Embed Size (px)
Citation preview
2005 update onmanagementof poisoning
Kent R. Olson, MD
Medical Director, SF Division
California Poison Control System
UC San Francisco
Case
A 16 year old boy with nausea and vomiting Broke up with his girlfriend last night “Might have taken some aspirin” HR 100/min BP 120/70 T 98.6 F RR 12 Exam unremarkable Na 140 K 3.8 Cl 108 HCO3 22 Salicylate = not detectable UTox = negative
Acetaminophen ingestion
Often overlooked Hx incorrect or not available Hidden ingredient in many drugs Nonspecific symptoms (N/V) Initial labs usually normal
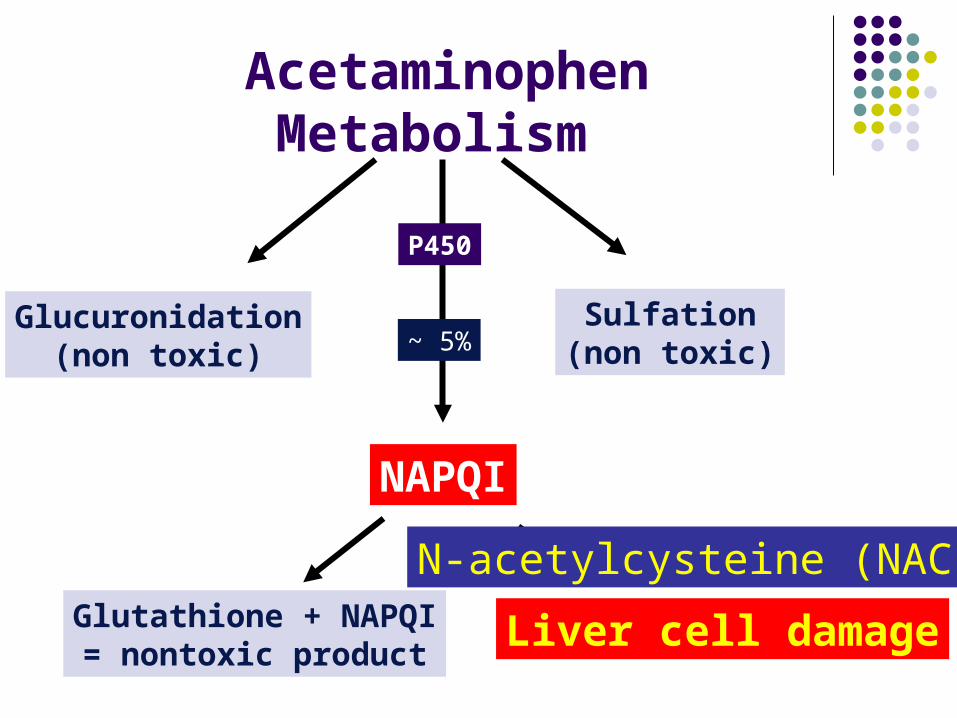
AcetaminophenMetabolism
Glucuronidation(non toxic)
Sulfation(non toxic)
NAPQI
P450
~ 5%
Glutathione + NAPQI= nontoxic product
Liver cell damage
N-acetylcysteine (NAC)
NAC treatment
Best if started within 8 hours of ingestion However, late treatment still beneficial
Vomiting often complicates PO dosing Use antiemetics? Give via NG tube? Give the NAC intravenously?
So what’s new?
IV acetylcysteine Duration of treatment Other tidbits:
Acidosis early after ingestion Early (transient) elevated INR
IV acetylcysteine
Conventional product (Mucomyst) not FDA approved for parenteral use But, can be given IV via micropore filter
New, approved IV product = Acetadote™ Advantages? Side effects?
IV acetylcysteine
Both products can cause an anaphylactoid reaction (flushing, hypotension) May be infusion rate related (despite recent
report in Ann Emerg Med 2005 Apr;45(4):402-8)
We recommend giving initial loading dose more slowly (45-60 min versus 15 min)
Oral or IV?
