Embed Size (px)
DESCRIPTION
Expedient Trauma Course
Citation preview

Immediate Bystander Aid in Response to Blast and Ballistic Trauma Events
Dr S.J. Hatfill MDAdjunct Assistant Professor
Department of Emergency MedicineGeorge Washington University Medical Center
Department of Emergency Medicine
Division of Clinical Research and Leadership

Medical Environment of the Military Battlefield
• Rapidly developing scenarios.• Confusion • Severe trauma casualties.• Multiple area mass casualties.• Limited medical personnel.• Limited on-site medical supplies.• Disorganized or overtaxed medical
support infrastructure.

Some Natural and Social Disasters have a Medical Environment Similar to the Battlefield
Breslan School
Virginia Tech
North Hollywood Shootout
Oklahoma City London Bombings
Interstate Multiple Car Crash

Bystanders May Be the First Responders After a Mass Casualty Event Involving Blast and Ballistic Trauma
However, some type of training is necessary

This Course
• The material you will be taught today is derived from the U.S. Special Operations Command Doctrine of Tactical Combat Casualty Care.
• TCCC is taught to all SEALS, Army RANGERS and Special Forces, as well as all Army Medics and Navy and Corpsmen.
• It is designed to control the preventable causes of death resulting from blast and ballistic injury until higher level care can be provided.

Course Content
• You will be introduced to the major causes of death in blast and ballistic trauma and learn how to:
- control catastrophic hemorrhage - manage an airway - manage an open chest wound - i.d. casualties requiring immediate advanced care

Course Content
• You will be able to accomplish these tasks using only minimal improvised equipment.
• You will also learn how to create a prepackaged Emergency Trauma Medical Kit using commercially available medical materials.

Mechanism of Blast and Ballistic Injury

Explosive Blast
• Rapid conversion of an explosive solid or liquid into highly pressurized gases which expand / compress the surrounding air.
• Thermal pulse, pressure wave, blast wind, and shrapnel are generated and spread in all directions.

Blast Injuries
Related to the distance from the epicenter of the blast
(reversed in water)
Ballistic
Distance from epicenter1.0
Inur
y T
ype
ThermalPressure Shock Wave

Blast Injury
• THERMAL PULSE Burn damage, 1o to full thickness skin and soft tissue.
• BALLISTIC Shrapnel Fragments and Debris - 5,900 ft/sec to 1,900 ft/sec.
• OVERPRESSURE Partial or complete traumatic amputation. Debris, bone fragments, and other tissues are driven up between proximal tissue planes with muscles stripped from the bone.

Primary Effects of Blast Injury
• Combined thermal, overpressure blast, and ballistic injury.
• Blasts may cause multiple life-threatening injuries.
• Hidden patterns of injury may be present.

Primary Blast Injuries: TM RuptureTympanic Membrane ( Eardrum) Rupture
• Tympanic membrane rupture indicates an exposure to an over-pressurization wave.
• It may be found as an isolated injury or in association with other severe blast injuries.
• However, its presence does not indicate that more sinister blast injuries exist.

Blast Injury to Lung
• Over-pressure injury spreads down the trachea and bronchi causing alveolar rupture with hemorrhage into the alveoli. Bleeding can be significant (1000ml) in severe cases.
• “LEAF effect” - blast wave disrupts alveolar tissue but leaves overall bronchiole structure.

Blast Injury to Lung
Systemic Air Embolism
• Most common cause of blast - related sudden death in the 1st hour
• Direct leak of air from
alveoli and bronchial tree into the pulmonary vasculature

Blast Injury to Lung
Possible Systemic Air Embolism Signs
• Chest pain• Signs of a Stroke• Unilateral Blindness• Tongue blanching• Cutus Marmorata

Overpressure Blast Injury to Gut
Abdomen / GIT• Bowel wall contusions
• Blood may appear in stool.
• Can cause perforation from 24 - hours up to 1-2 weeks later.

Blunt Force Traumatic Brain Injury
Sudden force applied to side of head
Coup-Countercoup Mechanism

Overpressure Blast Injury to BrainTraumatic Brain Injury (TBI )
• Damage to select surface areas of the brain caused by blast pressure wave
• Nerve fibers stretched and broken.
• Unconsciousness.
• Length of Coma indicates severity of damage

Severe TBI Is Associated With Prolonged Coma
• Damage to select areas of the brain.
• Damage to the wiring that connects these different surface areas.

Traumatic Brain Injury (TBI)
• Consider the proximity of the casualty to the blast - particularly when given complaints of:
– Loss of consciousness.– Headache.– Fatigue.– Later persisting poor concentration, lethargy, amnesia,
or other constitutional symptoms.
• The symptoms of concussion and mild TBI can be similar.

Secondary Blast Injuries
• Injury from flying debris
• Responsible for the majority of casualties
• Small skin wound but devastating underlying trauma
• Essential to perform a careful primary survey of any blast casualty.

Secondary Blast Injury The Eye :
Up to 10% blast injuries will havesignificant eye injury with initially
only minimal discomfort
• Pain• Photophobia• Burning/irritation• Foreign body sensation• Altered vision• Periorbital swelling

Mechanisms of Ballistic Injury
• Permanent Cavity - localized tissue death along bullet tract• Temporary Cavity - elastic tissue displacement and rebound • Exit wounds are not always greater than entrance wounds
Temporary Cavity
Sonic Shock Wave
Permanent Cavity
Deceleration Yaw
SOFT TISSUE

Tissue Ballistics
Tissue Destruction
36% Fragmentation

Ballistic Injury To Solid Organs
Effect of temporary cavitation in a solid organ as a result of a penetrating high-velocity projectile (7.62.x39 mm).

Ballistic Injury to Air-Filled OrgansCrushed Tissue and Contusion
• Contusion (severe bruising) can be seen in both blast and ballistic injury.
• A minor degree may occur with trauma or high velocity non-penetrating plate strikes.
• Micro-hemorrhage into the lung alveoli in addition to the penetrating injury.

The Revolution in Battlefield Medicine

Beginning Of The Revolution In Modern Combat Medicine
• Operation Just Cause, Panama
• 01h00 December 20, 1989
• Navy SEAL Task Force PAPA tasked to destroy Noriega’s personal jet aircraft located at Punta Paitilla Airfield.
• 3 SEAL Assault platoons encircled the Learjet hanger the night of the invasion.

