Embed Size (px)
DESCRIPTION
ED Neurological Emergencies Patients’ Neuroresuscitation Update: Coma, CNS Infection, TBI, & Hypothermic Resuscitation. 2007 EMA Advanced Emergency & Acute Care Medicine Conference Atlantic City, NJ September 24, 2007. - PowerPoint PPT Presentation
Citation preview

Edward P. Sloan, MD, MPH, FACEP
ED Neurological ED Neurological Emergencies Patients’ Emergencies Patients’
Neuroresuscitation Update:Neuroresuscitation Update: Coma, CNS Infection, TBI, & Coma, CNS Infection, TBI, & Hypothermic ResuscitationHypothermic Resuscitation

Edward P. Sloan, MD, MPH, FACEP
2007 EMA Advanced Emergency & Acute Care Medicine Conference
Atlantic City, NJAtlantic City, NJ
September 24, 2007September 24, 2007

Edward P. Sloan, MD, MPH, FACEP
Edward P. Sloan, MD, MPH FACEP
Professor
Department of Emergency MedicineUniversity of Illinois College of Medicine
Chicago, IL

Edward P. Sloan, MD, MPH, FACEP
Attending PhysicianEmergency Medicine
University of Illinois HospitalOur Lady of the Resurrection Hospital
Chicago, IL

Edward P. Sloan, MD, MPH, FACEP
DisclosuresDisclosures• FERNE Chairman and PresidentFERNE Chairman and President
• No individual financial disclosuresNo individual financial disclosures

Edward P. Sloan, MD, MPH, FACEP
Global ObjectivesGlobal Objectives
• Improve neurological emergencies Rx
• Know how to quickly evaluate patients
• Determine how to use empiric meds
• Provide evidence-based protocols
• Facilitate disposition, improve pt outcome
• Improve Emergency Medicine practice

Edward P. Sloan, MD, MPH, FACEP
Session ObjectivesSession Objectives
• Present relevant patient cases
• Discuss key clinical questions
• Review the procedures
• Restate driving principles
• Coma, suspected meningitis, SE
• Elevated ICP in TBI, INR in ICH, BP in AIS

Edward P. Sloan, MD, MPH, FACEP
MethodologyMethodology
• Identify key neurological emergencies
• Consider key clinical questions
• Search the medical literature
• Focus on evidence that supports practice
• Utilize www.guidelines.gov, www.acep.org
• Integrate into procedures

Edward P. Sloan, MD, MPH, FACEP
A Guidelines PerspectiveA Guidelines Perspective• Key questions define clinical practice
• Robust literature, accessed via internet
• Actual practice standards are limited
• Most of what we do is well defined
• No need to greatly vary what we do best: empirically treat, stabilize, diagnose, and disposition pts during unstable ED period

Edward P. Sloan, MD, MPH, FACEP
A Perspective on ProceduresA Perspective on Procedures
• Critically ill ED patients
• True medical emergencies
• Limited time and resources
• A need to diagnose and act
• “Emergency physicians take a surgeon’s approach to medical emergencies.”
• We do procedures, we are good at them

Edward P. Sloan, MD, MPH, FACEP
Procedures & Clinical PracticeProcedures & Clinical Practice• Guidelines, pathways, protocols
• Procedures
• Translate research into clinical practice
• Specific, quantifiable
• Documented via medical record
• Viewed favorably in retrospect
• Lead to consistency, improved pt outcome

Edward P. Sloan, MD, MPH, FACEP
A Clinical Case:A Clinical Case:The Comatose PatientThe Comatose Patient

Edward P. Sloan, MD, MPH, FACEP
Patient Clinical HistoryPatient Clinical History
• 46 yo male
• EMS to ED
• Unresponsive
• Unable to be intubated in the field

Edward P. Sloan, MD, MPH, FACEP
ED PresentationED Presentation
• Responds to painful stimuli only
• GCS = 5
• No apparent trauma

Edward P. Sloan, MD, MPH, FACEP
Key Clinical QuestionsKey Clinical Questions
• Can you manage the comatose patient?
• Can you conduct a useful neuro exam?
• Can you determine the coma etiology?
• Do you know any useful mnemonics?

Edward P. Sloan, MD, MPH, FACEP
Empiric Comatose Patient Empiric Comatose Patient Therapies: Therapies:
The ProcedureThe Procedure

Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Control the airway, ventilate
Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Control the airway, ventilate
• Do a bedside glucose determination– Provide D50 for hypoglycemia
– Avoid hyperglycemia

Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Control the airway, ventilate
• Do a bedside glucose determination– Provide D50 for hypoglycemia
– Avoid hyperglycemia
• Detect hypoperfusion (Decreased CPP) – CPP = MAP – ICP (MAP > 90 mmHg key)
– NS fluid boluses up to 500 cc each

Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Assess for narcotic overdose– Nalaxone 2 mg IV or sublingual
– Be prepared to restrain patient

Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Assess for narcotic overdose– Nalaxone 2 mg IV or sublingual
– Be prepared to restrain patient
• Assess for benzodiazepine overdose– Flumazenil 0.2 mg IVP x 5 (max dose 1 mg)
– If acute ingestion, initial dose OK, no seizure

