Embed Size (px)
Citation preview
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 1
American College of Radiology Annual Progress Report: 2008 Formula Grant Reporting Period July 1, 2011 – June 30, 2012 Formula Grant Overview The American College of Radiology received $2,144,345 in formula funds for the grant award period January 1, 2009 through December 31, 2012. Accomplishments for the reporting period are described below. Research Project 1: Project Title and Purpose Methods and Strategies to Incorporate Radiotherapy Delivery Uncertainties in Clinical Trials Outcome Analysis - Randomized clinical trials provide evidence-based medicine that has become the foundation of radiation oncology. Numerous technologies are being used to deliver targeted radiotherapy. These technologies all have their own operational characteristics and uncertainties. Significant variations also exist in individual implementation of these technologies. These uncertainties may influence, to a critical extent, the outcome of clinical trials. However, they have not been addressed so far in a systematic manner in the outcome analysis. This study aims at bridging this gap with theoretical methodologies for critical assessment and propagation of uncertainties of radiation deliveries as a complement to current clinical trial analysis. Our hypothesis is that by properly accounting for the delivery uncertainties, we will allow better prediction of outcome. Anticipated Duration of Project 1/1/2009 - 12/31/2012 Project Overview The objective of this study is to bridge a gap between present radiotherapy related clinical trials, where essential delivery uncertainties are not included in the outcome analysis, and computational implementation that has the ability to propagate these uncertainties through the analysis process. These methodologies will have the ability to propagate the uncertainties that arise from the treatment unit calibration, throughout the treatment process to the outcome. The quantitative analysis model will employ algorithms that enable self-adaptation, definability, and extendibility. The analysis process can also be reversed to create quality assurance guidance for limiting these uncertainties of radiotherapy delivery. Specifically, the tasks include the following:
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 2
A. To quantify the uncertainties associated with radiation therapy delivery process with accumulated data, which include identification of key components of the process, such as radiation calibration, patient setup, etc., where potential variation can occur, uncertainties associated with each component and the accumulative effect from all. B. To investigate the optimal statistical methods for propagating these uncertainties in outcome analysis modeling. Extensive research has been carried out in the mathematical methods in the uncertainty modeling and the propagation methods. We intend to evaluate the various strategies and algorithms and select the optimum ones that best suit our process. C. To implement these mathematical methods into established biological modeling open source software system available for radiotherapy researchers. Ample considerations will be given for further extension and adaptation of the open software. D. To develop a reverse process that can start from the endpoint of the outcome and predict the limit for uncertainties, thereby offering outcome based quality assurance guidelines for the delivery technologies, benefiting future design of clinical trials. Principal Investigator Ying Xiao, PhD Associate Professor Jefferson Medical College G-321D Bodine Center 111 South 11th Street Philadelphia, PA 19107 Other Participating Researchers Elizabeth O’Meara - employed by American College of Radiology Yan Yu, Adam Dicker, James M. Galvin, DSc - employed by Jefferson Medical College Expected Research Outcomes and Benefits Randomized clinical trials have been the foundation of modern medicine. They are the cornerstone of radiation therapy development. A large portion of recent development of radiotherapy treatment strategies and techniques is the direct or indirect result from these randomized clinical trials. Collection of appropriate data associated with these clinical trials and the analysis of the data with the most accurate and suitable tools are essential elements to the success of these trials. There are uncertainties associated with all the processes of the radiotherapy treatments and data collection. The outcome analysis should consider these uncertainties. Many of these uncertainties are addressed in various ways. Among these, the heterogeneity of reporting has been addressed in guidelines and standards for reporting the results from clinical trials. The uncertainty of radiotherapy delivery, with a disconcerting amount of discrepancies reported from institutions (around 30% failure rate from a radiological physics center head and neck phantom test), is
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 3
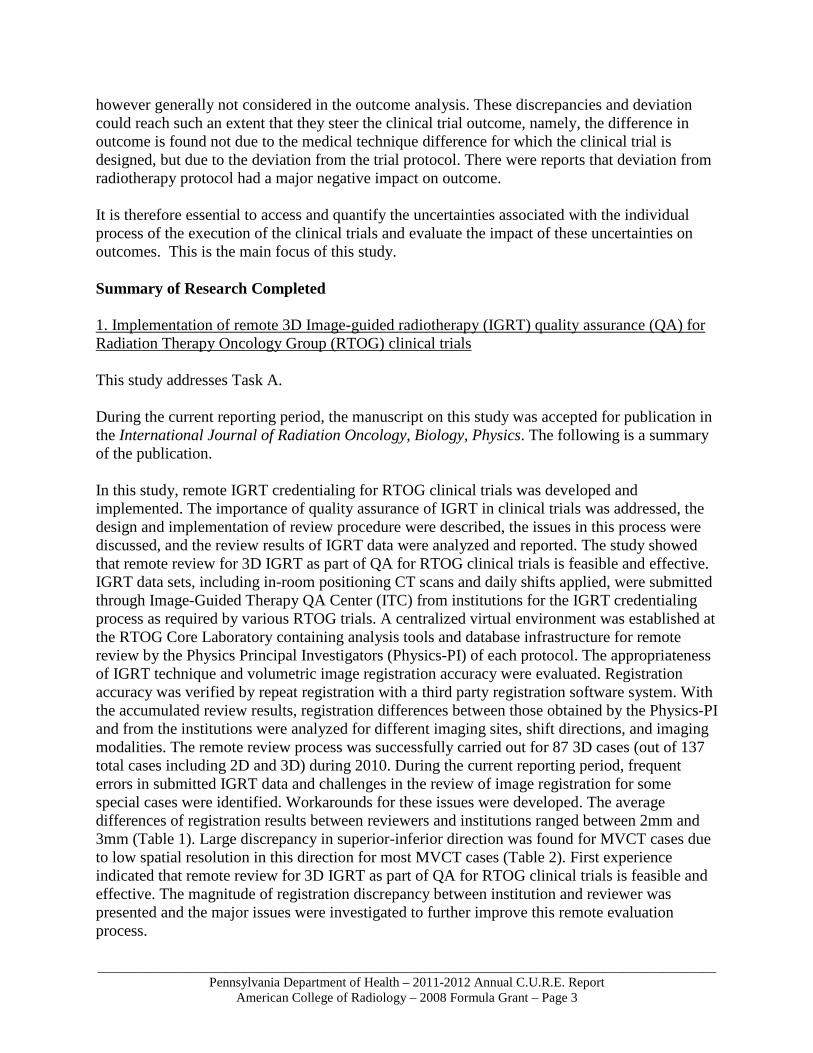
however generally not considered in the outcome analysis. These discrepancies and deviation could reach such an extent that they steer the clinical trial outcome, namely, the difference in outcome is found not due to the medical technique difference for which the clinical trial is designed, but due to the deviation from the trial protocol. There were reports that deviation from radiotherapy protocol had a major negative impact on outcome. It is therefore essential to access and quantify the uncertainties associated with the individual process of the execution of the clinical trials and evaluate the impact of these uncertainties on outcomes. This is the main focus of this study. Summary of Research Completed 1. Implementation of remote 3D Image-guided radiotherapy (IGRT) quality assurance (QA) for Radiation Therapy Oncology Group (RTOG) clinical trials This study addresses Task A. During the current reporting period, the manuscript on this study was accepted for publication in the International Journal of Radiation Oncology, Biology, Physics. The following is a summary of the publication. In this study, remote IGRT credentialing for RTOG clinical trials was developed and implemented. The importance of quality assurance of IGRT in clinical trials was addressed, the design and implementation of review procedure were described, the issues in this process were discussed, and the review results of IGRT data were analyzed and reported. The study showed that remote review for 3D IGRT as part of QA for RTOG clinical trials is feasible and effective. IGRT data sets, including in-room positioning CT scans and daily shifts applied, were submitted through Image-Guided Therapy QA Center (ITC) from institutions for the IGRT credentialing process as required by various RTOG trials. A centralized virtual environment was established at the RTOG Core Laboratory containing analysis tools and database infrastructure for remote review by