Sudden Contact
• Combat involved 48 SEALS and a small number of gunmen inside the hanger.
• 3 initial casualties turned into 14.
• 6 SEALS Killed, 8 Wounded.
• The incident prompted a full review of Navy Special Operations Medicine and Tactics.

Major Military Research Undertaken Into Combat Death
• Special Operations and Army medical community conduct a complete review of numerous previous conflicts and battlefield deaths.
• Thousands of cases of combat death were examined in detail.

Hallmark Historical Study Of Blast and Ballistic Death In Ground Combat
Bellamy, RF. Causes of Death in Conventional Land Warfare

KIA: 31% Head Trauma With Brain Injury

Expectant Head Casualties(Unconscious With Visible Brain Tissue)

KIA: 25%
Surgically Uncorrectable Torso Trauma

Direct Gunshot Wound to Heart

10% KIA Delayed Management of Potentially Correctable
Torso Trauma
Causes of death in potentially correctable torso
trauma:
- Failure to control preventable causes of death at the
site of injury
- Improperly managed:
- Hypothermia
- Shock
- Delayed TACEVAC.

Delayed Care and Shock
Normal 2500ml Loss Unconscious Death Probable

The Golden Hour In Severe Shock
• Shock Kidney• Shock Lung• Shock Liver
Minutes
50
0
100
30 60 90
Perc
en
t S
urv
ival
Shock becomes irreversible.
Progressive organ failure leads to eventual death.

DOW: 12% Wound Infections and Irreversible Shock
Prolonged Shock
Lactic Acid Buildup in the Blood
Bleeding Abnormalities
Multiple Organ Dysfunction and Failure Days Later
Hypothermia

KIA: 5% Tension Pneumothorax

KIA: 1%Airway Obstruction and Suffocation
Simple Unconscious Airway Obstruction Complicated Airway Trauma

7 % KIA Multisystem Mutilating Blast Trauma

KIA: 9% Bleeding to Death from Extremity Wounds

Irrespective of the Conflict Studied Ground Combat Shows a Trimodal
Distribution of Death Im m e d ia te : C NS in ju ry o r h e a rt a n d g re a t ve sse l in ju ry
Ea rly: Ma jo r He m o rrh a g e
La te : In fe c tio n a n d Multio rg a n fa ilu re
0 1 2 4 3
Ho u rs a fte r in ju ry
1 -2 5 -6
We e ks
1 0
2 0
3 0
4 0
5 0
0
Perc
ent
of t
raum
a d
ea
ths
Where can the greatest medical impact be made to improve survival from
blast and ballistic trauma ?
First peak of deaths occurs with minutes from tears of aorta, heart, brain, major extremity hemorrhage.
Second peak occurs from 1-4 hours from pneumothorax, shock, or internal bleeding.
Third peak days or weeks later from sepsis, and multiple organ failure from prolonged shock.

Preventable Death In Blast and Ballistic Injury
15% of Blast and Ballistic Deaths are Preventable

Before We Learn to Manage the Preventable Causes of Death----
It is Necessary to Understand Some Basic Trauma Anatomy

Musculoskeletal System
Muscle tissue will always
be involved in blast and
ballistic injury.
These wounds may appear to
be horrible when in fact, they
are a minor surgical nature and
not immediately life threatening.

Soft Tissue Injury
Jagged Edge Laceration
Avulsion Deep Laceration

Soft Tissue Surgical Management
Irrigation and Cleaning
Surgical Debridement
Wound Packing

The Severity of Soft Tissue Injury Is Based On Hemorrhage NOT the Appearance Of The Wound

Head and Airway Anatomy

Neck Anatomy
Penetrating shrapnel injury with laceration of the right common carotid artery

The Thoracic Cavity

Respiratory System

Cardiovascular System
SuperiorVena Cava
Aorta
Inferior Vena Cava
Midline Vascular Structures

Tissue Circulation
ArteriolesVeinule
s
Valve
Muscle Layers
Gas and Fluid exchange with tissues
Total Blood Volume- 5 L

Human Pelvis Anatomy
Major Pelvic Fracture – Break in the Pelvic Ring in more than 1 place

Unstable Pelvic Fractures Can Lead to Fatal Internal Hemorrhage
Massive Retroperitoneal Hemorrhage

Anatomy of the Abdomen

Anatomical Distribution of Penetrating Wounds ( % ) in Blast and Ballistic Injury

Basic Arm Anatomy
Note: The major artery in the upper arm is located in the axilla.

Basic Leg Anatomy
The major artery in the thigh is just below the skin.

Take a 5-Minute Break

The S. C. A. B Survey
Bystander Management of the Preventable Causes of Death From Blast and Ballistic
Trauma

Get off the X
The SCAB Acronym
• Situation• Catastrophic Bleeding / Communicate
• Airway• Breathing

Situation“Assess the Situation You Are In”
Fallujah, Iraq
• Soldier wounded in Femoral artery.
• 2d soldier and a medic rush from cover to assist casualty. 2d soldier is shot.

Assess the Situation
Boston Bombing

Catastrophic Hemorrhage Must be Controlled First
• Bleeding from extremity wounds is the number one cause of preventable death in blast and ballistic trauma.
• 90 seconds to 3 minutes to die from a Femoral Artery and Vein disruption

Immediate Pressure Point Technique
• Apply manual direct pressure to bleeding site or at a pressure point.
• This is a stop-gap measure while getting a tourniquet applied.
• Apply Direct Pressure to yourself if you are injured

Immediate Pressure Point Technique

The Tourniquet
• Tourniquet for catastrophic extremity hemorrhage.
• Manufactured tourniquets are designed for a single use.
• Apply over clothing as high as possible

Emergency Use of Tourniquet
• Direct the casualty to control hemorrhage by direct pressure if able.
• Use a tourniquet as a definitive treatment for limb hemorrhage.
- Apply tourniquet high on limb, over clothing. - Tighten, and reassess the situation. - Periodically reassess for tourniquet effectiveness
• Tourniquet application causes significant pain, and is not an indication of incorrect application, or that the tourniquet should be discontinued.