Edward P. Sloan, MD, MPH, FACEP
Empiric TherapyEmpiric Therapy
• Assess for narcotic overdose– Nalaxone 2 mg IV or sublingual– Be prepared to restrain patient
• Assess for benzodiazepine overdose– Flumazenil 0.2 mg IVP x 5 (max dose 1 mg)– If acute ingestion, initial dose OK, no
seizure
• Examine for likely EtOH abuse – Thiamine 100 mg IVP or to IVF

Edward P. Sloan, MD, MPH, FACEP
Empiric Therapies: PrinciplesEmpiric Therapies: Principles• Airway management:
– Nasal or oral airway, ventilate, prepare for RSI
• Oxygen therapy• Obtain an accucheck, administer glucose• Fluid bolus for hypotension• Naloxone if evidence of narcotic use/abuse• Judicious flumazenil use for benzo abuse• Thiamine in alcohol abuse

Edward P. Sloan, MD, MPH, FACEP
Coma Patient Evaluation: Coma Patient Evaluation: The ProcedureThe Procedure

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Assess the pt’s overall mental status

Edward P. Sloan, MD, MPH, FACEP
Mental Status DescriptionMental Status Description
• AVPU– Alert– Responds to verbal stimuli– Responds to painful stimuli only– Unresponsive
• Start with this description. It sets the tome for the complete presentation to consultants.
Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Assess the pt’s overall mental status
• Assess the ABCs (trauma)– Airway & gag reflex
– Breathing pattern and sufficiency
– Circulation adequacy and hypotension

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Assess the pt’s overall mental status
• Assess the ABCs (trauma) – Airway & gag reflex
– Breathing pattern and sufficiency
– Circulation adequacy and hypotension
• Assess the skin, breath (toxidromes)

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Assess the pt’s overall mental status
• Assess the ABCs– Airway & gag reflex
– Breathing pattern and sufficiency
– Circulation adequacy and hypotension
• Assess the skin, breath (toxidromes)
• Detect posturing following stimulation

Edward P. Sloan, MD, MPH, FACEP
Decorticate posturing in comatose patient
Lesion above the red nucleus
Lower limbs extend, upper limbs flex following stimulus
Activity in the brainstem flexor center, the red nucleus
Edward P. Sloan, MD, MPH, FACEP
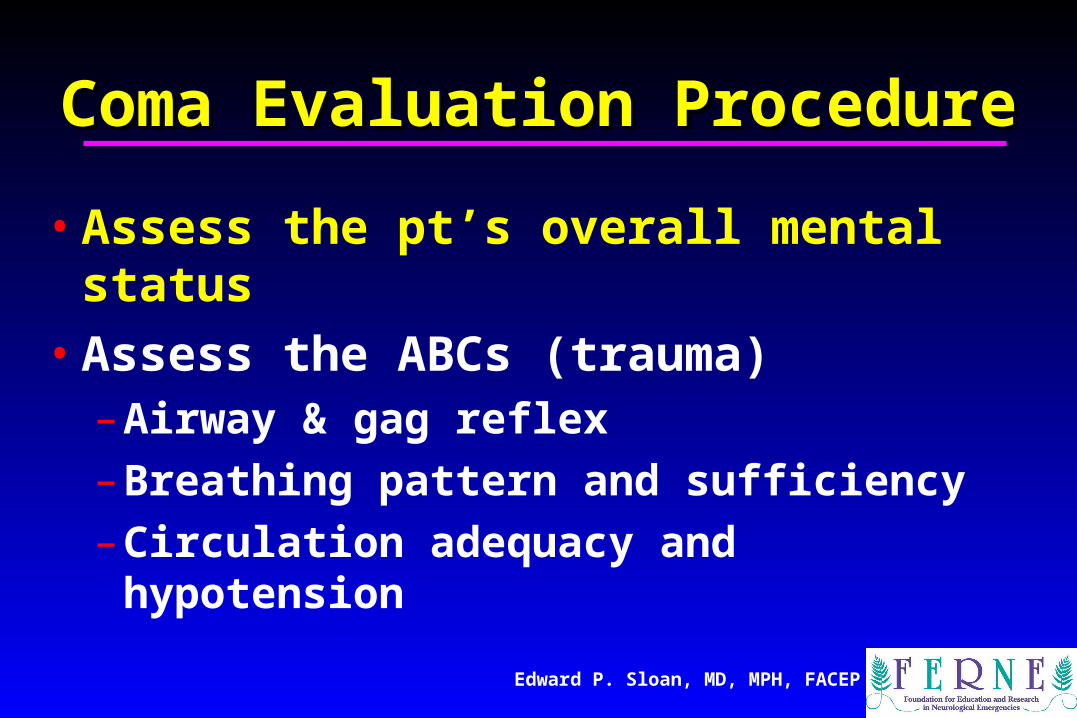
Decerebrate posturing in comatose patient
Upper and lower limbs extend following stimulus (pain, startle,or auditory)
Normal inhibition by cortex on the extensor facilitation part ofret form is missing, so extensors hyperactive
Lat vest nuclei involved, ablate and extensor posturing reduced

Edward P. Sloan, MD, MPH, FACEP
Clinical Value of Decorticate & Decerebrate Posturing
Decorticate posturing (flexion) indicates a higher level of brainstem function (a good thing) than decerebrate (extension) posturing; therefore:
Comatose patients who go from decerebrate to decorticate (ascending progression of impaired area) havea better prognosis than those that go from decorticate todecerebrate (descending progression of impaired area).
Descending impairment will be uniformly fatal if medullary respiratory and cardiovascular centers are damaged

