Embed Size (px)
Citation preview

1
2011 Vaeth Lecture2011 Vaeth Lecture
Sarah S. Donaldson, MDSarah S. Donaldson, MDStanford UniversityStanford University
Jerome M. Vaeth, MDJerome M. Vaeth, MD1925 1925 -- 19981998
Lessons in Radiation Therapy Lessons in Radiation Therapy from the Clinical Trials in from the Clinical Trials in
Pediatric Sarcoma ManagementPediatric Sarcoma Management
2011 Vaeth Lecture 2011 Vaeth Lecture Sarah S. Donaldson, MDSarah S. Donaldson, MD
Stanford UniversityStanford University
Clinical Trials Clinical Trials ––A challenge in pediatric cancerA challenge in pediatric cancer
•• cchildhood cancers are rare; need large hildhood cancers are rare; need large numbers, long follownumbers, long follow--upup
•• risk of late effects, often unknownrisk of late effects, often unknown•• barriers to overcomebarriers to overcome•• nneed to collaborate and participate in eed to collaborate and participate in
clinical trialsclinical trials

2
Participation in Clinical Trials by Age Ewing's Sarcoma – Chemotherapy + RadiotherapyPOG 8346 – Radiotherapy randomization
Standard whole boneStandard whole bone Experimental involved fieldExperimental involved field
Ewing's SarcomaProblemProblem
-- Many primary tumors are smallMany primary tumors are small-- IF same as whole bone IF same as whole bone -- No difference in 2 study groupsNo difference in 2 study groups
SolutionSolution-- Administer Rx to IF Administer Rx to IF -- Study patterns of failureStudy patterns of failure
OutcomeOutcome-- Local failures are centralLocal failures are central-- IF + chemotherapy became IF + chemotherapy became
standard of carestandard of care
Localized Ewing's Sarcoma – Treatment: Chemotherapy + Local Therapy
Radiotherapy or Surgery?
Induction chemotherapy 12 wks Randomize Rx Induction chemotherapy 12 wks Randomize Rx
Randomize to RT or ResectionRandomize to RT or Resection
Problem: Problem: Local therapy can not be predicted up front. Local therapy can not be predicted up front. Patients, families + physicians want to choose Patients, families + physicians want to choose their therapy.their therapy.

3
No randomized study comparing XRT vs SurgeryNo randomized study comparing XRT vs Surgery
Bias in selection factorsBias in selection factors
Resectable lesions are likely to be:Resectable lesions are likely to be:Smaller tumorsSmaller tumorsPeripheral rather than centralPeripheral rather than centralFollowing good response to induction chemotherapyFollowing good response to induction chemotherapyand may require postoperative, supplemental XRTand may require postoperative, supplemental XRT
Irradiated lesions are likely to be:Irradiated lesions are likely to be:NonNon--resectableresectableLarger tumorsLarger tumorsCentral (axial skeleton)Central (axial skeleton)Following poor response to induction chemotherapyFollowing poor response to induction chemotherapy
OSOS 69%69%
RFSRFS 69%69% 70%70% 7474%% 66%66%
LCLC 86%86% 100100%% 95%95%
CESS-86 Outcome @ 5 years
XRTXRT SurgSurg Surg + XRTSurg + XRT
Summary: Considering the selection criteria forSummary: Considering the selection criteria forlocal therapy, XRT yielded RFS & OS local therapy, XRT yielded RFS & OS comparable to radical surgerycomparable to radical surgery
Protocol DevelopmentProtocol Development
Look at what’s been doneLook at what’s been done
To know what to do nextTo know what to do next
Rewards from clinical trials ...Rewards from clinical trials ...CChildhood hildhood RRhabdomyosarcoma habdomyosarcoma -- IRSGIRSG
Grouping SystemGrouping System
I. Localized disease completely resected;
(Regional nodes not involved)
II. Grossly resected, microscopic residual (with or without regional nodal disease)
III. Incomplete resection, biopsy only, gross residual disease
IV. Metastatic disease
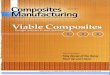
4
0
25
50
75
100
I II III IV
Clinical Grouping SystemClinical Grouping SystemIRS IIIRS II
1313 1717
5353
1717
%%
FFS by Group FFS by Group -- IRS IVIRS IV
0.0
0.2
0.4
0.6
0.8
1.0
YearsYears0 2 4 6 8 10
Group II
Group IGroup I
Group IIIGroup III
Group IV Group IV
P < 0.001P < 0.001
Group I Localized disease, completely resected
•• IRS I: Patients randomized to postoperative RT vs no RT
• Dose: 40 - 60 Gy in 1.5 – 2 Gy fractions
• Time: Immediately after surgery, week 0
• Conclusion: 5 yr DFS not improved by RT;RT for Grp I patients omitted
p < 0.001p < 0.001
IRS IRS –– I / II, with RTI / II, with RT
IRS IRS –– I / II, no RTI / II, no RT
IRS IRS -- III, with RTIII, with RT
IRS IRS -- III, no RTIII, no RT
Grp I Grp I -- Failure Free SurvivalFailure Free SurvivalAlveolar and Undifferentiated Sarcoma HistologyAlveolar and Undifferentiated Sarcoma Histology
0.00.0
0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
00 22 44 66 88 1010
Wolden et al. JCO 17: 3468, 1999Wolden et al. JCO 17: 3468, 1999