Tissue Damage After Tourniquet Application
Damage to the arm or leg is rare if the tourniquet is left on less than a110 minutes. Pneumatic tourniquets are often left in place for 2 hours during elective surgical procedures.
1 2 3 4 5 6
Nerve and Muscle Compression Injury
Severe Effects Upon Tourniquet Removal (Cardiac, Renal)
Widespread Muscle and Nerve Damage
Hours
Increasing Pain
111 minutes Possible Limb Loss

Prolonged 5-6 Hour Tourniquet Use
• Muscle cell death releases myoglobin and potassium into the circulation when tourniquet is removed.
• Causes sudden heartbeat irregularities and Kidney damage. Further increased tissue damage when the extremity is re-perfused with blood.

Even if Not BleedingAll Amputations or Partial Amputations Need a
Tourniquet
Even if Not BleedingAll Amputations or Partial Amputations Need a
Tourniquet
Active hemorrhage can occur at any time
Do not apply over a Joint

The Field Expedient Tourniquet
• Cravat & Windlass
• Other Materials:
- 3” x 3’ clothing
- 4 pencils or pens
- Debris from explosion
- Purse strap
Waist belts do not work

Improvised Tourniquet Use
• Maintain DIRECT PRESSURE while applying the tourniquet.
• If limb is fully exposed ; apply 2-3 inches above injury and tightened effectively
• Constantly reassess to ensure effectiveness

Blast Debris Used as an Improvised Tourniquet
Boston Bombing

The Medical Emergency Tourniquet ®® The Medical Emergency Tourniquet ®®
• Lightweight
• Does not need to be fully cinched tight before operating windlass
• Aluminum Non-breakable windlass
• Simple operation
• Can be applied and secured in seconds

Answer This
Does This Wound Need a Tourniquet ?
Where Is the Correct Placement For a Tourniquet In This Casualty ?

Example of Ineffective Tourniquet ApplicationExample of Ineffective Tourniquet Application
• Casualty wounded by RPG and sustained a leg wound with major femoral bleeding
• Bled to death despite the placement of 3 field-expedient tourniquets
• The soldier lacked an adequate tourniquet and was unable to improvise an effective one.

Cargo-Strap Tourniquet “Ranger Ratchet”

CAT® (Combat Application Tourniquet)
• Simple operation
• Must be fully cinched tight before operating windlass.
• The friction adaptor buckle should be inserted.
• Occasional length problem with some thick thighs

Tourniquets
• Get tourniquets on BEFORE onset of shock.
– Mortality is very high if casualties are already in shock before tourniquet application
• If bleeding not controlled with first tourniquet – use a second one just proximal to first

Get off the “X”
One-Person Drag
Two- Person Drag
Cradle Drop Drag

SEAL Team Two-Person Lift and Carry
1 2
3 4

Summary
• Assess the safety of the scene-beware of secondary explosive devices.
• Stop life-threatening limb hemorrhage with tourniquet.
• For life threatening bleeding not anatomically amendable to a tourniquet, continue to use direct pressure if possible.
Situation - Control Hemorrhage - Airway - Breathing

Hands-on Practice
• Tourniquet Demonstration
•
• Partner-up for Scenario - Move to Casualty
- Apply Direct Manual Pressure to Pressure Points
- Apply Tourniquet High on Limp Over Clothing

The Situation is Now Safe or You are Behind Cover

Continue Hemorrhage Control
• If tourniquet application is ineffective or unfeasible because of the anatomical location of the wound, proceed to the use of Wound Packing and a Pressure Bandage.
• Reassess all previous tourniquet applications.

Wound Packing and Pressure Bandage for Hemorrhage Control
• Junctional Hemorrhage is the most difficult to manage.
• If a tourniquet cannot be applied, the techniques of wound packing and pressure bandage can be used for hemorrhage control.

Wound Packing
• Placement of any “foreign material” directly into an open wound, directly activates the clotting mechanism
• Fully expose the wound and pack tightly from wall to wall and apex to apex Combat Gauze
folded fluff bandageimpregnated with
Hemostatic Agent
GAUZE ROLL6-ply sterile crinkle cotton folded fluff
bandage

Elastic “Pressure” Bandage
Packing

The Pressure Bandage
Packing, together with an overlying Pressure Bandage can control life threatening bleeding on most of the arm
and from the knee down
Pressure Bandage applied over the gauze packing applies high direct pressure over damaged tissue arteries
Collateral circulation to the distal extremity still remains.

Minimize Pain / Trauma During Pressure Bandage Application
Limb-Groin Technique
• Avoids repetitive lifting of injured limb
• Allows operator to use both hands to apply the dressing
• By leaning back slightly, effective traction is placed on a fracture
From the personal archive of Dr. S. Hatfill MD

Pressure Dressings Problems
From the Front Line
- Wound not fully exposed
- Gauze not properly packed - Bandage not tight
- Bandage not secured with an added half hitch - Bandage allowed to spindle.

Use of Hemostatic Agents
• Certain types of life-threatening hemorrhage cannot be controlled with tourniquets or bandages because of anatomical constraints (high groin, neck, deep armpit).
• Hemostatic agents may assist in these cases.

Hemostatic Agents
• Hemostatic agents incorporate proteins or chemicals designed to initiate and accelerate the fibrin clotting process.
• Some agents act to chemically seal damaged arteries and veins involved in uncontrolled hemorrhage.
• Must be used with sustained direct pressure.
• Takes 3-4 minutes of continued direct pressure to work.

4-Generations of Hemostatic Agents Have Been Developed
1 3 4

Primary Agent : Combat Gauze
• CoTCCC 1st line agent of choice
• Does not generate heat
• Effectively combines clotting agent with packing gauze
• The recommended time for direct pressure has been changed from 2 minutes to 3 minutes.

