Embed Size (px)
Citation preview

*¶dAm
A
CJpGAS
Ar
p
Journal of the American College of Cardiology Vol. 55, No. 14, 2010© 2010 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/10/$36.00P
PRACTICE GUIDELINE: FULL TEXT
2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVMGuidelines for the Diagnosis and Management ofPatients With Thoracic Aortic DiseaseA Report of the American College of Cardiology Foundation/American Heart Association Task Forceon Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for CardiovascularAngiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine
Endorsed by the North American Society for Cardiovascular Imaging
WRITING GROUP MEMBERSLoren F. Hiratzka, MD, Chair*; George L. Bakris, MD†; Joshua A. Beckman, MD, MS‡;Robert M. Bersin, MD§; Vincent F. Carr, DO�; Donald E. Casey Jr, MD, MPH, MBA¶;
Kim A. Eagle, MD*#; Luke K. Hermann, MD**; Eric M. Isselbacher, MD*;Ella A. Kazerooni, MD, MS††; Nicholas T. Kouchoukos, MD‡‡; Bruce W. Lytle, MD§§;
Dianna M. Milewicz, MD, PhD; David L. Reich, MD��; Souvik Sen, MD, MS¶¶;Julie A. Shinn, RN, MA, CCRN†; Lars G. Svensson, MD, PhD##;
David M. Williams, MD#***
ACCF/AHA TASK FORCE MEMBERSAlice K. Jacobs, MD, FACC, FAHA, Chair 2009–2011; Sidney C. Smith, Jr, MD, FACC, FAHA,
Immediate Past Chair 2006–2008†††; Jeffery L. Anderson, MD, FACC, FAHA, Chair-Elect;Cynthia D. Adams, MSN, PhD, FAHA†††; Christopher E. Buller, MD, FACC;
Mark A. Creager, MD, FACC, FAHA; Steven M. Ettinger, MD, FACC;Robert A. Guyton, MD, FACC, FAHA; Jonathan L. Halperin, MD, FACC, FAHA;
Sharon A. Hunt, MD, FACC, FAHA†††; Harlan M. Krumholz, MD, FACC, FAHA†††;Frederick G. Kushner, MD, FACC, FAHA; Bruce W. Lytle, MD, FACC, FAHA†††;Rick Nishimura, MD, FACC, FAHA†††; Richard L. Page, MD, FACC, FAHA†††;Barbara Riegel, DNSc, RN, FAHA***; William G. Stevenson, MD, FACC, FAHA;
Lynn G. Tarkington, RN; Clyde W. Yancy, MD, FACC, FAHA
ACCF/AHA Representative. †AHA Representative. ‡SVM Representative. §SCAI Representative. �ACCF Board of Governors Representative.American College of Physicians Representative. #Recused from Section 9.2.2.3.1. Recommendations for Descending Thoracic Aorta and Thoracoab-ominal Aortic Aneurysms. **American College of Emergency Physicians Representative. ††ACR Representative. ‡‡STS Representative. §§ACCF/HA Task Force Liaison. ��SCA Representative. ¶¶ASA Representative. ##AATS Representative. ***SIR Representative. †††Former Task Forceember during this writing effort.Authors with no symbol by their name were included to provide additional content expertise apart from organizational representation.This document was approved by the American College of Cardiology Foundation Board of Trustees and the American Heart Association Science
dvisory and Coordinating Committee in January 2010. All other cosponsoring organizations approved in February 2010.The American College of Cardiology Foundation requests that this document be cited as follows: Hiratzka LF, Bakris GL, Beckman JA, Bersin RM,
arr VF, Casey DE Jr, Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos NT, Lytle BW, Milewicz DM, Reich DL, Sen S, ShinnA, Svensson LG, Williams DM. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management ofatients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practiceuidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascularnesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, andociety for Vascular Medicine (developed in collaboration with the American College of Emergency Physicians). J Am Coll Cardiol 2010;55:e27–129.This article has been copublished in Circulation.Copies: This document is available on the World Wide Web sites of the American College of Cardiology (www.acc.org) and the American Heart
ssociation (my.americanheart.org). For copies of this document, please contact Elsevier Inc. Reprint Department, fax 212-633-3820, e-mail:[email protected].
ublished by Elsevier Inc. doi:10.1016/j.jacc.2010.02.015
Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the expressermission of the American College of Cardiology Foundation. Please contact Elsevier’s permission department at [email protected].

P
e28 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
TABLE OF CONTENTS
reamble . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e31
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e31
1.1. Methodology and Evidence Review . . . . . .e311.2. Organization of the Writing Committee . .e321.3. Document Review and Approval . . . . . . . . .e321.4. Scope of the Guideline . . . . . . . . . . . . . . . . . .e33
1.4.1. Critical Issues . . . . . . . . . . . . . . . . . . . . .e351.5. Glossary of Terms and Abbreviations Used
Throughout Guideline . . . . . . . . . . . . . . . . . . .e35
2. The Thoracic Aorta . . . . . . . . . . . . . . . . . . . . . . . . . . .e36
2.1. The Normal Aorta . . . . . . . . . . . . . . . . . . . . . . .e362.2. Normal Thoracic Aortic Diameter . . . . . . . .e36
3. Thoracic Aortic Histopathology . . . . . . . . . . . . . . .e37
3.1. Atherosclerosis . . . . . . . . . . . . . . . . . . . . . . . . .e373.2. Aneurysms and Dissections . . . . . . . . . . . . .e373.3. Vasculitis and Inflammatory Diseases. . . .e38
4. Imaging Modalities . . . . . . . . . . . . . . . . . . . . . . . . . . .e39
4.1. Recommendations for Aortic ImagingTechniques to Determine the Presence andProgression of Thoracic Aortic Disease . .e39
4.2. Chest X-Ray . . . . . . . . . . . . . . . . . . . . . . . . . . . .e404.3. Computed Tomographic Imaging . . . . . . . . .e40
4.3.1. Computed Tomographic ImagingTechnique . . . . . . . . . . . . . . . . . . . . . . . .e42
4.4. Magnetic Resonance Imaging . . . . . . . . . . .e424.4.1. Magnetic Resonance Imaging
Technique . . . . . . . . . . . . . . . . . . . . . . . .e434.4.2. Black Blood Imaging . . . . . . . . . . . . . . .e434.4.3. Noncontrast White Blood Imaging . . .e434.4.4. Contrast-Enhanced Magnetic Resonance
Angiography. . . . . . . . . . . . . . . . . . . . . . .e434.4.5. Phase Contrast Imaging. . . . . . . . . . . . .e43
4.5. Standards for Reporting of the ThoracicAorta on Computed Tomography andMagnetic Resonance Imaging . . . . . . . . . . .e43
4.6. Angiography . . . . . . . . . . . . . . . . . . . . . . . . . . . .e444.7. Echocardiography . . . . . . . . . . . . . . . . . . . . . . .e45
4.7.1. Echocardiographic Criteria for ThoracicAortic Aneurysms . . . . . . . . . . . . . . . . . .e45
4.7.2. Echocardiographic Criteria for AorticDissection. . . . . . . . . . . . . . . . . . . . . . . . .e454.7.2.1. DIAGNOSTIC ACCURACY OF
ECHOCARDIOGRAPHY FOR AORTICDISSECTION. . . . . . . . . . . . . . . . . . . . . . .e46
4.7.2.2. DIAGNOSTIC ACCURACY OFECHOCARDIOGRAPHY FOR ACUTEINTRAMURAL HEMATOMA . . . . . . .e46
4.7.2.3. ROLE OF ECHOCARDIOGRAPHY INFOLLOWING PATIENTS WITHCHRONIC AORTIC DISEASE . . . . . .e47
5. Genetic Syndromes Associated With ThoracicAortic Aneurysms and Dissections . . . . . . . . . . . .e47
5.1. Recommendations for GeneticSyndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e475.1.1. Marfan Syndrome . . . . . . . . . . . . . . . . . .e48
5.1.2. Loeys-Dietz Syndrome . . . . . . . . . . . . . .e495.1.3. Ehlers-Danlos Syndrome, Vascular Formor Type IV . . . . . . . . . . . . . . . . . . . . . . . .e49
5.1.4. Turner Syndrome . . . . . . . . . . . . . . . . . .e495.1.5. Other Genetic Syndromes With
Increased Risk for Thoracic AorticAneurysms and Dissections . . . . . . . . . .e50
5.1.6. Recommendations for Familial ThoracicAortic Aneurysms and Dissections . . . .e50
5.2. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e51
6. Other Cardiovascular Conditions Associated WithThoracic Aortic Aneurysm and Dissection. . . . . .e52
6.1. Recommendations for Bicuspid Aortic Valveand Associated Congenital Variants inAdults . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e52
6.2. Aberrant Right Subclavian Artery . . . . . . . .e536.3. Coarctation of the Aorta . . . . . . . . . . . . . . . .e536.4. Right Aortic Arch . . . . . . . . . . . . . . . . . . . . . . .e53
7. Inflammatory Diseases Associated With ThoracicAortic Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e53
7.1. Recommendations for Takayasu Arteritisand Giant Cell Arteritis . . . . . . . . . . . . . . . . . .e53
7.2. Takayasu Arteritis . . . . . . . . . . . . . . . . . . . . . .e547.3. Giant Cell Arteritis . . . . . . . . . . . . . . . . . . . . . .e567.4. Behcet Disease . . . . . . . . . . . . . . . . . . . . . . . . .e577.5. Ankylosing Spondylitis
(Spondyloarthropathies) . . . . . . . . . . . . . . . .e577.6. Infective Thoracic Aortic Aneurysms . . . . .e57
8. Acute Aortic Syndromes . . . . . . . . . . . . . . . . . . . . . .e58
8.1. Aortic Dissection . . . . . . . . . . . . . . . . . . . . . . .e588.1.1. Aortic Dissection Definition . . . . . . . .e588.1.2. Anatomic Classification of Aortic
Dissection. . . . . . . . . . . . . . . . . . . . . . . .e588.1.3. Risk Factors for Aortic Dissection . . .e618.1.4. Clinical Presentation of Acute Thoracic
Aortic Dissection . . . . . . . . . . . . . . . . .e628.1.4.1. SYMPTOMS OF ACUTE THORACIC
AORTIC DISSECTION . . . . . . . . . . . .e628.1.4.2. PERFUSION DEFICITS AND END-
ORGAN ISCHEMIA . . . . . . . . . . . . . . .e628.1.5. Cardiac Complications . . . . . . . . . . . . .e64
8.1.5.1. ACUTE AORTICREGURGITATION . . . . . . . . . . . . . . . .e64
8.1.5.2. MYOCARDIAL ISCHEMIA ORINFARCTION . . . . . . . . . . . . . . . . . . . . .e64
8.1.5.3. HEART FAILURE AND SHOCK . . .e648.1.5.4. PERICARDIAL EFFUSION AND
TAMPONADE. . . . . . . . . . . . . . . . . . . . .e648.1.6. Syncope . . . . . . . . . . . . . . . . . . . . . . . . .e648.1.7. Neurologic Complications . . . . . . . . . .e658.1.8. Pulmonary Complications . . . . . . . . . .e658.1.9. Gastrointestinal Complications. . . . . .e65
8.1.10. Blood Pressure and Heart RateConsiderations . . . . . . . . . . . . . . . . . . . .e65
8.1.11. Age and Sex Considerations . . . . . . . .e658.2. Intramural Hematoma . . . . . . . . . . . . . . . . . . .e668.3. Penetrating Atherosclerotic Ulcer . . . . . . .e678.4. Pseudoaneurysms of the Thoracic Aorta .e678.5. Traumatic Rupture of the Thoracic Aorta .e678.6. Evaluation and Management of Acute
Thoracic Aortic Disease . . . . . . . . . . . . . . . . .e68
1
e29JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
8.6.1. Initial Evaluation and Management. . .e688.6.1.1. RECOMMENDATIONS FOR
ESTIMATION OF PRETEST RISK OFTHORACIC AORTIC DISSECTION . .e68
8.6.1.2. LABORATORY TESTING. . . . . . . . . . .e688.6.1.3. RECOMMENDATIONS FOR
SCREENING TESTS . . . . . . . . . . . . . . . .e698.6.1.4. RECOMMENDATIONS FOR
DIAGNOSTIC IMAGING STUDIES . .e698.6.1.5. RECOMMENDATIONS FOR INITIAL
MANAGEMENT . . . . . . . . . . . . . . . . . . . .e698.6.1.6. RECOMMENDATIONS FOR
DEFINITIVE MANAGEMENT . . . . . .e698.6.2. Evaluation and Management
Algorithms . . . . . . . . . . . . . . . . . . . . . . . .e708.6.3. Initial Management . . . . . . . . . . . . . . . .e71
8.6.3.1. BLOOD PRESSURE AND RATECONTROL THERAPY . . . . . . . . . . . . . .e71
8.6.3.2. ADDITIONAL ANTIHYPERTENSIVETHERAPY . . . . . . . . . . . . . . . . . . . . . . . . . .e73
8.6.3.3. PAIN CONTROL . . . . . . . . . . . . . . . . . . .e738.6.3.4. HYPOTENSION . . . . . . . . . . . . . . . . . . . .e738.6.3.5. DETERMINING DEFINITIVE
MANAGEMENT . . . . . . . . . . . . . . . . . . . .e738.6.4. Recommendation for Surgical
Intervention for Acute Thoracic AorticDissection. . . . . . . . . . . . . . . . . . . . . . . . .e73
8.6.5. Endovascular Interventions . . . . . . . . . .e738.6.6. Principles of Treatment for Intramural
Hematoma and PenetratingAtherosclerotic Ulcer . . . . . . . . . . . . . . .e748.6.6.1. INTIMAL DEFECT WITHOUT
INTRAMURAL HEMATOMA . . . . . . .e748.6.6.2. INTIMAL DEFECT WITH
INTRAMURAL HEMATOMA . . . . . . .e748.6.6.3. RECOMMENDATION FOR
INTRAMURAL HEMATOMAWITHOUT INTIMAL DEFECT . . . . .e74
8.7. Treatment for the Management ofTraumatic Aortic Rupture. . . . . . . . . . . . . . . .e74
9. Thoracic Aortic Aneurysms . . . . . . . . . . . . . . . . . . .e75
9.1. General Approach to the Patient. . . . . . . . .e769.1.1. Recommendation for History and
Physical Examination for ThoracicAortic Disease . . . . . . . . . . . . . . . . . . . . .e769.1.1.1. CORONARY ARTERY DISEASE . . . .e779.1.1.2. EMBOLI . . . . . . . . . . . . . . . . . . . . . . . . . . .e789.1.1.3. ASSOCIATED RENAL ISCHEMIA . .e789.1.1.4. ASSOCIATED MESENTERIC
ISCHEMIA . . . . . . . . . . . . . . . . . . . . . . . . .e789.1.1.5. ASSOCIATED PERIPHERAL
ISCHEMIA . . . . . . . . . . . . . . . . . . . . . . . . .e789.1.2. Differential Diagnosis. . . . . . . . . . . . . . .e78
9.1.2.1. SYMPTOMS . . . . . . . . . . . . . . . . . . . . . . . .e789.1.2.2. PHYSICAL FINDINGS . . . . . . . . . . . . . .e78
9.1.3. Considerations for Imaging . . . . . . . . . .e799.2. General Medical Treatment and Risk Factor
Management for Patients With ThoracicAortic Disease . . . . . . . . . . . . . . . . . . . . . . . . . .e799.2.1. Recommendation for Medical Treatment
of Patients With Thoracic AorticDiseases . . . . . . . . . . . . . . . . . . . . . . . . . .e799.2.1.1. RECOMMENDATIONS FOR BLOOD
PRESSURE CONTROL . . . . . . . . . . . . .e80
9.2.1.2. RECOMMENDATION FORDYSLIPIDEMIA . . . . . . . . . . . . . . . . . . . .e80
9.2.1.3. RECOMMENDATION FOR SMOKINGCESSATION. . . . . . . . . . . . . . . . . . . . . . . .e80
9.2.2. Surgical and Endovascular Treatment byLocation of Disease . . . . . . . . . . . . . . . .e819.2.2.1. ASCENDING AORTA AND AORTIC
SINUSES . . . . . . . . . . . . . . . . . . . . . . . . . . .e819.2.2.1.1. Recommendations for
Asymptomatic PatientsWith AscendingAortic Aneurysm . . . . . .e81
9.2.2.1.2. Recommendation forSymptomatic PatientsWith ThoracicAortic Aneurysm . . . . . .e81
9.2.2.1.3. Endovascular Graftingfor Ascending AorticAneurysm. . . . . . . . . . . .e82
9.2.2.1.4. Recommendations forOpen Surgery forAscending AorticAneurysm. . . . . . . . . . . .e82
9.2.2.2. RECOMMENDATIONS FOR AORTICARCH ANEURYSMS . . . . . . . . . . . . . . . .e849.2.2.2.1. Open Surgery . . . . . . . . .e84
9.2.2.3. DESCENDING THORACIC AORTAAND THORACOABDOMINALAORTA . . . . . . . . . . . . . . . . . . . . . . . . . . . .e849.2.2.3.1. Recommendations for
Descending ThoracicAorta andThoracoabdominalAortic Aneurysms . . . . .e84
9.2.2.3.2. Endovascular VersusOpen SurgicalApproach . . . . . . . . . . . .e85
9.2.2.3.3. End-OrganPreservationDuring ThoracicEndograftImplantation. . . . . . . . . .e86
9.2.2.3.4. PeriproceduralComplications ofEndograftProcedures . . . . . . . . . . .e87
9.2.2.3.5. Open Surgical . . . . . . . .e889.2.2.3.6. End-Organ
PreservationDuring OpenThoracoabdominalRepairs . . . . . . . . . . . . . .e89
9.2.2.3.7. Aortic Dissection WithMalperfusion . . . . . . . . .e89
0. Special Considerations in Pregnant Patients WithAortic Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e89
10.1. Effects of Pregnancy on the Aorta. . . . . .e8910.2. Epidemiology of Chronic and Acute Aortic
Conditions in Pregnancy . . . . . . . . . . . . . . .e8910.3. Counseling and Management of Chronic
Aortic Diseases in Pregnancy . . . . . . . . . .e90

1
1
1
1
1
1
1
1
R
AO
Aan
A
e30 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
10.3.1. Recommendations for Counseling andManagement of Chronic AorticDiseases in Pregnancy . . . . . . . . . . . .e89
10.4. Evaluation and Management of AcuteAortic Syndromes During Pregnancy . . . .e90
1. Aortic Arch and Thoracic Aortic Atheroma andAtheroembolic Disease . . . . . . . . . . . . . . . . . . . . . . .e90
11.1. Recommendations for Aortic Arch andThoracic Aortic Atheroma andAtheroembolic Disease . . . . . . . . . . . . . . . .e90
11.2. Clinical Description . . . . . . . . . . . . . . . . . . . .e9011.3. Risk Factors. . . . . . . . . . . . . . . . . . . . . . . . . . .e9111.4. Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e9111.5. Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e91
11.5.1. Anticoagulation Versus AntiplateletTherapy . . . . . . . . . . . . . . . . . . . . . . . .e91
11.5.2. Lipid-Lowering Agent . . . . . . . . . . . .e9211.5.3. Surgical and Interventional
Approaches . . . . . . . . . . . . . . . . . . . . .e92
2. Porcelain Aorta . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e92
3. Tumors of the Thoracic Aorta . . . . . . . . . . . . . . . . .e93
4. Perioperative Care for Open Surgical andEndovascular Thoracic Aortic Repairs . . . . . . . . .e93
14.1. Recommendations for PreoperativeEvaluation. . . . . . . . . . . . . . . . . . . . . . . . . . . . .e9314.1.1. Preoperative Risk Assessment. . . . . .e94
14.2. Recommendations for Choice ofAnesthetic and Monitoring Techniques. .e9514.2.1. Temperature Monitoring . . . . . . . . . .e9514.2.2. Hemodynamic Monitoring . . . . . . . .e9514.2.3. Transesophageal Echocardiography . .e9614.2.4. Transesophageal Echocardiography for
Endovascular Repairs of theDescending Thoracic Aorta. . . . . . . .e96
14.3. Airway Management for DescendingThoracic Aortic Repairs . . . . . . . . . . . . . . . .e96
14.4. Recommendation for TransfusionManagement and Anticoagulation inThoracic Aortic Surgery . . . . . . . . . . . . . . . .e96
14.5. Organ Protection . . . . . . . . . . . . . . . . . . . . . .e9714.5.1. Recommendations for Brain Protection
During Ascending Aortic andTransverse Aortic Arch Surgery . . . .e97
14.5.2. Recommendations for Spinal CordProtection During Descending AorticOpen Surgical and EndovascularRepairs . . . . . . . . . . . . . . . . . . . . . . . . .e9814.5.2.1. MONITORING OF SPINAL
CORD FUNCTION INDESCENDING THORACICAORTIC REPAIRS. . . . . . . . . . . . . .e99
14.5.2.2. MAINTENANCE OF SPINAL CORDARTERIAL PRESSURE. . . . . . . . . .e99
14.5.2.3. CEREBROSPINAL FLUIDPRESSURE AND DRAINAGE . . .e99
14.5.2.4. HYPOTHERMIA . . . . . . . . . . . . . .e10014.5.2.5. GLUCOCORTICOIDS AND
MANNITOL . . . . . . . . . . . . . . . . . . .e10014.5.3. Recommendations for Renal
Protection During Descending Aortic
Open Surgical and EndovascularRepairs . . . . . . . . . . . . . . . . . . . . . . . .e100
14.6. Complications of Open SurgicalApproaches . . . . . . . . . . . . . . . . . . . . . . . . . .e100
14.7. Mortality Risk for Thoracic AorticSurgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e101
14.8. Postprocedural Care . . . . . . . . . . . . . . . . . .e10214.8.1. Postoperative Risk Factor
Management . . . . . . . . . . . . . . . . . . .e10214.8.2. Recommendations for Surveillance of
Thoracic Aortic Disease or PreviouslyRepaired Patients . . . . . . . . . . . . . . .e102
5. Nursing Care and Patient/Family Education . .e103
15.1. Nursing Care of Medically ManagedPatients. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e103
15.2. Preprocedural Nursing Care . . . . . . . . . . .e10315.3. Postprocedural Nursing Care . . . . . . . . . .e10315.4. Nursing Care of Surgically Managed
Patients. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e104
6. Long-Term Issues . . . . . . . . . . . . . . . . . . . . . . . . . . .e105
16.1. Recommendation for Employment andLifestyle in Patients With Thoracic AorticDisease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e105
7. Institutional/Hospital Quality Concerns . . . . . .e106
17.1. Recommendations for Quality Assessmentand Improvement for Thoracic AorticDisease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e106
17.2. Interinstitutional Issues . . . . . . . . . . . . . .e107
8. Future Research Directions and Issues. . . . . . .e107
18.1. Risks and Benefits of Current ImagingTechnologies . . . . . . . . . . . . . . . . . . . . . . . . .e107
18.2. Mechanisms of Aortic Dissection . . . . . .e10818.3. Treatment of Malperfusion and
Reperfusion Injury . . . . . . . . . . . . . . . . . . . .e10818.4. Gene-Based Mechanisms and Models . .e108
18.4.1. Aortic Disease Management Based onthe Underlying Genetic Defects . . .e108
18.4.2. Biomarkers for Acute AorticDissection . . . . . . . . . . . . . . . . . . . . .e108
18.4.3. Genetic Defects and MolecularPathway Analyses . . . . . . . . . . . . . . .e108
18.4.4. Clinical Trials for Medical Therapy forAortic Aneurysms . . . . . . . . . . . . . . .e108
18.5. Aortic Atheroma and AtherosclerosisIdentification and Treatment . . . . . . . . . .e108
18.6. Prediction Models of Aortic Rupture and theNeed for Preemptive Interventions . . . . .e108
18.7. National Heart, Lung, and Blood InstituteWorking Group Recommendations . . . . .e108
eferences . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e109
ppendix 1. Author Relationships With Industry andther Entities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e126
ppendix 2. Reviewer Relationships With Industryd Other Entities. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .e128
ppendix 3. Abbreviation List . . . . . . . . . . . . . . . . . . . .e130

P
Itcranofavrianefprprasde
anencaFoupdiovasdepr
sedafrcolitagesPatiethstouin
evoforcarerewrecomnorewwinguthduco
listiotoinguAthavC
prgeanshardeciafevFoarid
rePrreBadpracst
pacajubyciarar
Acudi
1
1TthPuw
e31JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
reamble
is essential that the medical profession play a central role initically evaluating the evidence related to drugs, devices,d procedures for the detection, management, or preventiondisease. Properly applied, rigorous, expert analysis of theailable data documenting absolute and relative benefits and
sks of these therapies and procedures can improve outcomesd reduce costs of care by focusing resources on the most
fective strategies. One important use of such data is theoduction of clinical practice guidelines that, in turn, canovide a foundation for a variety of other applications suchperformance measures, appropriate use criteria, clinical
cision support tools, and quality improvement tools.The American College of Cardiology Foundation (ACCF)d the American Heart Association (AHA) have jointlygaged in the production of guidelines in the area ofrdiovascular disease since 1980. The ACCF/AHA Taskrce on Practice Guidelines is charged with developing,dating, and revising practice guidelines for cardiovascularseases and procedures, and the Task Force directs andersees this effort. Writing committees are charged withsessing the evidence as an independent group of authors tovelop, update, or revise recommendations for clinicalactice.Experts in the subject under consideration have beenlected from both organizations to examine subject-specificta and write guidelines in partnership with representatives
om other medical practitioner and specialty groups. Writingmmittees are specifically charged to perform a formalerature review, weigh the strength of evidence for orainst particular treatments or procedures, and includetimates of expected health outcomes where data exist.tient-specific modifiers, comorbidities, and issues of pa-nt preference that may influence the choice of tests orerapies are considered. When available, information fromudies on cost is considered, but data on efficacy and clinicaltcomes constitute the primary basis for recommendationsthese guidelines.The ACCF/AHA Task Force on Practice Guidelines makesery effort to avoid actual, potential, or perceived conflictsinterest that may arise as a result of industry relationshipspersonal interests among the writing committee. Specifi-
lly, all members of the writing committee, as well as peerviewers of the document, are asked to disclose all currentlationships and those 24 months prior to initiation of theriting effort that may be perceived as relevant. All guidelinecommendations require a confidential vote by the writingmmittee and must be approved by a consensus of theembers voting. Members who were recused from voting areted on the title page of this document. Members mustcuse themselves from voting on any recommendationhere their relationships with industry (RWI) apply. If ariting committee member develops a new relationship withdustry during his/her tenure, he/she is required to notifyideline staff in writing. These statements are reviewed bye Task Force on Practice Guidelines and all membersring each conference call and/or meeting of the writing
mmittee, updated as changes occur, and ultimately pub- rehed as an appendix to the document. For detailed informa-n regarding guideline policies and procedures, please referthe methodology manual for ACCF/AHA Guideline Writ-
g Committees (1). RWI and other entities pertinent to thisideline for authors and peer reviewers are disclosed in
ppendixes 1 and 2, respectively. Disclosure information fore ACCF/AHA Task Force on Practice Guidelines is alsoailable online at (http://www.acc.org/about/overview/
linicalDocumentsTaskForces.cfm).These practice guidelines are intended to assist healthcareoviders in clinical decision making by describing a range ofnerally acceptable approaches for diagnosis, management,d prevention of specific diseases or conditions. Cliniciansould consider the quality and availability of expertise in theea where care is provided. These guidelines attempt tofine practices that meet the needs of most patients in mostrcumstances. The recommendations reflect a consensuster a thorough review of the available current scientificidence and are intended to improve patient care. The Taskrce recognizes that situations arise where additional data
e needed to better inform patient care; these areas will beentified within each respective guideline when appropriate.Patient adherence to prescribed and agreed upon medicalgimens and lifestyles is an important aspect of treatment.escribed courses of treatment in accordance with thesecommendations are effective only if they are followed.ecause lack of patient understanding and adherence mayversely affect outcomes, physicians and other healthcareoviders should make every effort to engage the patient’stive participation in prescribed medical regimens and life-yles.If these guidelines are used as the basis for regulatory oryer decisions, the goal should be improvement in quality ofre and aligned with the patient’s best interest. The ultimatedgment regarding care of a particular patient must be madethe healthcare provider and the patient in light of all of the
rcumstances presented by that patient. Consequently, theree circumstances in which deviations from these guidelinese appropriate.The guidelines will be reviewed annually by the ACCF/
HA Task Force on Practice Guidelines and consideredrrent unless they are updated, revised, or withdrawn fromstribution.
Alice K. Jacobs, MD, FACC, FAHAChair, ACCF/AHA Task Force on Practice Guidelines
Sidney C. Smith, Jr, MD, FACC, FAHAImmediate Past Chair, ACCF/AHA Task Force on
Practice Guidelines
. Introduction
.1. Methodology and Evidence Reviewhe writing committee conducted a comprehensive search ofe medical and scientific literature through the use of-bMed/MEDLINE. Searches were limited to publications
ritten in the English language. Compiled reports were
viewed and additional articles were provided by committee
mthspaoaodiangiinsyaoanaodiaoenbaPrwmwonfo
cuasclabsiwrestevdespfobaraperaenhiclspthLscevthtrtr
warth(Nodde
wth
foclthfaforeizwprmtifi
hithacwofco
1TexnuguorthsumspcawprwAicat(SveSolaPh(AWoftaCananR
1TnaAor
e32 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
embers. Specifically targeted searches were conducted one following subtopics: acute aortic dissection, ankylosingondylitis, aortic dissection and litigation, aortic neoplasm,rtic tumors, Behçet disease, bicuspid aortic valve, calcifiedrta, chronic dissection, coarctation of the aorta, D-dimer,ssecting aneurysm, Ehlers-Danlos syndrome, endovasculard aortic aneurysms, medial degeneration, porcelain aorta,ant cell arteritis, imaging and thoracic aortic disease,flammatory disease, intramural hematoma, Loeys-Dietzndrome, Marfan syndrome, Noonan syndrome, penetratingrtic ulcer, polycystic kidney disease, thoracic and aorticeurysms, thoracic aortic disease and patient care, thoracicrtic disease and surgery, thoracic aorta and Kawasakisease, Takayasu arteritis, thoracoabdominal and aorta orrtic disease, and Turner syndrome. More than 850 refer-ces were reviewed, with 829 used as the primary evidencese for the final guideline. The ACCF/AHA Task Force onactice Guidelines methodology processes were followed torite the text and recommendations. In general, publishedanuscripts appearing in journals listed in Index Medicusere used as the evidence base. Published abstracts were usedly for emerging information but were not used in thermulation of recommendations.The committee reviewed and ranked evidence supportingrrent recommendations with the weight of evidence rankedLevel A if the data were derived from multiple randomized
inical trials or meta-analyses. The committee ranked avail-le evidence as Level B when data were derived from a
ngle randomized trial or nonrandomized studies. Evidenceas ranked as Level C when the primary source of thecommendation was consensus opinion, case studies, orandard of care. In the narrative portions of these guidelines,idence is generally presented in chronological order ofvelopment. Studies are identified as observational, retro-ective, prospective, or randomized. For certain conditionsr which inadequate data are available, recommendations aresed on expert consensus and clinical experience and arenked as Level C. An analogous example is the use ofnicillin for pneumococcal pneumonia, where there are nondomized trials and treatment is based on clinical experi-ce. When recommendations at Level C are supported bystorical clinical data, appropriate references (includinginical reviews) are cited if available. For issues wherearse data are available, a survey of current practice amonge clinicians on the writing committee formed the basis forevel C recommendations and no references are cited. Thehema for classification of recommendations and level ofidence is summarized in Table 1, which also illustrates howe grading system provides an estimate of the size of theeatment effect and an estimate of the certainty of theeatment effect.To provide clinicians with a comprehensive set of data,
henever possible, the exact event rates in various treatmentms of clinical trials are presented to permit calculation ofe absolute risk difference (ARD), number needed to harmNH); the relative treatment effects are described either asds ratio (OR), relative risk (RR), or hazard ratio (HR)
pending on the format in the original publication. Along SCith all other point statistics, confidence intervals (CIs) forose statistics are added when available.The writing committee recognized that the evidence baser this guideline is less robust in terms of randomizedinical trials than prior ACCF/AHA guidelines, particularlyose focused on coronary artery disease (CAD) and heartilure. As the reader will discern, much of the evidence baser this topic consists of cohort studies and retrospectiveviews, which largely emanate from centers with a special-ed interest in specific types of thoracic aortic disease. Theriting committee attempted to focus on providing theactitioner with recommendations for evaluation and treat-ent wherever possible and where controversy exists, iden-ed as such in the text.The writing committee acknowledges the expertise of theghly experienced and effective practice guidelines staff ofe ACCF and AHA. The writing committee chair alsoknowledges the commitment and dedication of the diverseriting committee members who were able to put aside issues
specialty “turf” and focus on providing the medicalmmunity with a guideline aimed at optimal patient care.
.2. Organization of the Writing Committeehe guideline was written by a committee comprised ofperts in cardiovascular medicine, surgery, radiology, andrsing. For many of the previous ACCF/AHA practiceidelines, writing expertise has been available within these 2ganizations. Because of the broad scope and diversity oforacic aortic diseases, as well as the specialists who treatch patients, the ACCF and AHA sought greater involve-ent from many specialty organizations. Most, but not all,ecialty organizations that represent the major stakeholdersring for patients with thoracic aortic diseases providedriting committee members and financial support of theoject, and they are recognized as marquee level partnersith the ACCF and AHA. These organizations included themerican Association for Thoracic Surgery (AATS), Amer-an College of Radiology (ACR), American Stroke Associ-ion (ASA), Society of Cardiovascular AnesthesiologistsCA), Society for Cardiovascular Angiography and Inter-ntions (SCAI), Society of Interventional Radiology (SIR),ciety of Thoracic Surgeons (STS), and Society for Vascu-
r Medicine (SVM). The American College of Emergencyysicians (ACEP) and the American College of PhysiciansCP) were also represented on the writing committee.here additional expertise was needed, the scientific councilsthe AHA were contacted for writing committee represen-
tives. Representation was provided or facilitated by theouncils on Cardiovascular Nursing, Cardiovascular Surgeryd Anesthesia, Cardiovascular Radiology and Intervention,d Clinical Cardiology, Council for High Blood Pressure
esearch, and Stroke Council.
.3. Document Review and Approvalhis document was reviewed by 3 outside reviewers nomi-ted by the ACCF and 2 outside reviewers nominated by theHA, as well as 1 or 2 reviewers from each of the followingganizations: the AATS, ACP, ACEP, ACR, ASA, SCA,
AI, SIR, STS, and the SVM. It was also reviewed by 6
inAthman
erAenIm
1TofmC
datonuuntioditwaoAdicaem
alaf
Ta
mMbe
rethinc individ
e33JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
dividual content reviewers—2 content reviewers from theCCF Catherization Committee and 1 content reviewer frome ACCF Interventional Council. All reviewer RWI infor-ation was collected and distributed to the writing committeed is published in this document (see Appendix 2).This document was approved for publication by the gov-ning bodies of the ACCF and the AHA and the AATS,CR, ASA, SCA, SCAI, SIR, STS, and SVM and wasdorsed by the North American Society for Cardiovascularaging.
.4. Scope of the Guidelinehe term “thoracic aortic disease” encompasses a broad rangedegenerative, structural, acquired, genetic-based, and trau-
atic disease states and presentations. According to the
ble 1. Applying Classification of Recommendations and Level
*Data available from clinical trials or registries about the usefulness/efficacyyocardial infarction, history of heart failure, and prior aspirin use. A recommendany important clinical questions addressed in the guidelines do not lend them
a very clear clinical consensus that a particular test or therapy is useful or†In 2003, the ACCF/AHA Task Force on Practice Guidelines developed a
commendations have been written in full sentences that express a completee rest of the document (including headings above sets of recommendations),rease readers’ comprehension of the guidelines and will allow queries at the
enters for Disease Control and Prevention death certificate ag
ta, diseases of the aorta and its branches account for 43 00047 000 deaths annually in the United States (2). The precisember of deaths attributable to thoracic aortic diseases isclear. However, autopsy studies suggest that the presenta-n of thoracic aortic disease is often death due to aortic
ssection (AoD) and rupture, and these deaths account forice as many deaths as attributed to ruptured abdominalrtic aneurysms (AAAs) (3). The diagnosis of acute thoracicoD or rupture is often difficult and delayed, and errors inagnosis may account for deaths otherwise attributed tordiac arrhythmia, myocardial infarction (MI), pulmonarybolism, or mesenteric ischemia.The University HealthSystem Consortium (UHC) is an
liance of more than 100 academic medical centers andfiliate hospitals. UHC’s Clinical DataBase/Resource Man-
ence
rent subpopulations, such as sex, age, history of diabetes, history of priorth Level of Evidence B or C does not imply that the recommendation is weak.o clinical trials. Even though randomized trials are not available, there may.suggested phrases to use when writing recommendations. All guideline, such that a recommendation, even if separated and presented apart fromstill convey the full intent of the recommendation. It is hoped that this willual recommendation level.
of Evid
in diffeation wiselves teffectivelist of
thoughtwould
er allows comparison of patient-level risk-adjusted out-

cowbahoagnuthao20rupe20wA
Stthtiowin
beevmhemwdiprunouao
addidiredapr
Ta
AoCa
Th
Ab
Th
Ao
TaUH
AoCa
Th
rup
Ab
rup
Th
rup
Ao
rup
Toca
Toinpdis
e34 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
mes for performance improvement. The UHC provided theriting committee with a summary of recent informationsed on ICD-9 codes for thoracic aortic disease–relatedspitalizations from the Clinical DataBase/Resource Man-er (Tables 2A and 2B). This data table demonstrates a highmber of hospital discharges (more than 135 000) fororacic, abdominal, thoracoabdominal, and “unspecified”rtic aneurysms in the 5-year period between 2002 and07. Subcategories include those with dissection, those withpture, and those with neither. In the most recent 1-yearriod assessed (fourth quarter 2006 through third quarter07), there were nearly 9000 cases representing all patients
ith thoracic aortic disease discharged from UHC hospitals.lthough these data are unavailable for the entire United
ble 2A. ICD-9 Procedure Codes For Aortic Aneurysms
rtic Aneurysmtegory Dissection Ruptured
No Mention ofRupture
oracic 441.01 441.1 441.2
dominal 441.02 441.3 441.4
oracoabdominal 441.03 441.6 441.7
rtic (unspecified) 441.00 441.5 441.9
Table courtesy of UHC Clinical DataBase/Resource Manager.
ble 2B. Number of Discharges by Year by Category of Aortic AC Clinical Database*
rtic Aneurysmtegory 2002q4–2003q3 2003q4–2004q3 2004q4–2005q3
oracic
Dissection 1607 1683 2028
Ruptured 187 225 219
No mention ofture
3086 4026 4953
Subtotal 4880 5934 7200
dominal
Dissection 553 630 747
Ruptured 651 657 720
No mention ofture
12 075 13 280 15 882
Subtotal 13 279 14 567 17 349
oracoabdominal
Dissection 583 587 674
Ruptured 150 129 110
No mention ofture
1091 1183 1472
Subtotal 1824 1899 2256
rtic (unspecified)
Dissection 223 310 326
Ruptured 9 3 15
No mention ofture
310 385 505
Subtotal 542 698 846
tal No. ofses
20 525 23 098 27 651
tal No. ofatientcharges
2679334 2777880 3018141
UHC indicates University HealthSystem Consortium.*Note: Year-to-year increases are due in part to changes in number of report
Table courtesy of UHC Clinical DataBase/Resource Manager.
ates, they provide important estimates of the magnitude ofe prevalence of thoracic aortic disease. Additional informa-n regarding the patient admission source, particularly those
ith acute presentations, is pertinent to the discussion regard-g interinstitutional transfer (see Section 17.2).Most patients with significant thoracic aortic disease willdirected to specialized practitioners and institutions. How-
er, the importance of early recognition and prompt treat-ent and/or referral for various thoracic aortic diseases by allalthcare professionals provides the rationale for this docu-ent. This guideline will attempt to provide the practitionerith a sufficient description of background information,agnostic modalities, and treatment strategies so that appro-iate care of these patients can be facilitated and betterderstood. The goal of this guideline is to improve the healthtcomes and quality of life for all patients with thoracicrtic disease.Other practice guidelines developed by ACCF and AHAdress the management of patients with cardiac and vascularseases. The ACCF/AHA guidelines on peripheral arterialsease (4) include recommendations for lower extremity,nal, mesenteric, and abdominal aortic diseases. Data stan-rds on this topic are currently in development, as is aactice guideline on extracranial carotid and vertebral artery
sm Among Academic Medical Centers Reporting Data to the
4–2006q3 2006q4–2007q35-YearTotal
Category %Distribution
% of AllCategories
25.9
1 2355 9994 28.5
4 251 1116 3.2
0 6156 23 954 68.3
5 8762 35 064
62.7
867 3664 4.3
702 3464 4.1
818 18 683 77 738 91.6
419 20 252 84 866
8.3
834 3433 30.5
127 673 6.0
1773 7140 63.5
2734 11 246
3.0
339 1541 37.6
9 45 1.1
701 2513 61.3
1049 4099
201 32 797 135 275
222542 3297834 14995731
itals.
neury
2005q
232
23
573
828
867
734
17
19
755
157
1621
2533
343
9
612
964
31
3
ing hosp

diJotioA
ofdiouarreA
mwenbeindidoanmvimtoca
1.Acr
•
•
•
•
•
•
•
1U
A
P
E
A
e35JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
seases. The ACCF/AHA guidelines are published in theurnal of the American College of Cardiology and Circula-n and are available on both the ACC (www.acc.org) and
HA (my.americanheart.org) Web sites.This guideline includes diseases involving any or all partsthe thoracic aorta with the exception of aortic valve
seases (5) and includes the abdominal aorta when contigu-s thoracic aortic diseases are present. Specific disease statese described in the following sections, and the reader isferred to the glossary of terminology in Section 1.5 andppendix 3 for abbreviations used throughout the guideline.The reader will note that several topics or referenced areasay appear more than once throughout the guideline. Thisill appear to be redundant to those who choose to read thetire document, but the writing committee believed thatcause of the multidisciplinary nature of and organizationalvolvement in this project, individuals representing specificsciplines may choose to read and extract portions of thecument for their own use. Inclusion of the narrative textd references was thought to be appropriate to facilitate aore complete understanding for these disciplines and indi-duals. Accordingly, the organization of the guideline iseant to be less of a textbook presentation of the variouspics but rather a more clinically oriented document appli-ble to a variety of disciplines.
4.1. Critical Issuess the writing committee developed this guideline, severalitical issues emerged:
Thoracic aortic diseases are usually asymptomatic and noteasily detectable until an acute and often catastrophiccomplication occurs. Imaging of the thoracic aorta withcomputed tomographic imaging (CT), magnetic resonanceimaging (MR), or in some cases, echocardiographic exam-ination is the only method to detect thoracic aortic diseasesand determine risk for future complications (see Section 4).Radiologic imaging technologies have improved in termsof accuracy of detection of thoracic aortic disease. How-ever, as the use of these technologies has increased, so alsohas the potential risk associated with repeated radiationexposure, as well as contrast medium–related toxicity.Whether these technologies should be used repeatedly as awidespread screening tool is discussed in Section 4. Inaddition, the writing committee formulated recommenda-tions on a standard reporting format for thoracic aorticfindings as discussed in Section 4.5.Imaging for asymptomatic patients at high risk based onhistory or associated diseases is expensive and not alwayscovered by payers.For many thoracic aortic diseases, results of treatment forstable, often asymptomatic, but high-risk conditions are farbetter than the results of treatment required for acute andoften catastrophic disease presentations. Thus, the identi-fication and treatment of patients at risk for acute andcatastrophic disease presentations (e.g., thoracic AoD,thoracic aneurysm rupture) prior to such an occurrence areparamount to eliminating the high morbidity and mortality
associated with acute presentations (see Section 8.1).A subset of patients with acute AoD are subject to missedor delayed detection of this catastrophic disease state.Many present with atypical symptoms and findings, mak-ing diagnosis even more difficult (see Sections 8.1.4 and8.6). This issue has come under greater medical-legalscrutiny, and specific cases have been widely discussed inthe public domain. Widespread awareness of the variedand complex nature of thoracic aortic disease presentationshas been lacking, especially for acute AoD. Risk factorsand clinical presentation clues are noted in Section 8.1.4.The collaboration and cosponsorship of multiple medicalspecialties in the writing of this guideline will provideunique opportunities for widespread dissemination ofknowledge to raise the level of awareness among allmedical specialties.There is rapidly accumulating evidence that genetic alter-ations or mutations predispose some individuals to aorticdiseases (see Section 5). Therefore, identification of thegenetic alterations leading to these aortic diseases has thepotential for early identification of individuals at risk. Inaddition, biochemical abnormalities involved in the pro-gression of aortic disease are being identified throughstudies of patients’ aortic samples and animal models ofthe disease (6,7). The biochemical alterations identified inthe aortic tissue have the potential to serve as biomarkersfor aortic disease. Understanding the molecular pathogen-esis may lead to targeted therapy to prevent aortic disease.Medical and gene-based treatments are beginning to showpromise for reducing or delaying catastrophic complica-tions of thoracic aortic diseases (see Section 9.2).As noted in Section 18, there are several areas wheregreater resources for research and both short- and long-term outcomes registries are needed.
.5. Glossary of Terms and Abbreviationssed Throughout Guideline
neurysm (or true aneurysm): a permanent localized dila-tation of an artery, having at least a 50% increase indiameter compared with the expected normal diameter ofthe artery in question. Although all 3 layers (intima,media, and adventitia) may be present, the intima andmedia in large aneurysms may be so attenuated that insome sections of the wall they are undetectable.
seudoaneurysm (or false aneurysm): contains blood re-sulting from disruption of the arterial wall with extrava-sation of blood contained by periarterial connective tissueand not by the arterial wall layers (see Section 8.4). Suchan extravascular hematoma that freely communicates withthe intravascular space is also known as a pulsatinghematoma (8–10).
ctasia: arterial dilatation less than 150% of normal arterialdiameter.
rteriomegaly: diffuse arterial dilatation involving severalarterial segments with an increase in diameter greaterthan 50% by comparison to the expected normal arterial
diameter.
T
A
A
2
2T(wcu(wbebratthtodeorarth
la
In
M
A
2In(Tao
dipamimdimyefoinm
siw
Ta
T
Ro
Ro
As(fe
M(fe
M(m
Di(fe
Di(m
e36 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
horacoabdominal aneurysm (TAA): aneurysm involvingthe thoracic and abdominal aorta (see Section 9.2.2.3).
bdominal aortic aneurysm (AAA): aneurysm involvingthe infradiaphragmatic abdominal aorta.
ortic dissection (AoD): disruption of the media layer of theaorta with bleeding within and along the wall of the aorta.Dissection may, and often does, occur without an aneu-rysm being present. An aneurysm may, and often does,occur without dissection. The term “dissecting aorticaneurysm” is often used incorrectly and should be re-served only for those cases where a dissection occurs in ananeurysmal aorta (see Section 8.1).
. The Thoracic Aorta
.1. The Normal Aortahe thoracic aorta is divided into 4 parts: the aortic roothich includes the aortic valve annulus, the aortic valvesps, and the sinuses of Valsalva); the ascending aortahich includes the tubular portion of the ascending aortaginning at the sinotubular junction and extending to theachiocephalic artery origin); the aortic arch (which beginsthe origin of the brachiocephalic artery and is the origin ofe head and neck arteries, coursing in front of the trachea and
the left of the esophagus and the trachea); and thescending aorta (which begins at the isthmus between theigin of the left subclavian artery and the ligamentumteriosum and courses anterior to the vertebral column, anden through the diaphragm into the abdomen).The normal human adult aortic wall is composed of 3
yers, listed from the blood flow surface outward (Figure 1):
tima: endothelial layer on a basement membrane withminimal ground substance and connective tissue.
edia: bounded by an internal elastic lamina, a fenestratedsheet of elastic fibers; layers of elastic fibers arrangedconcentrically with interposed smooth muscle cells;bounded by an external elastic lamina, another fenestrated
sheet of elastic fibers. apdventitia: resilient layer of collagen containing the vasavasorum and nerves. Some of the vasa vasorum canpenetrate into the outer third of the media.
.2. Normal Thoracic Aortic Diameter1991, the Society for Vascular Surgery created a table
able 3) describing the normal diameter of the adult thoracicrta based on CT and chest x-ray (12).Since then, it has been recognized that the “normal aorticameter” is influenced by a number of factors, includingtient age, sex, and body size; location of aortic measure-ent; method of measurement; and the robustness and type ofaging methods used. Hannuksela et al (13) noted that
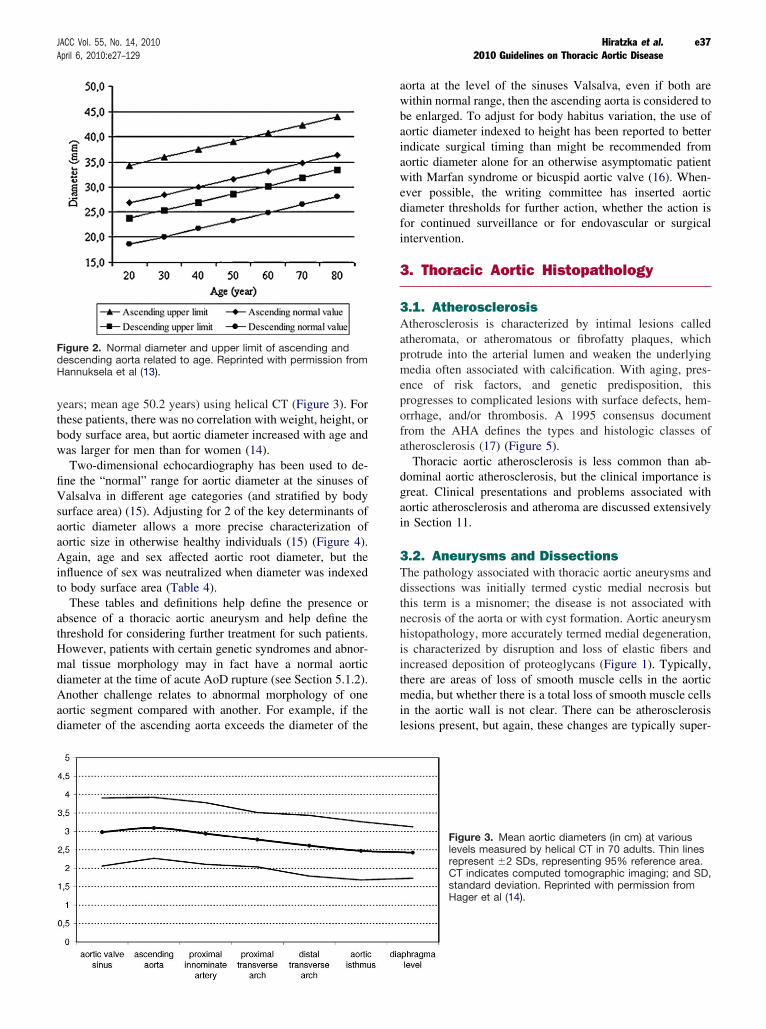
ameter increased by 0.12 to 0.29 mm/y at each leveleasured by CT for 41 men and 36 women aged 18 to 82ars (Figure 2). Aortic diameter for men was larger than thatr women, but the difference decreased with age. Body massdex also affected aortic diameter by 0.27 mm (0.14 to 0.44m) per unit of body mass index (13).Aortic diameter gradually tapers downstream from the
nuses of Valsalva. Hager et al (14) examined 46 men and 24omen without cardiovascular disease (age range 1 to 89
ble 3. Normal Adult Thoracic Aortic Diameters
horacic AortaRange of Reported
Mean (cm)Reported SD
(cm)Assessment
Method
ot (female) 3.50 to 3.72 0.38 CT
ot (male) 3.63 to 3.91 0.38 CT
cendingmale, male)
2.86 NA CXR
id-descendingmale)
2.45 to 2.64 0.31 CT
id-descendingale)
2.39 to 2.98 0.31 CT
aphragmaticmale)
2.40 to 2.44 0.32 CT
aphragmaticale)
2.43 to 2.69 0.27 to 0.40 CT, arteriography
CT indicates computed tomographic imaging; CXR, chest x-ray; and NA, not
Figure 1. Aortic pathology associated with thoracicaortic aneurysm involving the ascending aorta. Allpanels are identically oriented with the adventitia atthe top and the intima at the bottom. H&E staining ofaortic sections from a control (a) and a patient (b) witha TAA demonstrates medial degeneration with thefragmentation of elastic fibers, accumulation of pro-teoglycans, and regions of smooth muscle cell loss.Movat staining of aortic sections from control (c) andpatient with an aneurysm (d) shows fragmentation ofelastic fibers (stained black), loss of smooth musclecells (cells stained red and nuclei stained violet), andaccumulation of proteoglycans (stained blue) in themedial layer. 40� magnification; scale bars represent500 mcg. H&E indicates hematoxylin and eosin; andTAA, thoracic aortic aneurysm. Modified fromMilewicz et al (11).
plicable. Reprinted with permission from Johnston et al (12).
yethbow
finVsuaoaoAinto
abthHmdiAaodi
aowbeaoinaowevdifoin
3
3Aatprmenprorfrat
dograoin
3Tdithnehiisinthminle
FideH
e37JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
ars; mean age 50.2 years) using helical CT (Figure 3). Forese patients, there was no correlation with weight, height, ordy surface area, but aortic diameter increased with age and
as larger for men than for women (14).Two-dimensional echocardiography has been used to de-e the “normal” range for aortic diameter at the sinuses of
alsalva in different age categories (and stratified by bodyrface area) (15). Adjusting for 2 of the key determinants ofrtic diameter allows a more precise characterization ofrtic size in otherwise healthy individuals (15) (Figure 4).gain, age and sex affected aortic root diameter, but thefluence of sex was neutralized when diameter was indexedbody surface area (Table 4).These tables and definitions help define the presence orsence of a thoracic aortic aneurysm and help define thereshold for considering further treatment for such patients.owever, patients with certain genetic syndromes and abnor-al tissue morphology may in fact have a normal aorticameter at the time of acute AoD rupture (see Section 5.1.2).nother challenge relates to abnormal morphology of onertic segment compared with another. For example, if theameter of the ascending aorta exceeds the diameter of the
gure 2. Normal diameter and upper limit of ascending andscending aorta related to age. Reprinted with permission from
annuksela et al (13).
rta at the level of the sinuses Valsalva, even if both areithin normal range, then the ascending aorta is considered to
enlarged. To adjust for body habitus variation, the use ofrtic diameter indexed to height has been reported to betterdicate surgical timing than might be recommended fromrtic diameter alone for an otherwise asymptomatic patientith Marfan syndrome or bicuspid aortic valve (16). When-er possible, the writing committee has inserted aorticameter thresholds for further action, whether the action isr continued surveillance or for endovascular or surgicaltervention.
. Thoracic Aortic Histopathology
.1. Atherosclerosistherosclerosis is characterized by intimal lesions calledheromata, or atheromatous or fibrofatty plaques, whichotrude into the arterial lumen and weaken the underlyingedia often associated with calcification. With aging, pres-ce of risk factors, and genetic predisposition, thisogresses to complicated lesions with surface defects, hem-rhage, and/or thrombosis. A 1995 consensus documentom the AHA defines the types and histologic classes ofherosclerosis (17) (Figure 5).Thoracic aortic atherosclerosis is less common than ab-minal aortic atherosclerosis, but the clinical importance iseat. Clinical presentations and problems associated withrtic atherosclerosis and atheroma are discussed extensivelySection 11.
.2. Aneurysms and Dissectionshe pathology associated with thoracic aortic aneurysms andssections was initially termed cystic medial necrosis butis term is a misnomer; the disease is not associated withcrosis of the aorta or with cyst formation. Aortic aneurysmstopathology, more accurately termed medial degeneration,characterized by disruption and loss of elastic fibers and
creased deposition of proteoglycans (Figure 1). Typically,ere are areas of loss of smooth muscle cells in the aorticedia, but whether there is a total loss of smooth muscle cellsthe aortic wall is not clear. There can be atherosclerosis
sions present, but again, these changes are typically super-
Figure 3. Mean aortic diameters (in cm) at variouslevels measured by helical CT in 70 adults. Thin linesrepresent �2 SDs, representing 95% reference area.CT indicates computed tomographic imaging; and SD,standard deviation. Reprinted with permission fromHager et al (14).

imdedito
mHstinMmstasofelinpa(2paarofdesyAm
anla
vaofaomryin(2waclehympafowpaman
3Ath
Ta
Ao
An
Si
Si
Pr
e38 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
posed on medial degenerative disease. Although medialgeneration was initially described as a noninflammatorysease, recent literature supports the presence of inflamma-ry cell infiltration in this disease (18,19).The biochemical pathways and proteins involved withedial degeneration have not been clearly delineated.owever, multiple studies have found increased immuno-aining for a subset of matrix metalloproteinases (MMPs)
the media of thoracic aortic aneurysms, particularlyMP-2 and MMP-9 (20 –23). Immunostaining of aorticedia from patients with Marfan syndrome has demon-rated increases in MMP-2 and MMP-9, which weresociated with smooth muscle cells at the borders of areasmedial degeneration and on the surface of disrupted
astic fibers. Elevated MMP-2 and MMP-9 immunostain-g has been demonstrated in ascending aneurysms fromtients with either tricuspid or bicuspid aortic valves1,23) and inconsistently in ascending aortic tissue fromtients with tricuspid aortic valves (22). These 2 MMPse known to have elastolytic activity. Variable expression
MMPs and tissue inhibitors of MMPs has also beenmonstrated in aortic tissue of patients with Marfanndrome versus patients without Marfan syndrome (24).lthough accumulation of proteoglycans in the aorticedia is another consistent finding in thoracic aortic
ble 4. Sex Differences in Aortic Root Dimensions in Adults
rtic RootAbsolute Values
(cm) Men P Value
nulus 2.6�0.3 �0.001
nuses of Valsalva 3.4�0.3 �0.001
notubular junction 2.9�0.3 �0.001
oximal ascending aorta 3.0�0.4 �0.001
NS indicates not significant.
Adapted from Roman et al (15).eurysms, no studies have determined why this accumu-tion occurs or whether these are causative in nature.Medial degeneration is also associated with focal loss ofscular smooth muscle cells. Although there are regionssmooth muscle cell loss, morphometric analysis of
rtic tissue has suggested that hyperplastic cellular re-odeling of the media in ascending thoracic aortic aneu-sms may be an initial adaptive response to minimizecreased wall stress resulting from vascular dilatation5). More recent studies of the aortic pathology associatedith myosin heavy chain 11, smooth muscle (MYH11), andtin, alpha 2, smooth muscle aorta (ACTA2) mutationsading to ascending aortic aneurysms demonstrate aperplastic response by smooth muscle cells in the aorticedia. The aortic media in aneurysm tissue taken fromtients harboring mutations in these genes demonstratedcal hyperplasia associated with smooth muscle cells thatere remarkable for a lack of structured orientationrallel to the lumen of the aorta, but instead, the smoothuscle cells were oriented randomly with respect to oneother (26,27).
.3. Vasculitis and Inflammatory Diseasesvariety of inflammatory vasculitides may also result in
oracic aortic disease. These include giant cell arteritis
Figure 4. Sinus of Valsalva diameter, bybody surface area. Left, The 95% normalconfidence limits for aortic root diameter atthe sinuses of Valsalva in relation to bodysurface area in adults �40 years of age.Right, The 95% normal confidence limits forthe proximal ascending aortic diameter in re-lation to body surface area in adults �40years of age. SEE indicates standard error ofthe estimate. Reprinted with permission fromRoman et al (15).
menIndexed
Values (cm/m2) Men P Value Women
0.2 1.3�0.1 NS 1.3�0.1
0.3 1.7�0.2 NS 1.8�0.2
0.3 1.5�0.2 NS 1.5�0.2
0.4 1.5�0.2 NS 1.6�0.3
Wo
2.3�
3.0�
2.6�
2.7�

(G7)wgembecytiindial
4
4TePCL
1.
2.
3.
4.
5.
6.
Ta
1.
2.
3.
4.
5.
6.
7.
8.
e39JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
CA), Takayasu arteritis, and Behçet disease (see Section. The pathophysiology of GCA shares important featuresith Takayasu arteritis (28). T-cell clonal expansion sug-sts a specific antigenic response, which currently re-ains unelucidated. The inflammatory response, whichgins in the adventitial layer, is marked by augmentedtokine and MMP production causing granuloma forma-
on. Granuloma formation both shields the vessel from theciting antigen and causes vessel destruction (29). Behçetsease is a vasculitis affecting both arteries and veins, ofl sizes.
. Imaging Modalities
.1. Recommendations for Aortic Imagingchniques to Determine the Presence and
rogression of Thoracic Aortic DiseaseASS I
Measurements of aortic diameter should be taken at reproduc-ible anatomic landmarks, perpendicular to the axis of bloodflow, and reported in a clear and consistent format (see Table5). (Level of Evidence: C)For measurements taken by computed tomographic imagingor magnetic resonance imaging, the external diametershould be measured perpendicular to the axis of blood flow.For aortic root measurements, the widest diameter, typi-cally at the mid-sinus level, should be used. (Level ofEvidence: C)For measurements taken by echocardiography, the internal diam-eter should be measured perpendicular to the axis of blood flow.For aortic root measurements, the widest diameter, typically at
the mid-sinus level, should be used. (Level of Evidence: C) ulcAbnormalities of aortic morphology should be recognized andreported separately even when aortic diameters are withinnormal limits. (Level of Evidence: C)The finding of aortic dissection, aneurysm, traumatic injuryand/or aortic rupture should be immediately communicated tothe referring physician. (Level of Evidence: C)Techniques to minimize episodic and cumulative radiationexposure should be utilized whenever possible. (30,31) (Levelof Evidence: B)
Figure 5. Atherosclerotic lesions. Flow dia-gram in center column indicates pathways inevolution and progression of human athero-sclerotic lesions. Roman numerals indicatehistologically characteristic types of lesionsdefined at the left of the flow diagram. Thedirection of the arrows indicates the se-quence in which characteristic morphologiesmay change. From Type I to Type IV,changes in lesion morphology occur primarilybecause of increasing accumulation of lipid.The loop between Types V and VI illustrateshow lesions increase in thickness whenthrombotic deposits form on their surfaces.Thrombotic deposits may form repeatedlyover varied time spans in the same locationand may be the principal mechanism forgradual occlusion of medium-sized arteries.Adapted from Stary et al (17).
ble 5. Essential Elements of Aortic Imaging Reports
The location at which the aorta is abnormal (see Section 2).
The maximum diameter of any dilatation, measured from the externalwall of the aorta, perpendicular to the axis of flow, and the length of theaorta that is abnormal.
For patients with presumed or documented genetic syndromes at risk foraortic root disease measurements of aortic valve, sinuses of Valsalva,sinotubular junction, and ascending aorta.
The presence of internal filling defects consistent with thrombus oratheroma.
The presence of IMH, PAU, and calcification.
Extension of aortic abnormality into branch vessels, including dissectionand aneurysm, and secondary evidence of end-organ injury (e.g., renalor bowel hypoperfusion).
Evidence of aortic rupture, including periaortic and mediastinalhematoma, pericardial and pleural fluid, and contrast extravasation fromthe aortic lumen.
When a prior examination is available, direct image to image comparisonto determine if there has been any increase in diameter.
IMH indicates intramural hematoma; and PAU, penetrating atherosclerotic
er.
CL
1.
Deaimmstcamexboththpoagfib
rinaagmremlo
thcapeopprof
fobeaoinsucemaoecetananinSttowminof
4RaoC
woffinx-prthstasni(3ragelikinwtivAso21aoog
scshusmloanththnoon
4Cid
Ficaao
e40 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ASS IIa
If clinical information is available, it can be useful to relateaortic diameter to the patient’s age and body size. (Level ofEvidence: C)
efinitive identification or exclusion of thoracic aortic dis-se or one of its anatomic variants requires dedicated aorticaging. Selection of the most appropriate imaging study
ay depend on patient-related factors (i.e., hemodynamicability, renal function, contrast allergy) and institutionalpabilities (i.e., rapid availability of individual imagingodalities, state of the technology, and imaging specialistpertise). Consideration should be given to patients withrderline abnormal renal function (serum creatinine greateran 1.8 to 2.0 mg/dL)—specifically, the tradeoffs betweene use of iodinated intravenous contrast for CT and thessibility of contrast-induced nephropathy, and gadoliniuments used with MR and the risk of nephrogenic systemicrosis (32).Radiation exposure should be minimized (31,33–36). The
sk of radiation-induced malignancy is the greatest in neo-tes, children, and young adults (31). Generally, above thee of 30 to 35 years, the probability of radiation-inducedalignancy decreases substantially (30,31). For patients whoquire repeated imaging to follow an aortic abnormality, MRay be preferred to CT. MR may require sedation due tonger examination times and tendency for claustrophobia.CT as opposed to echocardiography can best identifyoracic aortic disease, as well as other disease processes thatn mimic aortic disease, including pulmonary embolism,ricardial disease, and hiatal hernia. After intervention oren surgery, CT is preferred to detect asymptomatic post-ocedural leaks or pseudoaneurysms because of the presencemetallic closure devices and clips.We recommend that external aortic diameter be reportedr CT or MR derived size measurements. This is importantcause lumen size may not accurately reflect the externalrtic diameter in the setting of intraluminal clot, aortic wallflammation, or AoD. A recent refinement in the CT mea-rement of aortic size examines the vessel size using anterline of flow, which reduces the error of tangentialeasurement and allows true short-axis measurement ofrtic diameter. In contrast to tomographic methods,hocardiography-derived sizes are reported as internal diam-er size. In the ascending aorta, where mural thrombus ineurysms is unusual, the discrepancy between the internald external aortic diameters is less than it is in the descend-g or abdominal aorta, where mural thrombus is common.andardization of aortic diameter measurements is importantthe planning of endovascular treatment of an aneurysm,
here the diameter of the aorta in the seal zone must beatched to the diameter of an endograft. Here, the choice ofternal or external diameter is specified by the manufacturerthe endograft.
.2. Chest X-Rayoutine chest x-ray may occasionally detect abnormalities ofrtic contour or size that require definitive aortic imaging.
hest x-ray often serves as a part of the evaluation of patients th
ith potential acute AoD, primarily to identify other causespatient’s symptoms, but also as a screening test to identifydings due to a dilated aorta or bleeding. However, chestray is inadequately sensitive to definitively exclude theesence of AoD in all except the lowest-risk patients anderefore rarely excludes the disease. Pooled data from 10udies places the predictive sensitivity of a widened medi-tinum or an abnormal aortic contour associated with sig-ficant thoracic aortic disease at 64% and 71%, respectively7). In the same analysis, however, including all abnormaldiographic findings increased the sensitivity to 90%, sug-sting that a completely normal chest x-ray does lower theelihood of AoD and may provide meaningful clinical
formation in very low-risk patients (37). The presence of aidened mediastinum or other radiographic findings sugges-e of thoracic aortic disease increases the likelihood of
oD, particularly among patients who lack a clear alternativeurce for their symptoms. In a blinded prospective study of6 patients who underwent evaluation for acute thoracicrtic disease, the specificity of chest x-ray for aortic pathol-y was 86% (38).For patients with chest trauma, chest x-ray is a poorreening test for the diagnosis of aortic injury (39–41). Aarply demarcated normal mediastinal contour is sometimesed to exclude mediastinal hematoma (suggesting a wideediastinum, abnormal mediastinal contour, left apical cap,ss of the aortic knob, depression of the left main bronchus,d deviation of an indwelling esophageal tube). However,ese signs of hemomediastinum are more often false positivean true positive for aortic injury (40). Figure 6 illustrates thermal appearance of the thoracic aorta, and its components,a posteroanterior chest x-ray.
.3. Computed Tomographic ImagingT scanning has been used for more than 2 decades toentify acute AoD and to diagnose and measure other
gure 6. Chest x-ray of a normal thoracic aorta. Arrows indi-te arch, and arrowheads show ascending and descendingrta.
oracic aortic diseases (42) (see Section 5.1). Advantages
inenidan(iulcoEpocoin
sc98Aaoity(Tusfir
adw
acdecodianthininnetose
raaoTprfo(F
enao
Fitratetodeasto
Ficrpsnusiimaoto
e41JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
clude near universal availability—the ability to image thetire aorta, including lumen, wall, and periaortic regions; toentify anatomic variants and branch vessel involvement;d to distinguish among types of acute aortic syndromes
.e., intramural hematoma [IMH], penetrating atheroscleroticcer [PAU], and acute AoD)—and the short time required tomplete the imaging process and the 3-dimensional data.
lectrocardiogram (ECG)-gated techniques have made itssible to generate motion-free images of the aortic root andronary arteries, similar to coronary CT angiographic imag-g.Reports of newer-generation multidetector helical CTanners show sensitivities of up to 100% and specificities of% to 99% (43–46). Data from the International Registry of
cute Aortic Dissection (IRAD) show that for patients withrtic dissection, CT was the initially used diagnostic modal-
in 61% of patients and transthoracic echocardiographyTE) and/or transesophageal echocardiography (TEE) wased first in 33% of patients. Whether this was because the
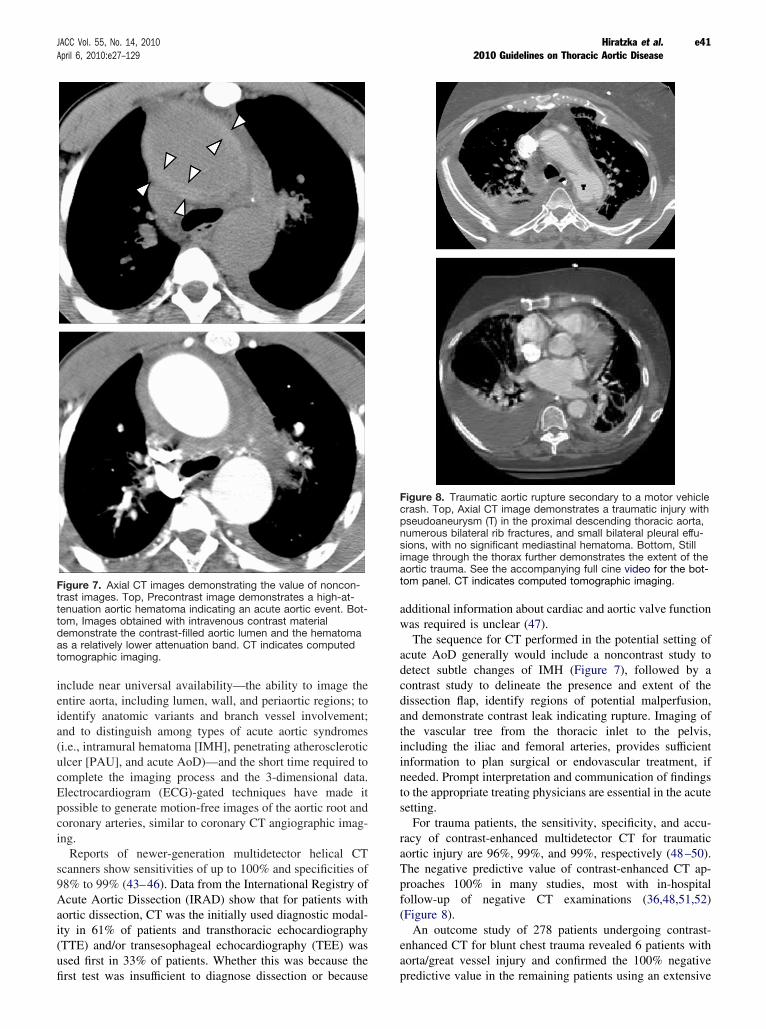
gure 7. Axial CT images demonstrating the value of noncon-st images. Top, Precontrast image demonstrates a high-at-
nuation aortic hematoma indicating an acute aortic event. Bot-m, Images obtained with intravenous contrast materialmonstrate the contrast-filled aortic lumen and the hematomaa relatively lower attenuation band. CT indicates computed
mographic imaging.
st test was insufficient to diagnose dissection or because pr
ditional information about cardiac and aortic valve functionas required is unclear (47).The sequence for CT performed in the potential setting ofute AoD generally would include a noncontrast study totect subtle changes of IMH (Figure 7), followed by antrast study to delineate the presence and extent of thessection flap, identify regions of potential malperfusion,d demonstrate contrast leak indicating rupture. Imaging ofe vascular tree from the thoracic inlet to the pelvis,cluding the iliac and femoral arteries, provides sufficientformation to plan surgical or endovascular treatment, ifeded. Prompt interpretation and communication of findingsthe appropriate treating physicians are essential in the acutetting.For trauma patients, the sensitivity, specificity, and accu-cy of contrast-enhanced multidetector CT for traumaticrtic injury are 96%, 99%, and 99%, respectively (48–50).
he negative predictive value of contrast-enhanced CT ap-oaches 100% in many studies, most with in-hospitalllow-up of negative CT examinations (36,48,51,52)igure 8).An outcome study of 278 patients undergoing contrast-hanced CT for blunt chest trauma revealed 6 patients withrta/great vessel injury and confirmed the 100% negative
gure 8. Traumatic aortic rupture secondary to a motor vehicleash. Top, Axial CT image demonstrates a traumatic injury witheudoaneurysm (T) in the proximal descending thoracic aorta,merous bilateral rib fractures, and small bilateral pleural effu-
ons, with no significant mediastinal hematoma. Bottom, Stillage through the thorax further demonstrates the extent of thertic trauma. See the accompanying full cine video for the bot-m panel. CT indicates computed tomographic imaging.
edictive value in the remaining patients using an extensive

rem
shof336coarcothno
4.Athshspminmim3-grsideaxop
tioingr14
aothoftioqucacotoimasandrtrmth
deuscoth
tioinortioknthfidnach3-
e42 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
view of medical databases with a median follow-up of 20.5onths (53).Regarding other thoracic aortic diseases, CT has beenown to have a 92% accuracy for diagnosing abnormalitiesthe thoracic aorta, in a series of examinations that includedthoracic aneurysms, 3 ruptured thoracic aortic aneurysms,
PAUs, 5 AoDs, and 2 pseudoaneurysms. In addition, CTrrectly predicted the need for hypothermic circulatoryrest during surgical repair in 94% of patients (54). Forngenital and inflammatory conditions of the thoracic aorta,e literature is primarily descriptive, and accuracy data aret available.
3.1. Computed Tomographic Imaging Techniquelthough nonhelical CT scanners are capable of diagnosingoracic aortic disease, the technique used is axial step-and-oot technology. Inherent limitations include slow scaneed, relatively poor spatial resolution given thicker colli-ation used to extend the needed craniocaudal coverage, andherently a noncontiguous dataset. Any patient motion, eveninimal, between the acquisition of each image or cluster ofages creates a stair-step artifact on multiplanar anddimensional renderings. Helical CT scanners of 4 andeater detector rows consistently provide volumetric acqui-tions of the thoracic aorta. Scanners with 16 and greatertector rows provide isotropic resolution in the x, y, and zes, which allows the datasets to be reconstructed in thetimum imaging plane best suited to any individual vessel.Technical parameters recommended for image reconstruc-n are slices of 3-mm or less thickness with a reconstruction
terval of 50% or less than the slice thickness at 50% oreater overlap, tube rotation of 1 second or less, and 120 to
0 kVp (55). ECG gating is particularly useful for ascending rortic disease, eliminating motion artifact at the aortic rootat can simulate an AoD (Figure 9), and allowing evaluationaortic valve morphology and function, as well as evalua-n of the proximal coronary arteries. If appropriately ac-ired, an aorta CT and a complete CT coronary angiogramn be obtained in 1 CT acquisition. For AoD, the scanverage should start above the aortic arch and extend at leastthe aortoiliac bifurcation, and probably the groin. This isportant to determine both branch vessel involvement, suchlesion extension into the abdominal aorta and iliac arteriesd characterization and diagnosis of malperfusion syn-ome, and to evaluate access for percutaneous repair whenansluminal therapy is being considered. (For further infor-ation on technique parameters and anatomic coverage, seee online-only Data Supplement.)The CT angiographic acquisition uses intravenous contrastlivered at rate of 3 to 5 mL/s by a power injector andually followed by a saline bolus. The total volume ofntrast used should be kept as low as possible, to no greateran 150 mL.Although axial sections remain the mainstay of interpreta-n, 2- and 3-dimensional reconstructions, such as maximum
tensity projection, multiplanar and curved multiplanar ref-mations, and volume rendering, may augment interpreta-n and improve communication of the findings (54). To ourowledge, it has not been scientifically shown that the use ofese tools increases diagnostic accuracy or diagnostic con-ence among specialists. For example, in 1 study multipla-r reconstructions when added to axial images aloneanged the interpretation in only 1 case (54). However,dimensional reconstruction is likely to play an important
Figure 9. Mimic of aortic dissection created bymotion of the aortic root. Top left, Image at thelevel of the right pulmonary artery demonstrates anormal descending thoracic aorta and pseudodis-section of the ascending aorta due to motion arti-fact that occurs on non–ECG-gated CT examina-tions (arrow). Top right, Image at the aortic rootshows a double contour to the aortic root that maysimulate a dissection flap (arrow). Bottom, Still im-age through the thoracic aorta further delineatesthe extent of the motion artifact. See the accom-panying full cine video. CT indicates computedtomographic imaging; and ECG, electrocardio-gram.
le in the planning of surgical or endovascular approaches.