< 7 hours after OD Use oral dosing regimen if not vomiting Switch promptly to IV if begins vomiting
> 7 hours after OD Start IV dosing immediately Either product is okay Can give first dose IV then switch to PO
How long to treat?
Conventional US protocol was 72 hours Shorter regimens have proven effective
We have used 24-36 hours for years Europeans have always used 20 hrs Acetadote uses 20-hour IV infusion
Bottom line: 20 hours IV or PO okay in most cases Treat longer if evidence of liver toxicity
Other acetaminophen tidbits
Acidosis early after ingestion Usually with levels > 500-600 mg/L May also see early coma, hypotension
with acute massive overdose Not secondary to liver failure
Transient early rise in PT/INR First 24 hrs Not secondary to liver failure
Case
A 15 year old was found in status epilepticus at home. Seizures stopped briefly after diazepam, but recurred in the ED. Patient arrived in U.S. one year ago from Mexico.
Fingerstick glucose: 120 Serum bicarbonate: 6 mEq/L
Case, continued
Further information: a empty bottle of isoniazid (INH) was found in the bathroom. Up to 30 gm (100 tablets 300 mg) missing.
Pyridoxine was ordered from the pharmacy, but they had only 3 g on hand. Other hospitals were immediately contacted to try and find more.
Isoniazid overdose
Clues to diagnosis: Recent immigrant or known TB patient Marked metabolic acidosis Note: INH not on most tox screens
Treatment: Pyridoxine (Vitamin B-6) Dose: #g for #g ingested, at least 5 g IV Hospital should stock at least 20 g
Antidote Supplies
Commonly understocked meds: Atropine Deferoxamine Fab digoxin antibodies Glucagon Pralidoxime (2-PAM) Pyridoxine (B-6)
Skolfield et al: J Clin Toxicol 1997; 35:490
Case
A 52 year old man was unconscious after overdose of Glucotrol (glipizide)
Initial glucose = 12 mg/dL Glucose remained less than 60 after 100
gm of D50 (4 amps) and a D10 drip. Single dose of OCTREOTIDE 50 mcg
reversed hypoglycemia within 60 min.
Sulfonylurea overdose
Enhance insulin release Some agents have long half-lives,
prolonged effect Admit all symptomatic cases
Antidotes: Glucose Inhibit insulin release:
Diazoxide (older agent)Octreotide (somatostatin analog) - PREFERRED
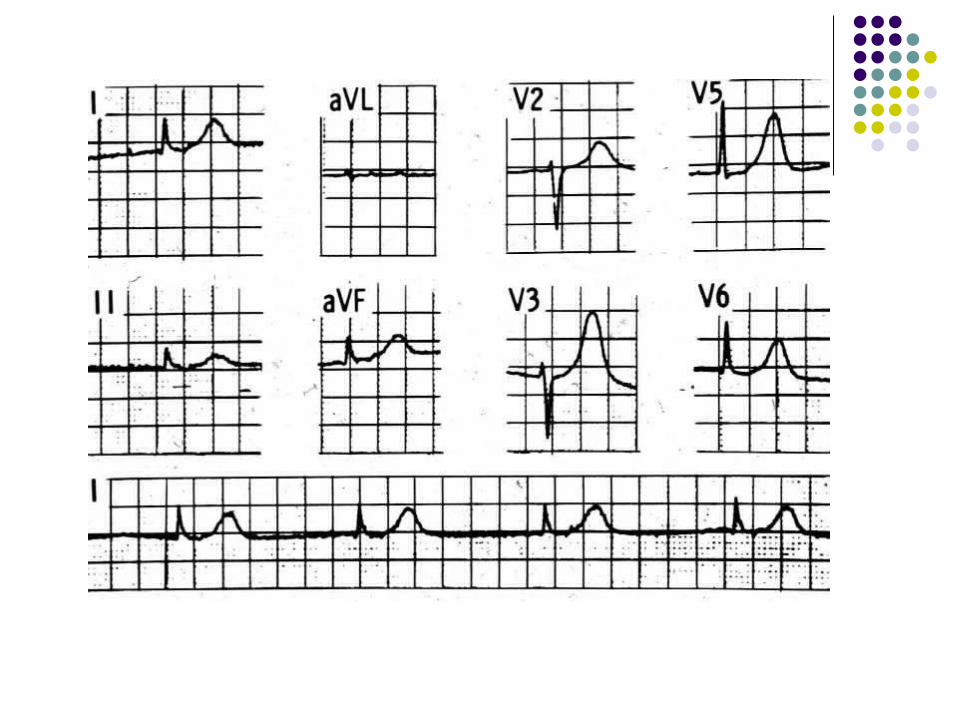
Case
A 65 year old woman presented with nausea, diaphoresis, weakness.
