Embed Size (px)
Citation preview

2011
Group Dental Product Guide
For plans effectiveJune 1, 2011 or later

Table of Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Plan Summaries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Advanced Consumer Tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
DentalBlue Traditional – Groups 2-9 Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
DentalBlue Traditional Choice Plus – Groups 2-9 Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
DentalBlue Traditional – Groups 10+ Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
DentalBlue Traditional Choice Plus – Groups 10+ Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
DentalBlue Select (Voluntary) Plans – Groups 2+ Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
DentalBlue Consumer-Directed – Groups 2+ Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10
DentalBlue Consumer-Directed Choice Plus – Groups 2+ Enrolled . . . . . . . . . . . . . . . . . . . . . . . . . .11
DentalBlue - Covered Services, Limitations and Exclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
BluePerks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
BluePerks Discount Drug Card . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13

1
Coverage You Can Smile About
DentalBlue plans from BlueCross BlueShield of Tennessee offer flexibility, convenience and exceptional customer service – all from one of the most trusted names in the business.
Whether added as a complement to an existing health plan or as stand-alone coverage, DentalBlue advantages include:
• Largest dental PPO network in Tennessee; plus a comprehensive national solution• A wide selection of comprehensive and preventive plans• DentalBlue Select Plans (Voluntary)• Reasonable and customary plans with no penalties for members going out of network• Easier administration for groups with combined dental and medical plans; one member ID
card and one bill
The DentalBlue network is second to none, with more than 2,600 access points in Tennessee and growing. Nationwide, the number of network dentists grows to more than100,000, giving our members great access to provider discounts across the country. And what is a network if it does not deliver savings? DentalBlue members save more than 20 percent off the average submitted charge.
Did you know that
in 2010 more than
80 percent of all
BlueCross BlueShield
of Tennessee
members utilized
network dentists?

2
Choices for Groups of All SizesDentalBlue is flexible and includes a variety of plan designs and options to meet the needs of any size group.
DentalBlue Traditional PlansDentalBlue Traditional is a great option for groups with 50 percent or more employee participation and is available with or without employer contribution. Groups with 2-9 enrolled and groups with 10 or more enrolled can both choose from all plan designs.
DentalBlue Select (Voluntary) PlansGroups with at least 20 percent participation can choose our DentalBlue Select and employer contribution is not required. Standard, Basic and Preventive plans give groups more choices for their employees.

3
Consumer-Directed Dental PlansConsumer-Directed Dental Plans offer only two coinsurance levels, provide more coverage for major restorative dental procedures and a higher maximum to cover dental needs. For employees, it’s a way to trade lower premiums for an increased level of responsibility and involvement in personal oral care decisions with the same great network and coverage.
Health Maintenance OptionGroups can exclude diagnostic and preventive services (coverage “A”) from the annual maximum and help employees see the benefit of regular dental visits by eliminating cost barriers to preventive dental care. This feature may be added to any DentalBlue plan with very little impact to monthly rates.
Non-Network Dental OptionsAll plans have access to the DentalBlue network in Tennessee and more than 100,000 dentists nationwide. The out-of-network reimbursement has one of two options for many of the plan designs and is noted on each of the dental benefit plan pages.
• With the PPO Preferred Option, maximum claims savings is achieved through a discounted maximum allowable charge (MAC) payment schedule for non-network dentists.
• With the Freedom of Choice Option, or passive PPO, a higher usual and customary rate (UCR) schedule means employees have lower out-of-pocket costs at non-network dentists, compared to PPO Preferred.
• With the Choice Plus Option, plans have a lower coinsurance out-of-network, while maintaining the usual and customary rate (UCR) schedule.
Combine DentalBlue with a BlueCross BlueShield of Tennessee Health PlanBlueCross BlueShield of Tennessee encourages the total health of our members. When a group combines medical and dental coverage, members receive more advantages at no additional cost.
Advantages of Combined Dental and Health Coverage• One ID card for members
• One bill and one eligibility feed
• Oral Health Program; which includes extra cleanings for certain health conditions
• Secondary coverage from medical for impacted wisdom teeth
• Single point of service for members and group administrators