4Mthar(4ofcofrabaspathtaduininbiavMchstofleinanis
4.Ainmblgathurmwrephtimimimse
4.Bevanofthidgadoblcawwblanax
4.TortewblSSManobante3-arinatno9-spfincafosu
4.RFousacrocacochobobmschaentimMorarw
4.TacImardicola
4AMV
e43JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
.4. Magnetic Resonance ImagingR has been shown to be very accurate in the diagnosis oforacic aortic disease, with sensitivities and specificities thate equivalent to or may exceed those for CT and TEE4,58–62). Like CT, MR provides a multiplanar evaluationthe thoracic aorta, and the examination can be extended inverage to include the length of the aorta and branch vessels,
om skull base to the toes. Advantages of MR include theility to identify anatomic variants of AoD (IMH and PAU),sess branch artery involvement, and diagnose aortic valvethology and left ventricular dysfunction without exposinge patient to either radiation or iodinated contrast. Disadvan-ges include prolonged duration of imaging acquisitionring which the patient is inaccessible to care providers;ability to use gadolinium contrast in patients with renalsufficiency; contraindication in patients with claustropho-a, metallic implants, or pacemakers; and lack of widespreadailability on an emergency basis. Although time-resolvedR techniques are improving, MR often cannot clearlyaracterize the relationship of an intimal flap and aortic root
ructures, specifically the coronary arteries. Likely as a resultthese considerations, data from IRAD found that MR was the
ast-used imaging study, used in only 1% of patients as theitial diagnostic study (63). For traumatic injury and congenitald inflammatory conditions of the thoracic aorta, the literatureprimarily descriptive, and accuracy data are not available.
4.1. Magnetic Resonance Imaging Techniquecomprehensive MR examination of the thoracic aorta mayclude many components, including black blood imaging,ay include basic spin-echo sequences, noncontrast whiteood imaging, contrast-enhanced MR angiography usingdolinium based agents, and phase-contrast imaging. MR ofe thoracic aorta in the acute setting can be shortened to meetgent patient assessment needs. The use of each is describedore specifically later. MR examinations have become faster,ith advances in gradient hardware that have significantlyduced repetition times, resulting in ultrafast MR angiogra-y techniques. However, MR examinations remain 2 to 4es longer than CT examinations. MR terminology across
aging vendors is less consistent than that of CT; therefore,aging sequences are described later as general types ofquences without vendor-specific details (58,59).
4.2. Black Blood Imaginglack blood imaging, using spin-echo sequences, is used toaluate aortic anatomy and morphology (such as aortic sized shape), and the aortic wall for hematoma or other causesthickening such as vasculitis. They may be repeated after
e administration of gadolinium-based contrast agents toentify wall enhancement. These sequences should use ECGting at end-diastole and may be performed with or withoutuble inversion recovery techniques that null the signal fromood. These sequences generate 2-dimensional images thatn be obtained in the axial, sagittal, and coronal planes, asell as the oblique sagittal or “candy cane” view. T1-eighted gradient echo sequences may be used in place ofack blood images and are usually performed both befored after contrast administration. They can be obtained in the
ial, sagittal, and coronal planes. ar4.3. Noncontrast White Blood Imaginghis is performed using either basic gradient echo sequences
the more advanced balanced steady-state free precessionchniques (SSFP) that are T2*weighted and generate imagesith subsecond temporal resolution. Signal is generated fromood, making it appear white in the absence of contrast.FP techniques use ultrashort repetition times that requireR scanners with high-performance gradients. For the latter,in-plane resolution of approximately 2.0�1.5 mm2 can betained using a repetition time of 3.2 ms, TE of 1.6 ms, flipgle of 60 to 70 degrees, and a 256�256 matrix. SSFPchniques can be performed to generate 2-dimensional,dimensional, and cine images; the 2-dimensional imagese usually performed in the axial, sagittal, and coronal planesan interleaved manner and use ECG gating with triggeringend-diastole to generate images in less than 500 ms that dot require breath holding. Cine SSFP sequences require 7- tosecond breath holding and are usually only performed atecific anatomic locations of interested, as determined by thedings on the previously generated images. For patients whonnot hold their breath, cine SSFP sequences can be per-rmed without using ECG gating or breath holding but withbstantially lower spatial and temporal resolution.
4.4. Contrast-Enhanced Magneticesonance Angiographyr the thoracic aorta, contrast-enhanced MR angiography isually performed with ECG gating. Although this increasesquisition time, it provides motion-free images of the aorticot and ascending aorta. For patients without a contraindi-tion to receiving a gadolinium-based contrast agent,ntrast-enhanced MR angiography is often the sequence ofoice from which most of the diagnostic information istained. Contrast-enhanced MR angiography images aretained as a 3-dimensional volumetric dataset, which can beanipulated and viewed in much the same manner as CTan datasets. Advances in MR, particularly gradient strength,ve markedly reduced the acquisition times of contrast-hanced MR angiography possible to subsecond acquisitiones. This temporally resolved subsecond contrast-enhanced
R angiography is particularly useful in critically ill patientspatients who cannot hold their breath, where motion
tifact can degrade other sequences that take longer to acquire,ith the tradeoff being a reduction of in-plane resolution.
4.5. Phase Contrast Imaginghese sequences are usually performed to evaluate gradientsross an area of stenosis, across an intimal or cardiac valve.age contrast is produced by differences in velocity. Images
e obtained using ECG gating or triggering. Two-mensional images are generated that center on the area ofncern. Peak flow and velocity measurements may be calcu-ted, and time–flow and time–velocity curves are generated.
.5. Standards for Reporting of the Thoracicorta on Computed Tomography andagnetic Resonance Imagingiewing and measuring are best accomplished at a picture
chiving and communications system workstation or an
inroaoinm
qu
enaltonaofFimte
4Adithanmlimle
inbetotim3)
Fimcrca
e44 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
dependent computer workstation, in which the aorta can betated into the best orientation to review each segment of therta and the aortic branches. This minimizes the chance ofadvertently confusing normal structures for vascular abnor-ality (Figure 10).
gure 10. Left brachiocephalic vein mimics an intramural he-atoma on CT. Axial CT image demonstrates a low-attenuationescent of material anterior to the innominate artery. CT indi-tes computed tomographic imaging.
The writing committee believes that specific qualitative andantitative elements are important to include in reports (Table 5).Diameter measurements taken from axial images are inher-tly incorrect unless the artery being measured is perfectlyigned in cross section on the image (Figure 11). It is preferablemake diameter measurements perpendicular to the longitudi-l or flow axis of the aorta to correct for the variable geometrythe aorta. Suggested standard anatomic locations are noted in
gure 12. The use of standardized measurements helps mini-ize errant reports of significant aneurysm growth due tochnique or interreader variability in measuring technique.
.6. Angiographyngiography provides accurate information about the site ofssection, branch artery involvement, and communication ofe true and false lumens (60,61). Additionally, angiographicd catheter-based techniques allow for evaluation and treat-ent of coronary artery (62) and aortic branch (visceral and
b artery) disease, as well as assessment of aortic valve andft ventricular function (60,63).Disadvantages of angiography compared with other lessvasive modalities include 1) not being universally availablecause it requires the presence of an experienced physicianperform the study; 2) being an invasive procedure that ise consuming and requires exposure to iodinated contrast;having poor ability to diagnose IMH given a lack of
Figure 11. Markedly tortuous aorta with thoraco-abdominal aortic aneurysm demonstrated on (A)3-dimensional shaded surface display rendering. Band C represent incorrect measurement of theaorta on standard coronal and axial images re-spectively, while D is an image of the aorta per-pendicular to the centerline or axis of the aorta,with the arrow demonstrating the correct locationfor diameter measurement, which in this case was7.8 cm.

lureopsetiootTlinaolaquea
4Tecmviaspaarsuheeaotto
thtiofothmRus
4.ATryrebootopagimpraset
4.ATtifi(Fandiimecthdithsethst
FistilluCtioM4,teclatte6gico
FiMin
e45JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
minal disruption; 4) potentially producing false negativesults when a thrombosed false lumen prevents adequateacification to identify the dissection; and 5) reportednsitivities and specificities of angiography for the evalua-n of acute AoD that are slightly lower than those for the
her less invasive modalities (42,64,65). Thus, CT, MR, andEE have replaced catheter-based angiography as the first-e diagnostic tests to establish the presence of the acutertic syndrome (60,63,66,67). Multidetector CT has alsorgely replaced angiography for the anatomic studies re-ired for treatment planning and monitoring of aortic dis-se (68).
.7. Echocardiographyhe aorta and its major branches can be visualized withhocardiography using a variety of imaging fields as well asethods of ultrasound. The suprasternal view is best forsualizing the aortic arch, whereas the aortic root andcending aorta are best seen in the left (and sometimes right)rasternal projection. When involvement of the innominatetery, left subclavian artery, or left common carotid artery isspected, orthogonal and longitudinal scanning planes arelpful. Imaging of the descending thoracic aorta is lesssily accomplished with echocardiography compared withher imaging modalities. Abdominal scan planes can be used
gure 12. Normal anatomy of the thoracoabdominal aorta withandard anatomic landmarks for reporting aortic diameter asstrated on a volume-rendered CT image of the thoracic aorta.
T indicates computed tomographic imaging. Anatomic loca-ns: 1, Aortic sinuses of Valsalva; 2, Sinotubular junction; 3,id ascending aorta (midpoint in length between Nos. 2 and 4);Proximal aortic arch (aorta at the origin of the innominate ar-
ry); 5, Mid aortic arch (between left common carotid and sub-avian arteries); 6, Proximal descending thoracic aorta (beginsthe isthmus, approximately 2 cm distal to left subclavian ar-
ry); 7, Mid descending aorta (midpoint in length between Nos.and 8); 8, Aorta at diaphragm (2 cm above the celiac axis ori-n); 9, Abdominal aorta at the celiac axis origin. CT indicatesmputed tomographic imaging.
visualize the caudal descending aorta. lu
In general, TEE is superior to TTE for assessment of theoracic aorta. Through the use of multiplane image acquisi-n, 3-dimensional Doppler TEE is safe and can be per-rmed at the bedside, with a low risk of complications (lessan 1% overall, less than 0.03% for esophageal perforation),ost of which are related to conscious sedation (69,70).econstruction of the aorta can be performed. Intraoperativee of TEE is noted in Sections 14.2.3 and 14.2.4.
7.1. Echocardiographic Criteria for Thoracicortic Aneurysmshe echocardiographic diagnosis of thoracic aortic aneu-sms is determined on demonstration of aortic enlargementlative to the expected aortic diameter, based on age- anddy size–adjusted nomograms (Figures 2, 3, 4, and 13). Forher aortic segments, such nomograms have not been devel-ed, so aortic dilatation is diagnosed when the aorta exceedsgenerally agreed to standard diameter (Table 3) or when aven aortic segment is larger than contiguous aortic seg-ent(s) of apparently normal size. Beyond establishing theesence of aortic enlargement, echocardiography may revealsociated cardiac pathology that suggests the underlyingiology of the aortic disease (e.g., bicuspid aortic valve).
7.2. Echocardiographic Criteria forortic Dissectionhe echocardiographic diagnosis of an AoD requires the iden-cation of a dissection flap separating true and false lumensigure 14). However, one of the major limitations of both TTEd TEE is the frequent appearance of artifacts that mimic assection flap (Figure 15). These usually arise from a mirrorage or reverberation artifact that appears as a mobile linearhodensity overlying the aortic lumen. It is therefore essentialat the echocardiographer make certain to distinguish truessection flaps from such artifacts. The first step is to confirme presence of the dissection flap from several angles and fromveral transducer locations. The second step is to confirm thate dissection flap has a motion independent of surroundingructures and that the apparent flap is contained within the aortic
gure 13. Transthoracic echocardiogram of a patient witharfan syndrome with mitral valve prolapse and 4-cm ascend-g aortic aneurysm.
men (i.e., does not pass through the aortic wall in any view).

TdicaDtrcointosyevsifodeththm(“th
inpodiphve
midmprsecaef
4.FO
Ttothacshthseofdi63botiv95
foofdiinvoad(psetiodeprcabeorAabsy
4.FO
IMecmthIntyaoththmthwsmra
Fisew
e46 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
he third step is to usecolor-flow Doppler to demonstratefferential flow on the 2 sides of the dissection flap. Often onen visualize 1 or more sites of intimal tears, with color-flowoppler demonstrating sites of flow between the 2 lumens. Theue lumen typically exhibits expansion during systole andllapse during diastole. Additional signs of the true lumenclude little or nospontaneous echocardiographic contrast, sys-lic jets directed away from the lumen, and forward flow duringstole. The false lumen often exhibits diastolic expansion,idence of spontaneous contrast, complete or partial thrombo-
s, and reversed, delayed, or absent blood flow. Imaging criteriar distinguishing the true and false lumens have also beenscribed for intravascular ultrasound (71) and CT (72). Featuresat characterize the false lumen of an acute dissection includee wedgelike angle (the “beak sign”) where the dissection flapeets the aortic wall, the presence of strandlike structurescobwebs”) in the lumen, and the lack of a laminar structure ine outer wall of the lumen.Associated echocardiographic findings of clinical importance
clude identification of a pericardial effusion. Indeed, it is oftenssible to see a layer of echogenic material within the pericar-al fluid that is indicative of hemopericardium. Echocardiogra-y can provide important information about right and left
gure 14. Arch aneurysm with dissection flap. Top, Arch dis-ction, 2-dimensional view. Bottom, Arch dissection (arrow)
ith color-flow Doppler margination.
ntricular function and myocardial ischemia based on assess- w
ent of left ventricular segmental wall motion. On TEE, one canentify the ostia of the 2 coronary arteries and detect involve-ent by the dissection flap. Echocardiography also identifies theesence of aortic regurgitation and permits grading of itsverity. On TEE, the mechanisms of acute aortic regurgitationn be defined, and these data can be used to guide the surgeon’sforts to spare the valve at the time of aortic repair.
7.2.1. DIAGNOSTIC ACCURACY OF ECHOCARDIOGRAPHY
R AORTIC DISSECTION
TE has a sensitivity of 77% to 80% and a specificity of 93%96% for identification of proximal AoD. For distal AoD,
e sensitivity of TTE is lower. TEE improves the diagnosticcuracy substantially, particularly when a patient’s bodyape, chest wall, or concomitant pulmonary disease restrictse transthoracic windows for aortic imaging. With TEE,nsitivity for proximal AoD is 88% to 98% with a specificity90% to 95% (46). A 2006 meta-analysis that evaluated the
agnostic utility of TEE in suspected thoracic AoD included0 patients from 10 different studies. TEE was shown toth accurately identify and rule out acute AoD with sensi-ities and specificities of 98% (95% CI 95% to 99%) and% (95% CI 92% to 97%), respectively (46).
Major advantages of TEE include its portability (allowingr bedside patient evaluation), rapid imaging time, and lackintravenous contrast or ionizing radiation. Additionally,
ssection-related cardiac complications can be evaluatedcluding aortic regurgitation, proximal coronary artery in-lvement, and the presence of tamponade physiology. Dis-vantages of TEE include a potential lack of availabilityarticularly at small centers and during off hours) anddation requirements that may include endotracheal intuba-n (73). The accuracy of TEE can be quite operatorpendent. For the very distal ascending aorta and theoximal aortic arch, TEE may be limited by a blind spotused by interposition of the trachea and left main bronchustween the esophagus and aorta. Small, circumscribed AoDsIMHs in this region are less well visualized by TEE.
nother limitation of TEE is its inability to visualize thedominal aorta; if there is concern of a malperfusionndrome, an abdominal CT may also be required.
7.2.2. DIAGNOSTIC ACCURACY OF ECHOCARDIOGRAPHY
R ACUTE INTRAMURAL HEMATOMA
H of the aorta has a distinctly different appearance onhocardiography. In contrast to classic AoD, in IMH there is noobile intimal flap within the aortic lumen, and in most casese aortic lumen has a relatively normal round appearance.stead, in IMH there is thickening of the aortic wall that ispically crescentic in shape and extends along a length of therta. In some cases it can be difficult to distinguish the wallickening of IMH from diffuse aortic atherosclerosis or muralrombus lining an aortic aneurysm. However, atheroma andural thrombus protrude from the aortic intima into the lumen,us giving both the aortic wall and the lumen an irregular shape,hereas in IMH the inner lining of the aortic lumen remainsooth. Moreover, in the presence of intimal calcification, intramu-
l thrombus will present as thickening external to calcification,
hereas mural thrombus will be internal to calcification.
4.TI
Gpreacoasfodoimdisytosu
al
5T
5CL
1.
2.
3.
4.
5.
Fifa
e47JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
7.2.3. ROLE OF ECHOCARDIOGRAPHY IN FOLLOWING PA-
ENTS WITH CHRONIC AORTIC DISEASE
iven that TEE is a semi-invasive procedure; it is usually noteferred for surveillance of patients with thoracic aortic dis-ses. Also, although TTE is noninvasive, its failure to visualizensistently and measure accurately the tubular portion of thecending thoracic aorta is problematic. It is not typically used tollow aneurysms in that aortic segment. However, because TTEes accurately visualize the aortic root, its primary role as anaging method for serial follow-up is in patients with aortic
sease limited to the root, particularly those with Marfanndrome. It is also used, often in conjunction with CT or MR,observe patients with concomitant structural heart disease,
ch as bicuspid aortic valve, mitral valve prolapse, cardiomeg-
y, or cardiomyopathy.
. Genetic Syndromes Associated Withhoracic Aortic Aneurysms and Dissection
.1. Recommendations for Genetic SyndromesASS I
An echocardiogram is recommended at the time of
gure 15. Artifact mimicking dissection. Top left, 2-dimensional vct not seen in this view.
diagnosis of Marfan syndrome to determine the aortic
root and ascending aortic diameters and 6 months thereaf-ter to determine the rate of enlargement of the aorta. (Levelof Evidence: C)Annual imaging is recommended for patients with Marfansyndrome if stability of the aortic diameter is documented. Ifthe maximal aortic diameter is 4.5 cm or greater, or if theaortic diameter shows significant growth from baseline,more frequent imaging should be considered. (Level ofEvidence: C)Patients with Loeys-Dietz syndrome or a confirmed geneticmutation known to predispose to aortic aneurysms and aorticdissections (TGFBR1, TGFBR2, FBN1, ACTA2, or MYH11)should undergo complete aortic imaging at initial diagnosisand 6 months thereafter to establish if enlargement is occur-ring. (74–77) (Level of Evidence: C)Patients with Loeys-Dietz syndrome should have yearly mag-netic resonance imaging from the cerebrovascular circulationto the pelvis. (23,78,79) (Level of Evidence: B)Patients with Turner syndrome should undergo imaging of theheart and aorta for evidence of bicuspid aortic valve, coarcta-tion of the aorta, or dilatation of the ascending thoracic aorta.(80) If initial imaging is normal and there are no risk factors foraortic dissection, repeat imaging should be performed every 5to 10 years or if otherwise clinically indicated. If abnormalitiesexist, annual imaging or follow-up imaging should be done.
p right, Color-flow Doppler without margination. Bottom, Arti-
iew. To(Level of Evidence: C)

CL
1.
2.
3.
CL
1.
5.MtisprrecoFthreencecaelthfibsyinfoMth(TLbasyhi
caManthduin
retoTboscitiladuselepasy
tioInpraoecwantodithofvaseseththdimthcaV
rapaha
wfetiopranthwimcostdiwtrof
paththA
e48 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ASS IIa
It is reasonable to consider surgical repair of the aorta in alladult patients with Loeys-Dietz syndrome or a confirmed TG-FBR1 or TGFBR2 mutation and an aortic diameter of 4.2 cm orgreater by transesophageal echocardiogram (internal diame-ter) or 4.4 to 4.6 cm or greater by computed tomographicimaging and/or magnetic resonance imaging (external diame-ter). (78) (Level of Evidence: C)For women with Marfan syndrome contemplating pregnancy, itis reasonable to prophylactically replace the aortic root andascending aorta if the diameter exceeds 4.0 cm. (74) (Level ofEvidence: C)If the maximal cross-sectional area in square centimeters ofthe ascending aorta or root divided by the patient’s height inmeters exceeds a ratio of 10, surgical repair is reasonablebecause shorter patients have dissection at a smaller size and15% of patients with Marfan syndrome have dissection at asize less than 5.0 cm. (16,76,81) (Level of Evidence: C)
ASS IIb
In patients with Turner syndrome with additional risk factors,including bicuspid aortic valve, coarctation of the aorta,and/or hypertension, and in patients who attempt to becomepregnant or who become pregnant, it may be reasonable toperform imaging of the heart and aorta to help determine therisk of aortic dissection. (Level of Evidence: C)
1.1. Marfan Syndromearfan syndrome is a heritable disorder of the connectivesue with a high penetrance but variable expression. Ap-oximately 25% of patients do not have a family history andpresent new cases due to sporadic mutations for thendition. Marfan syndrome results from mutations in the
BN1 gene, with over 600 mutations currently entered intoe FBN1 mutation database causing Marfan syndrome orlated conditions (http://www.umd.be/). The FBN1 genecodes fibrillin-1, a large glycoprotein that is secreted fromlls and deposited in the extracellular matrix in structureslled microfibrils. Microfibrils are found at the periphery ofastic fibers, including the elastic fibers in the medial layer ofe ascending aorta, and in tissues not associated with elasticers (82). Only 12% of FBN1 mutations causing Marfanndrome have been observed more than once in unrelateddividuals, a fact that complicates using mutational detectionr diagnosis. A second locus for Marfan syndrome, termedFS2, was recently identified to be caused by mutations ine transforming growth factor-beta type II receptorGFBR2) (83). The phenotype of this locus may overlap for
oeys-Dietz syndrome. The criteria for Marfan syndrome issed primarily on clinical findings in the various organstems affected in the Marfan syndrome, along with familystory and FBN1 mutations status (84).The cardinal features of Marfan syndrome involve therdiovascular, ocular, and skeletal systems. Patients witharfan syndrome are highly predisposed to thoracic aorticeurysm and/or dissection, with virtually every patient withe syndrome having evidence of aortic disease at some pointring their lifetime. Other cardiovascular manifestations
clude valvular disease, primarily mitral valve prolapse and wgurgitation (85). Aortic regurgitation can result from dis-rtion of the aortic valve cusps by an enlarged aortic root.he skeletal manifestations reflect overgrowth of the longnes and include arachnodactyly, dolichostenomelia, kypho-oliosis, dolichocephaly, and pectus deformities. Abnormal-es in the connective tissues are also manifested as jointxity, recurrent or incisional hernias, striae atrophica, andral ectasia (84). The ocular manifestation that is bothnsitive and fairly specific for Marfan syndrome is ectopiantis or lens dislocation. The presence of ectopia lentis is articularly useful clinical finding to differentiate Marfanndrome from Loeys-Dietz syndrome (78).Most patients with Marfan syndrome present with dilata-n of the aortic root/ascending aorta or Type A dissection.ternal aortic diameter measured at the sinuses of Valsalvaovides a baseline for future evaluations because this is thertic segment that dilates in Marfan syndrome. Of note,hocardiographic studies measure the internal diameter,hereas most patients undergo definitive imaging by CTd/or MR, which measures the external diameter (expectedbe 0.2 to 0.4 cm larger than internal diameter), and externalameter is the measurement used in most cases to determinee threshold for surgical repair. There is growing awareness
the importance of relating this measurement to normallues based on age and body surface area (15) (Table 4). Theverity of the aortic disease is related to the degree andgment length of aortic dilatation with dilatation limited toe sinuses of Valsalva having a less malignant prognosisan dilatation that extends to the aortic arch (86). Afteragnosis, follow-up imaging studies are recommended at 6onths and then annually if stability is documented based one high likelihood of aortic disease progression. In mostses, TTE can be used to monitor the size of the sinuses ofalsalva.A subset of patients present with Type B dissection, and a
re patient will present with AAA. The poor outcome oftients with Marfan syndrome with acute Type B dissectionss led some to advocate early surgical repair (87).Studies addressing the efficacy of beta blockade in patients
ith Marfan syndrome have shown slower aortic root growth,wer cardiovascular end points (defined as aortic regurgita-n, dissection, surgery, heart failure, or death), and im-oved survival (88). Patients continue to enlarge their aortad dissect on therapy, so such medication does not precludee need for routine imaging and prophylactic aortic repairhen the diameter of the aorta warrants repair. It is alsoportant to note that significant aortic root dilatation isrrelated negatively with therapeutic response (88). Recent
udies in a mouse model of Marfan syndrome with aorticsease similar to that seen in humans showed that treatmentith losartan normalized aortic root growth (6), and a clinicalial using losartan in Marfan syndrome patients under the age
25 years is in progress (89,90) (see Section 9.2.1.1).Surgical repair of the dilated aortic root/ascending aorta fortients with Marfan syndrome is usually performed at areshold of a external diameter of 5.0 cm (91), smaller thanat for other patients because of the greater tendency foroD at a smaller diameter (see Section 9.2.2.1). Factors that
ill prompt repair at an external diameter of less than 5.0 cm
arhiof
andineSucathplaocasosp
riSefranwduse
5.Tan(7ei(Tth
oupaThepathmarducedimromDreyoDthaoaosuactioth
ve
yethmacduca
5.orTauthrugarutinbydiabarmdocaheplthsysyanthsudlsufainwruinDtifge
5.T145fincaemanao8%Tonsypo
e49JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
e rapid growth defined as greater than 0.5 cm/y, familystory of AoD at a diameter less than 5.0 cm, or the presencesignificant aortic regurgitation.After prophylactic repair of the ascending aorta, the archd descending aorta are sites for later-onset aneurysms andssections in patients with Marfan syndrome, prompting theed for routine imaging of the arch and descending aorta.rvival in patients with Marfan syndrome has been signifi-ntly improved with medical and surgical management ofe aortic disease (76,92,93). The David valve sparing reim-antation operation for suitable patients undergoing electivertic root surgery at centers with a high volume of theseses has become standard practice (76,92–99), althoughme have reported less-optimal long-term results with valve-aring procedures (100,101).Pregnant patients with Marfan syndrome are at increased
sk for AoD if the aortic diameter exceeds 4 cm (102) (seection 10). All women with Marfan syndrome warrant
equent cardiovascular monitoring throughout pregnancyd into the puerperium. Limited data on the treatment ofomen with Marfan syndrome who experience dissectionsring pregnancy suggest a better outcome with cesareanction with concomitant aortic repair (103).
1.2. Loeys-Dietz Syndromehe Loeys-Dietz syndrome is an autosomal dominant aorticeurysm syndrome with involvement of many other systems8,104). Loeys-Dietz syndrome results from mutations inther the transforming growth factor receptor Type I or IIGFBR1 or TGFBR2) genes and the diagnosis is confirmedrough mutational analysis of these genes (105).The disease is characterized by the triad of arterial tortu-sity and aneurysms, hypertelorism and bifid uvula or cleftlate, or a uvula with a wide base or prominent ridge on it.
he arterial tortuousity is most commonly observed in thead and neck vessels but can occur in other vessels. Thesetients also have a spectrum of other features, which includee following: velvety and translucent skin, craniosynostosis,alar hypoplasia, retrognathia, blue sclera, patent ductusteriosus, skeletal features similar to Marfan syndrome,ral ectasia, atrial septal defects, developmental delay,rvical spine abnormalities, and joint laxity. The vascularsease in these patients is particularly aggressive with aean age of death of 26 years (78). Most patients have aorticot aneurysms (98%) that lead to AoD. Because there areultiple reports of AoD occurring in patients with Loeys-ietz when the aortic diameter was less than 5.0 cm, repair iscommended at smaller diameters (78) (see Section 5.1). Forung children with severe systemic manifestations of Loeys-
ietz syndrome, specifically prominent craniofacial featuresat are associated with more severe aortic disease, once thertic diameter exceeds the 99th percentile for age and thertic valve annulus reaches 1.8 to 2.0 cm, prophylacticrgery allows for the placement of a graft of sufficient size tocommodate growth. Of note, echocardiographic examina-ns that measure the internal aortic diameter were used in
ese studies to determine the threshold for surgical repair.Patients with Loeys-Dietz also develop aneurysms of other
ssels (53%), leading to the recommendation that they have dearly MR imaging from the cerebrovascular circulation toe pelvis. Current studies indicate that aggressive surgicalanagement of the aneurysms in these patients can behieved with few complications (23,78). Surgical proce-res in patients with Loeys-Dietz syndrome are not compli-ted by tissue fragility (23,79).
1.3. Ehlers-Danlos Syndrome, Vascular FormType IV
he vascular form of Ehlers-Danlos syndrome is a raretosomal dominant disorder characterized by easy bruising,in skin with visible veins, characteristic facial features, andpture of arteries, uterus, or intestines. Rupture of thestrointestinal tract is more likely to occur prior to arterialpture, and the majority of patients survive the gastrointes-al rupture (106). Most of the fatal complications are causedarterial rupture, with most deaths attributable to arterial
ssections or ruptures involving primarily the thoracic ordominal arteries, including AoDs and ruptures. Theseterial ruptures lead to reduced life expectancy, with theedian survival of only 48 years, and often no aneurysms arecumented. If the rupture of an artery is life threatening, itn be surgically repaired, but tissue fragility, tendency tomorrhage extensively, and poor wound healing may com-icate the surgical repair (107). Whether there is a role fore repair of unruptured aneurysms in patients with thisndrome is not clear, which is in contrast to Loeys-Dietzndrome, where a role for prophylactic surgical repair ofeurysms is already well established. Nevertheless, whenese patients present with AoD or aortic root aneurysms,ccessful aortic surgery can be achieved with careful han-ing of tissues and resewing of anastomoses with pledgetedtures (76). Noninvasive vascular imaging is preferred astal complications have been associated with invasive imag-g in these patients (106). The outcome of pregnancy inomen with Ehlers-Danlos syndrome is poor because ofpture of the gravid uterus and vessel rupture at delivery orthe postpartum period. The diagnosis of vascular Ehlers-
anlos syndrome is based on DNA or protein studies iden-ying a defect in type III collagen, encoded by the COL3A1ne.
1.4. Turner Syndromeurner syndrome is defined as complete or partial absence ofsex chromosome in a phenotypic female, most commonly, X. Short stature and ovarian failure are the most prevalentding, but women with Turner syndrome have an increasedrdiovascular mortality rate from both structural and isch-ic heart disease, especially AoD (108,109). Between 10%
d 25% of patients with Turner syndrome have a bicuspidrtic valve. Aortic coarctation is present in approximately
of patients. Determining aortic dilatation in patients withurner syndrome is difficult because aortic dilatation is based
body surface area so the aortas of patients with Turnerndrome are expected to be smaller than those of the generalpulation because of the patient’s short stature. If one
fines aortic dilatation as an ascending-to-descending aortic
diT
anD00TDlopaTocascoTfoavdihemforeye(1faRmassthytr
5.foAdrroraarhagr
reinAdisothinth
thNTisalth
5.ACL
1.
2.
CL
1.
2.
CL
1.
2.
AanFathgethanhiasiDaummicryanTTAis
th
e50 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ameter ratio of greater than 1.5, then 33% of women withurner syndrome had aortic dilatation (110).The average age of AoD in Turner syndrome was 31 years,d less than half of the patients survived the event (111).ata indicate a population-based AoD incidence of 36:1000 Turner syndrome years (1.4% among individuals with
urner syndrome) compared with 6:100 000 in the generalanish population (112). Therefore, the risk of AoD is muchwer in patients with Turner syndrome compared withtients with Marfan syndrome or Loeys-Dietz syndrome.
he majority of dissections in women with Turner syndromecur in patients with known risk factors for dissection, suchcardiovascular malformations (bicuspid aortic valve or
arctation of the aorta), systemic hypertension, or both.herefore, the evidence base regarding the value of screeningr aortic disease in women with Turner syndrome is notailable. However, there appears to be an increased risk forssection in these women, suggesting that imaging of theart, aorta, and pulmonary veins at the time of diagnosisight be valuable (80,113). For patients with no risk factorsr AoD (bicuspid aortic valve, coarctation, dilated aorta),-evaluation of the aorta has been suggested every 5 to 10ars or if clinically indicated (e.g., attempting pregnancy14) or transition to an adult clinic). Patients with riskctors for AoD should undergo more frequent imaging.ecently, studies have not shown an effect of growth hor-one treatment in women with Turner syndrome on eithercending or descending aortic diameter (113). In addition,udies have not found any evidence of left ventricularpertrophy in patients with Turner syndrome who were
eated with growth hormone (115,116).
1.5. Other Genetic Syndromes With Increased Riskr Thoracic Aortic Aneurysms and Dissectionssubstantial proportion of patients with Ehlers-Danlos syn-ome who do not have the vascular form also have aorticot dilatation, but the progression of this dilatation to AoD isre (76,117). Similarly, patients with congenital contracturalachnodactyly or Beals syndrome due to mutations in FBN2ve had aortic root enlargement without documented pro-ession to dissection (118,119).There are other genetic syndromes that have multiple
ports or documentation of thoracic aortic aneurysms lead-g to Type A dissections. There are multiple case reports ofoD in patients with autosomal dominant polycystic kidneysease (120,121). Although AoD is a complication of auto-mal dominant polycystic kidney disease, it is less commonan cerebral aneurysms leading to subarachnoid hemorrhagethis population. There is insufficient information to gauge
e value of routine or screening imaging for these patients.Similar to autosomal dominant polycystic kidney disease,
ere are multiple reports in the literature of patients withoonan syndrome who are experiencing AoDs (122–124).he value of imaging or routine monitoring of these patientsunknown. A review of 200 patients with Alagille syndromeso identified thoracic aortic disease in a small subset of
ese patients (125). TG1.6. Recommendations for Familial Thoracic Aorticneurysms and DissectionsASS I
Aortic imaging is recommended for first-degree relatives ofpatients with thoracic aortic aneurysm and/or dissection toidentify those with asymptomatic disease. (126,127) (Level ofEvidence: B)If the mutant gene (FBN1, TGFBR1, TGFBR2, COL3A1, ACTA2,MYH11) associated with aortic aneurysm and/or dissection isidentified in a patient, first-degree relatives should undergocounseling and testing. Then, only the relatives with thegenetic mutation should undergo aortic imaging. (Level ofEvidence: C)
ASS IIa
If one or more first-degree relatives of a patient with knownthoracic aortic aneurysm and/or dissection are found to havethoracic aortic dilatation, aneurysm, or dissection, then imag-ing of second-degree relatives is reasonable. (126) (Level ofEvidence: B)Sequencing of the ACTA2 gene is reasonable in patients witha family history of thoracic aortic aneurysms and/or dissec-tions to determine if ACTA2 mutations are responsible for theinherited predisposition. (26,27,77,78,128,129) (Level of Ev-idence: B)
ASS IIb
Sequencing of other genes known to cause familial thoracicaortic aneurysms and/or dissection (TGFBR1, TGFBR2,MYH11) may be considered in patients with a family historyand clinical features associated with mutations in thesegenes. (26,27,77,78,128,129) (Level of Evidence: B)If one or more first-degree relatives of a patient with knownthoracic aortic aneurysm and/or dissection are found to havethoracic aortic dilatation, aneurysm, or dissection, then refer-ral to a geneticist may be considered. (Level of Evidence: C)
genetic basis of nonsyndromic familial thoracic aorticeurysms and dissection has only recently been defined.milial aggregation studies of patients referred for repair oforacic aortic aneurysm and dissection that did not have anetic defect have indicated that between 11% and 19% ofese patients have a first-degree relative with thoracic aorticeurysms and dissection (127,130). Patients with a familystory of thoracic aortic aneurysm and dissection present atyounger mean age than do sporadic patients but at a
gnificantly older age than patients with Marfan or Loeys-ietz syndrome. The disease is primarily inherited in antosomal dominant manner with decreased penetrance pri-arily in women and variable expression (131). Theseapping studies have firmly established that there is signif-ant genetic heterogeneity for familial thoracic aortic aneu-sm and dissection (i.e., many different genes can be mutatedd cause the same clinical condition) (27,77,129,132–134).
he causative gene has been identified for the following loci:AD2 is due to TGFBR2 mutations, the mutant gene at 16p
the MYH11 gene, and the TAAD4 defective gene is ACTA2.The defective gene at the TAAD2 locus for familial
oracic aortic aneurysms and dissection was identified as
FBR2, which is the same gene that is mutated in approx-
imGaom4ofastiomasincesiwtoin(7
dito(1sm(MmuntioDantifiretharfawth
laansmcolafa
Awflobesedididithof3or
facrmfomdiprlehafuunreimim
5TryTastiomdi
scattio
Ta
DeF
An
TG
M
AC
re
e51JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
ately two thirds of patients with Loeys-Dietz syndrome.enetic testing of unrelated families with familial thoracicrtic aneurysm and dissections demonstrated that TGFBR2utations were only present in 1% to 5% of families (26). Allfamilies had mutations that affected TGFBR2 arginine 460
the receptor, suggesting that missense mutation wassociated with familial thoracic aortic aneurysm and dissec-n (i.e., genotype-phenotype correlation). Although the
ajority of vascular disease in these families involved thecending aorta, affected family members also had descend-g aortic disease and aneurysms of other arteries, includingrebral, carotid, and popliteal aneurysms. It is notable thatmilar to Loeys-Dietz syndrome, AoDs occur in patientsith TGFBR2 mutation at diameters less than 5.0 cm, leadingthe recommendation that aortic repair be considered at a
ternal diameter by echocardiography of 4.2 cm or greater8) (see Section 5.1).A large French family with thoracic aortic aneurysm and
ssection associated with patent ductus arteriosus was usedmap the defective gene causing this phenotype to 16p
35). The defective gene at this locus was identified as theooth muscle cell–specific myosin heavy chain 11YH11), a major protein in the contractile unit in smooth
uscle cells (77). Subsequent analysis of DNA from 93related families with thoracic aortic aneurysm and dissec-n failed to identify any MYH11 mutations. Sequencing
NA from 3 unrelated families with thoracic aortic aneurysmd dissection associated with patent ductus arteriosus iden-ed MYH11 mutations in 2 of these families (26); the
maining family had a TGFBR2 mutation as the cause of theoracic aortic aneurysm and dissection and patent ductusteriosus. Therefore, MYH11 mutations are responsible formilial thoracic aortic aneurysm and dissection associatedith patent ductus arteriosus and a rare cause of familialoracic aortic aneurysm and dissection.A defective gene at the locus 10q23–24 was identified in a
rge family with multiple members with thoracic aorticeurysm and dissection as ACTA2, which encodes the theooth muscle-specific alpha-actin, a component of thentractile complex and the most abundant protein in vascu-r smooth muscle cells (27,136). Approximately 15% of
ble 6. Gene Defects Associated With Familial Thoracic Aortic
fective Gene Leading toamilial Thoracic Aorticeurysms and Dissection
Contribution to Familial ThoracicAortic Aneurysms and
Dissection
FBR2 mutations 4%
YH11 mutations 1%
TA2 mutations 14%
ACTA2 indicates actin, alpha 2, smooth muscle aorta; MYH11, smooth muscceptor type II.
milies with thoracic aortic aneurysm and dissection have un
CTA2 mutations (27). Features identified in some familiesith ACTA2 mutation included livedo reticularis and iriscculi, although the prevalence of these features has noten determined. The majority of affected individuals pre-nted with acute Type A or B dissections or Type Bssections, with 16 of 24 deaths occurring due to Type Assections. Two of 13 individuals experienced Type Assections with a documented ascending aortic diameter lessan 5.0 cm. AoDs occurred in 3 individuals under 20 yearsage, and 2 women died of dissections postpartum. Finally,
young men had Type B dissection complicated by ruptureaneurysm formation at the ages of 13, 16, and 21 years.Identification of the underlying genetic mutation leading to
milial thoracic aortic aneurysms and dissections providesitical clinical information for the family. First, only familyembers who harbor mutations need to be routinely imagedr aortic disease. Second, identification of the underlyingutation may lead to different management of the aorticsease, as is the case for TGFBR2 mutations. In addition tooviding information to families, identification of genesading to familial thoracic aortic aneurysms and dissectionss emphasized the roles of smooth muscle contractilenction in preventing aortic diseases (11). Individuals whodergo genetic testing for thoracic aortic disease shouldceive genetic counseling prior to the testing to explain theplications for the testing for their medical follow-up andplications for family members.
.2. Summaryhe genes leading to nonsyndromic forms of aortic aneu-sms and dissections are in the early stages of identification.ables 6 and 7 summarize the current clinical featuressociated with mutations in these genes and recommenda-ns for when to sequence these genes in families with
ultiple members with familial thoracic aortic aneurysm andssection.Given the familial risk of thoracic aortic aneurysms,reening the proband’s first-degree relatives with appropri-e imaging studies is indicated in the absence of identifica-n of the defective gene leading to the disease.Because thoracic aortic disease is typically asymptomatic
sm and Dissection
Associated Clinical Features Comments on Aortic Disease
Thin, translucent skin Multiple aortic dissectionsdocumented at aorticdiameters �5.0 cm
Arterial or aortic tortuosity
Aneurysm of arteries
Patent ductus arteriosus Patient with documenteddissection at 4.5 cm
Livedo reticularis Two of 13 patients withdocumented dissections
�5.0 cmIris flocculi
Patent ductus arteriosus
Bicuspid aortic valve
fic beta-myosin heavy chain; and TGFBR2, transforming growth factor-beta
Aneury
le speci
til a life-threatening event (e.g., AoD) occurs, evaluating

otdediTthofbasiposeinwat
6AA
6VinCL
1.
2.
Bm1%ha(1spguaswnoanvacomfoconacoleleatthsureasva
Ta
Ge
Ma
Lo
Ehva
Tu
imphenot
e52 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
her family members can potentially prevent prematureaths. Most syndromes and familial forms of thoracic aorticsease are inherited in an autosomal dominant manner.herefore, an individual with an inherited predisposition tooracic aortic aneurysm and dissections has up to a 50% riskpassing on this predisposition to their children, which is thesis for genetic evaluation of the offspring. In addition,
blings and parents of the patient need to be evaluated forssible predisposition to thoracic aortic aneurysm and dis-ctions. Because of the variable age of onset of aortic diseasefamilial thoracic aortic aneurysms and dissections, the
riting committee believes that imaging of family membersrisk of the disease every 2 years is warranted.
. Other Cardiovascular Conditionsssociated With Thoracic Aorticneurysm and Dissection
.1. Recommendations for Bicuspid Aorticalve and Associated Congenital VariantsAdults
ASS I
First-degree relatives of patients with a bicuspid aortic valve,premature onset of thoracic aortic disease with minimal riskfactors, and/or a familial form of thoracic aortic aneurysm anddissection should be evaluated for the presence of a bicuspidaortic valve and asymptomatic thoracic aortic disease. (Level
ble 7. Genetic Syndromes Associated With Thoracic Aortic An
netic Syndrome Common Clinical Features Gen
rfan syndrome Skeletal features (see text) FBN1Ectopia lentisDural ectasia
eys-Dietz syndrome Bifid uvula or cleft palate TGFBRmArterial tortuosity
Hypertelorism
Skeletal features similar to MFS
Craniosynostosis
Aneurysms and dissections of otherarteries
lers-Danlos syndrome,scular form
Thin, translucent skin COL3
Gastrointestinal rupture
Rupture of the gravid uterus
Rupture of medium-sized to largearteries
rner syndrome Short stature 45,X
Primary amenorrhea
Bicuspid aortic valve
Aortic coarctation
Webbed neck, low-set ears, low hairline,broad chest
AoD indicates aortic dissection; COL3A1, type III collagen; CT, computed tomoaging; TEE, transesophageal echocardiogram; TGFBR1, transforming growth fa
*The defective gene at a second locus for MFS is TGFBR2 but the clinical
of Evidence: C) dr
All patients with a bicuspid aortic valve should have both theaortic root and ascending thoracic aorta evaluated for evi-dence of aortic dilatation. (137–140) (Level of Evidence: B)
icuspid aortic valves is the most common congenital abnor-ality affecting the aortic valve and the aorta and is found in
to 2% of the population (137). Nine percent of patientsve family members who also have bicuspid aortic valves41). The ACC/AHA Valvular Heart Disease Guidelinesecifically address this condition (5). Of importance to thisideline, bicuspid aortic valves can be inherited in familiesan autosomal dominant condition and may be associated
ith thoracic aortic aneurysm formation. It is important tote that in these families, members can have thoracic aorticeurysms in the absence of bicuspid aortic valves (142). Thelves are prone to either aortic valve regurgitation, mostmmonly seen in younger patients, or aortic valve stenosis,ore common in older patients. Bicuspid aortic valve repairr regurgitation has excellent long-term results, an importantnsideration in the absence of prosthetic aortic valve alter-tives in this young population (99,139,140,143). The mostmmon site of fusion of the leaflets is at the left and rightaflet commissure, and less so at the right noncoronaryaflet commissure. The latter is typically more often associ-ed with aortic valve stenosis. In a study of 2000 patients ate Cleveland Clinic who underwent bicuspid aortic valvergery, 20% had concurrent ascending aortic aneurysms thatquired repair (139,140). AoD is also common, and as many
15% of patients with acute AoD have bicuspid aorticlves (144), a frequency more common than Marfan syn-
and Dissection
ct Diagnostic Test Comments on Aortic Disease
ns* Ghent diagnostic criteria Surgical repair when the aorta reaches5.0 cm unless there is a family history
of AoD at �5.0 cm, a rapidlyexpanding aneurysm or presence orsignificant aortic valve regurgitation
DNA for sequencing
BR1 DNA for sequencing Surgical repair recommended at anaortic diameter of �4.2 cm by TEE
(internal diameter) or 4.4 to �4.6 cmby CT and/or MR (external diameter)
ions DNA for sequencing Surgical repair is complicated byfriable tissues
Noninvasive imaging recommendedDermal fibroblasts for
analysis of type IIIcollagen
pe Blood (cells) forkaryotype analysis
AoD risk is increased in patients withbicuspid aortic valve, aortic coarctation,
hypertension, orpregnancy
imaging; FBN1, fibrillin 1; MFS, Marfan syndrome; MR, magnetic resonanceta receptor type I; TGFBR2, transforming growth factor beta receptor type II.ype as MFS is debated.
eurysm
etic Defe
mutatio
2 or TGFutations
A1 mutat
karyoty
graphicctor-be
ome. AoD was present in 12.5% of patients with bicuspid

vapasi
scrempambiredikn
6Abrappathmanmofaoalaralismsuinsisuancaex
6CthasounpaprhyAreprchdu
wwAqum
vico2-descanbesubewtiopr
6Athsotothcoabty
acoenvaIIincoarenararcaariofartyfoifsu
7W
7aSeCL
1.
e53JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
lves with an aortic diameter less than 5 cm, reminiscent oftients with Marfan syndrome in whom 15% had AoD at a
ze less than 5 cm (16,143).The writing committee discussed the potential need toreen relatives of patients who have undergone aortic valveplacement before age 70, as these younger patients wereore likely to have had bicuspid aortic valve as their primarythology. However, 40% of women and around one third ofen over age 70 undergoing aortic valve replacement havecuspid aortic valve disease (145). The yield from screeninglatives of younger patients with bicuspid aortic valvesease compared with relatives of older patients is notown.
.2. Aberrant Right Subclavian Arteryberrant right subclavian artery, which arises as the fourthanch from the aorta, courses behind the esophagus inproximately 80% of patients and causes dysphagia in manytients (146–149). The dysphagia usually occurs in adults ase artery enlarges (Kommerell diverticulum) (150,151). Inost adult patients, the aorta is also abnormal and is prone toeurysm formation, dissection, and rupture. Surgical treat-ent in adults involves resection of the aneurysmal segmentthe subclavian artery (the diverticulum) and the adjacent
rta and replacement of the aorta with a graft (152). Anternative treatment is exclusion of the right subclaviantery origin and adjacent aorta using an aortic endograft,though long-term follow-up of this endovascular approachnot available and the compression and aneurysm growth
ay continue (153). The distal normal segment of thebclavian artery is usually not reimplanted into the descend-g aorta directly but rather revascularized using an interpo-tion graft or carotid-subclavian bypass. Alternatively, thebclavian artery can be ligated or coiled distal to theeurysm, implanting the distal segment into the adjacentrotid artery in the neck and thus restoring flow to the uppertremity and the ipsilateral vertebral artery (148,149,152).
.3. Coarctation of the Aortaoarctation of the aorta is a relatively common abnormalityat occurs in about 40 to 50 of every 100 000 live births, with2:1 ratio in males versus females. Most lesions are treatedon after birth or in childhood, and adults presenting withtreated coarctation of the aorta are rare. More often,tients have had previous procedures and present with lateroblems such as heart failure, intracranial hemorrhage,pertension particularly with exercise, aneurysm formation,
oD, rupture of old repairs, undersized grafts of previouspairs, and infections. It is of particular importance ineviously treated patients with some aortic narrowing toeck for a gradient across the stenosis and for hypertensionring exercise testing (154).Untreated coarctation of the aorta has a dismal prognosis,
ith 80% of patients dying from complications associatedith the coarctation. Approximately one quarter will die fromoD or rupture, one quarter will die from heart failure, onearter will die from intracranial hemorrhage, and the re-
ainder will die from other complications.Surgical options, depending on the lesion, include subcla-an artery patch aortoplasty, patch aortoplasty, bypass of thearctation, tube graft replacement, aneurysm replacement,stage combined bicuspid valve surgery, and arch andscending aorta replacement or ascending aorta–to–de-ending aorta bypass (3). Endovascular balloon dilatationd stent placement has been used successfully and iscoming a less invasive alternative to conventional openrgical procedures (155). Occasionally, the adult aorta mayredundant and kinked opposite the ligamentum arteriosum
ithout any pressure gradient, the so-called pseudocoarcta-n. Aneurysms that require surgical treatment may developoximal and distal to the kinked area (156).
.4. Right Aortic Archright-sided aortic arch is present in approximately 0.5% ofe population and rarely requires surgical repair. However,me patients present with dysphagia or asthma-like symp-ms with expiratory wheezing. CT or MR readily diagnosese problem of either tracheal compression or esophagealmpression with the esophagus enlarged and filled with gasove the level of the arch. Felson and Palayew described 2pes (157).In Type I, the great vessels come off the right-sided arch in
manner that is a mirror image to normal anatomy; however,mpression of the esophagus or trachea is caused by anlarged aorta where it crosses the vertebral bodies or by thescular ring formed by the atretic ductus arteriosus. In Type
, the aberrant left subclavian artery comes off the descend-g aorta and typically runs posterior to the trachea andmpresses the trachea. As with an aberrant right subclaviantery, the proximal segment of the subclavian artery maylarge and form a Kommerell diverticulum. Other variationse also seen but are exceedingly rare. A separate trunk mayise from the arch, and from this trunk, the innominate,rotid, and subclavian arteries arise. Another rare finding isright-sided arch with a stump of left-sided aorta joining theght-sided arch after it crosses into the left chest. The stumpthe left-sided aorta gives off a branch to the left subclavian
tery. The aorta with right-sided arches is also abnormal andpically very fragile and prone to AoD, rupture, or aneurysmrmation. Surgical repair involves resection of the aorta and,needed, reimplantation or bypass of the aberrant left
bclavian artery.
. Inflammatory Diseases Associatedith Thoracic Aortic Disease
.1. Recommendations for Takayasu Arteritisnd Giant Cell Arteritise Table 8.
ASS I
Initial therapy for active Takayasu arteritis and active giantcell arteritis should be corticosteroids at a high dose (pred-nisone 40 to 60 mg daily at initiation or its equivalent) toreduce the active inflammatory state. (158,159) (Level of
Evidence: B)
2.
3.
4.
CL
1.
7Tidanfo
Omalmwcothdebe
vetyanartisintountioioca
19ondiaothev(Ftivreercypadi
inastioswthremclcuahym
Inne(1deao60foaom
TaAo
Na
Taart
Giaart
Bedis
Ansp
e54 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
The success of treatment of patients with Takayasu arteritisand giant cell arteritis should be periodically evaluated todetermine disease activity by repeated physical examinationand either an erythrocyte sedimentation rate or C-reactiveprotein level. (160,161) (Level of Evidence: B)Elective revascularization of patients with Takayasu arteritisand giant cell arteritis should be delayed until the acuteinflammatory state is treated and quiescent. (162) (Level ofEvidence: B)The initial evaluation of Takayasu arteritis or giant cell arteritisshould include thoracic aorta and branch vessel computedtomographic imaging or magnetic resonance imaging to inves-tigate the possibility of aneurysm or occlusive disease in thesevessels. (Level of Evidence: C)
ASS IIa
It is reasonable to treat patients with Takayasu arteritisreceiving corticosteroids with an additional anti-inflammatoryagent if there is evidence of progression of vascular disease,recurrence of constitutional symptoms, or re-elevation of in-flammatory marker. (158) (Level of Evidence: C)
.2. Takayasu Arteritisakayasu arteritis, also known as pulseless disease, is aniopathic vasculitis of the elastic arteries, involving the aortad its branches. Initially described in Japan, the disease is
ble 8. Inflammatory Diseases Associated With Thoracicrtic Aneurysm and Dissection
mesCriteria Used in
Diagnosis/SourceWhen Is Diagnosis
Established?
kayasueritis (163)
Age of onset �40 y �3 criteria arepresent (sensitivity90.5%; specificity
97.8%)
Intermittent claudication
Diminished brachial arterypulse
Subclavian artery or aortic bruit
Systolic BP variation of�10 mm Hg between arms
Aortographic evidence of aortaor aortic branch stenosis
nt celleritis (164)
Age �50 y �3 criteria arepresent (sensitivitygreater than 90%;specificity �90%)
Recent-onset localizedheadache
Temporary artery tenderness orpulse attenuation
Elevated erythrocytesedimentation �50 mm/h
Arterial biopsy showsnecrotizing vasculitis
hcetease (165)
Oral ulceration Oral ulceration plus 2of the other 3 criteriaRecurrent genital ulceration
Uveitis or retinal vasculits
Skin lesions—erythemanodosum, pseudo-folliculitis, or
pathergy
kylosingondylitis (166)
Onset of pain �40 y 4 of the diagnosticcriteria are presentBack pain for �3 mo
Morning stiffness
Subtle symptom onset
Improvement with exercise
BP indicates blood pressure.
und worldwide. In the United States, a review of cases in ry
lmsted County, Minn, reported a rate of 2.6 cases perillion persons (158). In the United States, the disease affectsl ethnic and racial groups in proportion to the census with aoderate Asian overrepresentation. The disease affectsomen approximately 10 times more often than men. Mostmmonly diagnosed in the third decade (i.e., the 20s) of life,e disease has been found in children and adults in the fifthcade (i.e., the 40s). Two specific disease distributions haveen reported: Japanese and Indian (167,168).In the Japanese distribution, the thoracic aorta and greatssels are most commonly affected. In contrast, in the Indianpe, the disease most commonly affects the abdominal aortad the renal arteries (28). The pathogenesis of Takayasuteritis remains poorly defined. A T-cell–mediated panarteri-, the disease proceeds from adventitial vasa vasorumvolvement inward. The antigen for the localized inflamma-ry process is undefined but likely specific as the T cellsdergo clonal expansion. The outcome process of destruc-n and fibrotic repair depends on the dominant pathophys-
logic process: destruction yields aneurysms while fibrosisuses stenosis.The diagnosis of Takayasu arteritis may be made using the90 American College of Rheumatology criteria: 1) age ofset younger than 40 years, 2) intermittent claudication, 3)minished brachial artery pulse, 4) subclavian artery orrtic bruit, 5) systolic blood pressure variation of greateran 10 mm Hg between arms, and 6) angiographic (CT, MR)idence of aorta or aortic branch vessel stenosis (163)igure 16). When 3 of the criteria are manifest, the sensi-ity and specificity for diagnosis are 90.5% and 97.8%,
spectively. Laboratory testing may aid in diagnosis. Mark-s of inflammation, such as C-reactive protein and erythro-te sedimentation rate, are elevated in approximately 70% oftients in the acute phase and 50% in the chronic phase ofsease (158).The clinical manifestations of the disease typically develop2 phases: acute and chronic. Acutely, the inflammation
sociated with Takayasu arteritis causes a host of constitu-nal, or “B,” symptoms, such as weight loss, fatigue, nighteats, anorexia, and malaise (158). More chronically, once
e vascular process has endured, patients report symptomsferable to the organs involved. In the largest US experience,ore than half of all patients experienced upper extremityaudication, half had symptoms associated with cerebrovas-lar insufficiency (vision loss, lightheadedness, stroke), andthird reported carotid artery pain (158). In an Indian series,pertension as a result of renal artery involvement was theost common presenting sign (169).The aorta itself may develop either aneurysm or stenosis.a Japanese series of 116 patients with Takayasu arteritis,arly 32% of the patients had aortic aneurysm formation70). Most commonly, aneurysm formation developed in thescending aorta, followed by the abdominal, then ascendingrtic segments. In the National Institutes of Health series ofpatients with Takayasu arteritis, 23% had aortic aneurysm
rmation (158). Aneurysms most commonly formed in thertic arch or root, abdomen, and then other thoracic seg-ents. Stenosis of the aorta is more common than is aneu-
sm formation, occurring in 53% of patients in the National
FiananviInthna
e55JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
gure 16. Takayasu arteritis with involvement of the thoracoabdominal aorta and great vessels as shown on contrast-enhanced CTd MR examinations. Note narrowing of the arterial lumen and circumferential soft tissue thickening of the walls of the great vesselsd thoracic and abdominal aorta. Panel A, Image through the great vessels with narrowing of the left common carotid and left subcla-
an arteries. Panel B, Mid descending thoracic aorta (arrowheads). Panel C, Aorta just above the diaphragm (arrowheads). Panel D,frarenal aorta. Panel E, Volume-rendered image from CT demonstrates the extent of involvement. Panel F, Oblique sagittal MR of theoracic aorta. Panel G, Coronal MR of the abdominal aorta. CT indicates computed tomographic imaging; and MR, magnetic reso-
nce imaging.
Ininth
rehiermtroftiouscrofDno
foseTinremisMpranth
7Gvabrafpewofeppenapr
hethloprthantocldeaschtrreneinfo
popa
th50pa18inAAcoof(1twC
folotemvaandiofoftoda
wclwreaufothflapolompo
tieclredaav2fenetradlabldiletio
e56 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
stitutes of Health series. Any segment of the aorta may bevolved, but the abdominal aortic segment is affected morean 70% of the time if stenosis is found.Treatment of Takayasu arteritis begins with inflammationduction with corticosteroids. Steroids are typically started atgh dose, 40 to 60 mg daily at initiation to lower theythrocyte sedimentation rate or C-reactive protein to nor-al, and are required for 1 to 2 years to ensure proper diseaseeatment (169). Despite the prolonged regimen, nearly half
the patients will relapse during tapering, requiring addi-nal immunosuppression. Second-line agents that have beened include methotrexate, azathioprine, and antitumor ne-osis factor-alpha agents (158,169). Unfortunately, markersinflammation are imperfect barometers of disease activity.
isease progression has been shown to occur in the setting ofrmal marker levels (158).Revascularization for aortic stenosis or aneurysm occursr the same indications as in noninflammatory disorders:condary organ vascular insufficiency or risk of rupture.here are no randomized trials of percutaneous or surgicaltervention in this disease (158,171–173). Nonrandomizedports have shown that revascularization of either varietyay be appropriate, with one caveat. The risk of graft failurehigher in patients with active local inflammation (162).oreover, the presence of aneurysmal disease itself may beoblematic. One report documented a 12% incidence ofastomotic aneurysms over 2 decades of follow-up related toe presence of aneurysms at surgery (174).
.3. Giant Cell ArteritisCA, also known as temporal arteritis, is an elastic vesselsculitis involving the aorta and its secondary and tertiaryanches. Distinguishing it from Takayasu arteritis, GCAfects patients above the age of 50 years, with an incidenceaking in the eighth decade of life (175). The disease affectsomen in a 3:2 ratio to men and has a predilection for those
northern European ancestry (29). In the United States,idemiologic investigation reports a prevalence of 20 casesr 100 000 persons. The incidence is higher in Scandinaviantions but lower in southern Europe, suggesting a geneticedisposition in certain populations (176).The clinical presentation of GCA is varied, requiring aightened suspicion by clinicians for early diagnosis. Half ofe patients report constitutional symptoms, such as weightss, night sweats, malaise, and fever (177). Because of theedilection for secondary and tertiary thoracic branches ofe aorta, cranial symptoms are common. Scalp tendernessd headache are present in two thirds of patients and in up90% of patients with biopsy-proved disease (177). Jaw
audication is common and affects half of the patients, 20%velop visual changes, and other neurologic symptoms suchstroke or neuropathy occur in nearly one third (29). Visualanges are particularly important to notice, because early
eatment may prevent permanent blindness. Patients mayport diplopia, amaurosis fugax, or blurriness prior to blind-ss. Polymyalgia rheumatica characterized by a generalizedflammatory state with proximal muscle involvement is
und in nearly half of patients with GCA (29). Patients with arlymyalgia rheumatica report muscular pain and stiffness,rticularly on initiation of movement.Extracranial vascular involvement is less common in GCAan in Takayasu arteritis, occurring in 25% of patients. In a-year study of Olmsted County, Minn, that included 168tients with GCA, aortic aneurysm/dissection was found in% of the subjects, whereas large-artery stenosis was noted13% of patients (178). No patient had stenosis of the aorta.
ortic aneurysm formation represents an important marker.lthough aneurysm formation per se does not reduce survivalmpared with the GCA cohort as a whole, AoD in the settingan aneurysm reduces survival to an average of 1.1 years
78). Similarly, aortic aneurysm rupture or dissection causedo thirds of deaths in a series of patients with GCA in
alifornia (179).The American College of Rheumatology diagnostic criteriar GCA include 1) age older than 50 years, 2) recent-onsetcalized headache, 3) temporal artery pulse attenuation ornderness, 4) erythrocyte sedimentation rate greater than 50m/h, and 5) an arterial biopsy demonstrating necrotizingsculitis (164). Three or more criteria confer a sensitivityd specificity above 90% for the disease. With intracranialsease, temporal artery biopsies are diagnostic in up to 80%cases (180). The rate of positivity declines with initiationglucocorticoid therapy, but this should not delay treatmentavoid GCA complications. Biopsies performed within 7
ys of steroid initiation retain a high diagnostic yield (181).The pathophysiology of GCA shares important features
ith Takayasu arteritis (28). GCA is marked by a T-cellonal expansion suggesting a specific antigenic response,hich currently remains unelucidated. The inflammatorysponse, which begins in the adventitial layer, is marked bygmented cytokine and MMP production causing granulomarmation. Granuloma formation both shields the vessel frome inciting antigen and causes vessel destruction. The in-mmatory environment within the vessel wall with thessible formation of aneurysms or vessel stenosis is histo-gically identical to that of Takayasu arteritis. Because of theultiyear cyclical nature of disease incidence, some havesited an infectious etiology (29).Corticosteroids represent the standard in therapy for pa-nts with GCA (182). The typical treatment regimen in-
udes starting prednisone dose of 40 to 60 mg daily, althoughcent evidence suggests a similar efficacy with 30 to 40 mgily (183). Therapy is typically required for 1 to 2 years tooid recurrence, although the dose may be tapered beginningto 3 months after initiation. Patients commonly report
eling much better rapidly but, as with Takayasu arteritis,w vascular involvement may occur in up to half of patients
eated with steroids (184). In contrast to Takayasu arteritis,ditional immunomodulatory agents do not seem to modu-te the disease’s progress. Methotrexate studied in a double-ind, placebo-controlled study as an adjunct to prednisoned not reduce morbidity, erythrocyte sedimentation ratevel, or cumulative prednisone dose (184a). Revasculariza-n recommendations follow the same pattern as in Takayasu
teritis.