5
Group II Group II
a a -- Microscopic residual diseaseMicroscopic residual disease
b b -- Regional lymphatic spread, resectedRegional lymphatic spread, resected
c c -- BothBoth
Gross Total ResectionGross Total Resection
5 yr FFS Group II patients5 yr FFS Group II patients
IRS IV IRS IV 87 %87 %
Prognostic FactorsPrognostic Factors
-- EmbryonalEmbryonal histology vs otherhistology vs other
-- Subgroup II a / II b Subgroup II a / II b
-- IRS III / IV IRS III / IV
Local failure Local failure -- 8 %8 %
Regional Regional -- 4 %4 %
Distant Distant -- 14 %14 %
Smith et al. JCO 19:4058, 2001Smith et al. JCO 19:4058, 2001
Group IIIGroup III
Incomplete resection with Incomplete resection with gross residual diseasegross residual disease
5 Year Data, IRS5 Year Data, IRS--III, Group IIIIII, Group III
ENDPOINTENDPOINT
FFS 70 %FFS 70 %Survival 78 %Survival 78 %
FAILURE SITE FAILURE SITE
Local 19 % Local 19 % Regional 2 %Regional 2 %Distant 11 %Distant 11 %
Wharam et al. JCO 22:1902, 2004Wharam et al. JCO 22:1902, 2004

6
Factors Affecting Failure Factors Affecting Failure at 5 yrs: IRSat 5 yrs: IRS--III, Group IIIIII, Group III
FACTORFACTOR LOCAL (%)LOCAL (%) DISTANT (%)DISTANT (%)
All PatientsAll Patients 1919 1111
NNOO / N/ N11 16 / 3216 / 32 9 / 279 / 27
< 5 / ≥ 5 cm< 5 / ≥ 5 cm 16 / 2116 / 21 8 / 178 / 17
TT11 / T/ T22 14 / 1914 / 19 8 / 148 / 14
Wharam et al. JCO 22:1902, 2004Wharam et al. JCO 22:1902, 2004
Radiotherapy DoseRadiotherapy DoseIRS IRS -- III, Group IIIIII, Group III
AGEAGE < 5 cm< 5 cm ≥≥ 5 cm5 cm
< 6 yrs.< 6 yrs. 41.4 Gy 45 Gy41.4 Gy 45 Gy
≥≥ 6 yrs.6 yrs. 45 Gy45 Gy 50.4 Gy50.4 Gy
Local FailureLocal FailureAge, Tumor Size, and RT DoseAge, Tumor Size, and RT Dose
Age / SizeAge / Size Dose Dose Local Failure Local Failure
< 6 yr, < 5cm< 6 yr, < 5cm 41.4 Gy41.4 Gy 14 %14 %
< 6 yr, ≥ 5cm< 6 yr, ≥ 5cm≥ 6 yr, < 5cm≥ 6 yr, < 5cm
45 Gy45 Gy 23 %23 %
≥ 6 yr, ≥ 5cm≥ 6 yr, ≥ 5cm 50.4 Gy50.4 Gy 16 %16 %
p = .20p = .20 Wharam et al. JCO 22:1902, 2004Wharam et al. JCO 22:1902, 2004
RT Volume GuidelinesRT Volume Guidelines
IRS I Involved muscle compartmentIRS II Initial tumor volume + 5 cmIRS III Initial tumor volume + 5 cmIRS IV Initial tumor volume + 2 cmIRS V 3D – CRT to GTV + 1.5 cm CTV + 0.5 cm PTV*IRS VI IMRT – GTV + 1.5 cm CTV + 0.5 cm PTV*
* Volume reduction @36 Gy
Group IIIGroup III

