observed when comparedto the NM emission intensity, due to higher hemoglobin con-tent, which is the main endogenous absorber. Excitation at406 nm provided the spectra with best fluorescence discrim-ination in all analysis performed. Although, excitation at532 nm reach a deeper region in the tissue, the endoge-nous fluorophores involved in OSCC are better excited atthe ultraviolet region and the initial changes of epithelialtissue start at the most superficial layers.
Spectral results from NM at normal volunteers and NM atPMD patients presented distinct patterns.
Initially, principal component analysis (PCA) was per-formed to compare the raw spectra of PMD versus NMfrom the PMD patients versus NM from volunteers, with-out discrimination of the anatomical site. Secondly, thecomparison was performed of PMD, OSCC and NM from volun-teers. No satisfactory result was achieved for 406 or 532 nmexcitation, even after pre-processing data, as spectral nor-malization tools.
The spectral index analysis was performed for spectracollected from normal volunteer (NM) and normal con-tralateral mucosa (NC). Fifty patients and 75 sites wereselected. However only 36 cases presented contralateralnormal mucosa (NC), for intrapatient comparison. High vari-ance was observed for the calculated index values of C andNC oral mucosa. The standard deviation for the normal oralmucosa is lower when compared to the cancer at the same
Table 1 Distribution of lesions by anatomic site correlated with the histopathological diagnosis.
Anatomical site Total number of lesions Number of lesions by histological diagnosis
Potentially malignantdisorders
In situcarcinoma
Microinvasivecarcinoma
Invasivecarcinoma
Border of tongue 39 14 2 0 23Floor of the mouth 11 6 2 0 3Buccal mucosa 21 10 0 1 10Labial mucosa 8 3 0 0 5Gingiva 11 8 0 0 3Retromolar 4 0 0 1 3Palate 5 2 1 0 2

86 A.L.N. Francisco et al.
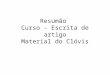
Fig. 3 Comparison between normal mucosa, potentiallymalignant disorder and border of lesion of OSCC in anatomicsite border of tongue, the excitation of 406 nm (A) and 532 nm(B).
site location. This result is correlated to the distinct histol-ogy and clinical patterns for the oral carcinoma that arepresented. Despite of this, the spectral indexes analysisdid not result in clear distinction between the classifica-tion groups at a global comparison. In a intra-site analysisthe NM, C and PMD groups were separated. However, due tosmall sampling, statistical analysis could not be evaluated.
The classification using computational classifiers was per-formed in the whole dataset (NM, PMD, and C). In theproposed analysis with the computational classifiers (P vs.NN), the computational k-nearest neighbor (kNN), was usedfollowed by two other algorithms: the Bayes and J48. Themissing values in Table 2, marked with (***) are algorithmsthat were time consuming and did not show expressiveresults. The J48 decision tree presented the best result, bothfor 532 nm and 406 nm excitations. For excitation at 406 nm,algorithm J48 + CFS showed 88.5% of sensitivity and 93.8% ofspecificity, while for excitation at 532 nm the same methodobtained 87% of sensitivity and 91.2% of specificity (bothwith normalization by the maximum intensity emission)(Table 2). Considering just PMD and NM group, the J48 + CFSshows a sensitivity equals to 92% and a specificity of 96.5%.
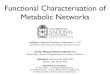
Fig. 4 Comparison between normal mucosa, potentiallymalignant disorder and border of lesion of OSCC in anatomicsite buccal mucosa, the excitation of 406 nm (A) and 532 nm(B).
Discussion
Changes on tissue architecture and biochemical composi-tion that occur during establishment and progression ofthe pathology result in modification of the tissue fluores-cence emission. The optical path of the photons travelingin the tissue is driven by these microscopic characteris-tics. The collection geometry of the spectroscopy systemmay also play an important role on the final collected flu-orescence spectrum [24—26]. For oral cancer diagnostics,excitation wavelength presented as more effective is in the400—450 nm interval [25,27]. Our results also showed thatthe 406 nm excitation presented more tissue informationconcerning malignant characteristics, even though 532 nmcould potentially interrogate a deeper tissue layer.
