2007 FDA drug approvals: a year of fluxSpecialty products dominate innovative drug approvals — a trend that looks set to continue.
Bethan HughesThe US FDA approved 17 new molecular entities
(NMEs) and2 biologic license applications (BLAs) in 2007 (TABLE 1;
FIG. 1), the lowest number recorded since 1983.Unsurprisingly, one
factor to which the scarcity of approvals has been attributed by
some is an increased level of regulatory caution in the wake of
high-profile safety issues, such as those for Avandia
(rosiglitazone; GlaxoSmithKline) last year. It does appear that the
agencyis changing how it assesses benefits and risks when it
approves new products. It is extremely concerning to us if the
outcome of this effortis a slow down in drug approvals,says Sara
Radcliffe, Vice President for Science and Regulatory Affairs at the
Biotechnology Industry Organization. But it is statistically
difficult to identify a trend, she adds.Alternatively, as the FDA
has reportedly countered, it could be that their expectations have
not increased, but rather that they have simply become better at
identifying potential risks, and that not only have the number of
applications decreased, they are also not good enough.Unless you go
through piece by piece to compare packages, which is not easy to
do, it is hard to see who is correct. It appears that the bar is
being raised a bit, and maybe that is necessary, says
Christopher-Paul Milne, Associate Director of the Tufts Center for
the Study of Drug Development, USA. From a public health
standpoint, the FDA is leaning towards asking for more information
rather than allowing the product on the market and dealing with any
problems as they arise.Specialty trend continuesAccording to Milne,
another reason why the FDA wants to see more information is often
because less scientific and medical literature is available for
novel drugs. In newer fields the FDA wants to see more [data]
because their familiarity is less. It makes the FDA cautious about
what they are willing to approve.However, a new drug that addresses
an unmet medical need may tip the riskbenefit balance towards
approval, suggests Milne. When you are dealing with[an indication]
for which there are very few, or no, treatmentsyou can perhaps
accept that more risk can be borne than you would have in any other
situation because the benefits are greater.Nine out of the 17 NMEs
and 2 BLAs approved in 2007 received priority review status, a
designation given to drugs that are considered to offer major
advances in treatment, or provide a treatment for which no adequate
therapy exists (TABLE 1).This reflects an ongoing trend, says
Senior Research Analyst Eric Schmidt of Cowen and Company, USA.
Drugs that meet unmet medical needs such as Soliris for PNH
[paroxysmal nocturnal haemoglobinuria] and Kuvan for PKU
[phenylketonuria] are the ones getting through. Michael Hay Senior
Analyst and Project Manager of BioMedTracker, Sagient Research, USA
also observes that more infectious disease and oncology therapies
are being approved because from the riskbenefit profile, you can
tolerate more risk. Indeed, 2007 saw the approval of the first new
types of oral anti-HIV drugs in a decade: the CCR5 antagonist
Selzentry (maraviroc; Pfizer) and the HIV-1 integrase inhibitor
Isentress (raltegravir; Merck), for the treatment of HIV-1. Also, 4
out of the 17 NMEs in 2007 were indicated for the treatment of
cancer, one of which was designated as an orphan drug, Torisel
(temsirolimus; Wyeth), for the treatment of advanced renal cell
carcinoma.Regulatory setbacksLast year also saw a number of
high-profile regulatory delays. Perhaps the most prominent was
Provenge (Sipuleucel-T; Dendreon), a pioneering prostate cancer
vaccine. In May 2007, the FDA asked for more data about the
effectiveness, chemistry and manufacturing of the vaccine, even
though an FDA advisory committee had voted in favour of its
efficacy and safety in March. Analysts expect more data in 2008,