7Inbaanledies(1naatuvnothocco(HthcoboredithwTtioth
BpuhihivatofomAarABfapsseinre
7(STlinco(1thenwhe
ofth
wfoofpasytiem40reaova(1ab
7Intuan(1noagbupsanprsithTmadinpafrheseinsiacracatinm
tioarPgr
ricamaoinwtypavi
e57JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
.4. Behcet Disease1937, Hulusi Behçet described his eponymous syndrome
sed on a set of 3 symptoms: uveitis, aphthous stomatitis,d genital ulcers. Most common in Turkey, with a preva-nce of 80 to 370 cases per 100 000 persons (185,186), thesease is much less common in the United States, with antimated prevalence of 1 to 3 cases per million persons87). The diagnostic criteria were established by the Inter-tional Group for Behçet’s disease and require oral ulcer-ion and 2 of these 3 lesions: recurrent genital ulceration,eitis or retinal vasculitis, or skin lesions, such as erythemadosum, pseudofolliculitis, or pathergy (188). In addition toese cardinal manifestations, vascular involvement maycur in one third of patients. A small vessel vasculitismmonly associated with the human leukocyte antigenLA) B51 allele (187), Behçet disease is 1 of 2 vasculitides
at may also involve veins. Venous involvement is mostmmonly superficial thrombophlebitis, but deep vein throm-sis in the vena cava, varices, and cerebral sinuses has beenported (189). The small vessel involvement of Behçetsease may result in nonvascular complaints, such as ery-ema nodosum, arthritis, and gastrointestinal involvementith diarrhea, gastrointestinal bleeding, or perforation (187).reatment of Behçet disease varies based on the manifesta-n of disease. Systemic corticosteroids are the typical
erapy for those with vascular involvement.Specifically with regard to vascular manifestations of
ehçet disease, any artery or vein, large or small, systemic orlmonary, may be involved by the vasculitic process. Aorticstopathology shows lymphocytic infiltration mixed withstiocytes and eosinophils with giant cells around vasasorum of media and adventitia. Destruction of media leadsaneurysm formation and may proceed to pseudoaneurysm
rmation and rupture. Aneurysm formation may occur inultiple sites and in different sites over a period of follow-up.neurysm, stenotic lesions, and occlusion of brachiocephalicteries may occur with or without aortic involvement.lthough aortic involvement is unusual for patients withehçet vasculitis, aneurysm rupture can be unpredictable andtal (190,191). With regard to surgical repair, anastomoticeudoaneurysms often occur (12.9% within 18 months in 1ries) and may be related to ongoing inflammatory changesthe area of anastomotic suture lines (192). Endovascular
pair with stent grafts has also been described (193).
.5. Ankylosing Spondylitispondyloarthropathies)
he group of diseases labeled spondyloarthropathies areked by the strong association of major histocompatibilitymplex HLA B-27 and the absence of rheumatoid factor94,195). Several features are common to the spondyloar-ropathies, including sacroilitis, inflammatory arthritis orthesitis (inflammation of tendon insertions), associationsith inflammatory bowel disease or psoriasis, and aortitis andart block (195).Ankylosing spondylits is the most common variant andten begins with back pain and stiffness in the second or
ird decade of life. It affects men 2 to 3 times as often as cromen, worsens with inactivity, and commonly takes yearsr the diagnosis to be made (196). The diagnosis requires 4the 5 criteria: onset of pain at younger than 40 years, backin for longer than 3 months, morning stiffness, subtlemptom onset, and improvement with exercise (197). Pa-nts may also report constitutional symptoms, such asalaise or fever. Acute anterior uveitis is reported in up to% of patients. Aortic root and aortic valve involvement areported in up to 80% of patients (198). When involved, thertic valve may have a nodular appearance, and aorticlvular regurgitation is present in nearly half of the patients98). Treatment of aortic root expansion and aortic valvularnormalities is the same as for other conditions.
.6. Infective Thoracic Aortic Aneurysmsfection (due to bacterial, fungal, viral, spirochetal, orbercular organisms) is a rare cause of thoracic aorticeurysms. Originally named mycotic endarteritis by Osler99), the terms infected aneurysm or infectious aortitis arew used more commonly, because the majority of etiologicents are nonfungal. Saccular aneurysms are most common,t infected aneurysms can be fusiform and often eveneudoaneurysms. The ascending thoracic aorta, aortic arch,d descending thoracic aorta can all be affected, as canosthetic aortic grafts and aortic homografts. Typically, thetes of infected aneurysms are opposite the great vessels ine aortic arch or opposite the visceral ateries in the abdomen.here are several mechanisms by which the aortic infectionay arise. First, there may be contiguous spread fromjacent thoracic structures, such a mediastinitis, abscess,fected lymph nodes, infectious pericarditis, empyema, orravertebral abscess. Second, there may be septic emboli
om underlying bacterial endocarditis. Third, there may bematogenous dissemination of bacteria in the setting ofpsis or intravenous drug abuse. Infection most often arisesa diseased aorta, either in a preexisting aneurysm, at the
te of an atherosclerotic plaque, or at the site of somecidental or iatrogenic aortic trauma. Indeed, infected tho-cic aortic aneurysms may arise as a late complication ofrdiac surgery, often associated with postoperative medias-itis, typically at the sites of aortic cannulation or anasto-
otic suture lines (200,201).Various organisms can infect the aorta, with most infec-ns being bacterial. Staphylococcus aureus and Salmonella
e the organisms most commonly identified (202–204).neumococcus and Escherichia coli are relatively commonam-positive and gram-negative pathogens, respectively.Treponema pallidum, the gram-negative spirochete bacte-
um that causes syphilis, as well as other Treponema species,n cause infected aortitis, with the ascending thoracic aortaost often involved. However, in syphilitic aortitis, thoracicrtic aneurysm does not appear for 10 to 25 years after theitial spirochetal infection. Fungal infections of the aorta,ith either Candida or Aspergillus, occur less often (205) andpically occur in the setting of impaired immunity, such astients with systemic illness, human immunodeficiencyrus, or prior organ or bone marrow transplant.Indeed, patients with impaired immunity are also at in-
eased risk of tuberculous aortitis attributable to mycobac-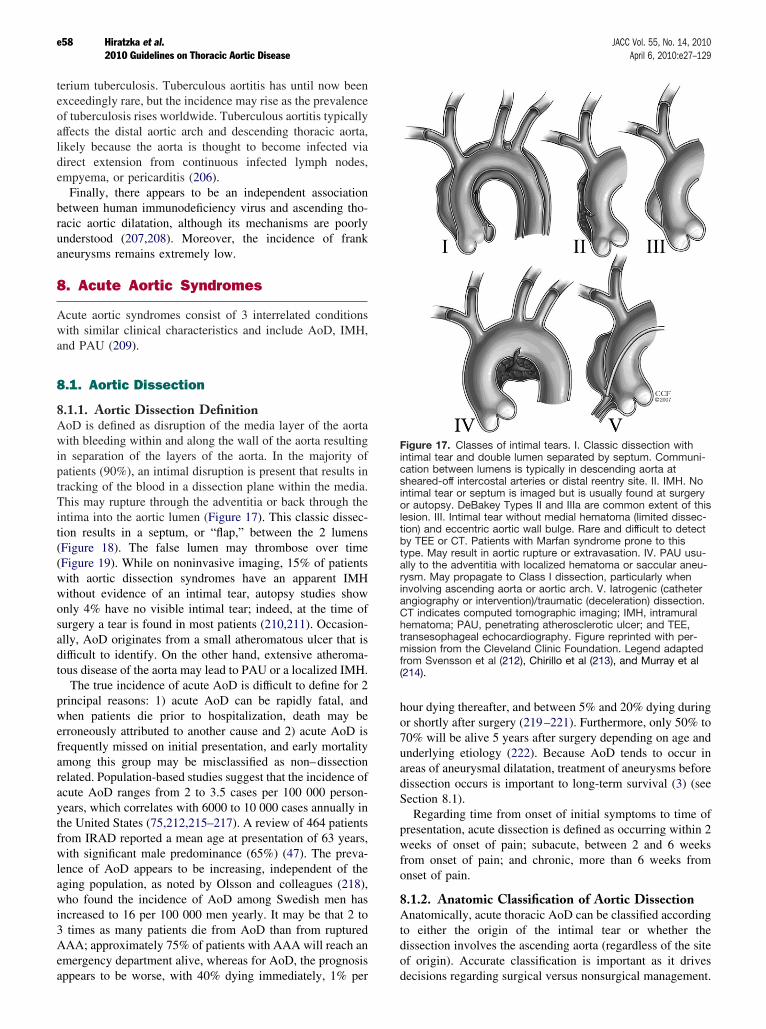
teexofaflikdiem
beraunan
8
Awan
8
8.AwinpatrTintio(F(Fwwonsualdito
prwerframreacyethfrwleagwin3Aemap
hoor70unardiSe
prwfron
8.Atodiof
FiincashinorletiobytyalryinanChetramfro(2
e58 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
rium tuberculosis. Tuberculous aortitis has until now beenceedingly rare, but the incidence may rise as the prevalencetuberculosis rises worldwide. Tuberculous aortitis typically
fects the distal aortic arch and descending thoracic aorta,ely because the aorta is thought to become infected via
rect extension from continuous infected lymph nodes,pyema, or pericarditis (206).Finally, there appears to be an independent associationtween human immunodeficiency virus and ascending tho-cic aortic dilatation, although its mechanisms are poorlyderstood (207,208). Moreover, the incidence of frankeurysms remains extremely low.
. Acute Aortic Syndromes
cute aortic syndromes consist of 3 interrelated conditionsith similar clinical characteristics and include AoD, IMH,d PAU (209).
.1. Aortic Dissection
1.1. Aortic Dissection DefinitionoD is defined as disruption of the media layer of the aortaith bleeding within and along the wall of the aorta resultingseparation of the layers of the aorta. In the majority of
tients (90%), an intimal disruption is present that results inacking of the blood in a dissection plane within the media.his may rupture through the adventitia or back through thetima into the aortic lumen (Figure 17). This classic dissec-n results in a septum, or “flap,” between the 2 lumensigure 18). The false lumen may thrombose over timeigure 19). While on noninvasive imaging, 15% of patientsith aortic dissection syndromes have an apparent IMHithout evidence of an intimal tear, autopsy studies showly 4% have no visible intimal tear; indeed, at the time ofrgery a tear is found in most patients (210,211). Occasion-ly, AoD originates from a small atheromatous ulcer that isfficult to identify. On the other hand, extensive atheroma-us disease of the aorta may lead to PAU or a localized IMH.The true incidence of acute AoD is difficult to define for 2incipal reasons: 1) acute AoD can be rapidly fatal, andhen patients die prior to hospitalization, death may beroneously attributed to another cause and 2) acute AoD isequently missed on initial presentation, and early mortality
ong this group may be misclassified as non–dissectionlated. Population-based studies suggest that the incidence ofute AoD ranges from 2 to 3.5 cases per 100 000 person-ars, which correlates with 6000 to 10 000 cases annually ine United States (75,212,215–217). A review of 464 patientsom IRAD reported a mean age at presentation of 63 years,ith significant male predominance (65%) (47). The preva-nce of AoD appears to be increasing, independent of theing population, as noted by Olsson and colleagues (218),ho found the incidence of AoD among Swedish men hascreased to 16 per 100 000 men yearly. It may be that 2 totimes as many patients die from AoD than from rupturedAA; approximately 75% of patients with AAA will reach anergency department alive, whereas for AoD, the prognosis
pears to be worse, with 40% dying immediately, 1% per de
ur dying thereafter, and between 5% and 20% dying duringshortly after surgery (219–221). Furthermore, only 50% to% will be alive 5 years after surgery depending on age andderlying etiology (222). Because AoD tends to occur ineas of aneurysmal dilatation, treatment of aneurysms beforessection occurs is important to long-term survival (3) (seection 8.1).Regarding time from onset of initial symptoms to time ofesentation, acute dissection is defined as occurring within 2eeks of onset of pain; subacute, between 2 and 6 weeksom onset of pain; and chronic, more than 6 weeks fromset of pain.
1.2. Anatomic Classification of Aortic Dissectionnatomically, acute thoracic AoD can be classified according
either the origin of the intimal tear or whether thessection involves the ascending aorta (regardless of the site
origin). Accurate classification is important as it drives
gure 17. Classes of intimal tears. I. Classic dissection withtimal tear and double lumen separated by septum. Communi-tion between lumens is typically in descending aorta ateared-off intercostal arteries or distal reentry site. II. IMH. Notimal tear or septum is imaged but is usually found at surgeryautopsy. DeBakey Types II and IIIa are common extent of this
sion. III. Intimal tear without medial hematoma (limited dissec-n) and eccentric aortic wall bulge. Rare and difficult to detectTEE or CT. Patients with Marfan syndrome prone to this
pe. May result in aortic rupture or extravasation. IV. PAU usu-ly to the adventitia with localized hematoma or saccular aneu-sm. May propagate to Class I dissection, particularly whenvolving ascending aorta or aortic arch. V. Iatrogenic (cathetergiography or intervention)/traumatic (deceleration) dissection.
T indicates computed tomographic imaging; IMH, intramuralmatoma; PAU, penetrating atherosclerotic ulcer; and TEE,nsesophageal echocardiography. Figure reprinted with per-
ission from the Cleveland Clinic Foundation. Legend adaptedm Svensson et al (212), Chirillo et al (213), and Murray et al
14).
cisions regarding surgical versus nonsurgical management.
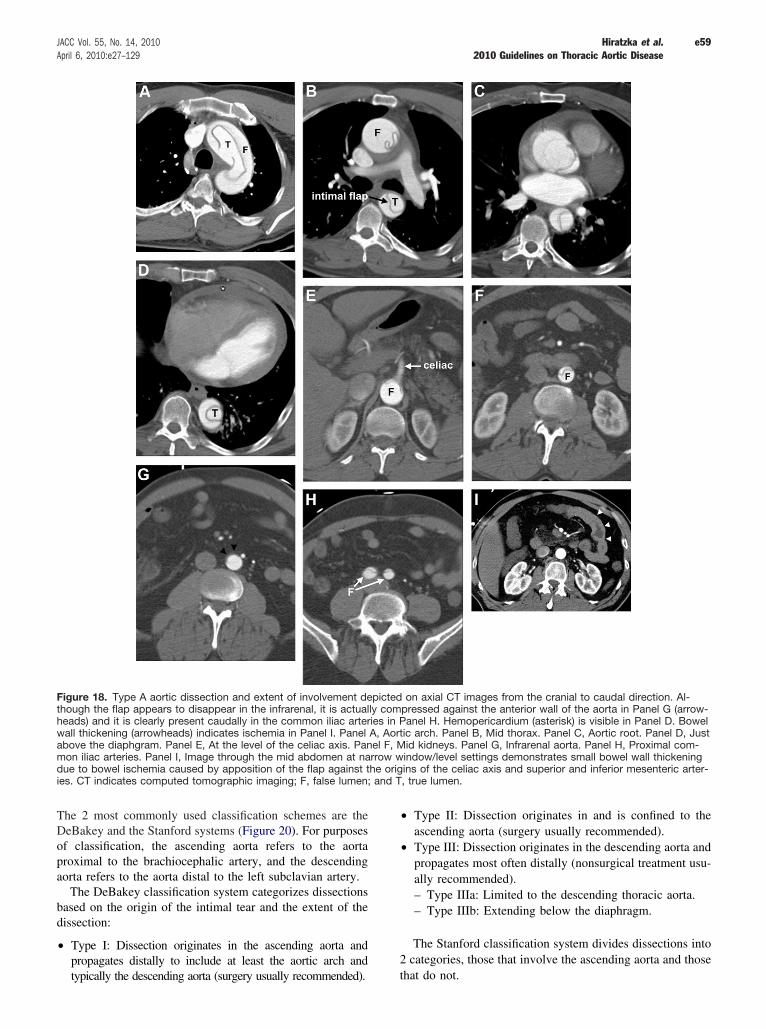
TDofprao
badi
•
•
•
2
Fithhewabmduie nd T,
e59JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
he 2 most commonly used classification schemes are theeBakey and the Stanford systems (Figure 20). For purposes
classification, the ascending aorta refers to the aortaoximal to the brachiocephalic artery, and the descendingrta refers to the aorta distal to the left subclavian artery.The DeBakey classification system categorizes dissectionssed on the origin of the intimal tear and the extent of thessection:
Type I: Dissection originates in the ascending aorta andpropagates distally to include at least the aortic arch and
gure 18. Type A aortic dissection and extent of involvement depough the flap appears to disappear in the infrarenal, it is actuallyads) and it is clearly present caudally in the common iliac arterie
all thickening (arrowheads) indicates ischemia in Panel I. Panel Aove the diaphgram. Panel E, At the level of the celiac axis. Paneon iliac arteries. Panel I, Image through the mid abdomen at narre to bowel ischemia caused by apposition of the flap against th
s. CT indicates computed tomographic imaging; F, false lumen; a
typically the descending aorta (surgery usually recommended). th
Type II: Dissection originates in and is confined to theascending aorta (surgery usually recommended).Type III: Dissection originates in the descending aorta andpropagates most often distally (nonsurgical treatment usu-ally recommended).– Type IIIa: Limited to the descending thoracic aorta.– Type IIIb: Extending below the diaphragm.
The Stanford classification system divides dissections intocategories, those that involve the ascending aorta and those
n axial CT images from the cranial to caudal direction. Al-ressed against the anterior wall of the aorta in Panel G (arrow-nel H. Hemopericardium (asterisk) is visible in Panel D. Bowelarch. Panel B, Mid thorax. Panel C, Aortic root. Panel D, Just
d kidneys. Panel G, Infrarenal aorta. Panel H, Proximal com-dow/level settings demonstrates small bowel wall thickenings of the celiac axis and superior and inferior mesenteric arter-true lumen.
icted ocomps in Pa, Aorticl F, Miow wine origin
at do not.

• •
e60 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
Type A: All dissections involving the ascending aortaregardless of the site of origin (surgery usually recom-mended) (Figures 18 and 20).
Type B: All dissections that do not involve the ascendingaorta (nonsurgical treatment usually recommended). Noteinvolvement of the aortic arch without involvement of the
Figure 19. Type A Aortic dissection with throm-bosed false lumen and left renal artery involvementdepicted on axial CT images. Demonstratesmarked narrowing of the true lumen, patent rightrenal artery arising from the true lumen (bottomleft, arrow), and narrow left renal artery com-pressed by thrombus in the false lumen, with sec-ondary decreased enhancement of the left kidneycompared with the right kidney. Top left, At thelevel of the left main coronary artery. Top right, Atthe celiac axis. Bottom left, At the right renal artery(arrow). Bottom right, At the left renal artery (ar-row). *Thrombus in false lumen. CT indicates com-puted tomographic imaging; L, left kidney; and R,right kidney.
Figure 20. Aortic dissection classification:DeBakey and Stanford Classifications. Re-printed with permission from the ClevelandClinic Foundation.

clwapeiofpainbywpasideblus
cl(F
8.Rm(Thysisydrsyunsyeahi
anstsyreTsyfoguthpr
aoancounofcohathA
anantieD
TaAo
Co
Co
e61JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
ascending aorta in the Stanford classification is labeled asType B (Figure 21).
At this time, there is no unanimity regarding whichassification system is the ideal one to use. Some of theriting committee members believe that a more pragmaticproach is to refer to the dissection involving the aorta asther proximal or distal to the left subclavian artery. Othersthe writing committee do not use this approach. Thus, if atient has an arch dissection even without ascending aorticvolvement, then immediate surgery would be recommended
some, if feasible and the patient is viable. Others on theriting committee would select medical management if thetient has only an arch dissection without proximal exten-
on, malperfusion, or bleeding, as long as repeat imagingmonstrates stability. If there is evidence of malperfusion oreeding in such a patient, then the writing committee wouldually select a surgical approach.The intimal tear and AoD can also be categorized into
asses that may have a bearing on treatment (212,213)igure 17).
1.3. Risk Factors for Aortic Dissectionisk factors for AoD include conditions that result in aorticedial degeneration or place extreme stress on the aortic wallable 9). Two thirds to three quarters of patients havepertension, which is often uncontrolled. Genetic predispo-
tion (see Section 5) to AoD can occur in the context of androme, such as Marfan syndrome or Loeys-Dietz syn-ome, or can be inherited in families in the absence ofndromic features (3). IRAD data showed that of patientsder 40 years of age with AoD, 50% had a history of Marfanndrome (223). Other congenital or genetically based dis-ses as well as inflammatory conditions associated with agher risk of AoD are noted in Sections 6.3, 6.4, and 7.First and foremost, a family history of thoracic aorticeurysm is an important risk factor. In 2 separate clinical
udies, 13% to 19% of patients without an identified geneticndrome with thoracic aortic aneurysms had first-degreelatives with thoracic aortic aneurysms or AoD (127,130).he term “familial thoracic aortic aneurysm and dissectionndrome” is often applied (see Section 5). In taking a historyr thoracic aortic disease, one should be careful to distin-ish a history of an abdominal aortic aneurysm from aoracic aortic aneurysm. Many people, even healthcare
oviders, mistakenly use the terms AAA or triple A for anyrtic aneurysm, regardless of location. Clarifying that theeurysm was thoracic rather than abdominal affects one’snsideration of risk. Also, one must consider the potentialderlying diagnosis when a patient reports a family history“sudden death” or “heart attack” when there was no
nfirmatory autopsy. If the patient’s father, at the age of 45,d sudden onset of chest pain and then died moments later,ere is a chance that the death may have been from an acuteoD rather than an acute MI.The history may reveal syndromic causes of thoracic aorticeurysm and dissections, especially Marfan, Loeys-Dietz,d vascular Ehlers-Danlos syndromes. In some cases, pa-nts have only some of the features of Marfan or Loeys-
ietz syndrome, rather than the full-blown clinical syndrome,
Figure 21. Type B aortic dissection with mediasti-nal hematoma and pleural blood. Ruptured Type Baortic dissection with mediastinal hematoma (*)and pleural blood. Left, Flap arises in the proximaldescending thoracic aorta, with faint contrast-en-hanced blood adjacent to the site of rupture out-side the confines of the aortic wall (arrow). Right,At the level of the aortopulmonary window. FL in-dicates false lumen; PL, pleural blood; and TL, truelumen.
ble 9. Risk Factors for Development of Thoracicrtic Dissection
nditions associated with increased aortic wall stress
Hypertension, particularly if uncontrolled
Pheochromocytoma
Cocaine or other stimulant use
Weight lifting or other Valsalva maneuver
Trauma
Deceleration or torsional injury (e.g., motor vehicle crash, fall)
Coarctation of the aorta
nditions associated with aortic media abnormalities
Genetic
Marfan syndrome
Ehlers-Danlos syndrome, vascular form
Bicuspid aortic valve (including prior aortic valve replacement)
Turner syndrome
Loeys-Dietz syndrome
Familial thoracic aortic aneurysm and dissection syndrome
Inflammatory vasculitides
Takayasu arteritis
Giant cell arteritis
Behcet arteritis
Other
Pregnancy
Polycystic kidney disease
Chronic corticosteroid or immunosuppression agent administration
Infections involving the aortic wall either from bacteremia or extensionof adjacent infection

soprofpiaoadm
8.ATthtominsu
8.AO
PafaAcogaco8asof(2rito(5quPare
sidiorIRfrdeAreabaomanSochrepaloclin458%
(2paofwpapaw
8.PeofcotiomnidiorexOemcobyfadile
iscriswcono
Ta(IRAo
Pr
Hy
No
Hy
Sh
Ca
M
Pu
Pe
Ce
Isc
Isc
Isc
Co
Co
Fir
Fir
e62 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
a history of any phenotypic features, such as mitral valveolapse or pectus excavatum, should prompt considerationthoracic aortic aneurysms or dissections (224,225). Bicus-
d aortic valve is a strong risk factor for ascending thoracicrtic aneurysms, as well as coarctation of the aorta. Indition, a history of extreme exertion or emotional distressay preceed the onset of pain (226).
1.4. Clinical Presentation of Acute Thoracicortic Dissectionhe clinical presentation of acute AoD spans a spectrum frome overt with classic pain and physical examination findings
the enigmatic as a painless process with few physicalanifestations of the disease (Table 10). Given its exceed-gly high mortality, clinicians must maintain a high index ofspicion for acute AoD, as noted in Section 8.6 (Figure 22).
1.4.1. SYMPTOMS OF ACUTE THORACIC
RTIC DISSECTION
tients with acute aortic syndromes often present in a similarshion, regardless of whether the underlying condition isoD, IMH, PAU, or contained aortic rupture. Pain is the mostmmonly reported presenting symptom of acute AoD re-rdless of patient age, sex, or other associated clinicalmplaint (228–235). Pooled data from over 1000 patients instudies found that the pain of acute dissection is perceivedabrupt in onset in 84% of cases (95% CI 80% to 89%) andsevere intensity in 90% of cases (95% CI 88% to 92%)
36). Although classically described as having a tearing orpping quality, registry data suggest patients are more likely
describe the pain of acute dissection as sharp or stabbing1% to 64%, respectively) and that report of a migratingality to pain is highly variable (12% to 55%) (228,236).in may subsequently ease or abate, leading to a false
ble 10. International Registry of Acute Aortic DissectionAD) Physical Findings of 591 Patients With Type Artic Dissection
esenting Hemodynamics and Clinical Findings Frequency/Finding
pertensive 32%
rmotensive 45%
potensive 14%
ock 13%
rdiac tamponade 5%
urmur of aortic insufficiency 45%
lse deficits 26%
ricardial friction rub 2%
rebrovascular accident 8%
hemic peripheral neuropathy 3%
hemic spinal cord damage 2%
hemic lower extremity 10%
ma/altered consciousness 12%
ngestive heart failure 5%
st blood pressure systolic, mean 130 mm Hg
st blood pressure diastolic, mean 75 mm Hg
Adapted from Pape et al (227).
assurance on the part of the patients and physicians. th
Pain location and other associated symptoms reflect thete of initial intimal disruption and may change as thessection extends along the aorta or involves other arteries organ systems (236). Data from 464 patients enrolled inAD found that patients with Type A dissections most
equently present with chest pain (80%), more commonlyscribed as anterior (71%) than as posterior (32%) (228).lthough less common, patients with Type A dissectionport back pain (47%) and abdominal pain (21%), presum-ly as a result of antegrade dissection into the descendingrta (228). In contrast, patients with Type B dissections areost likely to present with back pain (64%) followed by chestd abdominal pain (63% and 43%, respectively) (228).me patients present with abdominal pain in the absence ofest pain or with only painful or numb lower extremitieslated to end-organ ischemia. In 1 retrospective study of 44tients ultimately diagnosed with acute thoracic AoD, thecation of the patient’s pain was highly predictive of theinician’s suspicion for acute AoD; dissection was suspected86% of patients who presented with chest and back pain,% of those who presented with chest pain alone, and only
of those primarily abdominal pain (237).
Although uncommon, acute AoD may present without pain38–240). In a separate analysis of 977 IRAD patients, 63tients (6.4%) presented without pain (241,242). This grouppatients was noted to be older and more likely to present
ith syncope, stroke, or congestive heart failure than weretients with painful dissection (241). Patients on steroids andtients with Marfan syndrome may be more prone to presentithout pain (243).
1.4.2. PERFUSION DEFICITS AND END-ORGAN ISCHEMIA
rfusion deficits as a result of dissection-related obstructionaortic branch vessels have long been recognized as a
mmon clinical manifestation, resulting in organ complica-ns at initial presentation (Table 11). End-organ involve-
ent in acute thoracic AoD can occur via several mecha-sms. Most occlusions are caused by obstruction by thessection flap, which can either prolapse across a vesseligin without entering it (dynamic obstruction) or directlytend into a vessel (static obstruction) (244) (Figure 18).ther causes include postobstructive arterial thrombosis,bolism to branches of either the true or false lumen, direct
mpression of an aortic branch artery or adjacent structuresan expanding false lumen (245), rupture or leakage of the
lse lumen into contiguous structures, and occlusion orssection of coronary arteries and/or aortic valve distortionading to heart failure.
Physical examination is insensitive to renal and mesentericchemia early in the course of acute AoD. Elevated serumeatinine or refractory hypertension may be due to renalchemia but may represent the clinical baseline in a patientith poorly documented or inadequately treated prior medicalnditions. Serologic markers of mesenteric ischemia mayt be present until hours after onset.
Combined data from over 1500 patients in 16 studies found
at pulse deficits were present in 31% of cases (95% CI 24%
to(pprpawanco(2nu
exisdiascaasisca
Fidies
e63JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
39%) and, when present, were strongly suggestive of AoDositive likelihood ratio 5.7; 95% CI 1.4 to 23) (37) andedict increased risk. Of 513 cases of Type A dissection,tients with perfusion deficits were more likely to presentith hypotension, shock, neurologic deficits, and tamponaded were more likely to have higher rates of hospitalmplications and mortality (41% versus 25%, P�0.0002)46). Furthermore, overall mortality rates correlated with the
gure 22. Acute surgical management pathway for AoD. *Additionssection; CABG, coronary artery bypass graft surgery; CAD, coroophageal echocardiogram.
mber of pulse deficits present, likely as a reflection of the pa
tent of vascular compromise and associated end-organchemia (246). Similarly, of 118 patients with Type A acutessection, limb ischemia (defined as loss of pulse withsociated pain and neurologic symptoms) was present in 38ses (32%) (247). The presence of limb ischemia wassociated with an increased likelihood of other end-organchemia (i.e., cerebral, visceral, or coronary) and a signifi-nt increase in overall mortality (247). Among the 38
appropriate’ based on Patel et al. (226a) AoD indicates aorticrtery disease; TAD, thoracic aortic disease; and TEE, trans-
of ‘ifnary a
tients with limb ischemia, in-hospital mortality was 45%

com
addiEhaofvenefu
8.TAenrere
8.Acaridipenafadivaprthclaonafa
8.Mco
thto98prCfasi(2
drabinth
8.HfosecitaAprTinthmcoth(2
8.PeT(3thspef(2peheadacpoinca(2
8.Syocmsecabl(e(e(2seIn
Ta
Ty
Ca
Ne
Pu
Ga
Re
Ex
e64 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
mpared with 15% among the 61 patients without organalperfusion (247).
These studies underscore the clinical importance of anequate vascular examination to help both identify thesease and stratify risk once the diagnosis is established.very patient being evaluated for possible acute AoD shouldve pulses checked in all extremities to identify the presenceperfusion deficits. In patients with acute limb ischemia
rsus those without, renal and mesenteric malperfusion werearly 2-fold more frequent and mortality was twice as high,rther highlighting the importance of this finding (248).
1.5. Cardiac Complicationshe heart is the most frequently involved end organ in acuteoD involving the ascending aorta. In distinction to otherd-organ pathology, most cardiac complications are a directsult of dissection-related disruption of normal anatomiclationships (215,245).
1.5.1. ACUTE AORTIC REGURGITATION
cute aortic regurgitation is the most commonly recognizedrdiac complication of Type A dissection (228–234), occur-
ng in 41% to 76% of cases (228–232). Three distinctssection-related mechanisms for acute aortic valve incom-tence have been identified, and they can occur in combi-tion: 1) acute dilatation of the aortic root by an expandinglse lumen, resulting in incomplete aortic valve closure; 2) assection extending into the aortic root and disrupting aorticlve commissural attachments, resulting in valve leafletolapse; and 3) a portion of dissection flap prolaping throughe aortic valve in diastole, preventing adequate leafletosure (235). Clinical manifestations of dissection-relatedrtic regurgitation span the spectrum from only a hemody-mically insignificant diastolic murmur to congestive heartilure and cardiogenic shock (236,249).
1.5.2. MYOCARDIAL ISCHEMIA OR INFARCTION
yocardial ischemia or infarction is an infrequent but serious
ble 11. End-Organ Complications of Acute Aortic Dissection
pe End-Organ Complication
rdiovascular Aortic insufficiency
Syncope
Pericardial tamponade
Myocardial ischemia or infarction
Congestive heart failure
urologic Ischemic stroke or transient ischemic attack
Peripheral neuropathy
Paraplegia/paraparesis
Spinal ischemia
lmonary Pleural effusion
Aortopulmonary fistula with hemorrhage
strointestinal Mesenteric ischemia or infarction
Aortoenteric fistula with hemorrhage
nal Renal failure
Renal ischemia or infarction
tremities Limb ischemia
mplication of acute AoD. Registry and review data suggest of
at ECG evidence of myocardial ischemia was present in up19% of patients with acute AoD, whereas pooled data from8 patients in 9 different studies found that acute MI wasesent in 7% of cases (95% CI 4% to 14%) (37,47,250).oronary artery flow can be compromised by an expandinglse lumen compressing the proximal coronary or by exten-on of the dissection flap into the coronary artery ostium51).
Clinically, a dissection-related cardiac malperfusion syn-ome may present with ECG changes that are indistinguish-le from those of primary myocardial ischemia or infarction,creasing the likelihood of misdiagnosis and inappropriateerapeutic intervention (252).
1.5.3. HEART FAILURE AND SHOCK
eart failure is a relatively uncommon complication of AoD,und to occur in approximately 6% of cases (236). In thistting, heart failure may result from acute aortic insuffi-ency, acute myocardial ischemia or infarction, or cardiacmponade. Registry data suggest that patients with acuteoD complicated by heart failure are often atypical in theiresentation, frequently leading to a delay in diagnosis (236).he largest study to evaluate heart failure in acute AoDcluded 1069 patients from the IRAD database and foundat patients with AoD and concomitant heart failure wereore likely to present in shock but were less likely tomplain of chest pain and that, when chest pain was present,e pain was more often mild and less often abrupt in onset36).
1.5.4. PERICARDIAL EFFUSION AND TAMPONADE
ricardial pathology is a frequent complication of acuteype A AoD and can occur via 2 distinct mechanisms7,253–256). Most commonly, transudation of fluid acrosse thin wall of an adjacent false lumen into the pericardialace leads to a hemodynamically insignificant pericardialfusion (256), which is present in about one third of patients57). Less often, the dissected aorta ruptures directly into thericardium, leading rapidly to tamponade physiology andmodynamic compromise (245,258,259). Cardiac tampon-e is diagnosed in 8% to 10% of patients presenting withute Type A AoD and is an ominous clinical predictor ofor outcomes (260), as well as the leading cause of mortalitythis group (47,215,231). Consequently, the presence of
rdiac tamponade should prompt truly urgent aortic repair60).
1.6. Syncopencope is a well-recognized dissection-related complaintcurring in approximately 13% of cases (242,261) withultiple potential etiologies, including: 1) cardiac (e.g.,vere aortic regurgitation, ventricular outflow obstruction,rdiac tamponade), 2) vascular (e.g., impaired cerebralood flow and aortic baroreceptor activation); 3) neurologic.g., vasovagal in response to pain), and 4) volume-related.g., false lumen rupture into the pleural space) causes40,261–267). Regardless of its etiology, syncope in thetting of AoD increases the risk of near-term adverse events.a review of 728 cases of acute AoD, patients with a history
syncope were significantly more likely to die than were
thPsystis
8.Aropadi17tecowprha37se
spmpa
sypapltr
8.Plofwfrtyto
didem27profanty
8.Mcoercaisnoofeaissabeac
streblheluthshbl
8.BinhyhaveneHaoisfa10adplde
coarintode
8.A95palemorpaabtaoffoto(mnibepa
Inw6paprfanohi
e65JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
ose without syncope (34% versus 23%, respectively;�0.01) (242). Additionally, patients who presented withncope more frequently had associated cardiac tamponade,roke, decreased consciousness, and evidence of spinal cordchemia (242).
1.7. Neurologic Complicationscute AoD frequently presents with dissection-related neu-logic complications. Pooled data from more than 1300tients in 13 studies that included both Type A and Bssections found that neurologic symptoms were reported in% (37). Neurologic complications may result from hypo-
nsion, malperfusion, distal thromboembolism, or nervempression (251,253,254). In a recent study of 102 patientsith Type A AoD, 29% had neurologic symptoms on initialesentation (253); of those with neurologic symptoms, 53%d ischemic stroke (predominantly right hemispheric) and% had ischemic neuropathy (described as limb pain withnsory or motor deficit) (253).Last, although uncommon, acute paraplegia as a result ofinal cord malperfusion has been described as a primaryanifestation of thoracic AoD, occurring in 1% to 3% oftients (215,251,253,254,268,269).Of clinical note, up to 50% of dissection-related neurologicmptoms may be transient and as many as one-third oftients with neurologic symptoms present without com-aints of chest pain, complicating appropriate diagnosis andeatment (253,255,256,262,269–271).
1.8. Pulmonary Complicationseural effusion, the most common pulmonary complicationacute AoD, is noted in 16% of cases at presentation (37);
hereas large effusions may result from leaking of bloodom the aorta into the pleural space, small effusions arepically a nonhemorrhagic exudate believed to be inflamma-ry in origin (37,272–275).Other pulmonary complications of acute AoD include
ssection-related compression of the pulmonary artery andvelopment of an aortopulmonary fistula, either of whichay present with dyspnea as a prominent symptom (276–8). Hemoptysis, noted in 1 study in 3% of patientsesenting with thoracic AoD, may result from compressionlung parenchyma by an expanding false lumen or via directeurysmal rupture into the lung, leading to massive hemop-sis and death (215,279,280).
1.9. Gastrointestinal Complicationsesenteric ischemia is the most common gastrointestinalmplication of acute AoD (228) and can result from malp-fusion or systemic hypotension. It is the most commonuse of death among those with Type B AoD. Mesentericchemia is associated with abdominal pain, but pain may benspecific and out of proportion to the physical examinationthe abdomen, so the cause of pain often goes unrecognizedrly on. Unfortunately, by the time serum markers of bowelchemia or infarction turn positive, it is often too late tolvage the bowel or the patient. Therefore, it is essential to
viligant for mesenteric ischemia in every patient with
ute AoD and associated abdominal pain. mGastrointestinal hemorrhage is a rare but potentially cata-rophic complication of acute AoD (281–283). Dissection-lated gastrointestinal bleeding may present with limitedeeding as a result of mesenteric infarction or as massivemorrhage secondary to an aortoesophageal fistula or falsemen rupture into proximal small bowel (281–283). Al-ough rare, dissection-related gastrointestinal hemorrhageould be in the differential of all patients presenting witheeding and complaints of thoracic or abdominal pain.
1.10. Blood Pressure and Heart Rate Considerationslood pressure abnormalities are common in patients present-g with acute thoracic AoD. About half of patients arepertensive at presentation, with 71% of Type B patientsving a systolic blood pressure greater than 150 mm Hgrsus only 36% of Type A patients (284–287). Conversely,arly 20% present with either hypotension or shock (37).ypotension and shock can result from cardiac tamponade,rtic hemorrhage, severe aortic insufficiency, myocardial
chemia or infarction, true lumen compression by distendedlse lumen, or an intra-abdominal catastrophe. Of more than00 patients with acute AoD, those with hypotension onmission were found more likely to have neurologic com-ications; myocardial, mesenteric, or limb ischemia; andath (249).Accurate systemic blood pressure measurement may bemplicated by dissection-related occlusion of aortic branchteries, resulting in erroneously low blood pressure readingsthe affected limb. Accordingly, blood pressures may needbe measured in both arms and, at times, both legs to
termine the highest central blood pressure.
1.11. Age and Sex Considerationscute AoD presentation varies with patient age and sex. In1 IRAD patients, 7% were younger than 40 years. Com-red with patients 40 years of age and older, this group wasss likely to have a history of hypertension and significantlyore likely to have Marfan syndrome, bicuspid aortic valve,a history of prior aortic surgery (223). Clinically, young
tients in this study were more likely to describe pain asrupt in onset but less likely to be hypertensive at presen-tion (25% versus 45%) (223). In contrast, a separate studyIRAD data evaluating 550 patients with Type A dissection
und that among patients more than 70 years of age (32% oftal), typical symptoms (abrupt onset of pain) and signsurmur of aortic regurgitation or pulse deficits) were sig-
ficantly less common, suggesting that extra vigilance mayrequired to identify acute AoD in young and elderly
tients (288).Sex appears to affect the presentation of acute AoD as well.a study of 1078 patients enrolled in IRAD, 32% were
omen. Women were older; were less likely to present withinhours of symptom onset, to complain of abrupt onset ofin, and to have a pulse deficit; and were more likely toesent with either altered mental status or congestive heartilure. Consequently, women were less likely to be diag-sed within 24 hours of symptom onset and had significantlygher in-hospital mortality (30% versus 21%, P�0.001) than
en (289).
8Aco29imorrhtharreresi(6acIM
aowth
frcigrtewan(2inprlufu
suIMlucocoinbaao
endiTanaomIMblshsiin(2asindi(2wclotan90
Filearwto mputed
e66 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
.2. Intramural Hematomamong acute aortic syndromes, acute dissection is the mostmmon, but approximately 10% to 20% of patients (290–2) with a clinical picture of dissection exhibit an IMH viaaging without identification of blood flow in a false lumenan intimal lesion. Some believe IMH arises from hemor-
age of the vasa vasorum located within the medial layer ofe aorta (293,294), whereas others argue that the hematomaises from microscopic tears in the aortic intima. Thesulting hematoma may then propagate in an antegrade or atrograde manner, producing symptoms that may be impos-ble to differentiate clinically from those of a classic AoD1). IMH has a variable radiologic appearance (Figure 23)cording to the area of the aorta involved. In some cases,H may be associated with a PAU (see Section 8.2 or 8.3).Clinically, IMH most commonly occurs in the descendingrta and in older patients. Pain is characteristic of IMH,hereas malperfusion and pulse deficit are much less likelyan with classic AoD (295,296).Imaging criteria of IMH are based on the appearance of
esh thrombus in the aortic wall. These include crescentic orrcular thickening of the aortic wall with maximal thicknesseater than or equal to 7 mm on TEE without intimal flap orar or longitudinal flow in the false lumen. The thickenedall has a higher tissue density than unenhanced blood on CTd is without enhancement after contrast on the CT/MR90,296–298). When the term IMH is used strictly, notimal defect such as a tear or an ulcer is present. But inactice, the term is used loosely to mean a thrombosed falsemen regardless of a small intimal defect. The distinction is
gure 23. Intramural hematoma demonstrated as a low-attenuatioft, Axial image at the level of the aortic arch. Top middle, Througtery with narrowing of the aortic lumen. Bottom left, Oblique sagithout the use of ECG gating). Bottom right, Coronal reformattedma, and an incidental infarenal aortic aneurysm. CT indicates co
rther blurred by the facts that the intimal defect may be tiv
btle and difficult to exclude and that some patients withH begin with a CT scan that shows a thrombosed false
men with no apparent intimal defect and then over theurse of 1 or 2 months develop 1 or more distinct ulcerlikemmunications (299,300). Because of this overlap in imag-g findings, it is difficult and perhaps somewhat arbitrary tose treatment on the appearance of the CT snapshot of therta in its disease progression.The natural history of IMH is variable. The hematoma maytirely resolve (10%) (301), it may convert to a classicssection, or the aorta may enlarge and potentially rupture.he clinical behavior of IMH varies according to the locationd mimics that of classic AoD. IMH involving the ascendingrta has a high, early risk of complication and death withedical treatment alone, and surgery is usually indicated.H involving the descending aorta may be treated with
ood pressure control, and the use of beta blockers has beenown to improve the long-term survival rate (296). Conver-on of the IMH to a more classic picture of dissection occurs
3% to 14% of cases involving the descending aorta97,298,302,303) and in 11% to 88% of cases involving thecending aorta (302–305), with that figure increasing withcreased length of follow-up. Progressive increase in aorticameter has been demonstrated by serial imaging studies98,306). In 1 study, the mortality after 2 years of patientsith acute proximal Type A IMH versus that of patients withassic dissection was not significantly different (307). An-her group found improved actuarial survival rates at 1, 2,d 5 years in patients with IMH versus classic dissection:%, 90%, and 90% versus 67%, 66%, and 62%, respec-
d of hematoma (arrows) in the aortic wall on CT images. Topid thorax. Top right, At the level of the superior mesenteric
ormatted image through the thorax (note band artifact evidentthrough the abdomen demonstrate the length of the hema-tomographic imaging; and ECG, electrocardiogram.
n banh the mittal refimage
ely, for Type A (304), and 100%, 97%, and 97% versus

83alfoasth
8PApefoleveincoratamhaba(udibucoemfoin
euanbyofdicousrese(2
8PstoveAmaf
fope“npo(mpsussi
8Atharuarthonaninw
riauthaoao
thhife(3
x-fogadi(4dublteusbeesul
e67JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
%, 79%, and 79%, respectively, for Type B (297). Song etalso described increased risk for complications or mortalityr patients with IMH involving the ascending aorta whencending aortic diameter is greater than 4.8 cm or IMHickness is greater than 11 mm (308).
.3. Penetrating Atherosclerotic UlcerU refers to an atherosclerotic lesion with ulceration that
netrates the internal elastic lamina and allows hematomarmation within the media of the aortic wall (309). Thission sets the stage for development of IMH, AoD, or frankssel rupture (309) (Figure 24). Anatomically PAUs developaortic segments where atherosclerotic changes are most
mmon and therefore are localized to the descending tho-cic aorta in over 90% of cases (310). When viewedngentially, the classic appearance of the lesion is aushroom-like outpouching of the aortic lumen with over-nging edges, resembling a gastric ulcer, as depicted on arium study (Figure 24). The typical patient is elderlysually over 65 years of age) and has hypertension andffuse atherosclerosis, who presented with chest or back paint without signs of aortic regurgitation or malperfusion. Lessmmonly, patients presented only with signs of distalbolization (311). Asymptomatic patients may also be
und with aortic lesions that are indistinguishable, by imag-g criteria, from PAUs (310,311).Two entities can mimic PAUs. A branch artery pseudoan-rysm represents a small collection of flowing blood withinotherwise thrombosed aortic false lumen, which is createdan injury to a small branch artery during the propagationthe IMH (312). These are usually incidental findings, are
stinguished from ulcers by the apparent absence of ammunication with the aortic lumen by CT, and do notually require specific treatment. A dissection entry orentry tear may develop in an area of IMH as detected byveral imaging studies over a period of several months97,299,300,306).
.4. Pseudoaneurysms of the Thoracic Aortaeudoaneurysms of the thoracic aorta are frequently relateddeceleration or torsional trauma to the aorta from motorhicle accidents, falls, and sports injuries (3,313–319).ortic pseudoaneurysms are relatively rare, with posttrau-atic pseudoaneurysms having an incidence of 3% to 4%
ter blunt trauma (51). Other pseudoaneurysms may occur callowing aortic surgery, catheter-based interventions, ornetrating trauma. Pseudoaneurysms often have a slimeck” that leads to the “aneurysm” that corresponds toints of penetration and containment (320). Aortic infectionsycotic aneurysms) and penetrating ulcers may also result ineudoaneurysms (see Section 9.2.2). Penetrating injuries areually repaired immediately whenever recognized and fea-ble (317,318,321).
.5. Traumatic Rupture of the Thoracic AortaUK survey of all motor vehicle accident fatalities found
at approximately 20% of patients had an autopsy finding ofruptured aorta, emphasizing the importance of traumaticpture of the aorta (TRA). In the United States, there areound 40 000 motor vehicle deaths annually, and it is likelyat around 8000 of the victims had TRA. It is estimated thatly 9% to 14% of patients with TRA reach a hospital alived only 2% ultimately survive. In this survey, 29% werevolved with frontal impact crashes and 44% were involvedith side impact crashes (318,319).Parmley and colleagues (318) noted the correlation of high
sk of early death and the sites of TRA on the basis oftopsies in 275 deaths from unrelated aortic rupture. In 45%,e tear was at the aortic isthmus; 23%, in the ascendingrta; 13%, in the descending aorta; 8%, in the transverserta; 5%, in the abdominal aorta; and 6%, multiple sites.Examination of the patient usually reveals signs similar toose of coarctation of the aorta with arm blood pressuregher than leg blood pressure, delay between radial versusmoral artery pulsation, and a harsh interscapular murmur). Evidence of polytrauma is, however, common.The best method for detection of a TRA is debated. A chestray with a nasogastric tube in position has 80% sensitivityr suggesting TRA by showing displacement of the naso-stric tube by the hematoma. However, signs of hemome-astinum are more often false positive than true positive0). Even when present, mediastinal blood is less likely to bee to arterial/aortic injury than to less-consequential venouseeding. A biplane contrast aortogram may fail to detect thear until the development of a pseudoaneurysm. TEE may beed, but if dilatation has not occurred, the diagnosis may still
in doubt. CT is used but is not absolutely certain totablish the diagnosis. In questionable cases, intravasculartrasound can also be used (3,322,323) (Figure 8). Realisti-
Figure 24. Penetrating atherosclerotic ulcer of theproximal descending thoracic aorta. Axial CT im-ages at the level of the aortopulmonary window(left) and at the level of the left pulmonary artery(right) demonstrate a small penetrating ulcer (longarrow, U) that extends beyond the expected con-fines of the aortic lumen with adjacent IMH both atthe level of the ulcer itself and that extends a fewcentimeters caudally in the wall of the descendingthoracic aorta (short arrows). CT indicates com-puted tomographic imaging; IMH, intramural he-matoma; and U, penetrating ulcer.
lly, the imaging sequence often depends on the stability of

thinthte
8Th
8.
8.RI
CL
1.
2.
3.
4.
5.
6.
8.SeutmClare
aclyserefibrepu
scineiofAseAfrIM(3
behestnoshmprfoCityva“preaslu
e68 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
e patient and the need for the diagnosis of concomitantjuries. Sometimes, this may even fail to detect the tear, ande study may have to be repeated at a later date to detect thear.
.6. Evaluation and Management of Acuteoracic Aortic Disease
6.1. Initial Evaluation and Management
6.1.1. RECOMMENDATIONS FOR ESTIMATION OF PRETEST
SK OF THORACIC AORTIC DISSECTION
ASS I
Providers should routinely evaluate any patient presenting withcomplaints that may represent acute thoracic aortic dissectionto establish a pretest risk of disease that can then be used toguide diagnostic decisions. This process should include spe-cific questions about medical history, family history, and painfeatures as well as a focused examination to identify findingsthat are associated with aortic dissection, including:a. High-risk conditions and historical features (47,127,223,
261) (Level of Evidence: B):• Marfan syndrome, Loeys-Dietz syndrome, vascular
Ehlers-Danlos syndrome, Turner syndrome, or other con-nective tissue disease.
• Patients with mutations in genes known to predisposeto thoracic aortic aneurysms and dissection, such asFBN1, TGFBR1, TGFBR2, ACTA2, and MYH11.
• Family history of aortic dissection or thoracic aorticaneurysm.
• Known aortic valve disease.• Recent aortic manipulation (surgical or catheter-based).• Known thoracic aortic aneurysm.
b. High-risk chest, back, or abdominal pain features (37,47,215,223,261,264,288) (Level of Evidence: B):• Pain that is abrupt or instantaneous in onset.• Pain that is severe in intensity.• Pain that has a ripping, tearing, stabbing, or sharp
quality.c. High-risk examination features (37,47,253,257,261,324)
(Level of Evidence: B):• Pulse deficit.• Systolic blood pressure limb differential greater than 20
mm Hg.• Focal neurologic deficit.• Murmur of aortic regurgitation (new).
Patients presenting with sudden onset of severe chest, back,and/or abdominal pain, particularly those less than 40 years ofage, should be questioned about a history and examined forphysical features of Marfan syndrome, Loeys-Dietz syndrome,vascular Ehlers-Danlos syndrome, Turner syndrome, or otherconnective tissue disorder associated with thoracic aorticdisease. (223) (Level of Evidence: B)Patients presenting with sudden onset of severe chest, back,and/or abdominal pain should be questioned about a history ofaortic pathology in immediate family members as there is astrong familial component to acute thoracic aortic disease.(223) (Level of Evidence: B)Patients presenting with sudden onset of severe chest, back,
and/or abdominal pain should be questioned about recent seaortic manipulation (surgical or catheter-based) or a knownhistory of aortic valvular disease, as these factors predisposeto acute aortic dissection. (Level of Evidence: C)In patients with suspected or confirmed aortic dissection whohave experienced a syncopal episode, a focused examinationshould be performed to identify associated neurologic injury orthe presence of pericardial tamponade (see Section 8.1.6).(Level of Evidence: C)All patients presenting with acute neurologic complaintsshould be questioned about the presence of chest, back,and/or abdominal pain and checked for peripheral pulse defi-cits as patients with dissection-related neurologic pathologyare less likely to report thoracic pain than the typical aorticdissection patient (253) (see Section 8.1.7). (Level of Evi-dence: C)
6.1.2. LABORATORY TESTING
veral plasma markers have been investigated for theirility in the evaluation of acute AoD. Plasma smooth muscleyosin heavy chain protein, D-dimer, and high-sensitivity-reactive protein have shown diagnostic promise, although ack of large prospective studies precludes a recommendationgarding their use (325–328).
Elevation of D-dimer levels occurs with intravasculartivation of the coagulation cascade and secondary fibrino-sis and in conditions such as venous thromboembolism,psis, disseminated intravascular coagulation, malignancies,cent trauma or surgery, and acute MI and followingrinolytic therapy. The ACEP has published guidelines
garding the use of certain D-dimer assays to rule outlmonary embolism in low-risk patients (329).
Regarding the potential role of plasma D-dimer levels toreen for AoD, significant elevations of D-dimer were seenall 24 patients with documented acute AoD involving
ther the ascending or descending thoracic aorta regardlesstime from presentation, ranging from 1 to 120 hours (325).meta-analysis of 11 studies (330) noted that the pooled
nsitivity of D-dimer in 349 patients with documented acuteoD was 94% (95% CI 91% to 96%) with specificity rangingom 40% to 100%. Two patients had limited ascending aortic
H without intimal flap and had negative D-dimer assays31).
Some authors (325,332) recommend that D-dimer assaysperformed in all patients where clinical suspicion exists, tolp identify those who do not require definitive imaging
udies. However, the efficacy and safety of this strategy havet been tested in a large clinical trial, and several caveatsould apply. The negative likelihood ratio provided by theost sensitive D-dimer assay is not of sufficient magnitude toovide useful information in high-risk individuals and there-re cannot be used to “rule out” the disease in this group.linical scoring systems to identify the true pretest probabil-
for AoD in individual patients have not been developed orlidated, thus limiting an accurate determination of the trueosttest” probability associated with a negative D-dimersult. Finally, there are reports of negative D-dimer assayssociated with ascending aortic IMH or a thrombosed falsemen, such that further studies are needed regarding the
nsitivity of D-dimer levels to detect the presence of IMH or
PAreev
lacoan
8.CL
1.
2.
3.
CL
1.
8.IM
CL
1.
2.
8.CL
1.
CL
1.
8.CL
1.
2.
3.
EinAthim
1.
e69JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
U (331). Given these issues, the writing committee cannotcommend serum D-dimer screening for all patients beingaluated for AoD.
Where a high level of suspicion for acute AoD exists,boratory testing aimed at presurgical screening (bloodunt, serum chemistries, coagulation profiles, and blood typed screen) may reduce preoperative delays.
6.1.3. RECOMMENDATIONS FOR SCREENING TESTS
ASS I
An electrocardiogram should be obtained on all patients whopresent with symptoms that may represent acute thoracicaortic dissection.a. Given the relative infrequency of dissection-related coro-
nary artery occlusion, the presence of ST-segment eleva-tion suggestive of myocardial infarction should be treatedas a primary cardiac event without delay for definitiveaortic imaging unless the patient is at high risk for aorticdissection. (37,47,333) (Level of Evidence: B)
The role of chest x-ray in the evaluation of possible thoracicaortic disease should be directed by the patient’s pretest riskof disease as follows:a. Intermediate risk: Chest x-ray should be performed on all
intermediate-risk patients, as it may establish a clearalternate diagnosis that will obviate the need for definitiveaortic imaging. (Level of Evidence: C)
b. Low risk: Chest x-ray should be performed on all low-riskpatients, as it may either establish an alternative diagnosisor demonstrate findings that are suggestive of thoracicaortic disease, indicating the need for urgent definitiveaortic imaging. (Level of Evidence: C)
Urgent and definitive imaging of the aorta using transesoph-ageal echocardiogram, computed tomographic imaging, ormagnetic resonance imaging is recommended to identify orexclude thoracic aortic dissection in patients at high risk forthe disease by initial screening. (42–46,67,73) (Level ofEvidence: B)
ASS III
A negative chest x-ray should not delay definitive aortic imag-ing in patients determined to be high risk for aortic dissectionby initial screening. (Level of Evidence: C)
6.1.4. RECOMMENDATIONS FOR DIAGNOSTIC
AGING STUDIES
ASS I
Selection of a specific imaging modality to identify or excludeaortic dissection should be based on patient variables andinstitutional capabilities, including immediate availability.(Level of Evidence: C)If a high clinical suspicion exists for acute aortic dissection butinitial aortic imaging is negative, a second imaging studyshould be obtained. (212) (Level of Evidence: C)
6.1.5. RECOMMENDATIONS FOR INITIAL MANAGEMENT
ASS I
Initial management of thoracic aortic dissection should bedirected at decreasing aortic wall stress by controlling heart
rate and blood pressure as follows:a. In the absence of contraindications, intravenous betablockade should be initiated and titrated to a target heartrate of 60 beats per minute or less. (Level of Evi-dence: C)
b. In patients with clear contraindications to beta blockade,nondihydropyridine calcium channel-blocking agentsshould be used as an alternative for rate control. (Level ofEvidence: C)
c. If systolic blood pressures remain greater than 120 mm Hgafter adequate heart rate control has been obtained, thenangiotensin-converting enzyme inhibitors and/or other va-sodilators should be administered intravenously to furtherreduce blood pressure that maintains adequate end-organperfusion. (Level of Evidence: C)
d. Beta blockers should be used cautiously in the setting ofacute aortic regurgitation because they will block thecompensatory tachycardia. (5) (Level of Evidence: C)
ASS III
Vasodilator therapy should not be initiated prior to rate controlso as to avoid associated reflex tachycardia that may increaseaortic wall stress, leading to propagation or expansion of athoracic aortic dissection. (Level of Evidence: C)
6.1.6. RECOMMENDATIONS FOR DEFINITIVE MANAGEMENT
ASS I
Urgent surgical consultation should be obtained for allpatients diagnosed with thoracic aortic dissection regard-less of the anatomic location (ascending versus descending)as soon as the diagnosis is made or highly suspected. (Levelof Evidence: C)Acute thoracic aortic dissection involving the ascending aortashould be urgently evaluated for emergent surgical repairbecause of the high risk of associated life-threatening compli-cations such as rupture. (47) (Level of Evidence: B)Acute thoracic aortic dissection involving the descendingaorta should be managed medically unless life-threateningcomplications develop (i.e., malperfusion syndrome, progres-sion of dissection, enlarging aneurysm, inability to controlblood pressure or symptoms). (285,288,334–337) (Level ofEvidence: B)
arly identification of acute thoracic dissection is challeng-g. During the initial evaluation, the correct diagnosis ofoD has been made in only 15% to 43% of patients initiallyought to have the disease (215,237,252). Factors that maypede accurate diagnosis of AoD include the following:
Acute AoD is often believed to be a rare disease (2.9 to 3.5cases per 100 000 person-years) (215,217), whereas theincidence of acute MI is several orders of magnitudegreater (more than 200 cases per 100 000 person-years)(338). Data previously cited in this guideline from UHCsuggest that acute AoD is not “rare.” Some commonexplanations that clinicians give for this underlying beliefinclude the following:a. It is difficult for clinicians to effectively separate
patients with AoD from the multitude of other patients
who present to emergency departments and primary
2.
3.
4.
8.6ThpamathomaspewhmasuphisvasugorancatreqimAoreqprebealttio
incbe
presex22intea(47
25
codiacothoaltdeonpro
paan(24
thediathrdicforFigimlacthethe
mocotimersagwinoadean
ofmeadpapre
risaltuapayemaere
accInitoof
TeitieMR
e70 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
care physicians with common complaints that aremuch more often not due to acute AoD.
b. Front-line medical providers may have little directexperience with acute AoD and are unlikely to beaware of the subtleties of its presenting signs andsymptoms.
c. Institutional multidisciplinary pathways developed forother emergencies such as ST-elevation myocardialinfarction (STEMI) or acute stroke have not generallyexisted for acute AoD.
In contrast to other more common cardiovascular emer-gencies, acute AoD may occur in younger patients. Accu-rate identification of acute AoD; however, requires thatclinicians recognize on a routine basis that the disease maypresent in younger patients. Case reports exist of childrenas young as 3 years of age presenting with acute AoD(105).Acute AoD may present with a wide range of unusualmanifestations that do not conform with classic “textbookfindings.” (339–341)There are no well-studied, rapidly available, and effectivescreening tests for acute AoD.
.2. Evaluation and Management Algorithmse provided algorithms guide the initial evaluation oftients whose presentations are concerning for AoD and thenagement of patients in whom the diagnosis of acuteracic AoD is confirmed. Although clinicians may ulti-tely choose to deviate from the pathway for patient-cific reasons, the algorithms provide a framework withich to quickly diagnose (Figure 25) and provide earlynagement (Figure 26) of AoD. This decision model isported by several large studies that indicate a targetedtory and physical examination are likely to identify thest majority of patients who present with acute AoD,gesting that adequate screening need not be time intensive
technology dependent (47,215,264). Using a target historyd physical examination, patients can be placed into 1 of 3egories: 1) those with immediately apparent acute AoDuiring emergent surgical evaluation and expedited aorticaging, 2) those whose presentation is concerning for acuteD and in the absence of a clear alternative diagnosisuire expedited aortic imaging, and 3) those whose clinicalsentation is not initially suggestive of acute AoD but may
nefit from aortic imaging in the absence of a likelyernative diagnosis at the completion of the initial evalua-n.Several high-risk conditions (Figure 25, T2–1) greatlyrease the likelihood that presenting complaints that coulda result of acute AoD.Pain (Figure 25, T2–2) is the most commonly reportedsenting symptom of acute AoD regardless of patient age,, or other associated clinical complaint (37,47,215,
3,242,264,289). Pain described as abrupt or instantaneousonset, that is severe in intensity, or that has a ripping orring quality establishes a high pretest probability for AoD,261).
The combination of 2 or more high-risk features (Figure
, T3) is strongly suggestive of acute AoD. accThe presence of a single high-risk feature (i.e., high-riskndition, pain, or physical examination) may trigger imme-te concern for acute AoD; however, other diagnostic
nsiderations may exist. Pain with high-risk features, al-ugh suggestive of acute AoD, may occur as a result of an
ernate disease process (Table 12). For patients who aretermined to have an intermediate probability of acute AoD
the basis of initial bedside assessment, Figure 25, T4,vides a pathway for further evaluation.
Figure 25, T5, provides a pathway for further evaluation oftients without any high risk features. Delay in diagnosisd increased mortality is common in this group1,288,289).
For patients presenting with new ST-segment elevations oninitial ECG and without high-risk AoD features, imme-
te coronary angiography and reperfusion therapy (i.e.,ombolysis or percutaneous coronary intervention) are in-ated (333). However, if coronary angiography is per-med and no culprit coronary lesion is identified, thenure 25, T6, provides a pathway to dedicated aortic
aging. As approximately 40% of chest films in acute AoDk a widened mediastinum, and as many as 16% are normal,absence of radiographic abnormalities does not excludediagnosis of AoD (37,47) (Figure 25, T7).
Missed or delayed diagnosis of acute AoD is most com-nly ascribed to an incorrect working diagnosis of acute
ronary syndrome, a condition that may require a prolongede interval to correctly identify (i.e., serial cardiac biomark-) and whose management with antiplatlet and antithrombinents may cause harm to the patient with AoD. For patientsth an intermediate-risk profile for acute AoD and who dot have diagnostic STEMI but who are being evaluated forpossible acute coronary syndrome, aortic imaging maytect AoD prior to the administration of antiplatelet andtithrombin agents (Figure 25, T8).Unexplained hypotension is present in approximately 20%patients with acute AoD (37,47). Similarly, a wideneddiastinum on chest x-ray strongly suggests the need for
ditional definitive diagnostic aortic imaging, particularly intients without a clear alternative explanation for theirsenting complaint (342) (Figure 25, T9).Some patients with acute AoD present without any high-k features, making early diagnosis difficult. If a clearernative diagnosis is not established after the initial eval-tion, then obtaining a diagnostic aortic imaging study,rticularly in patients with advanced age (older than 70ars), syncope, focal neurologic deficit, or recent aorticnipulation (surgery or catheter based), should be consid-d (47,242,253,288,343) (Figure 25, T10).Multidetector CT with contrast, TTE, and MR all provideeptable diagnostic accuracy for the diagnosis of acute AoD.patients with hemodynamic instability, requiring close mon-ring, bedside TEE is preferred to avoid moving the patient outthe acute care environment (Figure 25, T11).The most recent comparative study with nonhelical CT, 0.5sla MR and TEE showed 100% sensitivity for all modal-s, with better specificity of CT (100%) than for TEE and
(44). A recent meta-analysis that evaluated the diagnostic
uracy of TEE, helical CT, and MR for suspected AoD
fodimin
tivAevocexst25
8.O(Ilimshw
8.Acobl
FineST ease; a
e71JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
und that all 3 imaging techniques provided equally reliableagnostic values (46). Accordingly, selection of an imagingodality is influenced by individual patient variables andstitutional capabilities.The diagnosis of acute AoD cannot be excluded defini-ely based on the results of a single imaging study.
lthough TEE, CT, and MR are all highly accurate for thealuation of acute AoD; false-negative studies can and docur (47) (Figures 9 and 15). If a high clinical suspicionists for acute AoD but initial aortic imaging is negative,
rongly consider obtaining a second imaging study (Figure
gure 25. AoD evaluation pathway. ACS indicates acute coronaryrvous system; CT, computed tomographic imaging; CXR, chestEMI, ST-elevation myocardial infarction; TAD; thoracic aortic dis
, T12). er
6.3. Initial Managementnce the diagnosis of AoD or one of its anatomic variantsMH or PAU) is obtained, initial management is directed at
iting propagation of the false lumen by controlling aorticear stress while simultaneously determining which patientsill benefit from surgical or endovascular repair (Figure 26).
6.3.1. BLOOD PRESSURE AND RATE CONTROL THERAPY
ortic wall stress is affected by the velocity of ventricularntraction (dP/dt), the rate of ventricular contraction, andood pressure. Initial medical stabilization using beta block-
ome; AoD, aortic dissection; BP, blood pressure; CNS, centralEKG, electrocardiogram; MR, magnetic resonance imaging;nd TEE, transesophageal echocardiogram.
syndrx-ray;
s controls these 3 parameters by reducing heart rate and

bladarbe
ishaw
puexalpoagvabl
FiTT
e72 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ood pressure to the lowest amounts that will still maintainequate end-organ perfusion (61). Reasonable initial targetse a heart rate less than 60 bpm and a systolic blood pressuretween 100 and 120 mm Hg (61).
Intravenous propranolol, metoprolol, labetalol, or esmololan excellent choice for initial treatment. In patients whove a potential contraindication to beta blockade (e.g., those
gure 26. Acute AoD management pathway. AoD indicates aorticE, transthoracic echocardiogram.
ith asthma, congestive heart failure, or chronic obstructive (v
lmonary disease), esmolol may be a viable option given itstremely short half-life. Use of labetalol, which is both anpha- and beta-receptor antagonist, offers the advantage oftent heart rate and blood pressure control from a singleent, potentially eliminating the need for a secondarysodilator. In patients who are unable to tolerate betaockade, nondihydropyridine calcium channel antagonists
tion; BP, blood pressure; MAP, mean arterial pressure; and
dissecerapamil, diltiazem) offer an acceptable, although less-