4
Advanced Consumer ToolsAn informed consumer is a better consumer – dental and health care are no different. The consumer tools in BlueAccess, the secure member section at bcbst.com, are a great resource that can help members be better dental care consumers. They can even check the estimated cost of advanced dental procedures before they receive care.
To help control costs, it makes sense to encourage members to check and compare procedures – before they make decisions that affect their health and their wallet. Informed members who take advantage of their preventive dental benefits save money, for themselves and for their groups.
DentalBlue Members Can:
• Find a dentist from the extensive PPO network panel
• Receive cost estimates for dental procedures
• Find information on oral health issues and children’s dental care
• View plan details and recent claims
• Take a personal health analysis
• Create a personal online health center

5
DentalBlue Traditional Plans
Groups 2-9 EnrolledBlueCross BlueShield of Tennessee offers flexible plan designs to meet your group’s needs. DentalBlue Traditional plans are available with the Choice and Preferred Reimbursement Options.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
Plan Summary Standard Preventive
Where To Receive Services Any Dentist Any Dentist
Coverage A • Exams, X-rays• Cleanings, Fluoride• Sealants, Space Maintainers
100% 100%
Coverage B [1] • Basic Restorative Services• Basic and Major Endodontics• Basic and Major Periodontics• Basic and Major Oral Surgery
80% 50%
Coverage C [1] • Major Restorative, Prosthodontics & Implants 50% 0%
Annual Deductible (Per Member, Max 3 per family) Not applicable to Coverage A $50 $25
Annual Maximum Benefit (Per Member) $1,000, $1,500 or $2,000 $500
Dependent age limit to age 26
Additional Features To Customize Your PlanExclude Class A from Annual Maximum Coverage A services received do not count toward the annual maximum benefit
Class C waiting period [2] 12 months (optional)
Coverage D Orthodontics Not available with Preventive Plan
Coinsurance 50% Coinsurance, No Deductible
Maximum $1,000 or $1,500 - Per Member, Per Lifetime
Age Limit Child Only to age 18
Limitations 12-month waiting period applies [2]
Plan Reimbursements [3] • Freedom of Choice Option Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Usual and Customary Rate (UCR)
• PPO Preferred Option Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Maximum Allowable Charge (MAC)
Plan RequirementsStand Alone Dental Minimum of five enrolled
Group Participation 50% enrolled
Employer Contribution No requirement if group has current dental coverage
1 Services may be moved between coverage levels in accordance with underwriting guidelines.2 Waived at initial enrollment for those covered under prior carrier plan.3 Members are responsible for paying any amounts exceeding the UCR or MAC when Non-Network Dentists are used.

6
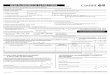
DentalBlue Traditional Choice Plus
Groups 2-9 EnrolledBlueCross BlueShield of Tennessee offers flexible plan designs to meet your group’s needs.
• With Choice Plus, members receive a higher coinsurance percentage when network dentists are used.
• Also with Choice Plus Plans, a higher Usual and Customary Rate (UCR) schedule means employees have lower out-of-pocket costs at non-network dentists.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
Standard Preventive
Plan Summary 90 80 90 50
Where To Receive Services In- Network
Out-of-Network
In- Network
Out-of-Network
In- Network
Out-of-Network
In- Network
Out-of- Network
Coverage A
• Exams, X-rays• Cleanings, Fluoride• Sealants, Space Maintainers
100% 100% 100% 100% 100% 100% 100% 100%
Coverage B [1]
• Basic Restorative Services• Basic and Major Endodontics• Basic and Major Periodontics• Basic and Major Oral Surgery
90% 80% 80% 70% 90% 80% 50% 40%
Coverage C [1]
• Major Restorative, Prosthodontics & Implants 60% 50% 50% 40% 10% 0% 10% 0%
Annual Deductible (Per Member, Max 3 per family) Not applicable to Coverage A
$50 $50 $50 $25
Annual Maximum Benefit (Per Member)
$1,000, $1,500 or $2,000
$1,000, $1,500 or $2,000 $500 or $1,000 $500
Dependent Age Limit to age 26
Additional Features To Customize Your PlanExclude Class A from Annual Maximum Coverage A services received do not count toward the annual maximum benefit.
Class C waiting period [2] 12 months (optional)
Coverage D Orthodontics Not available with Preventive Plan
Coinsurance 50% Coinsurance, No Deductible
Maximum $1,000 or $1,500 - Per Member, Per Lifetime
Age Limit Child Only to age 18
Limitations 12-month waiting period applies [2]
Plan Reimbursement [3] • Freedom of Choice Option Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Usual and Customary Rate (UCR)
Plan RequirementsStand Alone Dental Minimum of five enrolled
Group Participation 50% enrolled
Employer Contribution No requirement if group has current dental coverage1 Services may be moved between coverage levels in accordance with underwriting guidelines.2 Waived at initial enrollment for those covered under prior carrier plan.3 Members are responsible for paying any amounts exceeding the UCR or MAC when Non-Network Dentists are used.

