Embed Size (px)
Citation preview

Abdominal wall
M. Miserez, F. M. Miserez, F. MuysomsMuysomsLeuven, GentLeuven, Gent
““WarmWarm--up Packageup Package”” EighthEighth editioneditionStrasbourg, April 7, 2011Strasbourg, April 7, 2011
Laparoscopic Laparoscopic inguinal hernia repairinguinal hernia repair

InguinalInguinal hernia hernia treatmenttreatment::factors to factors to considerconsider
Recurrence
Quality of lifepostoperative recovery, chronic pain
Safetyrisk for perioperative complications
Learning curvegrade of difficulty/reproducibility
Costhospital and society costs
Let Let usus thenthen speakspeak the the samesame languagelanguage
•• Hernia Hernia classificationclassification
•• OutcomeOutcome parametersparameters

The EHS Groin Hernia ClassificationThe EHS Groin Hernia Classification
≤ 1 finger 1-2 fingers
> 2 fingers
indirect
femoral
direct
The EHS guidelines on the treatmentof inguinal hernia in adult patients
Simons et al, Hernia 2009; 13: 343-403

TopicsTopics•• Risk factors/Risk factors/preventionprevention•• DiagnosticsDiagnostics•• IndicationsIndications forfor treatmenttreatment•• ClassificationClassification•• TreatmentTreatment
– General– Bilateral– Recurrent– Laparoscopy: TAPP vs TEP– Women– Young men (18-30)
•• BiomaterialsBiomaterials
Simons et al, Hernia 2009; 13: 343-403
TopicsTopics•• Training/specialist centersTraining/specialist centers
•• ComplicationsComplications ((exclexcl recurrencerecurrence))
•• ChronicChronic painpain
•• AntibioticAntibiotic prophylaxisprophylaxis•• AnesthesiaAnesthesia•• DayDay SurgerySurgery•• PostoperativePostoperative pain pain controlcontrol•• PostoperativePostoperative recoveryrecovery•• AftercareAftercare
•• CostsCosts
Simons et al, Hernia 2009; 13: 343-403

Levels of evidenceOxford Centre Oxford Centre forfor EvidenceEvidence--basedbased MedicineMedicine LevelsLevels of of EvidenceEvidence (2001)(2001)
1a systematic reviews of RCTs1b individual high quality RCT
2a systematic reviews of cohort studies2b individual cohort study or low quality RCT2c “outcomes” research
3a systematic reviews of case-control studies3b individual case-control study
4 case-series and poor quality cohort and case-control studies
5 expert opinion
RecommendationA
B
C
D
WhichWhich techniquestechniques are are necessarynecessary to to learnlearn duringduring surgicalsurgical residencyresidency??
1. Lichtenstein1. Lichtenstein
2. TEP2. TEP
3. TAPP3. TAPP
4. 4. StoppaStoppa
5. 5. ShouldiceShouldice

Treatment:
All male adult (>30 years) patients with a All male adult (>30 years) patients with a symptomatic inguinal hernia should be operated symptomatic inguinal hernia should be operated on using a mesh technique.on using a mesh technique.
The open Lichtenstein and endoscopic inguinal The open Lichtenstein and endoscopic inguinal hernia techniques are recommended as the best hernia techniques are recommended as the best evidenceevidence--based options for repair of a primary based options for repair of a primary unilateral hernia unilateral hernia providing the surgeon is sufficiently providing the surgeon is sufficiently experienced in the specific procedure. experienced in the specific procedure.
Grade AGrade A Mc Mc CormackCormack et al, 2005et al, 2005SchmedtSchmedt et al, 2005et al, 2005
Lichtenstein Lichtenstein hernioplastyhernioplasty
Lichtenstein and Shulman, Int Surg 1986

large prosthesiswithreinforcementof the whole myopectineal orifice
~ minimally invasive STOPPA repair~ minimally invasive STOPPA repair (GPRVS)Chirurgie, 1973; 99: 119-123
EndoscopicEndoscopic groingroin hernia hernia repairrepair
Flow diagram treatmentFlow diagram treatment