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Calculate the Glasgow Coma Scale score– Eye Opening (4), Verbal (5), Motor (6)
– 13-15 Mild AMS, 4-8 Coma, 3 Vegetative

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Calculate the Glasgow Coma Scale score– Eye Opening (4), Verbal (5), Motor (6)
– 13-15 Mild AMS, 4-8 Coma, 3 Vegetative
• Detect abnormal reflexes– Corneal reflex
– Babinski (Chadduck)

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Examine the pupils– Size and equality
– Light reactivity, consensual response
• Differentiate anisocoria from a true “blown pupil” and herniation
• Note that blown pupils do not occur in awake and responsive patients

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Examine the pupils– Size and equality
– Light reactivity, consensual response
• Perform the Doll’s eye maneuver

Edward P. Sloan, MD, MPH, FACEP
Doll’s Eye ManeuverDoll’s Eye Maneuver
• Oculocephalic reflex
• Caution with suspected c-spine injury
• Eyes should continue to face to ceiling
• If eyes follow movement of head to side, suspect brainstem involvement in coma

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Examine the pupils– Equality
– Light reactivity
• Perform the Doll’s eye maneuver
• Detect evidence of psychogenic coma– Protective reflex
– Propriety reflex

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Look for ongoing seizure activity

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Look for ongoing seizure activity
• Perform cold calorics

Edward P. Sloan, MD, MPH, FACEP
Cold Caloric ExaminationCold Caloric Examination
• Oculovestibular reflex• Normal for slow movement of eyes
towards, fast movement away from cold water into ear canal
• If eyes move towards cold water, intact brainstem despite coma
• If no eye movement towards stimulation, suspect brainstem injury

Edward P. Sloan, MD, MPH, FACEP
Coma Evaluation ProcedureComa Evaluation Procedure
• Look for ongoing seizure activity• Perform cold calorics• Document checklist of coma findings
– Presence of coma, responsiveness, GCS– Vital signs, ABCs, empiric therapies– Exam findings checklist – Likely etiology– Likely location of lesion

Edward P. Sloan, MD, MPH, FACEP
Coma EtiologiesComa Etiologies
• T trauma, temperature
• I infections
• P psychiatric, porphyria
• S space-occupying lesion, stroke, SAH

Edward P. Sloan, MD, MPH, FACEP
Coma EtiologiesComa Etiologies
• A alcohol, other toxins
• E endocrine
• I insulin (DM complications)
• O oxygen deficiency, opiates
• U uremia, renal disorders

Edward P. Sloan, MD, MPH, FACEP
Coma Exam: PrinciplesComa Exam: Principles
• Many etiologies are apparent on exam
• Step-wise approach allows for detection
• Follows empiric therapies
• Precedes, directs neuroimaging
• Establishes baseline
• Mental status change then detectable

Edward P. Sloan, MD, MPH, FACEP
A Clinical Case:A Clinical Case: A Suspected Meningitis PatientA Suspected Meningitis Patient

Edward P. Sloan, MD, MPH, FACEP
Patient Clinical HistoryPatient Clinical History
• 63 yo female
• Weakness, fever, dehydration
• Mental status begins to deteriorate at home; 911 called
• EMS to ED

Edward P. Sloan, MD, MPH, FACEP
ED PresentationED Presentation
• Responds to verbal stimuli
• Delirious
• Fever of 102 degrees

Edward P. Sloan, MD, MPH, FACEP
Key Clinical QuestionsKey Clinical Questions
• When do you give the ceftriaxone?• Do you have to give decadron? When?• When are vancomycin, ampicillin, and
acyclovir indicated?• IS there and optimal approach to
performing the lumbar puncture? • When might the LP be deferred? Why?

Edward P. Sloan, MD, MPH, FACEP

Edward P. Sloan, MD, MPH, FACEP
Lumbar Puncture Lumbar Puncture in Suspected in Suspected
Meningitis Patients: Meningitis Patients: The ProcedureThe Procedure

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a complete neurological exam

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a complete neurological exam
• Evaluate clinically for increased ICP

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a complete neurological exam
• Evaluate clinically for increased ICP
• Obtain a CT prior to LP, assess ICP signs

Edward P. Sloan, MD, MPH, FACEPAndrew Perron, MD
Quadrigeminal cistern
Supracellar cistern

Edward P. Sloan, MD, MPH, FACEP
Quadrigeminal cistern
Sylvian cisterns

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a systematic neuro exam
• Evaluate clinically for increased ICP
• Obtain a CT prior to LP, assess ICP signs
• Measure opening pressure when feasible– Measure in all LPs when feasible
– May lead to other diagnoses

Edward P. Sloan, MD, MPH, FACEP
Opening PressureOpening Pressure• Normal: 60-200 mm H2O (obese
patients up to 250mm H20• Elevated: Suggest increased ICP
(>250 mm H20)–Mass lesion (neoplasm, hemorrhage,
infection)–Overproduction of CSF–Defective Outflow Mechanics

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a systematic neuro exam
• Evaluate clinically for increased ICP
• Obtain a CT prior to LP, assess ICP signs
• Measure opening pressure when feasible
• Consider sitting position, assess airway