7
Appropriate AppropriateAppropriate
Cumulative Incidence of Local Failure by Cumulative Incidence of Local Failure by QARC Guidelines and Quality ControlQARC Guidelines and Quality Control
Major or Minor DeviationMajor or Minor Deviation
6655 77 88 99 1010 1111 1212 1313 141444332211000055
10101515
20202525
30303535
4040
4545
5050
YearsYearsp = .012p = .012 Wharam et al. JCO 22:1902, 2004Wharam et al. JCO 22:1902, 2004
24 %24 %
15 %15 %
Conclusions / ChallengesConclusions / Challenges
•• IRS III, Group III local failure rate was IRS III, Group III local failure rate was unacceptably high for all primary sites, especially unacceptably high for all primary sites, especially NN1 1 patients.patients.
•• Optimal radiotherapy dose has not been Optimal radiotherapy dose has not been determined. determined.
•• Optimal radiotherapy volume has not been Optimal radiotherapy volume has not been defined.defined.
•• Role of delayed surgery has not been defined.Role of delayed surgery has not been defined.
•• Risk of local failure exceeds distant failure.Risk of local failure exceeds distant failure.
IRS IV Radiation GuidelinesIRS IV Radiation Guidelines
–– Group I Group I -- No RTNo RT–– Group II Group II -- 41.4 Gy (1.8 Gy / day)41.4 Gy (1.8 Gy / day)
–– Group IIIGroup III
–– Volume Volume -- GTV + 2 cmGTV + 2 cm–– Timing Timing -- Week 9 for all exceptWeek 9 for all except
PM with high risk features, day 0PM with high risk features, day 0
Conv Conv -- 50.4 Gy (1.8 Gy/ day)50.4 Gy (1.8 Gy/ day)HF HF -- 59.4 Gy (1.1 Gy bid)59.4 Gy (1.1 Gy bid)
Crist et al. JCO 19:3091, 2001Crist et al. JCO 19:3091, 2001
FFS by Type of RadiationFFS by Type of RadiationGroup III Group III
P = 0.76P = 0.760.0
0.2
0.4
0.6
0.8
1.0
Years0 5
ConventionalConventional
Hyperfractionated
Donaldson et al. IJROBP 51: 718, 2001Donaldson et al. IJROBP 51: 718, 2001

8
Response Driven Therapy Response Driven Therapy –– IRS IVIRS IV
RateRate FFSFFS
CR CR 22%22% 81%81%
PRPR 59%59% 72%72%
NRNR 19%19% 84%84%
P = 0.34P = 0.34 Burke M. JCO 25:4909, 2007Burke M. JCO 25:4909, 2007
End of Rx ResponseEnd of Rx Response 5yr FFS5yr FFS
CRCR 81%81% 80%80%PR/NR (residual mass)PR/NR (residual mass) 19%19% 78% 78% p = 0.4p = 0.4
Rodeberg, D, JCO 27:2009Rodeberg, D, JCO 27:2009
Rhabdomyosarcoma IRS IV, Group IIIRhabdomyosarcoma IRS IV, Group IIIResponse to therapy by imaging (CT / MR)Response to therapy by imaging (CT / MR)
•• Response to Rx does not predict outcome Response to Rx does not predict outcome (FFS / OS)(FFS / OS)
•• CR at end of Rx does not improve outcomeCR at end of Rx does not improve outcome
PR/NR (residual mass)PR/NR (residual mass) 8/16 (50%) have viable tumor8/16 (50%) have viable tumor
of whom only 3/8 with viable of whom only 3/8 with viable tumor obtain atumor obtain acomplete resectioncomplete resection
Rodeberg, D, JCO 27:2009Rodeberg, D, JCO 27:2009
Rhabdomyosarcoma IRS IV, Group IIIRhabdomyosarcoma IRS IV, Group IIIPathologic response after resection of residual mas sPathologic response after resection of residual mas s
•• Only 50% of residual masses represent viable tumorOnly 50% of residual masses represent viable tumor•• Resection of residual mass does not improve outcome Resection of residual mass does not improve outcome
(FFS or OS)(FFS or OS)
Rhabdomyosarcoma IRS IV, Group IIIRhabdomyosarcoma IRS IV, Group III
•• High risk of morbidity High risk of morbidity -- loss of organ function 5 8%loss of organ function 58%
•• Low likelihood of complete resection Low likelihood of complete resection 29%29%
•• Given the small benefit and the morbidity, there is no Given the small benefit and the morbidity, there is no justification for attempted resection of a residual mass justification for attempted resection of a residual mass at the end of therapyat the end of therapy
•• It is not necessary to extend treatment (surgery, It is not necessary to extend treatment (surgery, radiotherapy, or chemotherapy) of a residual mass a t radiotherapy, or chemotherapy) of a residual mass a t the end of planned therapythe end of planned therapy
Rodeberg, D, JCO 27:2009Rodeberg, D, JCO 27:2009
Resection of residual massResection of residual mass