esdireaf
8.Itlemtioblestitanapprcraogaanhyplenreou
8.Atoblgeva
8.Mre
trapadfacrth
haasAthcodibydeththmer
supacafo
8.InmprStSevithm
8.ACL
1.
Wthofpodiaosa
8.Eth
TaEx
Ch
Ab
Ba
Pu
Fo
e73JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
tablished, alternative (61). Beta blockers, verapamil, orltiazem for rate control in patients with significant aorticgurgitation may be problematic because of deleteriousfects on reflex tachycardia.
6.3.2. ADDITIONAL ANTIHYPERTENSIVE THERAPY
is frequently difficult to reduce blood pressure to optimumvels (285–287,344–346). In 1 study, patients required aedian of 4 different antihypertensive drugs (347). In addi-n to beta blockade, vasodilators may be required to control
ood pressure. Intravenous sodium nitroprusside is the mosttablished agent and offers the advantage of being rapidlyratable (61). Nicardipine (348), nitroglycerin, fenoldopam,d various other intravenous antihypertensive agents arepropriate for this situation. Vasodilator therapy withoutior beta blockade may cause reflex tachycardia and in-eased force of ventricular contraction leading to greaterrtic wall stress and potentially causing false lumen propa-tion (42). Following initial stabilization with intravenoustihypertensives, most patients will require long-term anti-pertensive treatment including the use of a beta blockerus additional classes of agents. Angiotensin-convertingzyme inhibitors or angiotension receptor blockers maytard aortic dilatation and their use may be indicated astlined in Section 9.2.1.1.
6.3.3. PAIN CONTROL
dequate pain control is essential in the setting of acute AoDdecrease sympathetic mediated increases in heart rate and
ood pressure. Appropriate use of intravenous opiate anal-sia will help augment the effects of rate control andsodilator agents.
6.3.4. HYPOTENSION
edical management options for all forms of dissection-
ble 12. Differential Diagnosis for High-Risk Pain oramination Features
est pain
● Acute myocardial infarction
● Pulmonary embolism
● Spontaneous pneumothorax
● Esophageal rupture
dominal pain
● Renal/biliary colic
● Bowel obstruction/perforation
● Non–dissection-related mesenteric ischemia
ck pain
● Renal colic
● Musculoskeletal pain
● Intervertebral disk herniation
lse deficit
● Non–dissection-related embolic phenomena
● Non–dissection-related arterial occlusion
cal neurologic deficit
● Primary ischemic cerebrovascular accident
● Cauda equina syndrome
lated hypotension are limited. Volume administration ti- us
ated to improvement of blood pressure is a reasonable firstproach. Vasopressors can be added, if needed, to maintainequate perfusion but have the potential to cause furtherlse lumen propagation. Inotropic agents are likely to in-ease the force and rate of ventricular contraction anderefore increase sheer stress on the aortic wall.
Pericardiocentesis for dissection-related hemopericardiums been associated with recurrent pericardial bleeding andsociated mortality (307,349,350). Several articles from thesian literature suggest that pericardiocentesis may be safe ine setting of acute Type A IMH (351,352). Other cardiacmplications that may result in hypotension include severessection-related aortic regurgitation, true lumen obstruction
a compressing false lumen, and acute MI. All requirefinitive operative management. Hypotension or shock ine setting of AoD may also result from contained rupture ofe false lumen into adjacent structures (i.e., pleural space orediastinum), a scenario that also mandates immediate op-ative intervention.
Ultimately, hypotension or shock in the acute AoD patientggests the need for immediate operative management. Fortients with hemopericardium and cardiac tamponade whonnot survive until surgery, pericardiocentesis can be per-rmed by withdrawing just enough fluid to restore perfusion.
6.3.5. DETERMINING DEFINITIVE MANAGEMENT
the clinically stable patient, the decision for surgical versusedical management of patients with acute AoD is basedimarily on the location of the dissection as described by theanford and DeBakey classification systems (61,353) (seection 8.1.2). A prompt cardiac surgical consultation pro-des the best management resource, regardless of location ofe AoD, as it is impossible to predict which complicationsay develop or when they may occur.
6.4. Recommendation for Surgical Intervention forcute Thoracic Aortic DissectionASS I
For patients with ascending thoracic aortic dissection, all ofthe aneurysmal aorta and the proximal extent of the dissec-tion should be resected. A partially dissected aortic rootmay be repaired with aortic valve resuspension. Extensivedissection of the aortic root should be treated with aorticroot replacement with a composite graft or with a valvesparing root replacement. If a DeBakey Type II dissection ispresent, the entire dissected aorta should be replaced.(Level of Evidence: C)
hen a Type A AoD involves the aortic root, resuspension ofe valve with preservation of the aortic sinuses and excision
the sinuses and resuspension of the valve within alyester graft are suitable options. If the aortic root islated, or if there is extensive dissection and disruption of thertic sinuses, replacement with a composite graft is neces-ry.
6.5. Endovascular Interventionsndovascular stent grafts are not approved for AoD involvinge ascending aorta or aortic arch. Endovascular stent grafts
ed for descending thoracic aortic dissection is discussed in
Secu
8.HTprursuticantrclanmdiinIM
8.TseimblardicasudewthWemb(2
8.TcuasfirspderemrethafisEexbeatatviTTsu
m(ecothin
8.W
CL
1.
AAin(3declre
tachonthaodewofimaoprabegicotris
8TrT35lesuripemcatron35insuat
e74 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ction 9.2.2.3.1. Indications for either surgical or endovas-lar interventions are discussed in Section 9.
6.6. Principles of Treatment for Intramuralematoma and Penetrating Atherosclerotic Ulcer
he goals of treatment are to prevent aortic rupture orogression to classic AoD, allow patient stabilization beforegent surgery, and reduce complexity of unavoidable aorticrgery. Aggressive medical treatment usually includes, par-ularly in symptomatic patients, beta blockers and othertihypertensive therapy. Indications for open or endograft
eatment are based on the anatomic features of the lesion,inical presentation and course, patient comorbidities, andatomic constraints related to endograft technology. Treat-ent by endografts or open aortic reconstruction can bescussed in the context of 3 overlapping aortic lesions:timal defect without IMH, intimal defect with IMH, andH without an intimal defect.
6.6.1. INTIMAL DEFECT WITHOUT INTRAMURAL HEMATOMA
hese are localized lesions and may involve a limitedgment of the aorta. They are often an incidental finding. Byaging criteria, they include uncomplicated aortic ulcers,
ebs, and eccentric or saccular aneurysms of the aorta. Theye treated as saccular aneurysms based on their maximumameter and clinical feature (212,306,354). These lesionsn be treated with open reconstruction and are the mostitable of the 3 groups for treatment by endografts, if in thescending thoracic aorta. They involve a limited segment,hich can easily be excluded from the circulation, as long asere is an adequate distance from a critical branch artery.hen these limited dissections involve the ascending aorta,ergency surgery is indicated as for other types of AoD
ecause rupture or cardiac tamponade can occur12,306,354).
6.6.2. INTIMAL DEFECT WITH INTRAMURAL HEMATOMA
he intimal defect again presents a target lesion for endovas-lar treatment in the descending thoracic aorta, but thesociated IMH involves a longer segment of aorta than thest category. If the patient becomes asymptomatic in re-onse to aggressive medical treatment, it may be possible tolay endovascular or open reconstruction until the IMH hasabsorbed and organized. (Of note, some writing committeeembers have observed healing of IMH such that immediateconstruction was not required but have continued to followat small number of patients closely.) Two considerationsfect the length of aorta bordering the intimal defect, which
to be included in the segment targeted for treatment.vidence of adjacent atheromatous wall should favor moretensive treatment of the aorta with longer endografts,cause radiographic imaging underestimates shallow ulcer-ed atheromas, and the ulcer typically arises in a bed ofheromatous intima. Treatment with longer endografts pro-des a safety margin against undertreating the intimal defect.he second consideration is the extent of associated IMH.he self-expanding endograft may tear through the intimal
rface into underlying thrombosed false lumen. When treat- saent of this lesion in the acute stage is clinically necessary.g., persisting pain, evidence for expansion or rupture,mpromise of critical branches), it is preferable to anchore endograft in the noninvolved wall above and below thetimal defect.
6.6.3. RECOMMENDATION FOR INTRAMURAL HEMATOMA
ITHOUT INTIMAL DEFECT
ASS IIa
It is reasonable to treat intramural hematoma similar to aorticdissection in the corresponding segment of the aorta. (Level ofEvidence: C)
s noted earlier, some authors suggest treating IMH as anoD in the corresponding aortic territory. Others recommendvasive treatment regardless of location or aortic diameter54). However, small patient series, incomplete anatomicscription of case material, and lack of explicit anatomic orinical guidelines indicating open or endovascular aorticpair make it difficult to generalize from the literature.
The absence of an intimal defect, which can serve as arget lesion, presents a diagnostic as well as treatmentallenge. Intimal tears can be extremely subtle, dependingthe size of the intimal tear and the amount of intramedial
rombus, which can sometimes fill the cavity flush with thertic lumen. The intimal tear may be remote in the aortaspite leaking into the chest. IMH in a normal caliber aortaithout an apparent intimal tear precludes limited treatmenta target lesion. There are no data supporting prophylacticplantation of endografts covering the entire descendingrta, yet in unusual circumstances one may be forced toopose such treatment. IMH in an aneurysmal aorta presentsparticularly urgent problem, because this complication may
a precursor to aneurysm rupture. Although the literatureves no compelling guidelines for treatment, the writingmmittee believes that treatment of IMH corresponding to
eatment of AoD in the corresponding segment of the aortareasonable.
.7. Treatment for the Management ofaumatic Aortic Rupture
he management of blunt TRA is evolving (3,318,319,5,356). On the basis of the report by Parmley and col-
agues (318), most surgeons have recommended immediatergical repair. However, when other serious traumatic inju-
es are present including head injuries and long bone orlvic fractures, immediate surgery may not be feasible oray be dangerous. Multiple studies appear to show that ifreful blood pressure control is used, many patients can be
eated initially conservatively and then undergo operationce their other injuries have been stabilized (3,321,357–9). In a review by Svensson et al (359) of 44 patientsitially treated with careful blood pressure control whobsequently had delayed open surgery, there were no oper-ive deaths. This approach has also been reported as being
fe by Pate and colleagues and others (3,321,357,358). Thus,
inblao
In(3m(1sethOfobypam11reasm
enenstAbesprele6.copapacomef
inshpainthstlifwensedi
beanththtoenliCAbom
tasuCva
9
Mdiininpe
inmaidrySe(sSoaaoar
toottorebrdyedreaomscthdesymsc
mroinindisyprthropeca
issuno
e75JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
selected patients at high risk for other injuries andeeding, delayed repair of traumatic contained rupture of therta may be an option.The open surgical repair of TRA has evolved over time.a meta-analysis of 596 TRA patients by Svensson et al
59), the highest mortality rate was noted with cardiopul-onary bypass (16.7%), the rate was less with shunts1.4%), and the rate was lowest with a simple “clamp andw” approach (5.8%, P�0.01). There was no difference ine risk of postoperative paralysis. Subsequently, vonppell and colleagues (360) reviewed 1742 patients andund the risk of death was 18.2% with cardiopulmonarypass, 11.9% for distal perfusion with atriofemoral by-ss, 12.3% for shunts, and 16% for the “clamp and sew”ethod. The respective paralysis rates were 2.4%, 1.7%,.1%, and 19.2%, respectively. The key factor in openpairs has been to keep the total aorta cross-clamp time to
short a period as possible, especially less than 45inutes (3,359,361–364).The latest evolution in managing TRA is the use ofdovascular deployed graft covered stents. Althoughdovascular stent grafting has not been prospectively
udied for this clinical scenario, US Food and Drugdministration–approved devices are being used “off la-l,” with considerable success reported based on retro-ective studies. In a collected series of 284 patientsported in the literature, Lettinga-van de Poll and col-agues reported the procedure-related mortality was 1.5%,7% had endoleaks, and 14.4% had procedure-relatedmplications (358,365–370). In a multicenter study of 30tients with 100% implantation success, 6% to 7% oftients died, 1 had a stroke (3.3%), and 1 had partial stentllapse (3.3%) (370). Reporting bias of favorable resultsay be an issue regarding interpretation of the safety andficacy of this approach.The problems with endovascular grafting for TRA havecluded the need to cover the left subclavian artery; the acutearp angle of the distal aortic arch, particularly in youngtients; and the lack of sufficiently small prostheses for useyoung patients. The size and angle problem can result in
e “bird beak” deformity, where the proximal edge of theent is not in contact with the aortic wall and can result inting or collapse of the stent (366) (Figure 27). Similarly,hen the stent graft is larger than the aortic diameter,folding of the stent and collapse can occur. On cross-ctional views, the stent graft has the appearance of aagrammatic heart.Over time, it is hoped newer iterations of endografts will
developed that are better able to accommodate thegulation of the distal arch and are smaller. It is unlikelyat a prospective randomized study will be performed foris because of the small number of patients who make it
any surgical center and because initial results withdografting of TRA, with exception of the problems
sted earlier, have been reasonable. The Expert Opinionommittee of the Society of Thoracic Surgeons and themerican Association of Thoracic Surgeons suggested thatth acute and chronic ruptures be considered for treat-
ent with endografts. Some measures of caution must be alken because these are young patients who may bebjected to cumulative radiation exposure with multipleT scans and because the long-term durability of endo-scular stent grafts is not known (371).
. Thoracic Aortic Aneurysms
ost thoracic aortic aneurysms are caused by degenerativesease resulting in dilatation of the aorta (Figure 28). Thecidence of thoracic aortic aneurysms is estimated to becreasing and there are around 10.4 cases per 100 000rson-years (372).Risk factors for development of thoracic aortic aneurysmsclude hypertension, smoking, and chronic obstructive pul-onary disease. In addition, several genetic syndromes withpredisposition for thoracic aortic aneurysms have beenentified and are listed in Section 5. Thoracic aortic aneu-sms are also associated with bicuspid aortic valve (seection 6.1) and other congenital cardiovascular anomalies
ee Section 6) and inflammatory diseases (see Section 7).me thoracic aortic aneurysms are due to an inheritance ofpredisposition for the disease, termed familial thoracicrtic aneurysm syndrome (see Section 5.1.6), and still otherse idiopathic.Many patients with a thoracic aortic aneurysm are asymp-matic and diagnosed by chest x-ray or CT scan obtained forher reasons. An aneurysm may cause compressive symp-ms on adjacent structures including hoarseness, from leftcurrent laryngeal nerve stretching; stridor, from tracheal oronchial compression; dyspnea, from lung compression;sphagia, from esophageal compression; and plethora andema, from superior vena cava compression. Aortic valvegurgitation may develop due to aortic root or ascendingrtic dilatation and result in heart failure. Neck and jaw painay occur with aortic arch aneurysms, whereas back, inter-apular, and/or left shoulder pain may occur with descendingoracic aortic aneurysms. Embolization of atheroscleroticbris with end-organ symptoms may occur. Finally, acutendromes including dissection or rupture without dissectionay occur with potentially catastrophic outcomes as de-ribed in Section 8.5.Thoracic aortic aneurysms may involve different seg-ents of the aorta. The ascending thoracic aorta and/orot is most commonly involved, with the descending aortavolved less often. Involvement of the aortic arch occursonly 10%. The etiology, natural history, and treatments
ffer somewhat for aneurysms in each location. In Marfanndrome, aneurysms typically arise in the aortic root, aocess often referred to as annuloaortic ectasia. Becausee leaflets of the aortic valve are suspended within theot, successful repair of the aortic root may requirerformance of a valve-sparing root repair or, in someses, a composite aortic graft.The average rate of expansion of thoracic aortic aneurysmsestimated to be 0.10 to 0.42 cm/y (373–375). Medical andrgical treatment considerations and selection criteria areted in Section 9.2.A leaking or ruptured aneurysm (see Section 9.1.2.1) may
so present as chest pain with hypotension due to hemor-
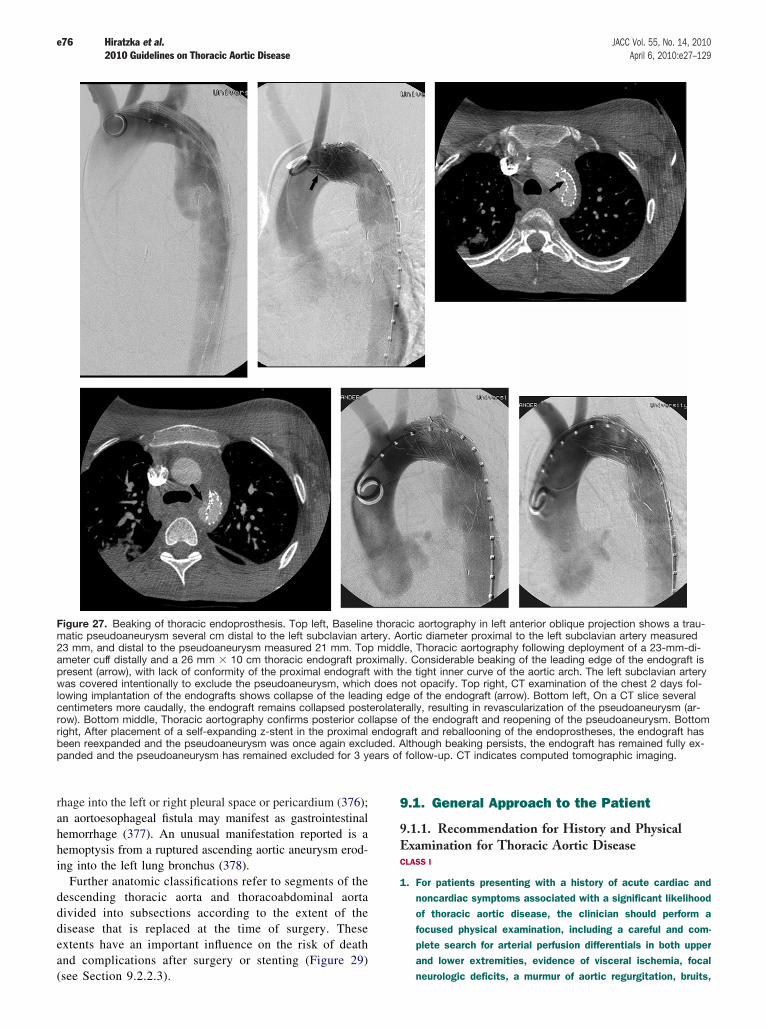
rhanhehein
dedidiexan(s
9
9.ECL
1.
Fim23amprwlocerorigbepa rs of f
e76 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
age into the left or right pleural space or pericardium (376);aortoesophageal fistula may manifest as gastrointestinal
morrhage (377). An unusual manifestation reported is amoptysis from a ruptured ascending aortic aneurysm erod-g into the left lung bronchus (378).Further anatomic classifications refer to segments of thescending thoracic aorta and thoracoabdominal aortavided into subsections according to the extent of thesease that is replaced at the time of surgery. Thesetents have an important influence on the risk of deathd complications after surgery or stenting (Figure 29)
gure 27. Beaking of thoracic endoprosthesis. Top left, Baselineatic pseudoaneurysm several cm distal to the left subclavian arte
mm, and distal to the pseudoaneurysm measured 21 mm. Topeter cuff distally and a 26 mm � 10 cm thoracic endograft prox
esent (arrow), with lack of conformity of the proximal endograft was covered intentionally to exclude the pseudoaneurysm, which dwing implantation of the endografts shows collapse of the leadinntimeters more caudally, the endograft remains collapsed postew). Bottom middle, Thoracic aortography confirms posterior collaht, After placement of a self-expanding z-stent in the proximal een reexpanded and the pseudoaneurysm was once again excludnded and the pseudoaneurysm has remained excluded for 3 yea
ee Section 9.2.2.3).
.1. General Approach to the Patient
1.1. Recommendation for History and Physicalxamination for Thoracic Aortic DiseaseASS I
For patients presenting with a history of acute cardiac andnoncardiac symptoms associated with a significant likelihoodof thoracic aortic disease, the clinician should perform afocused physical examination, including a careful and com-plete search for arterial perfusion differentials in both upperand lower extremities, evidence of visceral ischemia, focal
c aortography in left anterior oblique projection shows a trau-rtic diameter proximal to the left subclavian artery measured, Thoracic aortography following deployment of a 23-mm-di-Considerable beaking of the leading edge of the endograft istight inner curve of the aortic arch. The left subclavian artery
ot opacify. Top right, CT examination of the chest 2 days fol-of the endograft (arrow). Bottom left, On a CT slice severallly, resulting in revascularization of the pseudoaneurysm (ar-
f the endograft and reopening of the pseudoaneurysm. Bottomft and reballooning of the endoprostheses, the endograft hasthough beaking persists, the endograft has remained fully ex-ollow-up. CT indicates computed tomographic imaging.
thoraciry. Aomiddleimally.ith theoes n
g edgerolaterapse ondograed. Al
neurologic deficits, a murmur of aortic regurgitation, bruits,

Tsunebadiretr
foca
“tor
diitfinul
9.Tpa
e77JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
and findings compatible with possible cardiac tamponade.(339–341) (Level of Evidence: C)
he physical findings of thoracic aortic diseases may bebtle indirect manifestations of uncommon underlying ge-tically predisposing conditions. In evaluating the evidencese for physical examination of patients with thoracic aorticsease, there are no controlled or blinded experimentalsearch studies that have stratified patients into differenteatment categories based on physical findings.For all patients with thoracic aortic disease, the first andremost issue is to identify those who are acutely at risk for
tastrophic harm as early as possible. Establishing a set of etriggers” or “red flags” may serve as alerts to either excludeidentify life-threatening thoracic aortic disease.Given the growing awareness of an extensive variety of
seases associated with nonemergent thoracic aortic disease,is important to be aware of the many different physicaldings associated with extracardiovascular etiologies partic-
arly those of genetic origin (see Section 5).
1.1.1. CORONARY ARTERY DISEASE
he frequency of coexisting CAD varies widely amongtient subgroups with thoracic aortic disease as does the
Figure 28. Ascending thoracic aortic aneurysm ina patient with calcific aortic stenosis. Top left, Ax-ial CT image demonstrates an enlarged ascendingthoracic aorta (A) and normal caliber descendingthoracic aorta (D). Top right, Axial CT image dem-onstrates extensive aortic valve leaflet calcification(arrows). Middle left, Coronal CT image also dem-onstrates the dilated ascending aorta (A) and aor-tic valve leaflet calcification (arrows). Middle right,Volume rendered CT image demonstrates the di-lated ascending thoracic aorta (A), normal caliberaortic arch and descending thoracic aorta (D) andgreat vessels with a bovine arch configuration(INN, LCCA, LSCA). Bottom, Volume rendered ro-tating image of the thoracic aorta can be used todepict the anatomy, particularly the relationship ofan aortic abnormality to the great vessels, for sur-gical planning. See the accompanying full cinevideo for the bottom panel. CT indicates com-puted tomographic imaging; INN, innominate ar-tery; LCCA, left common carotid artery; LSCA, leftsubclavian artery; and LV, left ventricle.
iology of the coronary artery abnormalities, if present.
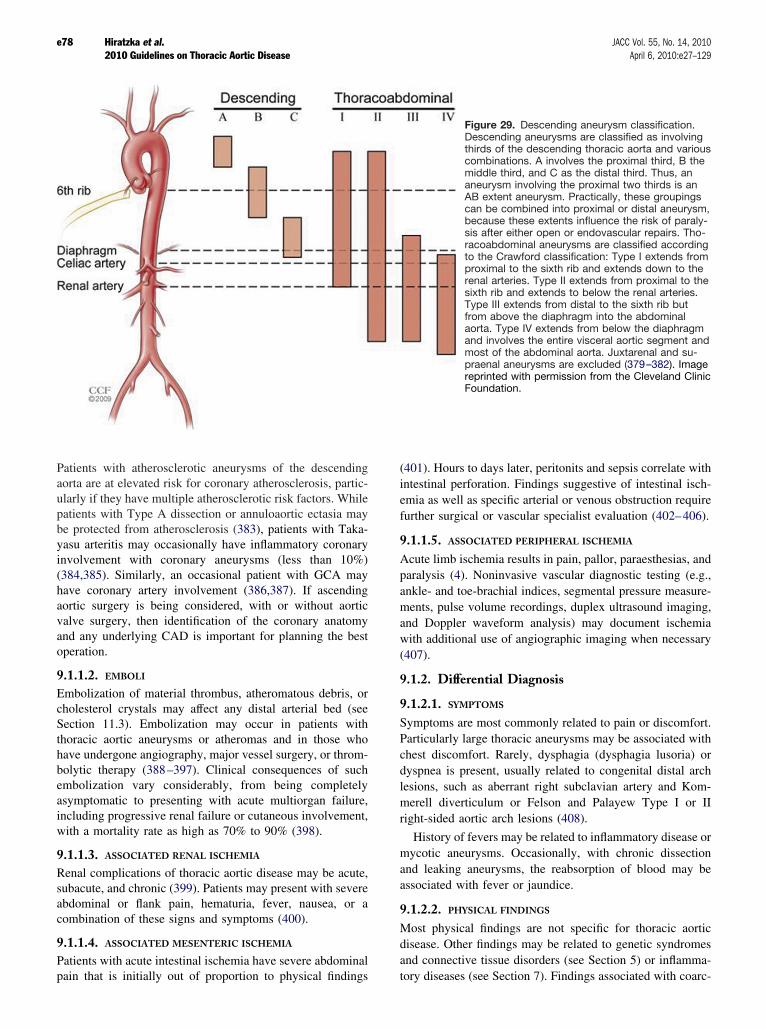
Paaoulpabeyain(3haaovaanop
9.EchSethhaboemasinw
9.Rsuabco
9.Papa
(4inemfu
9.Apaanmanw(4
9.
9.SyPachdylemri
manas
9.Mdian
e78 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
tients with atherosclerotic aneurysms of the descendingrta are at elevated risk for coronary atherosclerosis, partic-arly if they have multiple atherosclerotic risk factors. Whiletients with Type A dissection or annuloaortic ectasia mayprotected from atherosclerosis (383), patients with Taka-
su arteritis may occasionally have inflammatory coronaryvolvement with coronary aneurysms (less than 10%)84,385). Similarly, an occasional patient with GCA mayve coronary artery involvement (386,387). If ascendingrtic surgery is being considered, with or without aorticlve surgery, then identification of the coronary anatomyd any underlying CAD is important for planning the besteration.
1.1.2. EMBOLI
mbolization of material thrombus, atheromatous debris, orolesterol crystals may affect any distal arterial bed (seection 11.3). Embolization may occur in patients withoracic aortic aneurysms or atheromas and in those whove undergone angiography, major vessel surgery, or throm-lytic therapy (388–397). Clinical consequences of suchbolization vary considerably, from being completely
ymptomatic to presenting with acute multiorgan failure,cluding progressive renal failure or cutaneous involvement,ith a mortality rate as high as 70% to 90% (398).
1.1.3. ASSOCIATED RENAL ISCHEMIA
enal complications of thoracic aortic disease may be acute,bacute, and chronic (399). Patients may present with severedominal or flank pain, hematuria, fever, nausea, or ambination of these signs and symptoms (400).
1.1.4. ASSOCIATED MESENTERIC ISCHEMIA
tients with acute intestinal ischemia have severe abdominal
in that is initially out of proportion to physical findings to01). Hours to days later, peritonits and sepsis correlate withtestinal perforation. Findings suggestive of intestinal isch-ia as well as specific arterial or venous obstruction require
rther surgical or vascular specialist evaluation (402–406).
1.1.5. ASSOCIATED PERIPHERAL ISCHEMIA
cute limb ischemia results in pain, pallor, paraesthesias, andralysis (4). Noninvasive vascular diagnostic testing (e.g.,kle- and toe-brachial indices, segmental pressure measure-ents, pulse volume recordings, duplex ultrasound imaging,d Doppler waveform analysis) may document ischemiaith additional use of angiographic imaging when necessary07).
1.2. Differential Diagnosis
1.2.1. SYMPTOMS
mptoms are most commonly related to pain or discomfort.rticularly large thoracic aneurysms may be associated withest discomfort. Rarely, dysphagia (dysphagia lusoria) orspnea is present, usually related to congenital distal arch
sions, such as aberrant right subclavian artery and Kom-erell diverticulum or Felson and Palayew Type I or IIght-sided aortic arch lesions (408).
History of fevers may be related to inflammatory disease orycotic aneurysms. Occasionally, with chronic dissectiond leaking aneurysms, the reabsorption of blood may besociated with fever or jaundice.
1.2.2. PHYSICAL FINDINGS
ost physical findings are not specific for thoracic aorticsease. Other findings may be related to genetic syndromesd connective tissue disorders (see Section 5) or inflamma-
Figure 29. Descending aneurysm classification.Descending aneurysms are classified as involvingthirds of the descending thoracic aorta and variouscombinations. A involves the proximal third, B themiddle third, and C as the distal third. Thus, ananeurysm involving the proximal two thirds is anAB extent aneurysm. Practically, these groupingscan be combined into proximal or distal aneurysm,because these extents influence the risk of paraly-sis after either open or endovascular repairs. Tho-racoabdominal aneurysms are classified accordingto the Crawford classification: Type I extends fromproximal to the sixth rib and extends down to therenal arteries. Type II extends from proximal to thesixth rib and extends to below the renal arteries.Type III extends from distal to the sixth rib butfrom above the diaphragm into the abdominalaorta. Type IV extends from below the diaphragmand involves the entire visceral aortic segment andmost of the abdominal aorta. Juxtarenal and su-praenal aneurysms are excluded (379–382). Imagereprinted with permission from the Cleveland ClinicFoundation.
ry diseases (see Section 7). Findings associated with coarc-

tam
9.Basththvian
9FTh
9.PCL
1.
Tpomanscaooum
innowmlafr
Ta
Tr
Be
Anen
Anblo
St
rd devi
e79JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
tion of the aorta include brachial-femoral pulse delay andurmurs.
1.3. Considerations for Imagingecause most cases of chronic thoracic aortic disease areymptomatic and difficult to detect on physical examination,e clinician must have a low threshold for screening fororacic aortic disease. CT or MR is required to adequatelysualize the affected aorta. There has been no cost–benefitalysis of screening in these populations (see Section 18.1).
.2. General Medical Treatment and Riskactor Management for Patients Withoracic Aortic Disease
2.1. Recommendation for Medical Treatment ofatients With Thoracic Aortic DiseasesASS I
Stringent control of hypertension, lipid profile optimization,smoking cessation, and other atherosclerosis risk-reduction
ble 13. Studies of Medical Treatment of Thoracic Aortic Aneur
eatment Studies
ta blockers Genoni M, Paul M, Jenni R,et al (410)
Retrospectivmedical treaother antihy20 (45%) frincidence o40% (8 of 2
Shores J, Berger KR, Murphy EA,et al (88)
Open-label,The treatedtherapy slow
Ladouceur M, Fermanian C,Lupoglazoff JM, et al (411)
Retrospectivwas slowed
giotensin-convertingzyme inhibitors
Ahimastos AA, Aggarwal A,D’Orsa KM, et al (412)
Randomizedtaking beta-perindopril-the ascendireduction inrespectively
giotensin receptorckers
Mochizuki S, Dahlof B, Shimizu M,et al (413)
3081 Japancombinationother treatmreduction inin aortic dis
Brooke BS, Habashi JP, Judge DP,et al (89)
The clinicalin 1 patientroot enlargesignificantlyduring angioenlargemenmean differangiotensionchange in ddistal ascen
atins Diehm N, Decker G, Katzen B,et al (414)
A nonrandoof patientsStatin use wHR 0.613, 91.795, 95%
AAA indicates abdominal aortic aneurysm; CI, confidence interval; SD, standa
measures should be instituted for patients with small aneu- po
rysms not requiring surgery, as well as for patients who are notconsidered to be surgical or stent graft candidates. (Level ofEvidence: C)
he patient’s general status should be optimized wheressible. Respiratory illness, a common comorbid problem,ay be improved by stopping smoking, clearing bronchitis,d exercising regularly with walking. Because other athero-lerotic disease is usually present in patients with thoracicrtic aneurysms or atheroma, risk-reduction measures astlined in other guidelines are appropriate (409). Additionaledical management rationales are noted in Table 13.Patients who are not candidates for operative intervention
clude those whose aneurysms or other aortic pathology dot meet the criteria for surgical intervention and those in
hom the criteria are met but who are considered inoperable,ost commonly because of coexisting disease. Patients withrge aneurysms who are considered inoperable may benefitom stringent control of risk factors (see Section 3.2) to
Results
-record review of 78 patients with chronic Type B dissection who received51 of 71 received beta-blocker treatment, 20 of 71 were treated withve drugs. 10 of 51 (20%) of the beta-blocker–treated patients and 9 ofother treatment group needed dissection-related surgery (P�0.002). Theing aortic diameter was 12% (6 of 51) in the beta-blocker group ande other treatment group (P�0.002).
ized, control study of propranolol in 70 patients with Marfan syndrome.eceived a mean daily propranolol dose of 212�68 mg/d. Propranololic root dilation (0.023 vs 0.084 per year, P�0.001).
ation of aortic dilation in children with Marfan syndrome. Aortic dilatationmm/y in children treated with beta blockers.
-blind, placebo-controlled trial of 17 patients with Marfan syndrometherapy to perindopril or placebo. After 24 weeks of therapy, theubjects compared with placebo-treated subjects had smaller growth indiameter during systole (1.2 vs 0.3 mm/m2, P�0.01) and a significant
ing aortic diameter during diastole (0.4 vs �1.2 mm/m2, P�0.001),
ients with hypertension, coronary heart disease, heart failure, or aandomly assigned either to open-label valsartan (40 to 160 mg/d) or tohout angiotension receptor blockers. Patients randomized to valsartan hadsite cardiovascular outcome (OR 0.61, 95% CI 0.47 to 0.79) and reduction(OR 0.18, 95% CI 0.04 to 0.88). Open-label, randomized.
e to angiotension receptor blockers (losartan in 17 patients and irbesartanvaluated in pediatric patients with Marfan syndrome with severe aortiche mean (�SD) rate of change in aortic root diameter decreased.54�2.87 mm/y during previous medical therapy to 0.46�0.62 mm/yreceptor blocker therapy (P�0.001). The deviation of aortic rootormal, as expressed by the rate of change in z scores, was reduced by a1.47 z scores/y (95% CI 0.70 to 2.24, P�0.001) after the initiation ofor blocker therapy. The sinotubular junction showed a reduced rate ofduring angiotension receptor blocker therapy (P�0.05), whereas the
rta was not affected by angiotension receptor blocker therapy.
ropensity-score–adjusted study of statin use effect on long-term mortalityovascular repair of AAA (731 patients) or TAA (59 patients) was done.ciated with decreased long-term mortality in patients with AAA (adjusted.379 to 0.993, P�0.047), but not for patients with TAA (adjusted HR7 to 21.942; P�0.647).
ation; and TAA, thoracic aortic aneurysm.
ysm
e, casetment.pertensiom thef increas0) in th
randomgroup red aort
e evaluby 0.2
, doubleblocker
treated sng aorticascend
.
ese patwere rent witcompo
section
respons) were ement. Tfrom 3tension
t from nence of
receptiameterding ao
mized pafter endas asso5% CI 0CI 0.14
tentially slow the rate of growth and reduce the risk of
ruar
9.PR
CL
1.
2.
CL
1.
2.
TantrrehamRstheavain
tiotiodrwlaovonanTreprpeblbew
wan
tequ
9.CL
1.
Tmtr(4noan20thinCrethgrsiwdareWretaof
dedeclthha
9.CL
1.
Tindihaexbyraroco
e80 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
pture or dissection. Recommendations for periodic imaginge noted in Section 14.
2.1.1. RECOMMENDATIONS FOR BLOOD
ESSURE CONTROL
ASS I
Antihypertensive therapy should be administered to hyperten-sive patients with thoracic aortic diseases to achieve a goal ofless than 140/90 mm Hg (patients without diabetes) or lessthan 130/80 mm Hg (patients with diabetes or chronic renaldisease) to reduce the risk of stroke, myocardial infarction,heart failure, and cardiovascular death. (415–419) (Level ofEvidence: B)Beta adrenergic–blocking drugs should be administered to allpatients with Marfan syndrome and aortic aneurysm to reducethe rate of aortic dilatation unless contraindicated. (88) (Levelof Evidence: B)
ASS IIa
For patients with thoracic aortic aneurysm, it is reasonable toreduce blood pressure with beta blockers and angiotensin-converting enzyme inhibitors (412) or angiotensin receptorblockers (89,413) to the lowest point patients can toleratewithout adverse effects. (88,410,411) (Level of Evidence: B)An angiotensin receptor blocker (losartan) is reasonable forpatients with Marfan syndrome, to reduce the rate of aorticdilatation unless contraindicated. (89,90) (Level of Evi-dence: B)
reatment of hypertension to reduce end points of MI, stroke,d death is well established with many randomized clinical
ials (420). In the Jikei Heart Study, Japanese patients whoceived valsartan along with other antihypertensive therapyd a significantly lower rate of cardiovascular morbidity andortality compared with patients treated without valsartan.eductions noted in particular included lower incidence ofroke, transient ischemic attack (TIA), angina pectoris, andart failure. Moreover, pertinent to this guideline, there wassignificant reduction in the incidence of AoD in thelsartan-treated patients, which contributed to the reductionoverall cardiovascular morbidity and mortality (413).
Currently, beta adrenergic blockade serves as the founda-n of the medical regimen because of demonstrated inhibi-n of aneurysm expansion in patients with Marfan syn-ome. Shores and colleagues (88) randomized 70 patientsith Marfan syndrome to propranolol or placebo in a open-bel study demonstrating an attenuated rate of expansioner the 10-year follow-up. Dietz and colleagues (91) dem-strated that angiotensin receptor blocker therapy reduceseurysm expansion in animal models of Marfan syndrome.
his group has also recently demonstrated that angiotensionceptor blocker therapy slowed the rate of progression ofogressive aortic root dilatation in a preliminary study of 18diatric patients with Marfan syndrome (89). Both betaockade and angiotensin II receptor blockade therapy areing further investigated in a randomized trial for patientsith Marfan syndrome (90).
Lifestyle modifications of diet, weight reduction for over-eight or obese patients, moderation of alcohol consumption,
d aerobic exercise are standard approaches to treat hyper- plnsion (421), but pharmacological therapy is usually re-ired for patients with thoracic aortic diseases.
2.1.2. RECOMMENDATION FOR DYSLIPIDEMIA
ASS IIa
Treatment with a statin to achieve a target LDL cholesterol ofless than 70 mg/dL is reasonable for patients with a coronaryheart disease risk equivalent such as noncoronary atheroscle-rotic disease, atherosclerotic aortic aneurysm, and coexistentcoronary heart disease at high risk for coronary ischemicevents. (422–425) (Level of Evidence: A)
he National Cholesterol Education Program ATP III recom-ends that patients with noncoronary atherosclerosis beeated like patients with established coronary heart disease26). Atherosclerosis in the aorta, like atherosclerosis in anyncoronary vascular bed, markedly increases the risk of MId stroke. As a result of this high-risk status (greater than% event rate in 10 years), the goal for hypolipidemicerapy is an LDL level less than 100 mg/dL. Initial therapy
these patients should be a statin. After the Nationalholesterol Education Program ATP III guidelines wereleased in 2001, the Heart Protection Study reported in 2002at patients with atherosclerosis and a total cholesterol leveleater than 135 mg/dL benefited from the addition ofmvastatin 40 mg/d (427). The RR reductions remained evenhen LDL started at less than 100 mg/dL. In concert withta from patients with acute coronary syndromes, the morecent ACC/AHA Guidelines for the Management of Patientsith Peripheral Arterial Disease also gave a Class IIacommendation suggesting the use of a statin to achieve arget LDL of less than 70 mg/dL for patients at very high riskischemic events is reasonable (4).
There are experimental data demonstrating a delayedvelopment of atherosclerosis and prevention of aneurysmvelopment by statins (428–430). However, there are noinical outcomes data that justify their use acutely or suggestat statins prevent expansion after thoracic aortic aneurysmsve developed.
2.1.3. RECOMMENDATION FOR SMOKING CESSATION
ASS I
Smoking cessation and avoidance of exposure to environmen-tal tobacco smoke at work and home are recommended.Follow-up, referral to special programs, and/or pharmacother-apy (including nicotine replacement, buproprion, or vareni-cline) is useful, as is adopting a stepwise strategy aimed atsmoking cessation (the 5 A’s are Ask, Advise, Assess, Assist,and Arrange). (431–432b) (Level of Evidence: B)
here are no randomized or prospective trials that havevestigated the effect of smoking cessation on thoracic aorticsease. Patients with thoracic aortic aneurysm who smokeve double the rate of aneurysm expansion (433). Aneurysmpansion and rupture after Type B dissection are not affectedcigarette smoking (434). Smoking cessation reduces the
te of MI and death in patients with noncoronary atheroscle-sis (435). Patients who smoke require close follow-up innjunction with medical and other support to achieve com-
ete smoking cessation.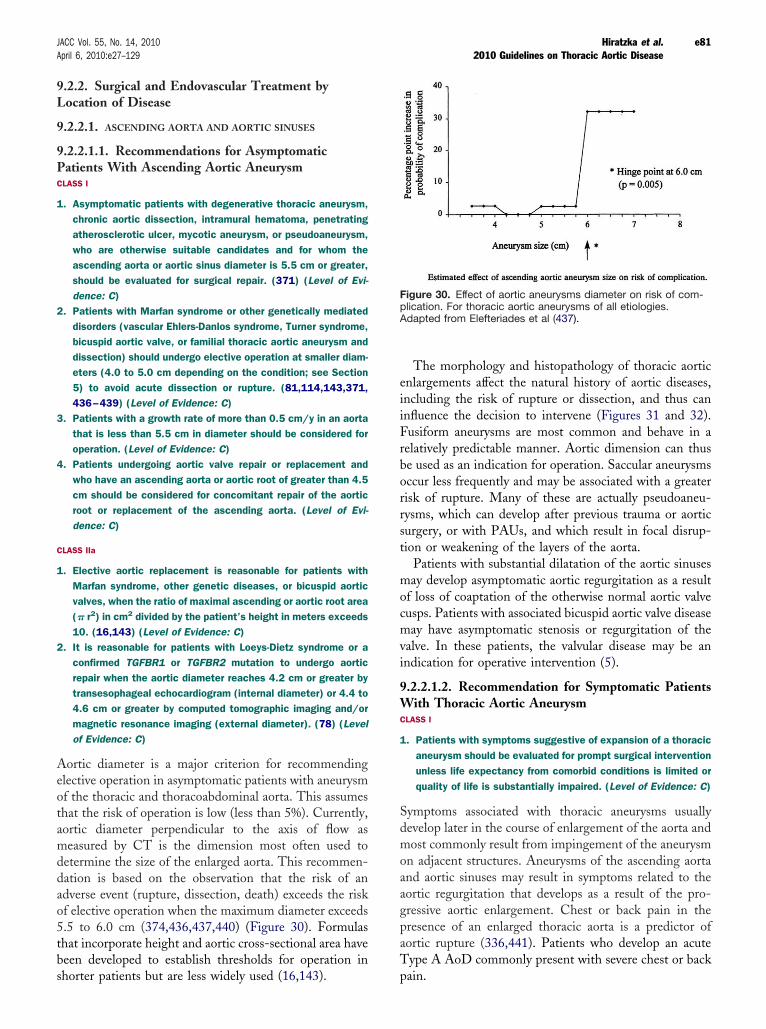
9.L
9.
9.PCL
1.
2.
3.
4.
CL
1.
2.
Aelofthaomdedaadof5.thbesh
enininFrebeocrirysuti
mofcumvain
9.WCL
1.
SdemonanaogrpraoT
FiplAd
e81JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
2.2. Surgical and Endovascular Treatment byocation of Disease
2.2.1. ASCENDING AORTA AND AORTIC SINUSES
2.2.1.1. Recommendations for Asymptomaticatients With Ascending Aortic AneurysmASS I
Asymptomatic patients with degenerative thoracic aneurysm,chronic aortic dissection, intramural hematoma, penetratingatherosclerotic ulcer, mycotic aneurysm, or pseudoaneurysm,who are otherwise suitable candidates and for whom theascending aorta or aortic sinus diameter is 5.5 cm or greater,should be evaluated for surgical repair. (371) (Level of Evi-dence: C)Patients with Marfan syndrome or other genetically mediateddisorders (vascular Ehlers-Danlos syndrome, Turner syndrome,bicuspid aortic valve, or familial thoracic aortic aneurysm anddissection) should undergo elective operation at smaller diam-eters (4.0 to 5.0 cm depending on the condition; see Section5) to avoid acute dissection or rupture. (81,114,143,371,436–439) (Level of Evidence: C)Patients with a growth rate of more than 0.5 cm/y in an aortathat is less than 5.5 cm in diameter should be considered foroperation. (Level of Evidence: C)Patients undergoing aortic valve repair or replacement andwho have an ascending aorta or aortic root of greater than 4.5cm should be considered for concomitant repair of the aorticroot or replacement of the ascending aorta. (Level of Evi-dence: C)
ASS IIa
Elective aortic replacement is reasonable for patients withMarfan syndrome, other genetic diseases, or bicuspid aorticvalves, when the ratio of maximal ascending or aortic root area(� r2) in cm2 divided by the patient’s height in meters exceeds10. (16,143) (Level of Evidence: C)It is reasonable for patients with Loeys-Dietz syndrome or aconfirmed TGFBR1 or TGFBR2 mutation to undergo aorticrepair when the aortic diameter reaches 4.2 cm or greater bytransesophageal echocardiogram (internal diameter) or 4.4 to4.6 cm or greater by computed tomographic imaging and/ormagnetic resonance imaging (external diameter). (78) (Levelof Evidence: C)
ortic diameter is a major criterion for recommendingective operation in asymptomatic patients with aneurysmthe thoracic and thoracoabdominal aorta. This assumesat the risk of operation is low (less than 5%). Currently,rtic diameter perpendicular to the axis of flow aseasured by CT is the dimension most often used totermine the size of the enlarged aorta. This recommen-tion is based on the observation that the risk of anverse event (rupture, dissection, death) exceeds the riskelective operation when the maximum diameter exceeds
5 to 6.0 cm (374,436,437,440) (Figure 30). Formulasat incorporate height and aortic cross-sectional area haveen developed to establish thresholds for operation in
orter patients but are less widely used (16,143). paThe morphology and histopathology of thoracic aorticlargements affect the natural history of aortic diseases,cluding the risk of rupture or dissection, and thus canfluence the decision to intervene (Figures 31 and 32).usiform aneurysms are most common and behave in alatively predictable manner. Aortic dimension can thusused as an indication for operation. Saccular aneurysms
cur less frequently and may be associated with a greatersk of rupture. Many of these are actually pseudoaneu-sms, which can develop after previous trauma or aorticrgery, or with PAUs, and which result in focal disrup-
on or weakening of the layers of the aorta.Patients with substantial dilatation of the aortic sinusesay develop asymptomatic aortic regurgitation as a resultloss of coaptation of the otherwise normal aortic valvesps. Patients with associated bicuspid aortic valve diseaseay have asymptomatic stenosis or regurgitation of thelve. In these patients, the valvular disease may be andication for operative intervention (5).
2.2.1.2. Recommendation for Symptomatic Patientsith Thoracic Aortic Aneurysm
ASS I
Patients with symptoms suggestive of expansion of a thoracicaneurysm should be evaluated for prompt surgical interventionunless life expectancy from comorbid conditions is limited orquality of life is substantially impaired. (Level of Evidence: C)
ymptoms associated with thoracic aneurysms usuallyvelop later in the course of enlargement of the aorta andost commonly result from impingement of the aneurysm
adjacent structures. Aneurysms of the ascending aortad aortic sinuses may result in symptoms related to thertic regurgitation that develops as a result of the pro-essive aortic enlargement. Chest or back pain in theesence of an enlarged thoracic aorta is a predictor ofrtic rupture (336,441). Patients who develop an acuteype A AoD commonly present with severe chest or back
gure 30. Effect of aortic aneurysms diameter on risk of com-ication. For thoracic aortic aneurysms of all etiologies.apted from Elefteriades et al (437).
in.

9.AgrAdi
9.ACL
1.
2.
A
Fiar netic re
e82 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
2.2.1.3. Endovascular Grafting for Ascending Aorticneurysm. At the time of this writing, endovascular stentafts have not been approved by the US Food and Drugdministration for treatment of aneurysms or other con-tions of the ascending aorta.
2.2.1.4. Recommendations for Open Surgery forscending Aortic AneurysmASS I
Separate valve and ascending aortic replacement are recom-
gure 31. Ascending aortic aneurysm of degenerative etiology. Ctery disease; CT, computed tomographic imaging; and MR, mag
mended in patients without significant aortic root dilatation, in se
elderly patients, or in young patients with minimal dilatationwho have aortic valve disease. (Level of Evidence: C)Patients with Marfan, Loeys-Dietz, and Ehlers-Danlos syn-dromes and other patients with dilatation of the aortic root andsinuses of Valsalva should undergo excision of the sinuses incombination with a modified David reimplantation operation iftechnically feasible or, if not, root replacement with valvedgraft conduit. (134,164,442–444) (Level of Evidence: B)
scending Aortic Aneurysms: The extent of aortic re-
dicates coronary artery bypass graft surgery; CAD, coronarysonance imaging.
ABG in
ction and the need for ancillary procedures are deter-

mAinmva
asmAnaci
rebycoan
biwjuca
Fitioandi esonan
e83JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
ined by preoperative testing and intraoperative findings.ncillary procedures that may be performed concurrentlyclude coronary artery bypass graft surgery, valve replace-ent or repair, repair of cardiac septal defects, closure ofscular fistulas, and ablative therapy for arrhythmias.For patients with isolated aneurysms confined to thecending aorta, resection and graft replacement is theost commonly performed and recommended procedure.lternatively, reduction aortoplasty with or without exter-l reinforcement has only been performed in very limited
gure 32. Ascending aortic aneurysms associated with genetic dns for Asymptomatic Patients With Ascending Aortic Aneurysmd Associated Congenital Variants in Adults (Section 6.1). CABG
sease; CT, computed tomographic imaging; and MR, magnetic r
rcumstances (445,446). pa
For patients with aortic valve stenosis who require valveplacement, the choice of valve substitute is determinedage of the patient, presence of comorbid disease, risk of
mplications related to anticoagulation and reoperation,d life expectancy (139).For patients with aortic regurgitation associated with acuspid aortic valve, repair of the aortic valve with orithout root remodeling or tailoring of the sinotubularnction is preferable if the valve is not severely fibrotic orlcified (99,140). For patients with a dilated aortic root,
. *Depends on specific genetic condition. †See Recommenda-n 9.2.2.1.1) and Recommendations for Bicuspid Aortic Valvees coronary artery bypass graft surgery; CAD, coronary arteryce imaging.
isorder(Sectioindicat
rticularly those with stenotic bicuspid valves, composite

vava
rereelaoac
reropavataCicst
9.CL
1.
2.
3.
4.
5.
6.
Aanadopadthmst
isaoofco
holaararSuasas
marnohoa
9.grAdiryopcearprcuarao
mthpr1peth(2reiewusdise
stzoth
9.TH
9.ACL
1.
e84 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
lve grafts containing either mechanical or biologicallves are implanted.Ascending aneurysms larger than 4.5 to 5.0 cm requirepair or tube graft replacement when aortic valve repair orplacement is the primary indication for operation (5). Inderly patients, ascending aortic aortoplasty when thertic diameter does not exceed 5.0 cm may be anceptable alternative.Aortic Valve and Root: In patients with aortic valvegurgitation and root dilatation, aortic valve repair andot-sparing procedure may be the primary procedure. Intients with Marfan syndrome or with tricuspid aorticlve regurgitation, a modification of the David reimplan-tion operation may be considered. (94,95,97–99,447)omposite valve grafts with either biological or mechan-al valves are an alternative option, particularly for valvularenosis (99,140,441,448).
2.2.2. RECOMMENDATIONS FOR AORTIC ARCH ANEURYSMS
ASS IIa
For thoracic aortic aneurysms also involving the proximalaortic arch, partial arch replacement together with ascendingaorta repair using right subclavian/axillary artery inflow andhypothermic circulatory arrest is reasonable. (222,449,450)(Level of Evidence: B)Replacement of the entire aortic arch is reasonable for acutedissection when the arch is aneurysmal or there is extensiveaortic arch destruction and leakage. (222,450) (Level ofEvidence: B)Replacement of the entire aortic arch is reasonable for aneu-rysms of the entire arch, for chronic dissection when the archis enlarged, and for distal arch aneurysms that also involve theproximal descending thoracic aorta, usually with the elephanttrunk procedure. (451–453) (Level of Evidence: B)For patients with low operative risk in whom an isolateddegenerative or atherosclerotic aneurysm of the aortic arch ispresent, operative treatment is reasonable for asymptomaticpatients when the diameter of the arch exceeds 5.5 cm. (374)(Level of Evidence: B)For patients with isolated aortic arch aneurysms less than 4.0cm in diameter, it is reasonable to reimage using computedtomographic imaging or magnetic resonance imaging, at 12-month intervals, to detect enlargement of the aneurysm. (Levelof Evidence: C)For patients with isolated aortic arch aneurysms 4.0 cm orgreater in diameter, it is reasonable to reimage using com-puted tomographic imaging or magnetic resonance imaging, at6-month intervals, to detect enlargement of the aneurysm.(Level of Evidence: C)
neurysms of the aortic arch are commonly associated witheurysmal disease or dissection of the ascending aorta or thejacent descending thoracic aorta, and the indications forerative intervention in these patients are those for thejacent aortic segment. This relates to the need for hypo-ermic cardiopulmonary bypass and an interval of hypother-ic circulatory arrest, and to higher operative mortality and
roke rates than those observed following operation forolated aneurysms of the ascending or descending thoracicrta (451–459). As with ascending aneurysms, a growth ratemore than 0.5 cm/y in the absence of symptoms could bensidered an indication for operation.
Symptoms associated with aortic arch aneurysms such asarseness resulting from stretching of the left recurrent
ryngeal nerve, dysphagia, dyspnea, and chest or back paine indications for operative intervention for patients withch aneurysms unless life expectancy is quite limited.itability for operative intervention involves similar risksessment to that for aneurysm or other disorders of thecending aorta and aortic root.
The innominate, left carotid, and left subclavian arteriesay require separate grafting. For short periods of circulatoryrest, the use of retrograde or antegrade brain perfusion hast conclusively been shown to add further brain protection;wever, use of the subclavian or axillary artery bypass withside graft reduces the risk of stroke (449).
2.2.2.1. Open Surgery. At present, endovascular stentafts have not been approved by the US Food and Drugdministration for treatment of aneurysms or other con-tions of the aortic arch. For patients with large aneu-sms who are not candidates for conventional openeration, experience is accumulating with operative pro-dures that involve translocation of the brachiocephalicteries from the aortic arch using branch grafts from theoximal ascending aorta, and placement of an endovas-lar graft into the distal ascending aorta, the entire aorticch, and a segment of the adjacent descending thoracicrta (371,460,461).Cardiopulmonary bypass with some degree of hypother-ia is required for operations that require replacement ofe aortic arch. Brain protection can be achieved byofound hypothermia alone, direct antegrade perfusion ofor more of the brachiocephalic arteries, or retrograderfusion using cold oxygenated blood that is infused intoe superior vena cava during the arrest period11,449,462–467) (see Section 14.5.1). The aortic arch isplaced with a synthetic graft. The brachiocephalic arter-s are attached to the graft using a patch of the aortahich contains the origins of the 3 vessels or separatelying a graft that contains 3 branches. The proximal andstal ends of the aortic graft are attached to normalgments of ascending and descending thoracic aorta.An “elephant trunk” procedure has been used to recon-
ruct the arch and then provide a Dacron graft landingne for endovascular stent graft treatment of descendingoracic aortic aneurysms (Figure 33).
2.2.3. DESCENDING THORACIC AORTA AND
ORACOABDOMINAL AORTA
2.2.3.1. Recommendations for Descending Thoracicorta and Thoracoabdominal Aortic AneurysmsASS I
For patients with chronic dissection, particularly if associated
with a connective tissue disorder, but without significant
2.
3.
4.
AcuDdesaaotiPeula
thtire
vah
9.pincoexaole
pasuwsuopinpaanveremisamtopatrth
pr
e85JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
comorbid disease, and a descending thoracic aortic diameterexceeding 5.5 cm, open repair is recommended. (371,382,468) (Level of Evidence: B)For patients with degenerative or traumatic aneurysms of thedescending thoracic aorta exceeding 5.5 cm, saccular aneu-rysms, or postoperative pseudoaneurysms, endovascular stentgrafting should be strongly considered when feasible.(371,469) (Level of Evidence: B)For patients with thoracoabdominal aneurysms, in whom endo-vascular stent graft options are limited and surgical morbidityis elevated, elective surgery is recommended if the aorticdiameter exceeds 6.0 cm, or less if a connective tissuedisorder such as Marfan or Loeys-Dietz syndrome is present.(371) (Level of Evidence: C)For patients with thoracoabdominal aneurysms and with end-organ ischemia or significant stenosis from atheroscleroticvisceral artery disease, an additional revascularization proce-dure is recommended. (470) (Level of Evidence: B)
t the time of publication of this document, 3 endovas-lar stent grafts have been approved by the US Food andrug Administration only for aneurysms involving thescending thoracic aorta. Although the feasibility andfety of endovascular stent grafting of the descendingrta have been demonstrated for other pathologic condi-
ons including acute and chronic Type B AoD, IMH,AU, acute traumatic aortic transsection, and pseudoan-rysms, these conditions are currently considered “offbel.”There are no published randomized trials that comparee outcomes of endovascular stent grafting with conven-
onal open operation or nonoperative management. Thus,
commendations for use are based principally on obser- pational studies and nonrandomized comparisons of co-orts of patients.
2.2.3.2. Endovascular Versus Open Surgical Ap-roach. The potential advantages of endovascular graft-g over open operation include the absence of a thora-tomy incision and the need for partial or totaltracorporeal circulatory support and clamping of therta, as well as lower hospital morbidity rates and shorterngth of hospital stay.Endovascular grafting may be of particular value intients with significant comorbid conditions (older age,bstantial cardiac, pulmonary and renal dysfunction) whoould be considered poor or noncandidates for openrgery. Patients who are not considered candidates foren surgery but who have undergone endovascular graft-g have substantially poorer long-term outcomes thantients who are reasonable candidates for open operationd are treated with endografts (471). Furthermore, inter-ntion (endovascular stent graft or open surgical graftplacement) for a descending aneurysm has real risks ofortality and morbidity, including the risk of spinal cordchemic injury. All physicians should work collaboratively
ong specialities during the initial decision-making stepsdetermine via consensus whether a particular patient’sthology, risk factors, and projected natural history if
eated medically justify an intervention on the descendingoracic aorta, either a stent graft or an open procedure.There are no data that conclusively demonstrate that theevalence of spinal cord ischemic injury (lower extremity
Figure 33. Elephant trunk procedure. Left,Preoperative disease. Middle, Stage I withreplacement of the ascending aorta and archwith a Dacron graft with the distal graft su-tured circumferentially to the aorta distal tothe left subclavian artery and the free end ofthe graft (“elephant trunk”) within the de-scending aneurysm. Right, Completion of theprocedure using an endovascular stent graftattached proximally to the “elephant trunk”and the distal end secured to a Dacron graftcuff. Images reprinted with permission fromthe Cleveland Clinic Foundation.
ralysis or paresis) is less for endovascular approaches

thdawinopmsuofpo
cuzonoiszoavth
lagrinemca
9.EcaduaninanTininarthagissupe48pr(4cothveMthbyrecopeprin
sepr
thisofsuw(espriwparecopaceagpa
inteInbycededobroppedealunushtiofimarco
lothorpaveotresicawcoHviprvecota
e86 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
an for open surgical repair. Similarly, there are no firmta to indicate that overall costs of medical care are lower
ith endovascular procedures. Although the costs of theitial hospitalization may be lower because of reducederative time and a shorter length of stay, these benefitsay be negated by the cost of the devices, the need forbsequent interventions, and the cost and dissatisfactionrepeated imaging studies, which are necessary in thestoperative period (472,473).Some patients are not suitable candidates for endovas-lar grafting procedures. Absence of suitable “landingnes” above and below the aneurysm (usually 2 to 3 cm ofrmal diameter aorta without circumferential thrombus)a contraindication. A width of the aorta at the landingnes that exceeds the recommended width for the largestailable endovascular grafts (generally 10% to 15% largeran the width of the aorta) is also a contraindication.Lack of vascular access sites to insert the relatively
rge-bore sheaths that are necessary for deployment of theafts is also a contraindication. Severe atherosclerosis andtraluminal thrombus of the aorta may increase the risk ofbolic stroke during manipulation of guidewires and
theters and represents a relative contraindication (474).
2.2.3.3. End-Organ Preservation During Thoracicndograft Implantation. Because aneurysmal diseasen involve any portion of the aorta, organ preservationring repair of either aneurysmal disease or dissection isimportant part of the implant procedure. Aneurysms
volving the aortic arch pose a significant risk to cerebrald upper extremity blood flow with endovascular repair.
he need to cover either the left common carotid or thenominate artery to treat arch aneurysmal disease isfrequent. Intentional coverage of the left subclaviantery is more common, occurring in approximately 50% oforacic endograft implants. Most patients tolerate cover-e of the left subclavian artery without upper extremity
chemia (475–478), but recently several groups haveggested that these patients may be at higher risk ofrioperative stroke and spinal cord ischemic injury (479–1). In the Talent VALOR trial, the need for intentionaleimplant left subclavian artery bypass was only 5.2%82). To minimize the risk associated with intentionalverage of the left subclavian artery, it is recommendedat the patency of the contralateral right subclavian andrtebral arteries be determined preoperatively by CT,R, or invasive angiography. Additionally, verificationat the vertebral arteries communicate at the basilar artery
either transcranial Doppler or angiography is alsocommended. If these steps are taken to ensure that thentralateral posterior circulation is intact, the need torform a left subclavian artery bypass postoperatively toevent symptomatic arm claudication or vertebral basilarsufficiency is infrequent.Spinal cord ischemia leading to paralysis is one of therious potential complications of the thoracic endograft
ocedure. Intercostal arteries are intentionally covered by coe endograft. There is evidence that the risk of spinal cordchemia may be greater when treatment involves coverage
most of the descending thoracic aorta (e.g., from leftbclavian to celiac artery) (483). Additionally, patientsho have had previous repair of abdominal aneurysmither open or endovascular) are at increased risk forinal cord ischemia and paraplegia (484). In 1 study, the
sk of spinal cord ischemia was 10% to 12% in patientsith previous abdominal aneurysm repairs and 2% intients who did not have previous abdominal aneurysmpairs (485). In circumstances where it is necessary tover most of the descending thoracic aorta or if thetient has had a previous abdominal aneurysm repair,rebrospinal fluid (CSF) pressure monitoring and drain-e are an important strategy to minimize the risk ofraplegia (486).Treatment of TAAs with an endograft may requiretentional coverage of the celiac and/or superior mesen-ric arteries to achieve a seal at the distal attachment site.
these instances, a superior mesenteric-to-celiac arterypass graft or an aorta-to-superior mesenteric and/orliac artery bypass graft has been used as a first-stagebranching procedure before proceeding with the en-graft implant (Figure 34). However, risk of the de-anching operation may be no lower than conventionalen repair, and therefore these operative approaches arerformed selectively (487). Fenestrated grafts are invelopment and are undergoing clinical trials. Roselli et(488) published initial results in the first 73 patientsdergoing in situ endovascular repair of extensive TAAsing a branch endograft with promising results in a
igh-risk population. With careful attention to preserva-on of blood flow to the mesenteric vessels, the incidencemesenteric ischemia with endograft implants is approx-ately 3% (482). Most instances of mesenteric ischemia
e the result of emboli rather than malperfusion owing toverage or occlusion of a mesenteric vessel.AoDs pose a complex situation for intestinal, renal, orwer extremity perfusion, as the branches of the aorta ine abdominal cavity may be perfused from either the truefalse lumen. Often, both the true and false lumens aretent and some of the visceral, renal, or lower extremityssels are fed by one channel and the remainder by theher. Thus, the operator must consider how blood flowaches vital organs in the abdominal cavity before con-dering treatment of an AoD with an endograft. In mostses, where descending thoracic dissections are treatedith an endograft, the important treatment principle is tover the proximal entry tear obliterating the false lumen.owever, if the false lumen supplies blood flow to thesceral vessels, blood flow to these organs may be com-omised after endograft implantation. Stenting of thessels at risk from the true lumen or establishing flowmmunication between true and false lumen more dis-lly with a fenestration procedure may prevent such
mpromise. In cases of acute Type B AoD treated with
enfaww(4
9.PdowisregrhsuacIntiblth(sth
Tve
topeSV8%remveT3%
toanrecrofvecoocre1.imseinry
ouan
Filesumgara
Ta
Ty
I
II
III
IV
V
e87JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
dografts, coverage of the proximal entry site into thelse lumen may result in healing of the tear downstreamith restoration of blood flow from the true lumenithout the need for adjunctive fenestration procedures90).
2.2.3.4. Periprocedural Complications of Endograftrocedures. The acute complications of thoracic en-graft procedures are related to problems with access and
ith device implantation. Vascular access is a substantialsue with thoracic endograft procedures. The sheathquired to deploy endovascular grafts is size 20 French oreater and can be up to size 25 French. Many patients
ave femoral arteries that are too small to accommodatech large sheaths. Use of the iliac artery or the aorta forcess is required in approximately 15% of the patients.fection at the access site is not an infrequent complica-
on. Bleeding complications are less frequent. Averageood loss in the Talent VALOR trial was 371 mL, ande need for transfusion in the STARZ TX2 clinical trialtudy results on the Zenith TX2 Endovascular Graft for
gure 34. Schema of TAA treated with initial left iliac artery–to–ft renal artery–to–superior mesenteric artery bypass graft andbsequent placement of a thoracoabdominal endograft. Proxi-al superior mesenteric artery and left renal arteries were li-ted. SMA indicates superior mesenteric artery; and TAA, tho-coabdominal aneurysm. Adapted from Flye et al (489).
e Thoracic Aortic Aneurysms) was 3% (469,482). ba
hromboemboli to mesenteric, renal, or lower extremityssels can also occur (491).Major adverse events related to the device occur in 10%12% of patients in the initial 30-day perioperative
riod. Stroke was observed in 2.5% of the patients in theTARZ TX2 clinical trial (469) and 3.6% in the TalentALOR trial (482). It has been reported to be as high as
in other studies (474,492). Most strokes occur as asult of atheroemboli from the transverse aortic arch withanipulation of the guidewires and device in the archssels (474). Paraplegia varied from 1.3% in the STARZX2 clinical trial to 1.5% in the Talent VALOR trial to
in the TAG trial (469,482,493).Cardiac complications, principally MI, occur rarely (2%4%) (469,482). Cardiac tamponade or rupture is rare
d may be caused by either the stiff guidewires that arequired to deliver the devices or excessive afterloadeated by the balloons that are inflated to produce a sealthe graft to the aortic wall. Ventricular tachycardia or
ntricular fibrillation has been reported (469). Pulmonarymplications include postoperative pneumonias, whichcur in less than 5% of patients. Acute renal failurequiring dialysis is also uncommon, reported to occur in3% of patients in the Talent VALOR trial (482). Deviceplant infection is exceedingly rare and has been ob-
rved mainly in situations where the device was implantedan infected medium emergently (i.e., mycotic aneu-
sms or aortoenteric fistulae) (482).Endoleak is defined as the persistence of blood flowtside the lumen of the endoluminal graft but within theeurysm sac, based on imaging. Endoleaks are classified
ble 14. Classification of Endoleaks
pe Cause of Perigraft Flow Sequelae and Treatment Strategy
Inadequate seal atproximal and/or distalgraft attachment site
Systemic arterial pressure transmitted tothe aneurysm sac, leading to expansionand rupture. Should be repaired when
diagnosed.
Retrograde aorticbranch arterial blood
flow into aneurysm sac
May spontaneously thrombose. Ifaneurysm is stable or shrinking,
observe. If aneurysm is expanding,embolic occlusion of branch artery
indicated but often difficult.
Structural failure ofendograft (e.g., stent
graft fractures, holes infabric, junctional
separations)
Systemic arterial pressure transmitted tothe aneurysm sac, leading to expansionand rupture. Should be repaired when
diagnosed.
Stent graft fabricporosity
Noted at time of implantation andusually resolved with reversal of
anticoagulation.
Expansion of aneurysmwithout demonstrableendoleak, also called
“endotension”
Reline the endograft with a secondendograft.
Adapted from Veith et al (494).
sed on the source of blood flow (Table 14).