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Perform a systematic neuro exam• Evaluate clinically for increased ICP• Obtain a CT prior to LP, assess ICP signs
• Measure opening pressure when feasible
• Consider sitting position, assess airway
• Caution with delirious patient

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Send CSF for interpretation:– Tube 1. Hematology: cell count, differential
– Tube 2. Microbiology: gram stain, cultures, antigen
testing
– Tube 3. Chemistry: glucose, protein
– Tube 4. Hematology: cell count, differential

Edward P. Sloan, MD, MPH, FACEP
Lumbar PunctureLumbar Puncture
• Send CSF for interpretation:– Tube 1. Hematology: cell count, differential
– Tube 2. Microbiology: gram stain, cultures
– Tube 3. Chemistry: glucose, protein
– Tube 4. Hematology: cell count, differential
• WBC, differential not subtle in bacterial meningitis and encephalitis??

Edward P. Sloan, MD, MPH, FACEP
CSF InterpretationCSF Interpretation
• Bacterial meningitis: – WBCs: Thousands+ WBCs, neutrophils– Frankly cloudy CSF fluid– Usually not CSF pleocytosis (inflammation)
• Viral meningitis, encephalitis:– CSF pleocytosis may be only finding– WBCs: lymphocytes, esp over time– CSF not frankly purulent

Edward P. Sloan, MD, MPH, FACEP
Traumatic TapTraumatic Tap
• Accidental trauma to a capillary, venule
• Increases both RBCs & WBCs in CSF
• If peripheral WBC normal subtract 1 WBC for every 500 RBC

Edward P. Sloan, MD, MPH, FACEP
XanthochromiaXanthochromia
• Rapid lysis of RBC in the CSF
• Results of breakdown of hemoglobin
• Begins to appear 2-4 hours after RBCs enter subarachnoid space
• If xanthochromia, not a traumatic tap
• Persists for 2-4 weeks

Edward P. Sloan, MD, MPH, FACEP
Calculating the Predicted Calculating the Predicted CSF WBC CountCSF WBC Count
Predicted CSF WBC count/microL =
CSF RBC count X (peripheral blood WBC count ÷ peripheral RBC count)

Edward P. Sloan, MD, MPH, FACEP
Validation of Prediction Validation of Prediction Calculation in AdultsCalculation in Adults
• 720 patients– CSF WBC count >10X predicted value
• Positive Predictive Value 48% for bacterial meningitis
– CSF WBC count < 10X predicted value• Negative Predictive Value 99% for bacterial
meningitis

Edward P. Sloan, MD, MPH, FACEP
Validation of Prediction Validation of Prediction Calculation in ChildrenCalculation in Children
• 92 children– CSF WBC count >10X predicted value
• 28/30 children (93%) bacterial meningitis
• 57 children– CSF WBC count < 10X predicted
• 100% prediction for the absence of bacterial meningitis

Edward P. Sloan, MD, MPH, FACEP
Lumbar Puncture: PrinciplesLumbar Puncture: Principles
• LP only if clinically feasible
• If increased ICP possible, careful CT review
• Sitting position, measure pressure fast flow
• Be careful in setting of delirium
• Treat with antibiotics first
• Bacterial meningitis interpretation useful

Edward P. Sloan, MD, MPH, FACEP
Antibiotic Therapy in Antibiotic Therapy in Suspected Meningitis Patients: Suspected Meningitis Patients:
The ProcedureThe Procedure

Edward P. Sloan, MD, MPH, FACEP
Antibiotic Rx ProcedureAntibiotic Rx Procedure
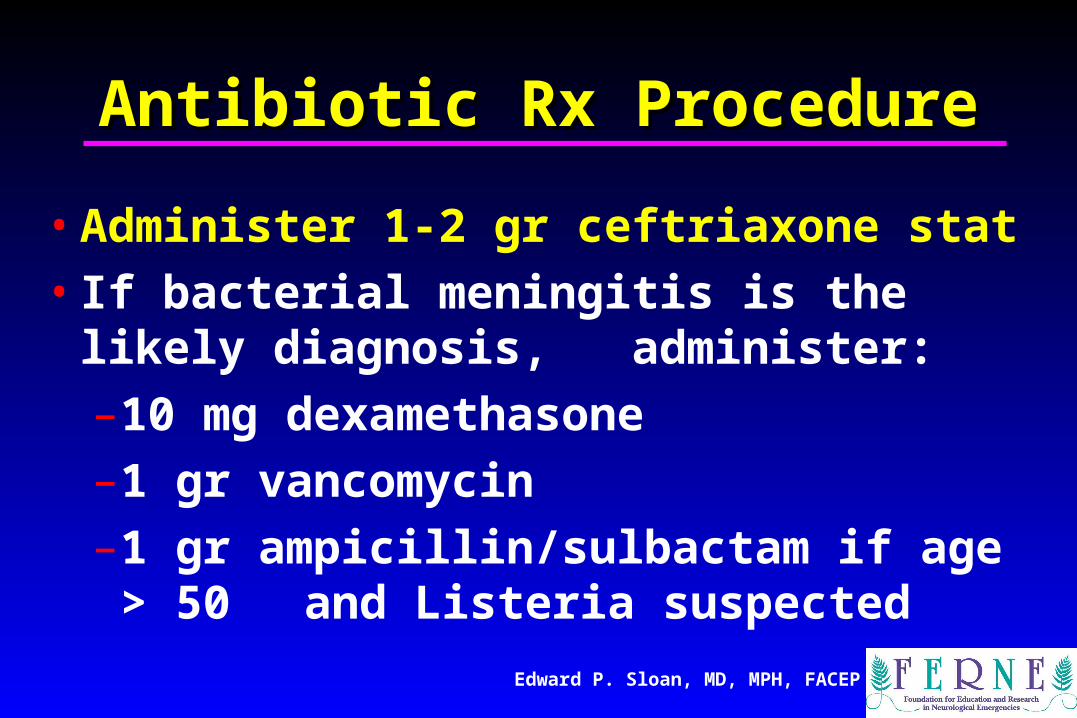
• Administer 1-2 gr ceftriaxone stat
Edward P. Sloan, MD, MPH, FACEP
Antibiotic Rx ProcedureAntibiotic Rx Procedure
• Administer 1-2 gr ceftriaxone stat
• If bacterial meningitis is the likely diagnosis, administer:
–10 mg dexamethasone
–1 gr vancomycin
–1 gr ampicillin/sulbactam if age > 50 and Listeria suspected