9
IRS IV, Group IIIIRS IV, Group III5 yr Local Control5 yr Local Control
–– Orbit Orbit 98 %98 %–– Head and neck Head and neck 88 %88 %–– Parameningeal Parameningeal 84 %84 %–– Bladder/prostateBladder/prostate 81 %81 %–– ExtremityExtremity 93 % 93 % –– Other Other 86 %86 %–– All sitesAll sites 87 %87 %
Donaldson et al. IJROBP 51:718, 2001Donaldson et al. IJROBP 51:718, 2001
Timing of RadiotherapyTiming of Radiotherapy
Grp II Grp III PM / High risk
IRS - I week 0 week 6 week 0, 6 / 0IRS - II week 0, 6 week 6 week 6, 9 / 0IRS - III week 2 week 6 week 6, 9 / 0 IRS - IV week 9 week 9 week 9 / 0
IRSIRS V V -- Risk Group AssignmentRisk Group Assignment
•• LowLow : ~ 35% of RMS: ~ 35% of RMS–– EmbryonalEmbryonal–– Favorable site, Group IFavorable site, Group I--IIIIII–– Unfavorable site, Group Unfavorable site, Group
I/III/II•• IntermediateIntermediate : ~ 50%: ~ 50%
–– Groups IGroups I--III AlveolarIII Alveolar–– Unfavorable site, Group Unfavorable site, Group
III III EmbryonalEmbryonal•• HighHigh : ~ 15% of RMS: ~ 15% of RMS
–– Metastatic diseaseMetastatic disease
0.00.0
0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
YearsYears
00 22 44 66
Pro
port
ion
FF
SP
ropo
rtio
n F
FS
88 1010
LowLow
IntermediateIntermediate
HighHigh
Timing of Timing of RadiotherapyRadiotherapyRisk based protocols Risk based protocols
Low Risk Low Risk Intermediate Risk Intermediate Risk
Grp II Grp III All PM / High risk
D9602 Week 3Week 3 Week 12Week 12 D9803D9803 WeekWeek 1212 Week 12/0Week 12/0
ARST0331
Week 13Week 13 Week 13Week 13 ARST0531
Week 4Week 4 Week 4Week 4

10
IRS V IRS V -- Local Control IssuesLocal Control Issues•• SurgerySurgery -- PreopPreop vsvs post op RT with post op RT with SLOSLO
•• XRTXRT -- Dose reductionsDose reductions for select patientsfor select patients–– Group I alveolar/undifferentiatedGroup I alveolar/undifferentiated 36 Gy36 Gy–– Group II NGroup II N 00 36 Gy36 Gy–– Group III orbit/eyelidGroup III orbit/eyelid 45 Gy45 Gy–– Group III second look operationGroup III second look operation
negative margins negative margins 36 Gy36 Gymicroscopically + marginsmicroscopically + margins 41.4 Gy41.4 Gy
Volume ReductionVolume Reduction , Group III @ , Group III @ 36 36 -- 41.4 Gy41.4 Gy
Timing Timing –– week 12week 12
LowLow -- 35%35%
Intermediate Intermediate -- 50%50%
High High -- 15%15%
35%35%
55%55%
10%10%
IRS V IRS V -- Risk Group Assignment / ResultRisk Group Assignment / Result
ExpectedExpected EnrolledEnrolled
Outcome Outcome –– 5 5 yryr survival 78%survival 78%
What’s new for COG RMS studies?What’s new for COG RMS studies?•• LowLow-- RiskRisk RMS (ARST 0331)RMS (ARST 0331)
–– Shorter treatment (subset 1) Shorter treatment (subset 1) –– Lower cyclophosphamide cumulative doseLower cyclophosphamide cumulative dose
(subset 2)(subset 2)•• Intermediate Intermediate -- RiskRisk RMS (ARST 0531) RMS (ARST 0531)
–– Randomized addition of irinotecanRandomized addition of irinotecan–– Early (week 4) radiotherapy for allEarly (week 4) radiotherapy for all–– Optional FDG PET imaging at weeks 1, 4, and 15Optional FDG PET imaging at weeks 1, 4, and 15
•• High High -- RiskRisk RMS (ARST 0431)RMS (ARST 0431)–– Most active drug pairs usedMost active drug pairs used–– Interval compression of VDC/IEInterval compression of VDC/IE
•• Goal Goal –– cure without late effectscure without late effects•• Strategy Strategy –– customize therapycustomize therapy
-- For radiation oncology For radiation oncology -- minimize minimize dose / dose / volume to achieve local volume to achieve local --regional controlregional control
-- For others For others -- omitting radiation?omitting radiation?