The collected fluorescence spectra differ depending onthe excitation wavelength, oral site, biochemical compo-sition and tissue architecture [28,29]. Distinct excitationwavelengths present different photon energies, resulting indistinct light-tissue interaction, and may excite differentendogenous fluorophores [26,30].

Detection of potentially malignant disorders 87
Table 2 Representation of the mathematical processing performed for analysis, with normalization by maximum, systemfluorescence spectroscopy to discrimination between normal and abnormal mucosa.
VE VI
Sensibility Specificity Accuracy FP rate Sensibility Specificity Accuracy FP rate
Bayes 0.513 0.8 0.513 0.200 0.618 0.744 0.618 0.256J48 0.829 0.888 0.829 0.112 0.887 0.936 0.887 0.064kNN k = 3 0.647 0.774 0.647 0.226 0.769 0.869 0.769 0.131kNN k = 7 0.641 0.766 0.641 0.234 0.76 0.863 0.760 0.137kNN k = 11 0.638 0.762 0.638 0.238 0.768 0.859 0.768 0.141kNN k = 15 0.641 0.769 0.641 0.231 0.75 0.845 0.750 0.155kNN k = 19 0.636 0.765 0.636 0.235 0.748 0.843 0.748 0.157Bayes + ReliefF (10%) 0.515 0.771 0.515 0.229 *** *** *** ***J48 + ReliefF (10%) 0.834 0.889 0.834 0.111 0.885 0.934 0.885 0.066Best kNN + ReliefF (10%) 0.63 0.761 0.630 0.239 *** *** *** ***Bayes + CFS 0.567 0.819 0.567 0.181 0.626 0.759 0.626 0.241J48 + CFS 0.87 0.912 0.870 0.088 0.885 0.938 0.885 0.062kNN + CFS 0.672 0.785 0.672 0.215 *** *** *** ***
Native tissue fluorescence originates from endoge-nous fluorophores, such as collagen, elastin, structuralcomponents of the tissue, and other biomolecules. The flu-orescence associated with the presence of aromatic aminoacids and proteins shows information about the cellular andtissue structure [23,30]. In contrast, the concentration ofderivatives of pyroxene, NADH and FAD, varies with themetabolic status of tissue [31] and their levels are alteredin the presence of pathological conditions. The fluores-cence of these molecules is dependent on its concentrationand distribution as well as physicochemical properties ofthe environment. Because the modification of protein andmetabolic conditions occurs during malignant transforma-tion, this fluorescence interrogation is a useful tool todifferentiate tumor from normal tissue [26].
When considering the collection of the emitted flu-orescence at tissue surface, not only the fluorophoresdistribution contributes for the spectral intensity and shapeof fluorescence detected, but also the absorbers andscatterers distributions. Collagen is one of the main contrib-utors for the oral mucosa fluorescence, and the decreasedemission is related to the breakdown of the fiber links,resulted from tumor cells invasion. Neoplasia progres-sion also involves angiogenesis, and structural epitheliumchanges, resulting in modification of tissue absorption andscattering [27,31,32].
According to Schwarz et al. [18], during carcinogenesisin the oral cavity, structural and biochemical changes inthe epithelium and stroma may alter the optical proper-ties of dysplastic and cancerous tissues. Increased nuclearsize and cytoplasm/nucleus ratio, microvascular changes,degradation of collagen fibers, increased of hemoglobin, andchanges in mitochondrial concentration of NADH and FAD,leading to changes in the optical scattering, absorption andintrinsic characteristics of tissue autofluorescence.