7
DentalBlue Traditional Plans
Groups 10+ EnrolledBlueCross BlueShield of Tennessee offers flexible plan designs to meet your group’s needs. DentalBlue Traditional plans are available with the Freedom of Choice and PPO Preferred Reimbursement Options.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
Plan Summary Deluxe Standard 60
Standard Basic Basic 10
Preventive 10
Preventive
Where To Receive Services Any Dentist
Any Dentist
Any Dentist
Any Dentist
Any Dentist
Any Dentist
Any Dentist
Coverage A • Exams, X-rays• Cleanings, Fluoride• Sealants, Space Maintainers
100% 100% 100% 80% 100% 100% 100%
Coverage B [1]
• Basic Restorative Services• Basic and Major Endodontics• Basic and Major Periodontics• Basic and Major Oral Surgery
100% 90% 80% 80% 80% 50% 50%
Coverage C [1] • Major Restorative,
Prosthodontics & Implants80% 60% 50% 50% 10% 10% 0%
Annual Deductible (Not applicable to Coverage A) $25 or $50 $25 or $50 $25 or $50 $25 or $50 $25 or $50 $0 or $25 $0 or $25
Annual Maximum Benefit (Per Member)
$1,000, $1,250,
$1,500 or $2,000
$1,000, $1,250,
$1,500 or $2,000
$1,000, $1,250,
$1,500 or $2,000
$1,000, $1,250,
$1,500 or $2,000
$1,000, $1,250,
$1,500 or $2,000
$500, $1,000 or $1,250
$500, $1,000 or $1,250
Dependent age limit to age 26
Additional Features To Customize Your PlanExclude Class A from Annual Maximum Coverage A services received do not count toward the annual maximum benefit.
Class C waiting period [2] 12 months (optional)
Coverage D Orthodontics Not available with Preventive Plan
Coinsurance 50% Coinsurance, No Deductible
Maximum $1,000 or $1,500 - Per Member, Per Lifetime
Age Limit Child Only (to age 18) or No age limit (groups 26+)
Waiting Period [2] 12 months or no waiting period
Family Deductible Max 3 per familyPer person no maximum
Plan Reimbursements [3] • Freedom of Choice Option Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Usual and Customary Rate (UCR)
• PPO Preferred Option Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Maximum Allowable Charge (MAC)
Plan RequirementsMulti-Option Groups with 26+ may offer two plansGroup Participation 50% enrolledEmployer Contribution No requirement if group has current dental coverage1 Services may be moved between coverage levels in accordance with underwriting guidelines.2 Waived at initial enrollment for those covered under prior carrier plan.3 Members are responsible for paying any amounts exceeding the UCR or MAC when Non-Network Dentists are used.

8
DentalBlue Traditional Choice Plus
Groups 10+ Enrolled BlueCross BlueShield of Tennessee offers flexible plan designs to meet your group’s needs.
• With Choice Plus, members receive a higher coinsurance percentage when network dentists are used.
• Also with Choice Plus Plans, a higher usual and customary rate (UCR) schedule means employees have lower out-of-pocket costs at non-network dentists.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
Standard Preventive
Plan Summary 90 80 90 50
Where To Receive Services In- Network
Out-of-Network
In- Network
Out-of-Network
In- Network
Out-of-Network
In- Network
Out-of- Network
Coverage A • Exams, X-rays• Cleanings, Fluoride• Sealants, Space Maintainers
100% 100% 100% 100% 100% 100% 100% 100%
Coverage B [1]
• Basic Restorative Services• Basic and Major Endodontics• Basic and Major Periodontics• Basic and Major Oral Surgery
90% 80% 80% 70% 90% 80% 50% 40%
Coverage C [1] • Major Restorative,
Prosthodontics & Implants60% 50% 50% 40% 10% 0% 10% 0%
Annual Deductible (Not applicable to Coverage A) $25 or $50 $25 or $50 $25 or $50 $0 or $25
Annual Maximum Benefit (Per Member)
$1,000, $1,250, $1,500 or $2,000
$1,000, $1,250, $1,500 or $2,000
$1,000, $1,250, $1,500 or $2,000 $500, $1,000 or $1,250
Dependent age limit to age 26
Additional Features To Customize Your PlanExclude Class A from Annual Maximum Coverage A services received do not count toward the annual maximum benefit.
Class C waiting period [2] 12 months (optional)
Coverage D Orthodontics Not available with Preventive Plan
Coinsurance 50% Coinsurance, No Deductible
Maximum $1,000 or $1,500 - Per Member, Per Lifetime
Age Limit Child Only (to age 18) or No age limit (Groups 26+)
Waiting Period [2] 12 months or no waiting period
Family Deductible Max 3 per familyPer person no maximum
Plan Reimbursement • Freedom of Choice Option [3] Network Dentists Paid at PPO Fee Schedule Non-Network Dentists Paid at Usual and Customary Rate (UCR)
Plan RequirementsMulti-Option Groups with 26+ may offer two plans
Group Participation 50% enrolled
Employer Contribution No requirement if group has current dental coverage1 Services may be moved between coverage levels in accordance with underwriting guidelines.2 Waived at initial enrollment for those covered under prior carrier plan.3 Members are responsible for paying any amounts exceeding the UCR when Non-Network Dentists are used.