but while they are waiting, it seems likely that the US Congress
will investigate why the FDA chose not to follow the advisory
committees recommendations to approve Provenge (Nature Biotech. 1,
1; 2008).Two major drugs that analysts had previously expected to
be launched in 2007, Acomplia (rimonabant; SanofiAventis) for
obesity and Galvus (vildagliptin; Novartis) for type 2 diabetes,
also remain unapproved by the FDA. Innovative Medicines Initiative
formally adopted p110AstraZeneca sues over generic Crestor
p112Stephen Friend discusses Mercks approach to anticancer R&D
p114Strategies for anti-angiogenesis drugs p115First integrase
inhibitor approved for treating HIV p1172007 FDA drug approvals: a
year of fluxSpecialty products dominate innovative drug approvals a
trend that looks set to continue.Its a period of flux in getting
from A to B.NATURE REVIEWS |
DRUGDISCOVERYVOLUME7|FEBRUARY2008|107NEWS & ANALYSIS 2008
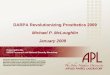
Nature Publishing Group Nature Reviews | Drug DiscoveryNumber of
drugs approved6050403010201996 1997 1998 1999 2000 2001 2002 2003
2004 2005 2006 200705336 7303935273 252417 17213118 182425 6 7New
Molecular EntitiesBiologic License ApplicationsFollowing a negative
FDA advisory committee vote in June that raised concerns about
central nervous system side effects, SanofiAventis decided to
withdraw its rimonabant new drug application (NDA) and plans to
resubmit the file to the FDA in the future. The vildagliptin NDA
remains filed, but at the approvable stage, after the FDA requested
more clinical trial data to demonstrate safety and efficacy in
specific patient groups with renal impairment. Both drugs were
approved in the EU last year.Apart from safety concerns, changes to
FDA internal processes may have also affected approvables this year
as recent draft guidelines for developing antibacterials were cited
as a reason for the antibiotic dalbavancin (Pfizer) receiving an
approvable letter in December 2007. This may also have affected
Theravances telavancin. The FDA is at a crossroads as per the
advice from some of its panels, with them moving the goal posts on
the companies for indication-specific guideline changes, says
Schmidt.Another reason thought to influence whether a drug is
considered approvable rather than granted approval is the increased
FDA workload. We looked at the report to Congress from fiscal year
2006, released in August 2007, and every metric of workload the
FDAs review staff has responsibility for is up considerably, says
Hay (http://www.fda.gov/ope/pdufa/report2006/PDUFA2006perf.pdf).
These findings are mirrored in a recent FDA subcommittee report
that found that demands on the FDA have increased dramatically
without resources increasing proportionally
(http://www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4329b_02_00_index.html).Delays
and failuresWhatever the reasons are for delaying approvals,
according to Sagient Research the number of approvable letters as a
percentage of all FDA decisions made has increased from 20% in 2006
to 28% in 2007 (FDA Approval Study, 2008. BioMedTracker, Sagient
Research Systems). Hay thinks that this increase also reflects
insufficient communication between the FDA and companies, which
could result in poor application packages. The issues being raised
by some of the approvable letters should have been addressed during
the first review process, he says.Most of the 3-month delays
occurred in biotech, says Stefan Ryser, Founding Partner of Bear
Stearns Health Innoventures, USA.By looking at approvals and
regulatory setbacks over the past 2 calendar years, Elizabeth
Czerepak and Stefan Ryser have observed that three-quarters of the
products with 3-month delays were from biotech companies (Nature
Rev. Drug Discov.; in the press). Interestingly, over the same time
period, they also identified that products originating from the