The fluorescence spectroscopy using a fiberoptic probeinterrogation provides the evaluation of a small tissue vol-ume, especially when considering the excitation wavelengthat the violet spectrum. Poh et al. [27] using wide field flu-orescence imaging showed the effectiveness of a simple
handheld fluorescence system (excitation at 400—460 nm)to delineate the full extent of a tumor which, in turn, canbe useful in guiding the complete tumor resection in theoperating room. Optical changes, specifically the loss offluorescence in the mucosa lesion and surrounding tissueswere used to map the field cancerization. Correlation ofhistopathological characteristics and specific genetic alter-ations indicate that fluorescence visualization is improvedlesion delineation (size) and field cancerization detectioncompared to clinical judgment [16,27,32,33]. The fluores-cence spectra collected in the same tissue show differentways depending on the excitation used. This variation occursbecause the penetration depth and the excited fluorophoresin each wavelength. The excitation at 532 nm has a greaterpenetration depth compared to excitation at 406 nm [25].Moreover, the characteristics of the tissue in which theendogenous fluorophores are present have higher influence.The hemoglobin, which is present in the vascular spacesand in the stromal layer absorbs a portion of the emit-ted fluorescence. This finding is particularly visible in theexcitation at 406 nm. Epithelial fluorophores such as NADHalso play a role in the features of the spectra of shal-low depths and stromal fluorophores, such as collagen,contribute to the measured signal from deeper regions[8,18,19].
Schwarz et al. [34] suggest that short wavelengthsmay be more sensitive than the profound changes in theuptake of optical scattering properties, where occur the ini-tial changes detected in epithelium, such as nuclear sizeand nucleus/cytoplasm ratio, and in the stromal surfaceregion. In non-keratinized tissue diagnostic performancewas achieved using only optical spectra short and mediumdepths. The discrimination spectra normal and abnormalsites is better when used excitations smaller ranges, whichis heavily skewed to the epithelial layer and minimizes theeffects of the absorption of hemoglobin [19,35]. Our opticalsystem do not have discrimination of the information fromdistinct tissue layers, the final response is the contributionof the total volume. This result in a less precise informationof each fluorophore contribution to the final spectrum, but

88 A.L.N. Francisco et al.
our results showed that even the superficial information canachieve satisfactory diagnostic performance.
Pavlova et al. [35] suggest that oral epithelium can bedivided into three layers with different optical properties.The oral epithelium is composed of a superficial layer of ker-atin, which varies in thickness depending upon the anatomiclocation. The main fluorophore of the surface epitheliumis keratin, in which there is a layer of non-keratinizedepithelium and is occupied by intermediate and basal cellsmetabolically active and with less dispersion. The fluores-cence from the non-keratinized epithelium is associatedwith metabolic indicators NADH and FAD, which increase insamples of oral dysplasia.
The presence of inflammation may be an additional com-plicating factor for spectroscopic diagnosis of oral lesions;autofluorescence due to reduced inflammation can be dif-ficult to distinguish from the reduced autofluorescencedue to neoplasia. As inflammation primarily affects thestroma while the dysplastic epithelium changes occur, thedepth sensitive spectral data, particularly obtained fromsuperficial layers may provide more useful information fordiscriminating benign lesions from malignant or dysplasticlesions [18].
Erythematous lesions have a lower fluorescence intensitycompared to leukoplakic lesions, probably the largest pres-ence of hemoglobin. Leukoplakic lesions behave differentlyin re-emission of light because they are rich in keratin, whichhas a prominent role in the phenomena of scattering andabsorption and fluorescence intensity re-emitted [36—38].Erythroplakic mucous membranes were already diagnosedwith a more advanced degree of atypia and frequently withan in situ or microinvasive cancer, these lesions producedmore altered fluorescence spectra compared to normal andthere was a tendency to have lower re-emission of light.These results corroborate the study Ebihara et al. [14].
Pavlova et al. [35], using a Monte Carlo model, foundthat 43—66% of the total light detected with a depth selec-tive probe, ranging from 280 nm to 420 nm, originated fromthe thickness of the non keratinized epithelium. The iden-tification of bacterial contamination is important becausesome bacteria produce porphyrins, and this may change theresult of the intrinsic fluorescence of the tissue. Leaving theplace of contamination by oral microorganisms optical dis-crimination has been primarily associated with a decreasein the intensity of fluorescence emitted in the tumor regionas compared to the healthy regions. This fact has been cor-related with decreased crosslinking of collagen fibers andmatrix components [8,36].