9
DentalBlue Select (Voluntary) Plans
Groups 2+ Enrolled BlueCross BlueShield of Tennessee offers dental plans with lower participation requirements to meet your group’s needs.
DentalBlue Select (Voluntary) Plans are available with the Freedom of Choice and PPO Preferred Reimbursement options.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
Plan Summary Standard Basic Preventive
Where To Receive Services Any Dentist Any Dentist Any DentistCoverage A • Exams, X-rays• Cleanings, Fluoride• Sealants, Space Maintainers
100% 80% 100%
Coverage B • Basic Restorative Services• Basic Endodontics• Basic Periodontics• Basic Oral Surgery
80% 80% 50%
Coverage C 12-month waiting period applies [1]
• Major Endodontics• Major Periodontics• Major Oral Surgery• Major Restorative, Prosthodontics &
Implants
50% 50% 0%
Annual Deductible (Not applicable to Coverage A) $25 or $50 $25 or $50 $0 or $25
Annual Maximum Benefit (Per Member) [2] $1,000, $1,250 $1,500, or $2,000
$1,000, $1,250 $1,500, or $2,000 $500, $1,000, $1,250
Dependent Age Limit to age 26
Additional Features To Customize Your PlanExclude Class A from annual maximum Coverage A services do not count toward the annual maximum benefit
Coverage D Orthodontics Not available with Preventive Plan
Coinsurance 50% Coinsurance, No Deductible
Maximum $1,000 or $1,500 - Per Member, Per Lifetime
Age Limit Child Only (to age 18) or No age limit (Groups 26+)
Waiting Period [1] 12 months or no waiting period
Family Deductible Max 3 per familyPer person no maximum
Plan Reimbursements [3] • Freedom of Choice Option (PPO fee schedule in-network; UCR out-of-network)
• PPO Preferred Option (PPO fee schedule in-network; percentage of PPO fee schedule out-of-network)
Plan RequirementsStand Alone Dental Minimum of five enrolledMulti-Option Groups with 26+ may offer two plansGroup Participation 20% enrolledEmployer Contribution No requirement1 Waived at intial enrollment for those covered under prior carrier plan.2 $1,250 annual maximum available for groups with 10+ enrolled only3 Members are responsible for paying any amounts exceeding the Maximum Allowable Charge or Usual and Customary Rate when Non-
Network Dentists are used.

