Embed Size (px)
Citation preview

Prepared by Dr Teresa Anderson Chief Executive
July 2010
2011/12 Service Agreement SLHD

Performance Framework • New Performance Management Framework which specifies
targets and goals and measures relative performance.
It assumes significant LHD autonomy as to how it will achieve performance and service expectations
It specifies the key minimum performance standards and thresholds, and specifies what level of performance will trigger closer Ministry support and scrutiny
It aims to create transparency of expectations. But leave Districts free to identify other areas of performance important for our local communities and clinicians
A framework has been developed to provide a consistent approach for working with Affiliated Health Organisations

Performance Framework
provides a clear and transparent outline of how the performance of Local Health Districts is assessed
outlines how responses to performance concerns are structured.
It provides a single, integrated process for performance review, escalation and management, with the over-arching objectives of improving service delivery, patient safety and quality.
The objectives of the LHD Service Agreement
To enable the Local Health District to deliver a coordinated, high quality health service to the communities serviced by the District and to support its teaching, training and research roles.
To clearly set out the service delivery and performance expectations for the funding and other support services provided to the District.
To promote accountability to Government and the community.

The objectives of the LHD Service Agreement
To ensure NSW Government and national health priorities, services, outputs and outcomes are achieved.
To establish with the Local Health District a Performance Management and Accountability System that assists the achievement of effective and efficient management and performance.
To provide the framework for the Local Health District Chief Executive to establish service and performance agreements within the Local Health District.

The objectives of the LHD Service Agreement
To facilitate the progressive implementation of a purchasing framework incorporating activity based funded services
To address the requirements of the NHRA in relation to Service Agreements, noting that the requirements will commence at different stages over a number of years.

Strategic Directions- Quality and safety
Priorities for all LHD
– Accreditation of Health Services
– Patient Satisfaction
– Patient Safety
SLHD additional priorities:
– Infection control
– Conscious sedation
– Clinical Handover
– Surgical/Procedural supervision
Strategic Directions- Patient Flow
Priorities for all LHDs
– Surgery Emergency Surgery Guidelines/ Predictable Surgery Program
– Patient Flow Systems and Predictive Capacity Planning
– Models of Care
– Integrated Clinical Service Networks and Plans
– Appropriate Utilisation of Hospitals
– Community Health Services

Strategic Directions- Patient Flow
Priorities for all LHDs
– Mental Health
– Aboriginal Health
– Dental Health
SLHD’s additional priorities:
– Ongoing Networking with SWSLHD
Strategic Directions- Finance & Management
Priorities for all LHDs
– National Agreements and Initiatives
– Performance Management Framework (PMF)
– E-Health Information and Communications Technology (e-health ICT)
– Workforce Action Plan
– Best Practice Financial Management
– Activity Based Funding costing.
– NSW Public Sector Workplace Health and Safety and Injury Management Strategy 2010 – 2012 -

Strategic Directions- Finance & Management
SLHD’s additional priorities:
– Staffing levels
– Workforce Development – continued implementation of programs to develop managers for the future including the DBA, Masters of Business Administration, Masters of Clinical Management and the Postgraduate Management Program
– Business Management

Strategic Directions- Population Health
Priorities for all LHDs
– Population health - Provide preventive care
– Connecting Care Program
– Aboriginal Health Strategies
– Keep Them Safe
– Emergency Response Planning and Readiness
SLHD’s additional priorities:
– Out of Home Care
– Aged Care
– Chronic disease management

KPIs Target
Not Performing
X
Underperforming
Performing
Safety and Quality
Tier 1
Staphylococcus aureus bloodstream infections (SA-BSI) (per 10,000 occupied bed days)
2 > 2.5 > 2 and < 2.5 < 2
Tier 2 Central Line Associated Bloodstream (CLAB) Infections (number)
0 > 1 N/A 0
Tier 2 Incorrect procedures (operating theatre) resulting in death or major loss of function
0 > 1 N/A 0