Edward P. Sloan, MD, MPH, FACEP
Antibiotic Rx ProcedureAntibiotic Rx Procedure
• If viral encephalitis is likely, administer:– 1 gr acyclovir IVPB over 1 hour

Edward P. Sloan, MD, MPH, FACEP
Antibiotic Rx ProcedureAntibiotic Rx Procedure• If viral encephalitis is likely, administer:
– 1 gr acyclovir IVPB over 1 hour
• Treat close contacts: cipro 500 po x 1, rifampin 600 PO BID x 2 days, or
ceftriaxone 250 IM x 1

Edward P. Sloan, MD, MPH, FACEP
Anbx Rx: Driving PrinciplesAnbx Rx: Driving Principles• Administer ceftriaxone early, prior to CT• Consider meningitis risk carefully• High risk patients: vancomycin,
ampicillin/sulbactam, steroids• Give steroids when pt deemed high risk • Add acyclovir when encephalitis possible• LP only if clinically feasible• Be cautious for increased ICP

Edward P. Sloan, MD, MPH, FACEP
A Clinical Case:A Clinical Case:Elevated ICP Management Elevated ICP Management
in a TBI Patientin a TBI Patient

Edward P. Sloan, MD, MPH, FACEP
Patient Clinical HistoryPatient Clinical History• 22 yo male
• EMS to ED
• MVC, high speed
• Initially lucid, then deterioration in mental status
• GCS 9

Edward P. Sloan, MD, MPH, FACEP
ED PresentationED Presentation

Edward P. Sloan, MD, MPH, FACEP
Key Clinical QuestionsKey Clinical Questions
• Can you manage the multiple trauma
• Can you detect and manage evidence of elevated ICP?
• Do you know neurosurgery indications?
• Do you know ICP monitoring indications?

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Therapy in Elevated ICP Therapy in TBI Patients: TBI Patients:
The ProcedureThe Procedure

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs

Edward P. Sloan, MD, MPH, FACEP
Global Resuscitation NeedsGlobal Resuscitation Needs
• Elevate head of bed
• Control airway
• Maintain SBP > 90 mm Hg
• Maintain oxygen sat > 90%

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs
• Consider decadron if brain edema noted in non-traumatic causes of elevated ICP

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs
• Consider decadron if brain edema noted
• Do not provide prophylactic osmotherapy

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs
• Consider decadron if brain edema noted
• Do not provide prophylactic osmotherapy
• Mannitol 20%, 100-200 cc (0.25-0.50 mg/kg) q 4 hr, not by continuous infusion

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs
• Consider decadron if brain edema noted
• Do not provide prophylactic osmotherapy
• Mannitol 20%, 100-200 cc (0.25-0.50 mg/kg) q 4 hr, not by continuous infusion
• Lasix 10 mg IVP q 8 hr

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Evaluate globally all resuscitation needs
• Consider decadron if brain edema noted
• Do not provide prophylactic osmotherapy
• Mannitol 20%, 100-200 cc (0.25-0.50 mg/kg) q 4 hr, not by continuous infusion
• Lasix 10 mg IVP q 8 hr
• Measure serum osmols BID, < 310 mOsm/L

Edward P. Sloan, MD, MPH, FACEP
Mannitol in Elevated ICPMannitol in Elevated ICP
• Indicated when clinical deterioration occurs (worsening mental status)
• Also useful when AMS present at baseline and cerebral edema noted
• In this instance not prophylactic per se

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Do not use prophylactic hyperventilation

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Do not use prophylactic hyperventilation
• With clinical deterioration, achieve hypocarbia to pCO2 30-35 mm Hg (25-30)

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Do not use prophylactic hyperventilation
• With clinical deterioration, achieve hypocarbia to pCO2 30-35 mm Hg (25-30)
• Raise ventilatory rate with constant tidal volume (rarely up to 12-14 ml/kg)

Edward P. Sloan, MD, MPH, FACEP
Elevated ICP Rx ProcedureElevated ICP Rx Procedure
• Do not use prophylactic hyperventilation
• With clinical deterioration, achieve hypocarbia to pCO2 30-35 mm Hg
• Raise ventilatory rate with constant tidal volume (rarely up to 12-14 ml/kg)
• Non-depolarizing paralytics, lidocaine to minimize ICP elevation bursts