tisystdowov(3inreTththocst
cltitiEfrtamat50inin
angrdetrneritaarcowreendointhvean
trandola(2riancotrdi
suthenunop
thforemwremlotrengrYen
gratin5%15du
9.retian
TaRe
En
Pe
Ac
Ch
Ac
Su
Ch
De
Ar
Th
e88 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
Perforation or dissection of the aorta at the implanta-on site is infrequent but usually reported with stentstems that have uncovered or bare proximal attachmentents (495–499). Involution or infolding of the en-grafts may occur and has been most frequently reported
ith grafts applied to a relatively small aorta whereersizing can be substantial, especially in trauma cases66,500,501). Infoldings can also occur when there isadequate conformity of the device to the aortic wall in agion of marked curvature or “beaking” (see Figure 27).his leads to collapse of the endograft, gross endoleak, ande potential for acute occlusion of flow to the descendingoracic aorta. It can be prevented (or managed after itcurs) with implantation of a reinforcing stainless steelent at the proximal leading edge of the implant (500).Late complications of thoracic aortic endografting in-
ude endoleaks, continued aneurysm growth, metal fa-gue and stent fracture and kinking, detachment, migra-on, perforation, and infection of the implanted device.ndoleaks occur in 10% to 20% of patients (482). Theequency is greatest in the first month following implan-tion and declines over the ensuing 5 years (502). Theost frequent type of endoleak is Type IA, or proximaltachment site failure (see Section 8.6) (469,482,503–5). Migration occurs infrequently—at 1-year follow-up0.4% of cases in the TAG clinical trial and 3.9% of casesthe Talent VALOR trial (469,482,506).Late perforations of the aorta by the endograft can occurd are common with the use of oversized grafts and/orafts with bare or uncovered stents (507,508). Most latevice complications such as endoleak and migration are
eatable with implantation of graft extensions. The overalled for repeat interventions to maintain endograft integ-
ty is 6% to 7%, most commonly in the form of implan-tion of an extension cuff. Conversions to open operatione rarely needed (1% to 2%) (476,480,505,509,510). Latemplications (9 to 24 months) include stent fractures,hich are often asymptomatic (511). There are caseports of fractures leading to endograft dysfunction,doleak, migration, and/or embolization (512). En-graft infection, usually as a result of an ongoing systemicfection, or as a result of infected structures adjacent toe graft (513,514), is uncommon, but when it occurs, it isry difficult to eradicate without explantation of the deviced, without explantation, can lead to aortic rupture (515).The experience with the use of endografts for the
eatment of acute descending AoD is limited. A meta-alysis of 609 published cases suggests that when en-grafts are used, mortality is slightly higher (5.3%) and
te conversions to open procedures are more frequent.5%) than data reported for treatment of aneurysms. Thesk of major complications including stroke, paraplegia,d aneurysm rupture appears to be similar in bothnditions (516). A complication unique to endografteatment of acute Type B dissections is conversion of the
ssection to a retrograde Type A dissection, creating a virgical emergency (480,517). Until and unless this life-reatening complication is understood and eliminated,dograft treatment of acute Type B dissections should bedertaken at institutions with a team qualified to performen aortic surgery.In the absence of Level A or Level B evidence regardinge relative efficacy of open and endovascular proceduresr treatment of descending aortic aneurysms, no firmcommendations can be made regarding the optimalethod of treatment. Among comparable patients treatedith either open or endovascular procedures, the midtermsults can be anticipated to be equivalent. The earlyortality advantage of endovascular procedures may best during follow-up such as that seen with endovasculareatment of AAAs (518,519). The long-term durability ofdovascular stent grafts is uncertain; currently, availableafts may have a durability of no more than 10 years.ounger patient age may be a relative contraindication todografting.There are no data to indicate that endovascular stentafting should be performed in patients with asymptom-ic descending aortic aneurysms that are less than 5.5 cmdiameter, because the risk of operation (approximately) exceeds the risk of rupture or dissection (371) (Table). Undoubtedly, as new iterations of devices are intro-ced, these guidelines will change.
2.2.3.5. Open Surgical. Diseases of the aorta thatquire extensive thoracoabdominal surgical or interven-onal approaches fall into 3 large groups: 1) degenerativeeurysms, 2) AoD resulting in subsequent aneurysms or
ble 15. Summary of Society of Thoracic Surgeonscommendations for Thoracic Stent Graft Insertion
tity/Subgroup ClassificationLevel ofEvidence
netrating ulcer/intramural hematoma
Asymptomatic III C
Symptomatic IIa C
ute traumatic I B
ronic traumatic IIa C
ute Type B dissection
Ischemia I A
No ischemia IIb C
bacute dissection IIb B
ronic dissection IIb B
generative descending
�5.5 cm, comorbidity IIa B
�5.5 cm, no comorbidity IIb C
�5.5 cm III C
ch
Reasonable open risk III A
Severe comorbidity IIb C
oracoabdominal/severe comorbidity IIb C
Reprinted from Svensson et al (371).
sceral ischemia, and 3) occlusive disease of the visceral

arsyisveabthimpawouwpatucopa3%
CprTdeTTIVabof
yeHpacoTCon
daanhy
9.rapaaoanbehtiattiwmte
arabthdu
lathvianar
9.naacdoApaanco(2aopacomism
1P
1Phnostinsutoteinthwsihianstca(5
1AMMthanbeinviad
e89JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
teries. Selection of patients for repair is based onmptoms, risk of death from rupture, and end-organchemia, provided associated comorbidity does not pre-nt surgical repair. In patients with lower chest or upperdominal pain, CT or MR is performed to determine ife patient has a contained rupture, leak, or an aneurysmpinging on surrounding structures that may be causingin. The perioperative risk of death is approximately 80%
ith emergency surgery; a few patients will recover with-t a major complication limiting quality of life, and few
ill be long-term survivors because of comorbid disease. Intients with pain from compression of surrounding struc-res, if comorbid disease is not a factor, results arensiderably better with a 10% to 20% risk of death. Intients undergoing elective surgery, the risk of death is
to 10%, depending on the extent of repair.The extent of repair for TAA is classified by the
rawford types: Type I is a repair that extends from theoximal descending aorta above T6 to the renal arteries;ype II, the highest risk group, extends from the proximalscending aorta above T6 to below the renal arteries;ype III extends from the distal descending aorta below6 to below the diaphragm for variable extents; and Type
extends from the diaphragm and involves most of thedominal aorta. This classification correlates with the riskparalysis, renal failure, and death.Open surgical repair of TAA improved over the past 15ars, particularly on preventing postoperative paralysis.istorically, one of the most serious complications wasralysis, either paraparesis or paraplegia, caused by spinalrd injury whose risk is for Type I TAA repair, 15%; forype II, 30%; Type III, 7%; and for Type IV, 4% (381).urrent risk of paralysis is 3% to 5%, depending somewhat
the extent of repair (381,382,520–526).The risk of renal failure may be reduced by preoperativey admission, fluid hydration starting the day before surgery,d the addition of bicarbonate to the hydration regimen andpothermia protection during the operative procedure.
2.2.3.6. End-Organ Preservation During Open Tho-coabdominal Repairs. For thoracoabdominal aortic re-irs done in combination with proximal repairs of thertic arch, the key vital end organs to protect are the heartd brain. Flooding the field with CO2 appears to beneficial (527,528). When the aortic arch requires repair,
ypothermic circulatory arrest is usually required. Protec-on of the brain involves ensuring that calcium plaques orheromata are not disturbed to prevent brain emboliza-on. The temperature and where it is best measured, athich circulatory arrest is commenced, are debated butost large series have recommended circulatory arrest at amperature below 20°C (211).Perfusion of the celiac artery or superior mesenterictery does not appear to be needed to protect thedominal organs in most patients where moderate hypo-ermia (30° to 32°C) is used. Protection of the left lung
ring left thoracotomy repairs is important to avoid jucerations and bleeding into the parenchyma. Deflation ofe left lung may be of benefit. However, disruption of thesceral pleura with attendant complications of bleedingd air leak may be unavoidable, particularly if adhesionse present due to prior surgery or inflammatory changes.
2.2.3.7. Aortic Dissection With Malperfusion. Re-l, mesenteric, lower extremity, or cord malperfusioncompanies up to one third of acute AoD and roughlyubles mortality (248,529,530). In the case of Type A
oD with malperfusion, there is controversy over whethertient outcomes are improved by first repairing the aortad then treating persistent malperfusion (531) or by firstrrecting the malperfusion and then repairing the aorta47,532). The general consensus is to first repair therta, because this will correct malperfusion in mosttients. In the case of Type B AoD, there is a generalnsensus that medical management should be supple-ented by open or endovascular intervention when thereevidence for renal, mesenteric, lower extremity, or cordalperfusion (248,490,533).
0. Special Considerations in Pregnantatients With Aortic Disease
0.1. Effects of Pregnancy on the Aortaysiologic effects of pregnancy may have a profound effectt only on aortic stress but potentially on arterial ultra
ructure as well. The pregnant state is characterized bycreases in maternal blood volume, heart rate, blood pres-re, stroke volume, and cardiac output (534,535). Takengether, the combined effects lead to greater arterial wallnsion as well as intimal shear forces. These changes beginthe first and second trimesters but are most notable in the
ird trimester and peripartum period. Whether arterial walleakening itself occurs during pregnancy remains controver-al. Arterial dissection and/or rupture may occur with theghest incidence in the third trimester (approximately 50%)d peripartum period (33%). In one of the few prospective
udies of pregnant patients with Marfan syndrome, 4.4% ofrefully monitored patients developed aortic dissection34). In unmonitored patients, the risk is likely higher.
0.2. Epidemiology of Chronic and Acuteortic Conditions in Pregnancyarfan syndrome, Ehlers-Danlos syndrome, and other non-arfan aortic disease may manifest during pregnancy. Al-ough clearly rare, it has been estimated that half of AoDd/or ruptures in women younger than 40 years of age haveen associated with pregnancy (536). Most dissections occurthe ascending aorta, although dissection or rupture of
rtually any artery in the body has been described. Indition, pregnancy-related expansion of the sinotubular
nction may lead to aortic valve insufficiency.
1A
10MCL
1.
2.
3.
4.
5.
CL
1.
CL
1.
Inprlemdihahaprdirepehidu
1APrvaanse
dulapeunao
mofwinananduaghydisechacundale
1A
1aACL
1.
CL
1.
1AonulplthcostcayeM50isthPpest
e90 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
0.3. Counseling and Management of Chronicortic Diseases in Pregnancy
.3.1. Recommendations for Counseling andanagement of Chronic Aortic Diseases in Pregnancy
ASS I
Women with Marfan syndrome and aortic dilatation, as well aspatients without Marfan syndrome who have known aorticdisease, should be counseled about the risk of aortic dissec-tion as well as the heritable nature of the disease prior topregnancy. (74,91) (Level of Evidence: C)For pregnant women with known thoracic aortic dilatation or afamilial or genetic predisposition for aortic dissection, strictblood pressure control, specifically to prevent Stage II hyper-tension, is recommended. (Level of Evidence: C)For all pregnant women with known aortic root or ascendingaortic dilatation, monthly or bimonthly echocardiographic mea-surements of the ascending aortic dimensions are recom-mended to detect aortic expansion until birth. (Level of Evi-dence: C)For imaging of pregnant women with aortic arch, descending,or abdominal aortic dilatation, magnetic resonance imaging(without gadolinium) is recommended over computed tomo-graphic imaging to avoid exposing both the mother and fetusto ionizing radiation. Transesophageal echocardiogram is anoption for imaging of the thoracic aorta. (Level of Evidence: C)Pregnant women with aortic aneurysms should be deliveredwhere cardiothoracic surgery is available. (Level of Evi-dence: C)
ASS IIa
Fetal delivery via cesarean section is reasonable for patientswith significant aortic enlargement, dissection, or severeaortic valve regurgitation. (91) (Level of Evidence: C)
ASS IIb
If progressive aortic dilatation and/or advancing aortic valveregurgitation are documented, prophylactic surgery may beconsidered. (537) (Level of Evidence: C)
this regard, risk of major aortic complications duringegnancy appears to be low when the aortic root diameter isss than 4.0 cm (538). Such individuals may have one orore successful pregnancies. For patients with an aorticameter greater than 4.0 cm and Marfan syndrome, half willve come to prophylactic surgery during pregnancy, willve a rupture, or will have life-threatening growth. Optimaleventive therapy in the pregnant woman with known aorticsease includes use of beta blockers to control heart rate andduce shear stresses, particularly in the third trimester andripartum period. Both angiotensin-converting enzyme in-bitors and angiotensin receptor blockers are contraindicatedring pregnancy.
0.4. Evaluation and Management of Acuteortic Syndromes During Pregnancyegnant women with Marfan syndrome, bicuspid aorticlve and ascending aneurysms, Ehlers-Danlos syndrome,d non-Marfan familial thoracic aortic aneurysm and dis-
ction may present with acute aortic syndromes at any point prring the pregnancy but are particularly prone to do so in thest trimester, during delivery, or in the early postpartumriod. Such women may have no knowledge of theirderlying aortic condition until presentation with their acutertic problem.Obviously, acute AoD poses a huge risk for both theother and the unborn child. Optimal treatment parallels thatnonpregnant women but with the added complication of
hen and how to deliver the child. Optimal care includesvolvement with a high-risk maternal-fetal team along with
aortic specialty team capable of medical, percutaneous,d surgical aortic treatment. For Type A AoD occurringring the first or second trimester, urgent surgical repair withgressive fetal monitoring is preferred. Fetal loss duringpothermia and cardiopulmonary bypass is common. Whenssection complicates the third trimester, urgent cesareanction followed by aortic repair appears to offer the bestance for survival for the unborn child and the mother. Forute arch or Type B AoD, medical therapy is preferredless percutaneous stent grafting or open surgery is man-ted by malperfusion, aortic rupture, or subacute aorticaking (539).
1. Aortic Arch and Thoracic Aortictheroma and Atheroembolic Disease
1.1. Recommendations for Aortic Archnd Thoracic Aortic Atheroma andtheroembolic DiseaseASS IIa
Treatment with a statin is a reasonable option for patients withaortic arch atheroma to reduce the risk of stroke. (540) (Levelof Evidence: C)
ASS IIb
Oral anticoagulation therapy with warfarin (INR 2.0 to 3.0) orantiplatelet therapy may be considered in stroke patients withaortic arch atheroma 4.0 mm or greater to prevent recurrentstroke. (Level of Evidence: C)
1.2. Clinical Descriptionortic arch atheroma is a risk factor for ischemic stroke based
autopsy (541,542), TEE (543–548), and intraoperativetrasonographic studies (549) (Figure 35). In particular,aques 4 mm or greater in thickness proximal to the origin ofe left subclavian artery are associated with stroke andnstitute one third of patients with otherwise unexplained
roke (542). These patients, even on antiplatelet therapy,rry a risk of recurrent ischemic stroke as high as 11% at 1ar, and the risk of a new vascular event (ischemic stroke,I, peripheral event, and vascular death) is 20%, 36%, and% at 1, 2, and 3 years, respectively (550). The RR of new
chemic stroke was 3.8 (95% CI 1.8 to 7.8, P�0.002), andat of new vascular events was 3.5 (95% CI 2.1 to 5.9,�0.001), independent of carotid stenosis, atrial fibrillation,ripheral artery disease, or other risk factors (550). Other
udies showed that aortic arch plaques were independent
edictors of recurrent strokes, MI and vascular death
(5ri
etasgr30inanreuslean(5prnere18stis
1RagidfutoortioplniwmthnacaCem
1Mpl
in(5plinofseriasorpltrpr
agad
totrinaslape
ancopa
agplinclplclfem
mtehanoatpofluplye
1Tpapl
11Man
Fi
e91JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
51–553). Patients with noncalcified plaques were at highersk for recurrent vascular events (554).Regarding the natural history of aortic arch atheroma, Senal (555) noted progression in 29% and regression (definedan increase or decrease in plaque thickness by 1 grade or
eater, respectively) in 9%. Montgomery et al (556) reportedpatients with moderate-to-severe aortic plaque noted on
itial bi/multiplanar TEE as part of a workup for cardiac orembolic event. Over a mean of 1 year, progression was
ported in 23% and regression in 10%. Pistavos et al (557)ed monoplanar TEE in 16 patients with familial hypercho-sterolemia taking pravastatin to show progression in 19%d regression in 38% over 2 years. Geraci and Weinberger58), using supraclavicular B-mode ultrasonography of theoximal aortic arch in 89 patients evaluated for transienturologic symptom, noted a progression rate of 19% and agression rate of 18% over a mean of 7.7 months (range 3 to
months). Sen et al (559) confirmed that in patients withroke/TIA, aortic arch atheroma progression over 12 monthsassociated with more vascular events.
1.3. Risk Factorsisk factors for the development of aortic atheroma includee, sex, heredity, hypertension, diabetes mellitus, hyperlip-emia, sedentary lifestyle, smoking, and endothelial dys-nction. Other factors include elevated levels of inflamma-ry markers (i.e., serum C-reactive protein), homocysteine,lipoprotein (560,561). Risk factors for embolic complica-ns include inflammation, shear forces of hypertension,
aque hemorrhage aneurysm formation, and iatrogenic ma-pulation. The likelihood of embolization is also increasedith complex aortic plaque, defined as plaque that containsobile thrombi or ulcerations or is 4 mm or greater inickness (562). Plaques with a larger lipid core, a predomi-nce of macrophages, a thin fibrous cap, and a lack oflcification are more “vulnerable” to disruption or rupture.alcified plaques are more stable and less likely to result in
gure 35. Ultrasound image of aortic atheroma.
bolic syndromes (562,564–565). ag
1.4. Diagnosisethods of imaging the aortic arch to detect and/or measureaque include:Transesophageal Echocardiography. TEE can provideformation of plaque mobility, ulceration, and composition66), as well as details on the anatomic relationship of theaque to the origin of the great vessels (69) with excellentterobserver and intraobserver reliability (567). LimitationsTEE in patients with stroke include the need for conscious
dation, patient cooperation for swallowing the probe, andsk of structural damage (566). A small portion of thecending aorta is masked by the tracheal air column near theigin of the innominate artery, with an estimated 2% ofaques being missed (568). Multiplanar probes may reduceacheal shadowing seen with monoplanar and biplanarobes (569).Transthoracic Echocardiography. TTE can usually im-e the aortic root and proximal ascending aorta but cannotequately assess aortic arch plaque (570,571).Epiaortic Ultrasonography. Epiaortic imaging is usefuldetect aortic arch plaque in the operative setting when the
ansducer may be placed directly over the aortic arch. Theformation may be used to select operative techniques suchoff-pump coronary artery bypass grafting to avoid cannu-
tion or cross-clamping of the aorta and reduce risk ofrioperative strokes (572,573).Contrast Aortography. The risk of invasive angiographyd the need for contrast injection and radiation makentrast aortography less useful to assess aortic arch plaque intients with stroke (574).Magnetic Resonance Imaging. MR has been validatedainst TEE for detection and measurement of aortic archaque (80% overall agreement) (568,575). It has limited usepatients who are obese, have metallic implants, or are
austrophobic. Contrast MR angiography underestimates theaque thickness but can identify morphologic features in-uding calcification, fibrocellular tissue, lipid, thrombus, andatures used to detect plaque stability and may be used toonitor aortic arch plaque progression and regression (572).Computed Tomography. CT can reliably detect andeasure protruding aortic arch plaques (568,576) and is thest of choice for detecting vascular calcification. Nonen-nced dual-helical CT may underestimate the amount ofncalcified plaque and mobile thrombus that presumably ishigh risk for embolization (568). In conjunction with
sitron emission tomography it can be used to localizeorodeoxyglucose uptake by the plaque, identifying active
aques and unstable plaques (577), but its clinical utility hast to be established.
1.5. Treatmenthere is no definitive therapeutic regimen for this high-risktient group because no randomized trial has been com-eted.
.5.1. Anticoagulation Versus Antiplatelet Therapyobile aortic atheroma have been noted to disappear duringticoagulant therapy (546) or with the use of a thrombolytic
ent (578). However, there is concern about the use of
wthbotioenthbomwthth13A
inpaawtrphofriplth1.ad(PpestTemasapareev0.mwem
paratrreCwst2.mev
11Tloatanplw
stLstthpltiodi
seobonfoprtioTinstditoao
11Awomprenpelimcasushemoculphof
1
Vcestasofdi
bechfinvainclin(F
retio
e92 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
arfarin in patients with aortic atheroma because of theeoretical risk of plaque hemorrhage resulting in atheroem-li syndrome (i.e., blue toes, renal failure, intestinal infarc-n) (579). Anticoagulation has been associated with wors-ing (580,581), as well as improvement of an aorticrombus on anticoagulation in a patient with the atheroem-li syndrome (582). Cholesterol emboli have been docu-ented on skin, muscle, and renal biopsy samples in patientsith aortic arch atheroma seen on TEE (553,583). However,e risk of clinical atheroemboli syndrome during warfarinerapy in such patients appears to be low (only 1 episode in4 patients according to the SPAF [Stroke Prevention in
trial Fibrillation] trial) (562).Three reports shed light on the potential benefit of warfarinpatients with aortic arch atheroma. The first described 31tients with mobile lesions in the aorta on TEE (585) wherehigher incidence of vascular events was seen in patientsho were not treated with warfarin compared with thoseeated with warfarin (at the discretion of the referringysicians) (45% versus 5%). In the SPAF randomized trialpatients with “high-risk” nonvalvular atrial fibrillation, the
sk of stroke at 1 year in 134 patients with complex aorticaque was found to be reduced from 15.8% (11 events) inose treated with fixed low-dose warfarin plus aspirin (INR2 to 1.5) to only 4% (3 events) in those treated withjusted-dose warfarin (INR 2.0 to 3.0), a 75% RR reduction�0.02) for patients with atheromas who received “thera-utic range” anticoagulation (562). A third observational
udy reported on 129 patients with aortic arch atheroma onEE performed to look for a source of cerebral or peripheral
bolization (586). Treatment with oral anticoagulation,pirin, or ticlopidine was not randomly assigned. There wassignificant reduction in the number of embolic events intients with plaques greater than or equal to 4 mm whoceived oral anticoagulants (0 events in 27 patients versus 5ents in 23 patients treated with antiplatelet agents) (OR06, 95% CI 0.003 to 1.2, P�0.016). For patients withobile lesions, there was a significant reduction in mortalityhile on anticoagulants, although the trend toward fewerbolic events did not reach statistical significance in this group.These 3 reports suggest that warfarin is not harmful intients with aortic arch atheroma and may reduce stroketes. However, these studies are not randomized trials ofeatment for patients with atheromas, and the numbers arelatively small. The current ARCH (Aortic Arch Relatederebral Hazard) trial is an open-label trial where patientsith aortic arch atheroma (4 mm or greater) and nondisablingroke are being assigned to oral anticoagulation (target INR0 to 3.0) versus aspirin (75 mg/d) plus clopidogrel (75g/d) and followed longitudinally for recurrence of vascularents.
.5.2. Lipid-Lowering Agenthere are no randomized trials to support specific lipid-wering drug therapy for a patient with stroke caused byheroembolism. However, 2 randomized studies of low-dosed higher-dose statin in patients with aortic and/or carotidaques showed significant regression in plaque seen on MR,
hich in 1 study was related to LDL cholesterol level but not neatin dosage (587) and, in the other study, was related to bothDL lowering and the statin dosage (588). It seems likely thatatin therapy decreases the risk of stroke. Mechanisms foris effect may involve pleiotropic effects of statins, includingaque regression, plaque stabilization, decreased inflamma-n, and inhibitory effects on the coagulation cascade at
fferent levels.No randomized trial on the use of statins in patients withvere aortic plaque has been published. However, in anservational study of 519 patients with severe aortic plaqueTEE (540), statin use was associated with an RR reduction
r ischemic stroke of 59%. Statins have reduced bothimary and secondary stroke in a variety of patient popula-ns (589,590). Hence, a majority of patients with stroke and
IA with identified aortic plaque already have other strongerdications for statin therapy (409). Recommendations foratins are noted for other manifestations of atheroscleroticseases (409) (see Section 9.2.1.2). Clinical trials are neededdetermine the effects of statins in patients with severe
rtic atheroma and risk of atheroembolism.
.5.3. Surgical and Interventional Approachesortic arch endarterectomy has been attempted for patientsith thromboembolism originating from aortic arch ather-
a. Although successful in a handful of case reports, thisocedure resulted in a relatively high rate (34.9% withdarterectomy versus 11.6% without endarterectomy) ofrioperative stroke and mortality when it was performed toit stroke during cardiac surgical procedures requiring
rdiopulmonary bypass (coronary bypass surgery and valvergery) (545). Covered stents offer the potential advantage ofielding severely diseased aortic segments to prevent furtherbolization. However, periprocedural embolization may
cur during diagnosis or interventional endovascular manip-ations. There is insufficient evidence to recommend pro-ylactic endarterectomy or aortic arch stenting for purposesstroke prevention.
2. Porcelain Aorta
ascular calcification occurs in the media and represents antral component of atherogenesis, typically signaling long-anding inflammation. The amount of calcification directlysociates with the extent of atherosclerosis, and the presence
aortic calcium predicts the presence of coronary heartsease (443).With severe atherosclerosis of the aorta, calcification maysevere and diffuse, causing an eggshell appearance seen onest x-ray or CT (444). Also termed “porcelain aorta,” thisding is usually noted during operation for coronary heart orlvular heart disease at the time of surgery. The calcificationterferes significantly with cannulation of the aorta, cross-amping, and placement of coronary bypass grafts, increas-g the risk of stroke and distal embolism significantlyigure 36).In these patients, direct manipulation of the aorta maysult in an unrepairable aortic injury and/or distal emboliza-n. Surgeons have used several techniques to reduce adverse
urologic events in these patients: internal aortic balloon
octecamat
1
Nrecisu(6
ofthpr
disythdishaor(6comno
1SA
1PCL
1.
2.
3.
CL
1.
e93JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
clusion (as apposed to aortic cross-clamping), a “no-touch”chnique to avoid the ascending aorta, alternate locations fornnulation or coronary bypass graft anastomoses, replace-ent of the ascending aorta, and intra-aortic filtration ofherosclerotic debris (591–599).
3. Tumors of the Thoracic Aorta
eoplasms of the thoracic aorta are usually secondary andlated to contiguous spread of adjacent primary malignan-es, particularly lung and adjacent primary malignancies, orbsequent metastases, particularly lung and esophagus00–603).Primary neoplasms of the thoracic aorta are rare. A reviewthe literature between 1873 and 2002 collated a total of 53
oracic and 10 thoracoabdominal tumors with most lesionsotruding into the aortic lumen (604) (Table 16).Metastatic disease is often demonstrated at the time ofagnosis of primary aortic neoplasms, so that constitutionalmptoms of malaise, fatigue, weight loss, and nausea may bee presenting complaints. Other presentations can includestal arterial embolization (with histopathologic examinationowing neoplasm or identified by imaging techniques duringsearch for an embolic source) (604–606). AoD mayiginate in the area of the neoplasm or the aortic occlusion07). Resection and reconstruction of the segment of aortantaining the neoplasm have been described, but becauseost patients present with metastatic disease, overall prog-
sis is poor (608).4. Perioperative Care for Openurgical and Endovascular Thoracicortic Repairs
4.1. Recommendations forreoperative EvaluationASS I
In preparation for surgery, imaging studies adequate to estab-lish the extent of disease and the potential limits of theplanned procedure are recommended. (Level of Evidence: C)Patients with thoracic aortic disease requiring a surgical orcatheter-based intervention who have symptoms or other find-ings of myocardial ischemia should undergo additional studiesto determine the presence of significant coronary artery dis-ease. (Level of Evidence: C)Patients with unstable coronary syndromes and significantcoronary artery disease should undergo revascularization priorto or at the time of thoracic aortic surgery or endovascularintervention with percutaneous coronary intervention or con-comitant coronary artery bypass graft surgery. (Level of Evi-dence: C)
ASS IIa
Additional testing is reasonable to quantitate the patient’scomorbid states and develop a risk profile. These may includepulmonary function tests, cardiac catheterization, aortogra-
Figure 36. Porcelain aorta. Top left and right, PA andlateral chest x-ray show an anterior mediastinal masswith curvilinear calcifications most likely representingthe wall of an ascending aortic aneurysm. Bottom left,CT scan slice at the level of the right pulmonary arteryconfirms a 10-cm aneurysm of the ascending aortawith dense mural calcifications. Bottom right, A maxi-mum intensity projection in the oblique sagittal planebetter demonstrates the fusiform aneurysm beginningat the sinotubular ridge and extending into the aorticarch. Dense mural calcification extends into the proxi-mal descending aorta. CT indicates computed tomo-graphic imaging; and PA, posteroanterior.
phy, 24-hour Holter monitoring, noninvasive carotid artery

2.
CL
1.
Prneplprthofinancanearpeflotivizrori
msuesco
raofco
inHadhytiopaareanisabestthludadelikda
14Mstafasishiandica
hacosubere
wreinstth(6grefhaCtiothsireofinth
TaRe
Hi
Sa
M
An
Le
Fib
M
Fib
He
He
M
Ao
M
En
Fib
Fib
e94 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
screening, brain imaging, echocardiography, and neurocogni-tive testing. (Level of Evidence: C)For patients who are to undergo surgery for ascending or archaortic disease, and who have clinically stable, but significant(flow limiting), coronary artery disease, it is reasonable toperform concomitant coronary artery bypass graft surgery.(Level of Evidence: C)
ASS IIb
For patients who are to undergo surgery or endovascularintervention for descending thoracic aortic disease, and whohave clinically stable, but significant (flow limiting), coronaryartery disease, the benefits of coronary revascularization arenot well established. (609–611) (Level of Evidence: B)
eoperative evaluation usually includes imaging studiescessary to establish the extent of disease, the limits of theanned procedure, and the clinical risks attendant to theocedure. When the writing committee was polled regardinge extent of usual preoperative laboratory testing, a variety
approaches emerged. In some centers, extensive testingcludes pulmonary function tests (particularly for smokersd those with Marfan syndrome), Holter monitoring, androtid duplex scans. In some centers, brain imaging andurocognitive testing are performed in patients with aorticch disease for whom arch repair or replacement requiring ariod of deep hypothermic circulatory arrest or low pumpw is planned (463). Other centers obtain fewer preopera-e tests and individualize such testing as cardiac catheter-
ation, 24-hour Holter monitoring, brain imaging, and neu-cognitive studies for patients to establish baseline states andsk.In many centers, where the diagnosis of acute AoD is eitherade or highly suspected, patients are immediately taken torgery, and TEE is performed in the operating room to eithertablish or confirm the diagnosis. Most of the writing
ble 16. Neoplasms of the Thoracic Aorta (Collectiveview Incidence)
stologyThoracic Aorta
(N�53)Thoracoabdominal
Aorta (N�10)
rcoma 15 1
alignant fibrous histiocytoma 11 1
giosarcoma 5 0
iomyosarcoma 6 2
rosarcoma 4 0
yxoma 3 1
romyxosarcoma 1 1
mangiopericytoma 2 0
mangioendothelioma 2 0
alignant endothelioma 2 0
rtic intimal sarcoma 0 2
yxosarcoma 0 1
dotheliosarcoma 1 0
romyxoma 0 1
roxanthosarcoma 1 0
Adapted from Oldenburg et al (604).
mmittee believes that the delay to obtain coronary angiog- di
phy was potentially dangerous unless patients had a historycoronary artery bypass graft surgery or a high likelihood ofexisting CAD.Most patients undergoing elective aortic root and ascend-g aortic surgery can be admitted the day of surgery.owever, some of the writing committee members routinelymit patients the day before surgery primarily for fluiddration (using 5% dextrose/0.5 normal saline with addi-nal potassium and sodium bicarbonate at 100 to 120 mL/h),rticularly those who are to have extensive open surgery forch, descending thoracic, or thoracoabdominal aortic dis-se. Preoperative use of acetylcysteine (600 mg by mouth atght and in the morning, or 500 mg in 500 mL of normalline solution over 3 hours before CT or surgery) has alsoen described (612,613). However, the effectiveness of these
rategies has not been tested in a clinical trial. Placement oforacic epidural catheters for postoperative analgesia ormbar spinal drains for CSF drainage is performed on they prior to surgery in some centers. Despite lack of evi-nce, there is concern that neuraxial hemorrhage is moreely if blood returns through the placement needle on they of surgery.
.1.1. Preoperative Risk AssessmentI, low cardiac output, respiratory failure, renal failure, androke are the principal causes of mortality and morbidityter operations on the thoracic aorta, and preoperativesessment of these organ systems prior to elective operationessential (381,441,614–617), especially in patients with astory of MI, angina pectoris, or symptoms of heart failured those older than 40 years. Patients with valvular heartsease are evaluated with echocardiography and cardiactheterization.Elderly patients with thoracic aortic disease are likely tove coexisting CAD. The benefits of prior or concomitantronary revascularization are controversial. Several studiesggested that prior coronary bypass graft surgery was ofnefit to patients undergoing major vascular surgery toduce cardiovascular mortality (618–622).More recent clinical trials comparing outcomes of patients
ith stable CAD treated with optimal medical therapy versusvascularization have not shown any significant reductions
cardiovascular events associated with revascularizationrategies (609–611). Major thoracic aortic surgery falls intoe highest-risk group for cardiac morbidity and mortality23), prompting some writing committee members to ag-essively screen for and treat coexisting CAD, but thefectiveness of such a strategy in patients with stable CADs not been clearly established. For patients with unstable
AD, left main stenosis, or 3-vessel disease, revasculariza-n is generally warranted prior to or concomitant with the
oracic aortic procedure. The use of drug-eluting stents forngle- or double-vessel disease may be problematic becausequired antiplatelet therapies may significantly raise the riskbleeding with the thoracic aortic procedure and withhold-
g antiplatelet therapies clearly increases the risk of stentrombosis.History of smoking and presence of chronic pulmonary
sease are important predictors of postoperative respiratory