BP 78/40 mm Heart Rate 51/min ECG: junctional rhythm
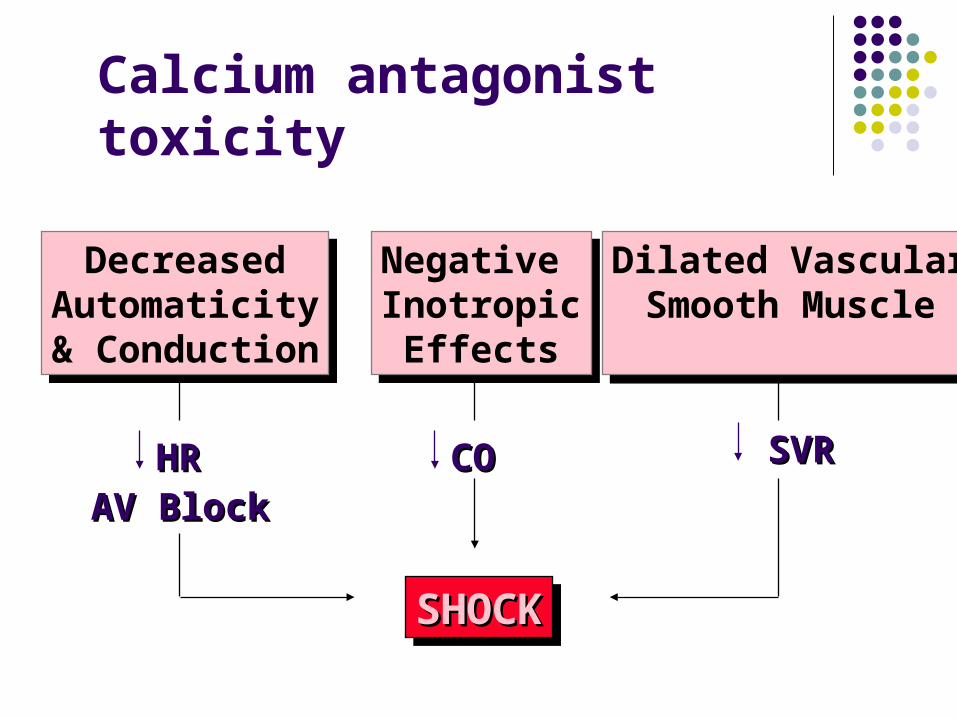
Negative InotropicEffects
Negative InotropicEffects
DecreasedAutomaticity& Conduction
DecreasedAutomaticity& Conduction
Dilated VascularSmooth Muscle
Dilated VascularSmooth Muscle
SVRSVRCOCOHRHRAV BlockAV Block
SHOCKSHOCKSHOCKSHOCK
Calcium antagonist toxicity
Reversal of CCB toxicity
Most sensitive to calcium administration: Reversal of negative inotropic effect
Less sensitive: Partial reversal of AV nodal conduction
block Not usually reversible by calcium:
Sinus node depression Reduced peripheral vascular resistance
Calcium doses for CCB toxicity
Initial dose 2-3 gm calcium chloride Repeated doses up to 10-12 gm reportedly
effective in severe poisonings Serum Ca++ levels as high as 16.3 mg/dL
(ref range 4.5-5.3) reported in one case involving sustained-release diltiazem.