EndoscopicEndoscopic vsvs LichtensteinLichtensteinFU > 48 FU > 48 monthsmonths
RecurrenceRecurrence
± 5%
Postoperative recovery
It is recommended that an endoscopic It is recommended that an endoscopic technique is considered if a quick technique is considered if a quick
postpost--operative recovery is particularly important.operative recovery is particularly important.
Grade AGrade A

EndoscopicEndoscopic meshmesh techniquestechniques resultresult in a in a lowerlower chancechance of of chronicchronic pain/pain/numbnessnumbnessthanthan LichtensteinLichtenstein..
In the In the longlong--termterm (> 3(> 3--4 4 yearsyears FU), these FU), these differencesdifferencesseemseem to to decreasedecrease forfor the aspect pain, the aspect pain, butbut notnot forfor numbnessnumbness..
Level 1B
Treatment : chronic pain
ItIt is is recommendedrecommended thatthat risksrisks of of developmentdevelopment of of chronicchronic postoperativepostoperative pain are taken pain are taken intointo accountaccountwhenwhen the the methodmethod of hernia of hernia repairrepair is is decideddecided uponupon
Grade BGrade B
lowerlower ageage ((levellevel 2A)2A)
preoperativepreoperative groin pain groin pain ((levellevel 2B)2B)
preoperative chronic pain conditions (level 2B)
female gender (level 2B)
Treatment – chronic pain

Minimally invasive surgery is there to stay Minimally invasive surgery is there to stay
ButBut……
Endoscopic hernia techniques vs. Endoscopic hernia techniques vs. Lichtenstein repair result in aLichtenstein repair result in a
Longer Longer operationoperation time (8time (8--13min),13min),HigherHigher incidence of incidence of seromaseroma
Level 1A
Mc Cormack et al, 2005Mc Cormack et al, 2005SchmedtSchmedt et al, 2005et al, 2005
Treatment
Need for general anesthesia

It is recommended that, It is recommended that, from a from a hospital hospital perspective, perspective, an open mesh procedure is used an open mesh procedure is used for the treatment of primary for the treatment of primary unilatunilat. inguinal hernia.. inguinal hernia.
From a From a sociosocio--economiceconomic perspective, perspective, an an endoscopicendoscopic procedure is proposed procedure is proposed for the active working population, for the active working population, especially for bilateral herniasespecially for bilateral hernias
Grade AGrade A
Costs
HowHow to to reducereduce hospitalhospital costscostsReusableReusable instrumentsinstruments
TrocarsTrocars
Fixation devices (selective)Fixation devices (selective)
AmbulatoryAmbulatory surgerysurgery

EndoscopicEndoscopic surgerysurgery::long and long and steepsteep learninglearning curvecurve
Treatment: Complications laparoscopy
There appears to be a higher rate of rare but There appears to be a higher rate of rare but serious complications with endoscopic repair,serious complications with endoscopic repair,
especiallyespecially duringduring the the learninglearning curve curve periodperiod
LevelLevel 2B2B

Training: the learning curve
The learning curve for performing endoscopic inguinal hernia repair (especially TEP) is longer than for open Lichtenstein repair,
and ranges between 50 and 100 procedures, with the first 30-50 being most critical
Level 2C
Learning curve errors in laparoscopic surgery
Not (longer) tolerated

The The learninglearning curve curve dependsdepends alsoalso onon the the structurestructure of the training program! of the training program!
A learning curve is far from a straight progression
The most important variables The most important variables in the in the learninglearning curvecurve
StructuredStructured training programtraining program
LaparoscopicLaparoscopic experienceexperience of the traineeof the trainee
Patient selection– No recurrent or scrotal hernia– No previous appendectomy for right sided hernia– Female patient
Type of Type of supervisionsupervision– Mentoring vs proctoring– Expertise and motivation of the trainer