biotech industry accounted for approximately two-thirds of all
approved new drug applications, but also for more than 90% of Phase
III failures.In keeping with this second observation is the fact
that pharma achieved more NME and BLA approvals than biotech in
2007 (TABLE 1). So, combining biotechs talent for innovation with
pharmas experience of the drug approval process through development
alliances may help increase the number of approvals over time. Its
the best of both worlds, says Ryser.Meanwhile, to mitigate the risk
and high R&D costs of developing novel agents, both
pharmaceutical and biotech companies are reformulating, generating
line extensions and looking for new indications for existing
products. Forecasted revenues for these strategies help to explain
why this makes good business sense. For example, Novartis Exforge
(amlodipine and valsartan) is forecast to have revenues above
US$600 million in the seven major markets (France, Germany, Italy,
Spain, UK, Japan and US) by 2012 according to Alistair Sinclair and
Tijana Ignjatovic, Senior Analysts at Datamonitor Europe,
headquartered in the UK.Financial timesAmong the NMEs or BLAs
anticipated to be the most commercially successful of those
approved in 2007 are Letairis (ambrisentan; Gilead), for the
treatment of pulmonary arterial hypertension, and Isentress for the
treatment of HIV-1. Letairis has sales forecast above $400 million
in the seven major markets by 2012 according to Datamonitor, and
Isentress has sales forecast above $500 million by 2010, with the
possibility of sales rising to $1 billion if the drug achieves
first-line approval (see page 117). Of the drugs currently in
late-stage development, analysts will be closely watching Amgens
denosumab for the treatment of osteoporosis and metastatic bone
disease, for which key clinical data is due out in the second half
of this year. It is make or break for Amgen because of the problems
with their EPO [erythropoietin] franchise, says Hay.In terms of
market share in 2008, Datamonitor expects oncology,
immunology/inflammation and infectious diseases to increase the
most, whereas cardiovascular, gastroenterology and respiratory are
predicted to decrease owing to major patent expiries.By dividing
agents into four categories small molecules, therapeutic proteins,
monoclonal antibodies (mAbs) and vaccines Datamonitor has predicted
that mAbsand vaccines will see a 25% rise in revenuesin 2008
compared with 2007, from$29.5 billion to $36.8 billion (across the
top50 companies in the seven major markets).In particular,
Datamonitor identify Roche/Genentechs Avastin, Herceptin and
Rituxan as the products that will drive an increase of revenues
derived from mAbs from a 6% market share in 2007 to 11% in 2012.
These forecasts also reflect mergers and acquisitions, in-licensing
and alliances activity last year with pharma investing heavily in
both ready-made biologics and platform technologies.A time of
changeThroughout 2008, analysts expect to see a continuation of
pharmabiotech deals to help expand pipelines, particularly in the
biologics arena. Some analysts say that figures already suggest
that there will be more NDAs in 2008; however, as it is election
year in the USA and with drug developers unsure as to how the
recently passed FDA Amendments Act 2007 will affect FDA
requirements, it is too early to predict.Figure 1 | FDA drug
approvals. New molecular entities and biologic license applications
approved by the US FDA by year.NEWS&ANALYSI S108
|FEBRUARY2008|VOLUME7www.nature.com/reviews/drugdisc 2008 Nature
Publishing Group Table 1 | New molecular entities and biologics
approved by the US FDA in 2007Generic name(Trade name)Company*
IndicationMode of action DateNew molecular entitiesLisdexamfetamine
dimesylate (Vyvanse)New River Attentiondeficit/hyperactivity
disorderhttp://www.fda.gov/cder/foi/label/2007/021977s002lbl.pdfProdrug
of dextroamphetamine with CNS stimulant activity23 Feb (S)Aliskiren