Life Threatening Hemorrhage Should Now Be Controlled
• Reassess situational awareness, consolidate cover
• Continue MARCH-E assessment of the casualty
• This involves assessing the airway next.
Copyright 2009 ATS Inc., LLC

Bleeding Control Is Often
Achieved By a Combination Of Methods
• Direct Manual Pressure
• Tourniquet
• Gauze Packing
• Pressure Bandage
• Haemostatic Agents

Hands-on Practice
• Pressure Bandage Demonstration
• Partner-up for Scenario - Move to Casualty
- Apply Direct Manual Pressure to Pressure Points
- Apply Packing and Pressure Dressing

Situation - Control Hemorrhage - Airway - Breathing

The Mass Casualty Collection Point
• In a CCP, all the casualties are grouped close together in a secure location.
• Then the airway and breathing are assessed.

The Upper Airway
Air
way

Manage the Airway
• If casualty is talking – They Have a Good Airway !
• Perform positioning on an unconscious casualty.
• Recognize potential complicated airway problems – and be ready to alert EMS personnel when they arrive.

Should diagnose this "from across the room" by observing :
Abnormal respiratory effort. Cyanosis. Intercostal / suprasternal / subcostal retractions. Snoring / gurgling / hoarseness / stridor. Agitation or decreasing consciousness.
Is There Airway Obstruction ?

Specific Causes of Airway Obstruction
• Decreased mental status: Shock, Head Injury
• Posture with casualty slumped forward
• Facial Fractures
• Blood , Vomit, Foreign Body (teeth).
• Unconscious with tongue blocking airway
• Increased pressure on the airway structures
- Neck hematomas from trauma
- Airway wall edema from burns/smoke inhalation

Stop-Gap Management Of Airway Obstruction
1. Airway opening maneuvers.
Positioning, Chin-lift, Jaw-thrust
2. Military uses an artificial airway for ALL Unconscious casualties - Nasopharyngeal airway
4. Place all unconscious casualties in recovery position when feasible.

Casualty Positioning
• A casualty with bleeding into the mouth or nose may be better able to maintain an airway by sitting up and leaning forward.
• Do not force them to lay down !

Massive Maxillofacial Trauma
• Severe airway damage, casualty awake and alert
• Medic attempted to force him into supine position - respiratory distress ensued
• Eventually transported sitting up and leaning forward
• Survived with good maxillofacial repair results
Casualty did not require advanced airway procedures in the field

Stop-Gap Airway Opening Maneuvers in an Unconscious Casualty
Chin lift

The Nasopharyngeal Airway(Prevents the tongue from blocking the upper airway)
From the personal archive of Dr. S. Hatfill MD
Place a NPA in all unconscious casualties

Placement of the Nasopharyngeal Airway
• Lubricate• Insert along floor of
nasal cavity• If resistance is met, use
back and forth motion• Do not force, use other
nostril• If patient gags, withdraw
slightly
Copyright 2009 ATS Inc., LLC
90 degrees

Contraindication To Nasopharyngeal Airway
• Relatively contraindicated in children (may cause bleeding from enlarged adenoids).
• Anatomical deformity complicating nasal passage of the NPA tube.

The Recovery Position
All unconscious casualties are placed in the recovery position (injured side of chest down)

Burns Can Cause Airway Obstruction Requiring Advanced Airway Management
• Severe facial and inhalation burns may cause rapid development of severe upper airway edema.
• NPA may not provide an adequate airway in these cases.
•

Advanced EMT Airway ManagementEndotracheal Intubation
- Medical Personnel
- Provides a temporary and secure airway.
- Vomit cannot be aspirated.
- Requires practice and skill.

Advanced EMT Airway Management The Emergency Cricoidotomy
• Surgical Cricoidotomy Fast, Simple, Safe, Medic/corpsman Level
• Surgical Tracheotomy Long Term Airway, Physician Level
Anatomical location, purpose, and level of procedure difficulty are different

Surgical Cricoidotomy
- Field emergency airway
- Airway not secure
- Vomit can be aspirated
Small tube inserted into the cricothyroid membrane to keep the airway open

Mismanagement of Airway Trauma
• Gunshot wound to the lower jaw that also damaged the tongue and upper airway structures
• Attempted field intubation was unsuccessful
• Died of airway obstruction.
• Airway could have been achieved with a Surgical Cricoidotomy.

Nasopharyngeal Demonstration

Escape For a 1-Hour Lunch Break

Situation - Control Hemorrhage - Airway - Breathing

Respiration
1. Assess the breathing of your casualty.
2. Seal any open chest wounds
3. Alert EMS personnel if your casualty has chest trauma and is developing progressive respiratory distress.

Check Respiration
What do we want to know about the Respiration ?
• Is casualty actually breathing?
• Is there respiratory difficulty (increased work of breathing)?
• Is there blunt or penetrating torso trauma?

Is the Casualty Actually Breathing ?
CPR is ineffective
in Trauma
• Time consuming
• Casualty stays dead
• CPR has not been shown to be effective in casualties with Trauma

Cardiopulmonary Resuscitation in Trauma
• Study of 138 Trauma patients with pre-hospital cardiac arrest with CPR resuscitation attempted.
• No Survivors
• Trauma patients in cardiopulmonary arrest should not be transported emergently to a trauma center even in a civilian setting, due to a lack of significant chance for survival.
Rosemurgy et al. J. Trauma 1993

Exceptions To The No CPR Rule
Only in the case of non-traumatic disorders should CPR be considered prior to Ambulance evacuation.
Hypothermia
Near-drowning
Electrocution
Use the Current American Heart Association Protocol of 2 Breaths /100 Compressions.

Nasal flaringNasal flaring
Excessive Excessive use of use of accessoryaccessorymusclesmuscles
Chest Chest TightnessTightness CyanosisCyanosis
Coughing Coughing
Respiratory Respiratory noisenoise• wheezingwheezing• rattlingrattling•StridorStridor
Impaired Impaired mentationmentation•dizzinessdizziness• anxiety,anxiety,•combativenesscombativeness• confusionconfusion•unconsciousnessunconsciousness
Is There Respiratory Difficulty ?

Is There Blunt or Penetrating Trauma ?
• Ask if there is chest pain.
• If unconscious, expose / examine the neck, axilla, front of chest
- Look at facial/lip skin color
- Look at chest for breathing
• Inspect the back only after pelvis has been checked.