Edward P. Sloan, MD, MPH, FACEP
Hyperventilation, Elevated ICPHyperventilation, Elevated ICP
• Tidal volume important
• 10 ml/kg in 80 kg pt: 800 cc tidal volume
• Most pts treated with smaller tidal volumes
• If pCO2 > 35, may need to both increase tidal volume and vent rate in order to maximize minute ventilation, oxygenation

Edward P. Sloan, MD, MPH, FACEP
Hyperventilation: TV ChangeHyperventilation: TV Change
• 80 kg person
• 700 cc tidal volume, rate 14
• Minute ventilation 9.8 L
• If pCO2 = 35, increase tidal volume to 800
• Minute ventilation increased to 11.2 L
• ~15% increase in tidal volume and minute ventilation
Edward P. Sloan, MD, MPH, FACEP
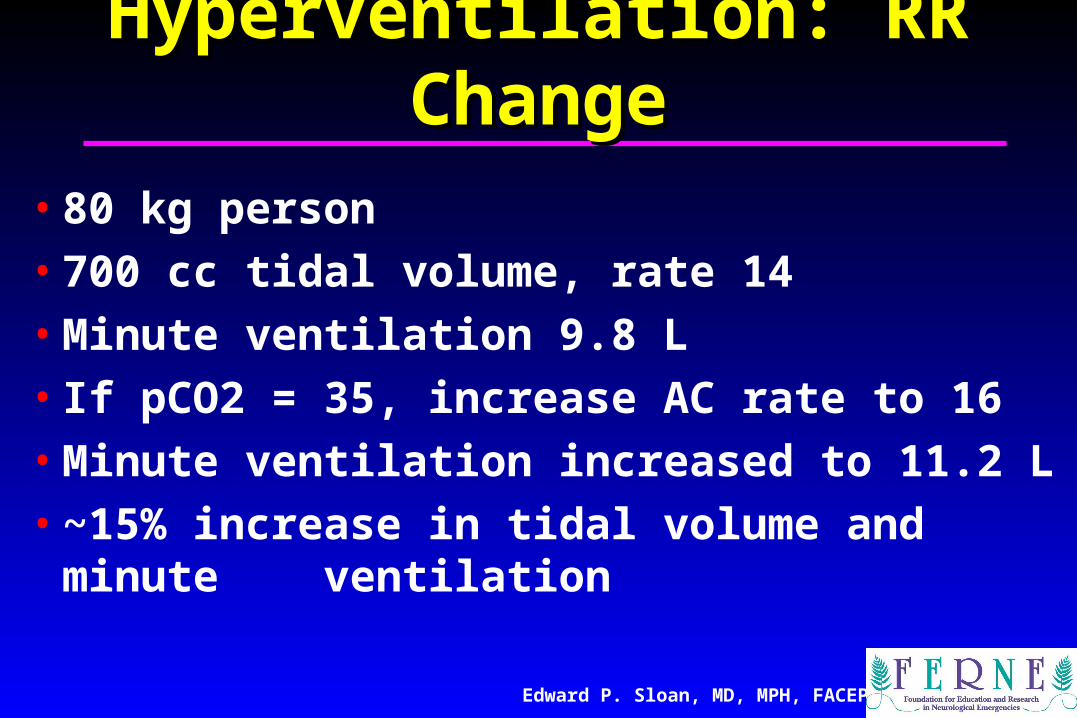
Hyperventilation: RR ChangeHyperventilation: RR Change
• 80 kg person
• 700 cc tidal volume, rate 14
• Minute ventilation 9.8 L
• If pCO2 = 35, increase AC rate to 16
• Minute ventilation increased to 11.2 L
• ~15% increase in tidal volume and minute ventilation

Edward P. Sloan, MD, MPH, FACEP
ICP Rx: Driving PrinciplesICP Rx: Driving Principles
• Know the clinical signs of elevated ICP
• Be able to detect elevated ICP on CT
• Consider decadron and mannitol use
• Consider prophylaxis with a phenytoin
• Be prepared to treat seizures and SE
• Know how to assess rostral-caudal deterioration (herniation)

Brian O’Neil, MD
Hypothermic Hypothermic Resuscitation in Patients Resuscitation in Patients
with CNS Injury Due to with CNS Injury Due to Cardiac Arrest Cardiac Arrest

Brian O’Neil, MD
Brian J. O’Neil, MD Professor
Department of Emergency MedicineWayne State University,
Research Director,William Beaumont Hospital
Royal Oak, MI

Brian O’Neil, MD
phospholipaseactivation
Free Arachidonate
ER Ca 2+ Depletion
REPERFUSION
EpinephrineATP
PKAactivation
PP2A
I 1activation
PP1inhibited
eIF2 kinase activation
eIF2 (P)
InhibitedProtein
SynthesisApoptosis
.O2-
Fe2+Lipid Peroxidation
Membrane Damage
InhibitedGrowth Factor
SignalingCHOP
Bad dephosphorylation,Bax, mitochondriarelease cytochrome c& caspase 9to APAF1
activecaspase 3
Cytosolic Ca 2+
ATP DepolarizationISCHEMIA
eIF4G & spectrindegradation
-calpainactivation calcineurin
activation NOSactivation
peroxynitrite
cAMP
AND REPERFUSION THAT LEAD TO NEURONAL DEATH
DEATH
MODEL OF MOLECULAR EVENTS DURING BRAIN ISCHEMIA