11
OrbitOrbit Chemotherapy Alone Chemotherapy Alone –– Orbital RMSOrbital RMS
MMT 84MMT 84 Rx: 3 Rx: 3 –– 10 c 10 c -- IfosIfos, VCR, Act, VCR, Act--DDif PR, 3c if PR, 3c CisplatinCisplatin, , AdriaAdriaif NR/PD, 45 Gyif NR/PD, 45 Gy
Results: Results: LF LF –– 37 %37 %4 4 yryr EFS 62 %, OS 86 %EFS 62 %, OS 86 %
Toxicity: 5 Toxicity: 5 ExenterationsExenterations, , I Cardiomyopathy, 1 RTAI Cardiomyopathy, 1 RTA
COG D 9602COG D 9602 Rx: VA + 45 GyRx: VA + 45 GyResults: Results: 3 3 yryr FFS 88 %, OS 99 %FFS 88 %, OS 99 %
GYN SitesGYN Sites
Uterus Uterus –– CervixCervixVulvaVulva
-- XRT XRT administrateredadministratered as as a function of Groupa function of Group
VaginaVagina - ““special”special”
Vaginal RMS Vaginal RMS –– Unique ApproachUnique Approach
- Favorable site & histologyFavorable site & histologyExcellent prognosis, high survivalExcellent prognosis, high survival
-- Goal: Avoid loss of organ function, Goal: Avoid loss of organ function, Avoid radical resection & XRTAvoid radical resection & XRT
-- Emphasis: Primary Emphasis: Primary chemoRchemoR xx x 12, 20, 24, 28 wks. x 12, 20, 24, 28 wks. Evaluate by: Imaging, EUA, Evaluate by: Imaging, EUA, BB xx
-- Plan: Delay resection & RT. Plan: Delay resection & RT. Omit RT if CROmit RT if CR

12
7 local recurrences – 26% 7 local recurrences – 43%
D 9602 1997 D 9602 1997 –– 20042004n = 25, Group II, IIIn = 25, Group II, IIIResults @ Results @ 55 yearsyears
ARST 0331 2004 ARST 0331 2004 –– 20082008n = 16, Group IIIn = 16, Group III@ @ 22 yearsyears
None of patients with local recurrences received XR T
IRSG Protocols for Vaginal RMSIRSG Protocols for Vaginal RMS
OS OS –– 88%88%
FFS FFS –– 42%42%
YearsYearsP
roba
bilit
yP
roba
bilit
yYearsYears
Pro
babi
lity
Pro
babi
lity
FFS FFS –– 70%70%
OS OS –– 100%100%
ConclusionsConclusions•• Higher rates of local failure in Group II / III vag inal Higher rates of local failure in Group II / III vag inal
patients related to attempt to delay /avoid RTpatients related to attempt to delay /avoid RT•• Goal of achieving good FFS while delaying / avoidin g Goal of achieving good FFS while delaying / avoidin g
RT was not achievedRT was not achieved•• Plan Plan –– modify recommendations for local therapy for modify recommendations for local therapy for
vaginal RMS to follow guidelines for other pelvic s itesvaginal RMS to follow guidelines for other pelvic s ites
Group I Group I -- no RTno RTII a II a -- 36 Gy @ week 1336 Gy @ week 13II b/c II b/c -- 41.4 Gy @ week 1341.4 Gy @ week 13IIIIII -- 50.4 Gy @ week 1350.4 Gy @ week 13
ProblemsProblems
•• Making the diagnosisMaking the diagnosis
Need Need H and EH and E plusplusImmunohistochemistryImmunohistochemistry plusplusMolecular geneticsMolecular genetics
Alveolar RMS PAXAlveolar RMS PAX--FKHR Fusions FKHR Fusions
FKHR ActivationFD FKHR (13q14)FKHR (13q14)
PAX3PAX3--FKHR FKHR t(2;13)t(2;13)
PB HD
PB HDPAX7PAX7--FKHR FKHR
t(1;13)t(1;13)
PAX3 (2q35)PAX3 (2q35)PB HD
PAX7 (1p36)PAX7 (1p36)PB HD
BreakpointBreakpoint