Groin hernia: Groin hernia: endoscopicendoscopic repairrepair
• TAPP (Transabdominal Preperitoneal)more easy to learn - endoscopic suturingtransperitoneal approach
higher risk for postoperative intestinal obstructionDuron et al, Arch Surg 2000 Bringman and Blomqvist, Hernia 2005
laparoscopic exploration
•TEP (Totally ExtraPeritoneal) more difficult to learn
anatomy more difficult to understandlimited working space
preservation of peritoneal integrity – safer?laparoscopic exploration also easily possible
Groin hernia: anatomic aspectsGroin hernia: anatomic aspects
Be familiar with the anatomy!Be familiar with the anatomy!
inguinal ligament (Poupart)
genital branch of genitofemoral nerve
falx inguinalis – conjoint tendon
lacunar ligament (Gimbernat)
obturator artery
= pectineal ligament
ramus superior ossis pubis
pubic symphysis
TRIANGLE OF PAINTRIANGLE OF DOOM
indirect inguinal herniadirect
inguinal hernia
femoral hernia

SystematicSystematic TEP TEP inguinalinguinal hernia hernia repairrepair in 10 in 10 consecutiveconsecutive stepssteps
MiserezMiserez et al, et al, SurgSurg Lap Lap EndoscEndosc PercutPercut Tech 2009Tech 2009
1.1. IntroductionIntroduction of of firstfirst trocartrocar2.2. IntroductionIntroduction of of secondsecond trocartrocar3.3. DissectionDissection to to BogrosBogros’’ spacespace and and
introductionintroduction of of thirdthird trocartrocar4.4. ReductionReduction of direct of direct inguinalinguinal herniahernia5.5. ReductionReduction of of femoralfemoral//obturatorobturator herniahernia6.6. ReductionReduction of indirect of indirect inguinalinguinal herniahernia7.7. LateralLateral dissectiondissection and and reductionreduction of of
preperitonealpreperitoneal lipoma lipoma 7’ Contralateral dissection8.8. PreparationPreparation and and introductionintroduction of the of the meshmesh9.9. Placement of the Placement of the meshmesh and and fixationfixation
in in selectedselected casescases10.10. DesufflationDesufflation basic advanced

20 20 yearsyears oldold malemaleunilateralunilateral symptomaticsymptomaticinguinalinguinal hernia hernia leftleft sideside
right right sideside positivepositive onon ultrasound,ultrasound,clinicalclinical examinationexamination?, ?, nono symptomssymptoms
1. unilateral TAPP1. unilateral TAPP
2. bilateral TAPP2. bilateral TAPP
3. unilateral TEP3. unilateral TEP
4. bilateral TEP4. bilateral TEP
5. other5. other
40 40 yearsyears oldold femalefemaleunilateralunilateral femoralfemoral hernia, hernia,
minimal minimal symptomssymptoms
1. unilateral TAPP1. unilateral TAPP
2. unilateral TEP2. unilateral TEP
3. bilateral TAPP or TEP3. bilateral TAPP or TEP
4. Lichtenstein4. Lichtenstein
5. wait and see5. wait and see

80 80 yearsyears oldold malemaleASA IIIASA III
unilateralunilateral nonreduciblenonreducibleinguinoscrotalinguinoscrotal hernia, hernia,
symptomaticsymptomatic
1. unilateral TAPP1. unilateral TAPP
2. unilateral TEP2. unilateral TEP
3. unilateral Lichtenstein3. unilateral Lichtenstein
4. wait and see4. wait and see
50 50 yearsyears oldold malemaleoraloral anticoagulantsanticoagulants forfor CVACVA
bilateralbilateral inguinalinguinal herniaherniasymptomaticsymptomatic
1. bilateral TAPP1. bilateral TAPP
2. bilateral TEP2. bilateral TEP
3. bilateral Lichtenstein3. bilateral Lichtenstein
4. wait and see4. wait and see

70 70 yearsyears oldold malemalerecurrentrecurrent hernia hernia afterafter TEPTEP
symptomaticsymptomatic
1. TAPP1. TAPP
2. 2. reTEPreTEP
3. Lichtenstein3. Lichtenstein
4. wait and see4. wait and see
45 45 yearsyears oldold femalefemaleincarceratedincarcerated inguinalinguinal oror femoralfemoral herniahernia
1. TAPP1. TAPP
2. TEP2. TEP
3. open approach3. open approach
4. laparoscopy and open repair4. laparoscopy and open repair
5. laparoscopy and laparoscopic repair (TAPP or TEP)5. laparoscopy and laparoscopic repair (TAPP or TEP)