Patient Flow
Tier 1 Ambulance Transfer of Care - < 30 minutes (%)
90 < 75% > 75% and < 90%
> 90%
Tier 1
Emergency Department Triage 3 – Cases treated within benchmark times (%) (within 30 minutes)
75 < 70% > 70% and < 75%
Target of 75% met or better
Tier 1
Emergency Admission Performance - Patients transferred to an inpatient bed within 8 hours of arrival in the ED (%)
80 < 75 % > 75 % and < 80%
> 80%
Tier 1
Overdue planned surgical patients (number):
• Category 1
0 > 5 >0 and <5 0
• Category 2 0 > 25 >5 and <25 <5
• Category 3 0 > 25 >5 and <25 <5
Tier 1
Unplanned hospital readmissions within 28 days of separation (%):
< Previous year
> 2% points above previous year
< 2% points above and >
previous year
< Previous
year
[
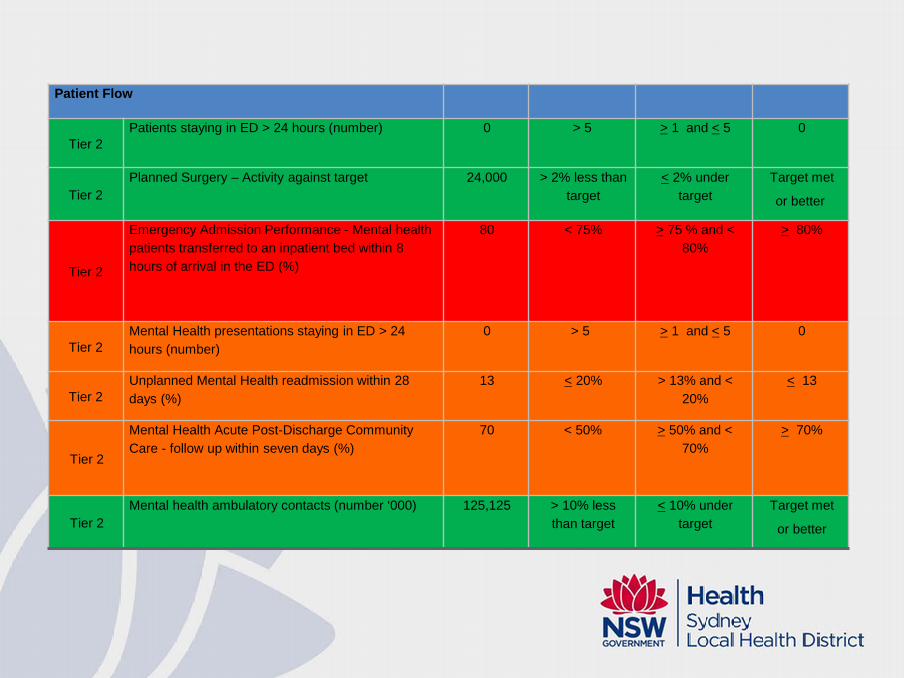
Patient Flow
Tier 2 Patients staying in ED > 24 hours (number) 0 > 5 > 1 and < 5 0
Tier 2 Planned Surgery – Activity against target 24,000 > 2% less than
target < 2% under
target Target met
or better
Tier 2
Emergency Admission Performance - Mental health patients transferred to an inpatient bed within 8 hours of arrival in the ED (%)
80 < 75% > 75 % and < 80%
> 80%
Tier 2 Mental Health presentations staying in ED > 24 hours (number)
0 > 5 > 1 and < 5 0
Tier 2 Unplanned Mental Health readmission within 28 days (%)
13 < 20% > 13% and < 20%
< 13
Tier 2
Mental Health Acute Post-Discharge Community Care - follow up within seven days (%)
70 < 50% > 50% and < 70%
> 70%
Tier 2 Mental health ambulatory contacts (number ‘000) 125,125 > 10% less
than target < 10% under
target Target met
or better