cotharchexchad
diaohypeco
neofpherorevprdi
la(3suleorde
1ACL
1.
CL
1.
2.
CL
1.
2.
CsuFoande(6iteseaanpeanantionepe
vegrflu(6an(6paresicaloandeanveaf
14Alotyce
14InsipeAcrthdi
filadby
e95JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
mplications and are frequently present in patients withoracic aortic disease (624). Pulmonary function tests andterial blood-gas analyses help to risk-stratify patients withronic pulmonary disease. If reversible restrictive disease orcessive sputum production is present, antibiotics and bron-odilators should be administered. Cessation of smoking isvisable.Preoperative renal dysfunction is the most important pre-
ctor of acute renal failure after operations on the thoracicrta (617,625,626). Preoperative hydration and avoidance ofpotension, low cardiac output, and hypovolemia in therioperative period may reduce the prevalence of thismplication.To minimize the risk of stroke or reversible ischemicurologic deficits and to determine the potential magnituderisk, duplex imaging of the carotid arteries and angiogra-y of the brachiocephalic arteries is often performed preop-atively particularly in patients with a history of stroke, TIA,other risk factors for cerebrovascular disease (627). How-er, the efficacy of treatment of significant carotid stenosisior to endovascular or open surgery for thoracic aorticsease has not been evaluated in a randomized clinical trial.Although older age is a risk factor for increased early andte death after operations on the thoracic aorta82,441,617,625,627–630), operations can be carried outccessfully with satisfactory outcomes in appropriately se-cted older patients. Emergency operation for aortic ruptureacute dissection is associated with a higher risk of early
ath after operation compared with elective operation (47).
4.2. Recommendations for Choice ofnesthetic and Monitoring TechniquesASS I
The choice of anesthetic techniques and agents and patientmonitoring techniques should be tailored to individual patientneeds to facilitate surgical and perfusion techniques and themonitoring of hemodynamics and organ function. (Level ofEvidence: C)
ASS IIa
Transesophageal echocardiography is reasonable in all opensurgical repairs of the thoracic aorta, unless there are specificcontraindications to its use. Transesophageal echocardiogra-phy is reasonable in endovascular thoracic aortic proceduresfor monitoring, procedural guidance, and/or endovasculargraft leak detection. (631–633) (Level of Evidence: B)Motor or somatosensory evoked potential monitoring can beuseful when the data will help to guide therapy. It is reasonableto base the decision to use neurophysiologic monitoring onindividual patient needs, institutional resources, the urgencyof the procedure, and the surgical and perfusion techniques tobe employed in the open or endovascular thoracic aortic repair.(634,635) (Level of Evidence: B)
ASS III
Regional anesthetic techniques are not recommended in pa-tients at risk of neuraxial hematoma formation due to thien-
opyridine antiplatelet therapy, low-molecular-weight heparins, tioor clinically significant anticoagulation. (636) (Level of Evi-dence: C)Routinely changing double-lumen endotracheal (endobron-chial) tubes to single-lumen tubes at the end of surgicalprocedures complicated by significant upper airway edema orhemorrhage is not recommended. (Level of Evidence: C)
hoice of anesthetic technique is dependent on the plannedrgical interventions and the patient’s comorbid conditions.r placement of endovascular aortic stent grafts, differentesthetic (local, regional, general) techniques have beenscribed, although adequate comparative studies are lacking37–643). Percutaneous placement of catheters with a lim-d incision may be tolerated with local anesthesia anddation. Extensive inguinal dissection or the construction offemoro–femoral bypass may favor either regional or generalesthesia. If surgical dissection is extended into the retro-ritoneum, a higher level of regional anesthesia or generalesthesia is required. If the patient is undergoing localesthesia or regional anesthesia, adequate intravenous seda-n is necessary because of agitation secondary to restless-ss and pain from lying in one position for a prolongedriod of time.Retrospective studies indicate that patients having localrsus regional or general anesthesia for endovascular stentafts tend to have lower use of vasoactive agents and lowerid requirements, shorter intensive care and hospital stays42), earlier ambulation and gastrointestinal function (637),d lower incidence of respiratory and renal complications43). In a large multicenter retrospective study of 5557tients undergoing endovascular aortic repairs (644), 69%ceived general anesthesia, 25% received regional anesthe-a, and 6% received local anesthesia. The incidence ofrdiac complications were significantly lower in both thecal or regional anesthesia group compared with generalesthesia (1.0% versus 2.9% versus 3.7%), and the inci-nce of sepsis was significantly lower in the regionalesthesia group compared with general anesthesia (0.2%rsus 1.0%). Selection bias and complexity of disease likely
fect these results.
.2.1. Temperature Monitoringt most centers, temperature is monitored in at least 2cations that estimate the brain/core (e.g., blood, esophageal,mpanic membrane, nasopharynx) temperature and the vis-ral (e.g., bladder or rectal) temperature (645).
.2.2. Hemodynamic Monitoringvasive arterial pressure monitoring is required in 1 or moretes depending on the surgical plan for cannulation andrfusion, particularly for thoracoabdominal aortic repairs.rterial pressure is universally monitored proximal to aorticoss-clamping sites, but there is institutional variability ine monitoring of distal arterial (aortic) pressure, even whenstal aortic perfusion is performed.Central venous cannulation allows measurement of cardiac
ling pressures, providing a route for vasoactive drug and fluidministration. Femoral venous catheterization is discouragedcurrent central line–associated bloodstream infection preven-
n guidelines, but the literature does not address the subject in
thrifo
mdosusu
14Tdireteapcathog
de
•
•
ex
•
•
14ETwnodivetointhAenseanpativ
dufotede
1ThAbr
exprpuputathmbech(tenratuai
chtutiountuevarAchth
1MACL
1.
TsesepucohethTthvoprblth
enwth
th
e96 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
oracoabdominal surgery (646,647). Nevertheless, many expe-enced centers use short-term catheterization of the femoral veinr volume management during surgery.Pulmonary artery catheterization is performed routinely in
any institutions for thoracic aortic surgery. The literaturees not specifically address the subject of thoracic aorticrgery, but the general perioperative literature does notpport the use of pulmonary artery catheterization (631).
.2.3. Transesophageal EchocardiographyEE is safe (648) and is used to confirm the preoperativeagnoses and detect pericardial or pleural effusions, aorticgurgitation, the extent of dissection, the location of intimalars, the size and integrity of aneurysms, and the presence ofpropriate flow in the true lumen upon commencement ofrdiopulmonary bypass. Current American Society of Anes-esiologists and the Society of Cardiovascular Anesthesiol-ists guidelines for TEE include the following (631):Category I Indications (supported by the strongest evi-nce or expert opinion):
Preoperative use in unstable patients with suspected tho-racic aortic aneurysms, dissection, or disruptions that needto be evaluated quickly.Intraoperative assessment of aortic valve function in repairof AoDs with possible aortic valve involvement.
Category II Indications (supported by weaker evidence orpert opinion):
Preoperative assessment of patients with suspected tho-racic AoDs, aneurysms, or disruption.Intraoperative use during repair of thoracic AoDs withoutsuspected aortic valve involvement.
.2.4. Transesophageal Echocardiography forndovascular Repairs of the Descending Thoracic AortaEE can provide views of the aorta and location of guide-ires and endografts prior to deployment in relation to thermal and diseased thoracic aorta (649,650). TEE hasstinct advantages over angiography by providing exactssel and lesion sizing and localization and can also be usedestimate endograft size and location. Although not imagedall patients, large intercostal arteries have been imaged,
us avoiding inadvertent obstruction by the aortic stent graft.fter stent graft placement, the presence or absence ofdoleaks can be determined by TEE with a high degree ofnsitivity and specificity particularly compared with contrastgiography (632,633,650). Finally, because most of thesetients have severe concomitant cardiac disease, periopera-e TEE allows dynamic assessments of cardiac function.Intravascular ultrasound is used for endovascular proce-res to visualize precise localization of branch arteries andr measurement of aortic and branch artery sizes. Plaques,ars, and saccular aneurysms can also be very accuratelymonstrated.
4.3. Airway Management for Descendingoracic Aortic Repairsdouble-lumen endotracheal tube or various types of endo-
onchial blockers facilitate surgical exposure (651). For setensive surgery of the left thorax, single-lung ventilationovides better surgical exposure, reduces the need forlmonary retraction, may decrease the severity of iatrogeniclmonary contusion, and protects the right lung from con-
mination by blood and secretions. A large descendingoracic aortic aneurysm may compress or distort the leftain bronchus such that left-sided endobronchial tubes mustused with caution. If a right-sided double-lumen endotra-
eal tube is placed, endoscopic confirmation of tube positiono ensure right upper lobe ventilation) is necessary. Forcefuldobronchial tube placement has been associated with tho-cic aortic aneurysm rupture. Therefore, using a differentbe or lung isolation method may be required when severerway distortion is encountered.At the end of surgery, some centers have advocatedanging a double-lumen endotracheal tube to a single-lumenbe to facilitate pulmonary toilet and to avoid the complica-ns associated with tube malposition in the intensive careit. The decision to change the double-lumen endotrachealbe to a single-lumen tube should be made after carefullyaluating the extent of airway edema, as these procedurese associated with significant facial and laryngeal edema.dvanced airway management devices, such as tube ex-anges and video laryngoscopy, may be of benefit; however,ere is no literature addressing this subject.
4.4. Recommendation for Transfusionanagement and Anticoagulation in Thoracicortic SurgeryASS IIa
An algorithmic approach to transfusion, antifibrinolytic, andanticoagulation management is reasonable to use in both openand endovascular thoracic aortic repairs during the periopera-tive period. Institutional variations in coagulation testing ca-pability and availability of transfusion products and otherprothrombotic and antithrombotic agents are important con-siderations in defining such an approach. (652) (Level ofEvidence: C)
horacic aortic surgery is associated with hemorrhage fromveral interrelated causes, including extensive surgical dis-ction, arterial and venous bleeding, hypothermia, cardio-lmonary bypass, fibrinolysis, dilution or consumption ofagulation factors, thrombocytopenia, poor platelet function,parin and other anticoagulants, preoperative antithromboticerapy, and other congenital and acquired coagulopathies.he extensive blood product and fluid requirements of openoracic aortic surgical repairs may exceed the total bloodlume of the patient in the most complicated cases. Clinicalactice guidelines for perioperative blood transfusion andood conservation in cardiac surgery have been published bye STS and the SCA (652).These guidelines do not specifically address open ordovascular descending thoracic aortic repairs, but theriting committee supports treatment strategies provided byese guidelines.Coagulopathies in open descending thoracic aortic andoracoabdominal repairs mirror many of the abnormalities
en in cardiac and thoracic aortic procedures requiring
casitisoganafocceDwvifiberactyacmemcl
epreloadvadofrInacintrwbyaode72caanab
1
14ACL
1.
CL
1.
CL
1.
Aopaomgrthexinpr
forape40tupebygrofbrcicopehy
prhybuincomsiinvalethlasiinheonthbaprpe(2
brimti(6
e97JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
rdiopulmonary bypass. Illig and colleagues (653) reportedgnificantly decreased euglobulin clot lysis times, elevatedsue plasminogen activator levels, elevated tissue plasmin-en activator–to–plasminogen activator inhibitor-1 ratios,d reduced alpha 2-antiplasmin levels within 20 minutester supraceliac cross-clamping, compared with infrarenalclusion, consistent with a primary fibrinolytic state. Vis-ral ischemia may be the condition that initiates fibrinolysis.uring supraceliac occlusion, fibrinolysis was attenuatedhen superior mesenteric artery perfusion was maintaineda a shunt (654). Peripheral ischemia may also result inrinolysis. Within 30 minutes of the onset of acute periph-
al ischemia (with infrarenal aortic occlusion) fibrinolytictivity increased, as demonstrated by an increase in tissue-pe plasminogen activity and a decrease in plasminogentivator inhibitor activity. This increase in tissue-type plas-inogen activity resulted from release of stores from isch-ic vascular tissues (655). Endotoxemia during aortic oc-
usion may also be associated with fibrinolysis (656).To counteract fibrinolysis, the use of lysine analogssilon-aminocaproic acid and tranexamic acid has beenported in cardiac surgery. The epsilon-aminocaproic acidading or bolus dose ranged from 75 to 150 mg/kg, withditional dosing from 12.5 to 30 mg/kg/h infused overrying time periods. For tranexamic acid, loading or bolusse, ranged from 2.5 to 100 mg/kg, with additional dosing
om 0.25 to 4.0 mg/kg/h delivered over 1 to 12 hours (657).a study of 21 adult cardiac surgical patients, the tranexamicid dosing regimen of 10 mg/kg initial dose, followed by anfusion of 1 mg/kg/h resulted in adequate plasma concen-ations defined by in vitro studies to prevent fibrinolysis,ith relatively stable drug levels throughout cardiopulmonarypass (658). Antifibrinolytic therapy for thoracoabdominalrtic surgery with distal perfusion was not associated withcreased bleeding or transfusion in a retrospective cohort ofpatients (659). The strong evidence derived from other
rdiac surgical studies has led to very common use oftifibrinolytic therapy in thoracic aortic surgery, despite thesence of specific evidence in this surgical subset.
4.5. Organ Protection
.5.1. Recommendations for Brain Protection Duringscending Aortic and Transverse Aortic Arch SurgeryASS I
A brain protection strategy to prevent stroke and preservecognitive function should be a key element of the surgical,anesthetic, and perfusion techniques used to accomplishrepairs of the ascending aorta and transverse aortic arch.(660–666) (Level of Evidence: B)
ASS IIa
Deep hypothermic circulatory arrest, selective antegrade brainperfusion, and retrograde brain perfusion are techniques thatalone or in combination are reasonable to minimize brain injuryduring surgical repairs of the ascending aorta and transverseaortic arch. Institutional experience is an important factor inselecting these techniques. (211,615,667–688) (Level of
Evidence: B) mASS III
Perioperative brain hyperthermia is not recommended in re-pairs of the ascending aortic and transverse aortic arch as it isprobably injurious to the brain. (689–691) (Level of Evi-dence: B)
brain protection strategy is an essential component of theerative technique for open surgical repairs of the ascendingrta and/or the aortic arch. Moderate or profound hypother-ia with periods of circulatory arrest and/or selective ante-ade brain perfusion and/or retrograde brain perfusion aree common strategies for achieving brain protection. Theperience and outcomes of the operating surgeon and thestitution are important considerations in selecting a brainotection strategy.Achieving brain hypothermia is nearly universally per-rmed using extracorporeal circulation, with temperaturesnging from 12° to 30°C. Retrograde (via jugular vein) brainrfusion is usually performed at a perfusion pressure of 20 tomm Hg at a mildly or profoundly hypothermic tempera-
re. Antegrade brain perfusion is usually performed at arfusion pressure of 50 to 80 mm Hg and may be instituted
direct cannulation of the brachiocephalic arteries, side-aft anastomosis to the axillary artery, or direct cannulationa portion of graft material that was anastomosed to the
achiocephalic arteries during a period of hypothermicrculatory arrest. The rewarming of a patient followingmpletion of the repair of the thoracic aorta is usuallyrformed at a measured rate so as not to induce brainperthermia.The reviewed literature describes an evolution of brainotection techniques over the past 2 to 3 decades. Deeppothermic circulatory arrest emerged as the first technique,t as a sole method of brain protection, it was limited bycreasing rates of neurologic morbidity, other adverse out-mes, and mortality as the period of arrest exceeded 25 to 45inutes (671,692). Deep hypothermic arrest without perfu-on adjuncts has been successful, especially when arresttervals are less than 40 minutes (693). Subsequently,rious combinations of retrograde brain perfusion and se-ctive antegrade brain perfusion were developed to extende “safe period” of interruption of full extracorporeal circu-tion. Monitoring of brain function and metabolic suppres-on by electroencephalography, evoked potentials, bispectraldex, noninvasive cerebral oximetry, and jugular bulb oxy-moglobin saturation are additional means used to guide theset of extracorporeal circulation interruption for repairinge distal ascending aorta and/or aortic arch. Some centers userbiturates, calcium channel blockers, or steroids for addedotection, but no prospective randomized trials have beenrformed to test the efficacy of pharmacological agents11,459).There is controversy regarding the ability of retrogradeain perfusion to support brain metabolic function and toprove neurologic outcomes, including transient postopera-
ve neurologic dysfunction, stroke rates, and mortality61,671,673–675,694–699). However, this technique can
aintain brain hypothermia (700) and has been associated
wpr
diarpefoWlacothusafarafmthhyreerrewanoususipa
maamhobrbeorFuthhyou
littioanagreco
14DECL
1.
CL
1.
2.
CL
1.
2.
Pacoaore2%hopediac
emaoclpaworthrigrclpaofaorepeopcospdi
mfo
e98 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
ith improved outcomes in the centers where it is used as aimary neuroprotection strategy.Selective antegrade brain perfusion may be provided byrect cannulation of 1 or more of the brachiocephalicteries, which permits brain perfusion with minimalriods of interruption. If unilateral cannulation is per-rmed, success may depend on patency of the circle ofillis. Alternatively, unilateral direct or side-graft cannu-tion of the (usually right) axillary artery permits extra-rporeal circulation and cooling without manipulation ofe diseased thoracic aorta. This same cannula can then beed for delivering antegrade brain perfusion immediatelyter the section of aorta from which the brachiocephalicteries originate is sutured to the graft or immediatelyter the brachiocephalic vessels are individually anasto-osed to a trifurcated graft. The time required to completeese maneuvers requires a relatively shorter period ofpothermic circulatory arrest compared with competeconstruction of the aortic arch (681,683,701–704). Bilat-al brachiocephalic artery cannulation has also beenported (705). The literature is insufficient to determinehether unilateral or bilateral perfusion or complete avoid-ce of circulatory arrest is associated with improvedtcomes. A retrospective analysis by Svensson et al (449)ggested that axillary artery perfusion via a prostheticde-graft was associated with improved outcomes com-red with femoral arterial cannulation.Finally, direct cannulation of the aortic replacement graft
ay be used to institute antegrade brain perfusion followingperiod of circulatory arrest. The variability of techniquesong surgical centers makes direct comparison difficult;wever, most studies with some type of antegrade arterialain perfusion report outcomes that are comparable to ortter than those using hypothermic circulatory arrest aloneretrograde brain perfusion (660,662,666,685,686,706,707).rthermore, selective antegrade brain perfusion may reduce
e period of brain ischemia and permit less profoundpothermia, which may be associated with good clinicaltcomes (676,687,708–712).Our ability to create evidence-based guidelines from theerature is particularly difficult in the case of brain protec-n. Changes in surgical technique, perfusion technology,esthetic and intensive care management, coagulation man-ement, prosthetic graft materials, and the experience of theporting centers and lack of randomized clinical trials arenfounding factors.
.5.2. Recommendations for Spinal Cord Protectionuring Descending Aortic Open Surgical andndovascular RepairsASS I
Cerebrospinal fluid drainage is recommended as a spinal cordprotective strategy in open and endovascular thoracic aorticrepair for patients at high risk of spinal cord ischemic injury.(522,523,713) (Level of Evidence: B)
ASS IIa
Spinal cord perfusion pressure optimization using techniques,
such as proximal aortic pressure maintenance and distal aortic reperfusion, is reasonable as an integral part of the surgical,anesthetic, and perfusion strategy in open and endovascularthoracic aortic repair patients at high risk of spinal cordischemic injury. Institutional experience is an important factorin selecting these techniques. (380,382,714,715) (Level ofEvidence: B)Moderate systemic hypothermia is reasonable for protection ofthe spinal cord during open repairs of the descending thoracicaorta. (525) (Level of Evidence: B)
ASS IIb
Adjunctive techniques to increase the tolerance of the spinalcord to impaired perfusion may be considered during open andendovascular thoracic aortic repair for patients at high risk ofspinal cord injury. These include distal perfusion, epiduralirrigation with hypothermic solutions, high-dose systemic glu-cocorticoids, osmotic diuresis with mannitol, intrathecal pa-paverine, and cellular metabolic suppression with anestheticagents. (520,715–717) (Level of Evidence: B)Neurophysiological monitoring of the spinal cord (somatosen-sory evoked potentials or motor evoked potentials) may beconsidered as a strategy to detect spinal cord ischemia and toguide reimplantation of intercostal arteries and/or hemody-namic optimization to prevent or treat spinal cord ischemia.(483,634,718,719) (Level of Evidence: B)
raparesis and paraplegia are perhaps the most fearedmplications following repair of the descending thoracicrta. Although rates as high as 23% have previously beenported, the current incidence is probably somewhere around
to 6% (483,521,634,718,720). In any specific patient,wever, the likelihood of neurological complications de-nds highly on individual anatomy, on whether the aorta isssected or aneurysmal, and on whether the pathology isute, chronic, or both.Risk factors for perioperative spinal cord injury includeergency surgery, dissection, extensive disease, prolonged
rtic cross-clamp time, aortic rupture, level of aortic cross-amp, patient age, prior abdominal aortic surgery, and, inrticular, hypogastric artery exclusion (143,144,721), asell as a history of renal dysfunction. The risk of paraplegiaparaparesis is minimal if the aortic cross-clamp time is less
an 15 minutes (722). Svensson et al (381) reported a 20%sk of neurological injury if aortic cross-clamp time waseater than 60 minutes and less than 10% if aortic cross-amp time was less than 30 minutes. Although paraplegia orraparesis has been reported with aortic cross-clamp timesless than 20 minutes (723), others have concluded that
rtic cross-clamp times greater than 40 minutes did notsult in increases in adverse spinal cord outcome, if distalrfusion was used (382). One study of patients undergoingen or endovascular repair of descending thoracic or thora-abdominal aortic aneurysms demonstrated a higher risk ofinal cord injury related to the extent of aorta treated but nofference between the operative approaches (724).Another option for spinal cord protection is deep hypother-
ic circulatory arrest (630). This has been a useful techniquer complex descending thoracic or thoracoabdominal aortic
pairs performed via a left thoracotomy approach.
14D
Inromso(Mlatinfrthsuinro
wpococoanlelimlamrepeSSstaopatrluprhareprisabpaw
coulof(5colaBnupoan
immcoofLth
atththexav
m56papacocheihewpa
14PrveastomalnoinIninsp
ditecobearblsh
14Anocarecrspanspsp
thNpldrpamtivC
e99JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
.5.2.1. MONITORING OF SPINAL CORD FUNCTION IN
ESCENDING THORACIC AORTIC REPAIRS
general, the comparatively low current incidence of neu-logic complications is attributable to the routine use ofultimodal neurophysiologic monitoring such as somatosen-ry evoked potentials (SSEP) and motor evoked potentialsEP) in conjunction with neuroprotective strategies noted
ter (526). Although these neuroprotective strategies con-ue to evolve and may differ slightly in their implementation
om center to center, monitoring of evoked potentials duringese cases has become common because it provides thergeon and anesthesiologist the opportunity to promptlytervene if alterations in monitored potentials indicate neu-logic compromise is occurring (524,526,719,725,726).
SSEPs are cerbral cortical electrical potentials recordedith scalp electrodes during electrical stimulation of thesterior tibial or peroneal nerves of the lower extremities,nducted via the lateral and posterior columns of the spinalrd (727). Because SSEP monitoring is less sensitive toesthetic drugs and paralytic agents may be used, its use isss complex than MEP monitoring. SSEP monitoring is
ited because it is only dependent on the integrity of theteral and posterior columns. The anterior motor column isore likely to be affected by ischemic injury during aorticconstruction. It is thus possible to sustain an isolatedrioperative anterior column injury without changes inEPs. In 1 study, SSEP monitoring influenced the surgical
rategy in 17 of 63 patients (27%) undergoing descendingrtic reconstruction (719). Corrective interventions includedrtial cardiopulmonary bypass initiated in 1 patient with
aumatic aortic rupture; reimplantation of critical intercostal,mbar, or sacral arteries in 11 patients; suture closure ofofusely back-bleeding intercoastal arteries in 1 patient;stening the proximal suture line in 1 patient; distal clamppositioning to a more proximal position in 1 patient; andoximal clamp repositioning in 2 patients with left carotidchemia. The authors reported no cases of unexplained SSEPnormalities. New immediate paraplegia was observed in 1tient with sustained SSEP absence, and 2 patients presentedith delayed paraplegia despite normal inoperative SSEP.
In contrast, MEPs are performed by stimulating the motorrtex (by either high-voltage short-duration electrical stim-us or magnetic induction) (728) and recording at the level
the spinal cord, peripheral nerves, or muscles24,526,725–727). Neurogenic MEPs are responses re-rded at the peripheral nerves, whereas myogenic MEPs arerge biphasic responses recorded over the muscle belly.ecause the amplitude of the response is proportional to thember of motor neurons being stimulated, these evokedtentials are very sensitive to neuromuscular blocking andesthetic agents (729–738).
Monitoring of SSEPs alone has not been demonstrated toprove outcomes in patients undergoing TAA repair. SSEP
onitoring is associated with delayed ischemia detectionmpared with transcranial MEPs (739), as well as high ratesboth false-negative and false-positive results (635,739).
yon et al (740) reported a significantly higher voltage
reshold for the generation of a 50 microV amplitude signal cothe end of the procedure compared with the beginning ofe procedure (“anesthetic fade”). This increased voltagereshold was directly proportional to the length of anestheticposure. Recognition of this phenomenon is important tooid false-positive MEP interpretation.
To demonstrate the greater sensitivity of MEP than SSEPonitoring, Dong et al (634) reported their experience with
patients undergoing descending aortic reconstruction. Alltients were monitored with both MEPs and SSEPs. Sixteentients (29%) had MEP evidence of perioperative spinalrd ischemia compared with 4 patients (7%) with SSEPanges. These changes were reversed in 13 patients withther segmental artery reimplantation or optimization ofmodynamics. Although one of these 13 patients awokeith immediate paraplegia, the remaining 3 patients awokeraplegic. All 3 patients had normal perioperative SSEPs.
.5.2.2. MAINTENANCE OF SPINAL CORD ARTERIAL PRESSURE
oximal hypertension may increase the contribution of thertebral artery–derived blood flow to the spinal cord as wellcollateral flow. Other methods of maintaining arterial flowthe spinal cord include the aggressive reimplantation of
ajor intercostal arteries into the aortic graft (715). Griepp et(742) emphasized the importance of prompt ligation ofnimplanted intercostal arteries to avoid “steal” from bleed-g during periods of ischemia to this collateral bed (741).trathecal papaverine has also been described as a method ofducing spinal cord arterial dilation, and thus increasinginal cord blood flow.
The literature is unclear with respect to the benefits ofstal perfusion alone on spinal cord protection because thechnique is not used in isolation. Several studies support thencept that distal perfusion combined with CSF drainage isneficial (380,382,468,714). The minimum desirable distalterial pressure is 60 mm Hg to ensure adequate spinal cordood flow, whereas maximal proximal mean arterial pressureould be about 90 to 100 mm Hg (743).
.5.2.3. CEREBROSPINAL FLUID PRESSURE AND DRAINAGE
pplication of a cross-clamp to the proximal descending aortat only creates a major hemodynamic load on the heart but alsouses an acute elevation in CSF pressure (744). Surgicaltraction of the aortic arch may also produce significant in-eases in CSF pressures (745). When CSF pressure exceedsinal venous pressure, a “critical closing pressure” is achieved,d the veins collapse independent of inflow pressure. Theinal cord perfusion pressure is therefore the difference betweeninal arterial pressure and CSF pressure.
Coselli et al (522) randomized 145 patients undergoingoracoabdominal aortic repair with or without CSF drainage.ine patients (13.0%) in the control group developed para-egia or paraparesis. In contrast, only 2 patients in the CSFainage group (2.6%) had deficits develop (P�0.03). Notients with CSF drainage had immediate paraplegia. Aeta-analysis by Khan and Stansby (713) and the retrospec-e analysis by Safi and colleagues (523) also concluded that
SF drainage was advantageous in reducing the risk of spinal
rd injury in open TAA repairs.
sprehespsuspocagdr(7drtefrinheco
14Mtiomdevopainveextupaerprsuoc
reatre(5ofprtom
mprnicuofcogr
14Aaftiomfr1.
spfa
14DECL
1.
2.
CL
1.
Inthrefaafthispahe(6
di(7winremprpo
fudeth
1AMcoth
tiegi
Intimm
e100 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
Possible complications of CSF drainage include headache,inal or epidural hematoma formation or inflammatoryaction, meningitis, and persistent CSF leaks. Subduralmatoma has been reported after thoracic aortic repair withinal fluid drainage (746). Introduction of blood into thebarachnoid space may result in vasospasm and decreases ininal blood flow (747). Decreases in CSF pressure maycur with phlebotomy, and aggressive use of hyperosmoticents and hyperventilation may be as effective as spinalainage in maintaining spinal cord perfusion pressure48,749). In a single-center report of 162 patients with CSFains, 6 patients (3.7%) had catheter-related complications:mporary abducens nerve palsy, 1 patient; retained catheteragments, 2 patients; retained catheter fragments and men-gitis, 1 patient; isolated meningitis, 1 patient; and spinaladache, 1 patient. There were no neuraxial hemorrhagicmplications in this series (750).
.5.2.4. HYPOTHERMIA
ild hypothermia may provide significant neuronal protec-n by mechanisms such as reducing excitatory neurotrans-
itter release, decreasing free oxygen radical production,creasing postischemic edema, and stabilizing central ner-us system blood flow (751,752). Hypothermia occurs viassive cooling in a cold operating room with a majorcision in addition to cooling blankets and unwarmed intra-nous fluids. If an extracorporeal circuit is used, a heatchanger permits warming or cooling of the body tempera-re. A temperature of 32°C is usually well tolerated bytients not undergoing full cardiopulmonary bypass. Mod-ate systemic hypothermia has been associated with im-oved outcomes following TAA surgery (525). Arrhythmias,ch as atrial fibrillation and even ventricular fibrillation, cancur if hypothermia is too severe.
Epidural infusion of cooled saline may be used to inducegional hypothermia. Although this technique was associ-ed with substantial increases in CSF pressure, a significantduction in postoperative neurologic deficits was noted20,716). A new, self-contained catheter for topical coolingthe spinal cord without infusion into the CSF or CSF
essure rise has been shown in the laboratory to providepical spinal cord hypothermia, while systemic normother-ia is maintained; clinical trials are being organized (753).
Postischemic hyperemia occurs in the spinal cord (754). Theagnitude of this hyperemia has been demonstrated to beoportional to the incidence of paraplegia. Possible mecha-sms for the increased neurologic injury associated with vas-lar hyperemia include edema formation with the developmenta compartment syndrome and subsequently decreased spinalrd perfusion and increased oxygen delivery that may result ineater free oxygen radical species generation.
.5.2.5. GLUCOCORTICOIDS AND MANNITOL
dministration of methylprednisolone (30 mg/kg) before andter aortic occlusion may result in better spinal cord protec-n (717). The mechanism of this protection is unclear, but it
ay be related to decreased spinal cord edema and improvedee oxygen radical scavenging. Similarly, mannitol (0.25 to
0 g/kg) has been used to modulate the extent of ischemic fainal cord injury. Mannitol is hypothesized to act in similarshion to methylprednisolone (715).
.5.3. Recommendations for Renal Protectionuring Descending Aortic Open Surgical andndovascular RepairsASS IIb
Preoperative hydration and intraoperative mannitol administra-tion may be reasonable strategies for preservation of renalfunction in open repairs of the descending aorta. (Level ofEvidence: C)During thoracoabdominal or descending aortic repairs withexposure of the renal arteries, renal protection by either coldcrystalloid or blood perfusion may be considered. (626,755,756) (Level of Evidence: B)
ASS III
Furosemide, mannitol, or dopamine should not be given solelyfor the purpose of renal protection in descending aortic repairs.(757,758) (Level of Evidence: B)
a cohort of 475 patients who underwent descendingoracic aortic repair, 25% developed acute postoperativenal failure, whereas 8% required hemodialysis (759). Riskctors that are associated with postoperative renal failureter descending thoracic aortic repair include age greateran 50 years, preexisting renal dysfunction, duration of renalchemia, administration of greater than 5 units or eithercked red cells or salvaged washed autologous blood,modynamic instability, and diffuse atherosclerosis26,759).There is controversy regarding the protective nature of
stal perfusion during aortic occlusion (626,759). Godet et al59) observed a decrease in the incidence of renal failureith the use of distal aortic perfusion. Others have observedcreases in renal failure with distal perfusion (626). Selectivenal artery perfusion during descending thoracic aortic repairay result in uninterrupted urine production throughout theocedure and may decrease the incidence of renal failurestoperatively (755).Pharmacological agents, including mannitol (760,761),rosemide (758), or dopamine (757,761–764), have not beenmonstrated to provide renal protection during descendingoracic aortic repair.
4.6. Complications of Open Surgicalpproachesyocardial infarction (1% to 5%): This is an uncommonmplication but it is associated with CAD or dissection ofe coronary artery ostia (228–234,250,441).Heart failure (1% to 5%): Myocardial protection difficul-s and ventricular distention from either aortic valve regur-tation or high right-sided pressures are often factors (765).Infections (1% to 5% superficial, less than 1% deep):traoperative contamination or inadequate or improperly
ed antibiotic coverage, obesity, immunosuppression, pul-onary disease, or suboptimal glucose control may be a
ctor (766).
prstwanwpe
nopratanprtio(2
blcaorcoco
fupoteshdipuinexWus
diafretoreoptiocatioofhastchw
ofTan(3mspmpareerC
aure
wprtoavofdaaopain
1AE
niAop
readasri
1.hewmdethre
Invawaowwbian10vare
hiAis(3
2%exmtivreni
e101JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
Stroke (2% to 8% permanent): As noted earlier, brainotection is important in preventing the complication ofroke. The causes are either embolic or ischemic. Patientsho on preoperative MR have evidence of ischemic changesd/or reduced neurocognitive function, who are elderly, orho have a history of stroke are at increased risk of arioperative stroke (76,99,139,211,449,453,466,767).Neurocognitive deficit: The exact incidence of deficits hast been studied much after circulatory arrest; however, in 1ospective randomized study, using 51 neurocognitive tests,2 to 3 weeks after surgery, 9% of patients had new deficits,d by 6 months, all new deficits had resolved. Patients witheoperative deficits were proved to have further deteriora-n; indeed, 38% of patients had preoperative deficits11,466).Reoperation for bleeding (1% to 6%): Reoperation foreeding is dependent on the extent of surgery, length ofrdiopulmonary bypass, reoperative status, underlying dis-der, and surgical technique. Obtaining hemostasis prior toming off cardiopulmonary bypass and correcting all bloodagulation defects are paramount (765,766).Respiratory failure (5% to 15%): Preoperative pulmonarynction testing helps to warn the surgeon about potentialstoperative respiratory problems. Sometimes operative
chnique can be adapted to lessen the risks—for example,ortening pump time and avoiding overtransfusion. Leftaphragmatic incisions and trauma may add to postoperativelmonary dysfunction. In patients with more than 7 kg ofcreased weight after surgery, delaying extubation untilcess fluid has been eliminated by diuresis is worthwhile.hite cell filtration and plasmapharesis on pump may beeful but have not been tested in randomized trials.Ventricular arrhythmias (1% to 5%): Ventricular tachycar-a or ventricular fibrillation was a common complicationter composite valve graft insertion a decade ago, withports of 19% to 21% risk. Some of these events were relatedundiagnosed myocardial ischemia from coronary button
attachment problems, which are usually apparent duringeration or shortly thereafter. Inadequate myocardial protec-n may also lead to both ventricular arrhythmias and lowrdiac output. The increasing use of amiodarone, optimiza-n of potassium and magnesium levels, and better methodsmyocardial protection including blood cardioplegia may
ve reduced this risk. Twenty-four–hour Holter monitoringudies may reveal underlying pathology, such as ischemicanges or prolonged QT interval, particularly in patientsith Marfan syndrome, that needs to be addressed.Paralysis: The most feared complication after these typesoperations is lower limb paralysis and neurogenic bladder.
his occurs in 2% to 4% of descending thoracic aortic repairsd in 3% to 10% of thoracoabdominal aortic repairs82,526,724,768–773). Most lesions predominantly involveotor function because the anterior motor nerve cells of theinal cord are most likely to be involved. The protectiveeasures were discussed earlier. Two thirds of patients withraparesis will recover, and about half with paraplegia willcover to the point of walking again. Prevention of postop-ative hypotension in the intensive care unit and continued
SF drainage for longer than 40 hours is deemed by most lethors to be beneficial in reducing the incidence of parapa-sis (380,522,523,525,713).Hoarseness: The incidence of hoarseness is related to
hether the arch needs to be clamped and whether theoximal descending aorta at the left subclavian artery needsbe transected. Transsection at this level is recommended tooid damage to the esophagus and to prevent the formationlate aortoesophageal fistulae. This, however, may result inmage to the recurrent laryngeal nerve as it wraps around therta and ligamentum arteriosum, resulting in left vocal cordralysis. This can usually be improved by vocal cordjection with either gel or collagen.
4.7. Mortality Risk for Thoracicortic Surgeryxpected results for risk of death are summarized next.Composite valve graft (1% to 5%): With modern tech-ques, death after elective repair is unusual (76,98,99,448).dditional comorbid states and the need for emergencyeration are associated with increased risk (765).Separate aortic valve replacement with ascending aortapair (1% to 5%) (448,628): Comorbid conditions such asvanced age and concomitant coronary bypass graft surgery,well as emergency operation, are associated with increased
sk (76,99,448,765,774,775).Valve-sparing aortic root reconstruction (less than 1% to5%): These patients are mostly young and otherwisealthy, and thus excellent results are expected comparedith other aortic operations. Indeed, in 1 series of over 200odified David reimplantations, there were no operativeaths (99). Late 10-year freedom from reoperation is betteran 92% for reimplantation procedures but lower for rootmodeling procedures (76,95,98,99,448,776).Bicuspid aortic valve and ascending aorta repair (1.5%):a large series of over 2000 patients with bicuspid aortic
lve surgery, the operative risk of death (1.5%) for patientsho had both a bicuspid valve procedure and ascendingrtic repair (n�200) was no different than the risk for thoseho underwent only a bicuspid valve procedure. For patientsith Marfan syndrome or connective tissue disorders orcuspid aortic valves, the long-term prognosis is excellentd reaches an average survival of 70 years (76,99). Late-year risk of reoperation is not as low as for tricuspid aorticlve repair but still is only 9% for bicuspid aortic valvepairs.Acute AoD (3.5% to 10% in experienced centers, butgher overall): The risk of death after surgical repair of acuteoD is strongly influenced by associated stroke, mesentericchemia, renal failure, and myocardial ischemia37,375,765,777).Total arch replacement: A 2% to 6% risk of death and a
to 7% risk of stroke have been reported for thesetensive and high-risk procedures. Emergency operationortality and stroke rates are higher (15% and 14%, respec-ely) (778). Careful brain and myocardial protection, cor-
ction of coagulopathies, and improved operative tech-ques, including the use of elephant trunk procedure, have
d to improved outcomes (680,779).
bitw
cuth
inexredodecesu
inaterresurereimpadetiv5-beexarestelha
rifopesicefrdohiabtietr
1
14Tprcaaohigrsinoru
in(s
14ACL
1.
2.
3.
4.
5.
TapinfoaoMwTnoprdianAstanfrbeesbl
printhanra
(3mdipefu
e102 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
Reoperations: The risk factors for reoperations are comor-d disease and extent of surgery with results varying be-een 2% to 6% for the risk of death (464).Descending aortic replacement: The risk of death withrrent techniques is 2% to 5% and the risk of paralysis is lessan 3% for elective surgical repairs (382).Thoracoabdominal repairs: The risk of death is stronglyfluenced by the urgency of surgery, comorbid disease, andtent of repair. Thus, Crawford Type I thoracoabdominalpairs have a risk of death of approximately 5%, but this isubled to approximately 10% for Type II repairs. The resultspicted earlier represent the work performed in high-volumenters and may not reflect results of all institutions at whichch surgery is performed (381,525,768,773,780,781).The late risk of death after aortic repair is stronglyfluenced by age and comorbid disease. Furthermore, aorticherosclerosis disease is a marker for more extensive ath-osclerosis. For patients undergoing degenerative and AoDpairs, usually at an average age of the lower 70s, 5-yearrvival rates of only 60% have been reported for ascendingpairs, arch repairs, descending repairs, thoracoabdominalpairs, and infrarenal repairs (3,381). Thus, it is initiallyportant to identify and to treat all comorbid disease,rticularly CAD, which is the most common cause of lateaths in this population (381). In patients undergoing elec-e root-sparing procedures or bicuspid valve procedures, theand 10-year survival rates are considerably improved—
tter than 80% to 90% 10-year survival rates can bepected (76,139). Sadly, even young patients with AoD havedismal 5-year survival rate of 50% after surgery due tosidual events related to unresected dissected aorta. Thisresses the importance of treating young patients withective surgery, with a less than 1% risk of death, if theyve aortic root dilatation (75,76).Repair of TAAs is one of the most extensive and highest-
sk operations done in patients. Hence, selection of patientsr repair and workup for surgery needs to be diligentlyrformed. Furthermore, the cited results are from reports of
ngle-center experiences and therefore representative ofnters of excellence in the treatment of aortic disease. Dataom “real world” experiences have demonstrated nearlyuble the morbidity and mortality rates, especially forgh-risk indications like acute aortic dissection and thoraco-dominal aortic aneurysms, suggesting that high-risk pa-nts may have better outcomes in centers specializing in the
eatment of thoracic aortic diseases (782,783).
4.8. Postprocedural Care
.8.1. Postoperative Risk Factor Managementhe recognition and treatment of thoracic aortic diseaseovide the opportunity to engage the patient in long-termrdiovascular risk factor management. Conditions such asrtic atherosclerosis and aortic aneurysm are recognized asgh-risk states by the National Cholesterol Education Pro-am, Adult Treatment Panel III and require maximal inten-ty therapy (784). In these patients, the risk of a fatal ornfatal MI is higher than the risk of amputation or aortic
pture. The risk factors with clinical trial evidence of benefit siclude hypertension, dyslipidemia, and cigarette smokingee Section 9.2.1).
.8.2. Recommendations for Surveillance of Thoracicortic Disease or Previously Repaired PatientsASS IIa
Computed tomographic imaging or magnetic resonance imag-ing of the thoracic aorta is reasonable after a Type A or B aorticdissection or after prophylactic repair of the aortic root/ascending aorta. (74) (Level of Evidence: C)Computed tomographic imaging or magnetic resonance imag-ing of the aorta is reasonable at 1, 3, 6, and 12 monthspostdissection and, if stable, annually thereafter so that anythreatening enlargement can be detected in a timely fashion.(Level of Evidence: C)When following patients with imaging, utilization of the samemodality at the same institution is reasonable, so that similarimages of matching anatomic segments can be compared sideby side. (Level of Evidence: C)If a thoracic aortic aneurysm is only moderate in size andremains relatively stable over time, magnetic resonance imag-ing instead of computed tomographic imaging is reasonable tominimize the patient’s radiation exposure. (Level of Evi-dence: C)Surveillance imaging similar to classic aortic dissection isreasonable in patients with intramural hematoma. (Level ofEvidence: C)
he mean rate of growth for all thoracic aortic aneurysms isproximately 1 mm/y, but that growth rate increases withcreasing aneurysm diameter. Growth rates tend to be fasterr aneurysms involving the descending versus the ascendingrta, for dissected versus nondissected aortas, for those witharfan syndrome versus those without (375), and for thoseith bicuspid versus those with tricuspid aortic valves (785).he frequency of surveillance imaging is not clear as there are
data to accurately dictate surveillance intervals. It seemsudent to obtain an initial follow-up imaging study beforescharge; at 1, 3, 6, and 12 months postoperatively; and thennually after a thoracic aortic aneurysm is first detected.ssuming the aneurysm is stable in size on the first follow-upudy, repeat imaging can reasonably be repeated on annual basis. For relatively small aneurysms that are stable
om year to year on annual imaging, the writing committeelieves that an imaging frequency of every 2 to 3 years,pecially in older patients, is currently reasonable (Ta-e 17).The writing committee believes that the anatomical detailovided by CT may be better than that for MR in manystances. However, for surveillance of stable and moderateoracic aortic aneurysms, MR provides adequate informationd avoids the potential problems associated with repeateddiation exposure of CT angiography.Dissected aortas also tend to dilate progressively over time
75,786). Therefore, those with a Type B AoD managededically or those with a Type A AoD with a persistent distalssection following ascending aortic repair must also undergoriodic surveillance imaging to monitor the affected aorta forrther dilatation. When the dissected aorta is relatively stable in
ze, annual surveillance imaging is usually sufficient. The most
prtheagrmruluchfrao
indisiapmriprsarifayean(2Csywingrtr
clm
1E
1MNedthcothimfocoimrear
arfaemspannoac
1Naftopr
1Paprtoinvisttioiste(7rilesebolebloubo
praneq
TaRe
Pa
Acdis
Chdis
Aore
AVas
Ao
Thste
Ac
becoofblAd
CXimec
e103JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
oximal portion of the descending thoracic aorta, just beyonde ostium of the left subclavian artery, is most prone to bothrly and late dilatation. If this segment expands to 6.0 cm oreater or if there is rapid growth, intervention or an open repairay become necessary. Predictors of progressive dilatation orpture of a dissected aorta include complete patency of the falsemen (787) and a large false lumen size (788). Those withronic AoD are also at risk for a second acute dissection arising
om the chronic dissection itself or de novo from undissectedrta.Those with IMH are also at risk of late complications,
cluding conversion to a classic AoD and progressive aorticlatation. Conversely, in other cases there may be progres-ve reabsorption of the IMH, and in time the radiographicpearance of the thoracic aorta normalizes. While this is aore favorable outcome, such patients remain at increasedsk of late complications as the apparently healed aorta isone to the development of “ulcer-like projections andccular aneurysm,” which are associated with an increasedsk of late aneurysm formation and rupture (297). Otherctors that predict adverse events are age greater than 70ars (297), a maximum aortic diameter of 40 mm or greater,d a maximum aortic wall thickness of 10 mm or greater98). The natural history of PAUs remains poorly defined.ertainly those who present with symptoms of an acute aorticndrome are likely to have increased risk of aortic rupture,hereas those without symptoms whose ulcers are discoveredcidentally are more likely to have a chronic or slowlyowing ulcer. Those with uncomplicated ulcers are often
ble 17. Suggested Follow-Up of Aortic Pathologies Afterpair or Treatment
thology Interval Study
utesection
Before discharge, 1 mo, 6mo, yearly
CT or MR, chest plusabdomen TTE
ronicsection
Before discharge, 1 y, 2to 3 y
CT or MR, chest plusabdomen TTE
rtic rootpair
Before discharge, yearly TTE
R pluscending
Before discharge, yearly TTE
rtic arch Before discharge, 1 y, 2to 3 y
CT or MR, chest plusabdomen
oracic aorticnt
Before discharge, 1 mo, 2mo, 6 mo, yearly Or 30
days*
CXR, CT, chest plusabdomen
ute IMH/PAU Before discharge, 1 mo, 3mo, 6 mo, yearly
CT or MR, chest plusabdomen
*US Food and Drug Administration stent graft studies usually requiredfore discharge or at 30-day CT scan to detect endovascular leaks. If there isncern about a leak, a predischarge study is recommended; however, the riskrenal injury should be borne in mind. All patients should be receiving beta
ockers after surgery or medically managed aortic dissection, if tolerated.apted from Erbel et al (539).
AVR indicates aortic valve replacement; CT, computed tomographic imaging;R, chest x-ray; IMH, intramural hematoma; MR, magnetic resonanceaging; PAU, penetrating atherosclerotic ulcer; and TTE, transthoracichocardiography.
eated medically with antihypertensive medications and tio
ose monitoring with serial imaging studies, similar to theanagement of a patient with a distal AoD (789).
5. Nursing Care and Patient/Familyducation
5.1. Nursing Care of Medicallyanaged Patientsursing care for patients with thoracic aortic disease requiresucation to ensure that both patient and family understande disease process, the importance of therapy includingntrol of hypertension and other risk factors (790,791), ande need for continued follow-up, including surveillanceaging. Because some aortic diseases are hereditary,llow-up might also include family member screening andunseling (792). For patients with acute aortic syndromes,mediate control of hypertension and pain, as well as
peated assessments of symptoms and hemodynamic status,e key elements (345).Patients transported from smaller hospitals to larger onese often alone, without the immediate support of theirmilies, and will be dependent on nursing personnel forotional support and reassurance, as well as clinical and
iritual care. Family members need to have their questionsswered honestly and in a way they can understand, to betified of any changes in the patient’s condition, and to havecess to their loved one(s) (793).
5.2. Preprocedural Nursing Careurses play a key role in answering questions that remainter initial explanations by physicians. Table 18 outlinespics that should be discussed as part of informed consentior to an endovascular or open surgical procedure.
5.3. Postprocedural Nursing Caretients with a lower acuity level after thoracic aorticocedures, including endovascular repair, are often admitteda postanesthesia care unit for initial recovery and then to antensive care unit that can provide frequent monitoring oftal signs, peripheral pulses, urine output, and neurologicalatus including lower extremity motor strength and sensa-n. Assessment of the skin in the extremities and lower torsoperformed to look for cyanotic discoloration and skin
mperature changes, which may be signs of embolization94). Embolization to cerebral vessels is another potentialsk of these procedures, so frequent monitoring of mentation,vel of consciousness, vision, speech, motor strength, andnsory function in the extremities is required. Thromboem-li to mesenteric, renal, and peripheral vascular beds may
ad to complaints of abdominal pain or the presence ofoody diarrhea or vomiting. Flank pain with changes in urinetput might indicate potential renal infarction from throm-emboli.The initial postprocedural management focuses on bloodessure control. Hypertension can result in stent migrationd bleeding from aortic suture lines. Hypotension can beually problematic with the potential to impair renal func-
n and spinal cord perfusion pressure. Hypotension presents
awpeparereysdelereanobdranim
toasreat
poof
letoaninbo
thanTasthmtioVmon
emsiawrepaanofsh
1MPaorinarhawaoaxthelInincedy
thdo
plpr
Ta
0�
1�
2�
3�
4�
Taan
Cl
Le
Po
Pr
Int
Tr
Ac
St
Du
e104 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
risk to spinal cord perfusion pressure and requires treatmentith fluids or vasopressors. The risk of inadequate spinal cordrfusion is spinal cord ischemia, dysfunction, and potentialraplegia. Any decrease in lower extremity function must beported to the physician team immediately as it couldpresent the onset of early and potentially reversible paral-is. A typical assessment consists of asking patients tomonstrate motor strength holding their extended, straightgs off the bed one at a time for at least 5 seconds (781), withpeated assessments performed frequently for the first hoursd days after an endovascular or open procedure. Anjective scale that can be useful is outlined in Table 19. CSFains are used for many patients undergoing endovasculard surgical procedures, and the nursing care is criticallyportant (see Section 14.4).Any new back or chest pain warrants further investigationrule out the possibility of myocardial ischemia or infarctionwell as a potential endoleak. New-onset pain of this nature
quires notification of the physician team for further evalu-ion.A phenomenon associated with stent graft placement isstimplantation syndrome, which can occur within 24 hours
ble 18. Topics of Discussion for Preoperative Instructiond Informed Consent
arification of the intervention or surgical procedure
ngth of the intervention or surgical procedure
tential complications
Endovascular leak
Stroke
Paralysis
Respiratory dysfunction/failure
Renal dysfunction/failure
Myocardial infarction (especially if known coronary disease)
eoperative preparation for elective procedures
Smoking cessation
Antiplatelet or anticoagulation adjustment
Preoperative testing and instructions for obtaining tests
Chlorhexidine showers or other skin preparation
ensive care stay and environment
What to expect: monitoring, staffing ratios, equipment
Length of stay
Visiting restrictions if any
Intravascular access
Central venous lines
Arterial lines
Ventilator support and weaning
Lumbar drains
Other lines and tubes
Pain management
ansitional care unit transfer
What to expect: monitoring, staffing ratios
Length of stay
tivity progression
ernal and other activity/lifestyle precautions
rable power of attorney for health care
placement of the graft. It is characterized by fever,
ukocytosis, and occasionally thrombocytopenia. The symp-ms, which usually resolve within 1 week, are managed withalgesics and anti-inflammatory agents (794). Heparin-duced thrombocytopenia can be another source for throm-embolic events and may require treatment.Routine assessment of the cannulation site used to deploye graft is necessary. Large sheaths are used to deliver stentsd can traumatize and occlude the femoral or iliac artery.
he postoperative period presents an optimal opportunity tosess and manage cardiovascular risk factors and to educatee patient and family on the benefits of risk-reductioneasures. The AHA/ACC Guidelines for Secondary Preven-n for Patients With Coronary and Other Atherosclerotic
ascular Disease (409) outlines guides to risk factor assess-ent, patient education, and possible interventions (see theline-only Data Supplement).Patient and family preparation for discharge includesphasis of the importance of medication compliance, inci-
on care, and the need for follow-up. They must be madeare of the signs and symptoms of infection, such as
dness, swelling, drainage, and fever. Unusual or severein, change in motor strength or sensation in the extremities,d sudden weakness or dizziness, which may be symptomsnew-onset bleeding or changes in spinal cord perfusion,
ould be promptly reported.
5.4. Nursing Care of Surgicallyanaged Patientstients who have undergone open repair of aortic aneurysmsdissection will require more intensive care. A distinguish-
g feature will be whether the patient had an ascending aorticch, or descending thoracic aortic repair. Patients who haved a dissection or an aneurysm of the ascending aorta or archill have a median sternotomy incision. Patients undergoingrtic arch procedures may also have an incision over theillary artery site. Cardiopulmonary bypass is required forese procedures and can be associated with fluid retention,ectrolyte abnormalities, coagulopathies, and hypothermia.addition, patients with aortic arch repairs are subjected to
tervals of circulatory arrest and retrograde or selectiverebral perfusion. These adjuncts can result in neurologicsfunction in the postoperative period.Patients with Type B aortic dissections or descendingoracic aneurysms will have lateral thoracic or thoracoab-minal incisions. These incisions are often extensive.These patients will often have lumbar drains that have beenaced to monitor CSF pressure and CSF fluid drainage. Theessure used as a target for drainage varies but will generally
ble 19. Lower Extremity Motor Function Assessment Scale
No movement
Flicker of movement
Able to bend knee to move leg
Unable to perform straight leg raise against gravity, but better legmovement
Normal movement with expected later or demonstrated ambulation
Note: A score of �3 may be an indication for a neurological evaluation.
Adapted from Svensson et al (781).
befrtaprlehetioNexin
veulfuthmnacalo
1
1LACL
1.
EaoreexboprviAdeNamantr
mitblmavtabeheenripo
fobeaeisprcicicolesuano
innesuasyrecoA(8stchmsethinsethhonoitphthexcoth
spthdipeskexavrosapagoin
wemesPa
e105JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
around 10 mm Hg. Pressures are checked hourly or moreequently in the early postoperative period. Care must beken to prevent drainage that is too rapid or too excessive toevent subdural hematoma formation (746). Any change invel of consciousness or onset of irritability, confusion,adache, or pupillary reactivity requires immediate notifica-n of the physician team and clamping of the drain.
eurologic monitoring also involves assessment of lowertremity motor and sensory function. Any deterioration maydicate inadequate spinal cord perfusion.Standard postoperative care of these patients includesntilator adjustments, optimization of blood volume, coag-ation parameters, and monitoring of other organ systemnctions (795–799). Following the transfer of patients frome intensive care unit, nursing care is focused on painanagement, progression to independent ambulation, pulmo-ry physiotherapy and incentive spirometry, and woundre. Preparation for discharge is similar to that described forwer-activity patients earlier in this section.
6. Long-Term Issues
6.1. Recommendation for Employment andifestyle in Patients With Thoracicortic DiseaseASS IIa
For patients with a current thoracic aortic aneurysm or dissec-tion, or previously repaired aortic dissection, employment andlifestyle restrictions are reasonable, including the avoidance ofstrenuous lifting, pushing, or straining that would require aValsalva maneuver. (Level of Evidence: C)
stablishing clear lifestyle goals for patients with thoracicrtic disease is important in improving long-term health andducing the risk of complications. Because regular aerobicercise, a low-fat and low-salt diet, and achieving an idealdy weight are tied to the ability to effectively control bloodessure, cholesterol, and associated aortic wall stress, pro-ding patients with clear lifestyle targets is important.voidance of tobacco is critical because it is linked to thevelopment of thoracic aortic disease and to aortic rupture.ot using cocaine or other stimulating drugs such as meth-phetamine is important as sudden surges in blood pressure
d pulse attributed to such agents have been described as aigger for aortic catastrophes (800).The prescription of exercise represents a dilemma in theanagement of patients with thoracic aortic disease. Becauseis thought that the sudden increases in dP/dt and systemicood pressure associated with physical and mental stressay be a trigger for AoD in many patients, the concept ofoiding such stresses makes sense (801). However, main-ining a regular routine of aerobic exercise has day-to-daynefits in helping patients achieve an ideal blood pressure,art rate, and body weight. Moreover, many patients simplyjoy engaging in sports such as tennis, basketball, golf, bike
ding, etc. and wish to continue in such activities if at all
ssible. thThere are no outcomes data, and scant data of any varietyr that matter, to indicate how much exercise is safe orneficial for patients with thoracic aortic disease. However,robic exercise, sometimes referred to as dynamic exercise,associated with only a modest increase in mean arterial
essure (802), and AoD rarely occurs during aerobic exer-se. Consequently, most experts believe that aerobic exer-se, particularly when heart rate and blood pressure are wellntrolled with medications, is beneficial overall. Neverthe-ss, if patients wish to engage in vigorous aerobic exercise,ch as running or basketball, one might consider performingsymptom-limited stress test to ensure that the patient doest have a hypertensive response to exercise.Conversely, with isometric exercise, there is a significantcrease in mean arterial pressure. When the Valsalva ma-uver is used for the lifting of heavy weights, there is aperimposed increase in intrathoracic pressure, followed bydramatic increase in systemic arterial pressure (802), withstolic pressures reaching 300 mm Hg or greater (803). As asult, most experts believe that heavy weight lifting ormpetitive athletics involving isometric exercise may triggeroD and/or rupture and that such activities should be avoided04). Working with patients on an individualized basis toreamline these goals based on insufficient data can beallenging. For patients who are very much interested inaintaining some sort of weight lifting program, choosingts of repetitive light weights appears to make more sensean permitting heavy weight lifting (802). For example,stead of bench-pressing 200 pounds, one might recommendlecting much lighter weights in repetitive sets to minimizee hemodynamic consequences. Patients often ask exactlyw much weight is permissible to lift. Unfortunately, it ist possible to provide a blanket answer to that question, asall depends on the patient’s size, muscular strength,ysical fitness, and how the weight is actually lifted. Ratheran try to define a numerical limit, it may be useful toplain that patients can lift whatever weight they canmfortably lift without having to “bear down” or performe Valsalva maneuver.In addition to the physiologic stress of exercise, certainorts, recreational activities, or sudden stress or trauma toe thorax can potentially precipitate aortic rupture and/orssection. Thoracic stress or trauma can occur during com-titive football, ice hockey, or soccer or may result from aiing accident, a fall while water skiing, etc. Therefore,perts often advise patients with thoracic aortic disease tooid these types of sports (805). Furthermore, rapid chesttational movement while straining or breath holding (Val-lva maneuver) may be a common denominator in manytients who develop aortic dissection (i.e., basketball, tennis,lf, baseball bat swing, chopping wood with an ax, shovel-g snow, and rapidly lifting heavy objects).In addition to the importance of setting clear lifestyle goals
ith patients with thoracic aortic disease, it is wise tophasize the importance of adherence to their medications,
pecially to beta blockers and other antihypertensive agents.tients who suddenly discontinue their medications because
ey fail to obtain a refill or perhaps forget their medications
atsi
mroexmtrmwanm
geTm(eupdeaoAwtoprInthth
nithwmbyevthneemSiunsy
1Q
1AACL
1.
2.
Qhathcaanplininmdapoofw
thphcaizexacexofth
•
•
becabePodu
e106 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
home when traveling, may find themselves in a hyperten-ve crisis with a potentially catastrophic result.Even patients who are compliant with their medicationsay find that their blood pressure may fluctuate betweenutine visits to their physician, resulting in months ofcessive hypertension. Therefore, patients may achieveore consistent control of their hypertension if they regularlyack their heart rate and blood pressure with a homeonitoring system. In addition, by regularly tracking theireight and activity profile, they can provide their physiciand other care members with accurate data with which toake adjustments in medication and lifestyle going forward.In terms of work, patients with thoracic aortic diseasenerally can function normally in most types of occupations.
he exception is any job involving heavy physical andanual labor accompanied by extreme isometric exercise.g., lifting heavy boxes in a stockroom, carrying furniture
and down stairs). As with the heavy weight liftingscribed earlier, this type of unusual sudden stress on therta may predispose to a triggering of either aortic rupture oroD (806). Therefore, when patients have a vocation inhich such extreme lifting might be required, it is importantdiscuss the details of their daily job responsibilities and toescribe avoidance of activities that might put them at risk.some cases patients can readily avoid such heavy lifting on
e job, but in many cases a letter from a physician explaininge restrictions may be required.Finally, patients with thoracic aortic disease should recog-ze that aortic disease is usually a lifelong condition that putsem at future risk for acute aortic syndromes. Even thoseho have received advanced surgical or endovascular therapyust understand that their aortic disease has not been “cured”
the interventions. Educating them about what to do in theent of the sudden onset of chest, back, or abdominal pain ore sudden development of an ischemic complication (i.e.,urological or limb) and the critical nature of getting to anergency department promptly is of the utmost importance.
milarly, those who live with or care for such patients shouldderstand what action needs to be taken should concerningmptoms arise.
7. Institutional/Hospitaluality Concerns
7.1. Recommendations for Qualityssessment and Improvement for Thoracicortic DiseaseASS I
Hospitals that provide regional care for patients with acutesequelae of thoracic aortic disease (e.g., procedures for tho-racic aortic dissection and rupture) should participate instandardized quality assessment and improvement activities,including thoracic aortic disease registries. Such activitiesshould include periodic measurement and regional/nationalinterfacility comparisons of thoracic aortic disease–relatedprocedural volumes, complications, and risk-adjusted mortality
rates. (Level of Evidence: C) adHospitals that provide regional care for patients with acutesequelae of thoracic aortic disease (e.g., procedures for tho-racic aortic dissection and rupture) should facilitate and coor-dinate standardized quality assessment and improvement ac-tivities with transferring facilities and emergency medicalservices teams. Such activities might include:a. Cooperative joint facility meetings to discuss opportunities
for quality improvement andb. Interfacility and emergency medical services team compar-
isons of pretransfer care based on available outcome dataand future performance measures developed in accordancewith this guideline. (Level of Evidence: C)
uality assessment of outcomes for thoracic aortic diseases been ongoing. Creation of one or more standardizedoracic aortic disease registries may significantly improvepacity for quality assessment and provide outcome resultsd meaningful performance benchmarks. IRAD is an exam-e of such a registry and consists of 12 large referral centers6 countries and contains information on 290 variables,
cluding demographics, history, physical findings, manage-ent, imaging studies, and outcomes (227). Commitment tota collection, analysis, measurement, validation, and re-rting should be factored into the payment structures, as allthis will consume time, effort, and infrastructure to do it
ell (47).Moderate evidence supports “evidence-based referral”—at is, limiting specific procedures only to hospitals andysicians with experience, expertise, and capacity to takere of complex problems, especially those requiring special-ed surgical skills and support teams. To date, there is noplicit evidence supporting such a recommendation forute thoracic aortic diseases (807), although this evidenceists for infrarenal aortic surgery (808–811). Data courtesythe UHC Clinical DataBase/Resource Manager for 2006q4
rough 2007q3 indicates that for patients with:
Ruptured thoracic aortic aneurysm:30% transferred from a different hospital34% were admitted from the emergency department19% referred from a clinic or physician’s office14% transferred from a skilled nursing facility or another
nonhospital facility3% other
Thoracic AoD:28% transferred from a different hospital35% were admitted from the emergency department23% referred from a clinic, physician’s office, or health
maintenance organization9% transferred from a skilled nursing facility or another
nonhospital facility5% other
Performance measures and quality metrics (811a) haveen developed to evaluate quality of care for many areas ofrdiac and vascular disease (5,812–814), but none have yeten established for patients with thoracic aortic diseases.ssible domains of quality to assess could include proce-ral volumes (facility and operator), outcomes (e.g., risk-
justed mortality, readmission, complications), time to di-
agtatinfoseth
limimdabecoinmrefe
caclw
1Athththmimavnaseancim
anbetr
phprim
inarreeveq
dimanthteapso
thspimgopoofvodetubaex2Bta
1a
Tnidiloar
1ImTpaquexmbaoftranexdiprpa
TaCo
●
●
●
●
●
●
●
●
●
●
●
●
●
e107JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
nosis and intervention, and structural measures (e.g., dis-nce to nearest referral center, services available, and con-gency planning) (815). The well-established evidence baser the regionalization of care for STEMI patients (816) mayrve as a model for similar initiatives for patients withoracic aortic disease (Table 20).Claims have been made that some centers either do or willit referrals of critically ill patients that may adversely
pact hospital mortality rates, although there are no discreteta to confirm or disprove this behavior (817). Hence,nchmarking and profiling efforts must recognize and ac-unt for the most physiologically precise severity-of-illnessformation and accurate and appropriate case-mix adjust-ents; otherwise, referral centers may have an incentive tofuse care for patients who could benefit from being trans-rred to their facility (818).Effective medical record systems are being developed andn enhance communication and provide caregivers withear documentation of a patient’s course and medications, asell as plans for future (819,820).
7.2. Interinstitutional Issuescute AoD or other acute problems involving any portion ofe aorta are life-threatening conditions and require placinge patient in a location where all appropriate diagnostic anderapeutic measures are available. The minimum require-ents for the care of patients with acute AoDs includeaging with CT, echocardiography, and angiography; theailability of cardiovascular surgery including cardiopulmo-ry bypass and endovascular interventions; an intensive caretting that allows continuous monitoring of blood pressured intravenous management of blood pressure; and physi-ans with personal experience and expertise in the manage-ent of patients with acute AoD (820).Transfer of patients with acute AoD from one institution toother represents a period of danger to the patient and mustplanned and carried out efficiently. It is incumbent on the
ble 20. Standardized Transferring Facility Assessment,mmunication, and Documentation for the Following Domains
Blood pressure control for hypertension
Heart rate control for tachycardia
Hemodynamic instability
Blood volume
Cardiac ischemia
Neurologic ischemia
Renal function
Mesenteric ischemia
Peripheral arterial pulses and perfusion
Activation of receiving team
Imaging expectations and communications
Timeliness and efficiency
EMS characteristics of transferring facility, including requisite personnel,requisite in-transport equipment, including catastrophic resuscitationcapabilities, in-transfer contingency planning, weather conditions,estimated transfer time, etc.
EMS indicates emergency medical services.
ansferring institution to provide prior physician-to- m
ysician communication, to stabilize and maintain bloodessure control throughout transport, and to send copies ofaging studies (821).Because patients with acute thoracic aortic diseases presentany emergency department or primary care setting, there
e opportunities for retrospective and comprehensive qualityview. Typical areas of quality assessment could include thealuation of timely detection in centers that typically are notuipped to manage such patients.Retrospective evaluation of patients with thoracic aorticseases, especially those for whom diagnosis was delayed orissed, is critical for learning about how best to more rapidlyd effectively identify future patients with life-threateningoracic aortic aneurysm and/or dissection. Independent ex-rnal review of poor outcomes may be necessary andpropriately constructed using de-identified clinical recordsthat bias is not introduced into the evaluation process.With the dissemination of this guideline, it is hoped thatese practice standards can form the basis for more wide-read use of a data registry for quality assessment andprovement for patients with thoracic aortic disease. Theals of such a data system would be to establish an extensivepulation of thoracic aortic disease patients with the intentevaluating clinical effectiveness. Domains could include
lume and outcome relationships, process of care patterns,velopment of standardized performance measures (struc-re, process, and outcomes), and facility and operator feed-ck quality data systems. It may also be possible to useisting data that use relevant ICD-9 codes (Table 2A and) and appropriate risk-adjusted methods to evaluate mor-
lity and complications.
8. Future Research Directionsnd Issues
he writing committee believes that there are many opportu-ties for additional meritorious research in thoracic aorticseases. Emerging research appears promising for the fol-wing areas, in addition to much needed research in othereas.
8.1. Risks and Benefits of Currentaging Technologies
here is a great need to balance the rapid identification oftients with acute AoD or rupture, and the relatively infre-ent occurrence against the potential risks of radiationposure and contrast toxicity incurred by current imagingethods, for the millions of patients who present with chest,ck, and/or abdominal pain. The rapid and correct diagnosisacute thoracic aortic diseases must not impose delays in
eatment of patients with acute MI. Additionally, screeningd serial radiographic imaging of younger patients clearlyposes those individuals to a risk of later radiation-relatedseases. Clinical studies of safety and efficacy of screeningotocols using current imaging methods to correctly identifytients who will benefit from surgical, endovascular, and/or
edical intervention are needed.
1TutmAwoffomteanvahethretioprindim
1RMextrarac
1
18UAfothcimaoledicaarm
18Aspofpr8.of
18PRthgeidun
almanfytisthdedi
18ARaotraoMmsydeagmgere
1IdAmemaonem
toat
1aWaobethrainusclroottopl
1InTGdereth
e108 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
8.2. Mechanisms of Aortic Dissectionhe year 2010 is the 250th anniversary of the death, attrib-able to AoD, of King George II of England, whose lastoments were memorably described by his valet (822).lthough a number of conditions are known to be associatedith dissection, such as hypertension and old age, the cause
spontaneous AoD is still unknown. Is an intimal tearllowed by a dissecting hematoma (823), or does an intra-ural hemorrhage ruptures into the lumen causing an intimalar? (824,825) In approximately 4% to 10% of dissections,
aortic intimal tear is not found. Bleeding from the vasasorum is hypothesized to be responsible for the intramuralmorrhage, but little is known about the microstructure ofe vasa vasorum walls; changes in the vasa vasorum insponse to aging, hypertension, and inflammation; and rela-n of extracellular and intracellular metalloproteinases tootein turnover in the walls of the vasa vasorum. Researchto these questions may shed light on the pathogenesis ofssection and provide opportunities for prevention and treat-ent.
8.3. Treatment of Malperfusion andeperfusion Injuryalperfusion of the gut, spinal cord, kidneys, and lowertremities doubles the mortality of AoD (247,826). New
eatment strategies for malperfusion and reperfusion injurye needed to improve the dismal prognosis of patients withute dissection and malperfusion syndromes.
8.4. Gene-Based Mechanisms and Models
.4.1. Aortic Disease Management Based on thenderlying Genetic Defectss genes are identified leading to an inherited predispositionr thoracic aortic disease, it is becoming increasingly evidentat the clinical management of thoracic aortic disease asso-ated with different gene mutations may differ. For example,utations in TGFBR1 and TGFBR2 predispose patients tortic dissection at an aortic diameter of 5.0 cm or less,ading to the recommendation that the aorta be replaced atameters as small as 4.0 cm. As genes are identified that canuse predisposition to thoracic aortic disease, clinical studiese needed on these patients to determine their optimalanagement.
.4.2. Biomarkers for Acute Aortic Dissectionquick laboratory test with at least a high sensitivity, if notecificity, could lead to fewer missed or delayed diagnoses
acute AoD. None currently exists. D-dimer has beenoposed as a screening test for acute AoD (see Section6.1.2). A prospective study regarding the safety and efficacysuch a strategy is needed.
.4.3. Genetic Defects and Molecularathway Analysesecent studies in the mouse model of Marfan syndrome ande identification of TGFBR1 and TGFBR2 mutations sug-sts that alteration of TGF-Beta signaling is involved. Theentification of mutations in 2 components of the contractile
it in smooth muscle cells, beta-myosin heavy chain and tepha actin, has indicated a role of maintenance of smoothuscle cell contractile function in preserving aortic structured preventing these aortic diseases. Further studies identi-ing defective genes and analyzing pathways using humansues or mouse models will be the basis for understandinge molecular pathology and will be the first step towardvelopment of rational medical therapies for thoracic aorticsease.
.4.4. Clinical Trials for Medical Therapy forortic Aneurysmsecent studies in the mouse model of Marfan syndrome withrtic disease similar to that seen in humans showed the
eatment with losartan normalized aortic root growth andrtic wall architecture (6). Doxycycline, an inhibitor ofMP, significantly delayed aneurysm rupture in this mouseodel. A clinical trial is ongoing in patients with Marfanndrome under the age of 25 years to determine if losartanlays aortic progression. More aggressive trials (otherents, 2 or 3 agent therapies) based on the results in mouseodels to prevent the onset of aortic disease in individualsnetically predisposed or to delay the enlargement of al-ady formed aneurysms are needed.
8.5. Aortic Atheroma and Atherosclerosisentification and Treatment
s noted in Section 11, there is a need for research into theechanistic aspects of aortic arch atheroma in causingbolic events. Additionally, for those patients with known
rtic arch atheroma, a randomized blinded controlled trial iseded to test currently available treatment options, bothedical and surgical, to prevent embolic vascular events.The value of current imaging (MR, CT, TEE) technologiesidentify and quantitate risk for patients with aortic arch
heroma is unknown.
8.6. Prediction Models of Aortic Rupturend the Need for Preemptive Interventionse need to have models or indices that are better than justrtic diameter to predict rupture and to better determine thest timing for surgical or endovascular intervention. Sincee advent of CT and MR scanning, a massive amount ofdiological data has accumulated with multiple studies individual patients that could be linked to clinical data anded for this purpose. The evidence base regarding theinical course of patients with Marfan syndrome is morebust than for patients with degenerative aneurysms andher thoracic aortic conditions. An ongoing registry similarthat used for patients with Marfan syndrome would be a
ace to start.
8.7. National Heart, Lung, and Bloodstitute Working Group Recommendations
he National Heart, Lung, and Blood Institute Workingroup on Research in Marfan Syndrome and Related Disor-rs (827) posted a summary of recommendations for futuresearch which apply to the broad range of patients withoracic aortic disease. The importance of multidisciplinary
ams and collaborative research models were stressed:
•
•
•
•
•
co
S
A
Jo
C
L
M
Su
E
Je
A
N
G
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
e109JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
Existing registries should be expanded or new registriesdeveloped to define the presentation, natural history, andclinical history of aneurysm syndromes.Biological and aortic tissue sample collection should beincorporated into every clinical research program onMarfan syndrome and related disorders and funds shouldbe provided to ensure that this occurs. Such resources,once established, should be widely shared among investi-gators.An Aortic Aneurysm Clinical Trials Network should bedeveloped to test both surgical and medical therapies inpatients with thoracic aortic aneurysms. Partnership in thiseffort should be sought with industry, academic organiza-tions, foundations, and other governmental entities.The identification of novel therapeutic targets and biomar-kers should be facilitated by the development of geneti-cally defined animal models and the expanded use ofgenomic, proteomic and functional analyses. There is aspecific need to understand cellular pathways that arealtered leading to aneurysms and dissections, and todevelop robust in vivo reporter assays to monitor TGF-Beta and other cellular signaling cascades.The developmental underpinnings of apparently acquiredphenotypes should be explored. This effort will be facili-tated by the dedicated analysis of both prenatal and earlypostnatal tissues in genetically defined animal models andthrough the expanded availability to researchers of surgicalspecimens from affected children and young adults.
The writing committee enthusiastically endorses thesencepts.
taff
merican College of Cardiology Foundation
hn C. Lewin, MD, Chief Executive Officer
harlene May, Senior Director, Science and Clinical Policy
isa Bradfield, CAE, Associate Director, Science and Clini-cal Policy
ark D. Stewart, MPH, Associate Director, Evidence-BasedMedicine
e Keller, BSN, MPH, Senior Specialist, Evidence-BasedMedicine
rin A. Barrett, Senior Specialist, Science and Clinical Policy
sse M. Welsh, Specialist, Science and Clinical Policy
merican Heart Association
ancy Brown, Chief Executive Officer
ayle R. Whitman, PhD, RN, FAHA, FAAN, Senior VicePresident, Office of Science Operations
eferences1. ACCF/AHA Task Force on Practice Guidelines. Manual for ACCF/AHA
Guideline Writing Committees: Methodologies and Policies from the
ACCF/AHA Task Force on Practice Guidelines. Available at: http://www.acc.org/qualityandscience/clinical/manual/pdfs/methodology.pdf andhttp://circ.ahajournals.org/manual/. Accessed January 7, 2010.
2. Svensson LG, Rodriguez ER. Aortic organ disease epidemic, and whydo balloons pop? Circulation. 2005;112:1082–4.
3. Svensson LG, Crawford ES. Cardiovascular and Vascular Disease of theAorta. Philadelphia, PA: WB Saunders Co; 1997.
4. Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 PracticeGuidelines for the management of patients with peripheral arterialdisease (lower extremity, renal, mesenteric, and abdominal aortic).Circulation. 2006;113:e463–654.
5. Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelinesfor the management of patients with valvular heart disease. Circulation.2006;114:e84–231.
6. Habashi JP, Judge DP, Holm TM, et al. Losartan, an AT1 antagonist,prevents aortic aneurysm in a mouse model of Marfan syndrome.Science. 2006;312:117–21.
7. Pannu H, Tran-Fadulu V, Papke CL, et al. MYH11 mutations result ina distinct vascular pathology driven by insulin-like growth factor 1 andangiotensin II. Hum Mol Genet. 2007;16:2453–62.
8. Kumar SR. Pathologic Basis of Disease. Philadelphia, PA: ElsevierSaunders. 2005.
9. Collins JS, Evangelista A, Nienaber CA, et al. Differences in clinicalpresentation, management, and outcomes of acute type A aortic dissec-tion in patients with and without previous cardiac surgery. Circulation.2004;110:II237–42.
0. Razzouk A, Gundry S, Wang N, et al. Pseudoaneurysms of the aortaafter cardiac surgery or chest trauma. Am Surg. 1993;59:818–23.
1. Milewicz DM, Guo DC, Tran-Fadulu V, et al. Genetic basis of thoracicaortic aneurysms and dissections: focus on smooth muscle cell contrac-tile dysfunction. Annu Rev Genomics Hum Genet. 2008;9:283–302.
2. Johnston KW, Rutherford RB, Tilson MD, et al. Suggested standards forreporting on arterial aneurysms. Subcommittee on Reporting Standardsfor Arterial Aneurysms, Ad Hoc Committee on Reporting Standards,Society for Vascular Surgery and North American Chapter, InternationalSociety for Cardiovascular Surgery. J Vasc Surg. 1991;13:452–8.
3. Hannuksela M, Lundqvist S, Carlberg B. Thoracic aorta: dilated or not?Scand Cardiovasc J. 2006;40:175–8.
4. Hager A, Kaemmerer H, Rapp-Bernhardt U, et al. Diameters of thethoracic aorta throughout life as measured with helical computedtomography. J Thorac Cardiovasc Surg. 2002;123:1060–6.
5. Roman MJ, Devereux RB, Kramer-Fox R, et al. Two-dimensionalechocardiographic aortic root dimensions in normal children and adults.Am J Cardiol. 1989;64:507–12.
6. Svensson LG, Khitin L. Aortic cross-sectional area/height ratio timingof aortic surgery in asymptomatic patients with Marfan syndrome.J Thorac Cardiovasc Surg. 2002;123:360–1.
7. Stary HC, Chandler AB, Dinsmore RE, et al. A definition of advancedtypes of atherosclerotic lesions and a histological classification ofatherosclerosis. A report from the Committee on Vascular Lesions of theCouncil on Arteriosclerosis, American Heart Association. Circulation.1995;92:1355–74.
8. He R, Guo DC, Estrera AL, et al. Characterization of the inflammatoryand apoptotic cells in the aortas of patients with ascending thoracicaortic aneurysms and dissections. J Thorac Cardiovasc Surg. 2006;131:671–8.
9. Tang PC, Coady MA, Lovoulos C, et al. Hyperplastic cellular remod-eling of the media in ascending thoracic aortic aneurysms. Circulation.2005;112:1098–105.
0. Segura AM, Luna RE, Horiba K, et al. Immunohistochemistry of matrixmetalloproteinases and their inhibitors in thoracic aortic aneurysms andaortic valves of patients with Marfan’s syndrome. Circulation. 1998;98:II331–II337.
1. Fedak PW, de Sa MP, Verma S, et al. Vascular matrix remodeling inpatients with bicuspid aortic valve malformations: implications foraortic dilatation. J Thorac Cardiovasc Surg. 2003;126:797–806.
2. Lemaire SA, Wang X, Wilks JA, et al. Matrix metalloproteinases inascending aortic aneurysms: bicuspid versus trileaflet aortic valves.J Surg Res. 2005;123:40–8.
3. Lemaire SA, Pannu H, Tran-Fadulu V, et al. Severe aortic and arterialaneurysms associated with a TGFBR2 mutation. Nat Clin Pract Cardio-vasc Med. 2007;4:167–71.
4. Ikonomidis JS, Jones JA, Barbour JR, et al. Expression of matrixmetalloproteinases and endogenous inhibitors within ascending aorticaneurysms of patients with bicuspid or tricuspid aortic valves. J Thorac
Cardiovasc Surg. 2007;133:1028–36.
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
e110 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
5. Dong C, Wu QY, Tang Y. Ruptured sinus of valsalva aneurysm: aBeijing experience. Ann Thorac Surg. 2002;74:1621–4.
6. Pannu H, Fadulu VT, Chang J, et al. Mutations in transforming growthfactor-beta receptor type II cause familial thoracic aortic aneurysms anddissections. Circulation. 2005;112:513–20.
7. Guo D, Pannu H, Tran-Fadula V, et al. Mutations in smooth musclealpha-actin (ACTA2). Nat Genet. 2007;39:1488–93.
8. Weyand CM, Goronzy JJ. Medium- and large-vessel vasculitis. N EnglJ Med. 2003;349:160–9.
9. Salvarani C, Gabriel SE, O’Fallon WM, et al. The incidence of giant cellarteritis in Olmsted County, Minnesota: apparent fluctuations in a cyclicpattern. Ann Intern Med. 1995;123:192–4.
0. Amis ES Jr., Butler PF, Applegate KE, et al. American College ofRadiology white paper on radiation dose in medicine. J Am Coll Radiol.2007;4:272–84.
1. Brenner DJ, Hall EJ. Computed tomography: an increasing source ofradiation exposure. N Engl J Med. 2007;357:2277–84.
2. Shellock FG, Spinazzi A. MRI safety update 2008: part 1, MRI contrastagents and nephrogenic systemic fibrosis. AJR Am J Roentgenol.2008;191:1129–39.
3. Cascade PN, Leibel SA. Decision-making in radiotherapy for the cancerpatient: the American College of Radiology Appropriateness CriteriaProject. CA Cancer J Clin. 1998;48:146–50.
4. International Commission on Radiological Protection (ICRP). Recom-mendations of the International Commission on Radiological Protection.Ann ICRP. 1977;1:1–53.
5. McCollough CH, Bruesewitz MR, Kofler JM Jr. CT dose reduction anddose management tools: overview of available options. Radiographics.2006;26:503–12.
6. Parker MS, Matheson TL, Rao AV, et al. Making the transition: the roleof helical CT in the evaluation of potentially acute thoracic aorticinjuries. AJR Am J Roentgenol. 2001;176:1267–72.
7. Klompas M. Does this patient have an acute thoracic aortic dissection?JAMA. 2002;287:2262–72.
8. von Kodolitsch Y, Nienaber CA, Dieckmann C, et al. Chest radiographyfor the diagnosis of acute aortic syndrome. Am J Med. 2004;116:73–7.
9. Woodring JH, King JG. The potential effects of radiographic criteria toexclude aortography in patients with blunt chest trauma. Results of astudy of 32 patients with proved aortic or brachiocephalic arterial injury.J Thorac Cardiovasc Surg. 1989;97:456–60.
0. Mirvis SE, Bidwell JK, Buddemeyer EU, et al. Value of chest radiog-raphy in excluding traumatic aortic rupture. Radiology. 1987;163:487–93.
1. Schwab CW, Lawson RB, Lind JF, et al. Aortic injury: comparison ofsupine and upright portable chest films to evaluate the widened medi-astinum. Ann Emerg Med. 1984;13:896–9.
2. Erbel R, Engberding R, Daniel W, et al. Echocardiography in diagnosisof aortic dissection. Lancet. 1989;1:457–61.
3. Yoshida S, Akiba H, Tamakawa M, et al. Thoracic involvement of typeA aortic dissection and intramural hematoma: diagnostic accuracy:comparison of emergency helical CT and surgical findings. Radiology.2003;228:430–5.
4. Sommer T, Fehske W, Holzknecht N, et al. Aortic dissection: acomparative study of diagnosis with spiral CT, multiplanar transesoph-ageal echocardiography, and MR imaging. Radiology. 1996;199:347–52.
5. Zeman RK, Berman PM, Silverman PM, et al. Diagnosis of aorticdissection: value of helical CT with multiplanar reformation andthree-dimensional rendering. AJR Am J Roentgenol. 1995;164:1375–80.
6. Shiga T, Wajima Z, Apfel CC, et al. Diagnostic accuracy of transesoph-ageal echocardiography, helical computed tomography, and magneticresonance imaging for suspected thoracic aortic dissection: systematicreview and meta-analysis. Arch Intern Med. 2006;166:1350–6.
7. Hagan PG, Nienaber CA, Isselbacher EM, et al. The InternationalRegistry of Acute Aortic Dissection (IRAD): new insights into an olddisease. JAMA. 2000;283:897–903.
8. Mirvis SE, Shanmuganathan K, Buell J, et al. Use of spiral computedtomography for the assessment of blunt trauma patients with potentialaortic injury. J Trauma. 1998;45:922–30.
9. Wicky S, Wintermark M, Schnyder P, et al. Imaging of blunt chesttrauma. Eur Radiol. 2000;10:1524–38.
0. Gavant ML, Helical CT. grading of traumatic aortic injuries. Impact onclinical guidelines for medical and surgical management. Radiol Clin
North Am. 1999;37:553–74.vi1. Mirvis SE, Shanmuganathan K, Miller BH, et al. Traumatic aorticinjury: diagnosis with contrast-enhanced thoracic CT: five-year experi-ence at a major trauma center. Radiology. 1996;200:413–22.
2. Scaglione M, Pinto A, Pinto F, et al. Role of contrast-enhanced helicalCT in the evaluation of acute thoracic aortic injuries after blunt chesttrauma. Eur Radiol. 2001;11:2444–8.
3. Ellis JD, Mayo JR. Computed tomography evaluation of traumaticrupture of the thoracic aorta: an outcome study. Can Assoc Radiol J.2007;58:22–6.
4. Quint LE, Francis IR, Williams DM, et al. Evaluation of thoracic aorticdisease with the use of helical CT and multiplanar reconstructions:comparison with surgical findings. Radiology. 1996;201:37–41.
5. ACR Accreditation Program Clinical Image and Quality Guide 2008.Available at: http://www.acr.org/accreditation/computed/qc_forms/image_guide.aspx. Accessed January 7, 2010.
6. American College of Radiology. ACR CT Accreditation Clinical ImageQuality Guide. Available at: http://www.acr.org/accreditation/computed/qc_forms/image_guide.aspx. Accessed January 7, 2010.
7. Practice Guideline for the Performance and Interpretation of ComputedTomography Angiography. Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/dx/cardio/ct_angiography.aspx. Accessed January 7, 2010.
8. Francois CJ, Carr JC. MRI of the thoracic aorta. Cardiol Clin. 2007;25:171–84, vii.
9. Kapustin AJ, Litt HI. Diagnostic imaging for aortic dissection. SeminThorac Cardiovasc Surg. 2005;17:214–23.
0. Cigarroa JE, Isselbacher EM, DeSanctis RW, et al. Diagnostic imagingin the evaluation of suspected aortic dissection. Old standards and newdirections. N Engl J Med. 1993;328:35–43.
1. Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation.2005;112:3802–13.
2. Miller JS, Lemaire SA, Coselli JS. Evaluating aortic dissection: when iscoronary angiography indicated? Heart. 2000;83:615–6.
3. Moore AG, Eagle KA, Bruckman D, et al. Choice of computedtomography, transesophageal echocardiography, magnetic resonanceimaging, and aortography in acute aortic dissection: InternationalRegistry of Acute Aortic Dissection (IRAD). Am J Cardiol. 2002;89:1235–8.
4. Bansal RC, Chandrasekaran K, Ayala K, et al. Frequency and explana-tion of false negative diagnosis of aortic dissection by aortography andtransesophageal echocardiography. J Am Coll Cardiol. 1995;25:1393–401.
5. Shugord WH. Problems in the aortographic diagnosis of dissectinganeuryms of the aorta. N Engl J Med. 1969;280:225–31.
6. Macura KJ, Szarf G, Fishman EK, et al. Role of computed tomographyand magnetic resonance imaging in assessment of acute aortic syn-dromes. Semin Ultrasound CT MR. 2003;24:232–54.
7. Nienaber CA, von Kodolitsch Y, Nicolas V, et al. The diagnosis ofthoracic aortic dissection by noninvasive imaging procedures. N EnglJ Med. 1993;328:1–9.
8. Beebe HG, Kritpracha B, Serres S, et al. Endograft planning withoutpreoperative arteriography: a clinical feasibility study. J Endovasc Ther.2000;7:8–15.
9. Katz ES, Konecky N, Tunick PA, et al. Visualization and identificationof the left common carotid and left subclavian arteries: a transesopha-geal echocardiographic approach. J Am Soc Echocardiogr. 1996;9:58–61.
0. Min JK, Spencer KT, Furlong KT, et al. Clinical features of complica-tions from transesophageal echocardiography: a single-center case seriesof 10,000 consecutive examinations. J Am Soc Echocardiogr. 2005;18:925–9.
1. Lee DY, Williams DM, Abrams GD. The dissected aorta: part II.Differentiation of the true from the false lumen with intravascular US.Radiology. 1997;203:32–6.
2. LePage MA, Quint LE, Sonnad SS, et al. Aortic dissection: CT featuresthat distinguish true lumen from false lumen. AJR Am J Roentgenol.2001;177:207–11.
3. Borner N, Erbel R, Braun B, et al. Diagnosis of aortic dissection bytransesophageal echocardiography. Am J Cardiol. 1984;54:1157–8.
4. Pearson GD, Devereux R, Loeys B, et al. Report of the National Heart,Lung, and Blood Institute and National Marfan Foundation WorkingGroup on research in Marfan syndrome and related disorders. Circula-
tion. 2008;118:785–91.
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
9
9
9
9
9
9
9
10
10
10
10
10
10
10
10
10
10
11
11
11
11
11
11
11
11
11
11
12
12
12
12
12
12
12
e111JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
5. Svensson LG, Crawford ES, Coselli JS, et al. Impact of cardiovascularoperation on survival in the Marfan patient. Circulation. 1989;80:I233–42.
6. Svensson LG, Blackstone EH, Feng J, et al. Are Marfan syndrome andmarfanoid patients distinguishable on long-term follow-up? Ann ThoracSurg. 2007;83:1067–74.
7. Zhu L, Vranckx R, Khau Van Kien P, et al. Mutations in myosin heavychain 11 cause a syndrome associating thoracic aortic aneurysm/aorticdissection and patent ductus arteriosus. Nat Genet. 2006;38:343–9.
8. Loeys BL, Schwarze U, Holm T, et al. Aneurysm syndromes caused bymutations in the TGF-beta receptor. N Engl J Med. 2006;355:788–98.
9. Williams JA, Loeys BL, Nwakanma LU, et al. Early surgical experiencewith Loeys-Dietz: a new syndrome of aggressive thoracic aortic aneu-rysm disease. Ann Thorac Surg. 2007;83:S757–63.
0. Bondy CA. Care of girls and women with Turner syndrome: A guidelineof the Turner Syndrome Study Group. J Clin Endocrinol Metab.2007;92:10–25.
1. Gott VL, Greene PS, Alejo DE, et al. Replacement of the aortic root inpatients with Marfan’s syndrome. N Engl J Med. 1999;340:1307–13.
2. Dietz HC, Pyeritz RE. Mutations in the human gene for fibrillin-1(FBN1) in the Marfan syndrome and related disorders. Hum Mol Genet.1995;4 Spec No:1799–809.
3. Mizuguchi T, Collod-Beroud G, Akiyama T, et al. HeterozygousTGFBR2 mutations in Marfan syndrome. Nat Genet. 2004;36:855–60.
4. De Paepe A, Devereux RB, Dietz HC, et al. Revised diagnostic criteriafor the Marfan syndrome. Am J Med Genet. 1996;62:417–26.
5. van Karnebeek CD, Naeff MS, Mulder BJ, et al. Natural history ofcardiovascular manifestations in Marfan syndrome. Arch Dis Child.2001;84:129–37.
6. Roman MJ, Rosen SE, Kramer-Fox R, et al. Prognostic significance ofthe pattern of aortic root dilation in the Marfan syndrome. J Am CollCardiol. 1993;22:1470–6.
7. Umana JP, Miller DC, Mitchell RS. What is the best treatment forpatients with acute type B aortic dissections: medical, surgical, orendovascular stent-grafting? Ann Thorac Surg. 2002;74:S1840–3.
8. Shores J, Berger KR, Murphy EA, et al. Progression of aortic dilatationand the benefit of long-term beta-adrenergic blockade in Marfan’ssyndrome. N Engl J Med. 1994;330:1335–41.
9. Brooke BS, Habashi JP, Judge DP, et al. Angiotensin II blockade andaortic-root dilation in Marfan’s syndrome. N Engl J Med. 2008;358:2787–95.
0. Lacro RV, Dietz HC, Wruck LM, et al. Rationale and design of arandomized clinical trial of beta-blocker therapy (atenolol) versusangiotensin II receptor blocker therapy (losartan) in individuals withMarfan syndrome. Am Heart J. 2007;154:624–31.
1. Milewicz DM, Dietz HC, Miller DC. Treatment of aortic disease inpatients with Marfan syndrome. Circulation. 2005;111:e150–7.
2. Silverman DI, Burton KJ, Gray J, et al. Life expectancy in the Marfansyndrome. Am J Cardiol. 1995;75:157–60.
3. Finkbohner R, Johnston D, Crawford ES, et al. Marfan syndrome.Long-term survival and complications after aortic aneurysm repair.Circulation. 1995;91:728–33.
4. Svensson LG. Sizing for modified David’s reimplantation procedure.Ann Thorac Surg. 2003;76:1751–3.
5. David TE, Feindel CM, Webb GD, et al. Aortic valve preservation inpatients with aortic root aneurysm: results of the reimplantation tech-nique. Ann Thorac Surg. 2007;83:S732–5.
6. Fazel SS, David TE. Aortic valve-sparing operations for aortic root andascending aortic aneurysms. Curr Opin Cardiol. 2007;22:497–503.
7. Kallenbach K, Baraki H, Khaladj N, et al. Aortic valve-sparing opera-tion in Marfan syndrome: what do we know after a decade? Ann ThoracSurg. 2007;83:S764–8.
8. Patel ND, Weiss ES, Alejo DE, et al. Aortic root operations for Marfansyndrome: a comparison of the Bentall and valve-sparing procedures.Ann Thorac Surg. 2008;85:2003–10.
9. Svensson LG, Deglurkar I, Ung J, et al. Aortic valve repair and rootpreservation by remodeling, reimplantation, and tailoring: technicalaspects and early outcome. J Card Surg. 2007;22:473–9.
0. Burkhart HM, Zehr KJ, Schaff HV, et al. Valve-preserving aortic rootreconstruction: a comparison of techniques. J Heart Valve Dis. 2003;12:62–7.
1. Zehr KJ, Matloobi A, Connolly HM, et al. Surgical management of theaortic root in patients with Marfan syndrome. J Heart Valve Dis.
2005;14:121–8.2. Rossiter JP, Repke JT, Morales AJ, et al. A prospective longitudinalevaluation of pregnancy in the Marfan syndrome. Am J Obstet Gynecol.1995;173:1599–606.
3. Sakaguchi M, Kitahara H, Watanabe T, et al. Successful surgicaltreatment for acute aortic dissection in pregnancy with Marfan’ssyndrome. Jpn J Thorac Cardiovasc Surg. 2005;53:220–2.
4. Singh KK, Rommel K, Mishra A, et al. TGFBR1 and TGFBR2mutations in patients with features of Marfan syndrome and Loeys-Dietzsyndrome. Hum Mutat. 2006;27:770–7.
5. Loeys BL, Chen J, Neptune ER, et al. A syndrome of altered cardio-vascular, craniofacial, neurocognitive and skeletal development causedby mutations in TGFBR1 or TGFBR2. Nat Genet. 2005;37:275–81.
6. Pepin M, Schwarze U, Superti-Furga A, et al. Clinical and geneticfeatures of Ehlers-Danlos syndrome type IV, the vascular type. N EnglJ Med. 2000;342:673–80.
7. Ascione R, Gomes WJ, Bates M, et al. Emergency repair of type Aaortic dissection in type IV Ehlers-Danlos syndrome. Cardiovasc Surg.2000;8:75–8.
8. Sybert VP. Cardiovascular malformations and complications in Turnersyndrome. Pediatrics. 1998;101:E11.
9. Gotzsche CO, Krag-Olsen B, Nielsen J, et al. Prevalence of cardiovas-cular malformations and association with karyotypes in Turner’s syn-drome. Arch Dis Child. 1994;71:433–6.
0. Ostberg JE, Brookes JA, McCarthy C, et al. A comparison of echocar-diography and magnetic resonance imaging in cardiovascular screeningof adults with Turner syndrome. J Clin Endocrinol Metab. 2004;89:5966–71.
1. Lin AE, Silberbach M. Focus on the heart and aorta in Turner syndrome.J Pediatr. 2007;150:572–4.
2. Gravholt CH, Landin-Wilhelmsen K, Stochholm K, et al. Clinical andepidemiological description of aortic dissection in Turner’s syndrome.Cardiol Young. 2006;16:430–6.
3. Bondy CA, Van PL, Bakalov VK, et al. Growth hormone treatment andaortic dimensions in Turner syndrome. J Clin Endocrinol Metab.2006;91:1785–8.
4. Boissonnas CC, Davy C, Bornes M, et al. Careful cardiovascularscreening and follow-up of women with Turner syndrome before andduring pregnancy is necessary to prevent maternal mortality. FertilSteril. 2009;9.e5–7.
5. Matura LA, Sachdev V, Bakalov VK, et al. Growth hormone treatmentand left ventricular dimensions in Turner syndrome. J Pediatr. 2007;150:587–91.
6. Sas TC, Cromme-Dijkhuis AH, de Muinck Keizer-Schrama SM, et al.The effects of long-term growth hormone treatment on cardiac leftventricular dimensions and blood pressure in girls with Turner’ssyndrome. Dutch Working Group on Growth Hormone J Pediatr.1999;135:470–6.
7. Wenstrup RJ, Meyer RA, Lyle JS, et al. Prevalence of aortic rootdilation in the Ehlers-Danlos syndrome. Genet Med. 2002;4:112–7.
8. Gupta PA, Putnam EA, Carmical SG, et al. Ten novel FBN2 mutationsin congenital contractural arachnodactyly: delineation of the molecularpathogenesis and clinical phenotype. Hum Mutat. 2002;19:39–48.
9. Gupta PA, Wallis DD, Chin TO, et al. FBN2 mutation associated withmanifestations of Marfan syndrome and congenital contractural arach-nodactyly. J Med Genet. 2004;41:e56.
0. Adeola T, Adeleye O, Potts JL, et al. Thoracic aortic dissection in apatient with autosomal dominant polycystic kidney disease. J Natl MedAssoc. 2001;93:282–7.
1. Lee CC, Chang WT, Fang CC, et al. Sudden death caused by dissectingthoracic aortic aneurysm in a patient with autosomal dominant polycys-tic kidney disease. Resuscitation. 2004;63:93–6.
2. Purnell R, Williams I, Von Oppell U, et al. Giant aneurysms of thesinuses of Valsalva and aortic regurgitation in a patient with Noonan’ssyndrome. Eur J Cardiothorac Surg. 2005;28:346–8.
3. Morgan JM, Coupe MO, Honey M, et al. Aneurysms of the sinuses ofValsalva in Noonan’s syndrome. Eur Heart J. 1989;10:190–3.
4. Shachter N, Perloff JK, Mulder DG. Aortic dissection in Noonan’ssyndrome (46 XY turner). Am J Cardiol. 1984;54:464–5.
5. McElhinney DB, Krantz ID, Bason L, et al. Analysis of cardiovascularphenotype and genotype-phenotype correlation in individuals with aJAG1 mutation and/or Alagille syndrome. Circulation. 2002;106:2567–74.
6. Albornoz G, Coady MA, Roberts M, et al. Familial thoracic aorticaneurysms and dissections: incidence, modes of inheritance, and phe-
notypic patterns. Ann Thorac Surg. 2006;82:1400–5.
12
12
12
13
13
13
13
13
13
13
13
13
13
14
14
14
14
14
14
14
14
14
14
15
15
15
15
15
15
15
15
15
15
16
16
16
16
16
16
16
16
16
16
17
17
17
17
17
17
17
17
17
e112 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
7. Coady MA, Davies RR, Roberts M, et al. Familial patterns of thoracicaortic aneurysms. Arch Surg. 1999;134:361–7.
8. Stheneur C, Collod-Beroud G, Faivre L, et al. Identification of 23TGFBR2 and 6 TGFBR1 gene mutations and genotype-phenotypeinvestigations in 457 patients with Marfan syndrome type I and II,Loeys-Dietz syndrome and related disorders. Hum Mutat. 2008;29:E284–95.
9. Guo DC, Papke CL, Tran-Fadulu V, et al. Mutations in smooth musclealpha-actin (ACTA2) cause coronary artery disease, stroke, and moya-moya disease, along with thoracic aortic disease. Am J Hum Genet.2009;84:617–27.
0. Biddinger A, Rocklin M, Coselli J, et al. Familial thoracic aorticdilatations and dissections: a case control study. J Vasc Surg. 1997;25:506–11.
1. Milewicz DM, Chen H, Park ES, et al. Reduced penetrance and variableexpressivity of familial thoracic aortic aneurysms/dissections. Am JCardiol. 1998;82:474–9.
2. Guo D, Hasham S, Kuang SQ, et al. Familial thoracic aortic aneurysmsand dissections: genetic heterogeneity with a major locus mapping to5q13-14. Circulation. 2001;103:2461–8.
3. Hasham SN, Willing MC, Guo DC, et al. Mapping a locus for familialthoracic aortic aneurysms and dissections (TAAD2) to 3p24-25. Circu-lation. 2003;107:3184–90.
4. Vaughan CJ, Casey M, He J, et al. Identification of a chromosome11q23.2-q24 locus for familial aortic aneurysm disease, a geneticallyheterogeneous disorder. Circulation. 2001;103:2469–75.
5. Khau Van Kien P, Mathieu F, Zhu L, et al. Mapping of familial thoracicaortic aneurysm/dissection with patent ductus arteriosus to 16p12.2-p13.13. Circulation. 2005;112:200–6.
6. Fatigati V, Murphy R. Actin and tropomyosin Variants. J Bio Chem.1984;259:14383–14388.
7. Braverman AC, Guven H, Beardslee MA, et al. The bicuspid aorticvalve. Curr Probl Cardiol. 2005;30:470–522.
8. Borger MA, David TE. Management of the valve and ascending aorta inadults with bicuspid aortic valve disease. Semin Thorac CardiovascSurg. 2005;17:143–7.
9. Svensson LG, Blackstone EH, Cosgrove DM, III. Surgical options inyoung adults with aortic valve disease. Curr Probl Cardiol. 2003;28:417–80.
0. Svensson LG. Aortic valve stenosis and regurgitation: an overview ofmanagement. J Cardiovasc Surg (Torino). 2008;49:297–303.
1. Huntington K, Hunter AG, Chan KL. A prospective study to assess thefrequency of familial clustering of congenital bicuspid aortic valve.J Am Coll Cardiol. 1997;30:1809–12.
2. Loscalzo ML, Goh DL, Loeys B, et al. Familial thoracic aortic dilationand bicommissural aortic valve: a prospective analysis of natural historyand inheritance. Am J Med Genet A. 2007;143A:1960–7.
3. Svensson LG, Kim KH, Lytle BW, et al. Relationship of aorticcross-sectional area to height ratio and the risk of aortic dissection inpatients with bicuspid aortic valves. J Thorac Cardiovasc Surg. 2003;126:892–3.
4. Larson EW, Edwards WD. Risk factors for aortic dissection: a necropsystudy of 161 cases. Am J Cardiol. 1984;53:849–55.
5. Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, andtricuspid aortic valves in adults having isolated aortic valve replacementfor aortic stenosis, with or without associated aortic regurgitation.Circulation. 2005;111:920–5.
6. Bayford D. An account of a singular case of obstructed deglutition.Memoirs Med Soc London. 1794;2:275–86.
7. Svensson LG, Crawford ES. Cardiovascular and Vascular Disease of theAorta. Philadelphia, PA: WB Saunders Co; 1997.
8. Austin EH, Wolfe WG. Aneurysm of aberrant subclavian artery with areview of the literature. J Vasc Surg. 1985;2:571–7.
9. Stone WM, Brewster DC, Moncure AC, et al. Aberrant right subclavianartery: varied presentations and management options. J Vasc Surg.1990;11:812–7.
0. Branscom JJ, Austin JH. Aberrant right subclavian artery. Findings seenon plain chest roentgenograms Am J Roentgenol Radium Ther NuclMed. 1973;119:539–42.
1. Freed K, Low VH. The aberrant subclavian artery. AJR Am J Roent-genol. 1997;168:481–4.
2. Kouchoukos NT, Masetti P. Aberrant subclavian artery and Kommerellaneurysm: surgical treatment with a standard approach. J Thorac
Cardiovasc Surg. 2007;133:888–92.3. Simon RW, Lachat M, Pfammatter T, et al. Giant aneurysm of anaberrant right subclavian artery from the left aortic arch. J ThoracCardiovasc Surg. 2006;132:1478–9.
4. Ou P, Mousseaux E, Celermajer DS, et al. Aortic arch shape deforma-tion after coarctation surgery: effect on blood pressure response. J Tho-rac Cardiovasc Surg. 2006;132:1105–11.
5. Kutty S, Greenberg RK, Fletcher S, et al. Endovascular stent grafts forlarge thoracic aneurysms after coarctation repair. Ann Thorac Surg.2008;85:1332–8.
6. Lajos TZ, Meckstroth CV, Klassen KP, et al. Pseudocoarctation of theaorta: a variant or an entity? Chest. 1970;58:571–6.
7. Felson B, Palayew MJ. The two types of right aortic arch. Radiology.1963;81:745–59.
8. Kerr GS, Hallahan CW, Giordano J, et al. Takayasu arteritis. Ann InternMed. 1994;120:919–29.
9. Mazlumzadeh M, Hunder GG, Easley KA, et al. Treatment of giant cellarteritis using induction therapy with high-dose glucocorticoids: adouble-blind, placebo-controlled, randomized prospective clinical trial.Arthritis Rheum. 2006;54:3310–8.
0. Ishikawa K, Maetani S. Long-term outcome for 120 Japanese patientswith Takayasu’s disease. Clinical and statistical analyses of relatedprognostic factors Circulation. 1994;90:1855–60.
1. Kyle V, Cawston TE, Hazleman BL. Erythrocyte sedimentation rate andC reactive protein in the assessment of polymyalgia rheumatica/giantcell arteritis on presentation and during follow up. Ann Rheum Dis.1989;48:667–71.
2. Fields CE, Bower TC, Cooper LT, et al. Takayasu’s arteritis: operativeresults and influence of disease activity. J Vasc Surg. 2006;43:64–71.
3. Arend WP, Michel BA, Bloch DA, et al. The American College ofRheumatology 1990 criteria for the classification of Takayasu arteritis.Arthritis Rheum. 1990;33:1129–34.
4. Hunder GG, Bloch DA, Michel BA, et al. The American College ofRheumatology 1990 criteria for the classification of giant cell arteritis.Arthritis Rheum. 1990;33:1122–8.
5. Evaluation of diagnostic (‘classification’) criteria in Behcet’s disease:towards internationally agreed criteria. The International Study Groupfor Behcet’s disease. Br J Rheumatol. 1992;31:299–308.
6. Goie The HS, Steven MM, van der Linden SM, et al. Evaluation ofdiagnostic criteria for ankylosing spondylitis: a comparison of the Rome,New York and modified New York criteria in patients with a positiveclinical history screening test for ankylosing spondylitis. Br J Rheuma-tol. 1985;24:242–9.
7. Hata A, Noda M, Moriwaki R, et al. Angiographic findings of Takayasuarteritis: new classification. Int J Cardiol. 54:Suppl1996;S155–63.
8. Yajima M, Numano F, Park YB, et al. Comparative studies of patientswith Takayasu arteritis in Japan, Korea and India: comparison of clinicalmanifestations, angiography and HLA-B antigen. Jpn Circ J. 1994;58:9–14.
9. Sharma BK, Sagar S, Singh AP, et al. Takayasu arteritis in India. HeartVessels Suppl. 1992;7:37–43.
0. Matsumura K, Hirano T, Takeda K, et al. Incidence of aneurysms inTakayasu’s arteritis. Angiology. 1991;42:308–15.
1. Weaver FA, Kumar SR, Yellin AE, et al. Renal revascularization inTakayasu arteritis-induced renal artery stenosis. J Vasc Surg. 2004;39:749–57.
2. Fava MP, Foradori GB, Garcia CB, et al. Percutaneous transluminalangioplasty in patients with Takayasu arteritis: five-year experience. JVasc Interv Radiol. 1993;4:649–52.
3. Tyagi S, Verma PK, Gambhir DS, et al. Early and long-term results ofsubclavian angioplasty in aortoarteritis (Takayasu disease): comparisonwith atherosclerosis. Cardiovasc Intervent Radiol. 1998;21:219–24.
4. Miyata T, Sato O, Deguchi J, et al. Anastomotic aneurysms aftersurgical treatment of Takayasu’s arteritis: a 40-year experience. J VascSurg. 1998;27:438–45.
5. Hunder GG. Epidemiology of giant-cell arteritis. Cleve Clin J Med.69:Suppl 22002;SII79–82.
6. Nordborg E, Andersson R, Bengtsson BA. Giant cell arteritis. Epidemi-ology and treatment. Drugs Aging. 1994;4:135–44.
7. Chmelewski WL, McKnight KM, Agudelo CA, et al. Presenting featuresand outcomes in patients undergoing temporal artery biopsy. A reviewof 98 patients. Arch Intern Med. 1992;152:1690–5.
8. Nuenninghoff DM, Hunder GG, Christianson TJ, et al. Incidence andpredictors of large-artery complication (aortic aneurysm, aortic dissec-
tion, and/or large-artery stenosis) in patients with giant cell arteritis: a
17
18
18
18
18
18
18
18
18
18
18
18
19
19
19
19
19
19
1919
19
19
20
20
20
20
20
20
20
20
20
2021
21
21
21
21
21
21
21
21
21
22
22
22
22
22
22
22
22
22
22
22
23
23
e113JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
population-based study over 50 years. Arthritis Rheum. 2003;48:3522–31.
9. Lie JT. Aortic and extracranial large vessel giant cell arteritis: a reviewof 72 cases with histopathologic documentation. Semin Arthritis Rheum.1995;24:422–31.
0. Taylor-Gjevre R, Vo M, Shukla D, et al. Temporal artery biopsy forgiant cell arteritis. J Rheumatol. 2005;32:1279–82.
1. Achkar AA, Lie JT, Hunder GG, et al. How does previous corticosteroidtreatment affect the biopsy findings in giant cell (temporal) arteritis? AnnIntern Med. 1994;120:987–92.
2. Hunder GG, Sheps SG, Allen GL, et al. Daily and alternate-daycorticosteroid regimens in treatment of giant cell arteritis: comparison ina prospective study. Ann Intern Med. 1975;82:613–8.
3. Nesher G, Rubinow A, Sonnenblick M. Efficacy and adverse effects ofdifferent corticosteroid dose regimens in temporal arteritis: a retrospec-tive study. Clin Exp Rheumatol. 1997;15:303–6.
4. Salvarani C, Cantini F, Boiardi L, et al. Polymyalgia rheumatica andgiant-cell arteritis. N Engl J Med. 2002;347:261–71.
4a.Hoffman GS, Cid MC, Hellmann DB, et al. A multicenter, randomized,double-blind, placebo-controlled trial of adjuvant methotrexate treat-ment for giant cell arteritis. Arthritis Rheum. 2002;46:1309–18.
5. Azizlerli G, Kose AA, Sarica R, et al. Prevalence of Behcet’s disease inIstanbul, Turkey. Int J Dermatol. 2003;42:803–6.
6. Idil A, Gurler A, Boyvat A, et al. The prevalence of Behcet’s diseaseabove the age of 10 years. The results of a pilot study conducted at thePark Primary Health Care Center in Ankara, Turkey OphthalmicEpidemiol. 2002;9:325–31.
7. Sakane T, Takeno M, Suzuki N, et al. Behcet’s disease. N Engl J Med.1999;341:1284–91.
8. Criteria for diagnosis of Behcet’s disease. International Study Group forBehcet’s Disease. Lancet. 1990;335:1078–80.
9. Sarica-Kucukoglu R, Akdag-Kose A, Kayaball M, et al. Vascularinvolvement in Behcet’s disease: a retrospective analysis of 2319 cases.Int J Dermatol. 2006;45:919–21.
0. Tunaci A, Berkmen YM, Gokmen E. Thoracic involvement in Behcet’sdisease: pathologic, clinical, and imaging features. AJR Am J Roentge-nol. 1995;164:51–6.
1. Kisacikoglu B, Tansal S, Tokcan A, et al. Bechet’s Disease and ArterialAneurysms. Journal of Islamic Academy of Sciences. 1992;290–3.
2. Hosaka A, Miyata T, Shigematsu H, et al. Long-term outcome aftersurgical treatment of arterial lesions in Behcet disease. J Vasc Surg.2005;42:116–21.
3. Park JH, Chung JW, Joh JH, et al. Aortic and arterial aneurysms inbehcet disease: management with stent-grafts: initial experience. Radi-ology. 2001;220:745–50.
4. Brewerton DA, Hart FD, Nicholls A, et al. Ankylosing spondylitis andHL-A 27. Lancet. 1973;1:904–7.
5. Khan MA. Update on spondyloarthropathies. Ann Intern Med. 2002;136:896–907.
6. Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369:1379–90.7. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic
criteria for ankylosing spondylitis. A proposal for modification of theNew York criteriac. Arthritis Rheum. 1984;27:361–8.
8. Roldan CA, Chavez J, Wiest PW, et al. Aortic root disease and valvedisease associated with ankylosing spondylitis. J Am Coll Cardiol.1998;32:1397–404.
9. Osler W. The Gulstonian lectures on malignant endocarditis. BMJ.1885;1:467–70.
0. Follis FM, Paone RF, Wernly JA. Mycotic aneurysm of the ascendingaorta after coronary revascularization. Ann Thorac Surg. 1994;58:236–8.
1. Morgan MB, Cintron G, Balis JU. Infective “mycotic” aortic rootaneurysm following coronary artery bypass grafting. Am J Med.1993;94:550–2.
2. Oz MC, Brener BJ, Buda JA, et al. A ten-year experience with bacterialaortitis. J Vasc Surg. 1989;10:439–49.
3. Cina CS, Arena GO, Fiture AO, et al. Ruptured mycotic thoracoabdomi-nal aortic aneurysms: a report of three cases and a systematic review. JVasc Surg. 2001;33:861–7.
4. Malouf JF, Chandrasekaran K, Orszulak TA. Mycotic aneurysms of thethoracic aorta: a diagnostic challenge. Am J Med. 2003;115:489–96.
5. Byard RW, Jimenez CL, Carpenter BF, et al. Aspergillus-related aortic
thrombosis. CMAJ. 1987;136:155–6.6. Allins AD, Wagner WH, Cossman DV, et al. Tuberculous infection ofthe descending thoracic and abdominal aorta: case report and literaturereview. Ann Vasc Surg. 1999;13:439–44.
7. Lai WW, Colan SD, Easley KA, et al. Dilation of the aortic root inchildren infected with human immunodeficiency virus type 1: TheProspective P2C2 HIV Multicenter Study. Am Heart J. 2001;141:661–70.
8. Brawley JG, Clagett GP. Mycotic aortic aneurysm. J Vasc Surg.2005;42:172.
9. Vilacosta I, Roman JA. Acute aortic syndrome. Heart. 2001;85:365–8.0. Roberts CS, Roberts WC. Aortic dissection with the entrance tear in the
descending thoracic aorta. Analysis of 40 necropsy patients. Ann Surg.1991;213:356–68.
1. Svensson LG, Nadolny EM, Kimmel WA. Multimodal protocol influ-ence on stroke and neurocognitive deficit prevention after ascending/arch aortic operations. Ann Thorac Surg. 2002;74:2040–6.
2. Svensson LG, Labib SB, Eisenhauer AC, et al. Intimal tear withouthematoma: an important variant of aortic dissection that can eludecurrent imaging techniques. Circulation. 1999;99:1331–6.
3. Chirillo F, Salvador L, Bacchion F, et al. Clinical and anatomicalcharacteristics of subtle-discrete dissection of the ascending aorta. Am JCardiol. 2007;100:1314–9.
4. Murray CA, Edwards JE. Spontaneous laceration of ascending aorta.Circulation. 1973;47:848–58.
5. Meszaros I, Morocz J, Szlavi J, et al. Epidemiology and clinicopathol-ogy of aortic dissection. Chest. 2000;117:1271–8.
6. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneu-rysms: a population-based study. Surgery. 1982;92:1103–8.
7. Clouse WD, Hallett JW, Jr., Schaff HV, et al. Acute aortic dissection:population-based incidence compared with degenerative aortic aneu-rysm rupture. Mayo Clin Proc. 2004;79:176–80.
8. Olsson C, Thelin S, Stahle E, et al. Thoracic aortic aneurysm anddissection: increasing prevalence and improved outcomes reported in anationwide population-based study of more than 14,000 cases from 1987to 2002. Circulation. 2006;114:2611–8.
9. Anagnostopoulos CE, Prabhakar MJ, Kittle CF. Aortic dissections anddissecting aneurysms. Am J Cardiol. 1972;30:263–73.
0. HIirst AE Jr., Johns VJ Jr., Kime SW Jr. Dissecting aneurysm of theaorta: a review of 505 cases. Medicine (Baltimore). 1958;37:217–79.
1. Masuda Y, Yamada Z, Morooka N, et al. Prognosis of patients withmedically treated aortic dissections. Circulation. 1991;84:III7–13.
2. Crawford ES, Kirklin JW, Naftel DC, et al. Surgery for acute dissectionof ascending aorta. Should the arch be included? J Thorac CardiovascSurg. 1992;104:46–59.
3. Januzzi JL, Isselbacher EM, Fattori R, et al. Characterizing the youngpatient with aortic dissection: results from the International Registry ofAortic Dissection (IRAD). J Am Coll Cardiol. 2004;43:665–9.
4. Milewicz DM, Michael K, Fisher N, et al. Fibrillin-1 (FBN1) mutationsin patients with thoracic aortic aneurysms. Circulation. 1996;94:2708–11.
5. Francke U, Berg MA, Tynan K, et al. A Gly1127Ser mutation in anEGF-like domain of the fibrillin-1 gene is a risk factor for ascendingaortic aneurysm and dissection. Am J Hum Genet. 1995;56:1287–96.
6. Hatzaras IS, Bible JE, Koullias GJ, et al. Role of exertion or emotion asinciting events for acute aortic dissection. Am J Cardiol. 2007;100:1470–2.
6a.Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascular-ization. J Am Coll Cardiol. 2009;53:530–53.
7. Pape LA, Tsai TT, Isselbacher EM, et al. Aortic diameter � or � 5.5 cmis not a good predictor of type A aortic dissection: observations from theInternational Registry of Acute Aortic Dissection (IRAD). Circulation.2007;116:1120–7.
8. Miller DC, Stinson EB, Oyer PE, et al. Operative treatment of aorticdissections. Experience with 125 patients over a sixteen-year period.J Thorac Cardiovasc Surg. 1979;78:365–82.
9. Cachera JP, Vouhe PR, Loisance DY, et al. Surgical management ofacute dissections involving the ascending aorta. Early and late results in38 patients. J Thorac Cardiovasc Surg. 1981;82:576–84.
0. Jex RK, Schaff HV, Piehler JM, et al. Repair of ascending aorticdissection. Influence of associated aortic valve insufficiency on early andlate results. J Thorac Cardiovasc Surg. 1987;93:375–84.
1. Fann JI, Smith JA, Miller DC, et al. 1995 Surgical management of aortic
dissection during a 30-year period. Circulation. 1995;92:II113–21.
23
23
23
23
23
23
23
23
24
24
24
24
24
24
24
24
24
24
25
25
25
25
25
25
25
25
25
25
26
26
26
26
26
26
26
26
26
26
27
27
27
27
27
27
27
27
27
27
28
28
28
28
28
28
28
e114 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
2. Mazzucotelli JP, Deleuze PH, Baufreton C, et al. Preservation of theaortic valve in acute aortic dissection: long-term echocardiographicassessment and clinical outcome. Ann Thorac Surg. 1993;55:1513–7.
3. Von Segesser LK, Lorenzetti E, Lachat M, et al. Aortic valve preser-vation in acute type A dissection: is it sound? J Thorac Cardiovasc Surg.1996;111:381–90.
4. Massimo CG, Presenti LF, Marranci P, et al. Extended and total aorticresection in the surgical treatment of acute type A aortic dissection:experience with 54 patients. Ann Thorac Surg. 1998;46:420–4.
5. Movsowitz HD, Levine RA, Hilgenberg AD, et al. Transesophagealechocardiographic description of the mechanisms of aortic regurgitationin acute type A aortic dissection: implications for aortic valve repair.J Am Coll Cardiol. 2000;36:884–90.
6. Januzzi JL, Eagle KA, Cooper JV, et al. Acute aortic dissectionpresenting with congestive heart failure: results from the InternationalRegistry of Acute Aortic Dissection. J Am Coll Cardiol. 2005;46:733–5.
7. Sullivan PR, Wolfson AB, Leckey RD, et al. Diagnosis of acute thoracicaortic dissection in the emergency department. Am J Emerg Med.2000;18:46–50.
8. Baydin A, Nargis C, Nural MS, et al. Painless, acute aortic dissectionpresenting as an acute stroke. Mt Sinai J Med. 2006;73:1129–31.
9. Ayrik C, Cece H, Aslan O, et al. Seeing the invisible: painless aorticdissection in the emergency setting. Emerg Med J. 2006;23:e24.
0. Young J, Herd AM. Painless acute aortic dissection and rupturepresenting as syncope. J Emerg Med. 2002;22:171–4.
1. Park SW, Hutchison S, Mehta RH, et al. Association of painless acuteaortic dissection with increased mortality. Mayo Clin Proc. 2004;79:1252–7.
2. Nallamothu BK, Mehta RH, Saint S, et al. Syncope in acute aorticdissection: diagnostic, prognostic, and clinical implications. Am J Med.2002;113:468–71.
3. Svensson LG, Crawford ES. Aortic dissection and aortic aneurysmsurgery: clinical observations, experimental investigations, and statisti-cal analyses. Part II Curr Probl Surg. 1992;29:913–1057.
4. Williams DM, Lee DY, Hamilton BH, et al. The dissected aorta: part III.Anatomy and radiologic diagnosis of branch-vessel compromise. Radi-ology. 1997;203:37–44.
5. Khan IA, Nair CK. Clinical, diagnostic, and management perspectivesof aortic dissection. Chest. 2002;122:311–28.
6. Bossone E, Rampoldi V, Nienaber CA, et al. Usefulness of pulse deficitto predict in-hospital complications and mortality in patients with acutetype A aortic dissection. Am J Cardiol. 2002;89:851–5.
7. Yagdi T, Atay Y, Engin C, et al. Impact of organ malperfusion onmortality and morbidity in acute type A aortic dissections. J Card Surg.2006;21:363–9.
8. Henke PK, Williams DM, Upchurch GR, Jr., et al. Acute limb ischemiaassociated with type B aortic dissection: clinical relevance and therapy.Surgery. 2006;140:532–9.
9. Tsai TT, Bossone E, Isselbacher EM, et al. Clinical characteristics ofhypotension in patients with acute aortic dissection. Am J Cardiol.2005;95:48–52.
0. Neri E, Toscano T, Papalia U, et al. Proximal aortic dissection withcoronary malperfusion: presentation, management, and outcome. J Tho-rac Cardiovasc Surg. 2001;121:552–60.
1. Lee SI, Pyun SB, Jang DH. Dysphagia and hoarseness associated withpainless aortic dissection: a rare case of cardiovocal syndrome. Dyspha-gia. 2006;21:129–32.
2. Hansen MS, Nogareda GJ, Hutchison SJ. Frequency of and inappropri-ate treatment of misdiagnosis of acute aortic dissection. Am J Cardiol.2007;99:852–6.
3. Gaul C, Dietrich W, Friedrich I, et al. Neurological symptoms in type Aaortic dissections. Stroke. 2007;38:292–7.
4. Zull DN, Cydulka R. Acute paraplegia: a presenting manifestation ofaortic dissection. Am J Med. 1988;84:765–70.
5. Fessler AJ, Alberts MJ. Stroke treatment with tissue plasminogenactivator in the setting of aortic dissection. Neurology. 2000;54:1010.
6. Morita S, Shibata M, Nakagawa Y, et al. Painless acute aortic dissectionwith a left hemiparesis. Neurocrit Care. 2006;4:234–6.
7. Armstrong WF, Bach DS, Carey LM, et al. Clinical and echocardio-graphic findings in patients with suspected acute aortic dissection. AmHeart J. 1998;136:1051–60.
8. Garcia-Jimenez A, Peraza TA, Martinez LG, et al. Cardiac tamponadeby aortic dissection in a hospital without cardiothoracic surgery. Chest.
1993;104:290–1.9. Pretre R, Von Segesser LK. Aortic dissection. Lancet. 1997;349:1461–4.
0. Gilon D, Mehta RH, Oh JK, et al. Characteristics and in-hospitaloutcomes of patients with cardiac tamponade complicating type A acuteaortic dissection. Am J Cardiol. 2009;103:1029–31.
1. von Kodolitsch Y, Schwartz AG, Nienaber CA. Clinical prediction ofacute aortic dissection. Arch Intern Med. 2000;160:2977–82.
2. Kawarabuki K, Sakakibara T, Hirai M, et al. Acute aortic dissectionpresenting as a neurologic disorder. J Stroke Cerebrovasc Dis. 2006;15:26–9.
3. Kuhlmann TP, Powers RD. Painless aortic dissection: an unusual causeof syncope. Ann Emerg Med. 1984;13:549–51.
4. Spittell PC, Spittell JA, Jr., Joyce JW, et al. Clinical features anddifferential diagnosis of aortic dissection: experience with 236 cases(1980 through 1990). Mayo Clin Proc. 1993;68:642–51.
5. Slater E. Aortic dissection: presentation and diagnosis. In: DorghaziRM, Slater E, editors. Aortic Dissection. New York, NY: McGraw-Hill1983;61–70.
6. Sanders JS, Ferguson DW, Mark AL. Arterial baroreflex control ofsympathetic nerve activity during elevation of blood pressure in normalman: dominance of aortic baroreflexes. Circulation. 1988;77:279–88.
7. Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosisand management: Part I: from etiology to diagnostic strategies. Circu-lation. 2003;108:628–35.
8. Holloway SF, Fayad PB, Kalb RG, et al. Painless aortic dissectionpresenting as a progressive myelopathy. J Neurol Sci. 1993;120:141–4.
9. Syed MA, Fiad TM. Transient paraplegia as a presenting feature ofaortic dissection in a young man. Emerg Med J. 2002;19:174–5.
0. Zaidat OO, Ubogu EE, Lerner AJ. Recurrent transient ischemic attacksas the initial presenting manifestation of type A aortic dissection. AnnVasc Surg. 2002;16:676–8.
1. John LC. Fluctuating neurological deficit with acute aortic dissection:the omega sign. Int J Cardiol. 2006;106:130–1.
2. Hata N, Tanaka K, Imaizumi T, et al. Clinical significance of pleuraleffusion in acute aortic dissection. Chest. 2002;121:825–30.
3. Gandelman G, Barzilay N, Krupsky M, et al. Left pleural hemorrhagiceffusion. A presenting sign of thoracic aortic dissecting aneurysm.Chest. 1994;106:636–8.
4. Tristano AG, Tairouz Y. Painless right hemorrhagic pleural effusions aspresentation sign of aortic dissecting aneurysm. Am J Med. 2005;118:794–5.
5. Little S, Johnson J, Moon BY, et al. Painless left hemorrhagic pleuraleffusion: An unusual presentation of dissecting ascending aortic aneu-rysm. Chest. 1999;116:1478–80.
6. Massetti M, Babatasi G, Saloux E, et al. Aorto-pulmonary fistula: a rareevent in the evolution of a dissecting aneurysm of the thoracic aorta. EurJ Cardiothorac Surg. 1997;11:994–6.
7. Takahashi M, Ikeda U, Shimada K, et al. Unilateral pulmonary edemarelated to pulmonary artery compression resulting from acute dissectingaortic aneurysm. Am Heart J. 1993;126:1225–7.
8. Masuo M, Takano H, Takamoto S, et al. Pulmonary artery obstructioncaused by thoracic aortic dissection: a case with unique pathologicalfindings. Circ J. 2004;68:392–5.
9. Guidetti AS, Pik A, Peer A, et al. Haemoptysis as the sole presentingsymptom of dissection of the aorta. Thorax. 1989;44:444–5.
0. Dickens P, Pittaluga S, Chau CH. Sudden death presenting as massivehaemoptysis due to ruptured intrapulmonary aortic aneurysm. ForensicSci Int. 1993;60:121–5.
1. Born C, Forster A, Rock C, et al. A case of an upper gastrointestinalbleeding due to a ruptured dissection of a right aortic arch. CardiovascIntervent Radiol. 2003;26:506–9.
2. Nath HP, Jaques PF, Soto B, et al. Aortic dissection masquerading asgastrointestinal disease. Cardiovasc Intervent Radiol. 1986;9:37–41.
3. Hollander JE, Quick G. Aortoesophageal fistula: a comprehensivereview of the literature. Am J Med. 1991;91:279–87.
4. Prisant LM, Nalamolu VR. Aortic dissection. J Clin Hypertens (Green-wich). 2005;7:367–71.
5. Suzuki T, Mehta RH, Ince H, et al. Clinical profiles and outcomes ofacute type B aortic dissection in the current era: lessons from theInternational Registry of Aortic Dissection (IRAD). Circulation. 2003;108 Suppl 1:II312–7.
6. Trimarchi S, Nienaber CA, Rampoldi V, et al. Role and results ofsurgery in acute type B aortic dissection: insights from the InternationalRegistry of Acute Aortic Dissection (IRAD). Circulation. 2006;114:
I357–64.
28
28
28
29
29
29
29
29
29
29
29
29
29
30
30
30
30
30
30
30
30
30
30
31
31
31
31
31
31
31
31
31
31
32
32
32
32
32
32
32
32
32
32
33
33
33
33
33
33
33
33
e115JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
7. Tsai TT, Fattori R, Trimarchi S, et al. Long-term survival in patientspresenting with type B acute aortic dissection: insights from theInternational Registry of Acute Aortic Dissection. Circulation. 2006;114:2226–31.
8. Mehta RH, O’Gara PT, Bossone E, et al. Acute type A aortic dissectionin the elderly: clinical characteristics, management, and outcomes in thecurrent era. J Am Coll Cardiol. 2002;40:685–92.
9. Nienaber CA, Fattori R, Mehta RH, et al. Gender-related differences inacute aortic dissection. Circulation. 2004;109:3014–21.
0. Evangelista A, Mukherjee D, Mehta RH, et al. Acute intramuralhematoma of the aorta: a mystery in evolution. Circulation. 2005;111:1063–70.
1. Nienaber CA, von KY, Petersen B, et al. Intramural hemorrhage of thethoracic aorta. Diagnostic and therapeutic implications. Circulation.1995;92:1465–72.
2. Mohr-Kahaly S, Erbel R, Kearney P, et al. Aortic intramural hemorrhagevisualized by transesophageal echocardiography: findings and prognos-tic implications. J Am Coll Cardiol. 1994;23:658–64.
3. O’Gara PT, DeSanctis RW. Acute aortic dissection and its variants.Toward a common diagnostic and therapeutic approach. Circulation.1995;92:1376–8.
4. Nienaber CA, Sievers HH. Intramural hematoma in acute aortic syn-drome: more than one variant of dissection? Circulation. 2002;106:284–5.
5. Vilacosta I, San Roman JA, Ferreiros J, et al. Natural history and serialmorphology of aortic intramural hematoma: a novel variant of aorticdissection. Am Heart J. 1997;134:495–507.
6. von Kodolitsch Y, Csosz SK, Koschyk DH, et al. Intramural hematomaof the aorta: predictors of progression to dissection and rupture.Circulation. 2003;107:1158–63.
7. Kaji S, Akasaka T, Katayama M, et al. Long-term prognosis of patientswith type B aortic intramural hematoma. Circulation. 2003;108 Suppl1:II307–11.
8. Sueyoshi E, Imada T, Sakamoto I, et al. Analysis of predictive factorsfor progression of type B aortic intramural hematoma with computedtomography. J Vasc Surg. 2002;35:1179–83.
9. Williams MP, Farrow R. Atypical patterns in the CT diagnosis of aorticdissection. Clin Radiol. 1994;49:686–9.
0. Sueyoshi E, Matsuoka Y, Sakamoto I, et al. Fate of intramuralhematoma of the aorta: CT evaluation. J Comput Assist Tomogr.1997;21:931–8.
1. Moizumi Y, Komatsu T, Motoyoshi N, et al. Clinical features andlong-term outcome of type A and type B intramural hematoma of theaorta. J Thorac Cardiovasc Surg. 2004;127:421–7.
2. Choi SH, Choi SJ, Kim JH, et al. Useful CT findings for predicting theprogression of aortic intramural hematoma to overt aortic dissection.J Comput Assist Tomogr. 2001;25:295–9.
3. Moriyama Y, Yotsumoto G, Kuriwaki K, et al. Intramural hematoma ofthe thoracic aorta. Eur J Cardiothorac Surg. 1998;13:230–9.
4. Kaji S, Akasaka T, Horibata Y, et al. Long-term prognosis of patientswith type A aortic intramural hematoma. Circulation. 2002;106:I248–52.
5. Murray JG, Manisali M, Flamm SD, et al. Intramural hematoma of thethoracic aorta: MR image findings and their prognostic implications.Radiology. 1997;204:349–55.
6. Lee YK, Seo JB, Jang YM, et al. Acute and chronic complications ofaortic intramural hematoma on follow-up computed tomography: inci-dence and predictor analysis. J Comput Assist Tomogr. 2007;31:435–40.
7. Song JK, Kim HS, Kang DH, et al. Different clinical features of aorticintramural hematoma versus dissection involving the ascending aorta.J Am Coll Cardiol. 2001;37:1604–10.
8. Song JM, Kim HS, Song JK, et al. Usefulness of the initial noninvasiveimaging study to predict the adverse outcomes in the medical treatmentof acute type A aortic intramural hematoma. Circulation. 2003;108Suppl 1:II324–8.
9. Stanson AW, Kazmier FJ, Hollier LH, et al. Penetrating atheroscleroticulcers of the thoracic aorta: natural history and clinicopathologiccorrelations. Ann Vasc Surg. 1986;1:15–23.
0. Cho KR, Stanson AW, Potter DD, et al. Penetrating atherosclerotic ulcerof the descending thoracic aorta and arch. J Thorac Cardiovasc Surg.2004;127:1393–9.
1. Harris JA, Bis KG, Glover JL, et al. Penetrating atherosclerotic ulcers of
the aorta. J Vasc Surg. 1994;19:90–8.2. Williams DM, Cronin P, Dasika N, et al. Aortic branch artery pseudoa-neurysms accompanying aortic dissection. Part I Pseudoaneurysm anat-omy. J Vasc Interv Radiol. 2006;17:765–71.
3. Pretre R, Chilcott M. Blunt trauma to the heart and great vessels. N EnglJ Med. 1997;336:626–32.
4. Heller G, Immer FF, Savolainen H, et al. Aortic rupture in high-speedskiing crashes. J Trauma. 2006;61:979–80.
5. Gurkan S, Sunar H, Canbaz S, et al. Late manifestation of a pseudoan-eurysm in the descending thoracic aorta. Vasa. 2006;35:112–4.
6. Patel TM, Shah SC, Ranjan A. Unusual retrograde aortic arch dissectionduring percutaneous coronary intervention: a case report. Angiology.2006;57:501–5.
7. Lundevall J. Traumatic rupture of the aorta, with special reference toroad accidents. Acta Pathol Microbiol Scand. 1964;62:29–33.
8. Parmley LF, Mattingly TW, Manion WC, et al. Nonpenetrating trau-matic injury of the aorta. Circulation. 1958;17:1086–101.
9. Richens D, Kotidis K, Neale M, et al. Rupture of the aorta followingroad traffic accidents in the United Kingdom 1992-1999. The results ofthe co-operative crash injury study. Eur J Cardiothorac Surg. 2003;23:143–8.
0. Joyce JW, Fairbairn JF, Kincaid OW, et al. Aneurysms of the thoracicaorta. a clinical study with special reference to prognosis. Circulation.1964;29:176–81.
1. Pate JW, Cole FH Jr., Walker WA, et al. Penetrating injuries of theaortic arch and its branches. Ann Thorac Surg. 1993;55:586–92.
2. Bruckner BA, DiBardino DJ, Cumbie TC, et al. Critical evaluation ofchest computed tomography scans for blunt descending thoracic aorticinjury. Ann Thorac Surg. 2006;81:1339–46.
3. Fabian TC, Davis KA, Gavant ML, et al. Prospective study of bluntaortic injury: helical CT is diagnostic and antihypertensive therapyreduces rupture. Ann Surg. 1998;227:666–76.
4. Roberts WC, Ko JM, Moore TR, et al. Causes of pure aortic regurgita-tion in patients having isolated aortic valve replacement at a single UStertiary hospital (1993 to 2005). Circulation. 2006;114:422–9.
5. Weber T, Hogler S, Auer J, et al. D-dimer in acute aortic dissection.Chest. 2003;123:1375–8.
6. Eggebrecht H, Naber CK, Bruch C, et al. Value of plasma fibrinD-dimers for detection of acute aortic dissection. J Am Coll Cardiol.2004;44:804–9.
7. Suzuki T, Katoh H, Watanabe M, et al. Novel biochemical diagnosticmethod for aortic dissection. Results of a prospective study using animmunoassay of smooth muscle myosin heavy chain. Circulation.1996;93:1244–9.
8. Suzuki T, Katoh H, Tsuchio Y, et al. Diagnostic implications of elevatedlevels of smooth-muscle myosin heavy-chain protein in acute aorticdissection. The Smooth Muscle Myosin Heavy Chain Study. Ann InternMed. 2000;133:537–41.
9. American College of Emergency PhysiciansClinical policy: criticalissues in the evaluation and management of adult patients presentingwith suspected pulmonary embolism. Ann Emerg Med. 2003;41:257–70.
0. Marill KA. Serum D-dimer is a sensitive test for the detection of acuteaortic dissection: a pooled meta-analysis. J Emerg Med. 2008;34:367–75.
1. Ohlmann P, Faure A, Morel O, et al. Diagnostic and prognostic value ofcirculating D-dimers in patients with acute aortic dissection. Crit CareMed. 2006;34:1358–64.
2. Elefteriades JA, Barrett PW, Kopf GS. Litigation in nontraumatic aorticdiseases: a tempest in the malpractice maelstrom. Cardiology. 2008;109:263–72.
3. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines forthe management of patients with ST-elevation myocardial infarction:executive summary. J Am Coll Cardiol. 2004;44:671–719.
4. Estrera AL, Miller CC III, Safi HJ, et al. Outcomes of medicalmanagement of acute type B aortic dissection. Circulation. 2006;114:I384–I389.
5. Umana JP, Lai DT, Mitchell RS, et al. Is medical therapy still theoptimal treatment strategy for patients with acute type B aortic dissec-tions? J Thorac Cardiovasc Surg. 2002;124:896–910.
6. Mehta RH, Suzuki T, Hagan PG, et al. Predicting death in patients withacute type A aortic dissection. Circulation. 2002;105:200–6.
7. Chiappini B, Schepens M, Tan E, et al. Early and late outcomes of acutetype A aortic dissection: analysis of risk factors in 487 consecutive
patients. Eur Heart J. 2005;26:180–6.
33
33
34
34
34
34
34
34
34
34
34
34
35
35
35
35
35
35
35
35
35
35
36
36
36
36
36
36
36
36
36
36
37
37
37
37
37
37
37
37
37
37
38
38
38
38
38
38
38
38
38
38
39
e116 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
8. Furman MI, Dauerman HL, Goldberg RJ, et al. Twenty-two year (1975to 1997) trends in the incidence, in-hospital and long-term case fatalityrates from initial Q-wave and non-Q-wave myocardial infarction: amulti-hospital, community-wide perspective. J Am Coll Cardiol. 2001;37:1571–80.
9. Isselbacher E. Cecil Medicine. 23rd ed. Philadelphia, PA: ElsevierHealth Sciences, 2008.
0. Libby P, Bonow RO, Mann DL, Zipes DP. Braunwald’s Heart Disease:A Textbook of Cardiovascular Medicine. 8th ed. Philadelphia, PA. 2007.
1. Townsend CM, Beauchamp RD, Evers BM, Mattox KL. SabistonTextbook of Surgery. 18th ed. Philadelphia, PA: Elsevier HealthSciences, 2008.
2. Mukherjee D, Eagle KA. Aortic dissection: an update. Curr ProblCardiol. 2005;30:287–325.
3. Januzzi JL, Sabatine MS, Eagle KA, et al. Iatrogenic aortic dissection.Am J Cardiol. 2002;89:623–6.
4. Kario K, Ishikawa J, Pickering TG, et al. Morning hypertension: thestrongest independent risk factor for stroke in elderly hypertensivepatients. Hypertens Res. 2006;29:581–7.
5. Khoynezhad A, Plestis KA. Managing emergency hypertension in aorticdissection and aortic aneurysm surgery. J Card Surg. 2006;21 Suppl1:S3–7.
6. Vriend JW, Mulder BJ. Late complications in patients after repair ofaortic coarctation: implications for management. Int J Cardiol. 2005;101:399–406.
7. Eggebrecht H, Schmermund A, von Birgelen C, et al. Resistanthypertension in patients with chronic aortic dissection. J Hum Hyper-tens. 2005;19:227–31.
8. Kim KH, Moon IS, Park JS, et al. Nicardipine hydrochloride injectablephase IV open-label clinical trial: study on the anti-hypertensive effectand safety of nicardipine for acute aortic dissection. J Int Med Res.2002;30:337–45.
9. Isselbacher EM, Cigarroa JE, Eagle KA. Cardiac tamponade complicat-ing proximal aortic dissection. Is pericardiocentesis harmful? Circula-tion. 1994;90:2375–8.
0. Kaji S, Nishigami K, Akasaka T, et al. Prediction of progression orregression of type A aortic intramural hematoma by computed tomog-raphy. Circulation. 1999;100:II281–6.
1. Motoyoshi N, Moizumi Y, Komatsu T, et al. Intramural hematoma anddissection involving ascending aorta: the clinical features and prognosis.Eur J Cardiothorac Surg. 2003;24:237–42.
2. Moizumi Y, Komatsu T, Motoyoshi N, et al. Management of patientswith intramural hematoma involving the ascending aorta. J ThoracCardiovasc Surg. 2002;124:918–24.
3. Elefteriades JA, Hartleroad J, Gusberg RJ, et al. Long-term experiencewith descending aortic dissection: the complication-specific approach.Ann Thorac Surg. 1992;53:11–20.
4. Tittle SL, Lynch RJ, Cole PE, et al. Midterm follow-up of penetratingulcer and intramural hematoma of the aorta. J Thorac Cardiovasc Surg.2002;123:1051–9.
5. Nagy K, Fabian T, Rodman G, et al. Guidelines for the diagnosis andmanagement of blunt aortic injury: an EAST Practice ManagementGuidelines Work Group. J Trauma. 2000;48:1128–43.
6. Xenos ES, Abedi NN, Davenport DL, et al. Meta-analysis of endovas-cular vs open repair for traumatic descending thoracic aortic rupture. JVasc Surg. 2008;48:1343–51.
7. Galli R, Pacini D, Di BR, et al. Surgical indications and timing of repairof traumatic ruptures of the thoracic aorta. Ann Thorac Surg. 1998;65:461–4.
8. Pate JW, Gavant ML, Weiman DS, et al. Traumatic rupture of the aorticisthmus: program of selective management. World J Surg. 1999;23:59–63.
9. Svensson LG, Antunes MD, Kinsley RH. Traumatic rupture of thethoracic aorta. A report of 14 cases and a review of the literature. S AfrMed J. 1985;67:853–7.
0. von Oppell UO, Dunne TT, De Groot MK, et al. Traumatic aorticrupture: twenty-year metaanalysis of mortality and risk of paraplegia.Ann Thorac Surg. 1994;58:585–93.
1. Katz NM, Blackstone EH, Kirklin JW, et al. Incremental risk factors forspinal cord injury following operation for acute traumatic aortic tran-section. J Thorac Cardiovasc Surg. 1981;81:669–74.
2. Verdant A, Page A, Cossette R, et al. Surgery of the descending thoracicaorta: spinal cord protection with the Gott shunt. Ann Thorac Surg.
1988;46:147–54.3. Hilgenberg AD, Logan DL, Akins CW, et al. Blunt injuries of thethoracic aorta. Ann Thorac Surg. 1992;53:233–8.
4. Pate JW, Fabian TC, Walker WA. Acute traumatic rupture of the aorticisthmus: repair with cardiopulmonary bypass. Ann Thorac Surg. 1995;59:90–8.
5. Lettinga-van de Poll T, Schurink GW, De Haan MW, et al. Endovas-cular treatment of traumatic rupture of the thoracic aorta. Br J Surg.2007;94:525–33.
6. Muhs BE, Balm R, White GH, et al. Anatomic factors associated withacute endograft collapse after Gore TAG treatment of thoracic aorticdissection or traumatic rupture. J Vasc Surg. 2007;45:655–61.
7. Neschis DG, Moaine S, Gutta R, et al. Twenty consecutive cases ofendograft repair of traumatic aortic disruption: lessons learned. J VascSurg. 2007;45:487–92.
8. Marcheix B, Dambrin C, Bolduc JP, et al. Endovascular repair oftraumatic rupture of the aortic isthmus: midterm results. J ThoracCardiovasc Surg. 2006;132:1037–41.
9. Kato N, Dake MD, Miller DC, et al. Traumatic thoracic aortic aneurysm:treatment with endovascular stent-grafts. Radiology. 1997;205:657–62.
0. Tehrani HY, Peterson BG, Katariya K, et al. Endovascular repair ofthoracic aortic tears. Ann Thorac Surg. 2006;82:873–7.
1. Svensson LG, Kouchoukos NT, Miller DC, et al. Expert consensusdocument on the treatment of descending thoracic aortic disease usingendovascular stent-grafts. Ann Thorac Surg. 2008;85:S1–S41.
2. Clouse WD, Hallett JW Jr., Schaff HV, et al. Improved prognosis ofthoracic aortic aneurysms: a population-based study. JAMA. 1998;280:1926–9.
3. Cambria RA, Gloviczki P, Stanson AW, et al. Outcome and expansionrate of 57 thoracoabdominal aortic aneurysms managed nonoperatively.Am J Surg. 1995;170:213–7.
4. Coady MA, Rizzo JA, Hammond GL, et al. What is the appropriate sizecriterion for resection of thoracic aortic aneurysms? J Thorac CardiovascSurg. 1997;113:476–91.
5. Davies RR, Goldstein LJ, Coady MA, et al. Yearly rupture or dissectionrates for thoracic aortic aneurysms: simple prediction based on size. AnnThorac Surg. 2002;73:17–27.
6. Josserand J, Boura B, Yakhou L, et al. Rupture of a thoracic aorticaneurysm into the right pleural cavity. Ann Fr Anesth Reanim. 2006;25:997–9.
7. Eagle KA, Armstrong WF. Disease of the aorta. In: Dale DC, FedermanDD, editors. Scientific American Medicine. New York, NY: WebMD;2003.
8. Tsokos M, Byard RW. Massive, fatal aspiration of blood: not necessarilya result of trauma. Am J Forensic Med Pathol. 2007;28:53–4.
9. Crawford ES, Crawford JL, Safi HJ, et al. Thoracoabdominal aorticaneurysms: preoperative and intraoperative factors determining imme-diate and long-term results of operations in 605 patients. J Vasc Surg.1986;3:389–404.
0. Estrera AL, Miller CC III, Chen EP, et al. Descending thoracic aorticaneurysm repair: 12-year experience using distal aortic perfusion andcerebrospinal fluid drainage. Ann Thorac Surg. 2005;80:1290–6.
1. Svensson LG, Crawford ES, Hess KR, et al. Experience with 1509patients undergoing thoracoabdominal aortic operations. J Vasc Surg.1993;17:357–68.
2. Svensson LG, Crawford ES, Hess KR, et al. Variables predictive ofoutcome in 832 patients undergoing repairs of the descending thoracicaorta. Chest. 1993;104:1248–53.
3. Achneck H, Modi B, Shaw C, et al. Ascending thoracic aneurysms areassociated with decreased systemic atherosclerosis. Chest. 2005;128:1580–6.
4. Anandaraja S, Mukhopadhyay S, Roy S, et al. Left main coronary arteryaneurysm in Takayasu arteritis. Echocardiography. 2006;23:430–1.
5. Haddy SM, Bhatt M, Patel JM. Right coronary artery aneurysm in apatient with Takayasu’s arteritis. Echocardiography. 2007;24:1108–9.
6. Chun PK, Jones R, Robinowitz M, et al. Coronary ostial stenosis inTakayasu’s arteritis. Chest. 1980;78:330–1.
7. Kihara M, Kimura K, Yakuwa H, et al. Isolated left coronary ostialstenosis as the sole arterial involvement in Takayasu’s disease. J InternMed. 1992;232:353–5.
8. Feder W, Uerbach R. “Purple toes”: an uncommon sequela of oralcoumarin drug therapy. Ann Intern Med. 1961;55:911–7.
9. Rosansky SJ, Deschamps EG. Multiple cholesterol emboli syndromeafter angiography. Am J Med Sci. 1984;288:45–8.
0. Ramirez G, O’Neill WM Jr., Lambert R, et al. Cholesterol embolization:
a complication of angiography. Arch Intern Med. 1978;138:1430–2.
39
39
39
39
39
39
39
39
39
40
40
40
40
40
40
40
40
40
40
41
41
41
41
41
41
41
41
41
41
42
42
42
42
42
42
42
42
42
42
43
43
43
43
43
43
43
43
43
43
43
e117JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
1. Drost H, Buis B, Haan D, et al. Cholesterol embolism as a complicationof left heart catheterisation. Report of seven cases. Br Heart J. 1984;52:339–42.
2. Hyman BT, Landas SK, Ashman RF, et al. Warfarin-related purple toessyndrome and cholesterol microembolization. Am J Med. 1987;82:1233–7.
3. Shapiro LS. Cholesterol embolization after treatment with tissue plas-minogen activator. N Engl J Med. 1989;321:1270.
4. Bols A, Nevelsteen A, Verhaeghe R. Atheromatous embolizationprecipitated by oral anticoagulants. Int Angiol. 1994;13:271–4.
5. Scolari F, Bracchi M, Valzorio B, et al. Cholesterol atheromatousembolism: an increasingly recognized cause of acute renal failure.Nephrol Dial Transplant. 1996;11:1607–12.
6. Dressler FA, Craig WR, Castello R, et al. Mobile aortic atheroma andsystemic emboli: efficacy of anticoagulation and influence of plaquemorphology on recurrent stroke. J Am Coll Cardiol. 1998;31:134–8.
7. Davila-Roman VG, Kouchoukos NT, Schechtman KB, et al. Athero-sclerosis of the ascending aorta is a predictor of renal dysfunction aftercardiac operations. J Thorac Cardiovasc Surg. 1999;117:111–6.
8. Blankenship JC, Butler M, Garbes A. Prospective assessment ofcholesterol embolization in patients with acute myocardial infarctiontreated with thrombolytic vs conservative therapy. Chest. 1995;107:662–8.
9. Meyrier A. Cholesterol crystal embolism: diagnosis and treatment.Kidney Int. 2006;69:1308–12.
0. Hazanov N, Somin M, Attali M, et al. Acute renal embolism. Forty-fourcases of renal infarction in patients with atrial fibrillation. Medicine(Baltimore). 2004;83:292–9.
1. Lock G. Acute intestinal ischaemia. Best Pract Res Clin Gastroenterol.2001;15:83–98.
2. Wolf EL, Sprayregen S, Bakal CW. Radiology in intestinal ischemia.Plain film, contrast, and other imaging studies. Surg Clin North Am.1992;72:107–24.
3. Rhee RY, Gloviczki P. Mesenteric venous thrombosis. Surg Clin NorthAm. 1997;77:327–38.
4. Rahmouni A, Mathieu D, Golli M, et al. Value of CT and sonography inthe conservative management of acute splenoportal and superior mes-enteric venous thrombosis. Gastrointest Radiol. 1992;17:135–40.
5. Kirkpatrick ID, Kroeker MA, Greenberg HM. Biphasic CT withmesenteric CT angiography in the evaluation of acute mesentericischemia: initial experience. Radiology. 2003;229:91–8.
6. Grierson C, Uthappa MC, Uberoi R, et al. Multidetector CT appearancesof splanchnic arterial pathology. Clin Radiol. 2007;62:717–23.
7. Kramer H, Nikolaou K, Sommer W, et al. Peripheral MR angiography.Magn Reson Imaging Clin N Am. 2009;17:91–100.
8. Robinson BL, Nadolny EM, Entrup MH, et al. Management of right-sided aortic arch aneurysms. Ann Thorac Surg. 2001;72:1764–5.
9. Smith SC Jr., Allen J, Blair SN, et al. AHA/ACC guidelines forsecondary prevention for patients with coronary and other atheroscle-rotic vascular disease. J Am Coll Cardiol. 2006;47:2130–9.
0. Genoni M, Paul M, Jenni R, et al. Chronic beta-blocker therapyimproves outcome and reduces treatment costs in chronic type B aorticdissection. Eur J Cardiothorac Surg. 2001;19:606–10.
1. Ladouceur M, Fermanian C, Lupoglazoff JM, et al. Effect of beta-blockade on ascending aortic dilatation in children with the Marfansyndrome. Am J Cardiol. 2007;99:406–9.
2. Ahimastos AA, Aggarwal A, D’Orsa KM, et al. Effect of perindopril onlarge artery stiffness and aortic root diameter in patients with Marfansyndrome: a randomized controlled trial. JAMA. 2007;298:1539–47.
3. Mochizuki S, Dahlof B, Shimizu M, et al. Valsartan in a Japanesepopulation with hypertension and other cardiovascular disease (JikeiHeart Study): a randomised, open-label, blinded endpoint morbidity-mortality study. Lancet. 2007;369:1431–9.
4. Diehm N, Becker G, Katzen B, et al. Statins are associated withdecreased mortality in abdominal, but not in thoracic aortic aneurysmpatients undergoing endovascular repair: propensity score-adjusted anal-ysis. Vasa. 2008;37:241–9.
5. Major outcomes in high-risk hypertensive patients randomized toangiotensin-converting enzyme inhibitor or calcium channel blocker vsdiuretic: The Antihypertensive and Lipid-Lowering Treatment to Pre-vent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981–97.
6. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for theevaluation and management of chronic heart failure in the adult:
executive summary. J Am Coll Cardiol. 2001;38:2101–13.7. Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance ofusual blood pressure to vascular mortality: a meta-analysis of individualdata for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
8. Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calciumantagonists, and other blood-pressure-lowering drugs: results of pro-spectively designed overviews of randomised trials. Blood PressureLowering Treatment Trialists’ Collaboration. Lancet. 2000;356:1955–64.
9. Ogden LG, He J, Lydick E, et al. Long-term absolute benefit of loweringblood pressure in hypertensive patients according to the JNC VI riskstratification. Hypertension. 2000;35:539–43.
0. Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associatedwith antihypertensive therapies used as first-line agents. A systematicreview and meta-analysis. JAMA. 1997;277:739–45.
1. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the JointNational Committee on Prevention, Detection, Evaluation, and Treat-ment of High Blood Pressure. Hypertension. 2003;42:1206–52.
2. Evans J, Powell JT, Schwalbe E, et al. Simvastatin attenuates the activityof matrix metalloprotease-9 in aneurysmal aortic tissue. Eur J VascEndovasc Surg. 2007;34:302–3.
3. Leurs LJ, Visser P, Laheij RJ, et al. Statin use is associated with reducedall-cause mortality after endovascular abdominal aortic aneurysm repair.Vascular. 2006;14:1–8.
4. Kurzencwyg D, Filion KB, Pilote L, et al. Cardiac medical therapyamong patients undergoing abdominal aortic aneurysm repair. Ann VascSurg. 2006;20:569–76.
5. Yilmaz MB, Biyikoglu SF, Guray Y, et al. Level of awareness ofon-treatment patients about prescribed statins. Cardiovasc Drugs Ther.2004;18:399–404.
6. Executive Summary of The Third Report of The National CholesterolEducation Program (NCEP) Expert Panel on Detection, Evaluation, AndTreatment of High Blood Cholesterol In Adults (Adult Treatment PanelIII). JAMA. 2001;285:2486–97.
7. MRC/BHF Heart Protection Study of cholesterol lowering with simva-statin in 20,536 high-risk individuals: a randomised placebo-controlledtrial. Lancet. 2002;360:7–22.
8. Schouten O, van Laanen JH, Boersma E, et al. Statins are associatedwith a reduced infrarenal abdominal aortic aneurysm growth. Eur J VascEndovasc Surg. 2006;32:21–6.
9. Diehm N, Baumgartner I. ACE inhibitors and abdominal aortic aneu-rysm. Lancet. 2006;368:622–3.
0. Verma S, Lindsay TF. Regression of aortic aneurysms through pharma-cologic therapy? N Engl J Med. 2006;354:2067–8.
1. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guide-lines for the management of patients with unstable angina/non-ST-elevation myocardial infarction. J Am Coll Cardiol. 2007;50:e1–157.
2. Ockene IS, Miller NH. Cigarette smoking, cardiovascular disease, andstroke: a statement for healthcare professionals from the American HeartAssociation. American Heart Association Task Force on Risk Reduc-tion. Circulation. 1997;96:3243–7.
2a.Daly LE, Mulcahy R, Graham IM, Hickey N. Long term effect onmortality of stopping smoking after unstable angina and myocardialinfarction. Br Med J (Clin Res Ed). 1983;287:324–6.
2b.U.S. Department of Health and Human Services, Public Health ServiceAgency. Clinical Practice Guidelines: Number 18. Smoking Cessation1996; AHCPR Publication 96-0692.
3. Dapunt OE, Galla JD, Sadeghi AM, et al. The natural history of thoracicaortic aneurysms. J Thorac Cardiovasc Surg. 1994;107:1323–32.
4. Griepp RB, Ergin MA, Galla JD, et al. Natural history of descendingthoracic and thoracoabdominal aneurysms. Ann Thorac Surg. 1999;67:1927–30.
5. Jonason T, Bergstrom R. Cessation of smoking in patients withintermittent claudication. Effects on the risk of peripheral vascularcomplications, myocardial infarction and mortalityActa Med Scand.1987;221:253–60.
6. Kouchoukos NT, Dougenis D. Surgery of the thoracic aorta. N EnglJ Med. 1997;336:1876–88.
7. Elefteriades JA. Natural history of thoracic aortic aneurysms: indicationsfor surgery, and surgical versus nonsurgical risks. Ann Thorac Surg.2002;74:S1877–80.
8. Tzemos N, Therrien J, Yip J, et al. Outcomes in adults with bicuspid
aortic valves. JAMA. 2008;300:1317–25.
43
44
44
44
44
44
44
44
44
44
44
45
45
45
45
45
45
45
45
45
45
46
46
46
46
46
46
46
46
46
46
47
47
47
47
47
47
47
47
47
47
48
48
48
48
48
48
48
48
48
e118 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
9. Vallely MP, Semsarian C, Bannon PG. Management of the ascendingaorta in patients with bicuspid aortic valve disease. Heart Lung Circ.2008;17:357–63.
0. Coady MA, Rizzo JA, Hammond GL, et al. Surgical intervention criteriafor thoracic aortic aneurysms: a study of growth rates and complications.Ann Thorac Surg. 1999;67:1922–6.
1. Kouchoukos NT. Composite graft replacement of the ascending aortaand aortic valve with the inclusion-wrap and open techniques. SeminThorac Cardiovasc Surg. 1991;3:171–6.
2. Abedin M, Tintut Y, Demer LL. Vascular calcification: mechanisms andclinical ramifications. Arterioscler Thromb Vasc Biol. 2004;24:1161–70.
3. Iribarren C, Sidney S, Sternfeld B, et al. Calcification of the aortic arch:risk factors and association with coronary heart disease, stroke, andperipheral vascular disease. JAMA. 2000;283:2810–5.
4. Chiu KM, Lin TY, Chen JS, et al. Images in cardiovascular medicine.Left ventricle apical conduit to bilateral subclavian artery in a patientwith porcelain aorta and aortic stenosis. Circulation. 2006;113:e388–9.
5. Robicsek F, Cook JW, Reames MK, Sret al. Size reduction ascendingaortoplasty: is it dead or alive? J Thorac Cardiovasc Surg. 2004;128:562–70.
6. Sievers HH. Reflections on reduction ascending aortoplasty’s liveliness.J Thorac Cardiovasc Surg. 2004;128:499–501.
7. Miller DC. Valve-sparing aortic root replacement: current state of the artand where are we headed? Ann Thorac Surg. 2007;83:S736–9.
8. Svensson LG, Longoria J, Kimmel WA, et al. Management of aorticvalve disease during aortic surgery. Ann Thorac Surg. 2000;69:778–83.
9. Svensson LG, Blackstone EH, Rajeswaran J, et al. Does the arterialcannulation site for circulatory arrest influence stroke risk? Ann ThoracSurg. 2004;78:1274–84.
0. Svensson LG, Crawford ES, Hess KR, et al. Dissection of the aorta anddissecting aortic aneurysms. Improving early and long-term surgicalresults. Circulation. 1990;82:IV24–38.
1. Greenberg RK, Haddad F, Svensson L, et al. Hybrid approaches tothoracic aortic aneurysms: the role of endovascular elephant trunkcompletion. Circulation. 2005;112:2619–26.
2. Svensson LG. The elephant trunk procedure: uses in complex aorticdiseases. Curr Opin Cardiol. 2005;20:491–5.
3. Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure:newer indications and uses. Ann Thorac Surg. 2004;78:109–16.
4. Kazui T, Washiyama N, Muhammad BA, et al. Total arch replacementusing aortic arch branched grafts with the aid of antegrade selectivecerebral perfusion. Ann Thorac Surg. 2000;70:3–8.
5. Kazui T, Washiyama N, Muhammad BA, et al. Improved results ofatherosclerotic arch aneurysm operations with a refined technique.J Thorac Cardiovasc Surg. 2001;121:491–9.
6. Kouchoukos NT, Mauney MC, Masetti P, et al. Single-stage repair ofextensive thoracic aortic aneurysms: experience with the arch-firsttechnique and bilateral anterior thoracotomy. J Thorac Cardiovasc Surg.2004;128:669–76.
7. Lemaire SA, Carter SA, Coselli JS. The elephant trunk technique forstaged repair of complex aneurysms of the entire thoracic aorta. AnnThorac Surg. 2006;81:1561–9.
8. Safi HJ, Miller CC III, Estrera AL, et al. Staged repair of extensive aorticaneurysms: long-term experience with the elephant trunk technique. AnnSurg. 2004;240:677–84.
9. Strauch JT, Spielvogel D, Lauten A, et al. Technical advances in totalaortic arch replacement. Ann Thorac Surg. 2004;77:581–9.
0. Czerny M, Gottardi R, Zimpfer D, et al. Transposition of the supraaorticbranches for extended endovascular arch repair. Eur J CardiothoracSurg. 2006;29:709–13.
1. Bergeron P, Mangialardi N, Costa P, et al. Great vessel management forendovascular exclusion of aortic arch aneurysms and dissections. Eur JVasc Endovasc Surg. 2006;32:38–45.
2. Griepp RB. Cerebral protection during aortic arch surgery. J ThoracCardiovasc Surg. 2001;121:425–7.
3. Lin R, Svensson L, Gupta R, et al. Chronic ischemic cerebral whitematter disease is a risk factor for nonfocal neurologic injury after totalaortic arch replacement. J Thorac Cardiovasc Surg. 2007;133:1059–65.
4. Hirose H, Svensson LG, Lytle BW, et al. Aortic dissection after previouscardiovascular surgery. Ann Thorac Surg. 2004;78:2099–105.
5. Svensson LG. Progress in ascending and aortic arch surgery: minimallyinvasive surgery, blood conservation, and neurological deficit preven-
tion. Ann Thorac Surg. 2002;74:S1786–8.6. Svensson LG, Nadolny EM, Penney DL, et al. Prospective randomizedneurocognitive and S-100 study of hypothermic circulatory arrest,retrograde brain perfusion, and antegrade brain perfusion for aortic archoperations. Ann Thorac Surg. 2001;71:1905–12.
7. Safi HJ, Brien HW, Winter JN, et al. Brain protection via cerebralretrograde perfusion during aortic arch aneurysm repair. Ann ThoracSurg. 1993;56:270–6.
8. Estrera AL, Rubenstein FS, Miller CC III, et al. Descending thoracicaortic aneurysm: surgical approach and treatment using the adjunctscerebrospinal fluid drainage and distal aortic perfusion. Ann ThoracSurg. 2001;72:481–6.
9. Matsumura JS, Cambria RP, Dake MD, et al. International controlledclinical trial of thoracic endovascular aneurysm repair with the ZenithTX2 endovascular graft: 1-year results. J Vasc Surg. 2008;47:247–57.
0. Svensson LG, Crawford ES, Hess KR, et al. Thoracoabdominal aorticaneurysms associated with celiac, superior mesenteric, and renal arteryocclusive disease: methods and analysis of results in 271 patients. J VascSurg. 1992;16:378–89.
1. Demers P, Miller DC, Mitchell RS, et al. Midterm results of endovas-cular repair of descending thoracic aortic aneurysms with first-generation stent grafts. J Thorac Cardiovasc Surg. 2004;127:664–73.
2. Aljabri B, Al WK, Abner D, et al. Patient-reported quality of life afterabdominal aortic aneurysm surgery: a prospective comparison of endo-vascular and open repair. J Vasc Surg. 2006;44:1182–7.
3. Kalef-Ezra JA, Karavasilis S, Ziogas D, et al. Radiation burden ofpatients undergoing endovascular abdominal aortic aneurysm repair. JVasc Surg. 2009;49:283–7.
4. Gutsche JT, Cheung AT, McGarvey ML, et al. Risk factors forperioperative stroke after thoracic endovascular aortic repair. AnnThorac Surg. 2007;84:1195–200.
5. Peterson BG, Eskandari MK, Gleason TG, et al. Utility of left subcla-vian artery revascularization in association with endoluminal repair ofacute and chronic thoracic aortic pathology. J Vasc Surg. 2006;43:433–9.
6. Rehders TC, Petzsch M, Ince H, et al. Intentional occlusion of the leftsubclavian artery during stent-graft implantation in the thoracic aorta:risk and relevance. J Endovasc Ther. 2004;11:659–66.
7. Riesenman PJ, Farber MA, Mendes RR, et al. Coverage of the leftsubclavian artery during thoracic endovascular aortic repair. J VascSurg. 2007;45:90–4.
8. Jackson BM, Carpenter JP, Fairman RM, et al. Anatomic exclusion fromendovascular repair of thoracic aortic aneurysm. J Vasc Surg. 2007;45:662–6.
9. Reece TB, Gazoni LM, Cherry KJ, et al. Reevaluating the need for leftsubclavian artery revascularization with thoracic endovascular aorticrepair. Ann Thorac Surg. 2007;84:1201–5.
0. Song TK, Donayre CE, Walot I, et al. Endograft exclusion of acute andchronic descending thoracic aortic dissections. J Vasc Surg. 2006;43:247–58.
1. Buth J, Harris PL, Hobo R, et al. Neurologic complications associatedwith endovascular repair of thoracic aortic pathology: Incidence and riskfactors. a study from the European Collaborators on Stent/Graft Tech-niques for Aortic Aneurysm Repair (EUROSTAR) registry. J Vasc Surg.2007;46:1103–10.
2. Fairman RM, Criado F, Farber M, et al. Pivotal results of the MedtronicVascular Talent Thoracic Stent Graft System: the VALOR trial. J VascSurg. 2008;48:546–54.
3. Schurink GW, Nijenhuis RJ, Backes WH, et al. Assessment of spinalcord circulation and function in endovascular treatment of thoracicaortic aneurysms. Ann Thorac Surg. 2007;83:S877–81.
4. Khoynezhad A, Donayre CE, Bui H, et al. Risk factors of neurologicdeficit after thoracic aortic endografting. Ann Thorac Surg. 2007;83:S882–S889.
5. Gravereaux EC, Faries PL, Burks JA, et al. Risk of spinal cord ischemiaafter endograft repair of thoracic aortic aneurysms. J Vasc Surg.2001;34:997–1003.
6. Cheung AT, Pochettino A, McGarvey ML, et al. Strategies to manageparaplegia risk after endovascular stent repair of descending thoracicaortic aneurysms. Ann Thorac Surg. 2005;80:1280–8.
7. Resch TA, Greenberg RK, Lyden SP, et al. Combined staged proceduresfor the treatment of thoracoabdominal aneurysms. J Endovasc Ther.2006;13:481–9.
8. Roselli EE, Greenberg RK, Pfaff K, et al. Endovascular treatment ofthoracoabdominal aortic aneurysms. J Thorac Cardiovasc Surg. 2007;
133:1474–82.
48
49
49
49
49
49
49
49
49
49
49
50
50
50
50
50
50
50
50
50
50
51
51
51
51
51
51
51
51
51
51
52
52
52
52
52
52
52
52
52
52
53
53
53
53
53
53
53
53
53
e119JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
9. Flye MW, Choi ET, Sanchez LA, et al. Retrograde visceral vesselrevascularization followed by endovascular aneurysm exclusion as analternative to open surgical repair of thoracoabdominal aortic aneurysm.J Vasc Surg. 2004;39:454–8.
0. Barnes DM, Williams DM, Dasika NL, et al. A single-center experiencetreating renal malperfusion after aortic dissection with central aorticfenestration and renal artery stenting. J Vasc Surg. 2008;47:903–10.
1. Gorich J, Kramer S, Tomczak R, et al. Thromboembolic complicationsafter endovascular aortic aneurysm repair. J Endovasc Ther. 2002;9:180–4.
2. Patel HJ, Williams DM, Upchurch GR Jr., et al. Long-term results froma 12-year experience with endovascular therapy for thoracic aorticdisease. Ann Thorac Surg. 2006;82:2147–53.
3. W.L. Gore & Associates I. Gore TAG thoracic endoprosthesis annualclinical update. Available at: http://www.resolutadapt.com/en/file/AK0314.pdf. Accessed January 7, 2010
4. Stavropoulos SW, Carpenter JP, Van den Brande P. Postoperativeimaging surveillance and endoleak management after endovascularrepair of thoracic aortic aneurysms. J Vasc Surg. 2006;43 SupplA:89A–93A.
5. Mita T, Arita T, Matsunaga N, et al. Complications of endovascularrepair for thoracic and abdominal aortic aneurysm: an imaging spectrum.Radiographics. 2000;20:1263–78.
6. Won JY, Suh SH, Ko HK, et al. Problems encountered during and afterstent-graft treatment of aortic dissection. J Vasc Interv Radiol. 2006;17:271–81.
7. Zhang R, Kofidis T, Baus S, et al. Iatrogenic type A dissection afterattempted stenting of a descending aortic aneurysm. Ann Thorac Surg.2006;82:1523–5.
8. Bethuyne N, Bove T, Van den BP, et al. Acute retrograde aorticdissection during endovascular repair of a thoracic aortic aneurysm. AnnThorac Surg. 2003;75:1967–9.
9. Nienaber CA, Kische S, Ince H. Thoracic aortic stent-graft devices:problems, failure modes, and applicability. Semin Vasc Surg. 2007;20:81–9.
0. Steinbauer MG, Stehr A, Pfister K, et al. Endovascular repair ofproximal endograft collapse after treatment for thoracic aortic disease. JVasc Surg. 2006;43:609–12.
1. Idu MM, Reekers JA, Balm R, et al. Collapse of a stent-graft followingtreatment of a traumatic thoracic aortic rupture. J Endovasc Ther.2005;12:503–7.
2. Parmer SS, Carpenter JP, Stavropoulos SW, et al. Endoleaks afterendovascular repair of thoracic aortic aneurysms. J Vasc Surg. 2006;44:447–52.
3. Hartung O, Alimi YS, Juhan C. Tinnitus resulting from tandem lesionsof the internal carotid artery: combined extracranial endarterectomy andintrapetrous primary stenting. J Vasc Surg. 2004;39:679–81.
4. Leurs LJ, Bell R, Degrieck Y, et al. Endovascular treatment of thoracicaortic diseases: combined experience from the EUROSTAR and UnitedKingdom Thoracic Endograft registries. J Vasc Surg. 2004;40:670–9.
5. Preventza O, Wheatley, GH IIIRamaiah VG, et al. Management ofendoleaks associated with endovascular treatment of descending tho-racic aortic diseases. J Vasc Surg. 2008;48:69–73.
6. Leon LR Jr., Rodriguez HE. Aortic endograft migration. Perspect VascSurg Endovasc Ther. 2005;17:363–73.
7. Panos A. Late retrograde aortic perforation by the uncovered part of anendograft: an increasing complication. Hellenic J Cardiol. 2007;48:115–6.
8. Malina M, Brunkwall J, Ivancev K, et al. Late aortic arch perforation bygraft-anchoring stent: complication of endovascular thoracic aneurysmexclusion. J Endovasc Surg. 1998;5:274–7.
9. Fattori R, Nienaber CA, Rousseau H, et al. Results of endovascularrepair of the thoracic aorta with the Talent Thoracic stent graft: theTalent Thoracic Retrospective Registry. J Thorac Cardiovasc Surg.2006;132:332–9.
0. Makaroun MS, Dillavou ED, Kee ST, et al. Endovascular treatment ofthoracic aortic aneurysms: results of the phase II multicenter trial of theGORE TAG thoracic endoprosthesis. J Vasc Surg. 2005;41:1–9.
1. Jacobs TS, Won J, Gravereaux EC, et al. Mechanical failure ofprosthetic human implants: a 10-year experience with aortic stent graftdevices. J Vasc Surg. 2003;37:16–26.
2. Bockler D, von Tengg-Kobligk H, Schumacher H, et al. Late surgicalconversion after thoracic endograft failure due to fracture of the
longitudinal support wire. J Endovasc Ther. 2005;12:98–102.3. Silberfein EJ, Lin PH, Bush RL, et al. Aortic endograft infection due toPasteurella multocida following a rabbit bite. J Vasc Surg. 2006;43:393–5.
4. Wheatley GH III, Gurbuz AT, Rodriguez-Lopez JA, et al. Midtermoutcome in 158 consecutive Gore TAG thoracic endoprostheses: singlecenter experience. Ann Thorac Surg. 2006;81:1570–7.
5. Parra JR, Lee C, Hodgson KJ, et al. Endograft infection leading torupture of aortic aneurysm. J Vasc Surg. 2004;39:676–8.
6. Eggebrecht H, Nienaber CA, Neuhauser M, et al. Endovascular stent-graft placement in aortic dissection: a meta-analysis. Eur Heart J.2006;27:489–98.
7. Bockler D, Schumacher H, Ganten M, et al. Complications afterendovascular repair of acute symptomatic and chronic expanding Stan-ford type B aortic dissections. J Thorac Cardiovasc Surg. 2006;132:361–8.
8. Endovascular aneurysm repair versus open repair in patients withabdominal aortic aneurysm (EVAR trial 1): randomised controlled trial.Lancet. 2005;365:2179–86.
9. Blankensteijn JD, de Jong SE, Prinssen M, et al. Two-year outcomesafter conventional or endovascular repair of abdominal aortic aneu-rysms. N Engl J Med. 2005;352:2398–405.
0. Cambria RP, Davison JK, Carter C, et al. Epidural cooling for spinalcord protection during thoracoabdominal aneurysm repair: a five-yearexperience. J Vasc Surg. 2000;31:1093–102.
1. Coselli JS, Conklin LD, Lemaire SA. Thoracoabdominal aortic aneu-rysm repair: review and update of current strategies. Ann Thorac Surg.2002;74:S1881–4.
2. Coselli JS, Lemaire SA, Koksoy C, et al. Cerebrospinal fluid drainagereduces paraplegia after thoracoabdominal aortic aneurysm repair:results of a randomized clinical trial. J Vasc Surg. 2002;35:631–9.
3. Safi HJ, Miller CC III, Huynh TT, et al. Distal aortic perfusion andcerebrospinal fluid drainage for thoracoabdominal and descending tho-racic aortic repair: ten years of organ protection. Ann Surg. 2003;238:372–80.
4. Svensson LG, Crawford ES, Patel V, et al. Spinal oxygenation, bloodsupply localization, cooling, and function with aortic clamping. AnnThorac Surg. 1992;54:74–9.
5. Svensson LG, Khitin L, Nadolny EM, et al. Systemic temperature andparalysis after thoracoabdominal and descending aortic operations. ArchSurg. 2003;138:175–9.
6. Svensson LG. Paralysis after aortic surgery: in search of lost cordfunction. Surgeon. 2005;3:396–405.
7. Martens S, Neumann K, Sodemann C, et al. Carbon dioxide fieldflooding reduces neurologic impairment after open heart surgery. AnnThorac Surg. 2008;85:543–7.
8. Nadolny EM, Svensson LG. Carbon dioxide field flooding techniquesfor open heart surgery: monitoring and minimizing potential adverseeffects. Perfusion. 2000;15:151–3.
9. Miller DC, Mitchell RS, Oyer PE, et al. Independent determinants ofoperative mortality for patients with aortic dissections. Circulation.1984;70:I153–64.
0. Lauterbach SR, Cambria RP, Brewster DC, et al. Contemporary man-agement of aortic branch compromise resulting from acute aorticdissection. J Vasc Surg. 2001;33:1185–92.
1. Girardi LN, Krieger KH, Lee LY, et al. Management strategies for typeA dissection complicated by peripheral vascular malperfusion. AnnThorac Surg. 2004;77:1309–14.
2. Deeb GM, Williams DM, Bolling SF, et al. Surgical delay for acute typeA dissection with malperfusion. Ann Thorac Surg. 1997;64:1669–75.
3. Hsu RB, Ho YL, Chen RJ, et al. Outcome of medical and surgicaltreatment in patients with acute type B aortic dissection. Ann ThoracSurg. 2005;79:790–4.
4. Pacini L, Digne F, Boumendil A, et al. Maternal complication ofpregnancy in Marfan syndrome. Int J Cardiol. 2009;136:156–61.
5. Strickland RA, Oliver WC Jr., Chantigian RC, et al. Anesthesia,cardiopulmonary bypass, and the pregnant patient. Mayo Clin Proc.1991;66:411–29.
6. Williams GM, Gott VL, Brawley RK, et al. Aortic disease associatedwith pregnancy. J Vasc Surg. 1988;8:470–5.
7. Immer FF, Bansi AG, Immer-Bansi AS, et al. Aortic dissection inpregnancy: analysis of risk factors and outcome. Ann Thorac Surg.2003;76:309–14.
8. Lind J, Wallenburg HC. The Marfan syndrome and pregnancy: aretrospective study in a Dutch population. Eur J Obstet Gynecol Reprod
Biol. 2001;98:28–35.
53
54
54
54
54
54
54
54
54
54
54
55
55
55
55
55
55
55
55
55
55
56
56
56
5656
56
56
56
56
56
57
57
57
57
57
57
57
57
57
57
58
58
58
58
5858
58
58
58
58
e120 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
9. Erbel R, Alfonso F, Boileau C, et al. Diagnosis and management ofaortic dissection. Eur Heart J. 2001;22:1642–81.
0. Tunick PA, Nayar AC, Goodkin GM, et al. Effect of treatment on theincidence of stroke and other emboli in 519 patients with severe thoracicaortic plaque. Am J Cardiol. 2002;90:1320–5.
1. Amarenco P, Duyckaerts C, Tzourio C, et al. The prevalence ofulcerated plaques in the aortic arch in patients with stroke. N EnglJ Med. 1992;326:221–5.
2. Khatibzadeh M, Mitusch R, Stierle U, et al. Aortic atheroscleroticplaques as a source of systemic embolism. J Am Coll Cardiol. 1996;27:664–9.
3. Amarenco P, Cohen A, Tzourio C, et al. Atherosclerotic disease of theaortic arch and the risk of ischemic stroke. N Engl J Med. 1994;331:1474–9.
4. Jones EF, Kalman JM, Calafiore P, et al. Proximal aortic atheroma. Anindependent risk factor for cerebral ischemia. Stroke. 1995;26:218–24.
5. Stern A, Tunick PA, Culliford AT, et al. Protruding aortic archatheromas: risk of stroke during heart surgery with and without aorticarch endarterectomy. Am Heart J. 1999;138:746–52.
6. Nihoyannopoulos P, Joshi J, Athanasopoulos G, et al. Detection ofatherosclerotic lesions in the aorta by transesophageal echocardiogra-phy. Am J Cardiol. 1993;71:1208–12.
7. Stone DH, Brewster DC, Kwolek CJ, et al. Stent-graft versus open-surgical repair of the thoracic aorta: mid-term results. J Vasc Surg.2006;44:1188–97.
8. Di Tullio MR, Sacco RL, Gersony D, et al. Aortic atheromas and acuteischemic stroke: a transesophageal echocardiographic study in anethnically mixed population. Neurology. 1996;46:1560–6.
9. Davila-Roman VG, Barzilai B, Wareing TH, et al. Atherosclerosis of theascending aorta. Prevalence and role as an independent predictor ofcerebrovascular events in cardiac patients. Stroke. 1994;25:2010–6.
0. The French Study of Aortic Plaques in Stroke Group. Atheroscleroticdisease of the aortic arch as a risk factor for recurrent ischemic stroke.N Engl J Med. 1996;334:1216–21.
1. Tunick PA, Rosenzweig BP, Katz ES, et al. High risk for vascular eventsin patients with protruding aortic atheromas: a prospective study. J AmColl Cardiol. 1994;23:1085–90.
2. Mitusch R, Doherty C, Wucherpfennig H, et al. Vascular events duringfollow-up in patients with aortic arch atherosclerosis. Stroke. 1997;28:36–9.
3. Davila-Roman VG, Murphy SF, Nickerson NJ, et al. Atherosclerosis ofthe ascending aorta is an independent predictor of long-term neurologicevents and mortality. J Am Coll Cardiol. 1999;33:1308–16.
4. Cohen A, Tzourio C, Bertrand B, et al. Aortic plaque morphology andvascular events: a follow-up study in patients with ischemic stroke.FAPS Investigators French Study of Aortic Plaques in Stroke. Circula-tion. 1997;96:3838–41.
5. Sen S, Oppenheimer SM, Lima J, et al. Risk factors for progression ofaortic atheroma in stroke and transient ischemic attack patients. Stroke.2002;33:930–5.
6. Montgomery DH, Ververis JJ, McGorisk G, et al. Natural history ofsevere atheromatous disease of the thoracic aorta: a transesophagealechocardiographic study. J Am Coll Cardiol. 1996;27:95–101.
7. Pitsavos CE, Aggeli KI, Barbetseas JD, et al. Effects of pravastatin onthoracic aortic atherosclerosis in patients with heterozygous familialhypercholesterolemia. Am J Cardiol. 1998;82:1484–8.
8. Geraci A, Weinberger J. Natural history of aortic arch atheroscleroticplaque. Neurology. 2000;54:749–51.
9. Sen S, Hinderliter A, Sen PK, et al. Aortic arch atheroma progressionand recurrent vascular events in patients with stroke or transientischemic attack. Circulation. 2007;116:928–35.
0. Agmon Y, Khandheria BK, Meissner I, et al. Independent association ofhigh blood pressure and aortic atherosclerosis: a population-based study.Circulation. 2000;102:2087–93.
1. Tsimikas S, Brilakis ES, Miller ER, et al. Oxidized phospholipids, Lp(a)lipoprotein, and coronary artery disease. N Engl J Med. 2005;353:46–57.
2. The Stroke Prevention in Atrial Fibrillation Investigators Committee onEchocardiography. Transesophageal echocardiographic correlates ofthromboembolism in high-risk patients with nonvalvular atrial fibrilla-tion. Ann Intern Med. 1998;128:639–47.
3. Deleted in proof.4. Agmon Y, Khandheria BK, Meissner I, et al. C-reactive protein and
atherosclerosis of the thoracic aorta: a population-based transesophageal
echocardiographic study. Arch Intern Med. 2004;164:1781–7.5. Konecky N, Malinow MR, Tunick PA, et al. Correlation betweenplasma homocyst(e)ine and aortic atherosclerosis. Am Heart J. 1997;133:534–40.
6. Kronzon I, Tunick PA. Aortic atherosclerotic disease and stroke.Circulation. 2006;114:63–75.
7. Zaidat OO, Suarez JI, Hedrick D, et al. Reproducibility of transesoph-ageal echocardiography in evaluating aortic atheroma in stroke patients.Echocardiography. 2005;22:326–30.
8. Tenenbaum A, Garniek A, Shemesh J, et al. Dual-helical CT fordetecting aortic atheromas as a source of stroke: comparison withtransesophageal echocardiography. Radiology. 1998;208:153–8.
9. Blanchard DG, Kimura BJ, Dittrich HC, et al. Transesophageal echo-cardiography of the aorta. JAMA. 1994;272:546–51.
0. Weinberger J, Azhar S, Danisi F, et al. A new noninvasive technique forimaging atherosclerotic plaque in the aortic arch of stroke patients bytranscutaneous real-time B-mode ultrasonography: an initial report.Stroke. 1998;29:673–6.
1. Schwammenthal E, Schwammenthal Y, Tanne D, et al. Transcutaneousdetection of aortic arch atheromas by suprasternal harmonic imaging.J Am Coll Cardiol. 2002;39:1127–32.
2. Gottsegen JM, Coplan NL. The atherosclerotic aortic arch: consider-ations in diagnostic imaging. Prev Cardiol. 2008;11:162–7.
3. Wareing TH, Davila-Roman VG, Barzilai B, et al. Management of theseverely atherosclerotic ascending aorta during cardiac operations. Astrategy for detection and treatment. J Thorac Cardiovasc Surg. 1992;103:453–62.
4. Khatri IA, Mian N, Alkawi A, et al. Catheter-based aortography fails toidentify aortic atherosclerotic lesions detected on transesophageal echo-cardiography. J Neuroimaging. 2005;15:261–5.
5. Corti R. Noninvasive imaging of atherosclerotic vessels by MRI forclinical assessment of the effectiveness of therapy. Pharmacol Ther.2006;110:57–70.
6. Kronzon I. Protruding aortic atheroma: is there a need for a new imagingmodality? Isr Med Assoc J. 2000;2:54–5.
7. Tahara N, Kai H, Ishibashi M, et al. Simvastatin attenuates plaqueinflammation: evaluation by fluorodeoxyglucose positron emission to-mography. J Am Coll Cardiol. 2006;48:1825–31.
8. Hausmann D, Gulba D, Bargheer K, et al. Successful thrombolysis of anaortic-arch thrombus in a patient after mesenteric embolism. N EnglJ Med. 1992;327:500–1.
9. Dahlberg PJ, Frecentese DF, Cogbill TH. Cholesterol embolism: expe-rience with 22 histologically proven cases. Surgery. 1989;105:737–46.
0. Bruns FJ, Segel DP, Adler S. Control of cholesterol embolization bydiscontinuation of anticoagulant therapy. Am J Med Sci. 1978;275:105–8.
1. Hyman BT, Landas SK, Ashman RF, et al. Warfarin-related purple toessyndrome and cholesterol microembolization. Am J Med. 1987;82:1233–7.
2. Blackshear JL, Jahangir A, Oldenburg WA, et al. Digital embolizationfrom plaque-related thrombus in the thoracic aorta: identification withtransesophageal echocardiography and resolution with warfarin therapy.Mayo Clin Proc. 1993;68:268–72.
3. Koppang JR, Nanda NC, Coghlan HC, et al. Histologically ConfirmedCholesterol Atheroemboli with Identification of the Source by Trans-esophageal Echocardiography. Echocardiography. 1992;9:379–83.
4. Deleted in proof5. Tunick PA, Culliford AT, Lamparello PJ, et al. Atheromatosis of the
aortic arch as an occult source of multiple systemic emboli. Ann InternMed. 1991;114:391–2.
6. Ferrari E, Vidal R, Chevallier T, et al. Atherosclerosis of the thoracicaorta and aortic debris as a marker of poor prognosis: benefit of oralanticoagulants. J Am Coll Cardiol. 1999;33:1317–22.
7. Corti R, Fuster V, Fayad ZA, et al. Effects of aggressive versusconventional lipid-lowering therapy by simvastatin on human athero-sclerotic lesions: a prospective, randomized, double-blind trial withhigh-resolution magnetic resonance imaging. J Am Coll Cardiol. 2005;46:106–12.
8. Yonemura A, Momiyama Y, Fayad ZA, et al. Effect of lipid-loweringtherapy with atorvastatin on atherosclerotic aortic plaques detected bynoninvasive magnetic resonance imaging. J Am Coll Cardiol. 2005;45:733–42.
9. Goldstein LB, Adams R, Alberts MJ, et al. Primary prevention ofischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the
Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working
59
59
59
59
59
59
59
59
59
59
60
60
60
60
60
60
60
60
60
60
61
61
61
61
61
61
61
61
61
61
62
62
62
62
62
62
62
62
62
62
63
63
63
63
63
63
e121JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
Group; Cardiovascular Nursing Council; Clinical Cardiology Council;Nutrition, Physical Activity, and Metabolism Council; and the Qualityof Care and Outcomes Research Interdisciplinary Working Group.Circulation. 2006;113:e873–923.
0. Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of strokein patients with ischemic stroke or transient ischemic attack: a statementfor healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by theCouncil on Cardiovascular Radiology and Intervention: the AmericanAcademy of Neurology affirms the value of this guideline. Stroke.2006;37:577–617.
1. Bar-El Y, Goor DA. Clamping of the atherosclerotic ascending aortaduring coronary artery bypass operations. Its cost in strokes. J ThoracCardiovasc Surg. 1992;104:469–74.
2. Cosgrove DM. Management of the calcified aorta: an alternative methodof occlusion. Ann Thorac Surg. 1983;36:718–9.
3. Grossi EA, Kanchuger MS, Schwartz DS, et al. Effect of cannula lengthon aortic arch flow: protection of the atheromatous aortic arch. AnnThorac Surg. 1995;59:710–2.
4. Mills NL, Everson CT. Atherosclerosis of the ascending aorta andcoronary artery bypass. Pathology, clinical correlates, and operativemanagement. J Thorac Cardiovasc Surg. 1991;102:546–53.
5. Peigh PS, DiSesa VJ, Collins JJ, Jr., et al. Coronary bypass grafting withtotally calcified or acutely dissected ascending aorta. Ann Thorac Surg.1991;51:102–4.
6. Rokkas CK, Kouchoukos NT. Surgical management of the severelyatherosclerotic ascending aorta during cardiac operations. Semin ThoracCardiovasc Surg. 1998;10:240–6.
7. Wimmer-Greinecker G. Reduction of neurologic complications byintra-aortic filtration in patients undergoing combined intracardiac andCABG procedures. Eur J Cardiothorac Surg. 2003;23:159–64.
8. Girardi LN, Krieger KH, Mack CA, et al. No-clamp technique for valverepair or replacement in patients with a porcelain aorta. Ann ThoracSurg. 2005;80:1688–92.
9. Aranki SF, Nathan M, Shekar P, et al. Hypothermic circulatory arrestenables aortic valve replacement in patients with unclampable aorta.Ann Thorac Surg. 2005;80:1679–86.
0. Deslauriers J, Gregoire J. Clinical and surgical staging of non-small celllung cancer. Chest. 2000;117:96S–103S.
1. Kameda K, Adachi S, Kono M. Detection of T-factor in lung cancerusing magnetic resonance imaging and computed tomography. J ThoracImaging. 1988;3:73–80.
2. Ohtsuka T, Minami M, Nakajima J, et al. Cine computed tomographyfor evaluation of tumors invasive to the thoracic aorta: seven clinicalexperiences. J Thorac Cardiovasc Surg. 1996;112:190–2.
3. Schroder C, Schonhofer B, Vogel B. Transesophageal echographicdetermination of aortic invasion by lung cancer. Chest. 2005;127:438–42.
4. Oldenburg WA. Primary Tumors of Major Blood Vessels. 6th ed.Philadelphia, PA: Elsevier Saunders, 2005.
5. Chen WJ, Chen CL, Liau CS, et al. Primary malignant fibrous histio-cytoma of the aorta associated with aortic dissection. Chest. 1991;99:1049–50.
6. Utsunomiya D, Ikeda O, Ideta I, et al. Malignant fibrous histiocytomaarising from the aortic wall mimicking a pseudoaneurysm with ulcer-ation. Circ J. 2007;71:1659–61.
7. Guttentag A, Lazar HL, Franklin P, et al. Malignant fibrous histiocytomaobstructing the thoracic aorta. Ann Thorac Surg. 1989;47:775–7.
8. Kouchoukos NT, Masetti P. Primary sarcoma of the thoracic aorta. AnnThorac Surg. 2007;83:e1.
9. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy withor without PCI for stable coronary disease. N Engl J Med. 2007;356:1503–16.
0. McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascular-ization before elective major vascular surgery. N Engl J Med. 2004;351:2795–804.
1. Poldermans D, Schouten O, Vidakovic R, et al. A clinical randomizedtrial to evaluate the safety of a noninvasive approach in high-riskpatients undergoing major vascular surgery: the DECREASE-V PilotStudy. J Am Coll Cardiol. 2007;49:1763–9.
2. Heng AE, Cellarier E, ublet-Cuvelier B, et al. Is treatment withN-acetylcysteine to prevent contrast-induced nephropathy when using
bicarbonate hydration out of date? Clin Nephrol. 2008;70:475–84.3. Nigwekar SU, Kandula P. N-Acetylcysteine in cardiovascular-surgery-associated renal failure: a meta-analysis. Ann Thorac Surg. 2009;87:139–47.
4. Juvonen T, Ergin MA, Galla JD, et al. Prospective study of the naturalhistory of thoracic aortic aneurysms. Ann Thorac Surg. 1997;63:1533–45.
5. Svensson LG, Crawford ES, Hess KR, et al. Deep hypothermia withcirculatory arrest. Determinants of stroke and early mortality in 656patients J Thorac Cardiovasc Surg. 1993;106:19–28.
6. Cain HD, Stevens PM, Adaniya R. Preoperative pulmonary function andcomplications after cardiovascular surgery. Chest. 1979;76:130–5.
7. Safi HJ, Harlin SA, Miller CC, et al. Predictive factors for acute renalfailure in thoracic and thoracoabdominal aortic aneurysm surgery. JVasc Surg. 1996;24:338–44.
8. Eagle KA, Rihal CS, Mickel MC, et al. Cardiac risk of noncardiacsurgery. CASS Investigators and University of Michigan Heart CarePrograminfluence of coronary disease and type of surgery in 3368operations. Coronary Artery Surgery Study. Circulation. 1997;96:1882–7.
9. Hertzer NR, Beven EG, Young JR, et al. Coronary artery disease inperipheral vascular patients. A classification of 1000 coronary angio-grams and results of surgical management. Ann Surg. 1984;199:223–33.
0. Hertzer NR, Young JR, Beven EG, et al. Late results of coronary bypassin patients with peripheral vascular disease. I. Five-year survivalaccording to age and clinical cardiac status. Cleve Clin Q. 1986;53:133–43.
1. Hertzer NR, Young JR, Beven EG, et al. Late results of coronary bypassin patients with peripheral vascular disease. II. Five-year survivalaccording to sex, hypertension, and diabetes. Cleve Clin J Med.1987;54:15–23.
2. Rihal CS, Eagle KA, Mickel MC, et al. Surgical therapy for coronaryartery disease among patients with combined coronary artery andperipheral vascular disease. Circulation. 1995;91:46–53.
3. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guidelineupdate on perioperative cardiovascular evaluation for noncardiac sur-gery. Circulation. 2006;113:2662–74.
4. Svensson LG, Hess KR, Coselli JS, et al. A prospective study ofrespiratory failure after high-risk surgery on the thoracoabdominal aorta.J Vasc Surg. 1991;14:271–82.
5. Kashyap VS, Cambria RP, Davison JK, et al. Renal failure afterthoracoabdominal aortic surgery. J Vasc Surg. 1997;26:949–55.
6. Svensson LG, Coselli JS, Safi HJ, et al. Appraisal of adjuncts to preventacute renal failure after surgery on the thoracic or thoracoabdominalaorta. J Vasc Surg. 1989;10:230–9.
7. Berens ES, Kouchoukos NT, Murphy SF, et al. Preoperative carotidartery screening in elderly patients undergoing cardiac surgery. J VascSurg. 1992;15:313–21.
8. Crawford ES, Svensson LG, Coselli JS, et al. Surgical treatment ofaneurysm and/or dissection of the ascending aorta, transverse aorticarch, and ascending aorta and transverse aortic arch. Factors influencingsurvival in 717 patients. J Thorac Cardiovasc Surg. 1989;98:659–73.
9. Coselli JS, Lemaire SA, Miller CC III, et al. Mortality and paraplegiaafter thoracoabdominal aortic aneurysm repair: a risk factor analysis.Ann Thorac Surg. 2000;69:409–14.
0. Kouchoukos NT, Masetti P, Rokkas CK, et al. Safety and efficacy ofhypothermic cardiopulmonary bypass and circulatory arrest for opera-tions on the descending thoracic and thoracoabdominal aorta. AnnThorac Surg. 2001;72:699–707.
1. Practice guidelines for perioperative transesophageal echocardiography.A report by the American Society of Anesthesiologists and the Societyof Cardiovascular Anesthesiologists Task Force on TransesophagealEchocardiography. Anesthesiology. 1996;84:986–1006.
2. Fattori R, Caldarera I, Rapezzi C, et al. Primary endoleakage inendovascular treatment of the thoracic aorta: importance of intraopera-tive transesophageal echocardiography. J Thorac Cardiovasc Surg.2000;120:490–5.
3. Abe S, Ono S, Murata K, et al. Usefulness of transesophageal echocar-diographic monitoring in transluminal endovascular stent-graft repair forthoracic aortic aneurysm. Jpn Circ J. 2000;64:960–4.
4. Dong CC, MacDonald DB, Janusz MT. Intraoperative spinal cordmonitoring during descending thoracic and thoracoabdominal aneurysmsurgery. Ann Thorac Surg. 2002;74:S1873–6.
5. Meylaerts SA, Jacobs MJ, van Iterson V, et al. Comparison of transcra-
nial motor evoked potentials and somatosensory evoked potentials
63
63
63
63
64
64
64
64
64
64
64
64
64
64
65
65
65
65
65
65
65
65
65
65
66
66
66
66
66
66
66
66
66
66
67
67
67
67
67
67
67
67
67
67
68
68
e122 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
during thoracoabdominal aortic aneurysm repair. Ann Surg. 1999;230:742–9.
6. Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in theanticoagulated patient: defining the risks (the second ASRA ConsensusConference on Neuraxial Anesthesia and Anticoagulation). Reg AnesthPain Med. 2003;28:172–97.
7. Aadahl P, Lundbom J, Hatlinghus S, et al. Regional anesthesia forendovascular treatment of abdominal aortic aneurysms. J EndovascSurg. 1997;4:56–61.
8. Kim SS, Leibowitz AB. Endovascular thoracic aortic aneurysm repairusing a single catheter for spinal anesthesia and cerebrospinal fluiddrainage. J Cardiothorac Vasc Anesth. 2001;15:88–9.
9. Henretta JP, Hodgson KJ, Mattos MA, et al. Feasibility of endovascularrepair of abdominal aortic aneurysms with local anesthesia with intra-venous sedation. J Vasc Surg. 1999;29:793–8.
0. Mathes DD, Kern JA. Continuous spinal anesthetic technique forendovascular aortic stent graft surgery. J Clin Anesth. 2000;12:487–90.
1. Lachat M, Pfammatter T, Turina M. Transfemoral endografting ofthoracic aortic aneurysm under local anesthesia: a simple, safe and fasttrack procedure. Vasa. 1999;28:204–6.
2. Bettex DA, Lachat M, Pfammatter T, et al. To compare general, epiduraland local anaesthesia for endovascular aneurysm repair (EVAR). Eur JVasc Endovasc Surg. 2001;21:179–84.
3. Verhoeven EL, Cina CS, Tielliu IF, et al. Local anesthesia for endovas-cular abdominal aortic aneurysm repair. J Vasc Surg. 2005;42:402–9.
4. Ruppert V, Leurs LJ, Steckmeier B, et al. Influence of anesthesia type onoutcome after endovascular aortic aneurysm repair: an analysis based onEUROSTAR data. J Vasc Surg. 2006;44:16–21.
5. Stone JG, Young WL, Smith CR, et al. Do standard monitoring sitesreflect true brain temperature when profound hypothermia is rapidlyinduced and reversed? Anesthesiology. 1995;82:344–51.
6. Pronovost P, Needham D, Berenholtz S, et al. An intervention todecrease catheter-related bloodstream infections in the ICU. N EnglJ Med. 2006;355:2725–32.
7. Merrer J, De JB, Golliot F, et al. Complications of femoral andsubclavian venous catheterization in critically ill patients: a randomizedcontrolled trial. JAMA. 2001;286:700–7.
8. Daniel WG, Erbel R, Kasper W, et al. Safety of transesophagealechocardiography. A multicenter survey of 10,419 examinations. Circu-lation. 1991;83:817–21.
9. Moskowitz DM, Kahn RA, Konstadt SN, et al. Intraoperative transoe-sophageal echocardiography as an adjuvant to fluoroscopy duringendovascular thoracic aortic repair. Eur J Vasc Endovasc Surg. 1999;17:22–7.
0. Orihashi K, Matsuura Y, Sueda T, et al. Echocardiography-assistedsurgery in transaortic endovascular stent grafting: role of transesopha-geal echocardiography. J Thorac Cardiovasc Surg. 2000;120:672–8.
1. Campos JH, Massa FC, Kernstine KH. The incidence of right upper-lobecollapse when comparing a right-sided double-lumen tube versus amodified left double-lumen tube for left-sided thoracic surgery. AnesthAnalg. 2000;90:535–40.
2. Ferraris VA, Ferraris SP, Saha SP, et al. Perioperative blood transfusionand blood conservation in cardiac surgery: the Society of ThoracicSurgeons and The Society of Cardiovascular Anesthesiologists clinicalpractice guideline. Ann Thorac Surg. 2007;83:S27–86.
3. Illig KA, Green RM, Ouriel K, et al. Primary fibrinolysis duringsupraceliac aortic clamping. J Vasc Surg. 1997;25:244–51.
4. Cohen JR, Schroder W, Leal J, et al. Mesenteric shunting duringthoracoabdominal aortic clamping to prevent disseminated intravascularcoagulation in dogs. Ann Vasc Surg. 1988;2:261–7.
5. Schneiderman J, Eguchi Y, Adar R, et al. Modulation of the fibrinolyticsystem by major peripheral ischemia. J Vasc Surg. 1994;19:516–24.
6. Welch M, Douglas JT, Smyth JV, et al. Systemic endotoxaemia andfibrinolysis during aortic surgery. Eur J Vasc Endovasc Surg. 1995;9:228–32.
7. Henry DA, Carless PA, Moxey AJ, et al. Anti-fibrinolytic use forminimising perioperative allogeneic blood transfusion. John Wiley &Sons, Ltd. Available at: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD001886/frame.html. Accessed January 7,2010.
8. Fiechtner BK, Nuttall GA, Johnson ME, et al. Plasma tranexamic acidconcentrations during cardiopulmonary bypass. Anesth Analg. 2001;92:
1131–6.9. Shore-Lesserson L, Bodian C, Vela-Cantos F, et al. Antifibrinolytic useand bleeding during surgery on the descending thoracic aorta: amultivariate analysis. J Cardiothorac Vasc Anesth. 2005;19:453–8.
0. Akashi H, Tayama K, Fujino T, et al. Cerebral protection selection inaortic arch surgery for patients with preoperative complications ofcerebrovascular disease. Jpn J Thorac Cardiovasc Surg. 2000;48:782–8.
1. Ehrlich MP, Fang WC, Grabenwoger M, et al. Impact of retrogradecerebral perfusion on aortic arch aneurysm repair. J Thorac CardiovascSurg. 1999;118:1026–32.
2. Di Eusanio M, Wesselink RM, Morshuis WJ, et al. Deep hypothermiccirculatory arrest and antegrade selective cerebral perfusion duringascending aorta-hemiarch replacement: a retrospective comparativestudy. J Thorac Cardiovasc Surg. 2003;125:849–54.
3. Hagl C, Ergin MA, Galla JD, et al. Neurologic outcome after ascendingaorta-aortic arch operations: effect of brain protection technique inhigh-risk patients. J Thorac Cardiovasc Surg. 2001;121:1107–21.
4. Reich DL, Uysal S, Sliwinski M, et al. Neuropsychologic outcome afterdeep hypothermic circulatory arrest in adults. J Thorac Cardiovasc Surg.1999;117:156–63.
5. Reich DL, Uysal S, Ergin MA, et al. Retrograde cerebral perfusionduring thoracic aortic surgery and late neuropsychological dysfunction.Eur J Cardiothorac Surg. 2001;19:594–600.
6. Usui A, Yasuura K, Watanabe T, et al. Comparative clinical studybetween retrograde cerebral perfusion and selective cerebral perfusion insurgery for acute type A aortic dissection. Eur J Cardiothorac Surg.1999;15:571–8.
7. Kunihara T, Grun T, Aicher D, et al. Hypothermic circulatory arrest isnot a risk factor for neurologic morbidity in aortic surgery: a propensityscore analysis. J Thorac Cardiovasc Surg. 2005;130:712–8.
8. Schepens MA, Dossche KM, Morshuis WJ, et al. The elephant trunktechnique: operative results in 100 consecutive patients. Eur J Cardio-thorac Surg. 2002;21:276–81.
9. Deeb GM, Williams DM, Quint LE, et al. Risk analysis for aorticsurgery using hypothermic circulatory arrest with retrograde cerebralperfusion. Ann Thorac Surg. 1999;67:1883–6.
0. Ehrlich MP, Schillinger M, Grabenwoger M, et al. Predictors of adverseoutcome and transient neurological dysfunction following surgicaltreatment of acute type A dissections. Circulation. 2003;108 Suppl1:II318–23.
1. Fleck TM, Czerny M, Hutschala D, et al. The incidence of transientneurologic dysfunction after ascending aortic replacement with circula-tory arrest. Ann Thorac Surg. 2003;76:1198–202.
2. Moshkovitz Y, David TE, Caleb M, et al. Circulatory arrest undermoderate systemic hypothermia and cold retrograde cerebral perfusion.Ann Thorac Surg. 1998;66:1179–84.
3. Okita Y, Takamoto S, Ando M, et al. Mortality and cerebral outcome inpatients who underwent aortic arch operations using deep hypothermiccirculatory arrest with retrograde cerebral perfusion: no relation of earlydeath, stroke, and delirium to the duration of circulatory arrest. J ThoracCardiovasc Surg. 1998;115:129–38.
4. Ueda Y, Okita Y, Aomi S, et al. Retrograde cerebral perfusion for aorticarch surgery: analysis of risk factors. Ann Thorac Surg. 1999;67:1879–82.
5. Wong CH, Bonser RS. Does retrograde cerebral perfusion affect riskfactors for stroke and mortality after hypothermic circulatory arrest?Ann Thorac Surg. 1999;67:1900–3.
6. Di Eusanio M, Schepens MA, Morshuis WJ, et al. Brain protection usingantegrade selective cerebral perfusion: a multicenter study. Ann ThoracSurg. 2003;76:1181–8.
7. Di Eusanio M, Schepens MA, Morshuis WJ, et al. Antegrade selectivecerebral perfusion during operations on the thoracic aorta: factorsinfluencing survival and neurologic outcome in 413 patients. J ThoracCardiovasc Surg. 2002;124:1080–6.
8. Di Eusanio M, Tan ME, Schepens MA, et al. Surgery for acute type Adissection using antegrade selective cerebral perfusion: experience with122 patients. Ann Thorac Surg. 2003;75:514–9.
9. Kazui T, Yamashita K, Washiyama N, et al. Impact of an aggressivesurgical approach on surgical outcome in type A aortic dissection. AnnThorac Surg. 2002;74:S1844–7.
0. Kazui T, Yamashita K, Washiyama N, et al. Aortic arch replacementusing selective cerebral perfusion. Ann Thorac Surg. 2007;83:S796–8.
1. Numata S, Ogino H, Sasaki H, et al. Total arch replacement usingantegrade selective cerebral perfusion with right axillary artery perfu-
sion. Eur J Cardiothorac Surg. 2003;23:771–5.
68
68
68
68
68
68
68
68
69
69
69
69
69
69
69
69
69
69
70
70
70
70
70
70
70
70
70
70
71
71
71
71
71
71
71
71
71
71
72
72
72
72
72
72
72
72
72
e123JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
2. Sasaki H, Ogino H, Matsuda H, et al. Integrated total arch replacementusing selective cerebral perfusion: a 6-year experience. Ann ThoracSurg. 2007;83:S805–10.
3. Strauch JT, Spielvogel D, Lauten A, et al. Axillary artery cannulation:routine use in ascending aorta and aortic arch replacement. Ann ThoracSurg. 2004;78:103–8.
4. Kamiya H, Hagl C, Kropivnitskaya I, et al. Quick proximal archreplacement with moderate hypothermic circulatory arrest. Ann ThoracSurg. 2007;83:1055–8.
5. Matalanis G, Hata M, Buxton BF. A retrospective comparative study ofdeep hypothermic circulatory arrest, retrograde, and antegrade cerebralperfusion in aortic arch surgery. Ann Thorac Cardiovasc Surg. 2003;9:174–9.
6. Okita Y, Minatoya K, Tagusari O, et al. Prospective comparative studyof brain protection in total aortic arch replacement: deep hypothermiccirculatory arrest with retrograde cerebral perfusion or selective ante-grade cerebral perfusion. Ann Thorac Surg. 2001;72:72–9.
7. Zierer A, Aybek T, Risteski P, et al. Moderate hypothermia (30 degreesC) for surgery of acute type A aortic dissection. Thorac CardiovascSurg. 2005;53:74–9.
8. Okita Y, Ando M, Minatoya K, et al. Predictive factors for mortality andcerebral complications in arteriosclerotic aneurysm of the aortic arch.Ann Thorac Surg. 1999;67:72–8.
9. Grigore AM, Grocott HP, Mathew JP, et al. The rewarming rate andincreased peak temperature alter neurocognitive outcome after cardiacsurgery. Anesth Analg. 2002;94:4–10.table
0. Grocott HP, Mackensen GB, Grigore AM, et al. Postoperative hyper-thermia is associated with cognitive dysfunction after coronary arterybypass graft surgery. Stroke. 2002;33:537–41.
1. Bar-Yosef S, Mathew JP, Newman MF, et al. Prevention of cerebralhyperthermia during cardiac surgery by limiting on-bypass rewarming incombination with post-bypass body surface warming: a feasibility study.Anesth Analg. 2004;99:641–6, table.
2. Chong SY, Chow MY, Kang DS, et al. Deep hypothermic circulatoryarrest in adults undergoing aortic surgery: local experience. Ann AcadMed Singapore. 2004;33:289–93.
3. Gega A, Rizzo JA, Johnson MH, et al. Straight deep hypothermic arrest:experience in 394 patients supports its effectiveness as a sole means ofbrain preservation. Ann Thorac Surg. 2007;84:759–66.
4. Bavaria JE, Pochettino A, Brinster DR, et al. New paradigms andimproved results for the surgical treatment of acute type A dissection.Ann Surg. 2001;234:336–42.
5. Bonser RS, Wong CH, Harrington D, et al. Failure of retrograde cerebralperfusion to attenuate metabolic changes associated with hypothermiccirculatory arrest. J Thorac Cardiovasc Surg. 2002;123:943–50.
6. Cheung AT, Bavaria JE, Pochettino A, et al. Oxygen delivery duringretrograde cerebral perfusion in humans. Anesth Analg. 1999;88:8–15.
7. Estrera AL, Miller CC III, Huynh TT, et al. Replacement of theascending and transverse aortic arch: determinants of long-term survival.Ann Thorac Surg. 2002;74:1058–64.
8. Lemaire SA, Bhama JK, Schmittling ZC, et al. S100beta correlates withneurologic complications after aortic operation using circulatory arrest.Ann Thorac Surg. 2001;71:1913–8.
9. Moon MR, Sundt TM III. Influence of retrograde cerebral perfusionduring aortic arch procedures. Ann Thorac Surg. 2002;74:426–31.
0. Ehrlich MP, Hagl C, McCullough JN, et al. Retrograde cerebralperfusion provides negligible flow through brain capillaries in the pig.J Thorac Cardiovasc Surg. 2001;122:331–8.
1. Karadeniz U, Erdemli O, Ozatik MA, et al. Assessment of cerebralblood flow with transcranial Doppler in right brachial artery perfusionpatients. Ann Thorac Surg. 2005;79:139–46.
2. Neri E, Massetti M, Barabesi L, et al. Extrathoracic cannulation of theleft common carotid artery in thoracic aorta operations through a leftthoracotomy: preliminary experience in 26 patients. J Thorac CardiovascSurg. 2002;123:901–10.
3. Wozniak G, Dapper F, Zickmann B, et al. Selective Cerebral perfusionvia innominate artery in aortic arch replacement without deep hypother-mic circulatory arrest. Int J Angiol. 1999;8:50–6.
4. Yilik L, Emrecan B, Kestelli M, et al. Direct versus side-graft cannu-lation of the right axillary artery for antegrade cerebral perfusion. TexHeart Inst J. 2006;33:310–5.
5. Olsson C, Thelin S. Antegrade cerebral perfusion with a simplifiedtechnique: unilateral versus bilateral perfusion. Ann Thorac Surg.
2006;81:868–74.6. Harrington DK, Walker AS, Kaukuntla H, et al. Selective antegradecerebral perfusion attenuates brain metabolic deficit in aortic archsurgery: a prospective randomized trial. Circulation. 2004;110:II231–6.
7. Neri E, Sassi C, Barabesi L, et al. Cerebral autoregulation afterhypothermic circulatory arrest in operations on the aortic arch. AnnThorac Surg. 2004;77:72–9.
8. Cook RC, Gao M, Macnab AJ, et al. Aortic arch reconstruction: safetyof moderate hypothermia and antegrade cerebral perfusion duringsystemic circulatory arrest. J Card Surg. 2006;21:158–64.
9. Bahktiary F. Cerebral profusion associated with profound hypothermia.J Thorac Cardiovasc Surg. 2006;132:153–4.Abstract
0. Kamiya H, Hagl C, Kropivnitskaya I, et al. The safety of moderatehypothermic lower body circulatory arrest with selective cerebralperfusion: a propensity score analysis. J Thorac Cardiovasc Surg.2007;133:501–9.
1. Kaneda T, Saga T, Onoe M, et al. Antegrade selective cerebral perfusionwith mild hypothermic systemic circulatory arrest during thoracic aorticsurgery. Scand Cardiovasc J. 2005;39:87–90.
2. Testolin L, Roques X, Laborde MN, et al. Moderately hypothermiccardiopulmonary bypass and selective cerebral perfusion in ascendingaorta and aortic arch surgery. Preliminary experience in twenty-twopatients. Cardiovasc Surg. 1998;6:398–405.
3. Khan SN, Stansby G. Cerebrospinal fluid drainage for thoracic andthoracoabdominal aortic aneurysm surgery. Cochrane Database SystRev. 2004;CD003635.
4. Safi HJ, Hess KR, Randel M, et al. Cerebrospinal fluid drainage anddistal aortic perfusion: reducing neurologic complications in repair ofthoracoabdominal aortic aneurysm types I and II. J Vasc Surg. 1996;23:223–8.
5. Hollier LH, Money SR, Naslund TC, et al. Risk of spinal corddysfunction in patients undergoing thoracoabdominal aortic replace-ment. Am J Surg. 1992;164:210–3.
6. Cambria RP, Davison JK, Zannetti S, et al. Clinical experience withepidural cooling for spinal cord protection during thoracic and thoraco-abdominal aneurysm repair. J Vasc Surg. 1997;25:234–41.
7. Woloszyn TT, Marini CP, Coons MS, et al. Cerebrospinal fluid drainageand steroids provide better spinal cord protection during aortic cross-clamping than does either treatment alone. Ann Thorac Surg. 1990;49:78–82.
8. Ogino H, Sasaki H, Minatoya K, et al. Combined use of adamkiewiczartery demonstration and motor-evoked potentials in descending andthoracoabdominal repair. Ann Thorac Surg. 2006;82:592–6.
9. Guerit JM, Witdoeckt C, Verhelst R, et al. Sensitivity, specificity, andsurgical impact of somatosensory evoked potentials in descending aortasurgery. Ann Thorac Surg. 1999;67:1943–6.
0. Mauney MC, Blackbourne LH, Langenburg SE, et al. Prevention ofspinal cord injury after repair of the thoracic or thoracoabdominal aorta.Ann Thorac Surg. 1995;59:245–52.
1. Niessen K, Karsan A. Notch signaling in the developing cardiovascularsystem. Am J Physiol Cell Physiol. 2007;293:C1–C11.
2. Crafoord C, Hiertonn T. Surgical treatment of thrombotic obliteration ofthe aortic bifurcation. Acta Chir Scand. 1952;104:81–6.
3. Hollier LH, Symmonds JB, Pairolero PC, et al. Thoracoabdominal aorticaneurysm repair. Analysis of postoperative morbidityArch Surg. 1988;123:871–5.
4. Greenberg RK, Lu Q, Roselli EE, et al. Contemporary analysis ofdescending thoracic and thoracoabdominal aneurysm repair: a compar-ison of endovascular and open techniques. Circulation. 2008;118:808–17.
5. Svensson LG, Patel V, Robinson MF, et al. Influence of preservation orperfusion of intraoperatively identified spinal cord blood supply onspinal motor evoked potentials and paraplegia after aortic surgery. JVasc Surg. 1991;13:355–65.
6. Svensson LG, Von Ritter CM, Groeneveld HT, et al. Cross-clamping ofthe thoracic aorta. Influence of aortic shunts, laminectomy, papaverine,calcium channel blocker, allopurinol, and superoxide dismutase onspinal cord blood flow and paraplegia in baboonsAnn Surg. 1986;204:38–47.
7. Juvonen T, Biancari F, Rimpilainen J, et al. Strategies for spinal cordprotection during descending thoracic and thoracoabdominal aorticsurgery: Up-to-date experimental and clinical results: a review. ScandCardiovasc J. 2002;36:136–60.
8. Lotto ML, Banoub M, Schubert A. Effects of anesthetic agents andphysiologic changes on intraoperative motor evoked potentials. J Neu-
rosurg Anesthesiol. 2004;16:32–42.
72
73
73
73
73
73
73
73
73
73
73
74
74
74
74
74
74
74
74
74
74
75
75
75
75
75
75
75
75
75
75
76
76
76
76
76
76
76
76
76
76
77
77
77
77
77
77
77
77
77
e124 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
9. Angel A, LeBeau F. A comparison of the effects of propofol with otheranaesthetic agents on the centripetal transmission of sensory informa-tion. Gen Pharmacol. 1992;23:945–63.
0. Chen Z. The effects of isoflurane and propofol on intraoperativeneurophysiological monitoring during spinal surgery. J Clin MonitComput. 2004;18:303–8.
1. Clapcich AJ, Emerson RG, Roye DP Jr., et al. The effects of propofol,small-dose isoflurane, and nitrous oxide on cortical somatosensoryevoked potential and bispectral index monitoring in adolescents under-going spinal fusion. Anesth Analg. 2004;99:1334–40.
2. King J, Sloan TB. Evoked Potentials Intraoperative Monitoring of theSpinal Cord and Peripheral Nerves. St. Louis, MO: Mosby; 2001.
3. Moller AR. Intraoperative Neurophysiologic Monitoring. Luxembourg:Harwood1995.
4. Nuwer MR, Dawson EG, Carlson LG, et al. Somatosensory evokedpotential spinal cord monitoring reduces neurologic deficits after scoli-osis surgery: results of a large multicenter survey. ElectroencephalogrClin Neurophysiol. 1995;96:6–11.
5. Peterson DO, Drummond JC, Todd MM. Effects of halothane, enflurane,isoflurane, and nitrous oxide on somatosensory evoked potentials inhumans. Anesthesiology. 1986;65:35–40.
6. Scheufler KM, Zentner J. Total intravenous anesthesia for intraoperativemonitoring of the motor pathways: an integral view combining clinicaland experimental data. J Neurosurg. 2002;96:571–9.
7. Sloan T. Evoked potentials. In: Albin MS, editor. A Textbook ofNeuroanesthesia With Neurosurgical and Neuroscience Perspectives.New York, NY: McGraw-Hill, 1997;221–76.
8. Sloan TB, Heyer EJ. Anesthesia for intraoperative neurophysiologicmonitoring of the spinal cord. J Clin Neurophysiol. 2002;19:430–43.
9. Crawford ES, Mizrahi EM, Hess KR, et al. The impact of distal aorticperfusion and somatosensory evoked potential monitoring on preventionof paraplegia after aortic aneurysm operation. J Thorac Cardiovasc Surg.1988;95:357–67.
0. Lyon R, Feiner J, Lieberman JA. Progressive suppression of motorevoked potentials during general anesthesia: the phenomenon of “anes-thetic fade.” J Neurosurg Anesthesiol. 2005;17:13–9.
1. Etz CD, Halstead JC, Spielvogel D, et al. Thoracic and thoracoabdomi-nal aneurysm repair: is reimplantation of spinal cord arteries a waste oftime? Ann Thorac Surg. 2006;82:1670–7.
2. Svensson LG, Stewart RW, Cosgrove DM III, et al. Intrathecal papav-erine for the prevention of paraplegia after operation on the thoracic orthoracoabdominal aorta. J Thorac Cardiovasc Surg. 1988;96:823–9.
3. Laschinger JC. Spinal cord injury following surgical correction of acuteaortic disruption. Semin Thorac Cardiovasc Surg. 1992;4:217–22.
4. Piano G, Gewertz BL. Mechanism of increased cerebrospinal fluidpressure with thoracic aortic occlusion. J Vasc Surg. 1990;11:695–701.
5. Spence PA, Lust RM, Iida H, et al. Reappraisal of the mechanism forcerebrospinal fluid hypertension during aortic surgery. Circulation.1990;82:IV51–IV57.
6. Dardik A, Perler BA, Roseborough GS, et al. Subdural hematoma afterthoracoabdominal aortic aneurysm repair: an underreported complica-tion of spinal fluid drainage? J Vasc Surg. 2002;36:47–50.
7. Roland PS, Marple BF, Meyerhoff WL, et al. Complications of lumbarspinal fluid drainage. Otolaryngol Head Neck Surg. 1992;107:564–9.
8. Mutch WA, Thomson IR, Teskey JM, et al. Phlebotomy reverses thehemodynamic consequences of thoracic aortic cross-clamping: relation-ships between central venous pressure and cerebrospinal fluid pressure.Anesthesiology. 1991;74:320–4.
9. Mutch WA, Thiessen DB, Girling LG, et al. Neuroanesthesia adjuncttherapy (mannitol and hyperventilation) is as effective as cerebrospinalfluid drainage for prevention of paraplegia after descending thoracicaortic cross-clamping in the dog. Anesth Analg. 1995;81:800–5.
0. Cheung AT, Pochettino A, Guvakov DV, et al. Safety of lumbar drainsin thoracic aortic operations performed with extracorporeal circulation.Ann Thorac Surg. 2003;76:1190–6.
1. Grocott HP, Nussmeier NA. Neuroprotection in cardiac surgery. Anes-thesiol Clin North Am. 2003;21:487–509, viii.
2. Hindman BJ, Todd MM. Improving neurologic outcome after cardiacsurgery. Anesthesiology. 1999;90:1243–7.
3. Moomiaie RM, Ransden J, Stein J, et al. Cooling catheter for spinal cordpreservation in thoracic aortic surgery. J Cardiovasc Surg (Torino).2007;48:103–8.
4. Barone GW, Joob AW, Flanagan TL, et al. The effect of hyperemia onspinal cord function after temporary thoracic aortic occlusion. J Vasc
Surg. 1988;8:535–40.5. Jacobs MJ, de Mol BA, Legemate DA, et al. Retrograde aortic andselective organ perfusion during thoracoabdominal aortic aneurysmrepair. Eur J Vasc Endovasc Surg. 1997;14:360–6.
6. Koksoy C, Lemaire SA, Curling PE, et al. Renal perfusion duringthoracoabdominal aortic operations: cold crystalloid is superior tonormothermic blood. Ann Thorac Surg. 2002;73:730–8.
7. Perdue PW, Balser JR, Lipsett PA, et al. “Renal dose” dopamine insurgical patients: dogma or science? Ann Surg. 1998;227:470–3.
8. Hager B, Betschart M, Krapf R. Effect of postoperative intravenous loopdiuretic on renal function after major surgery. Schweiz Med Wochen-schr. 1996;126:666–73.
9. Godet G, Fleron MH, Vicaut E, et al. Risk factors for acute postoper-ative renal failure in thoracic or thoracoabdominal aortic surgery: aprospective study. Anesth Analg. 1997;85:1227–32.
0. Nicholson ML, Baker DM, Hopkinson BR, et al. Randomized controlledtrial of the effect of mannitol on renal reperfusion injury during aorticaneurysm surgery. Br J Surg. 1996;83:1230–3.
1. Baldwin L, Henderson A, Hickman P. Effect of postoperative low-dosedopamine on renal function after elective major vascular surgery. AnnIntern Med. 1994;120:744–7.
2. Paul MD, Mazer CD, Byrick RJ, et al. Influence of mannitol anddopamine on renal function during elective infrarenal aortic clamping inman. Am J Nephrol. 1986;6:427–34.
3. Pavoni V, Verri M, Ferraro L, et al. Plasma dopamine concentration andeffects of low dopamine doses on urinary output after major vascularsurgery. Kidney Int Suppl. 1998;66:S75–S80.
4. Salem MG, Crooke JW, McLoughlin GA, et al. The effect of dopamineon renal function during aortic cross clamping. Ann R Coll Surg Engl.1988;70:9–12.
5. Zehr KJ, Orszulak TA, Mullany CJ, et al. Surgery for aneurysms of theaortic root: a 30-year experience. Circulation. 2004;110:1364–71.
6. Motomura N, Miyata H, Tsukihara H, et al. Risk model of thoracicaortic surgery in 4707 cases from a nationwide single-race populationthrough a web-based data entry system: the first report of 30-day and30-day operative outcome risk models for thoracic aortic surgery.Circulation. 2008;118:S153–9.
7. Kouchoukos NT, Masetti P, Mauney MC, et al. One-stage repair ofextensive chronic aortic dissection using the arch-first technique andbilateral anterior thoracotomy. Ann Thorac Surg. 2008;86:1502–9.
8. Coselli JS, Bozinovski J, Lemaire SA. Open surgical repair of 2286thoracoabdominal aortic aneurysms. Ann Thorac Surg. 2007;83:S862–4.
9. Etz CD, Luehr M, Kari FA, et al. Paraplegia after extensive thoracic andthoracoabdominal aortic aneurysm repair: does critical spinal cordischemia occur postoperatively? J Thorac Cardiovasc Surg. 2008;135:324–30.
0. Keyhani K, Miller CC III, Estrera AL, et al. Analysis of motor andsomatosensory evoked potentials during thoracic and thoracoabdominalaortic aneurysm repair. J Vasc Surg. 2009;49:36–41.
1. Lemaire SA, Jones MM, Conklin LD, et al. Randomized comparison ofcold blood and cold crystalloid renal perfusion for renal protectionduring thoracoabdominal aortic aneurysm repair. J Vasc Surg. 2009;49:11–9.
2. Safi HJ, Estrera AL, Azizzadeh A, et al. Progress and future challengesin thoracoabdominal aortic aneurysm management. World J Surg.2008;32:355–60.
3. Svensson LG, Hess KR, Coselli JS, et al. Influence of segmental arteries,extent, and atriofemoral bypass on postoperative paraplegia after thora-coabdominal aortic operations. J Vasc Surg. 1994;20:255–62.
4. Borger MA, Preston M, Ivanov J, et al. Should the ascending aorta bereplaced more frequently in patients with bicuspid aortic valve disease?J Thorac Cardiovasc Surg. 2004;128:677–83.
5. Sioris T, David TE, Ivanov J, et al. Clinical outcomes after separate andcomposite replacement of the aortic valve and ascending aorta. J ThoracCardiovasc Surg. 2004;128:260–5.
6. David TE, Ivanov J, Armstrong S, et al. Aortic valve-sparing operationsin patients with aneurysms of the aortic root or ascending aorta. AnnThorac Surg. 2002;74:S1758–61.
7. Trimarchi S, Nienaber CA, Rampoldi V, et al. Contemporary results ofsurgery in acute type A aortic dissection: The International Registry ofAcute Aortic Dissection experience. J Thorac Cardiovasc Surg. 2005;129:112–22.
8. Sundt TM III, Orszulak TA, Cook DJ, et al. Improving results of open
arch replacement. Ann Thorac Surg. 2008;86:787–96.
77
78
78
78
78
78
78
78
78
78
78
79
79
79
79
79
79
79
79
79
79
80
80
80
80
80
80
80
80
80
80
81
81
81
81
81
81
81
81
81
81
81
82
82
82
82
82
82
82
82
Kdiinao
e125JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
9. Spielvogel D, Halstead JC, Meier M, et al. Aortic arch replacementusing a trifurcated graft: simple, versatile, and safe. Ann Thorac Surg.2005;80:90–5.
0. Safi HJ, Estrera AL, Miller CC, et al. Evolution of risk for neurologicdeficit after descending and thoracoabdominal aortic repair. Ann ThoracSurg. 2005;80:2173–9.
1. Svensson LG, Hess KR, D’Agostino RS, et al. Reduction of neurologicinjury after high-risk thoracoabdominal aortic operation. Ann ThoracSurg. 1998;66:132–8.
2. Rigberg DA, McGory ML, Zingmond DS, et al. Thirty-day mortalitystatistics underestimate the risk of repair of thoracoabdominal aorticaneurysms: a statewide experience. J Vasc Surg. 2006;43:217–22.
3. Knipp BS, Deeb GM, Prager RL, et al. A contemporary analysis ofoutcomes for operative repair of type A aortic dissection in the UnitedStates. Surgery. 2007;142:524–8.
4. Grundy SM. United States Cholesterol Guidelines 2001: expanded scopeof intensive low-density lipoprotein-lowering therapy. Am J Cardiol.2001;88:23J–27J.
5. Davies RR, Kaple RK, Mandapati D, et al. Natural history of ascendingaortic aneurysms in the setting of an unreplaced bicuspid aortic valve.Ann Thorac Surg. 2007;83:1338–44.
6. Song JM, Kim SD, Kim JH, et al. Long-term predictors of descendingaorta aneurysmal change in patients with aortic dissection. J Am CollCardiol. 2007;50:799–804.
7. Halstead JC, Meier M, Etz C, et al. The fate of the distal aorta afterrepair of acute type A aortic dissection. J Thorac Cardiovasc Surg.2007;133:127–35.
8. Immer FF, Krahenbuhl E, Hagen U, et al. Large area of the false lumenfavors secondary dilatation of the aorta after acute type A aorticdissection. Circulation. 2005;112:I249–52.
9. Sundt TM. Intramural hematoma and penetrating atherosclerotic ulcer ofthe aorta. Ann Thorac Surg. 2007;83:S835–41.
0. Benowitz NL. Drug therapy. Pharmacologic aspects of cigarette smok-ing and nicotine addition. N Engl J Med. 1988;319:1318–30.
1. Grundy SM, Becker D.M.C.L.T.Third Report of the National Choles-terol Education Program (NCEP) Expert Panel on Detection, Evaluation,and Treatment of High Blood Cholesterol in Adults (Adult TreatmentPanel III) final report. Circulation. 2002;106:3143–421.
2. Wung SF, Aouizerat BE. Newly mapped gene for thoracic aorticaneurysm and dissection. J Cardiovasc Nurs. 2004;19:409–16.
3. Davidson JE, Powers K, Hedayat KM, et al. Clinical practice guidelinesfor support of the family in the patient-centered intensive care unit:American College of Critical Care Medicine Task Force 2004-2005. CritCare Med. 2007;35:605–22.
4. Latessa V. Endovascular stent-graft repair of descending thoracic aorticaneurysms: the nursing implications for care. J Vasc Nurs. 2002;20:86–93.
5. Garber AJ, Moghissi ES, Bransome ED Jr., et al. American College ofEndocrinology position statement on inpatient diabetes and metaboliccontrol. Endocr Pract. 2004;10:77–82.
6. Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulintherapy in the critically ill patients. N Engl J Med. 2001;345:1359–67.
7. Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusionreduces mortality in patients with diabetes undergoing coronary arterybypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007–21.
8. Inzucchi SE. Clinical practice. Management of hyperglycemia in thehospital setting. N Engl J Med. 2006;355:1903–11.
9. Miyairi T, Takamoto S, Kotsuka Y, et al. Comparison of neurocognitiveresults after coronary artery bypass grafting and thoracic aortic surgeryusing retrograde cerebral perfusion. Eur J Cardiothorac Surg. 2005;28:97–101.
0. Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aorticdissection in perspective. Circulation. 2002;105:1529–30.
1. Maron BJ, Chaitman BR, Ackerman MJ, et al. Recommendations forphysical activity and recreational sports participation for young patientswith genetic cardiovascular diseases. Circulation. 2004;109:2807–16.
2. Williams MA, Haskell WL, Ades PA, et al. Resistance exercise inindividuals with and without cardiovascular disease: 2007 update: ascientific statement from the American Heart Association Council onClinical Cardiology and Council on Nutrition, Physical Activity, andMetabolism. Circulation. 2007;116:572–84.
3. Palatini P, Mos L, Munari L, et al. Blood pressure changes duringheavy-resistance exercise. J Hypertens Suppl. 1989;7:S72–3.
4. Hatzaras I, Tranquilli M, Coady M, et al. Weight lifting and aortic
dissection: more evidence for a connection. Cardiology. 2007;107:103–6. di5. Nataf P, Lansac E. Dilation of the thoracic aorta: medical and surgicalmanagement. Heart. 2006;92:1345–52.
6. Elefteriades JA, Hatzaras I, Tranquilli MA, et al. Weight lifting andrupture of silent aortic aneurysms. JAMA. 2003;290:2803.
7. Williams OD. Quality of care versus provider volume: does one lead tothe other? Med Care. 2003;41:1127–8.
8. Hill JS, McPhee JT, Messina LM, et al. Regionalization of abdominalaortic aneurysm repair: evidence of a shift to high-volume centers in theendovascular era. J Vasc Surg. 2008;48:29–36.
9. Schermerhorn ML, Giles KA, Hamdan AD, et al. Population-basedoutcomes of open descending thoracic aortic aneurysm repair. J VascSurg. 2008;48:821–7.
0. Norgren L, Larzon T. Endovascular repair of the ruptured abdominalaortic aneurysm. Scand J Surg. 2008;97:178–81.
1. Troeng T. Volume versus outcome when treating abdominal aorticaneurysm electively: is there evidence to centralise? Scand J Surg.2008;97:154–9.
1a.Bonow RO, Masoudi FA, Rumsfeld JS, et al. ACC/AHA classificationof care metrics: performance measures and quality metrics: a report ofthe American College of Cardiology/American Heart Association TaskForce on Performance Measures. J Am Coll Cardiol. 2008;52:2113–7.
2. Estes NA III, Halperin JL, Calkins H, et al. ACC/AHA/Physician Consor-tium 2008 clinical performance measures for adults with nonvalvular atrialfibrillation or atrial flutter. J Am Coll Cardiol. 2008;51:865–84.
3. Krumholz HM, Anderson JL, Brooks NH, et al. ACC/AHA clinicalperformance measures for adults with ST-elevation and non-ST-elevation myocardial infarction. J Am Coll Cardiol. 2006;47:236–65.
4. Thomas RJ, King M, Lui K, et al. AACVPR/ACC/AHA 2007 Perfor-mance measures on cardiac rehabilitation for referral to and delivery ofcardiac rehabilitation/secondary prevention services. J Am Coll Cardiol.2007;50:1400–33.
5. Luft HS. From observing the relationship between volume and outcometo making policy recommendations: comments on Sheikh. Med Care.2003;41:1118–22.
6. Ting HH, Yang EH, Rihal CS. Narrative review: reperfusion strategiesfor ST-segment elevation myocardial infarction. Ann Intern Med.2006;145:610–7.
7. Luft HS, Bunker JP, Enthoven AC. Should operations be regionalized?The empirical relation between surgical volume and mortality. N EnglJ Med. 1979;301:1364–9.
8. Dudley RA, Johansen KL, Brand R, et al. Selective referral to high-volume hospitals: estimating potentially avoidable deaths. JAMA. 2000;283:1159–66.
9. Jacobs AK. Regional systems of care for patients with ST-elevationmyocardial infarction: being at the right place at the right time.Circulation. 2007;116:689–92.
0. Rosenberg AL, Hofer TP, Strachan C, et al. Accepting critically illtransfer patients: adverse effect on a referral center’s outcome andbenchmark measures. Ann Intern Med. 2003;138:882–90.
1. Kosseim M, Mayo NE, Scott S, et al. Ranking hospitals according toacute myocardial infarction mortality: should transfers be included?Med Care. 2006;44:664–70.
2. Leonard JC. Thomas Bevill Peacock and the early history of dissectinganeurysm. Br Med J. 1979;2:260–2.
3. Reece TB, Green GR, Kron IL. Aortic dissection. In: Cohn LH, editor.Cardiac Surgery in the Adult. New York, NY: McGraw-Hill, 2008;1195–222.
4. GORE I. Pathogenesis of dissecting aneurysm of the aorta. AMA ArchPathol. 1952;53:142–53.
5. Krukenberg E. Beiträge zur pathologischen Anatomie und zur allge-meinen Pathologie. Beitr Pathol Anat Allg Pathol. 1920;67:329–51.
6. Toda R, Moriyama Y, Masuda H, et al. Organ malperfusion in acuteaortic dissection. Jpn J Thorac Cardiovasc Surg. 2000;48:545–50.
7. Dietz H, Deveraux R, Loeys BL. NHLBI working group research inMarfan syndrome and related disorders. Available at: http://www.nhlbi.nih.gov/meetings/workshops/marfan20070430.htm. Ac-cessed January 7, 2010.
EY WORDS: ACC/AHA Clinical Practice Guideline � thoracic aorticsease � thoracic aortic dissection � thoracic aortic aneurysm �tramural hematoma � genetic syndromes associated with thoracicrtic aneurysm � emergency department � acute thoracic aortic
sease presentation and evaluation.
ApGu
CoMe
LorHirCh
GeBa
JosBe
RoBe
VinCa
DoCa
KimEag
LukHe
EriIss
EllaKa
NicKo
BruLyt
DiaMil
e126 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
pendix 1. Author Relationships With Industry and Other Entities—2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVMidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease
mmitteember Employment Consultant Speaker
Ownership/Partnership/
Principal Research
Institutional,Organizational or Other
Financial Benefit Expert Witness
en F.atzka,air
Cardiac, Vascular & ThoracicSurgeons Inc. and TriHealth
Inc.—Medical Director,Cardiac Surgery
None None None None None ● 2007; Defense;Aortic Dissection
orge L.kris
University of Chicago MedicalCenter—Professor ofMedicine; Director,
Hypertension Center
● Abbott● Boehringer Ingelheim● Bristol-Myers Squibb/
Sanofi-aventis● Forest Laboratories● GlaxoSmithKline● Merck
● Forest Laboratories● GlaxoSmithKline● Merck● Novartis
None ● Forest Laboratories● GlaxoSmithKline● Myogen● National Institutes
of Health (NIDDK/NHLBI)
None None
hua A.ckman
Brigham & Women’sHospital—Director,
Cardiovascular FellowsProgram
● Bristol-Myers Squibb● Sanofi-aventis
● Bristol-MyersSquibb
● GlaxoSmithKline● Merck● Sanofi-aventis
None None None None
bert M.rsin
Seattle Cardiology—Director,Endovascular Services &
Clinical Research
● Abbott Vascular● Boston Scientific● Bristol-Myers Squibb● Cordis Endovascular● Eli Lilly● EV3● ReVascular
Theraputics● Sanofi-aventis● Vascular Solutions● W.L. Gore
● Boston Scientific● Bristol-Myers
Squibb● Daiichi Sankyo● Eli Lilly● Sanofi-aventis● The Medicines
Company
● VascularSolutions
● Boston Scientific ● Boston Scientific● Cordis Endovascular● Vascular Solutions
● Expert witness ina case involvingiatrogenic type Bdissection
cent F.rr
Uniformed ServicesUniversity of Health
Science—Professor ofMedicine
None None None None None None
nald E.sey, Jr
Atlantic Health—VicePresident of Quality & ChiefMedical Officer; Associate
Professor of Medicine, MountSinai School of Medicine
None None None None None None
A.le
University of Michigan HealthSystem—Albion Walter
Professor of InternalMedicine; Clinical Director,
Cardiovascular Center
● NHLBI● Robert Wood Johnson
Foundation● Sanofi-aventis
None None ● Blue Cross/BlueShield
● Bristol-MyersSquibb
● National Institutesof Health
● Pfizer
None None
e K.rmann
Mount Sinai MedicalCenter—Assistant Professor
of Emergency Medicine;Director, Chest Pain Unit
None None None None None None
c M.elbacher
Massachusetts GeneralHospital—Associate
Professor of Medicine,Harvard Medical School;
Co-Director, Thoracic AorticCenter
None None None None None ● 2007; Plantiff;Aortic Dissection
A.zerooni
University of Michigan HealthSystem—Professor of
Medicine; Director,Cardiothoracic Radiology
● GE Healthcare● Vital Images
None None None ● GERRAF (GERadiology ResearchFellowship)
None
holas T.uchoukos
Missouri Baptist MedicalCenter—Cardiovascular
Surgeon
● Edwards Lifesciences None None None None ● 2006; Defense;Aortic Dissection
ce W.le
The Cleveland Clinic—Chair,Heart and Vascular Institute
None None None None None None
nna M.ewicz
University of TexasSouthwestern Medical
Center—President GeorgeH.W. Bush Chair in
Cardiovascular Medicine;Professor & Director, Division
of Medical Genetics
None None None ● Doris DukeFoundation
● Genetech● National Institutes
of Health● Vivian Smith
Foundation
None None
(Continued)