Treatment: laparoscopyTAPP vs. TEP
For endoscopic inguinal hernia techniques,For endoscopic inguinal hernia techniques,TAPP TAPP seemsseems to to bebe associatedassociated withwith higherhigher ratesratesof portof port--site site herniashernias and and visceralvisceral injuriesinjuries
whilewhile therethere appearappear to to bebe more conversions more conversions withwith TEPTEP
LevelLevel 2A2A TAPPTAPP TEPTEP openopen
VascularVascularinjuriesinjuries
0.13%0.13% 0%0% 0%0%
VisceralVisceralinjuriesinjuries
0.65%0.65% 0.16%0.16% 0.14%0.14%
MemonMemon et al, Br J et al, Br J SurgSurg 20032003McCormackMcCormack et al, Health et al, Health TechnologyTechnology AssessmentAssessment 20052005
Treatment: laparoscopy
TAPP vs. TEP
ItIt is is recommendedrecommended thatthat ananextraperitonealextraperitoneal approachapproach (TEP)(TEP)is is usedused forfor endoscopicendoscopic inguinalinguinal hernia hernia operationsoperations
Grade BGrade B

Our personal vision
“you do the best what you do the most”
posterior approach: laparoscopic (tep)
anterior approach: lichtenstein
Laparoscopic Laparoscopic ventral and incisional hernia repairventral and incisional hernia repair

IntroductionIntroductionDidDid youyou performperform laparoscopiclaparoscopic
ventral/ventral/incisionalincisional hernia hernia repairrepair yourselfyourself??
1. No1. No2. < 5 cases2. < 5 cases3. 53. 5--10 cases 10 cases 4. > 10 cases4. > 10 cases
IntroductionIntroductionWhatWhat is is youryour preferredpreferred techniquetechnique forfor
open open incisionalincisional hernia hernia repairrepair??
1. 1. OnlayOnlay2. 2. InlayInlay3. 3. SublaySublay
retromuscularretromuscular4. 4. UnderlayUnderlay

Mesh positioningMesh positioning
IPOM = intraperitoneal “onlay” = underlay!
?X
Mesh positioning: the gold standard?Mesh positioning: the gold standard?
retromuscularretromuscular((RivesRives--StoppaStoppa))
Rives et al, Bordeaux Med 1976; 26: 2115Stoppa, World J Surg 1989; 13: 545

LaparoscopicLaparoscopic vs. open: vs. open: argumentsarguments pro pro
minimal minimal abdominalabdominal wallwall tissue traumatissue traumalessless hematomahematoma, , seromaseroma, , woundwound infectioninfectionprostheticprosthetic infectioninfection??
cosmeticcosmetic benefitbenefit
shortershorter hospitalhospital staystay, , betterbetter recoveryrecovery
lessless postoperativepostoperative painpain
easiereasier explorationexploration of the of the wholewhole scarscarlessless recurrencesrecurrences ±± 5%??5%??
LaparoscopicLaparoscopic vs. open: vs. open: argumentsarguments concon
extensiveextensive adhesiolysisadhesiolysis necessarynecessary
prolongedprolonged ileusileus
missedmissed oror delayeddelayed enterotomyenterotomy, , postoperativepostoperative peritonitis, peritonitis, meshmesh infectioninfection & & removalremoval, , mortalitymortality
nono reconstructionreconstruction of the of the abdominalabdominal wallwall
recurrencerecurrence vs. vs. bulgingbulging
cavecave lightweightlightweight meshmesh
meshbridging
meshaugmentation
2%??