Similar results have been previously reported in otherclinical studies on detection of oral cancer. de Veld et al.[42] observed that dysplastic sites and tumors are accompa-nied by a progressive drop in fluorescence intensity, whereasLane et al. [31] reported a loss of signal in wide fieldfluorescence images from potentially malignant and malig-nant oral lesions compared to normal mucosa around of thelesion. The reduced fluorescence associated with neopla-sia was seen in a wide range of excitation wavelengths of330—470 nm in the study of Schwarz et al. [34].
Pavlova et al. [26] studied the UV excitation from four dif-ferent locations in the tongue of a single patient. The lesiondiagnosed with severe inflammation showed a large drop inboth fluorescence as epithelial and stroma. Moreover, while
the fluorescence of the stroma of normal tissue stemmedfrom collagen fibers, the stromal inflamed fluorescence orig-inated mainly inflammatory cells. The oral lesion diagnosedwith dysplasia was characterized by increased thickness flu-orescent epithelial cells throughout the epithelium and adecrease in fluorescence stromal surface.
McGee et al. [40] found that discrimination of dys-plastic lesions versus cancer was more successful whenalgorithms are designed for individual sites. Similar resultswere obtained in this study. The combination of sites withthe same spectral properties (floor of mouth and border ofthe tongue) produced a more accurate and consistent dis-crimination performance than algorithms developed for allsites.
The similarity between the shapes of the spectra ofnormal and cancerous tissues significantly reduces the reli-ability of this technique for cancer detection. Severalmethods have been investigated to solve this problem bya statistical analysis of spectral data to reduce the ‘‘noise’’or the employment of excitement in multiple lengths. Mul-tivariate analysis based on principal components analyses(PCA) and support vector machines have been introduced toidentify spectral features which can be correlated with thetissue pathology condition, but there are various types ofmathematical procedures that may be performed for opti-mal discrimination (classification) of the samples [16].
In the evaluation of biopsy specimens, Fryen et al. [41]observed that autofluorescence becomes heterogeneousin areas with neoplastic cell pleomorphism. The differ-ent degrees of keratinization according differentiation ofinjuries cause more distinct viewing of the change, unlikenormal epithelium. Even small precancerous lesions such asdysplasia and carcinoma in situ show different degrees ofautofluorescence.
Heintzelman et al. [8] found that the wavelengths of350 nm excitation, 380 nm and 400 may be suitable for oralcancer detection. By using the excitation wavelengths of350 nm and 400 nm in the oral cavity, obtained a fluores-cence emission at 472 nm, with 90% sensitivity and 88%specificity. In validation tests of the experiment, the authorsachieved 100% sensitivity and 98% specificity, using the sameparameters of wavelength. According to the authors, theoral mucosa showed a higher emission intensity of auto-fluorescence (450 nm) at a wavelength of 380 nm excitationrelative to neoplastic mucosa.
de Veld et al. [39] evaluated by fluorescence spec-troscopy 97 volunteers with normal oral mucosa usingseven different wavelengths of excitation in 13 anatom-ical locations. The intensity of autofluorescence showedits maximum between 500 and 510 nm. The lower fluo-rescence intensities were observed at the border of lipsemimucosa and border of the tongue, and the largest inpalate and buccal mucosa. The authors found that there aresmall spectroscopic differences between different anatom-ical locations. The total intensity of fluorescence cannotbe used as a reference to compare with a database, sincethere are different intensities of autofluorescence in differ-ent anatomical sites, and the variance between patients.
Palmer et al. [43] observed that the largest differencesbetween normal and dysplastic tissue were found in theexcitation wavelength of 410 nm. Dysplastic and malignantsamples had increased fluorescence above 600 nm, when

Detection of potentially malignant disorders 89
compared with normal samples indicating that dysplasticlesions exhibit a fluorescent characteristic which is notpresent in normal mucosa. The method used by the authorsshowed sensitivity, specificity and accuracy of fluorescenceto differentiate histologically normal tissue from dysplasticand neoplastic 90%, 91% and 91%, respectively.