Ap
CoMe
DaRe
So
JulSh
LarSve
DaWil
mre5%bysig
e127JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
pendix 1. Continued
mmitteember Employment Consultant Speaker
Ownership/Partnership/
Principal Research
Institutional,Organizational or Other
Financial Benefit Expert Witness
vid L.ich
Mount Sinai MedicalCenter—Professor & Chair,
Department ofAnesthesiology
None None None None None None
uvik Sen University of South CarolinaSchool of
Medicine–Professor andChair, Department of
Neurology
● Coaxia● Bristol-Myers Squibb● Pfizer● Sanofi-aventis
● BoehringerIngelheim
None ● American HeartAssociation
● Genetech● Sanofi-aventis
None None
ie A.inn
Stanford University School ofMedicine—CardiovascularClinical Nurse Specialist
None None None None None None
s G.nsson
The ClevelandClinic—Director, The Centerfor Aortic Surgery; Director,
Marfan Syndrome andCollective Tissue Disorder
Clinic
None None None ● EdwardsLifesciences
● Evalve
None None
vid M.liams
University of Michigan HealthSystem—Professor,
Department of Radiology;Director, Interventional
Radiology
● W.L. Gore None None ● W.L. Gore● Medtronic
None ● 2000; Defense;Failure todiagnose andtreat mesentericischemia withaortic dissection
● 2009; Defense;Failure todiagnose andtreat mesentericischemia withaortic dissection
NHLBI indicates National Heart, Lung, and Blood Institute; NIDDK, National Institute of Diabetes and Digestive and Kidney Diseases.This table represents the relevant relationships of committee members with industry and other entities that were reported orally at the initial writing committee
eeting and updated in conjunction with all meetings and conference calls of the writing committee during the document development process. It does not necessarilyflect relationships with industry at the time of publication. A person is deemed to have a significant interest in a business if the interest represents ownership of
or more of the voting stock or share of the business entity, or ownership of $10 000 or more of the fair market value of the business entity; or if funds receivedthe person from the business entity exceed 5% of the person’s gross income for the previous year. A relationship is considered to be modest if it is less thannificant under the preceding definition. Relationships noted in this table are modest unless otherwise noted.
*Significant (greater than $10 000) relationship.
ApGu
PeeRe
AmAlm
RicBe
ChE.
AlbCh
MicDa
AnGo
RoGu
ClifKa
Sco
RicKo
ChMoMa
SteMe
Eri
GeRu
FraRyb
ThoSu
RicWh
JamZid
Wy
JosKo
Em
e128 Hiratzka et al. JACC Vol. 55, No. 14, 20102010 Guidelines on Thoracic Aortic Disease April 6, 2010:e27–129
pendix 2. Reviewer Relationships With Industry and Other Entities—2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVMidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease
rviewer Representation Consultant Speaker
Ownership/Partnership/
Principal Research
Institutional,Organizational or Other
Financial Benefit Expert Witness
jadahameed
Official Reviewer—Societyfor Vascular Medicine
None None None None None None
hard A.rnstein
Official Reviewer—AmericanStroke Association
None None None None None None
ristopherBuller
Official Reviewer—ACCF/AHATask Force Lead Reviewer
None None None None None None
ert T.eung
Official Reviewer—Society ofCardiovascular
Anesthesiologists
● EKR Therapeutics● The Medicines
Company● Neuralstem● Schering Plough
● EKR Therapeutics● The Medicines
Company● PDL Biopharm
None ● The MedicinesCompany*
● Neuralstem*● PDL Biopharm
None None
hael D.ke
Official Reviewer—Society ofInterventional Radiologists
● W.L. Gore*● Medtronic
● Cook None ● Cook● W.L. Gore*● Medtronic
None None
tionette S.mes
Official Reviewer—AHACardiovascular Surgery and
Anesthesia Committee
None None None None None None
bert A.yton
Official Reviewer—ACCFBoard of Trustees
● Medtronic None None None None None
ford J.vinsky
Official Reviewer—Societyfor CardiovascularAngiography and
Interventions
None None None ● Possis Corp. None None
tt Kinlay Official Reviewer—Societyfor Vascular Medicine
None ● Merck● Pfizer
None ● Pfizer None None
hard J.vacs
Official Reviewer—ACCFBoard of Govenors
None None None None None None
ristinerangano
Official Reviewer—Society ofCardiovascular
Anesthesiologists
None None None None None None
ven R.ss|fe
Official Reviewer—AmericanStroke Association
None ● BoehringerIngelheim
None ● American HeartAssociation*
None None
c Roselli Official Reviewer—Society ofThoracic Surgeons
● Medtronic● Vascutek
None None ● Cook None None
off D.bin
Official Reviewer—AmericanCollege of Radiology
● Fovia ● Bracco ● TeraRecon ● Biosense-Webster* None None
nk J.icki
Official Reviewer—AmericanCollege of Radiology
● Bracco● Siemens Medical● Toshiba Medical
Systems*● Vital Images
● Bracco● Siemens Medical● Toshiba Medical
Systems*● Vital Images
● SiemensMedical
● Bracco● Toshiba Medical
Systems*
None None
ralf M.ndt
Official Reviewer—AmericanAssociation for Thoracic
Surgery
None None None ● Bolton Medical ● Atricure● Bolton Medical● Jarvik Heart● Medtronic● Sorin
Group/Carbomedics● St. Jude Medical● Thoratec
Corporation● Ventracor● W.L. Gore
None
hard D.ite
Official Reviewer—AHAPeripheral Vascular Disease
Council
None None None None None None
es P.ar
Official Reviewer—Societyfor CardiovascularAngiography and
Interventions
● Abbott Vascular● Cordis*● Medtronic Vascular
● Abbott Vascular● Cordis*● Medtronic Vascular
None ● Abbott Vascular● Cordis*● Medtronic Vascular
None None
att Decker Organizational Reviewer—American College of
Emergency Physicians
None None None None None None
h M.sowsky
Organizational Reviewer—American College of
Emergency Physicians
None None None None None None
ile Mohler Organizational Reviewer—American College of
Physicians
None None None None None None
(Continued)