Injuries you are looking for:
Penetrating Injuries• Open pneumothorax• Tension pneumothorax
Blunt Trauma• Bruising• Broken ribs• Flail chest

Penetrating Injury Of The Chest WallThe Open Pneumothorax
• Loss of negative pressure between lung and the chest wall.
• The elastic tissue of lung causes it to collapse towards the midline.
• An empty space is left inside the chest cavity on the injured side
Empty Space

Open Pneumothorax“Sucking Chest Wound”
• You may or may not hear air rushing in and out of the chest cavity (Sucking Chest Wound.”
• Open entrance wound > 5-cent coin allows air to move in and out of the pleural space.
• If chest wall opening is 2/3 or more of the diameter of the trachea, air will preferentially go into the chest cavity.

Anatomical Signs Of Open Pneumothorax
• Penetrating wound in chest larger than a nickel coin.
• Air may be moving in and out through the hole as the chest wall moves.
• Slight marginal wound bleeding with bubbles may be present.

Clinical Signs Of Open Pneumothorax)
Difficulty BreathingRapid Respiratory Rate
Possible Coughing Blood
Rapid Heartbeat
Bruising or Fractured Ribs
Cyanosis may be present

It is Imperative to Convert the Open Chest Wound Into a Closed Wound
• Inferior Vena Cava becomes repeatedly “pinched” as the chest wall moves and out.
• The return of venous blood to the heart is compromised.
• Poor air entry into good lung.
• All open or sucking chest wounds should be treated by applying an occlusive material to cover the defect.

Military Use Valve Chest Seals
• Valve Chest Seals are a self-adhesive occlusive dressing with a one-way Valve.
• Clean area around the wound using the pull-off gauze.
• Remove paper backing from the adhesive side of the Chest Seal.
• Apply carefully to the chest with the Chest Seal hole lined up over the wound.
Asherman Chest Seal

Expedient Chest Seal
• The occlusive material used in a chest seal may be any nonporous material such as plastic wrap or foil.
• The critical action is to
seal the chest wound.

Apply a Valve or Occlusive Chest Seal To Any Penetrating Wound Between the Navel and
Shoulder

The Chest Seal edges should be covered with tape when possible.
- Place a conscious casualty in the sitting position
(if possible).
- Place unconscious casualty in recovery position
(injured side down}
- Monitor for possible development of further difficulty such as a “Tension Pneumothorax”.
Reinforce The Chest Seal If Possible

The Tension Pneumothorax
• Small entrance wound allows air in the pleural space.
• Lung collapses, air continues to leak from damaged lung.
• Air is progressively trapped under increasing pressure.
• Increasing pressure presses on heart and trachea, and kinks major blood vessels.
Signs and symptoms develop over 10 – 60 minutes

Tension PneumothoraxA True Medical Emergency
Chest trauma PLUS…Chest trauma PLUS…• Increasing difficulty Increasing difficulty
breathing breathing • Chest pain.Chest pain.• ““Air hunger”. Air hunger”. • Increasing restlessness, Increasing restlessness,
agitation. agitation. • Increasing heart rateIncreasing heart rate• Progression into shockProgression into shock

Signs of a Tension Pneumothorax
Increasing cyanosis
Distended neck veins
Skin cold and “clammy”
Progressive difficulty breathing, air “hunger” and anxiety
Tracheal Displacement to normal side (late)
air bubbles under the skin
Stridor on Inspiration
Casualty becomes progressively worse

EMT Management Of Tension Pneumothorax
Done by EMT Medical Personnel
The Stop-Gap treatment for tension pneumothorax is to decompress the injured side of the chest cavity with a needle (needle thoracostomy).
This is done if a casualty has:1. Torso trauma
2. Increasing respiratory distress

2 to 3 finger widths
below the middle of
the collar bone
Needle Chest Decompression(Needle Thoracostomy)

Mistakes Made
• The midpoint of the mid-clavicular line is difficult to determine.
• Decompressions are being done too medially.
• Use entry point at or lateral to the nipple line The “Danger Box”

“What if the casualty does not have a tension pneumothorax when a needle
decompression is done?”
• If there is already a collapsed lung, blood, and air in the chest cavity.
• The needle won’t make it worse if there is no tension pneumothorax.

Broken Ribs Can Cause a Tension Pneumothorax.
• Broken Ribs puncture lung causing a closed Tension Pneumothorax.
• Hemothorax develops due to bleeding from the damaged lung tissue.
• Tension pneumothorax develops from air leaking from the collapsed lung into the closed chest cavity.
No visible penetrating injury

Tension pneumothorax is the second leading cause of preventable death in blast and ballistic trauma.
• In a casualty with progressive respiratory distress and known or suspected torso trauma, consider a tension pneumothorax.
• Alert EMS personnel about your casualty’s condition.
• EMS are trained to decompress on the side of the injury with a 14-gauge, 3.25 inch needle/catheter unit inserted in the second intercostal space at the mid-clavicular line.
• Frequently reassess

The Definitive Surgical Treatment for 80% of Penetrating Chest Wounds
Surgical Chest Tube
with Underwater
Drain

Blunt Trauma InjuriesBruising Indicates Blunt Trauma Has Occurred
• Possible Broken Ribs
• Possible Underlying Lung Contusion
• Possible Development of Tension Pneumothorax
• Severe Blunt Force Trauma May Have An Associated Head Injury

The Flail Chest Injury
• Flail chest caused by extreme blunt trauma.
• Mechanisms can be car accidents, falls, blasts etc…
• Defined as a break of two or more ribs in two or more places.
• The injured chest wall falls inward on inspiration.

Emergency Treatment Of Flail Chest
• Current concepts for medical treatment of a flail chest is conservative.
• Position casualty in lateral prone position (recovery position) to improve lung function.
Injured side goes down.
• Monitor for Tension Pneumothorax

Lung Ventilation / Perfusion Improved In Lateral Prone Position
“Immediate Care of the Wounded ,“ C.C. Cloonan , 2007, Brookside Associates, Ltd.

Finish The Front Survey For Injuries
• Quickly check abdomen for bruising or penetrating injury.
• Check the pelvis before lifting or rolling the casualty to examine the back.

Physical Exam : Assess Pelvic Stability
Grasp iliac wings and assess AP stability
Check for lateral stability
If pelvis is intact it is safe to move the patient to examine the back
Gently manipulate the pelvis by squeeze and rock.