The high level of sensitivity and specificity obtained witha noninvasive procedure demonstrates the power of fluo-rescence spectroscopy as a diagnostic tool for detection ofcarcinoma, especially considering that the carcinoma groupshowed great variability. A diagnostic technique with fastresponse can provide important information for the clini-cian, aid in the classification of the lesion, scanning largeareas, the delimitation of the lesion margin, and also in thechoice of the biopsy site [25].
The clinical characteristics were observed in various dif-ferent behaviors of fluorescence spectra. The excitationunder violet light showed higher levels of sensitivity andspecificity for discrimination of normal versus carcinomacompared with excitation at 532 nm. The analysis resultshowed better results with the algorithm J48 of violet exci-tation, compared to 532 nm.
Our results demonstrate the potential of diagnostic flu-orescence spectroscopy in an objective and non-invasive,dysplastic and cancerous sites distinguishing normal oralmucosa. Furthermore, these results support the use of a sys-tem for optical spectroscopy depth susceptible to improveperformance in diagnosis.
The fluorescence spectroscopy has significant sensitiv-ity and specificity for diagnosing neoplastic tissue, both inexcitation at 406 nm and at 532 nm. Excitation at 406 nmwas more efficient and can be used as an auxiliary tool inclinical diagnostic discrimination of mucosa normal versuspotentially malignant disorder versus oral cancer.
Acknowledgments
The financial support provided by FAPESP (CEPOF-CEPIDProgram, proc. no. 98/14270-8, aid research proc. no.07/57126-5 and ALNF scholarship no. 09/12938-8), CNPq(proc. no. 477439/2007-1), INCITO FAPESP (proc. no.2008/57887-9) and professor Dante Antonio Migliari of theSpecial Laboratory of Laser in Dentistry, School of Dentistryof São Paulo, University of São Paulo (USP).
References
[1] Warnakulasuriya S. Living with oral cancer: epidemiology withparticular reference to prevalence an life-style changes thatinfluence survival. Oral Oncol 2010;46:407—10.
[2] World Health Organization; 2010. Available in: http://www.who.int/cancer/en/index.html [accessed 28.12.10].
[3] Gorsky RD, Schwartz E, Dennis D. The morbidity, mortality,and economic costs of cigarette smoking in New Hampshire.J Community Health 1990;15(3):175—83.
[4] Parkin DM, Bray F, Feday J, Pisani P. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74—108.
[5] Rose BS, Jeong JH, Nath SK, Lu SM, Mell LK. Population-basedstudy of competing mortality in head and neck cancer. J ClinOncol 2011;29(September (26)):3503—9.
[6] Bagan JV, Scully C. Recent advanced in Oral Oncology 2007: epi-demiology, aetiopathogenesis, diagnosis and prognostication.Oral Oncol 2008;44(February (2)):103—8.
[7] Gillenwater A, Jacob R, Ganeshappa R, Kemp B, El-NaggarAK, Palmer L, et al. Noninvasive diagnosis of oral neoplasiabased on fluorescence spectroscopy and native tissue auto-fluorescence. Arch Otolaryngol Head Neck Surg 1998;124:1251—8.
[8] Heintzelman DL, Utzinger U, Fuchs H, Zuluaga A, GossageK, Gillenwater AM, et al. Optimal excitation wavelengths forin vivo detection of oral neoplasia using fluorescence spec-troscopy. Photochem Photobiol 2000;72:103—13.
[9] Warnakulasuriya S. Global epidemiology of oral and orop-haryngeal cancer. Oral Oncol 2009;45(April—May (4—5)):309—16.
[10] Jerjes W, Upile T, Petrie A, Riskalla A, Hamdoon Z, VourvachisM, et al. Clinicopathological parameters, recurrence, locore-gional and distant metastasis in 115 T1-T2 oral squamous cellcarcinoma patients. Head Neck Oncol 2010;2(April):9.
[11] Silverman Jr S, Gorsky M, Lozada F. Oral leukoplakia and malig-nant transformation: a follow-up study of 257 patients. Cancer1984;53:563—8.