Ap
PeeRe
Jam
EdwCh
MaCre
Jos
JohEle
D.Mil
RicNis
PatO’G
Ca
remthun
Ap
AA
Ao
CA
CS
CT
EC
GC
IM
IN
IR
M
M
M
M
PA
SS
SS
ST
TA
TE
TIA
TR
TT
UH
e129JACC Vol. 55, No. 14, 2010 Hiratzka et al.April 6, 2010:e27–129 2010 Guidelines on Thoracic Aortic Disease
pendix 2. Continued
rviewer Representation Consultant Speaker
Ownership/Partnership/
Principal Research
Institutional,Organizational or Other
Financial Benefit Expert Witness
es Burke Content Reviewer—ACCFCatherization Committee
None None None None None None
ard P.en
Content Reviewer None None None None None None
rk A.ager
Content Reviewer—ACCF/AHA Task Force on Practice
Guidelines
None None None None None None
e G. Diez Content Reviewer—ACCFCatherization Committee
● Sanofi-aventis None None None None None
n A.fteriades
Content Reviewer ● Baxter None ● Coolspine ● Celera Diagnostics None ● 2006; Plaintiff;Aortic Dissection*
Craigler
Content Reviewer ● Medtronic ● St. Jude Medical None ● NHLBI● Stanford PARTNER
Trial
khimura
Content Reviewer—ACCF/AHA Task Force on Practice
Guidelines
None None None None None None
rick T.ara
Content Reviewer None None None None None None
rlos Ruiz Content Reviewer—ACCFInterventional Council
None None None None None None
ACCF indicates American College of Cardiology Foundation; AHA, American Heart Association; and NHLBI, National Heart, Lung, and Blood Institute.This table represents the relevant relationships with industry and other entities that were disclosed at the time of peer review. It does not necessarily reflect
lationships with industry at the time of publication. A person is deemed to have a significant interest in a business if the interest represents ownership of 5% orore of the voting stock or share of the business entity, or ownership of $10 000 or more of the fair market value of the business entity; or if funds received bye person from the business entity exceed 5% of the person’s gross income for the previous year. A relationship is considered to be modest if it is less than significantder the preceding definition. Relationships in this table are modest unless otherwise noted. Names are listed in alphabetical order within each category of review.
*Significant (greater than $10 000) relationship.
pendix 3. Abbreviation List
A�abdominal aortic aneurysm
D�aortic dissection
D�coronary artery disease
F�cerebrospinal fluid
�computed tomographic imaging
G�electrocardiogram
A�giant cell arteritis
H�intramural hematoma
R�international normalized ratio
AD�International Registry of Acute Aortic Dissection
EP�motor evoked potential
I�myocardial infarction
MP�matrix metalloproteinase
R�magnetic resonance imaging
U�penetrating atherosclerotic ulcer
EP�somatosensory evoked potentials
FP�steady-state free precession
EMI�ST-elevation myocardial infarction
A�thoracoabdominal aneurysm
E�transesophageal echocardiogram
�transient ischemic attack
A�traumatic rupture of the aorta
E�transthoracic echocardiogram
C�University HealthSystem Consortium


