(Tekturna) Novartis
Hypertensionhttp://www.fda.gov/cder/foi/label/2007/021985lbl.pdfDirect
renin inhibitor 5 Mar (S)Lapatinib (Tykerb)GlaxoSmithKline Advanced
or metastatic breast
cancerhttp://www.fda.gov/cder/foi/label/2007/022059s002lbl.pdfKinase
inhibitor with targets including HER2 (also known as ERBB2)13 Mar
(P)Retapamulin (Altabax)GlaxoSmithKline
Impetigohttp://www.fda.gov/cder/foi/label/2007/022055lbl.pdf
Bacterial protein-synthesis inhibitor12 Apr (S)Rotigotine (Neupro)
Schwarz BioSciencesEarly stage idiopathic Parkinsons
diseasehttp://www.fda.gov/cder/foi/label/2007/021829lbl.pdf
Dopamine receptor agonist 9 May (S)Temsirolimus (Torisel) Wyeth
Advanced renal cell
carcinomahttp://www.fda.gov/cder/foi/label/2007/022088lbl.pdf
Mammalian target of rapamycin (mTOR) inhibitor30 May (P,
O)Ambrisentan (Letairis) Gilead Sciences Pulmonary arterial
hypertensionhttp://www.fda.gov/cder/foi/label/2007/022081s000_lbl.pdfEndothelin
receptor antagonist15 Jun (P, O)Maraviroc (Selzentry) Pfizer
CCR5-tropic
HIV-1http://www.fda.gov/cder/foi/label/2007/022128lbl.pdfCCR5
co-receptor antagonist6 Aug (P)Ammonia (Ammonia N13)Feinstein
Radioactive agent for positron emission tomography diagnosis of
coronary artery disease 23 Aug (S)Lanreotide(Somatuline
Depot)Biomeasure
Acromegalyhttp://www.fda.gov/cder/foi/label/2007/022074lbl.pdf
Somatostatin analogue 30 Aug (S, O)Doripenem(Doribax)Johnson &
JohnsonUrinary tract
infectionshttp://www.fda.gov/cder/foi/label/2007/022106lbl.pdfSynthetic
broad-spectrum carbapenem antibiotic12 Oct (S)Raltegravir potassium
(Isentress)Merck
HIV-1http://www.fda.gov/cder/foi/label/2007/022145lbl.pdf HIV
integrase strand transfer inhibitor12 Oct (P)Ixabepilone (Ixempra)
BristolMyers SquibbAdvanced or metastatic breast
cancerhttp://www.fda.gov/cder/foi/label/2007/022065lbl.pdfMicrotubule
inhibitor 16 Oct (P)Nilotinib (Tasigna) Novartis Chronic
myelogenous
leukaemiahttp://www.fda.gov/cder/foi/label/2007/022068lbl.pdf
BCRABL kinase inhibitor 29 Oct(S, O)Sapropterin dihydrochloride
(Kuvan)BioMarin
Hyperphenylalaninaemiahttp://www.fda.gov/cder/foi/label/2007/022181lbl.pdf
Synthetic tetrahydro-biopterin, cofactor forthe enzyme
phenylalaninehydroxylase13 Dec (P, O)Nebivolol (Bystolic) Mylan
Bertek Hypertension-adrenoceptor antagonist17 Dec (S)Hydroxyethyl
starch(Voluven)Fresenius Kabi Serious blood volume lossBlood volume
expander 27 Dec||BiologicsEculizumab (Soliris) Alexion Paroxysmal
nocturnal
haemogobinuriahttp://www.fda.gov/cder/foi/label/2007/125166lbl.pdfRecombinanthumanized
monoclonalimmunoglobulin G2/ 4 antibody that binds to complement
protein C516 Mar (P, O)Methoxy polyethylene glycol-epoetin beta
(Mircera)HoffmanLa-RocheAnaemia associated with chronic renal
failurehttp://www.fda.gov/cder/foi/label/2007/125164lbl.pdf
Erythropoietin receptor activator14 Nov (P)*The company that
submitted the original new drug application or biologic license
application to the US FDA. See full labelling information online.
Label not available at time of going to press. ||Information not
available at time of going to press. O, FDA Orphan designation; P,
FDA Priority Review; S, FDA Standard Review.As part of the Act,
Congress also established the ReaganUdall Foundation to identify
and address unmet scientific needs in the development, manufacture
and evaluation of FDA-regulated products, although the level of
funding is currently uncertain. And across the Atlantic, the EU has
just officially launched the Innovative Medicines Initiative, with
2 billion euros in funding from the EU and the pharmaceutical
industry, to find solutions to overcome research bottlenecks in the
drug development process. With such efforts to improve drug
development processes, there is much to be hopeful for in the
coming years, but there is no overnight remedy. Milne concludes:
Its a period of flux in getting from A to B.NEWS&ANALYSI
SNATURE REVIEWS | DRUGDISCOVERYVOLUME7|FEBRUARY2008|109 2008 Nature
Publishing Group