[12] van der Waal I. Potentially malignant disorders of the oral andoropharyngeal mucosa: present concepts of management. OralOncol 2010;46(June (6)):423—5.
[13] Kademani D. Oral cancer. Mayo Clin Proc 2007;82(July(7)):878—87.
[14] Ebihara A, Krasieva TB, Liaw LLH, Fago S, Messadi D, Osann K,et al. Detection and diagnosis of oral cancer by light-inducedfluorescence. Lasers Surg Med 2003;32:17—24.
[15] Kurachi C, Fontana CR, Melo CAS, Rosa LEB, Bagnato VS. Opticalbiopsy of chemical-induced tongue lesions in Goldem Syrianhamsters: an in vivo study. Laser Phys 2004;14(4):502—6.
[16] Hu X-H, Lu JQ. Optical detection of cancers. Encyclo-pedia of biomaterials and biomedical engineering. Tay-lor & Francis; 2005. http://www.tandfonline.com/doi/abs/10.1081/E-EBBE-120041300#.U0V UahdV1Z
[17] Georgakoudi I, Jacobson BC, Müller MG, Sheets EE, Badizade-gan K, Carr-Locke DL, et al. NAD(P)H and collagen as in vivoquantitative fluorescent biomarkers of epithelial precancerouschanges. Cancer Res 2002;62:682—7.
[18] Schwarz RA, Gao W, Weber CR, Kurachi C, Lee JJ, El-NaggarAK, et al. Noninvasive evaluation of oral lesions using depth-sensitive optical spectroscopy. Cancer 2009;15:1669—79.
[19] Pavlova I, Weber CR, Schwarz RA, Williams M, El-NaggarA, Gillenwater A, et al. Monte Carlo model to describedepth selective fluorescence spectra of epithelial tissue:applications for diagnosis of oral precancer. J Biomed Opt2008;13(6):064012.
[20] Ramanujam N, Mitchell MF, Mahadevan A, Thomsen S, MalpicaA, Wright T, et al. Development of a multivariate statisticalalgorithm to analyze human cervical tissue fluorescence spec-tra acquired in vivo. Lasers Surg Med 1996;19:46—62.
[21] Ingrams DR, Dhingra JK, Roy K, Perrault Jr DF, Bottrill ID, KabaniS, et al. Autofluorescence characteristics of oral mucosa. HeadNeck 1997;19(1):27—32.
[22] Ramanujam N. Fluorescence spectroscopy of neoplastic andnon-neoplastic tissues. Neoplasia 2000;2:89—117.
[23] Chu SC, Hsiao T-CR, Lin JK, Wang C-Y, Chiang HK. Compari-son of performance of linear multivariate analysis methods fornormal and dysplasia tissues differentiation using autofluores-cence spectroscopy. IEEE Trans Biomed Eng 2006;53:2265—73.
[24] Welch AJ, Gardner C, Richards-Kortum R, Chan E, Criswell G,Pfefer J, et al. Propagation of fluorescent light. Lasers SurgMed 1997;21:166—78.
[25] Kurachi C, Fontana CR, Rosa LEB, Bagnato VS. Fluorescencespectroscopy for the detection of tongue carcinoma — vali-dation in an animal model. J Biomed Opt 2008;13(3):1—6.
90 A.L.N. Francisco et al.
[26] Pavlova I, Weber CR, Schwarz RA, Williams M, Gillenwater A,Richards-Kortum R. Fluorescence spectroscopy of oral tissue:Monte Carlo modeling with site-specific tissue properties. JBiomed Opt 2009;14(1):014009.
[27] Poh CF, Zhang L, Anderson DW, Durham JS, Williams PM, PriddyRW, et al. Fluorescence visualization detection of field alter-ations in tumor margins of oral cancer patients. Clin CancerRes 2006;12:6716—22.
[28] Mallia RJ, Subhash N, Sebastian P, Kumar R, Thomas SS,Mathews A, et al. In vivo temporal evolution of ALA-inducednormalized fluorescence at different anatomical locations oforal cavity: application to improve cancer diagnostic contrastand potential. Photodiagn Photodyn Ther 2010;7(September(3)):162—75.