LaparoscopicLaparoscopic vs. open: vs. open: argumentsarguments concon
longlong--term effects of intraabdominal mesh term effects of intraabdominal mesh and fixation devicesand fixation devicesintestinal obstructionintestinal obstructionintestinal erosion and fistulisationintestinal erosion and fistulisation
more expensive prosthetic materialsmore expensive prosthetic materialsantiadhesive capacitiesantiadhesive capacities(chronic) infection risk(chronic) infection risk
chronic painchronic paintransfascial sutures and/or fixation devices?transfascial sutures and/or fixation devices?
chronic seroma formationchronic seroma formation ~ retention of hernia ~ retention of hernia sacsac
trocar site hernias trocar site hernias
longlong--termterm followfollow--up up necessarynecessary(min. 3 (min. 3 yearsyears))
muscles/anterior rectus sheath posterior rectus sheath/peritoneum
1. Onlay mesh bridging
2. Onlay mesh augmentation
3. Inlay mesh (= interposition)
4. Sublay mesh bridging
5. Sublay mesh augmentation
6. Underlay mesh bridging (= IPOM)
7. Underlay mesh augmentation
mesh

Meshes and fixation devicesMeshes and fixation devices
PolypropylenePolypropylene•• most most commonlycommonly usedused –– manymany different different
productsproducts
•• ProPro• macroporous (type I)• mostly monofilament• high tensile strength• mechanically stable• optimal tissue ingrowth• good tolerance to infection
•• ConCon• very rigid• not to be used in contact with viscera

Polyester (Polyester (polyethylenepolyethylene))•• MersileneMersilene ((EthiconEthicon) and ) and ParietexParietex ((CovidienCovidien))
•• ProPro• macroporous• optimal tissue ingrowth• softer than polypropylene
•• ConCon• multifilament (type III) ~ increased harvesting of bacteria• not to be used in contact with viscera• hydrolytic disintegration over years
(esp. in case of persisting infection)
ExpandedExpanded polytetrafluoroethylenepolytetrafluoroethylene((ePTFEePTFE))
•• ProPro• flexible, soft, nonfraying• high tensile strength• mechanically stable• can be used in contact with viscera• easily visible on ct-scan (foto dubois)
•• ConCon• microporous multifilament (type II)• less intense tissue ingrowth (encapsulation) – more
shrinkage• secure permanent fixation necessary• need for removal when infected (hydrophobic)

ClassificationClassification of of biomaterialsbiomaterialsType IType I totally macroporoustotally macroporous > 75> 75µµType IIType II totally microporoustotally microporous < 10< 10µµ
(in at least one of the 3 dimensions)(in at least one of the 3 dimensions)
Type IIIType III macroporous with multifilamentous or macroporous with multifilamentous or microporous componentsmicroporous components
Type IVType IV submicronic pore size submicronic pore size (only used in composite materials for adhesion prevention)(only used in composite materials for adhesion prevention)
pores > 75pores > 75µµ needed for admission of polymorphonuclear needed for admission of polymorphonuclear leucocytes (> 10leucocytes (> 10µµ), macrophages (), macrophages (≥≥ 5050µµ), fibroblasts, ), fibroblasts,
blood vessels and collagen fibers into the poresblood vessels and collagen fibers into the porestotal removal of the type II prosthesis and at least partial total removal of the type II prosthesis and at least partial
removal of the type III prosthesis is required removal of the type III prosthesis is required in order to manage infection (bacteria = 1in order to manage infection (bacteria = 1µµ))
Amid, Hernia 1997; 1: 15Amid, Hernia 1997; 1: 15
LightweightLightweight oror notnot??
• Current polypropylene meshes are likely to be too strong and too rigid
• Foreign body reaction too pronounced

• Pore size• Macroporous (> 75-100µm) vs. megaporous (> 700-1000µm)• Textile porosity vs. effective porosity
(% pores > 1000µm diameter)
• Weight or density
• > 80 g/m2
• < 40 g/m2
• Surface area
LightweightLightweight oror notnot::weightweight versus versus porepore sizesize
LightweightLightweight oror notnot??• Resulting mesh characteristics
• Tensile strength
• Uniaxial load testing• Load per unit width (N/cm)• Load per unit surface (N/cm2)
• Biaxial ball-burst testing
• Mesh elasticity
• Testing in different directionsfor anisotropic meshes
Cobb et al, Hernia 2009