Finance and Management
Tier 1 Cost weighted separations – Year to Date
140,377 > 2% less than or above
target
< 2% under or above
target
Target met
Tier 1
Expenditure matched to budget (General Fund): Year to Date; June projection
a) Year to date - General Fund (%) +/- 0.5 > 2.0% Unfavourable
> 0.5% but < 2.0%
Unfavourable
Favourable
or < 0.5% Unfavourable
b) June projection - General Fund (%)
0 > 1.0% Unfavourable
< 1.0% Unfavourable
On budget or Favourable
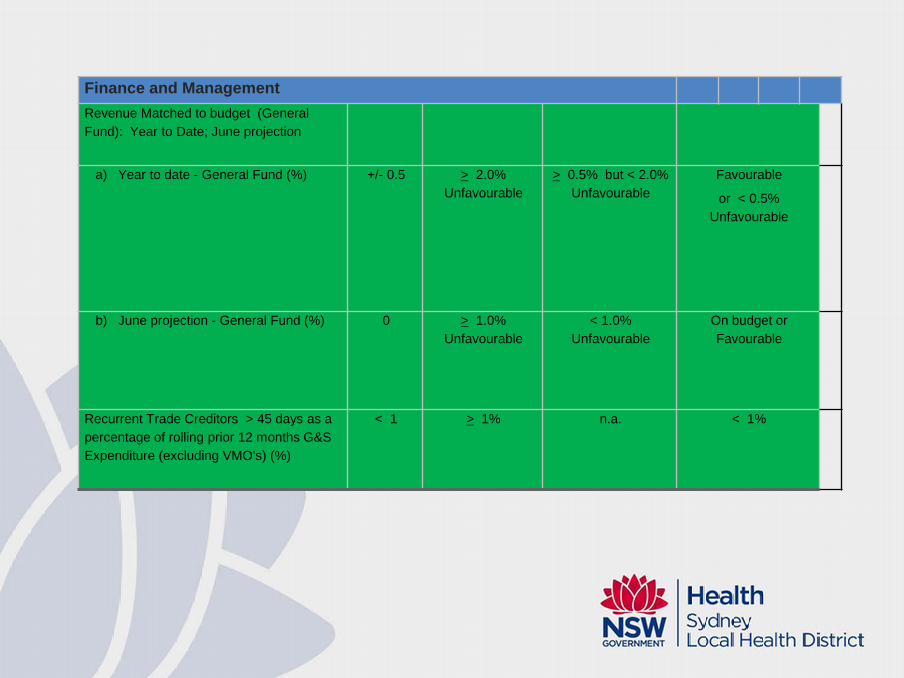
Finance and Management Revenue Matched to budget (General Fund): Year to Date; June projection
a) Year to date - General Fund (%) +/- 0.5 > 2.0%
Unfavourable > 0.5% but < 2.0%
Unfavourable Favourable
or < 0.5% Unfavourable
b) June projection - General Fund (%) 0 > 1.0% Unfavourable
< 1.0% Unfavourable
On budget or Favourable
Recurrent Trade Creditors > 45 days as a percentage of rolling prior 12 months G&S Expenditure (excluding VMO's) (%)
< 1 > 1% n.a. < 1%

Finance and Management Coding timeliness -Separations coded six week post discharge (%)
95 < 85% > 85% and < 95% > 95%
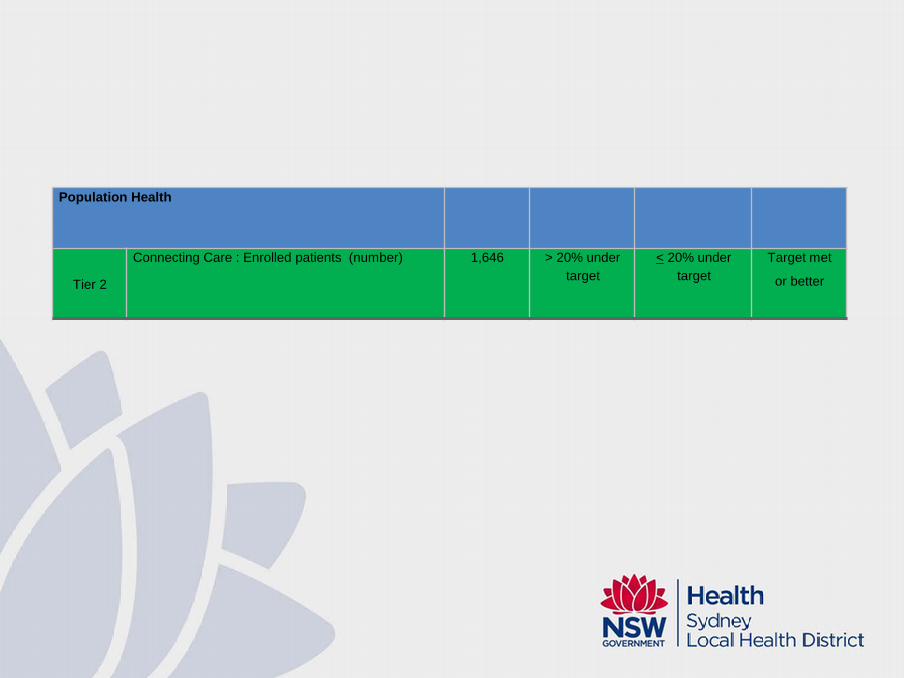
Population Health
Tier 2
Connecting Care : Enrolled patients (number) 1,646 > 20% under target
< 20% under target
Target met
or better