the Physics Principal Investigators (Physics-PI) of each protocol. The appropriateness of IGRT technique and volumetric image registration accuracy were evaluated. Registration accuracy was verified by repeat registration with a third party registration software system. With the accumulated review results, registration differences between those obtained by the Physics-PI and from the institutions were analyzed for different imaging sites, shift directions, and imaging modalities. The remote review process was successfully carried out for 87 3D cases (out of 137 total cases including 2D and 3D) during 2010. During the current reporting period, frequent errors in submitted IGRT data and challenges in the review of image registration for some special cases were identified. Workarounds for these issues were developed. The average differences of registration results between reviewers and institutions ranged between 2mm and 3mm (Table 1). Large discrepancy in superior-inferior direction was found for MVCT cases due to low spatial resolution in this direction for most MVCT cases (Table 2). First experience indicated that remote review for 3D IGRT as part of QA for RTOG clinical trials is feasible and effective. The magnitude of registration discrepancy between institution and reviewer was presented and the major issues were investigated to further improve this remote evaluation process.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 4
Table 1. Registration differences between institutions and reviewers (for different protocols)
Table 2. Registration differences between institutions and reviewers (for different imaging modalities)
Imaging modality Number of datasets
Absolute value of difference of shifts (mm); mean±SD (range) Left-Right Superior-Inferior Anterior-Posterior
kV CBCT 96 1.7 ± 1.1 (0.0 - 6.7) 1.6 ± 0.9 (0.0 - 6.9) 1.7 ± 1.1 (0.0 - 5.0) MVCT 37 1.5 ± 1.0 (0.1 - 5.1) 3.7 ± 1.7 (0.1 - 8.2) 1.9 ± 0.9 (0.0 - 7.3) Overall 133 1.7 ± 1.0 (0.0 - 6.7) 2.2 ± 1.5 (0.0 - 8.2) 1.8 ± 1.0 (0.0 - 7.3)
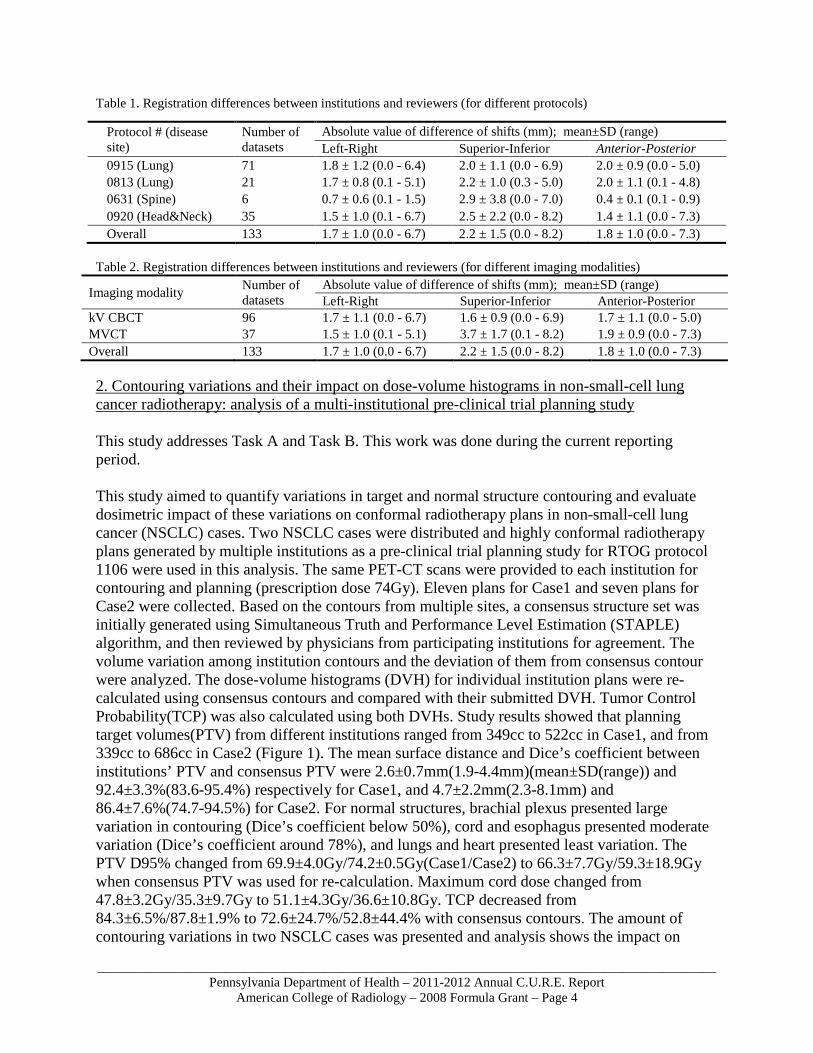
2. Contouring variations and their impact on dose-volume histograms in non-small-cell lung cancer radiotherapy: analysis of a multi-institutional pre-clinical trial planning study This study addresses Task A and Task B. This work was done during the current reporting period. This study aimed to quantify variations in target and normal structure contouring and evaluate dosimetric impact of these variations on conformal radiotherapy plans in non-small-cell lung cancer (NSCLC) cases. Two NSCLC cases were distributed and highly conformal radiotherapy plans generated by multiple institutions as a pre-clinical trial planning study for RTOG protocol 1106 were used in this analysis. The same PET-CT scans were provided to each institution for contouring and planning (prescription dose 74Gy). Eleven plans for Case1 and seven plans for Case2 were collected. Based on the contours from multiple sites, a consensus structure set was initially generated using Simultaneous Truth and Performance Level Estimation (STAPLE) algorithm, and then reviewed by physicians from participating institutions for agreement. The volume variation among institution contours and the deviation of them from consensus contour were analyzed. The dose-volume histograms (DVH) for individual institution plans were re-calculated using consensus contours and compared with their submitted DVH. Tumor Control Probability(TCP) was also calculated using both DVHs. Study results showed that planning target volumes(PTV) from different institutions ranged from 349cc to 522cc in Case1, and from 339cc to 686cc in Case2 (Figure 1). The mean surface distance and Dice’s coefficient between institutions’ PTV and consensus PTV were 2.6±0.7mm(1.9-4.4mm)(mean±SD(range)) and 92.4±3.3%(83.6-95.4%) respectively for Case1, and 4.7±2.2mm(2.3-8.1mm) and 86.4±7.6%(74.7-94.5%) for Case2. For normal structures, brachial plexus presented large variation in contouring (Dice’s coefficient below 50%), cord and esophagus presented moderate variation (Dice’s coefficient around 78%), and lungs and heart presented least variation. The PTV D95% changed from 69.9±4.0Gy/74.2±0.5Gy(Case1/Case2) to 66.3±7.7Gy/59.3±18.9Gy when consensus PTV was used for re-calculation. Maximum cord dose changed from 47.8±3.2Gy/35.3±9.7Gy to 51.1±4.3Gy/36.6±10.8Gy. TCP decreased from 84.3±6.5%/87.8±1.9% to 72.6±24.7%/52.8±44.4% with consensus contours. The amount of contouring variations in two NSCLC cases was presented and analysis shows the impact on
Protocol # (disease site)
Number of datasets
Absolute value of difference of shifts (mm); mean±SD (range) Left-Right Superior-Inferior Anterior-Posterior
0915 (Lung) 71 1.8 ± 1.2 (0.0 - 6.4) 2.0 ± 1.1 (0.0 - 6.9) 2.0 ± 0.9 (0.0 - 5.0) 0813 (Lung) 21 1.7 ± 0.8 (0.1 - 5.1) 2.2 ± 1.0 (0.3 - 5.0) 2.0 ± 1.1 (0.1 - 4.8) 0631 (Spine) 6 0.7 ± 0.6 (0.1 - 1.5) 2.9 ± 3.8 (0.0 - 7.0) 0.4 ± 0.1 (0.1 - 0.9) 0920 (Head&Neck) 35 1.5 ± 1.0 (0.1 - 6.7) 2.5 ± 2.2 (0.0 - 8.2) 1.4 ± 1.1 (0.0 - 7.3) Overall 133 1.7 ± 1.0 (0.0 - 6.7) 2.2 ± 1.5 (0.0 - 8.2) 1.8 ± 1.0 (0.0 - 7.3)
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 5
DVH parameters can be significant. Quality assurance of contouring is essential for successful multi-institutional clinical trials. This work has been presented in oral at the 2012 annual meeting of the American Association of Physicists in Medicine (AAPM).
Fig 1. Gross tumor volume (GTV) contours from different institutions. Red thick line represents the consensus contour. (a) Case1, (b) Case2.
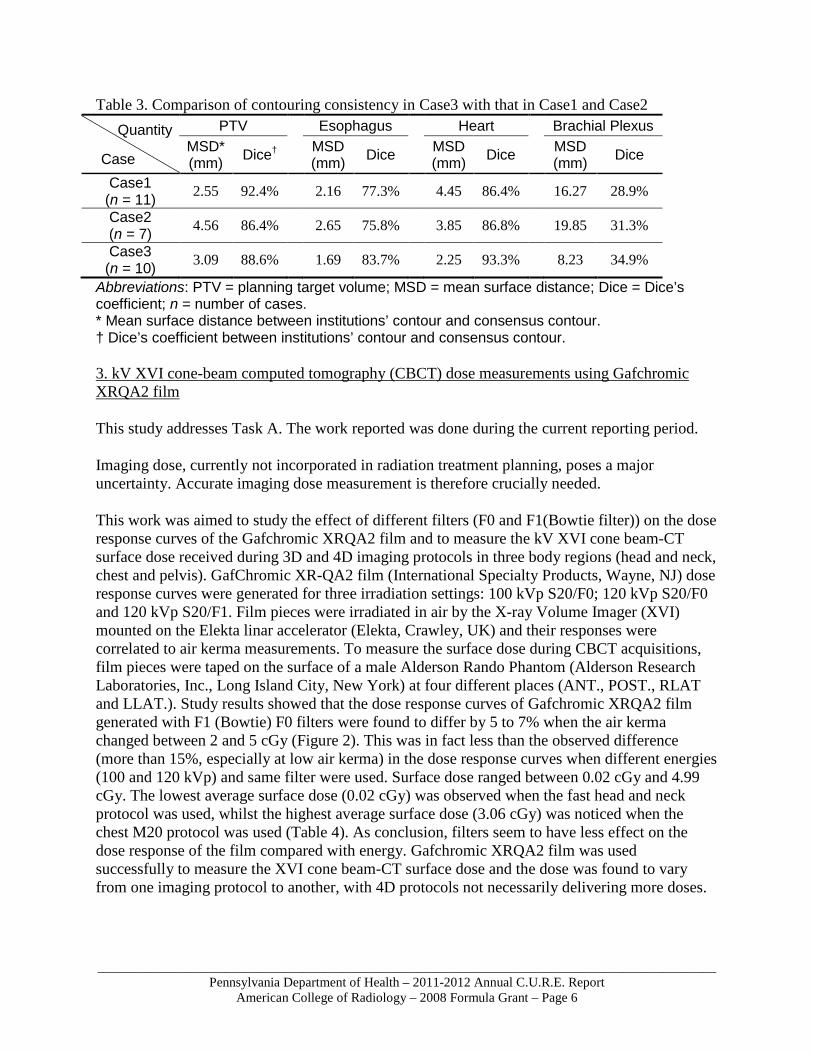
With contouring uncertainties from above study, further work was done to investigate if providing atlas can improve contouring variability in non-small-cell lung cancer radiotherapy. A segmentation atlas was constructed based on the consensus contours for Case1 and Case2, and was made available when the third case (Case3) was distributed for planning. Ten plans were submitted for Case3 and the contouring variability in these plans was compared with that in first two cases. Dice’s coefficient between institution’s contour and consensus contour was used to evaluate the contouring variability. The results are shown in Table 3. The Dice’s coefficient of PTV in Case3 was 88.6%±1.6%, which did not show improvement from Case1 (92.4%±3.3%) and Case2 (86.4%±7.6%). The Dice’s coefficients of esophagus and heart in Case3 significantly improved (t-test, p<0.05) from those in Case1 and Case2. The brachial plexus did not show significant improvement in Dice’s coefficient but the mean surface distance reduced dramatically in Case3. Dice and mean surface distance evaluations for cord were not performed due to different lengths contoured from different institutions. The atlas did not show obvious impact on PTV contouring partially due to the large variation in size, location, and nodal involvement of the target in different cases. Further efforts are needed for target definition consistency.
