Embed Size (px)
DESCRIPTION
2004 Public Health Training and Information Network (PHTIN) Series. Site Sign-in Sheet http://www.sph.unc.edu/nccphp/. First and Last Name Occupation Place of Employment Mailing Address Email Address. Site Sign-in Sheet http://www.sph.unc.edu/nccphp/. - PowerPoint PPT Presentation
Citation preview

2004 Public Health Training and
Information Network (PHTIN) Series

Site Sign-in Sheethttp://www.sph.unc.edu/nccphp/
First and Last Name
Occupation
Place of Employment
Mailing Address
Email Address

Site Sign-in Sheet http://www.sph.unc.edu/nccphp/
Please mail or fax your site’s sign-in sheet to:
Jennifer HorneyDirector of Training and EducationNC Center for Public Health PreparednessCB #8165, 400 RobersonChapel Hill, NC 27599
FAX: (919) 843 - 5563

Outbreak Investigation Methods
From Mystery to Mastery


2004 PHTIN Training Development Team
Jennifer Horney, MPH - Director, Training and Education, NCCPHP
Pia MacDonald, PhD, MPH - Director, NCCPHP
Amy Nelson, PhD
Penny Padgett, PhD, MPH
Sarah Pfau, MPH
Michelle Torok, MPH, Doctoral Candidate
Drew Voetsch, MPH, Doctoral Candidate

Future PHTIN Sessions
June 8th. . . . . . . . . . . . “Study Design”
August 17th. . . . . . . . . .“Interviewing Techniques”
September 14th. . . . . . .“Designing Questionnaires”
October 12th. . . . . . . . . “Analyzing Data”
December 14th. . . . . . . “Risk Communication”
Each session will be on a Tuesday from 10:00 am - 12:00 pm
(with time for discussion)

Session I – VI SlidesAfter the airing of each session, NCCPHP will post
PHTIN Outbreak Investigation Methods series slides on the following two web sites:
NCCPHP Training web site:http://www.sph.unc.edu/nccphp/training/index.html
North Carolina Division of Public Health, Office of Public Health Preparedness and Response
http://www.epi.state.nc.us/epi/phpr/

Session I
“Recognizing an Outbreak”

Today’s Presenters
Drew Voetsch, MPHResearch Associate and Doctoral Candidate, NCCPHP
Penny Padgett, PhD, MPHEpidemiologist / Surveillance Officer, NCCPHP
Ron HoldwayEnvironmental Health Director, Orange Co. Health Dept.
Sarah Pfau, MPHModerator

“Recognizing an Outbreak”Learning Objectives
At the end of this session, you will be able to:
• Identify multiple types of food borne illness surveillance systems
• Recognize uses of surveillance data
• Identify CDC’s steps of an outbreak investigation

“Recognizing an Outbreak”Learning Objectives (cont’d.)
At the end of this session, you will be able to:
• Develop and use a case definition
• Apply the process of case finding in an outbreak
• Follow methods for generating a hypothesis

“Recognizing an Outbreak”Session Content
• Introduction to surveillance
• Steps of an outbreak investigation
• Foodborne disease surveillance
• Case study investigated by Epi Team
professionals:
a. Epidemiologists
b. Public Health Laboratory specialists
c. Environmental Health specialists

Surveillance

What is Public Health Surveillance?
“The ongoing, systematic collection, analysis, and interpretation of health-related data essential to the planning, implementation, and evaluation of public health practice, closely integrated with the timely dissemination of these data to those responsible for prevention and control”
- CDC

Surveillance drives the cycle of public health prevention
Surveillance
Epidemiologic investigation
AppliedTargetedResearch
Preventionmeasures

Purpose of Surveillance
• Assess public health status
• Define public health priorities
• Evaluate programs
• Stimulate research

Surveillance Priority Areas
• Frequency
• Severity
• Cost
• Preventability
• Communicability
• Public interest

Uses of Surveillance
1. Estimate the magnitude of the problem
2. Determine the geographic distribution of
illness
3. Portray the natural history of a disease
4. Detect epidemics / define a problem
5. Generate hypotheses, stimulate research
6. Evaluate control measures
7. Monitor changes in infectious agents
8. Detect changes in health practice
9. Facilitate planning

http://www.epi.state.nc.us/epi/gcdc/pdf/10ANCAC41A.pdf
Reportable Diseases in NC

Estimate the Magnitude of the Problem
Cases and reported incidence (cases / 100,000) of food borne diseases in North Carolina, 2002
Disease Cases Incidence
Campylobacteriosis 683 8.2
E. coli O157 infection 244 2.9
Foodborne:other 281 3.4
Hepatitis A 209 2.5
Salmonellosis 1655 19.9
Shigellosis 1074 12.9
(http://www.epi.state.nc.us/epi/gcdcpdf/CD1991-2002.pdf)

Determine the Geographic Distribution of Illness

Portray the Natural History of a Disease
Incidence (cases per 100,000) of selected food borne diseases in North Carolina, 1991-2002
0
5
10
15
20
25
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002
Inci
den
ce
E. coli O157 Salmonella Campylobacter Hepatitis A