Tier 1: Areas of Risk Off Stretcher Time
Triage 3
Emergency Admission Performance

Strategies: Trial ambulance release teams
Enhanced escalation processes
Commencement of new Offload data collection system
Trial new ambulatory care models at RPAH, Concord and Canterbury as an alternative to ED
Strengthening the MAU
Inpatient co-ordinate care i.e. Fast Track
Tier 2: Areas of Risk
Central Line Associated Bloodstream (CLAB) Infections (number)
Mental Health Access- inpatient and community

Strategies: CLAB infections
Strategies implemented to reduce reoccurrence
Review of appropriate use of antibiotics with Infectious Diseases approval.
Strict adherence to Hand Hygiene and conduct regular hand hygiene audits
Further focus on ensuring the removal of infected Central Venous Catheters occurs according to guidelines
Further focus on ensuring that the insertion and maintenance of CVC occur according to guidelines (completing checklist and data collection form)

Strategies: CLAB infections
Daily review of line necessity
Maintaining competency packages for medical and nursing staff.
All CLABs will now be presented and reviewed at the District Infection Control Meeting to assist with peer learning
Environmental control strategies other than cleaning in other areas e.g. burns unit engineering action (minor modifications to drains, waste traps, showerheads, etc) in addition to additional cleaning

Strategies: CLAB infections
Models of care review in relation to management of central lines
Options for response to tourniquet study findings
Antibiotic stewardship
Plan for improved awareness of infection control procedures for non-ICU staff who enter the ICU.
Centralisation of PICC and CVAD insertion so there is a consistent and standardised process and environment for the insertion of these devices.
Strategies: Mental Health
Enhance community teams to improve follow-up and management out of hospital
Investigate alternate models of care

SLHD 2011/12 BUDGET ALLOCATION
Conditions of funding
comply with the provisions of the relevant Accounting Manual and the Accounts and Audit Determination for Public Health Organisations.
ensure compliance with specific conditions attached to funding.
correctly differentiate between General Fund and Special Purpose and Trust Funds.
operate within approved Net Cost of Services for both General Fund and Special Purpose and Trust Funds.

achieve approved Efficiency, Revenue and Turnaround Plans.
pay creditors within benchmark.
report on financial performance on a monthly basis through SMRT with accompanying narrative and submit financial reports and narratives by the 10th calendar day
Determination of LHD Budget allocations 2011/12 LHD budget allocations have been developed based on the
following key components:
– Annualised 2010/11 base budget including the 2010/11 COAG funded beds
– Escalation for background cost increases- approved award increases, increase nursing hours/patient and general CPI
– Additional funding for new services, specific election commitments and state priorities
Growth agreed between NSW Min of Health and LHD at hospital level for acute inpatients and/or ED activity funded at the marginal rate of 50% of the nominal price

Funding Recall strategy
Activity above the target - no additional funding will be provided
Activity below target- Ministry will recall funded (unless agreed as a change of model of care) based on marginal rates of the nominal price- LHD receiving recall advice will be requested to submit to the Ministry, explanation for the reduction in activity and a proposal to make up the activity shortfall. If such a proposal is agreed then recall will not be activated at that time.
LHD are to determine their own strategy for managing over and under target activity of individual hospitals with the overall activity targets.

2011/12 Expense, Revenue and Net Cost of Service Initial budget by fund type and cost line item

Net Cost of Service – Budget Allocation Account Class by Fund

Expenditure Issues
Whilst the budget suggests an increase of $44.292 m, many of the items esp. additional beds are not new as expenditure has already been incurred in 2010/11 and are now annualised in 2011/12 ($14.3m)
High Cost drugs $3.08m is offset with revenue $3.08m
The net CPI increase is $2.9m)
Net nurses aware allocations is $8.89m ($9.34m-0.449m)

Expenditure Issues:
Total new enhancement is approx. $12.377m
– ED strategy $0.285m
– Nursing hours $5.017m
– Nurses $0.208m
– LHD governance $0.169m
– General growth $6.698m