(a) (b)
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 6
Table 3. Comparison of contouring consistency in Case3 with that in Case1 and Case2 Quantity
Case
PTV Esophagus Heart Brachial Plexus MSD* (mm) Dice†
MSD (mm) Dice MSD
(mm) Dice MSD (mm) Dice
Case1 (n = 11) 2.55 92.4% 2.16 77.3% 4.45 86.4% 16.27 28.9% Case2 (n = 7) 4.56 86.4% 2.65 75.8% 3.85 86.8% 19.85 31.3% Case3
(n = 10) 3.09 88.6% 1.69 83.7% 2.25 93.3% 8.23 34.9%
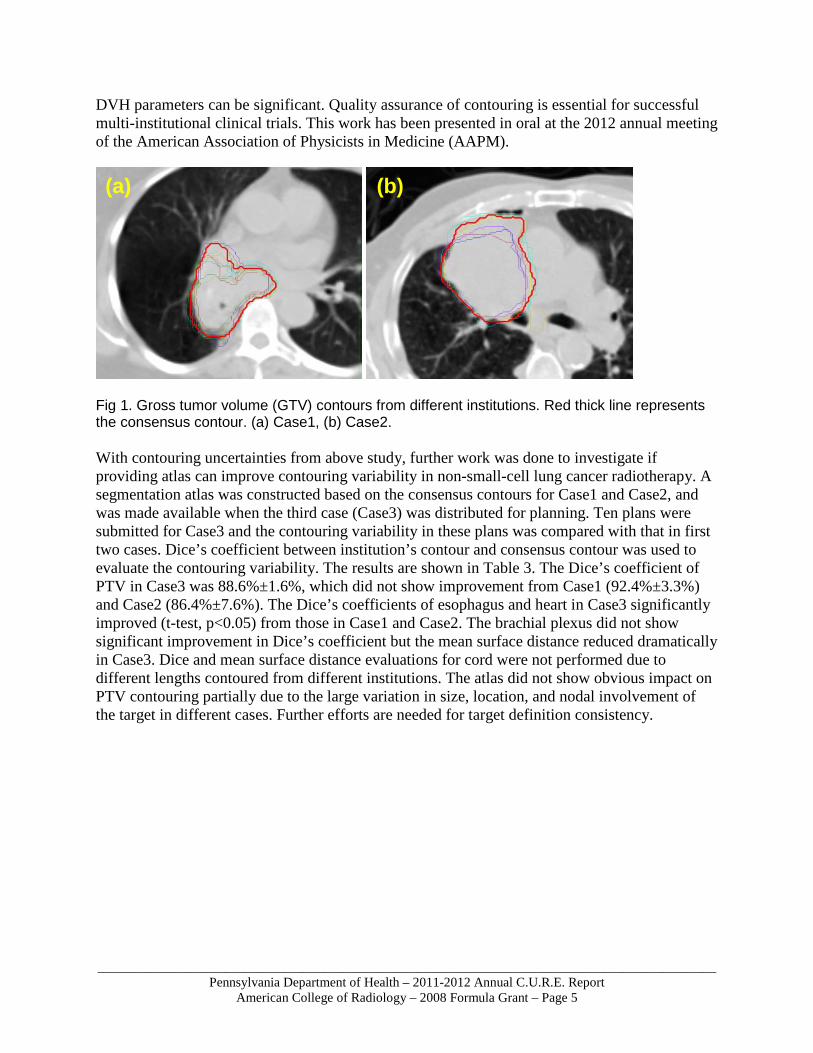
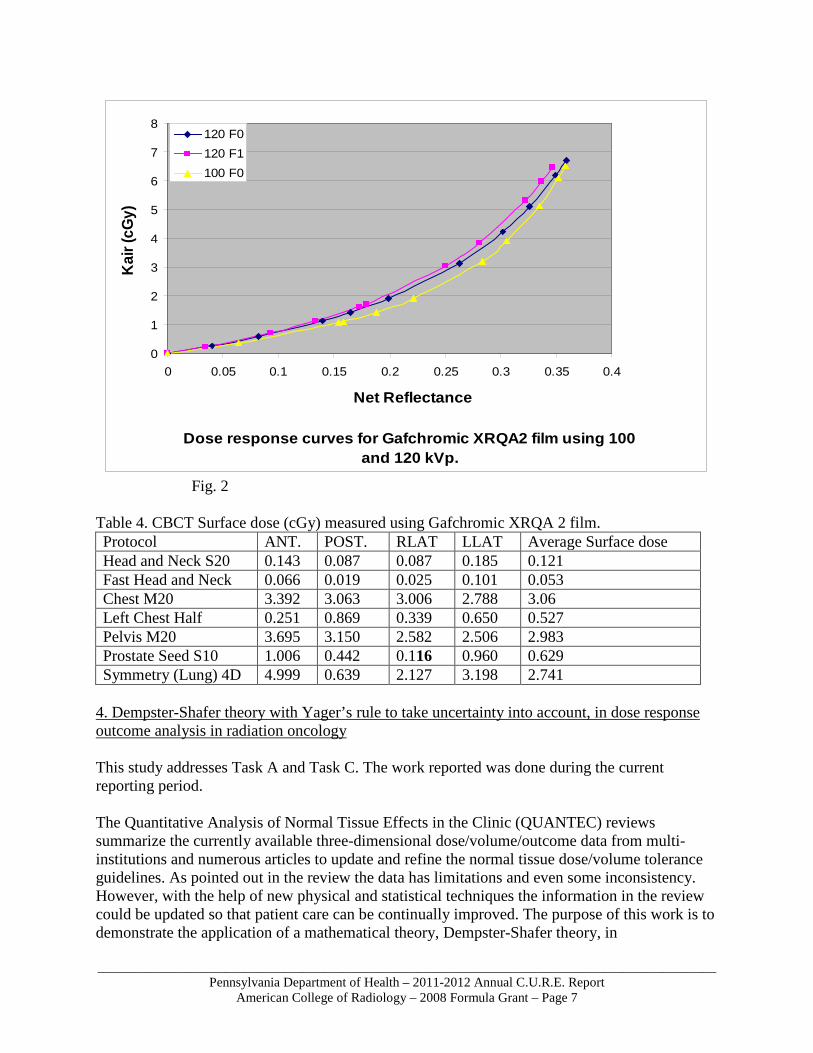
Abbreviations: PTV = planning target volume; MSD = mean surface distance; Dice = Dice’s coefficient; n = number of cases. * Mean surface distance between institutions’ contour and consensus contour. † Dice’s coefficient between institutions’ contour and consensus contour. 3. kV XVI cone-beam computed tomography (CBCT) dose measurements using Gafchromic XRQA2 film This study addresses Task A. The work reported was done during the current reporting period. Imaging dose, currently not incorporated in radiation treatment planning, poses a major uncertainty. Accurate imaging dose measurement is therefore crucially needed. This work was aimed to study the effect of different filters (F0 and F1(Bowtie filter)) on the dose response curves of the Gafchromic XRQA2 film and to measure the kV XVI cone beam-CT surface dose received during 3D and 4D imaging protocols in three body regions (head and neck, chest and pelvis). GafChromic XR-QA2 film (International Specialty Products, Wayne, NJ) dose response curves were generated for three irradiation settings: 100 kVp S20/F0; 120 kVp S20/F0 and 120 kVp S20/F1. Film pieces were irradiated in air by the X-ray Volume Imager (XVI) mounted on the Elekta linar accelerator (Elekta, Crawley, UK) and their responses were correlated to air kerma measurements. To measure the surface dose during CBCT acquisitions, film pieces were taped on the surface of a male Alderson Rando Phantom (Alderson Research Laboratories, Inc., Long Island City, New York) at four different places (ANT., POST., RLAT and LLAT.). Study results showed that the dose response curves of Gafchromic XRQA2 film generated with F1 (Bowtie) F0 filters were found to differ by 5 to 7% when the air kerma changed between 2 and 5 cGy (Figure 2). This was in fact less than the observed difference (more than 15%, especially at low air kerma) in the dose response curves when different energies (100 and 120 kVp) and same filter were used. Surface dose ranged between 0.02 cGy and 4.99 cGy. The lowest average surface dose (0.02 cGy) was observed when the fast head and neck protocol was used, whilst the highest average surface dose (3.06 cGy) was noticed when the chest M20 protocol was used (Table 4). As conclusion, filters seem to have less effect on the dose response of the film compared with energy. Gafchromic XRQA2 film was used successfully to measure the XVI cone beam-CT surface dose and the dose was found to vary from one imaging protocol to another, with 4D protocols not necessarily delivering more doses.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 7
Fig. 2 Table 4. CBCT Surface dose (cGy) measured using Gafchromic XRQA 2 film. Protocol ANT. POST. RLAT LLAT Average Surface dose Head and Neck S20 0.143 0.087 0.087 0.185 0.121 Fast Head and Neck 0.066 0.019 0.025 0.101 0.053 Chest M20 3.392 3.063 3.006 2.788 3.06 Left Chest Half 0.251 0.869 0.339 0.650 0.527 Pelvis M20 3.695 3.150 2.582 2.506 2.983 Prostate Seed S10 1.006 0.442 0.116 0.960 0.629 Symmetry (Lung) 4D 4.999 0.639 2.127 3.198 2.741
4. Dempster-Shafer theory with Yager’s rule to take uncertainty into account, in dose response outcome analysis in radiation oncology This study addresses Task A and Task C. The work reported was done during the current reporting period. The Quantitative Analysis of Normal Tissue Effects in the Clinic (QUANTEC) reviews summarize the currently available three-dimensional dose/volume/outcome data from multi-institutions and numerous articles to update and refine the normal tissue dose/volume tolerance guidelines. As pointed out in the review the data has limitations and even some inconsistency. However, with the help of new physical and statistical techniques the information in the review could be updated so that patient care can be continually improved. The purpose of this work is to demonstrate the application of a mathematical theory, Dempster-Shafer theory, in
Dose response curves for Gafchromic XRQA2 film using 100 and 120 kVp.
0
1
2
3
4
5
6
7
8
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4
Net Reflectance
Kai
r (cG
y)120 F0120 F1100 F0
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 8
dose/volume/outcome data analysis. We applied this theory to the original data obtained from published clinical studies describing dose response for radiation pneumonitis (RP). Belief and plausibility concepts were introduced for dose response evaluation. We were also able to consider the uncertainty and inconsistency of the data from these studies with Yager’s combination rule, a special methodology of Dempster-Shafer theory, to fuse the data at several specific doses. The values of belief and plausibility functions were obtained at the corresponding doses. Then we applied the Lyman-Kutcher-Burman (LKB) model to fit these values and a belief-plausibility range was obtained. This range could be considered as a probability range to assist physicians and treatment planners in determining acceptable dose-volume constraints. Finally, the parameters obtained from the LKB model fitting were compared with those in Emami and Burman’s papers and those from other frequentist statistics methods. We found that Emami and Burman’s parameters are within the probability range we calculated by Dempster-Shafer theory. Table. LKB parameters from Dempster-Shafer theory and other references. TD50 (Gy) ms Belief function's curve 26.75 0.125 Plausibility function's curve 20.87 0.252 Emami and Burman 24.5 0.18 Semenenko et al 2008 29.9 0.41 Mark et al 2010 30.75 --- The manuscript for this study was accepted by Physics in Medicine and Biology - IOPscience. 5. Quantitative evaluation of impact upon tumor control probability (TCP) from quality assurance criteria for non-small cell lung cancer from RTOG 1106 study This study addresses Task B and Task C. The work reported was done during the current reporting period. There are widely accepted heuristic quality assurance (QA) criteria such as percentage variation in dose, distance to agreement (DTA), or a combination of both (Gamma index). For example, for clinical trials credentialing, the Radiological Physics Center (RPC) uses the criteria of 7% dose variation and 4 mm distance to agreement. In this study, we quantitatively evaluated whether even variations considered acceptable by these QA criteria affect tumor control probability (TCP) using the equivalent uniform dose (EUD) based TCP model, which was originally derived from linear-quadratic cell survival model. We also evaluated the impact of variations in contouring between different physicians. We generated a reference plan on a CT data set of locally advanced non-small cell lung cancer used for credentialing on the RTOG 1106 trial, based on a set of contours from one institution. Using this same isodose plan, we calculated dose-volume histograms (DVH) for the PTVs and GTVs drawn by participating physicians from five different institutions, and their corresponding EUDs and TCPs. The EUD was calculated from the cumulative DVH. Although the PTV accounts for mechanical and patients setup uncertainties, the current margins one uses in many protocols are too small to include all possible uncertainties. We rescaled the dose within ±6% and/or shifted the location within ±3mm, meeting the RPC criteria, and evaluated the impact of these changes upon TCP in each case.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 9