[29] de Visscher SAHJ, Witjes MJH, Kascáková S, Sterenborg HJCM,Robinson DJ, Roodenburg JLN, et al. In vivo quantificationof photosensitizer concentration using fluorescence differ-ential path-length spectroscopy: influence of photosensitizerformulation and tissue location. J Biomed Opt 2012;17(June(6)):067001.
[30] Ganesan S, Sacks PG, Yang Y, Katz A, Al-Rawi M, Savage HE,et al. Native fluorescence spectroscopy of normal and malig-nant epithelial cells. Cancer Biochem Biophys 1998;16:365—73.
[31] Lane PM, Gilhuly T, Whitehead P, Zeng H, Poh CF, Ng S, et al.Simple device for the direct visualization of oral-cavity tissuefluorescence. J Biomed Opt 2006;11:1—7.
[32] Müller MG, Valdez TA, Georgakoudi I, Backman V, Fuentes C,Kabani S. Spectroscopic detection and evaluation of morpho-logic and biochemical changes in early human oral carcinoma.Cancer 2003;97:1681—92.
[33] Westra WH, Sidransky D. Fluorescence visualization in oralneoplasia: shedding light on an old problem. Clin Cancer Res2006;12(22):6594—7.
[34] Schwarz RA, Gao W, Weber CR, Kurachi C, Lee JJ, El-NaggarAK, et al. Noninvasive evaluation of oral lesions using depth-sensitive optical spectroscopy. Cancer 2008;15:1669—79.
[35] Pavlova I, Williams M, El-Naggar A, Richards-Kortum R,Gillenwater A. Understanding the biological basis of
autofluorescence imaging for oral cancer detection: high-resolution fluorescence microscopy in viable tissue. ClinCancer Res 2008;14:2396—404.
[36] van Staveren HJ, van Veen RLP, Speelman OC, WitjesMJH, Star WM, Roodenburg JLN. Classification of clinicalautofluorescence spectra of oral leukoplakia using an arti-ficial neural network: a pilot study. Oral Oncol 2000;36:286—93.
[37] Sharwani A, Jerjes W, Salih V, Swinson B, Bigio IJ, El-Maaytah M,et al. Assessment of oral premalignant using elastic scatteringspectroscopy. Oral Oncol 2006;42:343—9.
[38] Rahman MS, Ingole N, Roblyer D, Stepanek V, Richards-KortumR, Gillenwater A, et al. Evaluation of a low-cost, portable imag-ing system for early detection of oral cancer. Head Neck Oncol2010;2(April):10.
[39] de Veld DCG, Skurichina M, Witjes MJH, Duin RPW, SterenborgDJCM, Star WM. Autofluorescence characteristics of healthyoral mucosa at different anatomical sites. Lasers Surg Med2003;32:367—76.
[40] McGee S, Mardirossian V, Elackattu A, Mirkovic J, Pistey R, Gall-agher G, et al. Anatomy-based algorithms for detecting oralcancer using reflectance and fluorescence spectroscopy. AnnOtol Rhinol Laryngol 2009;118(11):817—26.
[41] Fryen A, Glanz H, Lohmann W, Dreyer T, Bohle RM. Significanceof autofluoresce for the optical demarcation of field can-cerisation in the upper aerodigestive tract. Acta Otolaryngol1997;117:316—9.
[42] de Veld DCG, Witjes MJH, Sterenborgb HJCM, Roodenburg JLN.The status of in vivo autofluorescence spectroscopy and imag-ing for oral oncology. Oral Oncol 2005;41:117—31.
[43] Palmer GM, Marshek CL, Vrotsos KM, Ramanujam N. Opti-mal methods for fluorescence and diffuse reflectancemeasurements of tissue biopsy samples. Lasers Surg Med2002;30:191—200.
[44] Hall M, Frank E, Holmes G, Pfahringer B, Reutemann P, WittenIH. The WEKA data mining software: an update. SIGKDD Explor2009;11(1).