10
Consumer-Directed Dental Plans
Groups 2+ EnrolledBlueCross BlueShield of Tennessee now offers consumer-directed dental plans to provide cost effective coverage with a higher annual maximum.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution.
DentalBlue High-Deductible Dental Plan (HDDP)
Plan Summary Standard Plans Copay Plans
Preventive Dental• Exams, X-rays• Cleanings, fluoride• Sealants, Space maintainers
100% 100%100% after $10 or
$25 Copay per visit
100% after $10 or $25
Copay per visit
Annual Deductible (Per member, Max 2 or 3 per family)(Applies to basic and major dental services only) $250 $250 $250 $250
Basic & Major Dental • Restorative (fillings & crowns) • Endodontics (pulpotomy & root canals)• Periodontics (scaling, root planing, gum &
osseous surgery) • Oral Surgery (extractions including impactions)• Prosthodontics (bridges & dentures)• Implants
70% 60% 70% 60%
Annual Maximum Benefit Per Member (Applies to basic and major dental services only) $2,500 $2,500 $2,500 $2,500
Dependent Age Limit To age 26
Additional Features To Customize Your PlanOrthodontics Coinsurance 50%
Deductible None
Maximum $1,000 per member per lifetime
Age Limit To age 18
Waiting Period None or 12 months
Plan Reimbursements • Freedom of Choice Option (PPO fee schedule in-network; UCR out-of-network) [1]
• PPO Preferred Option (PPO fee schedule in-network, Percentage of PPO fee schedule out-of-network)1
Plan RequirementsStand Alone Dental Minimum of five enrolled
Multi-Option Groups with 26+ may offer two plans
Group Participation 50% enrolled
Employer Contribution No requirement if group has current dental coverage1Members are responsible for paying any amount exceeding the UCR or maximum allowable charge when non-network dentists are used.

11
Consumer-Directed Dental Plans Choice Plus
Groups 2+ EnrolledBlueCross BlueShield of Tennessee now offers consumer-directed dental plans to provide cost effective coverage with a higher annual maximum.
Regardless of which option a group chooses, employees will always benefit from the savings generated by the LARGEST dental PPO network in the state of Tennessee and access to our national PPO solution, outside of Tennessee and contiguous counties.
DentalBlue High-Deductible Dental Plan (HDDP) with Choice Plus
Plan Summary Standard Plans Copay Plans
Preventive Dental• Exams, X-rays• Cleanings, fluoride• Sealants, Space maintainers
100% 100% 100% after $10 or $25 Copay per visit
100% after $10 or $25 Copay per visit
Annual Deductible (Per member, 2 or 3 per family)
(Applies to basic and major dental services only)
$250 $250 $250 $250
Network Dentist
Non-Network Dentist
Network Dentist
Non-Network Dentist
Network Dentist
Non-Network Dentist
Network Dentist
Non-Network Dentist
Basic & Major Dental • Restorative (fillings & crowns) • Endodontics (pulpotomy &
root canals)• Periodontics (scaling, root
planing, gum & osseous surgery)
• Oral Surgery (extractions including impactions)
• Prosthodontics (bridges & dentures)
• Implants
70% 50% 60% 50% 70% 50% 60% 50%
Annual Maximum Benefit Per Member
(Applies to basic and major dental services only)
$2,500
Dependent Age Limit To age 26
Plan Reimbursement Freedom of Choice Option (PPO fee schedule in-network; UCR out-of-network) [1]
Additional Features To Customize Your PlanOrthodontics Coinsurance 50%
Deductible NoneMaximum $1,000 per member per lifetimeAge Limit To Age 18Waiting Period None or 12 months
Plan RequirementsStand Alone Dental Minimum of five enrolled
Multi-Option Groups with 26+ may offer two plans
Group Participation 50% enrolled
Employer Contribution No requirement if group has current dental coverage
1 Members are responsible for paying any amounts exceeding the Usual and Customary Rate (UCR) when Non-Network Dentists are used.