Indications Of a Pelvic Fracture
• Local pain / tenderness on pressure
• Perineal bruising associated with a high-energy injury, strongly suggest a possible pelvic fracture.
• Look for perineal swelling and bruising above inguinal ligament.
• Take extreme care when moving the casualty.

If Pelvis is Intact Finish The Survey By Examining the Back
• Lift or roll casualty to examine the back.
• Apply an occlusive cover to any penetrating injury between the top of the hips and shoulder.

Respiration Summary
• Penetrating chest wounds should be closed immediately with an occlusive material, either a vented chest seal or some type of plastic occlusive dressing.
• Monitor the casualty for the development of a tension pneumothorax.

Respiration Summary
EMS personnel need to perform needle decompression for any casualty with chest trauma with a progressive respiratory distress.

Needle Decompression Done by EMS Personnel
• Chest exam– Exam for holes– Exam for Tension– Demo JVD– Talk through needle
drill
If the 2 ICS-MCL cannot be used, keep to the outside of the nipple line
2 ICS-MCLD
an
ger B
ox

Constructing an Individual Medical Kit for S.C.A.B. Management
• Commercial Tourniquet
• 3 x Ace Wraps
• 3 x Curlex packing
• 1 x Chest Seal
• 1 x NP Airway
• 1 x Hemostatic Gauze

5-minute Break

The Preventable Causes of Death in Blast and Ballistic Trauma Have now Been Addressed

“Head to Toe”“Treat as You Go”
Perform Another Survey to Assess For Other Injuries

Reassess the Casualty
• Is Casualty in Shock ?
• Identify Possible Head and Eye Injury
• Prevent Hypothermia
• Splinting

Determine if Casualty is in Shock
• Reassess all previous hemorrhage control
• Check to see if the casualty is in shock:
- Assess level of consciousness.
- Look for a pulse in the wrist. If both arms are injured, assess the femoral pulse in the leg.

What Is Hypovolemic Shock ?
• Caused by any significant reduction in cardiovascular system blood volume.
• Commonly due to hemorrhage.
• Can be due to other significant fluid loss:– Severe burns.– Protracted vomiting, diarrhea,
sweating.– Fluid shifts i.e. smoke inhalation.

Hypovolemic (Hemorrhage) Shock
• Blood volume has decreased to the point where blood flow through the capillaries is sluggish or has stopped.
• Cells switch from aerobic to anaerobic metabolism, energy production decreases.
• Lactic Acid and other waste products build-up.
• Cells / tissues in internal organs begin to die.

Hypovolemic (Hemorrhage) Shock
1500ml Loss
Alert / Anxious
Death Unlikely
2000ml Loss2000ml Loss
Confused / LethargicConfused / Lethargic
Possible DeathPossible Death
2500ml Loss
UnconsciousUnconscious
Death Death ProbableProbable
Radial Pulse Weak
Pulse 100
Respiration 30
Radial Pulse Weak
Pulse 120
Respiration 35
Femoral Pulse Weak
Pulse 140
Respiration >35
Class II Shock Class III Class IV

Casualties May Also Have Hidden Blood Loss
Hemothorax 1 Liter
Pelvic Fracture 1 Liter
Long Bone Fracture 500ml
2500ml
Well conditioned athlete has greater fluid and cardiac reserves, so a greater blood loss needed to progress through stages. Casualty may suddenly crash.

The “Golden Hour”
As the time between an injured patient developing serious shock (loss of radial pulse) and the onset of resuscitation increases, the percentage of surviving patients decreases.
The survival rate after 1 hour of severe, untreated shock is very low.
Death of Wounds 4-10 days later
Minutes
50
0
100
30 60 90
Perc
en
t S
urv
ival

Assess For ShockAVPU Consciousness Level
Decreasing consciousness is the best quick indication of shock in a non-head injured patient.
U - Unresponsive
A – Alert V – Verbal
P – Pain Responsive
“Open your eyes”

Location of the Pulse Helps To Determine Shock
Carotid (60mmHg)
Radial (80mmHg)
Femoral (70mmHg)
Pedal (90mmHg)

The Radial Pulse Is Lost In Significant Shock
• Check for a Radial Pulse in a non-injured arm.
• Note if the pulse is normal or fast.
An altered level of consciousness combined with a lost radial pulse, indicates significant shock is present
Copyright 2009 ATS Inc., LLC

Reassess Any Prior Tourniquet Application
• Expose wound and determine if tourniquet is needed. If so, apply another tourniquet 2-3 inches above wound and this time, apply directly to the skin.
• Remove 1st Tourniquet and ensure pulse is absent.
• If a distal pulse is still present, tighten the tourniquet to eliminate the pulse.
• Note the time of tourniquet application for later recording.

Diagnosis Of Shock
Clinical indicators of Significant Shock;– Decreased consciousness – Wrist pulse weak or absent.– Heart rate > 120 bpm.– Continued bleeding from non-compressible
wound.– Color- pallor/pale.

Elevating the Legs is NOT a Stop-Gap Treatment For Shock
• Elevation of the legs was a procedure adopted during WW I as an anti-shock technique.
• Continues to be popular despite repeated evidence that it has no effect in shock. (J. Trauma 1982; 22:190-193).
• The best management of hemorrhagic shock is to stop blood loss and replace lost circulatory fluid by using IV Fluids.

EMS Will Administer IV to Casualties in Shock
• Aggressive fluid resuscitation to normal BP level in severe trauma is dangerous.
NOT All Casualties Get an IV

Aggressive Fluid Resuscitation in Uncontrolled Hemorrhage Is Bad
Large Prospective Trial Bickell et al NEJM 1993
598 patients penetrating torso trauma /shock
• Aggressive fluid resuscitation -survival rate 62%.• No aggressive fluid replacement- survival rate 70%.
If bleeding is not controlled (internal) – fluids may hurt rather than help because raising the blood pressure to normal may increase the bleeding.