The effect of the location shift on TCP is directionally dependent, i.e., different variations of TCP with shifts in lateral, longitudinal and vertical directions, with more variation of TCP with shifts in lateral direction. For GTVs, the TCP values are negatively affected by the location-shifts from 0.72% to 2.15% (1.12%±0.7%); the dose rescales affect the TCP from 5.8% to 9.71%(7.51%±2.08%). For PTVs, the TCP values are dramatically affected by the location-shifts, even within the RPC criteria, i.e. decreasing from 3.63% to 28.21%(20.67%±10.17%); the dose rescales affect the TCP from 8.96% to 17.23%(12.89%±2.77%). In general increasing the prescription dose gives a higher control probability. For instance, 106% of the original dose can increase TCP by 10.18%. However, the effect of location displacement can definitely mitigate this increase if shifts are in the more sensitive direction. For instance, TCP drops 10.21% when the shift is in the negative lateral direction even with 106% of the original dose. Significant TCP variations were observed even from dosimetric variations meeting heuristic QA criteria. The target definition variation between clinicians is still a significant factor. The PTV expansion mitigates the dosimetric variations within QA tolerances. The solutions may be to require more stringent QA criteria and/or take these uncertainties into consideration explicitly in the PTV design. 6. Is Recontouring Organs-At-Risk (OAR) For Adaptive Radiotherapy Plans for Locally Advanced Lung Cancer Necessary? A Pre-Activation Analysis from Radiation Therapy Oncology Group (RTOG) 1106 This study addresses Task B. This work was done during the current reporting period. Adaptive radiotherapy (ART), which involves modifying the radiation plan for the target as it changes during therapy, is being explored for diseases such as lung cancer. Approximations are made in the protocol that organs-at-risk (OARs) remain constant in shape and relative location during ART. In this study, we investigated the accuracy of this assumption, volumetrically and dosimetrically. RTOG 1106 is a randomized Phase II Trial of Individualized Radiotherapy Using During-Treatment FDG-PET/CT (Dur-CT) and Modern Technology in Locally Advanced Non-Small Cell Lung Cancer (NSCLC). In the lead up to the study pre-clinical planning test cases were given to several institutions to study feasibility and consistency in contouring the target and OARs, and to generate treatment plans meeting predefined criteria. After the initial plan of around 50Gy, a “highest achievable dose” adaptive plan was generated using the target defined on CT acquired during the course of the treatment (Dur-CT). Targets are re-defined but not the OARs. In this study, we generated OARs for the adaptive course by deforming OAR contours from the Pre-CT to Dur-CT with visual validation. These contours were then transferred back to Pre-CT for dosimetry assessments. We evaluated dosimetric and volumetric parameters for three major OARs – cord, heart and lung from four institutions between pre-CT and dur-CT. There were significant volumetric variations: for cord, the volume difference ranged from 2.11% to 3.25% (2.51%±0.45%). For heart, it ranged from 25.73% to 28.84% (26.82%±1.34%). For lung, it ranges from 10.5% to 11.9% (11.06%±0.53%). There were also significant dosimetric variations when we applied the adaptive plan to the deformed and non-deformed OARs. For cord, the mean dose percentage change ranged from 16.07% to 19.63% (17.65%±1.53%); for heart, that ranged from 8.62% to
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 10
13.14% (9.78%±2.02%); for lung, that ranged from 8.01% to 11.04% (10.53%±0.44%). For cord, the max dose percentage change ranged from 6.04% to 16.14% (11.39%±3.64%); for heart, that ranged from 0.36% to 3.15% (1.45%±1.08%); for lung, that ranged from 0.59% to 2.86% (1.48%±0.86%). There are significant variations between initial OARs and OARs contoured from subsequent images, resulting in substantial deviations in dosimetry. Therefore, for precise adaptive planning, re-segmentation of OARs on subsequent images is recommended. Deformable registration can be used to facilitate the process. Research Project 2: Project Title and Purpose Development and Analysis of an Infrastructure for Review of Modern Clinical Trials that Include Radiotherapy - Cooperative group protocols have greatly increased in complexity over the past 15 years. At least for the radiotherapy component of these protocols, this dramatic change has created considerable difficulty when reviewing dose distributions to determine whether protocol requirements have been met. Much of the difficulty is due to the time it takes to review advanced technology protocols. This research study is designed to demonstrate that analysis tools are now available that can shorten the time for case review to the extent that accuracy is not lost in a tradeoff with efficiency. This study will also provide information for designing the review tools needed for future cooperative group protocols that might include one or more advanced technologies such as IMRT, IGRT, SBRT, 4D respiratory control, or deformable image registration using PET and/or MRI. Anticipated Duration of Project 1/1/2009 - 12/31/2012 Project Overview The Radiation Therapy Oncology Group (RTOG) has, over the past years, gathered state-of-the-art equipment that allows detailed review of radiotherapy dose distributions. However, during a similar time period, there has been a tremendous increase in both the complexity of dose distributions and the overall amount of data that must be analyzed to determine if protocol requirements have been met. These changes place considerable stress on the protocol Principal Investigators (PIs) to review submissions in a timely manner. This research project will compare 2D review techniques (i.e., sequential 2D cross-sectional review to accomplish 3D analysis) used for older 3D-CRT protocols with newer methodologies that allow multi-planar (e.g., coronal, sagittal, and cross-sectional) review of advanced technology protocols. Advanced technology protocols are studies that include Stereotactic Body Radiation Therapy (SBRT) treatments that use a large number of beam directions to achieve highly conformal dose distributions, dose-painting methodologies that include Intensity Modulated Radiation Therapy (IMRT), Image Guided Radiation Therapy (IGRT), 4D Respiration Controlled treatment, and the use of deformable fusion. The comparison will be accomplished by simply comparing the average review time for protocols that use the Advanced Technology Consortium (ATC) remote review tool (called QuASA2R for Quality Assurance Submission, Archive, Analysis, and Review System) to the average review time for protocols that use more versatile tools that potentially shorten the review time. Another possible limitation in the ability of PIs to rapidly review large

_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 11
numbers of submitted cases is the firewalls that are established by most institutions to protect information. This is the case for both the American College of Radiology (ACR) and the Image-Guided Therapy QA Center (ITC), the institutions holding the data for the RTOG. Such firewalls hamper the ability of a PI to review cases at will, and it is common practice to instead place data in a secure area for a limited amount of time at the request of the PI. Improvements in the area of data dissemination for review purposes will be investigated as part of this research. Principal Investigator Elizabeth O’Meara, BS, CCRP, ARRT (R), (T) Director, RT Quality Assurance & Core Lab Operations American College of Radiology 1818 Market Street, Suite 1600, Philadelphia, PA 19103 Other Participating Researchers Ying Xiao, PhD, James Galvin, DSc – employed by American College of Radiology Expected Research Outcomes and Benefits Many recent advanced technology treatment modalities have matured to the point where they are being used as part of large Phase III studies that are aimed at accruing in excess of 1,000 patients. Additionally, some studies use more than one advanced technology. For example, there is currently at least one Phase III trial that allows both IMRT and IGRT. The incorporation of these and other advanced technologies in large Phase III studies makes the research described here extremely important. As the number of cases requiring review increases dramatically, there is the possibility that the quality of review could be compromised. In order to avoid a decrease in the level of review for a particular study, it is necessary to improve the efficiency of the review process while maintaining quality. This is the aim of the research plan described here. One way of accomplishing this goal is to identify and implement more efficient case review tools. Another way is to create a case review environment that optimizes the use of existing equipment. In addition, remote review capabilities can be improved to allow for situations where it is not possible for one or more individuals to be involved in a central review process. Thus, this research will study the case review process with the goal of implementing and testing the improvements needed to meet the demands of the cooperative group protocols that utilize advanced technologies. Summary of Research Completed 1. Establishing the CAT network at RTOG - A rapid learning community The study described here provides a feasible solution to the data sharing issues between institutions and organizations who work on data analysis. Firewalls and political barriers that prevent institutions to share data with another party hampers the ability of a PI to review cases at will and hinders data analysis to be done. The strategy of CAT network overcame this issue and also demonstrated a good example of gathering and analyzing data on the effectiveness tool.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 12