Maximal abdominal pressure: 20 kPa (=150 mmHg)
• Mesh augmentation Thin walled ball
• Mesh bridging Thin walled cylinder
Maximal abdominal wall tensile strength: 82N/cm (horizontal)32N/cm (vertical)
FD
rD
l
D
L
Klinge et al, Chirurg 1996Klinge et al, World J Surg 2005
16N/cm
32N/cm
TensileTensile strengthstrength requirementsrequirements
•• ClosureClosure percutaneouslypercutaneously oror via via minilaparotomyminilaparotomy
•• Nonresorbable monofilament sutureNonresorbable monofilament suture
•• LessLess seromaseroma•• LessLess bulgebulge•• Not more chronic painNot more chronic pain
Chelala et al, Surg Endosc 2007Chelala et al, Surg Endosc 2007
•• Small defect (<5x5cm)Small defect (<5x5cm)not needednot needed
•• Large defect (>7x7cm)Large defect (>7x7cm)difficult/impossibledifficult/impossible
•• Intermediate defect orIntermediate defect orellipsoid defectellipsoid defect
ClosureClosure of the defect?of the defect?

MeshMesh elasticityelasticity most important most important in in verticalvertical directiondirection
Junge et al, Hernia 2001
EarlyEarly dislocationdislocation of a of a tootoo lightlightmeshmesh??

The ideal mesh for The ideal mesh for intraabdominalintraabdominal useuse
Optimal tissue incorporation/remodellingat the parietal side (macroporous)
No or minimal adhesion formationat the visceral side (microporous)
Easy handling capacities
Transparent and a bit sticky
Low cost
Tissue Tissue separatingseparating meshes (1):meshes (1):bioabsorbablebioabsorbable barriersbarriers
•• Hydrophilic collagenHydrophilic collagen--polyethylene glycolpolyethylene glycol--glycerol glycerol coatingcoating
– polyester Parietex® Composite– polypropylene Parietene®Composite
•• Sodium Sodium hyaluronatehyaluronate + + carboxymethylcellulosecarboxymethylcellulose((SeprafilmSeprafilm®®))
– polypropylene Sepramesh®
•• Oxidized regenerated cellulose (ORC)Oxidized regenerated cellulose (ORC)– polypropylene Proceed® (light weight)
•• Omega 3 fatty acidOmega 3 fatty acid– polypropylene C-Qur (Lite)™ (light weight)
AbsorbableAbsorbable barrierbarrierforfor
77--10 10 daysdaysSufficient?Sufficient?

Tissue separating meshes (2):Tissue separating meshes (2):composite meshes/coated meshescomposite meshes/coated meshes
•• ePTFEePTFE– polypropylene Composix®
Composix® E/X
Composix® L/P(lightweight)
Tissue Tissue separatingseparating meshes (3): meshes (3): ePTFEePTFE
– DualMesh®
– DualMesh® Plus• antimicrobial agents:
– silver– chlorhexidine
– DualMesh® Plus with Holes • macropores for faster tissue attachment
corduroy surface
20-22µ
< 3µ

HowHow to to choosechoose??
••A lot of (A lot of (oftenoften conflictingconflicting) ) animalanimal datadata
••No RCT No RCT comparingcomparing onlyonly twotwo different different meshmesh materialsmaterials
• No human clinical studies needed for FDA approval/CE marking
• Mesh half life is often (very) short
••RetrospectiveRetrospective data data onon meshmeshcomplicationscomplications
Few data on Few data on relookrelook laparoscopieslaparoscopiesChelalaChelala et al, Hernia 2010et al, Hernia 2010
••N=85N=85
••Neoperitoneum perfectly covering the Neoperitoneum perfectly covering the meshmesh
••No shrinking or wrinkling of the meshNo shrinking or wrinkling of the mesh

How to choose?How to choose?••CaveatCaveat
• ePTFE mesh component in case of (potential) contamination
• secure permanent fixation necessary when using full ePTFE
• Laparoscopic ventral/incisional hernia repair• Fragile antiadhesive barrier• Bulky mesh when rolling• Lightweight mesh for bridging large defect• Transparence, memory, abdominal wall adhesive capacity• Adequate dimension or easy to be cut without loosing
antiadhesive properties• Cost!
MeshMesh fixationfixation: : whatwhat to to useuse??
1. 1. suturessutures
2. 2. fixationfixation devicesdevices
3. 3. combinationcombination of of bothboth
4. 4. glueglue