12
DentalBlue - Covered Services, Limitations & Exclusions
Exams Covered: Standard exams including comprehensive, periodic, detailed/extensive and periodontal oral evaluations (exams). Emergency exams, including limited oral evaluations (exams). Limitations: No more than one standard exam in any 6 month period. No more than one emergency exam in any 12 month period. No more than one comprehensive, detailed/extensive, or periodontal exam in any 36 month period. Exclusions: Re-evaluations and consultations.
X-rays Covered: Full mouth series, intraoral and bitewing radiographs (X-rays). Limitations: No more than one full mouth set of X-rays in any 36 month period. A full mouth set of X-rays is defined as either an intraoral complete series or panoramic X-ray. Benefits provided for either include benefits for all necessary intraoral and bitewing films taken on the same day. No more than four bitewing films in any 12 month period. Bitewing films must be taken on the same date of service. Exclusions: Extraoral, skull and bone survey, sialography, TMJ, and tomographic survey X-ray films, cephalometric films and diagnostic photographs. Cephalometric films and diagnostic photographs may be Covered as orthodontic benefits under Coverage D.
Cleanings, Fluoride Treatment Covered: Adult and child prophylaxis (cleaning). Topical fluoride treatments, performed with or without a prophylaxis. Limitations: No more than one of any prophylaxis or periodontal maintenance procedure in any 6month period. Periodontal maintenance procedures are subject to additional limitations listed below under Basic Periodontics in Section VI, and may be subject to a different Coverage level under Attachment C: Schedule of Benefits. No more than one fluoride treatment in any 12 month period, for Members under age 19. Fluoride must be applied separately from prophylaxis paste.
Sealants, Space Maintainers Covered: Other Preventive Services, including sealants, space maintainers. Limitations: No more than one sealant per first or second molar tooth per lifetime, for Dependents under age 16. Space maintainers for Dependents under age 14. No more than one recementation in any 12month period. Exclusions: Nutritional and tobacco counseling, oral hygiene instructions.
Basic Restorative Services Covered: Basic restorative services, including amalgam restorations (silver fillings), resin composite restorations (tooth colored fillings), stainless steel crowns. Palliative (emergency) treatment for the relief of pain. Other restorative services, including repair of full and partial dentures. Limitations: No more than one amalgam or resin restoration per tooth surface in any 12 month period. Replacement of existing amalgam and resin composite restorations Covered only after 12 months from the date of initial restoration. Replacement of stainless steel crowns Covered only after 36 months from the date of initial restoration. No more than one repair per denture per 24 months. Exclusions: Gold foil restorations.
Major Restorative Services Covered: Single tooth restorations, including crowns (resin, porcelain, ¾ cast, and full cast), inlays and onlays (metallic, resin and porcelain), and veneers. Limitations: Only for the treatment of severe carious lesions or severe fracture on permanent teeth, and only when teeth cannot be adequately restored with an amalgam or resin composite restoration (filling). For permanent teeth only. For Dependents under age 12, benefits will not be provided for cast crowns or laminate veneers. Replacement of single tooth restorations Covered only after 60 months from the date of initial placement. Exclusions: Temporary and provisional crowns.
Prosthodontic Services - Fixed Bridges Covered: Fixed partial dentures (bridges), including pontics, retainers, and abutment crowns, inlays, and onlays (resin, porcelain, ¾ and full cast). Limitations: Only for treatment where a missing tooth or teeth cannot be adequately restored with a removable partial denture. For permanent teeth only, no benefits for Dependents under age 16. Replacement of fixed partial dentures Covered only after 60 months from the date of initial placement.
Prosthodontic Services - Removable Dentures Covered: Complete, immediate and partial dentures. Limitations: If, in the construction of a denture, the Member and the Dentist decide on a personalized restoration or to employ special rather than standard techniques or materials, benefits provided shall be limited to those which would otherwise be provided for the standard procedures or materials (as determined by the Plan). Benefits are not provided for Dependents under age 16. Replacement of removable dentures Covered only after 60 months from the date of initial placement. Exclusions: Interim (temporary) dentures.
Other Major Restorative & Prosthodontic Services Covered: Crown and bridge services including core buildups, post and core, recementation, and repair. Denture services including adjustment, relining, rebasing and tissue conditioning. Implants and supported prosthetics includes local anesthetic. Limitations: The benefits provided for crown and bridge restorations include benefits for the services of crown preparation, temporary or prefabricated crowns, impressions and cementation. Benefits will not be provided for a core build-up separate from those provided for crown construction, except in those circumstances where benefits are provided for a crown because of severe carious lesions or fracture is so extensive that retention of the crown would not be possible. Post and core services are Covered only when performed in conjunction with a Covered crown or bridge. Crown and bridge repair and re-cementation are Covered separately only after 12 months from the date of initial placement. Denture adjustments are Covered separately from the denture only after 6 months from the date of initial placement. No more than one denture reline or rebase in any 36 month period. Exclusions: Other major restorative services including sedative fillings and coping. Other prosthodontic services including overdenture, precision attachments, connector bars, stress breakers and coping metal.
Basic Endodontics Covered: Pulpotomy, pulpal therapy. Limitations: For primary teeth only. Not Covered when performed in conjunction with major endodontic treatment. The benefits for basic endodontic treatment include benefits for X-rays, pulp vitality tests, and sedative fillings provided in conjunction with basic endodontic treatment. Exclusions: Pulpal debridement.
Major Endodontics Covered: Root canal treatment and re-treatment, apexification, apicoectomy services, root amputation, retrograde filling, hemisection, pulp cap. Limitations: No more than one root canal treatment, re-treatment or apexification per tooth in 60month period. No more than one apicoectomy per root per lifetime. The benefits for major endodontic treatment include benefits for X-rays, pulp vitality tests, pulpotomy, pulpectomy and sedative fillings and temporary filling material provided in conjunction with major endodontic treatment. Exclusions: Implantation, canal preparation, and incomplete endodontic therapy.