13
Future Future 1. Rhabdomyosarcoma 1. Rhabdomyosarcoma –– 2 distinct diseases2 distinct diseases
2. 2. Need large data sets of clinical outcome Need large data sets of clinical outcome and large tissue banksand large tissue banks
3. 3. Need more clinical trialsNeed more clinical trials
Survival in RhabdomyosarcomaFour Decades of Progress
0
10
20
30
40
50
60
70
80
90
1960s Early1970s
Late1970s
Mid 1980s 1990s Early2000s
Era
5-yr
sur
viva
l (%
)
IRSIRS--IIIRSIRS--IIII
IRSIRS--IIIIIIIRSIRS--IVIV
PrePreCooperativeCooperative
GroupGroup
IRSIRS--VV
NCI Clinical Trials ProgramNCI Clinical Trials Program
“The system for conducting cancer clinical trials in “The system for conducting cancer clinical trials in the United States is approaching a state of crisis. ”the United States is approaching a state of crisis. ”
John Mendelsohn, Committee ChairJohn Mendelsohn, Committee Chair
“Adult cooperative groups are highly inefficient; “Adult cooperative groups are highly inefficient; CChange is clearly necessary”.hange is clearly necessary”.

14
NCI Cooperative Group ProgramNCI Cooperative Group Program
“… too slow, unwieldy, and fragmented, unable “… too slow, unwieldy, and fragmented, unable to deal with the increasingly complex to deal with the increasingly complex
molecularlymolecularly-- driven therapeutics research” driven therapeutics research”
especially in rare cancers such as sarcomasespecially in rare cancers such as sarcomas
Federal Funding for Cooperative Groups is Flat
1950 1960 1970 1980 1990
22
44
66
88
( )( )
Annual USA Cancer Mortality Rate Annual USA Cancer Mortality Rate Children < 15 YearsChildren < 15 Years
CCG
NWTSGIRSG
CALGB Pediatric DivisionCALGB Pediatric Division
SWOG Pediatric DivisionSWOG Pediatric Division POG
Pediatric Cooperative GroupsPediatric Cooperative Groups
2000
Mortality Mortality per per
100,000, 100,000, AgeAge--
AdjustedAdjusted
2005
CCOOGG
New NCI Clinical Trials ProgramNew NCI Clinical Trials Program

15
New Clinical Trials NetworkNew Clinical Trials Network
GoalGoal -- Promote scientific collaboration Promote scientific collaboration -- Improve therapeutic outcomes Improve therapeutic outcomes -- Improve efficiencyImprove efficiency
FacilitateFacilitate -- Study rare malignanciesStudy rare malignancies-- Use sophisticated imaging modalitiesUse sophisticated imaging modalities-- Promote molecular characterization of Promote molecular characterization of
tumorstumors-- Provide access to national tissue banksProvide access to national tissue banks
Be Optimistic…. Be Optimistic….
“ It is imperative to preserve and “ It is imperative to preserve and strengthen the unique capabilities of strengthen the unique capabilities of the cooperative group program”. the cooperative group program”.
-- All important lessons from the ChildrenAll important lessons from the Children



![Residual tumor micro-foci and overwhelming regulatory T ... tumor.pdf[12, 13] among tumor infiltrating lymphocytes (TIL) were associated with a better prognosis. Hence, IFNγ+ and](https://img.pdfslide.us/doc/110x75/5fbd8f5fb794822b78252cb7/residual-tumor-micro-foci-and-overwhelming-regulatory-t-tumorpdf-12-13-among.jpg)











![Measuring intracellular motion usin g dynamic light ... · tumor spheroids to differentiate between the viable rim and necrotic core [11]. The current work is a feasibility study](https://img.pdfslide.us/doc/110x75/5fa203366fd53f5ff830589a/measuring-intracellular-motion-usin-g-dynamic-light-tumor-spheroids-to-differentiate.jpg)