MeshMesh fixationfixation: : whatwhat to to useuse??suturessutures
nonnon--resorbableresorbable((slowlyslowly) ) resorbableresorbable
fixationfixation devicesdevicessingle single crowncrown
double double crowncrownCarbajoCarbajo et alet al
MoralesMorales--CondeConde et alet al
CombinationCombination
GlueGlueto cover to cover fixationfixation devicesdevices and and meshmesh edgesedges??to to diminishdiminish the the numbernumber of of fixationfixation devicesdevices??
??
Fixation: sutures + fixation devicesFixation: sutures + fixation devicesfull thickness transparietal sutures
slowly resorbableaccurate orientation and placement of the mesh
additional fixation first 3-4 weeks minimising the risk for chronic pain
at least 4 - every 6cm
careful grasping of the suture
enough tissue incorporation (1enough tissue incorporation (1--1.5cm)1.5cm)
nonresorbablenonresorbable sutures in case of full sutures in case of full ePTFEePTFE meshmesh

LVHR: fixation devicesLVHR: fixation devices
Protack®
titanium (n=30)
absorbable5mm
Sorbafix
AbsorbaTackabsorbable
5mm
TensileTensile strengthstrength andand adhesionadhesionformationformation toto fixationfixation systemssystems
Absorba Tack and SorbaFix are resp. solid and hollow screw tacks, completely resorbed after one year

Parietene Composite Parietene Composite --AbsorbatackAbsorbatack
TensileTensile strengthstrength andand adhesionadhesionformationformation toto fixationfixation systemssystems
HollinskyHollinsky et al, et al, SurgSurg EndoscEndosc 20102010
Rat modelParietex Composite mesh
Prolene suture

WhatWhat aboutabout painpain??KumarKumar BansalBansal et al, et al, SurgSurg EndoscEndosc 20112011
RCT, laparoscopic repair, majority polypropylene mesh
ProtackPolypropylene
ButButWassenaar et al, Wassenaar et al, SurgSurg EndoscEndosc 20102010
+ tacks+ tacks

Fixation: sutures + fixation devicesFixation: sutures + fixation devicesfixation devices
every 2cm and at least 1cm from the edge of the meshavoid recurrence between mesh and abdominal wall !avoid recurrence between mesh and abdominal wall !
double crown techniqueto reduce dead space
to increase tissue ingrowth
deep enough(≠ peritoneum or preperitoneal fat)
external counterpressure!
extra 5mm trocar contralaterally if needed

•• 10 RCT10 RCT
•• AlmostAlmost 1000 1000 patientspatients
•• ClinicalClinical• Hernia size/location
• Surgical technique• Open:
• onlay, sublay• fascial closure
• Laparoscopic: • mesh overlap• mesh fixation
• Learning curve effect
= IPOM
Large heterogeneity in the different Large heterogeneity in the different trialstrials

Large heterogeneity in the different Large heterogeneity in the different trialstrials
•• MethodologicalMethodological
randomisation process
(primary outcome parameter)
Operation timeOperation time
Results too heterogenous to be pooled

ComplicationsComplications
Any complicationAny complication
Major vs. minor complicationsMajor vs. minor complications•• MinorMinor
• Wound infection• Seroma formation: problem of definition• Hematoma• Acute and chronic pain
•• MajorMajor• (Missed) enterotomy• Mesh removal• Reoperation• Mortality

EnterotomyEnterotomy
recognisedrecognised andand unrecognisedunrecognised
No results extractableon ICU admission
No mortality(described)
HematomaHematoma--seromaseroma

SeromaSeroma vs. open vs. open meshmesh placementplacement
WoundWound infectioninfection

WoundWound infectioninfection vs. vs. open open meshmesh placementplacement
HospitalHospital staystay
SignificantlySignificantly shortershorter in 6/9 trialsin 6/9 trialsBut large But large heterogeneityheterogeneity