Brian O’Neil, MD
Historical ObservationsHistorical Observations• Not Dead till Warm and DeadNot Dead till Warm and Dead
• Cold patients would awaken in the MorgueCold patients would awaken in the Morgue
• Kids / Hockey Players- fall through ice, long Kids / Hockey Players- fall through ice, long rescue times, but good recoveryrescue times, but good recovery
• Hibernation: state of low oxygen, acidosis, Hibernation: state of low oxygen, acidosis, low energy supplylow energy supply
• Basic science animal research showed Basic science animal research showed promising resultspromising results

Brian O’Neil, MD
Hypothermia: Hypothermia: Potential MechanismsPotential Mechanisms
• 6% in metabolic rate per 1 C reduction in brain temperature
• CMR declined to 50% after brain cooling to 32 degrees C (CBF & CMR coupled)
• blocks release of excitatory amino acid• reduces early calcium rise• reduces calpain specific and cytoskeletal
damage

Brian O’Neil, MD
Clinical HypothermiaClinical Hypothermia
• Bernard et al (77 pts)• external cooling, ice bags, initiated by
EMS at ROSC • 33.5 C within two hours ROSC cooled
for 12 hours• Good outcome = 49% v 26%

Brian O’Neil, MD
Clinical HypothermiaClinical Hypothermia• The European group, 136 pts,
• VF arrest, comatose, stable hemodynamics • external cooling device,• 8 hrs = median time to target Temp (33 C)
• 14.4% did not reach target T° • Cooling for a mean of 24 hours• Good outcome = 55% v 39%

Brian O’Neil, MD
Hypothermia: Hypothermia: The Beaumont ExperienceThe Beaumont Experience
INCLUSION• Patients with witnessed out of hospital
cardiac arrest of presumed cardiac origin• any initial rhythm that had ACLS within 15
minutes• restoration of spontaneous circulation,
(ROSC) within 60 mins of collapse • able to obtain informed consent by
representative/family member were enrolled
Brian O’Neil, MD
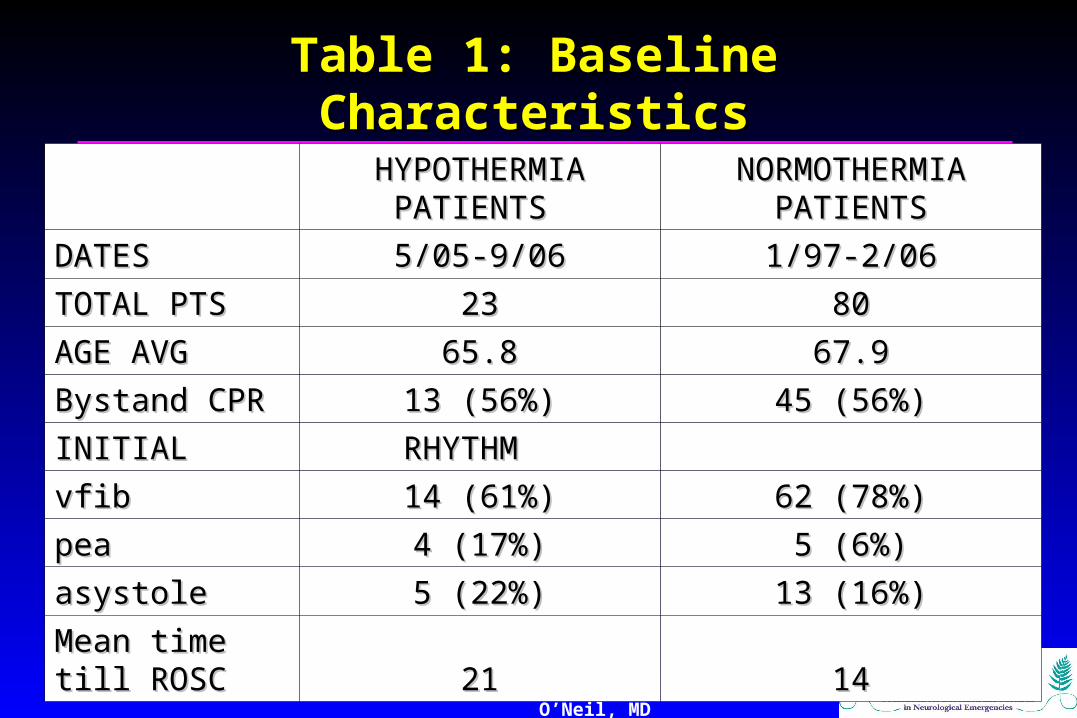
Table 1: Baseline CharacteristicsTable 1: Baseline Characteristics
HYPOTHERMIA HYPOTHERMIA
PATIENTS PATIENTS NORMOTHERMIA NORMOTHERMIA
PATIENTSPATIENTS
DATESDATES 5/05-9/065/05-9/06 1/97-2/061/97-2/06
TOTAL PTSTOTAL PTS 2323 8080
AGE AVGAGE AVG 65.865.8 67.967.9
Bystand CPRBystand CPR 13 (56%)13 (56%) 45 (56%)45 (56%)
INITIALINITIAL RHYTHM RHYTHM
vfibvfib 14 (61%)14 (61%) 62 (78%)62 (78%)
peapea 4 (17%)4 (17%) 5 (6%)5 (6%)
asystoleasystole 5 (22%)5 (22%) 13 (16%)13 (16%)
Mean time till Mean time till ROSC ROSC 2121 1414