No Aggressive Fluid Resuscitation in Uncontrolled Hemorrhage
Large Prospective Trial Bickell et al NEJM 1993 • 598 patients-penetrating torso trauma and hypotension.• Aggressive fluid resuscitation - survival rate of 62%.• No aggressive fluid replacement - survival rate of 70%.
• IV dilution of clotting factors. • Raising the blood pressure may increase bleeding.
• Permissive hypotension is allowed in all but severe head injury,

Head to Toe, Treat As You Go.
• Hypothermia• Head• Bandaging and Splinting• Burns and eye injury

Hypothermia and Shock
Hypothermia
Severe casualties do not produce enough body heat to stay warm.
Hypothermia occurs in Shock, even in hot environments.
Hypothermia decreases blood clotting and is a major factor in trauma death.

Prevention of Hypothermia
• Minimize Exposure
- Keep clothing on
- Expose only to treat wounds
- Replace wet clothing with dry
- Replace body armor
• Wrap Casualty
- Space Blanket, Dry blanket - Poncho liner, sleeping bag,
- Body bag, or even a trash bag liner.
Hypothermia Prevention Kits are available.

Small Individual Hypothermia Prevention Kit
• Space Blanket
• Chemical Warmers
- Tape to femoral pressure points
- Tape to axillary pressure points

Quickly Assess For Serious Head Injury
Monitor AVPU and note anychange
• Examine for depressed fractures and small wounds
• Check Pupils if possible
• Bleeding into brain may be evident by development of unequal pupils
• Alert EMS Personnel

Splinting Of Skeletal Fractures
• Open Fracture – Overlying skin is broken.• Closed Fracture – Overlying skin intact.

Clues to a Closed Fracture
• Trauma AND;
• Marked swelling
• Audible / perceived snap
• Length or shape of limb
• Loss of pulse or sensation
• Crepitus
• PAIN

Basic Fracture Management
Expose WoundPack and Pressure Dressing For Bleeding
Immobilize by Splinting

Fracture Splinting
Splinting Objectives:
• Prevent further injury
• Protect arteries and nerves - Check pulse before and after splinting
• Make casualty more comfortable

Splinting Materials
• Commercial
• Other body part
• Field expedient
Improvised
SAM Splint

Splinting Principals
• Try to splint before moving casualty.
• Give Pain Meds if not contra-indicated.
• Give Combat Pill Pack
• Splint in position of function.
• Pad bony prominences.

The Splinting Rule of Two’s
– Two Pulses (check before and after splinting).
– Two Ties (immobilize)• One above the injury• One below the injury
– Two Joints• One tie above the joint• One tie below the joint

It is Essential To Check For a Pulse After Splinting
• Major blood vessel pinched-off with progressive limb tissue death.
• Neurological damage with partial limb paralysis can also occur.

Things to Avoid in Splinting
• Minimize manipulation of extremity before splinting to avoid damaging blood vessels or nerves.
• Do not wrap the splint too tight and cut off the circulation to tissues below the splint.

Special Splinting Problem The Shattered Limb
• Use traction when moving limb• Long splint underneath extremity to stabilize the tissue.• Slightly-tight elastic bandage wrapped circumferentially.

Special Splinting ProblemEmergency Pelvic Stabilization
• Tie both feet and legs together.
• Use cargo belt or elastic
bandage below Pelvic Crest to stabilize the pelvis.

EMS Transport of Suspected Pelvic Fracture
• Tie feet and legs together. • Use of hard stretcher
• IV started for suspected posterior fractures

Special Splinting Problem Impaled Objects
Do not remove impaled objects…
• EMS will remove object only if:
• It prevents opening an airway, stopping life threatening hemorrhage, or prevents casualty evacuation.
Splint Object in place

Special Bandaging ProblemAcute Red Eye
• Any pain in the eye associated with exposure to shrapnel must be considered to be an open globe until an ophthalmologist says otherwise, especially in the setting of shrapnel injury to the face.
Iris Prolapsed

Special Care Must Be Used in Bandaging the Open Globe
• Aqueous Humor (low viscosity) fluid in the anterior chamber of the eye.
• Vitreous Humor (high viscosity) fluid in the posterior chamber.
• Care must be taken not to exert pressure on the eye in an open globe injury, to avoid further fluid loss from these chambers.

Eye Bandaging Obvious Open Globe
Field Expedient

Penetrating Eye Trauma
• Shield obvious or suspected eye wounds.• Avoids preventable and permanent loss of vision• Sunglasses / eyeglasses can be used for this purpose
Shield after injury No shield after injury

Penetrating Eye Trauma
If a penetrating eye injury is noted or suspected:
• Cover eye with rigid shield (NOT a pressure patch-do not allow shied to touch eyeball .)
• URGENT medical evacuation

Special Bandaging Problem Burn

Fluid Requirements In Second and Third Degree Burns
• Tremendous fluid requirements are associated with 30 burns.
• Shock can occur in 30 burns that cover over 10% body surface area (BSA).
• Early IV fluids.

Basic Early Burn Management
• Stop the Burning Process.
• Wrap affected area in loose Curlex.
• Early Airway Management following facial and inhalation burns.
• Alert EMS for burns greater than 10% BSA
• Prevent hypothermia.

Waiting for EMS

Waiting for EMS
• Establish a CCP.
• Reassess all Field Treatments
• Monitor Vital Signs, look for deterioration
• Identify most serious cases to EMS

Positioning The Casualty While Awaiting EMS
• Conscious casualties should be encouraged to sit upright - if not in shock.
• This may help the breathing. Makes it easier to watch the casualty for additional difficulty.
• Unconscious or casualties in shock are placed in the recovery position.
• Unconscious thorax injuries, place casualty with injured side down.