HospitalHospital staystay
ShortShort--term term painpain
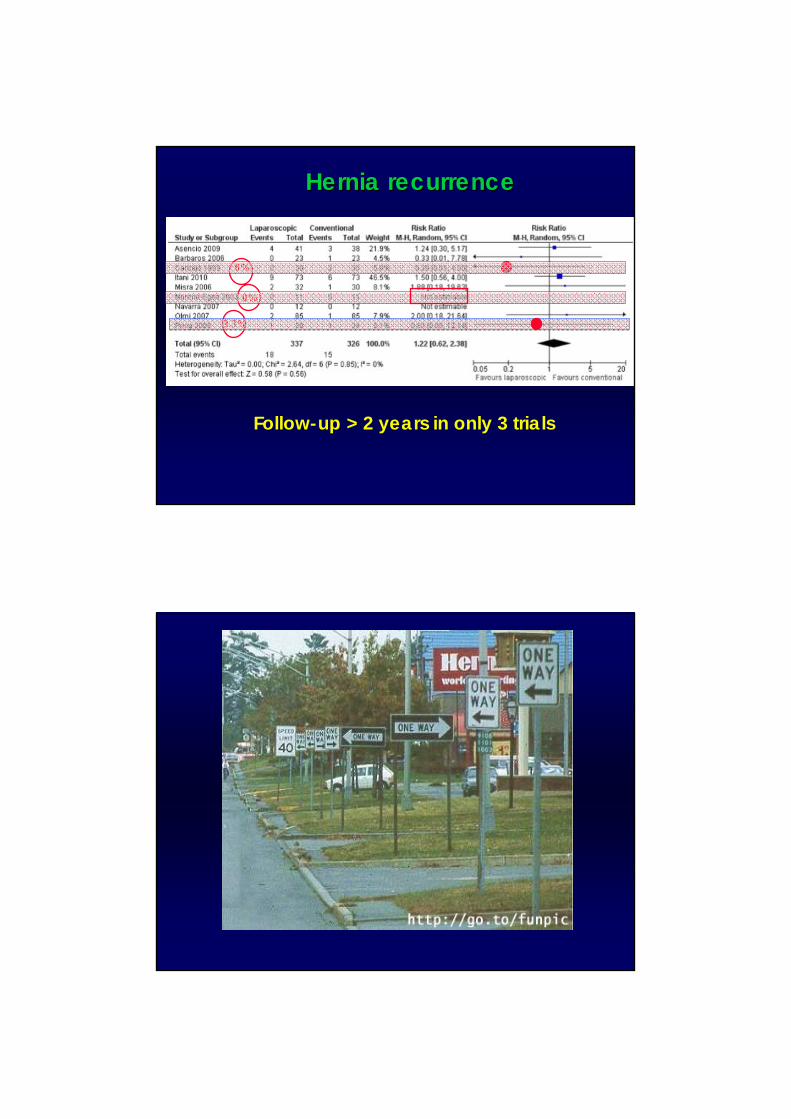
Hernia recurrenceHernia recurrence
Follow-up > 2 years in only 3 trials
3.3%
0%
0%

EBM based conclusionsEBM based conclusions
•• LargeLarge heterogeneityheterogeneity in the different trialsin the different trials
•• LaparoscopicLaparoscopic incisionalincisional hernia hernia repairrepair• Is safe • Benefit of decreased wound infections and shorter
hospital stay• No increased recurrence rates with medium-term
follow-up
• The key to succes is a careful adhesiolysis and avoiding/immediate treatment of enterotomy
• No decrease in acute pain
My personal conclusions My personal conclusions ••Excellent indication inExcellent indication in
• Obese patients – diabetics• Lateral hernias• Parastomal hernias
••Beware for patients withBeware for patients with• Wide hernias or a diffuse bulge• Hernias close to bony edges: extraperitoneal mesh
••Careful patient selection in learning curveCareful patient selection in learning curve• Eg. umbilical hernia/trocar site hernia in obese patient• Exploration of the whole scar
rectus muscle
posterior rectus sheath/peritoneum
Miserez and Penninckx, Surg Endosc 2002; 16: 1207-1213





