Brian O’Neil, MD
52%
33%
52%
28%
48%
72%
0%
10%
20%
30%
40%
50%
60%
70%
80%
DISCHARGED ALIVE CPC 1 or 2 CPC 3 or greater
MORTALITY AND NEUROLOGICAL OUTCOMES
HYPOTHERMIA PATIENTS NORMOTHERMIA PATIENTS
p = 0.033

Brian O’Neil, MD
Practical HypothermiaPractical Hypothermia• First thing you need are ChampionsFirst thing you need are Champions• Next get Buy In:Next get Buy In:
• ED, CCU, ICU, Nursing and AdministrationED, CCU, ICU, Nursing and Administration
• Sit down and hammer out a protocolSit down and hammer out a protocol• Educate StaffEducate Staff• Facilitate the first few patientsFacilitate the first few patients

Brian O’Neil, MD
Practical HypothermiaPractical Hypothermia• Initiation: Sooner the Better: Pre-hospital or in-hospitalInitiation: Sooner the Better: Pre-hospital or in-hospital
• Ice bags in Groin, Axilla and NeckIce bags in Groin, Axilla and Neck• Cold IV fluidsCold IV fluids• Regular cooling blanketRegular cooling blanket• Intravenous catheters / Gel PadsIntravenous catheters / Gel Pads
• More consistent temperature regulationMore consistent temperature regulation• Target 33.5 Target 33.5 C:C:
• Esophageal > bladder > rectal probesEsophageal > bladder > rectal probes• Bladder probes need urine outputBladder probes need urine output
• Watch for rapid drop, cooling is non-linear Watch for rapid drop, cooling is non-linear

Brian O’Neil, MD
Practical HypothermiaPractical Hypothermia• Paralyze / SedateParalyze / Sedate
• Ativan drip: added seizure controlAtivan drip: added seizure control• Watch for:Watch for:
• Low K+ and Mg ++Low K+ and Mg ++• High GlucoseHigh Glucose
• Stress dose insulin with bolusesStress dose insulin with boluses• BradycardiaBradycardia• Prolonged QTProlonged QT• BleedingBleeding• Pneumonia/ sepsisPneumonia/ sepsis

Brian O’Neil, MD
Practical HypothermiaPractical HypothermiaRe-warming:Re-warming:
• Not truly activeNot truly active• Decreased rate of coolingDecreased rate of cooling
• Beware of temperature overshootBeware of temperature overshoot• Stop re-warming around 35Stop re-warming around 35 C C
• Watch for:Watch for:• SeizuresSeizures• ArrhythmiasArrhythmias• FeversFevers

Brian O’Neil, MD
What the Future HoldsWhat the Future Holds• NMDA/ AMPA receptor antagonist and NMDA/ AMPA receptor antagonist and
• phase II trials have recently shown some efficacy in phase II trials have recently shown some efficacy in CHICHI
• Estradiols and ProgesteroneEstradiols and Progesterone• Hypothermia during resuscitationHypothermia during resuscitation• Cannabinoids::
• most potent antioxidants known, (dexanabinol)most potent antioxidants known, (dexanabinol)• Many receptor similarities to opioidsMany receptor similarities to opioids
• Also induces hypothermiaAlso induces hypothermia • Insulin and other growth factorsInsulin and other growth factors

Brian O’Neil, MD
What the Future HoldsWhat the Future HoldsOpioid receptor antagonistsOpioid receptor antagonists::
• -, DADLE, -, DADLE, opioid receptor, BRL-52537 opioid receptor, BRL-52537• proteins trigger hibernationproteins trigger hibernation
-opiate antagonists reverse hibernation-opiate antagonists reverse hibernation• pre-conditioning proteinpre-conditioning protein
- myocytes and neurons- myocytes and neurons• mechanisms: ATP-K+ channels, PKC, free radicalsmechanisms: ATP-K+ channels, PKC, free radicals
-increases ERK and bcl-2-increases ERK and bcl-2

Brian O’Neil, MD
ConclusionsConclusions• Post-ROSC Neurologic resuscitation:
• needs to improve
• Injury Mechanisms:•Complex, Multi-factoral•Silver Bullet Trials have Failed
• The Future Looks Bright• Therapeutic Hypothermia:
•Currently only proven therapy•Cheap, Easy, risk / benefit ratio is huge

Edward P. Sloan, MD, MPH
ConclusionsConclusions• Coma, CNS infection, TBI, and
hypothermic resuscitation after cardiac arrest all are important skills of the emergency care provider
• Treatment options are easy to identify • Procedures can be developed, followed• Pt outcomes can be optimized• EM clinical practice can be optimized

Thank you.Thank you.
[email protected]@ferne.org
[email protected]@uic.edu312 413 7490312 413 7490
ferne_ema_2007_neuroresus_cnspart2_sloan_092507_finalcd 04/19/23 18:21 Edward P. Sloan, MD, MPH, FACEP

Edward P. Sloan, MD, MPH, FACEP
www.ferne.orgwww.ferne.org