Hantsch et al: J Clin Toxicol 1997; 35:495
High-dose insulin therapy
Favorable animal studies and several human case reports Purported mechanism: enhanced
intracellular carbohydrate metabolism May also work for beta-blocker OD
Dose: 0.5-1 unit/kg regular insulin bolus 0.5-1 units/hr insulin infusion plus IV glucose to maintain euglycemia
recent lit review in Ann Pharmacotherapy 2005 May;39(5):923-30
GI decontamination for CCBs
Many are sustained-release preparations: Calan SR Diltiazem-CD
Aggressive GI decontamination needed: Activated charcoal Whole bowel irrigation
Whole bowel irrigation
Balanced electrolyte-PEG solution GoLytely, CoLyte No net fluid loss or gain No electrolyte abnormalities
Dose 2 L/hr via NG tube (kids 500 mL/hr) May use for several hours or even days
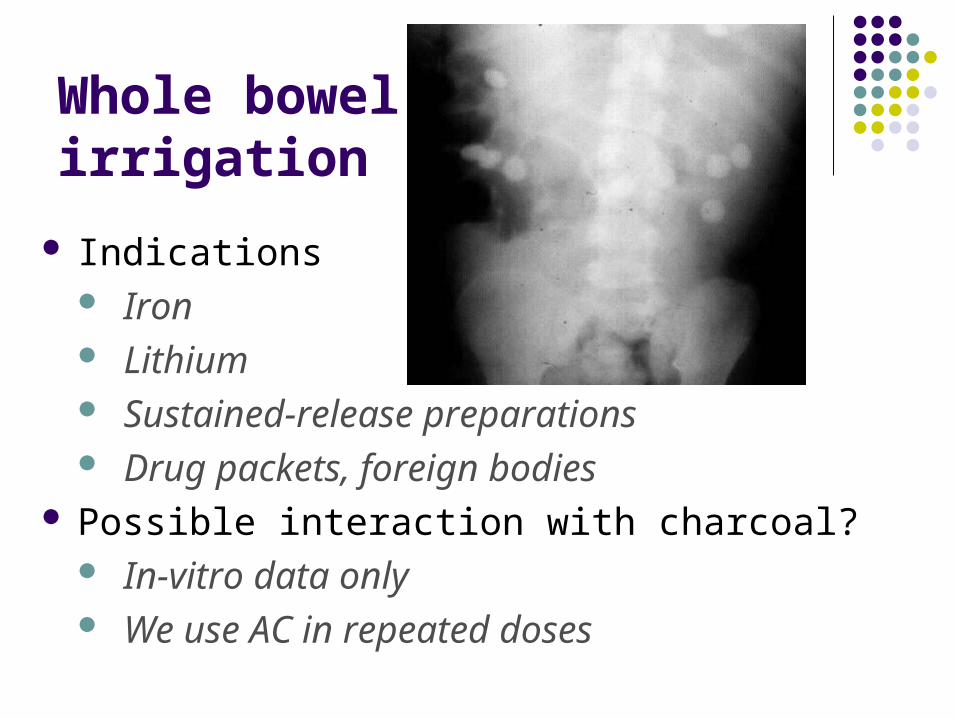
Whole bowel irrigation
Indications Iron Lithium Sustained-release preparations Drug packets, foreign bodies
Possible interaction with charcoal? In-vitro data only We use AC in repeated doses
Gut decontamination 2005
What’s OUT: Ipecac – except for rare use on scene if
hospital more than 60 min awayAAP no longer recommends home stocking
of ipecac ? Gastric Lavage
Most effective when used within 60 minConsider later use if massive ingestion, or
delayed gastric emptying likely (eg, ASA, anticholinergics, opioids, etc)
Gut decontamination 2005
What’s IN: Activated charcoal – if it can be given
early and airway is protectedConsider risk vs benefit in small ingestion of
moderate toxicity drug (eg, benzodiazepine) Whole bowel irrigation (WBI)
Calif. Poison Control System
24/7 access to expert advice Diagnosis & management Indications for and use of antidotes,
hemodialysis, antivenom MD-toxicologist back-up
1-800-8POISON (California)
1-800-222-1222 (nationwide)