Basic Periodontics Covered: Non-surgical periodontics, including periodontal scaling and root planing, full mouth debridement and periodontal maintenance procedure. Limitations: No more that one periodontal scaling and root planing per quadrant in any 24month period. No more than one full mouth debridement per lifetime. No more than one of any prophylaxis (cleanings) or periodontal maintenance procedure in any 6month period. Cleanings are subject to additional limitations listed under Preventive Services, and may be subject to a different Coverage level under Attachment C: Schedule of Benefits. Benefits for periodontal maintenance are provided only after active periodontal treatment (surgical or non-surgical), and no sOut-of-Networker than 90 days after completion of such treatment. Benefits for periodontal scaling and root planing, full mouth debridement, periodontal maintenance and prophylaxis are not provided when more than one of these procedures is performed on the same day. Exclusions: Provisional splinting, scaling in the presence of gingival inflammation, antimicrobial medication and dressing changes.
Major Periodontics Covered: Surgical periodontics including gingivectomy, gingivoplasty, gingival flap procedure, crown lengthening, osseous surgery and bone and tissue grafting. Limitations: No more than one major periodontal surgical procedure in any 36month period. Benefits provided for major periodontics include benefits for services related to 90 days of postoperative care. Exclusions: Tissue regeneration and apically positioned flap procedure.
Basic Oral Surgery Covered: Non-surgical or simple extractions. Limitations: Benefits provided for basic oral surgery include benefits or suturing and postoperative care. Exclusions: Benefits for general anesthesia or intravenous sedation when performed in conjunction with basic oral surgery.
Major Oral Surgery Covered: Surgical extractions (including removal of impacted teeth and wisdom teeth), and other oral surgical procedures typically not Covered under a medical plan. Limitations: Benefits provided for major oral surgery include benefits for local anesthesia, suturing and postoperative care. Benefits for general anesthesia or intravenous (IV) sedation are provided only in connection with major oral surgery procedures, and only when provided by a Dentist licensed to administer such agents. Exclusions: Oral surgery typically covered under a medical plan, including but not limited to, excision of lesions and bone tissue, treatment of fractures, suturing, wound and other repair procedures, TMJ and related procedures. Orthognathic surgery and treatment for congenital malformations.
Orthodontics Services Covered: Exams, photographic images, diagnostic casts, cephalometric X-rays, installation and adjustment of orthodontic appliances and treatment to reduce or eliminate an existing malocclusion. Limitations: The need for orthodontic services must be diagnosed, identifying a handicapping malocclusion that is both abnormal and correctable, and a Treatment Plan must be submitted to and approved by the Plan. The Plan reserves the right to review the Member’s dental records, including necessary X-rays, photographs, and models to determine whether orthodontic treatment is Covered. Orthodontic services may be limited to Dependents under a specified age limit, as defined on Attachment C: Schedule of Benefits. Orthodontic services may be limited by a Maximum Allowable Charge, Calendar Year Deductible and lifetime maximum as defined on Attachment C: Schedule of Benefits. Multiple occurrences of orthodontic treatment may be allowed subject to the lifetime maximum. All orthodontic services shall be deemed to have been concluded on the last date treatment performed during Member’s
Coverage, even if a prior approved Treatment Plan has not been completed. Exclusions: Replacement or repair of any lost, stolen and damaged appliance furnished under the Treatment Plan. Surgical procedures to aid in orthodontic treatment.
Other Exclusions From Coverage1) Dental services received from a dental
or medical department maintained by or on behalf of an Employer, mutual benefit association, labor union, trustee or similar person or group.
2) Charges for services performed by You or Your spouse, or Your or Your spouse’s parent, sister, brother or child.
3) Services rendered by a Dentist beyond the scope of his or her license.
4) Dental services which are free, or for which You are not required or legally obligated to pay or for which no charge would be made if You had no dental Coverage.
5) Dental services to the extent that charges for such services exceed the charge that would have been made and collected if no Coverage existed hereunder.
6) Dental services covered by any medical insurance coverage, or by any other non-dental contract or certificate issued by BlueCross BlueShield of Tennessee or any other insurance company, carrier, or plan. For example, removal of impacted teeth, tumors of lip and gum, accidental injuries to the teeth, etc.
7) Any court-ordered treatment of a Member unless benefits are otherwise payable.
8) Courses of treatment undertaken before You become Covered under this program.
9) Any services performed after You cease to be eligible for Coverage.
10) Dental care or treatment not specifically listed in Attachment C: Schedule of Benefits.
11) Any treatment or service that the Plan determines is not Necessary Dental Care, that does not offer a favorable prognosis that does not meet generally accepted standards of professional dental care, or that is experimental in nature.
12) Services or supplies for the treatment of work related illness or injury, regardless of the presence or absence of workers’ compensation coverage. This exclusion does not apply to injuries or illnesses of an employee who is (1) a sole-proprietor of the Group; (2) a partner of the Group; or (3) a corporate officer of the Group, provided the officer filed an election not to accept Workers’ Compensation with the appropriate government department.
13) Charges for any hospital or other surgical or treatment facility and any additional fees charged by a Dentist for treatment in any such facility.
14) Dental services with respect to congenital malformations or primarily for cosmetic or aesthetic purposes. This does not exclude those services provided under Orthodontic benefits (if applicable.)
15) Replacement of tooth structure lost from wear or attrition.
16) Dental services resulting from loss or theft of a denture, crown, bridge or removable orthodontic appliance.
17) Charges for a prosthetic device that replaces one or more lost, extracted or congenitally missing teeth before Your Coverage becomes effective under the Plan unless it also replaces one or more natural teeth extracted or lost after Your Coverage became effective.
18) Diagnosis for, or fabrication of, appliances or restorations necessary to correct bite problems or restore the occlusion or correct temporomandibular joint dysfunction (TMJ) or associated muscles.
19) Diagnostic dental services such as diagnostic tests and oral pathology services.
20) Adjunctive dental services including all local and general anesthesia, sedation, and analgesia (except as provided under major oral surgery).
21) Charges for the treatment of desensitizing medicaments, drugs, occlusal guards and adjustments, mouthguards, microabrasion, behavior management, and bleaching.
22) Charges for the treatment of professional visits outside the dental office or after regularly scheduled hours or for observation.