Revenue Issues
Enhancement increase of $0.964m
HCD rev. $3.083m will offset increase in exp. of $3.083m
HACC rev of $10.324m represent funding will come to SLHD via revenue income instead of Health subsidy- little impact unless Commonwealth reduces funding
Summary
The budget will be tight again in 2011/12
Budgets are currently being allocated to Facilities based on the historical budget plus escalation. SMRT- ABF system is being implemented to facilitate reporting of activity and expenditure
Activity targets are being allocated to facilities for acute, ED, ICU and Sub-acute care episodes

Risks
Not meeting the activity targets and having budget recall. Action: regular feedback to facilities and clinicians, implementation of ABF initiatives
Uncertainty associated with HACC funding into the future- HACC funding ($10.3 m now transferred from subsidy to revenue)- impact on Staff FTE expenditure- LHD has to manage excess staff if funding is reduced- Action: Balmain budget to be reviewed
Nursing hours provision ($5m) dependent on recruitment of positions to designated wards- Action: staffing levels will be monitored and funds will not be allocated to facilities until staff appointed
Risks
Management of staff expectations- COAG beds established in 2010/11 annualised in 2011/12. no new funds. Acton: regular feedback/ communication with clinicians and managers.
Meeting the increased revenue target. Action: LHD will need to drive revenue initiatives further, increased monitoring and feedback to facilities and clinicians
Growth of $6.698M less than 0.5% of total budget. Action: Growth funding will not be allocated in first 6 months.
1.5% efficiency and revenue target to be achieved. Action: implementation of the efficiency and revenue plan, regular monitoring of performance against targets.
Financial management strategies
Good cash management is about:
Knowing our budget
Knowing our commitments
Knowing our targets
Ensuring we have a clear plan for effectively managing our business
Recognising that we can’t spend more than we have in cash

Financial Management
Good cash management is about:
Recognising our responsibilities to our creditors
Having appropriate controls in place for expenditure
Frequent ongoing monitoring of expenditure against target

Managing staffing
The biggest driver of expenditure is salaries and wages
(around 65%), so we need to manage this by:
Establishing, disseminating and monitoring staffing targets
Ensuring effective controls are in place for all aspects of staffing – Recruitment (including walk-ins) – Overtime – Use of casuals – Use of agency staff – Extension of hours of part time staff

Managing staffing Ensuring effective governance including delegations, regular
meetings
– All recruitment (permanent/temporary) requires GM and CE/DOO approval
– Regular meetings with the CE/DOO to review performance against targets
– Individual
– Facility Executive
– Area Manager’s Meeting
– Clinical Stream meetings
Ensuring reliable data/reporting is provided to drive performance

Recruitment Controls
All recruitment requests (including re-advertising): – are reviewed centrally following local and facility management
review – Nursing recruitment is reviewed with the Area Director of
Nursing – Medical recruitment is reviewed with the Area Director of
Medical Administration – have to be justified including a review of:
– the need for the position, – staffing mix and – model of care
– are considered in light of facility and cost centre performance against staffing targets
– are prioritised according to clinical and operational need

Recruitment Controls Temporary Appointments
– reviewed centrally following local and facility management review, – reviewed against cost centre performance and staffing target
Casuals – approved centrally by DOO following review by GMs – approved at a facility executive level prior to allocations
Agency – approved at a facility executive level
Overtime – All nursing and corporate overtime requires facility executive
approval (except JMO) – All JMO overtime reviewed by DMSs (monitored by Area Exec)

Reports Fortnightly and Monthly reports provided to facilities including: Detailed Fortnightly Staff Profile
– FTE Staffing against target/ previous year performance • By cost centre • By staffing classification
– Overtime – Agency – Casuals – Commencements/cessations
Extended contract hours VMO hours/salaries
Communication
Periodic prompts to focus attention on areas of concern e.g. memos to GMs re: exceeded contract hours, monitoring of overtime performance, use of casuals etc
Phone calls following receipt of monthly Staff Profile to highlight areas requiring analysis prior meeting with CE.
Reflection of LHD practices at a facility level
Promotion of healthy competition between directorates to enhance performance

Other strategies to manage staffing
Reducing activity during holiday periods to refresh staff and reduce annual leave liability
Actively managing sick leave
Recruiting casual staff instead of using overtime or agency staff
Reducing the use of locum medical staff
Restructuring services to gain staffing efficiencies (aged care, community health, youth health, JMOs)
New models of care