In detail, a rapid learning health care system has been proposed to supplement or even drive clinical trials in personalised medicine. In such a system, routine clinical data is used to extract and continuously update knowledge. But the sharing of routine clinical data is hampered by political, administrative and ethical barriers. In this study we aimed to describe a rapid learning community that has overcome these barriers and shares routine patient data. We hypothesize that the knowledge extracted from this community is better than knowledge extracted from individual institutes. In detail, a rapid learning community was formed based on the Computer Assisted Theragnostics (CAT) system. This system meets three high level requirements: a) individual patient data never leaves the hospital, b) analysis comes to the data, is transparent and is statistical in nature, and c) full semantic interoperability is achieved for all patients with limited resources. The CAT system was used to learn a prediction model for two-year survival of head and neck cancer patients treated with radiation therapy. We compared learning the model in individual institutes to community learning, in which the model was learned in a distributed manner in data from two community members. The CAT system was reviewed and approved by seven institutes and review boards from five countries (Netherlands, Belgium, Italy, Germany and USA). As a result, community learning led to a prediction model that performed markedly and significantly better than a model based on learning the model from data from individual institutes (Table 1). In conclusion, a rapid learning community is feasible when it is supported by a system that addresses administrative, ethical and political barriers to sharing data. Such a community can be used to extract knowledge which is more accurate than the knowledge gained by individual centres. Table 1. Area-Under the Curve (AUC) discriminatory performance for models learned at MAASTRO (MMAASTRO), RTOG (MRTOG) and in both (MCOMMUNITY).
MMAASTRO MRTOG MCOMMUNITY Validated in MAASTRO 0.68* (0.62-0.74) 0.62* (0.56-0.68) 0.68* (0.62-0.74) Validated in RTOG 0.62* (0.56-0.68) 0.68* (0.62-0.74) 0.68* (0.62-0.74) Validated in COMMUNITY 0.64* (0.58-0.70) 0.64* (0.58-0.70) 0.68* (0.62-0.74)
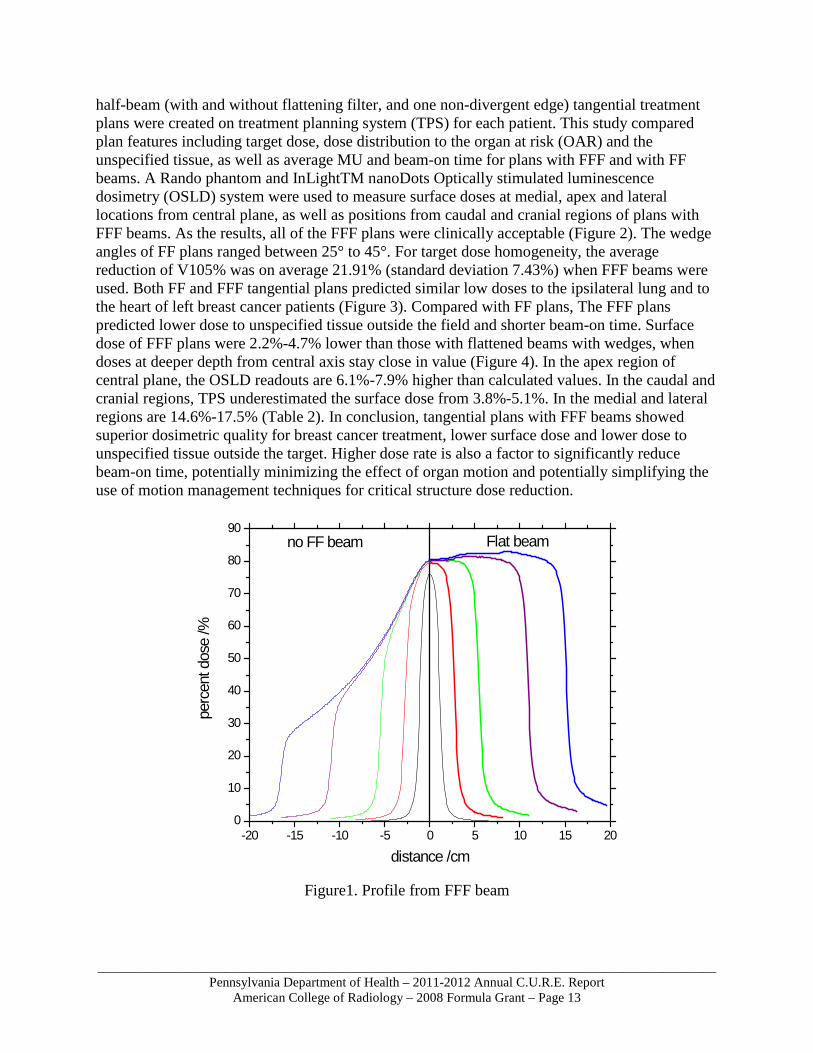
* different from random; (confidence interval) determined by bootstrapping. 2. Equip Core Lab with tools for latest technology and apply these tools for technology analysis - a planning study and surface dose verification for breast tangential treatment plan using flattening filter free beams This research study relates to the goal of implementing and testing the improvements needed to meet the demands of the cooperative group protocols that utilize advanced technologies. The latest flattening filter free beams were modelled in the treatment planning system in the Core Lab to provide a tool to review and analyze cases planed with this new technology. It relates to our strategic plan of gathering and analyzing data on the effectiveness of tools for case review. The study was aimed to evaluate the feasibility of using flattening filter free (FFF) beams (Figure 1) for tangential supine whole breast radiotherapy and to describe the dosimetric characteristics for supine whole breast tangential-field treatment plans using flattening filter (FF) beams with dynamic wedges. The study also performed surface dose measurements for FFF beams. In detail, supine breast cancer plans of ten patients were analyzed for the feasibility planning study. Two
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 13
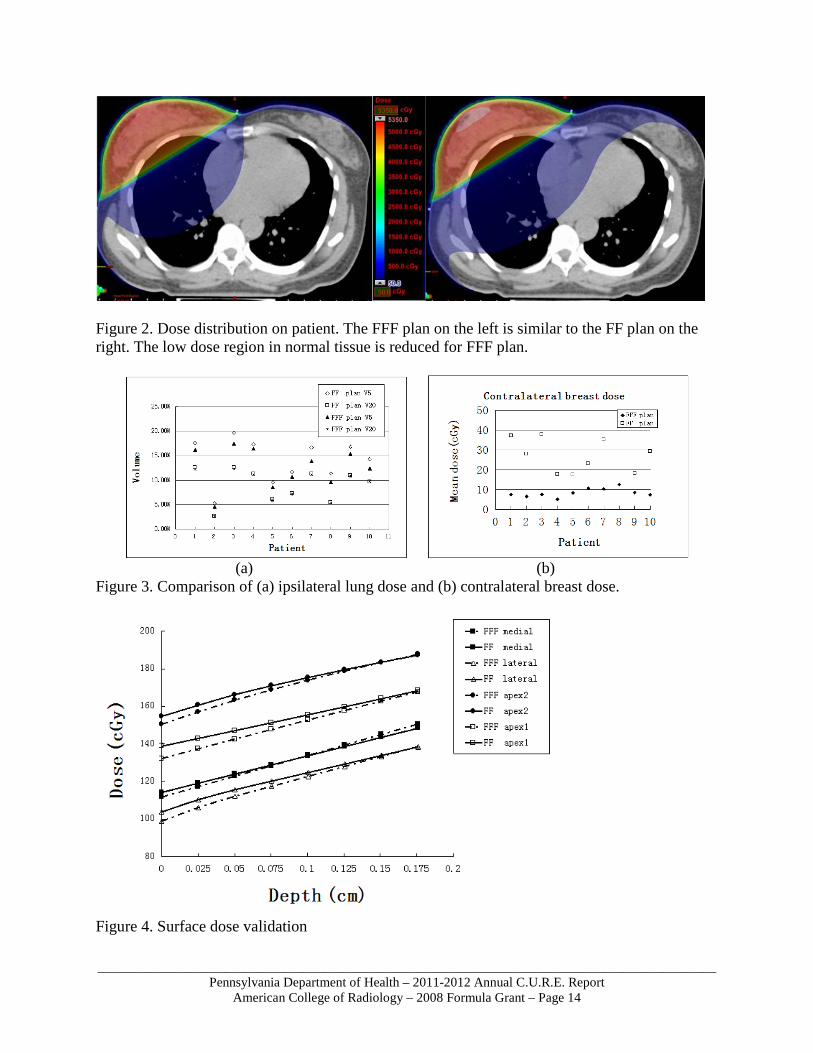
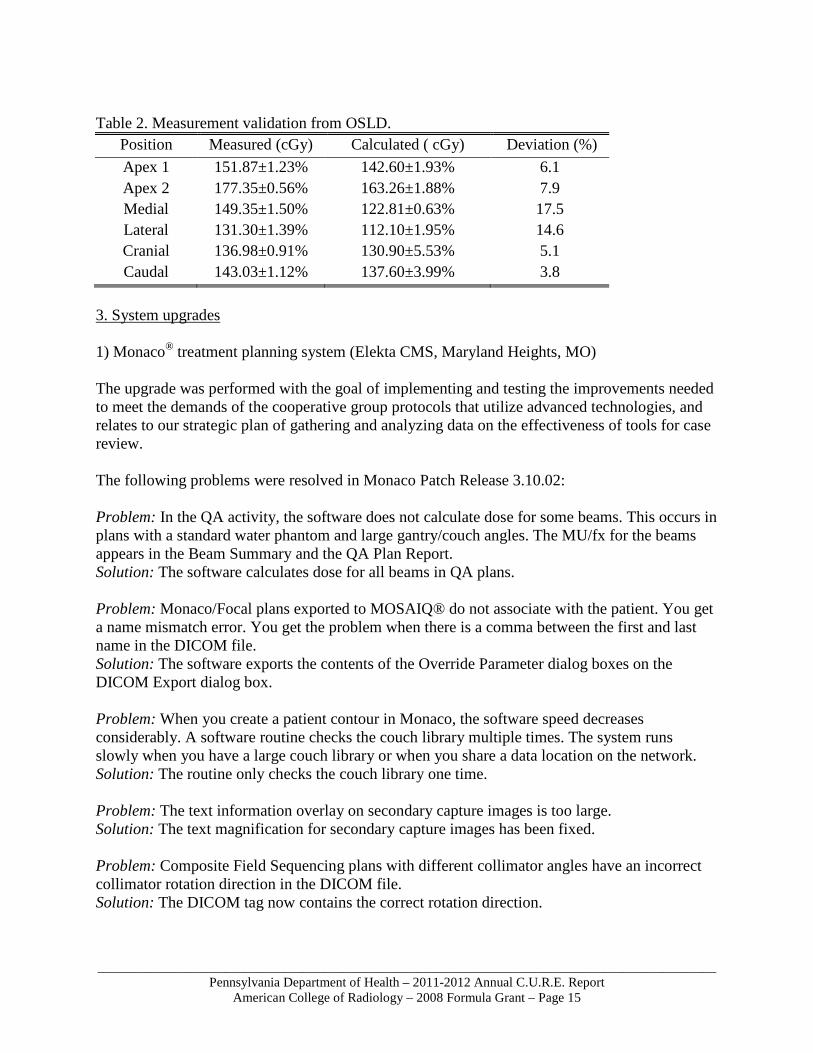
half-beam (with and without flattening filter, and one non-divergent edge) tangential treatment plans were created on treatment planning system (TPS) for each patient. This study compared plan features including target dose, dose distribution to the organ at risk (OAR) and the unspecified tissue, as well as average MU and beam-on time for plans with FFF and with FF beams. A Rando phantom and InLightTM nanoDots Optically stimulated luminescence dosimetry (OSLD) system were used to measure surface doses at medial, apex and lateral locations from central plane, as well as positions from caudal and cranial regions of plans with FFF beams. As the results, all of the FFF plans were clinically acceptable (Figure 2). The wedge angles of FF plans ranged between 25° to 45°. For target dose homogeneity, the average reduction of V105% was on average 21.91% (standard deviation 7.43%) when FFF beams were used. Both FF and FFF tangential plans predicted similar low doses to the ipsilateral lung and to the heart of left breast cancer patients (Figure 3). Compared with FF plans, The FFF plans predicted lower dose to unspecified tissue outside the field and shorter beam-on time. Surface dose of FFF plans were 2.2%-4.7% lower than those with flattened beams with wedges, when doses at deeper depth from central axis stay close in value (Figure 4). In the apex region of central plane, the OSLD readouts are 6.1%-7.9% higher than calculated values. In the caudal and cranial regions, TPS underestimated the surface dose from 3.8%-5.1%. In the medial and lateral regions are 14.6%-17.5% (Table 2). In conclusion, tangential plans with FFF beams showed superior dosimetric quality for breast cancer treatment, lower surface dose and lower dose to unspecified tissue outside the target. Higher dose rate is also a factor to significantly reduce beam-on time, potentially minimizing the effect of organ motion and potentially simplifying the use of motion management techniques for critical structure dose reduction.
-20 -15 -10 -5 0 5 10 15 200
10
20
30
40
50
60
70
80
90
perc
ent d
ose
/%
distance /cm
Flat beamno FF beam
Figure1. Profile from FFF beam
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 14
Figure 2. Dose distribution on patient. The FFF plan on the left is similar to the FF plan on the right. The low dose region in normal tissue is reduced for FFF plan.
(a) (b) Figure 3. Comparison of (a) ipsilateral lung dose and (b) contralateral breast dose.
Figure 4. Surface dose validation
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 15
Table 2. Measurement validation from OSLD.
Position Measured (cGy) Calculated ( cGy) Deviation (%) Apex 1 151.87±1.23% 142.60±1.93% 6.1 Apex 2 177.35±0.56% 163.26±1.88% 7.9 Medial 149.35±1.50% 122.81±0.63% 17.5 Lateral 131.30±1.39% 112.10±1.95% 14.6 Cranial 136.98±0.91% 130.90±5.53% 5.1 Caudal 143.03±1.12% 137.60±3.99% 3.8
3. System upgrades 1) Monaco® treatment planning system (Elekta CMS, Maryland Heights, MO) The upgrade was performed with the goal of implementing and testing the improvements needed to meet the demands of the cooperative group protocols that utilize advanced technologies, and relates to our strategic plan of gathering and analyzing data on the effectiveness of tools for case review. The following problems were resolved in Monaco Patch Release 3.10.02: Problem: In the QA activity, the software does not calculate dose for some beams. This occurs in plans with a standard water phantom and large gantry/couch angles. The MU/fx for the beams appears in the Beam Summary and the QA Plan Report. Solution: The software calculates dose for all beams in QA plans. Problem: Monaco/Focal plans exported to MOSAIQ® do not associate with the patient. You get a name mismatch error. You get the problem when there is a comma between the first and last name in the DICOM file. Solution: The software exports the contents of the Override Parameter dialog boxes on the DICOM Export dialog box. Problem: When you create a patient contour in Monaco, the software speed decreases considerably. A software routine checks the couch library multiple times. The system runs slowly when you have a large couch library or when you share a data location on the network. Solution: The routine only checks the couch library one time. Problem: The text information overlay on secondary capture images is too large. Solution: The text magnification for secondary capture images has been fixed. Problem: Composite Field Sequencing plans with different collimator angles have an incorrect collimator rotation direction in the DICOM file. Solution: The DICOM tag now contains the correct rotation direction.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 16
Problem: You can DICOM export plans in dose calculation. The DICOM file for these plans is not deliverable. It contains no segments. Solution: DICOM export is locked until you finish dose calculation. Problem: The Beam Description field on the Plan report is too long. The text goes to a second line. Solution: The text in the Beam Description field will truncate when it reaches the last available character space. Problem: Dynamic Conformal Arc plans violate the Constant MU per degree value. This causes plans to become undeliverable. Solution: Dose calculation has been fixed to make Constant MU per degree beams. Problem: The Default Leaf Insertion value for Elekta and Siemens machines is 0%. Solution: The Default Leaf Insertion value is set at 50%. 2) Oncentra® MasterPlan treatment planning system (Elekta Nucletron, Veenendaal, The Netherlands) The upgrade was performed with the goal of implementing and testing the improvements needed to meet the demands of the cooperative group protocols that utilize advanced technologies, and relates to our strategic plan of gathering and analyzing data on the effectiveness of tools for case review. This software system was upgraded to version 3.3 SP1. New functionality in this version of Oncentra® MasterPlan included:
• Model Based Segmentation (MBS) • Volumetric Modulated Arc Therapy (VMAT) • System Level Improvements • Improvements in Anatomy Modeling (AM) • Improvements in Beam Data Tool (BDT) • Improvements in Beam Modeling and Plan Evaluation (BM/PE) • Improvements in Connectivity Module (CM) • Improvements in Dose Calculation (DC) • Improvements in Documentation • Improvements in Plan Analysis (PA) • Improvements in Volume Rendering (VR)
3) VelocityAI (Velocity Medical Solutions, Atlanta, GA) The upgrade was performed with the goal of implementing and testing the improvements needed to meet the demands of the cooperative group protocols that utilize advanced technologies, and relates to our strategic plan of gathering and analyzing data on the effectiveness of tools for case review.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 17
This software system was upgraded to version 2.6.2. New features in this version of VelocityAI included:
• Viewer Improvements • SUV Calculation • Viewer Integrated Graphs • Histograms Statistics and Evaluation • Volume of Interest Histograms • Plotting Adaptive Histograms • Plotting Histograms of Volume Differences • 2D Plot Assessment • 3D Plot Assessment • Templates and Presets for Histogram Evaluations • Dose Scaling • MR Bias Correction • The Velocity Grid is iPad ready
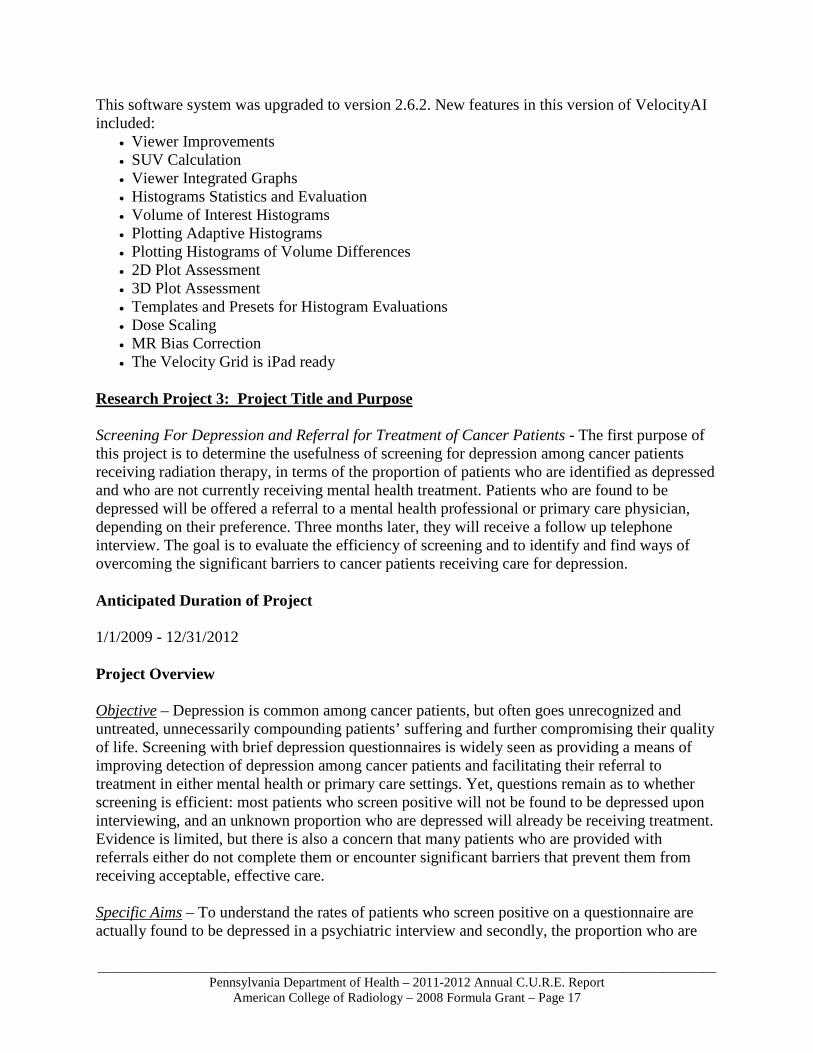
Research Project 3: Project Title and Purpose Screening For Depression and Referral for Treatment of Cancer Patients - The first purpose of this project is to determine the usefulness of screening for depression among cancer patients receiving radiation therapy, in terms of the proportion of patients who are identified as depressed and who are not currently receiving mental health treatment. Patients who are found to be depressed will be offered a referral to a mental health professional or primary care physician, depending on their preference. Three months later, they will receive a follow up telephone interview. The goal is to evaluate the efficiency of screening and to identify and find ways of overcoming the significant barriers to cancer patients receiving care for depression. Anticipated Duration of Project 1/1/2009 - 12/31/2012 Project Overview Objective – Depression is common among cancer patients, but often goes unrecognized and untreated, unnecessarily compounding patients’ suffering and further compromising their quality of life. Screening with brief depression questionnaires is widely seen as providing a means of improving detection of depression among cancer patients and facilitating their referral to treatment in either mental health or primary care settings. Yet, questions remain as to whether screening is efficient: most patients who screen positive will not be found to be depressed upon interviewing, and an unknown proportion who are depressed will already be receiving treatment. Evidence is limited, but there is also a concern that many patients who are provided with referrals either do not complete them or encounter significant barriers that prevent them from receiving acceptable, effective care. Specific Aims – To understand the rates of patients who screen positive on a questionnaire are actually found to be depressed in a psychiatric interview and secondly, the proportion who are
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 18
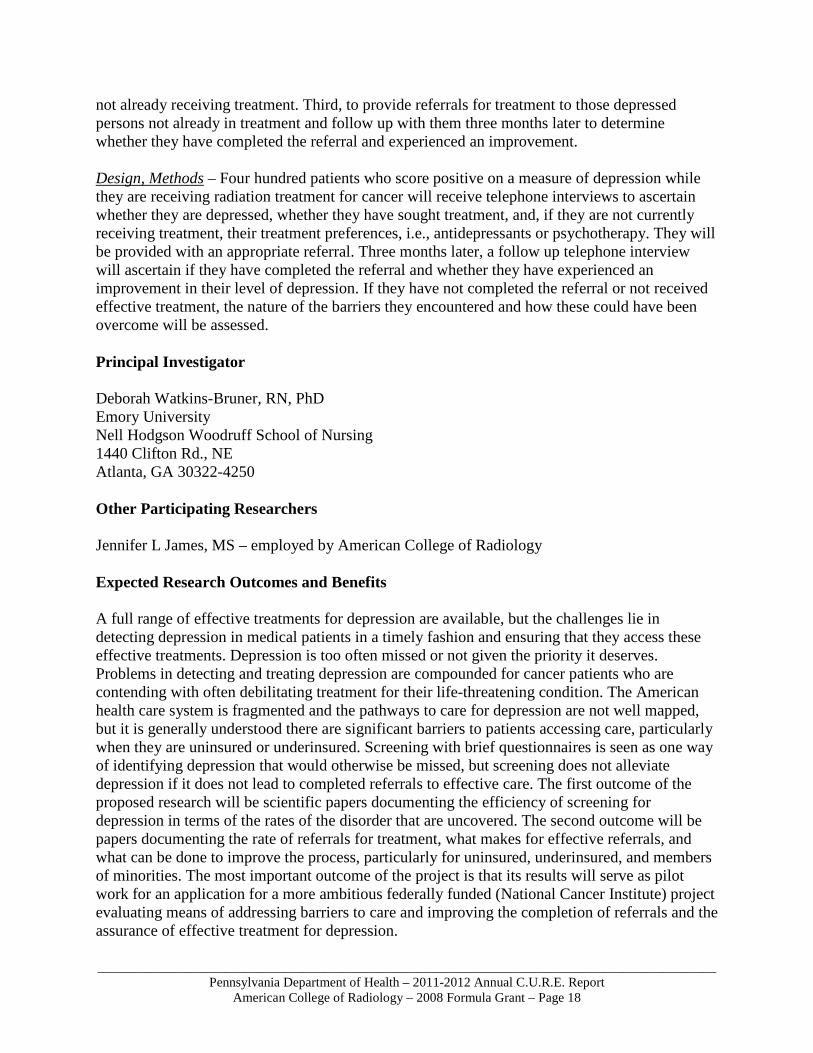
not already receiving treatment. Third, to provide referrals for treatment to those depressed persons not already in treatment and follow up with them three months later to determine whether they have completed the referral and experienced an improvement. Design, Methods – Four hundred patients who score positive on a measure of depression while they are receiving radiation treatment for cancer will receive telephone interviews to ascertain whether they are depressed, whether they have sought treatment, and, if they are not currently receiving treatment, their treatment preferences, i.e., antidepressants or psychotherapy. They will be provided with an appropriate referral. Three months later, a follow up telephone interview will ascertain if they have completed the referral and whether they have experienced an improvement in their level of depression. If they have not completed the referral or not received effective treatment, the nature of the barriers they encountered and how these could have been overcome will be assessed. Principal Investigator Deborah Watkins-Bruner, RN, PhD Emory University Nell Hodgson Woodruff School of Nursing 1440 Clifton Rd., NE Atlanta, GA 30322-4250 Other Participating Researchers Jennifer L James, MS – employed by American College of Radiology Expected Research Outcomes and Benefits A full range of effective treatments for depression are available, but the challenges lie in detecting depression in medical patients in a timely fashion and ensuring that they access these effective treatments. Depression is too often missed or not given the priority it deserves. Problems in detecting and treating depression are compounded for cancer patients who are contending with often debilitating treatment for their life-threatening condition. The American health care system is fragmented and the pathways to care for depression are not well mapped, but it is generally understood there are significant barriers to patients accessing care, particularly when they are uninsured or underinsured. Screening with brief questionnaires is seen as one way of identifying depression that would otherwise be missed, but screening does not alleviate depression if it does not lead to completed referrals to effective care. The first outcome of the proposed research will be scientific papers documenting the efficiency of screening for depression in terms of the rates of the disorder that are uncovered. The second outcome will be papers documenting the rate of referrals for treatment, what makes for effective referrals, and what can be done to improve the process, particularly for uninsured, underinsured, and members of minorities. The most important outcome of the project is that its results will serve as pilot work for an application for a more ambitious federally funded (National Cancer Institute) project evaluating means of addressing barriers to care and improving the completion of referrals and the assurance of effective treatment for depression.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 19
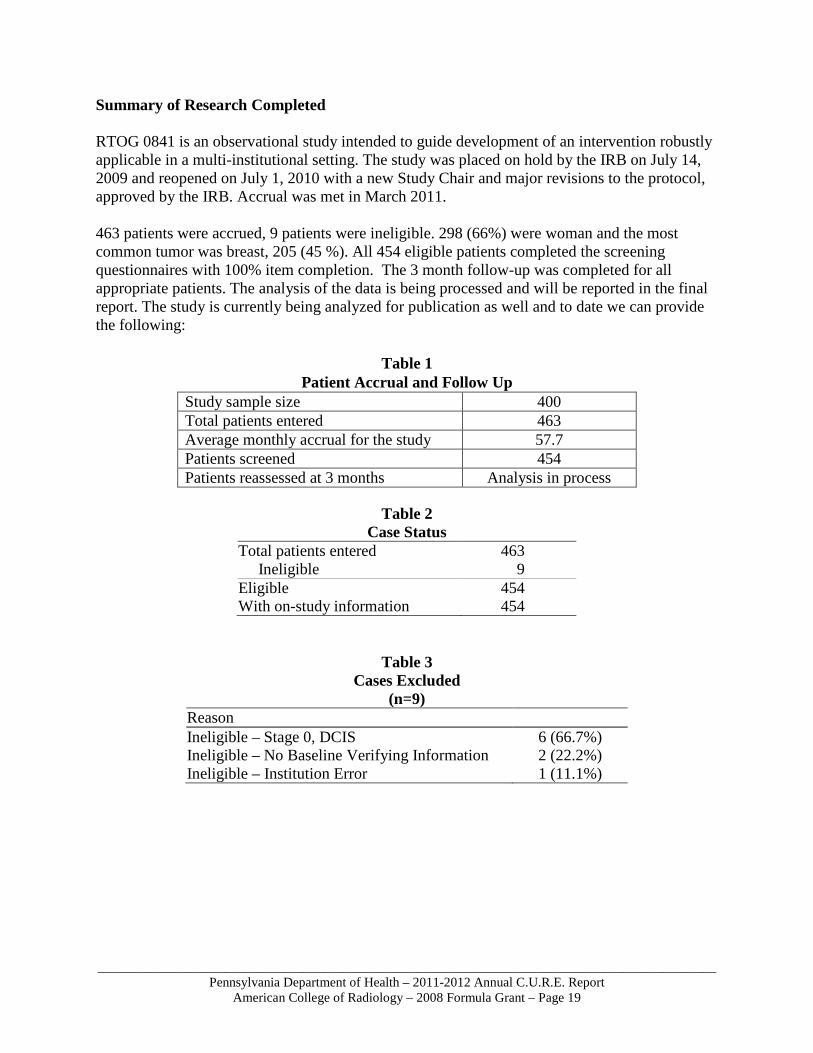
Summary of Research Completed RTOG 0841 is an observational study intended to guide development of an intervention robustly applicable in a multi-institutional setting. The study was placed on hold by the IRB on July 14, 2009 and reopened on July 1, 2010 with a new Study Chair and major revisions to the protocol, approved by the IRB. Accrual was met in March 2011. 463 patients were accrued, 9 patients were ineligible. 298 (66%) were woman and the most common tumor was breast, 205 (45 %). All 454 eligible patients completed the screening questionnaires with 100% item completion. The 3 month follow-up was completed for all appropriate patients. The analysis of the data is being processed and will be reported in the final report. The study is currently being analyzed for publication as well and to date we can provide the following:
Table 1
Patient Accrual and Follow Up Study sample size 400 Total patients entered 463 Average monthly accrual for the study 57.7 Patients screened 454 Patients reassessed at 3 months Analysis in process
Table 2
Case Status Total patients entered 463 Ineligible 9 Eligible 454 With on-study information 454
Table 3 Cases Excluded
(n=9) Reason Ineligible – Stage 0, DCIS 6 (66.7%) Ineligible – No Baseline Verifying Information 2 (22.2%) Ineligible – Institution Error 1 (11.1%)
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 20
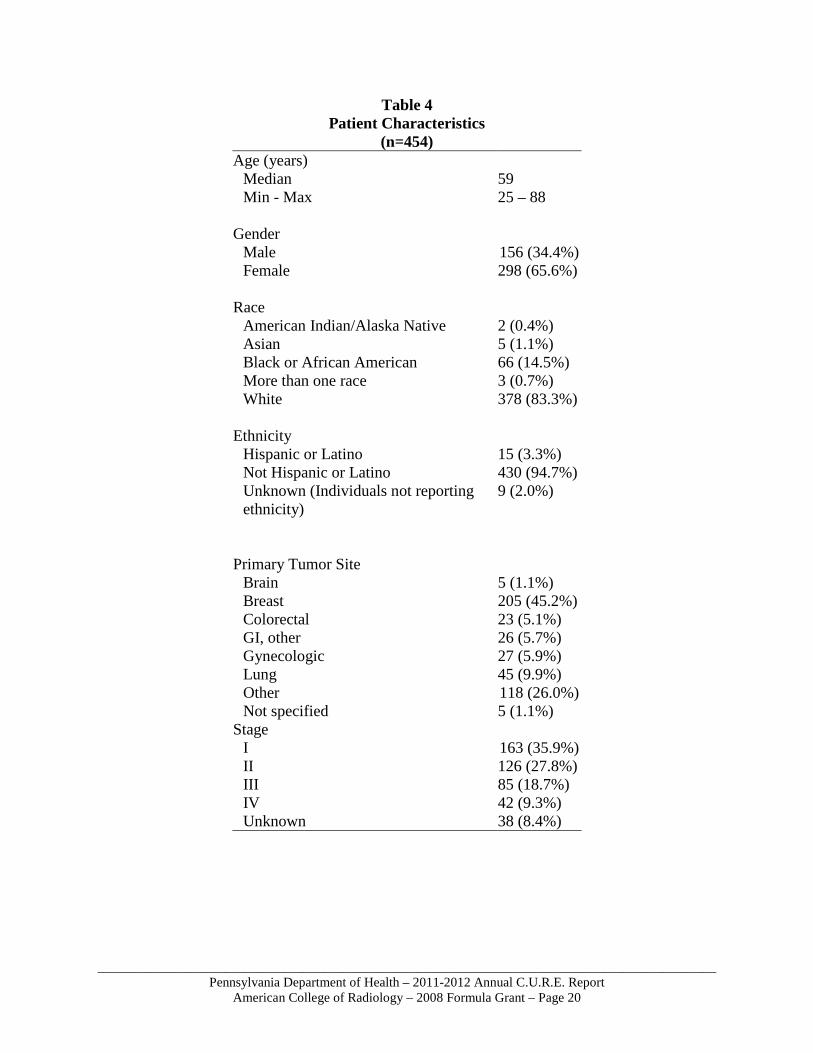
Table 4 Patient Characteristics
(n=454) Age (years)
Median 59 Min - Max 25 – 88
Gender Male 156 (34.4%) Female 298 (65.6%)
Race American Indian/Alaska Native 2 (0.4%) Asian 5 (1.1%) Black or African American 66 (14.5%) More than one race 3 (0.7%) White 378 (83.3%)
Ethnicity
Hispanic or Latino 15 (3.3%) Not Hispanic or Latino 430 (94.7%) Unknown (Individuals not reporting ethnicity)
9 (2.0%)
Primary Tumor Site
Brain 5 (1.1%) Breast 205 (45.2%) Colorectal 23 (5.1%) GI, other 26 (5.7%) Gynecologic 27 (5.9%) Lung 45 (9.9%) Other 118 (26.0%) Not specified 5 (1.1%)
Stage I 163 (35.9%) II 126 (27.8%) III 85 (18.7%) IV 42 (9.3%) Unknown 38 (8.4%)
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 21