13
BluePerks DiscountsExclusively for members, the BluePerks discount program features savings of up to 50 percent on health-related products and elective services. Typically not covered or even considered as part of a dental plan, BluePerks provides excellent added value to DentalBlue members.
BluePerks allows members to get discounts in these areas:
Any prescription drug not covered by a health or pharmacy benefit plan is eligible for a discount of up to 20 percent when the BluePerks Discount Drug Card* is used at participating pharmacies. Members can visit bcbst.com to print a discount drug card and see program details.
* The discount drug card is not insurance and cannot be used to purchase over-the-counter medications or prescription drugs covered by a health or pharmacy benefit plan.
• Acupuncture• Cosmetic services• Dental cosmetic services• Diet and supplement advisors• Eye exams• Fitness & gym memberships• Healthy events and activities• Health magazine subscriptions• Healthy foods/groceries
• Hearing exams and hearing aid technology
• Holistic physicians/ practitioners
• LASIK corrective vision surgery• Massage therapy• Mind/Body and
relaxation therapy• Outdoor fitness gear
• Personal trainers• Prescription drugs• Regional family attractions• Spa services• Vision care products• Vitamins• Weight-loss programs• Yoga and Tai Chi instruction
BluePerks Discount Drug Card

For information about these products and services, please contact your BlueCross BlueShield of Tennessee sales executive or account executive.
BlueCross BlueShield of Tennessee, Inc., an Independent Licensee of the BlueCross BlueShield Association If a conflict exists between the information contained in this Group Dental Product Reference Guide and the Group Agreement, the Group Agreement will control.
Information is current as of the printing of this guide and is subject to change.BlueCross BlueShield of Tennessee is not engaged in rendering tax, investment or legal advice. Federal and state tax regulations are subject to change.
If tax, investment, or legal advice is required, seek the services of a licensed professional. BlueCross BlueShield of Tennessee does not act as an administrator of HSAs.
The company only provides qualified high-deductible health plans. Although these plans meet federal requirements, some members may not be eligible to contribute to an HSA.
This document has been classified as public information
BlueCross BlueShield of Tennessee1 Cameron Hill Circle | Chattanooga, TN 37402
bcbst.com
COMM-DEN-023 (3/11)