Record the Time of Tourniquet Application
• Writing “T” on the casualty’s forehead does not work well.• Ink marker on tape applied to the casualty’s chest. • Package for hypothermia and transport• Identify most serious casualties to EMS

10 Triage Rules of Thumb
IMMEDIATE TACEVAC
• Shock.• Penetrating wounds to the chest with respiratory distress
unrelieved by needle decompression.• Face / neck trauma with airway problems. • Head trauma with consciousness.• Globe damage to eye.• 3d degree burns > than the surface area of one arm.
DELAYED TACEVAC
• Obvious brain damage + unconsciousness (Expectant).• Extremity bleeding controlled with Tourniquet. . • Soft tissue injuries don’t kill unless associated with shock.
Copyright 2009 ATS Inc., LLC

5-minute Breakand
Prepare for Individual Practice of S.C.A.B. Techniques

The Mass Casualty Scenario

Mass Casualties
A mass casualty situation is when there is one more
casualty than you can manage.
• There are 4 critical rules for managing a battlefield mass casualty situation.
• Failure to adhere to any one of these principles will result in excess casualty morbidity and mortality.
Copyright 2009 ATS Inc., LLC

Military Concept For Managing Multiple Casualties
Win the Fight or Control the Situation• Take a few seconds to assess the situation and the area
over which the mass casualties are spread.
• Select a potential Casualty Collection Point with good cover.
• Send recovery personnel to perform TCCC only to the extent of Control Catastrophic Hemorrhage.
• Move all casualties into a secure CCP
- All unconscious casualties are put in recovery position
Copyright 2009 ATS Inc., LLC

Rule 1:Establish a Casualty Collection Point
• Perimeter Security is established with Close Security around casualties being treated.
• All the casualties in the CCP are grouped close together for monitoring, medical C&C, and triage of medical supplies.
Copyright 2009 ATS Inc., LLC

Rule 2. Set up the CCP Correctly !! Catastrophic Hemorrhage Control is the Priority
• Arrange the casualties in a line with all heads facing the same way, or in a star with all heads pointing inwards with a Corpsman or medic, in the center.
• Corpsman/Medic works at the casualty’s head. Nonmedical personnel work from the foot-end and can be directed by the Corpsman/Medic.
• Keep enough space between casualties to
sit down to start an IV.
Copyright 2009 ATS Inc., LLC
M
M

Rule 3. Someone Must Take Charge of the CCP
(This Should Not Be the Medic or Corpsman).
• The individual in charge of the CCP cannot also be involved in providing medical treatment.
Copyright 2009 ATS Inc., Le
• The individual in charge of the CCP will :
- Manage the triage of medical supplies. - Keep track of the triage priorities of the casualties. - Make the initial TACEVAC request. - Control the security of the site.

Rule 4. Corpsman or Medic Will Use Operators
As Medical Assistants
• Once all life-threatening hemorrhage is controlled, all casualties are assessed for an adequate Airway.
• Corpsman / Medic will assist with complicated hemorrhage control and assist with complicated airway cases.
• At the same time, Corpsman / Medic will use Operators as Medical Assistants to perform the TCCC protocols for MARCH-E on all casualties.

Analysis of the Boston Marathon Bombing

Significant Event Planning by Boston EMS Special Operations Unit
– Large medical tent for race injuries. Dispatcher dedicated solely for marathon communications
– Medical response geared towards dehydration, exhaustion, and other race related injuries, not massive trauma.
– 50 additional EMS personnel strategically placed at
medical tents, water stations, on bicycle, 4-wheeled ATVs, and ambulances throughout the race route.
– 4 physicians on site for the event.

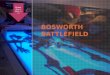
Boston Marathon
Finish Line
Medical tent
Boylston Street

• Explosions 12 seconds apart • No tertiary devices • Casualties 3 Dead • 264 Wounded
April 15, 2013 20:50.00 PM



Use of Field Expedient Devices
• Are there First Aid Kits in any of the surrounding shops and stores?
• What in the blast debris would be useful for constructing an improvised tourniquet ?


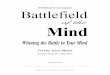
Explosive Device

• Explosions 12 seconds apart • No tertiary devices • Casualties 3 Dead • 264 Wounded
550 feet
12-Seconds Later Second Explosion





Can this patient hear ?



Explosive Device

Blast Analysis
• 2 Devices 6L Pressure Cookers filled with gunpowder from fireworks
–Black bags (duffel or back packs) Shrapnel Metallic BBs and Nails, contained with adhesive
• RC car remote • Hobby fuse • Yechnique detailed in AQ Inspire article

Medical tent already treating dozens for race injuries.
• Shortly following blast medical tent became
trauma center Staff began triage.
• Tent did have small number of tourniquets
available • By 1600L most patients moved to hospitals

Medical Tent Equipped to Handle Marathon Runners

Casualties Begin to Flow Into Medical Tent
Boston Globe



Rapid Medical Tent Reorganization






Transport to Area Medical Hospitals

Incident Time Line
• 3 Dead, 264 Wounded –16 Amputees –3 of which were multiple amputations –10 children among wounded
• Most injuries to lower extremities




General Notes
• Physicians and EMS personnel were already on-site for the Boston Marathon.
• Treatment tent was able to be rapidly reconfigured for trauma.
• A few tourniquets were available in medical tent but not brought to incident site. Airway problems in casualties were minimal.
• Bystanders had to try and provide initial life saving measures

General Notes
• Police were first on the scene but had no training in controlling hemorrhage and no lightweight tourniquet or pressure bandage.
• No secure CCP established and the scene remained essentially unsafe throughout the response, due to the potential risk of secondary explosive devices.

General Notes
• Civilian man-made mass casualty blast and ballistic events are becoming more frequent and such incidents can be expected to continue.
• Bystanders may be the initial first responders.
• The ability to control catastrophic hemorrhage and provide an airway should be a basic skill of every police officer on the street. It is not.

The National TECC Committee
• The concept, workshops, EMS doctrine, and equipment for Tactical Emergency Casualty Care have been promoted for the three years.
• A National TECC Committee exists.
• The doctrine is being adapted too slowly or not at all by many EMS departments and even fewer Police Departments.

Resources
• Boston Globe • •http://www.cnn.com/2013/04/15/us/boston-marathon-things-
we-know/index.html • •http://us.cnn.com/2013/04/15/us/boston-bombings-injuries/?
iref=obinsite • •http://www.boston.com/lifestyle/health/blogs/white-coat-
notes/2013/04/15/marathon-medical-tent-transformed-into-trauma-unit/gUAgQIMwTYqwzRkcIDs5PJ/blog.html
• •http://canton.patch.com/articles/boston-marathon-explosions-medical-tent-nurse-describes-monday-scene-to-canton-patch
• •http://espn.go.com/video/clip?id=9175656 • •http://healthybostonblog.wordpress.com/2013/

Questions and Discussion