Research Project 4: Project Title and Purpose Assessment of Methods to Increase Latino Enrollment into Cancer Clinical Trials - Despite national initiatives to increase the enrollment of racial and ethnic minorities into cancer clinical trials, participation by Latinos remains low. The Radiation Therapy Oncology Group (RTOG), which conducts cancer clinical trials involving radiotherapy, will develop and evaluate evidence-based, cuturally and linguistically appropriate patient education materials and investigator training programs to increase the enrollment of Latinos into cancer clinical trials in Pennsylvania and nationally. We will also use cartographic modeling techniques to do a gap analysis through identification of current RTOG sites and their Latino population density compared to high density areas of Pennsylvania and the United States where we do not have RTOG sites. This will help us strategically identify sites to recruit into the RTOG that will facilitate Latino access to state-of-the-art cancer clinical trials. Anticipated Duration of Project 1/1/2009 - 12/31/2012 Project Overview Research Objectives: 1) The RTOG will develop and evaluate evidence-based, cuturally and linguistically appropriate education and awarness programs and recruitment materials to increase the enrollment of Latinos into cancer clinical trials in Pennsylvania and nationally. We will identify 4 RTOG clinical trials to target and evaluate. 2) We will develop and assess cultural competency training for RTOG investigators and research staff. 3) We will conduct a gap analysis of current RTOG sites with high density Latino populations and areas of the Commonwealth of Pennsylvania and the country with high density populations where we do not have RTOG sites. This will help us strategically identify sites to recruit into the RTOG that will facilitate Latino access to state-of-the-art cancer clinical trials. Methods: 1) In consultation with our RTOG investigators and patient advocates, we will identify four protocols and use certified Spanish translators who will do back-forth translations of the informed consents and the study specific and general clinical trials and radiation therapy patient materials. Materials will be developed by our investigators and our in house marketing staff with input from patient advocates. 2) RTOG will develop a Latino Cultural Competency and Recruitment Training Program for physicians and clinical research associates (CRAs) who have primary contact with cancer patients and are located at facilities in geographic regions with Latino populations. The training program will instruct the caregivers in the barriers, myths, beliefs, and norms within the Latino culture that may impede clinical trial enrollment and provide strategies for overcoming these barriers. Video recordings of the training sessions will be made available for subsequent reinforcement of course material and for physicians and CRAs unable to attend in person. An interactive program with role playing will be used in the training sessions. Culturally appropriate Spanish language patient information brochures, posters, and Spanish translations of patient consent forms for RTOG’s larger randomized trials will be developed and provided to enrolling facilities. Pre and post knowledge tests will assess effectiveness of the training in enhancing cultural competence. 3) We will use cartographic
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 22
modeling techniques to do a gap analysis to assist with the identification of current RTOG sites with high density Latino populations and areas of Pennsylvania and the country with high density populations where we do not have RTOG sites. Principal Investigator Deborah Watkins-Bruner, RN, PhD Emory University Nell Hodgson Woodruff School of Nursing 1440 Clifton Rd., NE Atlanta, GA 30322-4250 Other Participating Researchers Jennifer James, MS, Sharon Hartson Stine, BA – employed by American College of Radiology Expected Research Outcomes and Benefits This research is designed to address the underrepresentation of Latinos in cancer clinical trials. The primary outcome will be a 10% increase in Latino recruitment by year 3 but we will continue to evaluate recruitment annually past the end of this study. We need to recognize the multifactorial nature of barriers to minority recruitment and that this study is only the beginning of testing evidence-based methods to begin to improve recruitment. Improvements are expected to be incremental with identification of evidence-based methods that show increased awareness, informed consent and accrual to research. RTOG will leverage this funding to continue to support the methods that show efficacy in increasing Latino recruitment. Increased minority recruitment to clinical trials provides the ability to generalize results to the Latino population which is the fastest growing minority in Pennsylvania and the United States. These strategies also enhance social justice by facilitating Latino access to state-of-the-art cancer clinical trials. Summary of Research Completed Recruitment for this study continued via the RTOG website until May 2012. Enrollment concluded with 66 patients that completed baseline and 42 that completed follow-up. The data is in analysis to provide pilot data for a funding application. Aim #3 - Cartographic modeling was utilized to identify current RTOG sites with high density African American populations and areas of Pennsylvania and the country with high density populations where we do not have RTOG sites.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 23
Research Project 5: Project Title and Purpose Emerging Imaging Technology Clinical Trials in PA: Reproducibility and Responsiveness of MRI Measures of Body Composition and Lipid Metabolism in Women with Gestational Diabetes The purpose of the multi-site Pennsylvania study is to evaluate the reproducibility and responsiveness of MRI measures of maternal body composition and lipid metabolism in the assessment of gestational diabetes. The MRI measures to be evaluated are associated with problems and diseases related to processing of blood sugar and obesity. Summary of Research Completed This project was deleted. No health research grant funds were spent on this project. Research Project 6: Project Title and Purpose Remote Review of Quality of Radiation Treatment for Lung Cancer: A Pilot Project - Definitive radiotherapy is the standard therapeutic approach for inoperable lung cancer. However, this treatment can potentially result in fatal treatment complications. The purpose of this pilot project
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 24
is to develop methods of collecting clinical data directly from distinct electronic medical record systems at a variety of radiotherapy facilities to assess quality of treatment delivery in lung cancer. The clinical data will be standardized and aggregated in a central database from which queries will be performed to retrieve critical data. The methods developed will assure secure transfer, review, and analysis in compliance with regulatory requirements. The overall goal will be to scale this approach for automated collection of quality of care data across multiple institutions to analyze and improve radiation treatment delivery for lung cancer patients. Duration of Project 1/1/2009 – 3/30/2012 Project Overview The hypothesis: Despite significant barriers to full interoperability, it will be possible to demonstrate remote secure access to Radiation Oncology Electronic Medical Records, to remotely retrieve clinically significant quality of care data on lung cancer patients, to remotely aggregate these at a central secure super server, and conduct initial analyses of these quality data to evaluate quality of Radiation Oncology delivered. Specific Aims include demonstrating the feasibility of collecting and aggregating in a central database established quality parameters for workup and radiation treatment of lung cancer from multiple institutions with different Electronic Medical Records (EMR) systems, validating the de-identification engine and confirming secure HIPAA compliant internet-based data transfer and software interoperability, performing data extractions on the aggregated data and analyzing quality parameters, and demonstrating compliance with the larger connectivity goals of the NCI Ca-BIG in clinical Radiation Oncology. The investigators will develop a core data set description to implement parallel processes and systems for radiation oncology facilities using the two different EMR systems. To facilitate the study and re-use of these data, the repository will follow and model the principles of the cancer Biomedical Informatics Grid (caBIG) and its related technologies, including the consistent definition and translation of data elements to NCI-defined ontologies and taxonomies. Where ontologies and taxonomies are undefined by caBIG (e.g., for radiotherapy delivery data), the researchers will cooperate with the vendors and standards bodies to define structure and vocabulary that will facilitate research against the unified database. In the current project, another process will be required wherein a data upload from each vendor system to a super-server will result in an aggregate of combined datasets. A requirement of this process will be that data from each vendor's dataset will be mapped and/or converted to standard caBIG-compliant data elements. In addition, software tools will be required to assure data quality and integrity, to provide data quality reports back to each of the vendors, and to provide outcome and analysis reports to Quality Research in Radiation Oncology (QRRO).
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 25
Principal Investigator Jean Owen, PhD Senior Director American College of Radiology 1818 Market St. 16th Floor Philadelphia, PA 19103 Other Participating Researchers Philip M. Devlin, MD, FACR – employed by Harvard Medical School Ramesh Rengan, MD, PhD – employed by University of Pennsylvania Joel Goldwein, MD – employed by Elekta AB Christopher Rose, MD, Eliot Levitt – employed by Vantage Oncology, Los Angeles, CA Expected Research Outcomes and Benefits At the present time, only 3% of all patients with a diagnosis of malignancy are enrolled into clinical trials. The therapeutic outcome data for the remaining 97% of patients is usually not collected and is rarely put to rigorous data analysis to identify predictors of outcome. One approach to overcome this obstacle is to aggregate and query data from multiple treatment sites so a more robust analysis on the larger patient population can be performed. We propose in this project to develop an approach to standardize and aggregate data at a remote site on lung cancer patients at multiple institutions receiving radiation treatment. The radiotherapeutic management of lung cancer is a rapidly evolving field with newly validated quality measures that correlate with likelihood of cure as well as toxicity. This approach could then be used to identify new measures of treatment outcome and quality of radiation treatment delivery. The ability to analyze larger, aggregated data on lung cancer patients would allow for identification of critical treatment parameters that would not be apparent on analysis of smaller subsets of patients. This will allow comprehensive assessment of quality of care during treatment and for recent time periods. Patients will benefit from a more timely quality of care assessment system. The long-term goal of this project would be to improve the baseline standard of radiotherapeutic treatment of lung cancer patients. Summary of Research Completed This project was proposed as a pilot project with a budget of approximately $35,000 and was intended to be complementary to other planned projects within the organization. It was planned to use the voluntary efforts of several experts from outside of Pennsylvania who were interested in related planned projects. Because these other projects have been delayed beyond our original expectations, it has not been possible to mobilize the voluntary resources to fulfill the plans for this project. Therefore this project received approval from the PA DOH to end. No grant funds were spent on this project.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 26
Research Project 7: Project Title and Purpose Quantitative Imaging Biomarker Tools – The purpose of this study is to evaluate, develop, unify, and evaluate standards-based tools that are used to collect, record, and analyze quantitative imaging data in order to discover imaging biomarkers for more accurate analysis of image results collected in clinical trials. The critical barriers being addressed by our study are that at present, the assessment of cancer treatment response based on image assessment is cumbersome, with poor tools for measuring and capturing vital image metadata required for this assessment. Our outcome will bridge these barriers and advance the field by improving the efficiency of response assessment evaluation on images. Anticipated Duration of Project 10/15/2010 – 12/31/2012 Project Overview Our objective is to develop and unify standards-based tools for collecting, recording, and analyzing quantitative imaging data for discovering and using imaging biomarkers for more accurate analysis of image results collected in clinical trials. The hypothesis is that by unifying the currently fragmented set of tools for quantitative image analysis, the evaluations researchers conduct will be more efficient and accurate. We will accomplish our objectives by pursuing the following specific research aims:
• Compile and refine tools enabling automated extraction of quantitative imaging biomarkers.
• Develop a standards-based software platform to unify quantitative imaging tools for efficient
image evaluation and data interoperability. • Assess our platform in a study requiring evaluation of quantitative imaging data.
Principal Investigator Mitchell Schnall, MD, PhD Professor of Radiology University of Pennsylvania Dept. of Radiology Hospital of the University of Pennsylvania 3400 Spruce St. Philadelphia, PA 19104 Other Participating Researchers Daniel Rubin, MD – employed by Stanford University Mehdi Adineh, PhD MD – employed by American College of Radiology Mark Rosen, MD, PhD – employed by University of Pennsylvania Constantine Gatsonis, PhD – employed by Brown University
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 27
Expected Research Outcomes and Benefits Our ultimate goal by developing these tools is to facilitate assessment of treatment response and clinical decision-making in cancer. Our unified tools will enable cancer researchers to validate and standardize methodologies and to share imaging data and related imaging meta-data for quantitative measurements of responses to cancer therapies. Our work will enable oncologists to make better treatment choices for their cancer patients – a potential benefit to over 1.4 million patients with new cancers annually. Summary of Research Completed We summarize our progress to date according to each of our three originally-proposed specific aims. 1. Compile and refine tools enabling automated extraction of quantitative imaging biomarkers.
We created an inventory of the major available quantitative imaging tools available and in use in the ACRIN core laboratory. We considered and reviewed the currently available tools used by the ACRIN Core Lab and determined refinements or extensions needed for their current functionality to provide the following essential capabilities for analyzing quantitative imaging data in the Core Lab. A report will be included as an Appendix in the final report; it addresses:
(1) Automated segmentation of tumors to enable reproducible measurement of lesions. (2) Extraction of quantitative features in images obtained from modalities such as: CT
for RECIST evaluations and Positron emission tomography (PET) (3) Unambiguous identification of target lesions and automated tracking of them on
images across various time points.
We found that no tools currently available provide open programming interfaces permitting us to extend the tools to provide these capabilities. Most notably, two areas of rigorous focus in the Core Lab center around quantitative analysis for PET imaging via Standardized Uptake Value (SUV), and 2D analysis for Response Evaluation Criteria in Solid Tumors (RECIST). While the lab is tooled with workstations specific to these analytic areas, they lack both a fundamental standardized structure for sharing analytic outputs, as well as the ability to capture semantic or descriptive language regarding disease presentation. We therefore decided to extend the open source tooling recently developed called the image physician annotation device (iPAD) to provide these capabilities in the form of a Web-based application called ePAD (see Specific Aim 2 for progress on this task). In order to keep the implementation tractable, we focused on RECIST analysis, as our needs assessment confirmed its use most critical in the ACRIN Core Lab, and because the software engineering task for other implementations proved to be substantial. RECIST provides standardized guidelines for solid tumor measurements and assessment of therapeutic tumor response. As such, RECIST is commonly used in phase II and phase III adult and pediatric cancer clinical trials.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 28
2. Develop a standards-based software platform to unify quantitative imaging tools for efficient
image evaluation and data interoperability. One challenge we identified as we compiled the requirements for efficient collection of quantitative imaging data (Aim 1) is the need to support multiple readers (radiologists) reviewing the same image studies. The readers should be using the same tools and record the image analysis results in a standardized manner to ensure effective data aggregation and analysis for the current clinical study. These readers could be at different institutions, and shipping and setting up an application for quantitative imaging analysis was impractical as it typically requires dedicated computer/server space and time to install and setup in a consistent manner at every institute. We thus decided to focus our development on an existing effort at Stanford University called ePAD (electronic physician annotation device), a Web-based software tool for quantitative image analysis which can be run anywhere and that was a re-implementation of the iPAD tool in Osirix (an open-source image viewer that is primarily used with Macintosh operating systems). To date, we have made substantial progress extending the ePAD tool. ePAD now integrates various basic quantitative imaging functions needed to support RECIST assessment, permitting an efficient workflow for evaluating image data in a variety of clinical trials. We are also able to support multi-reader evaluation at multiple different sites without having to bring all the readers to ACRIN headquarters. The platform stores all quantitative image data according to the National Cancer Institute’s caBIG® Annotation and Image Markup (AIM) standards for interoperability, as was our goal in the proposed work. RECIST assessments include serial (typically about 4) tumor evaluations, performed at protocol-specified time points, while patients are undergoing cancer treatment. Specific features of the current implementation of ePAD for fulfilling the RECIST assessment are:
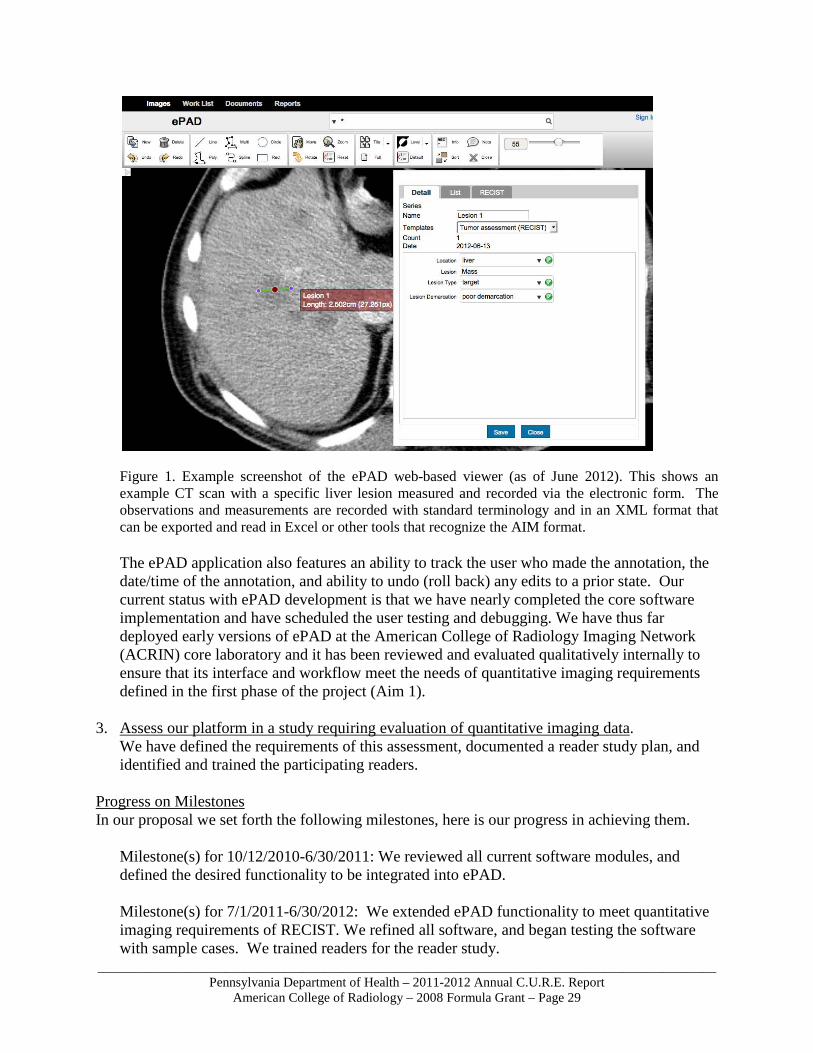
a) A web-based image viewer that permits the user to browse images, with proper login credentials, across the Internet (see Figure 1.). Users do not need to download applications to their desktop and the image studies do not have to be locally downloaded and stored to be able to view and make measurements via the web-based program.
b) Ability to make lesion measurements and designate them by name and classify them by lesion type (target, non-target, new lesion, resolved lesion; see Figure 1.).
c) A database of image annotations that is used to generate tabular summary of all target lesions, the tumor burden (via automated calculation of sum of linear dimension of target lesions), and the response rate (automated calculate of response change) and the response category.
d) An automatically-generated therapy response summary graph.
_____________________________________________________________________________________________Pennsylvania Department of Health – 2011-2012 Annual C.U.R.E. Report
American College of Radiology – 2008 Formula Grant – Page 29
Figure 1. Example screenshot of the ePAD web-based viewer (as of June 2012). This shows an example CT scan with a specific liver lesion measured and recorded via the electronic form. The observations and measurements are recorded with standard terminology and in an XML format that can be exported and read in Excel or other tools that recognize the AIM format. The ePAD application also features an ability to track the user who made the annotation, the date/time of the annotation, and ability to undo (roll back) any edits to a prior state. Our current status with ePAD development is that we have nearly completed the core software implementation and have scheduled the user testing and debugging. We have thus far deployed early versions of ePAD at the American College of Radiology Imaging Network (ACRIN) core laboratory and it has been reviewed and evaluated qualitatively internally to ensure that its interface and workflow meet the needs of quantitative imaging requirements defined in the first phase of the project (Aim 1).
3. Assess our platform in a study requiring evaluation of quantitative imaging data.
We have defined the requirements of this assessment, documented a reader study plan, and identified and trained the participating readers.
Progress on Milestones In our proposal we set forth the following milestones, here is our progress in achieving them.
Milestone(s) for 10/12/2010-6/30/2011: We reviewed all current software modules, and defined the desired functionality to be integrated into ePAD. Milestone(s) for 7/1/2011-6/30/2012: We extended ePAD functionality to meet quantitative imaging requirements of RECIST. We refined all software, and began testing the software with sample cases. We trained readers for the reader study.