Detect Epidemics / Define a Problem
• Identify baseline for disease
• Compare increase with baseline– Eyeball, experience
– CUSUM statistical methods
– Emerging Infect Dis. 1997; 3(3): 395-400

Underreporting in Surveillance
• Surveillance data may represent the “tip of the iceberg”
• True burden of disease depends on several factors– Clinical symptoms– Medical care seeking
behavior– Diagnosis– Reporting

Types of Surveillance
• Active vs. passive
• Clinician vs. laboratory

Outbreak Surveillance Sources
• Laboratory-confirmed reports of notifiable
diseases
• Clinician reports of notifiable disease
• Concerned parent/citizen reports to health
department
• Media

Outbreak Investigation

Why Investigate?
• Increase detected through surveillance
• Characterize the problem
• Prevention and control
• Research and answer scientific questions
• Train epidemiologists
• Political/legal concerns

CDC Guidelines for Systematic Investigations
• Verify diagnosis
• Confirm epidemic
• Identify and count cases (define)
• Tabulate and orient data: time, place, person
• Take immediate control measures

CDC Guidelines for Systematic Investigations (cont’d.)
• Initiate surveillance
• Formulate and test hypothesis
• Refine hypothesis
• Plan additional studies
• Implement and evaluate control measures
• Communicate findings

Exceptions to the Rule
• CDC guidelines provide a model for systematic outbreak investigations.
• No two outbreaks are alike!
• Steps of an outbreak could…– occur in a different order
– occur simultaneously
– be repeated after new information is discovered

Question and AnswerOpportunity

Case Study
The case study that will be used in today’s session and the June 8th session is based on an outbreak that occurred in Austin, Texas in 1998.

Case StudyToday we will review parts of the case study that
illustrate how to:
• Develop and use a case definition;
• Apply the process of case finding in detecting an outbreak;
• Verify the diagnosis; and
• Follow methods for generating a hypothesis.

Case Study
Disease Surveillance

Disease Surveillance
On the morning of March 11,1998, the
Texas Department of Health (TDH) received
a telephone call from a male student at a
nearby university

Disease Surveillance
• Student and his roommate were suffering from nausea, vomiting, and diarrhea– Both had become ill during the night– The roommate had taken medication – Neither student sought medical care– Both students believed a local pizzeria the
previous night was responsible– Students asked if they should go to class/take
midterm exam that afternoon

Disease Surveillance: Case Report
What questions would you ask the student?WHO: other ill persons – age, sex, symptoms, and whether
they sought care
WHAT: physical condition, symptoms, medication, and medical care sought
WHEN: when did the affected become ill
WHERE: city/school, address, telephone number of ill persons
WHY/HOW: suspected cause of illness, risk factors, modes of transmission, hints from those who did not become ill

Case Report:Who/Where

Case Report:What

Case Report:When/How

Case Report:When/How
• Student refused to provide food history beyond
foods eaten at local pizzeria
• He and his roommate shared no other meals in
the last 72 hours
• They ate separately at the University cafeteria

Disease Surveillance: Advice to the Caller
• What do you advise the student about attending classes
that day?
– Refer to personal clinician or student health center for
evaluation
– If asymptomatic, can return to normal activities
– Food handler?
– Work with high risk populations?

Disease Surveillance:What next?
• File the report and stop?
• Investigate further?

Deciding to Investigate
• Ideally, all reports of possible food borne
outbreaks should be investigated to:
– Prevent other persons from becoming ill
– Identify potentially problematic food handling
practices
– Add to the knowledge of food borne diseases

Maybe you should...
• If a severe (life-threatening) illness
• If there are confirmed clusters/large numbers
of a similar illness
• If food borne illness is in a food-handler
• If association with a commercially distributed
food

Deciding Not to Investigate
• Can’t investigate everything
• Often must choose the highest priority
• Outside pressure to investigate (media, politicians)

Maybe you shouldn’t...
• If signs/symptoms or confirmed diagnoses
among the affected suggest they might not
have the same illness
• If ill persons are not able to provide
adequate information for investigation,
including date and time of onset of illness,
symptoms, or a complete food history

Maybe you shouldn’t...
• If confirmed diagnosis and/or clinical symptoms
are not consistent with the foods eaten and the
onset of illness
• If there are repeated complaints made by the
same individual(s) for which prior investigations
revealed no significant findings

Case Study
Case Finding

Case Definition
To verify the existence of an outbreak, you must establish that a higher number of cases than expected is occurring.

Case Definition
A standard set of criteria for deciding whether an individual should be classified as having the disease of interest, including:
– Clinical criteria (signs, symptoms, and laboratory tests)
– Restrictions on time, place, and person

Case Definition
– The case definition can be modified as more data are obtained
– Do not include the hypothesis being tested in the case definition

Case Finding: Using the Case Definition
• Initial Case Definition: University student with diarrhea/vomiting in the previous 24 hours
• Look for more cases (student health center, hospitals, clinicians, dorm rooms) to determine the extent of the potential outbreak

Case Finding
• The pizzeria where the student and roommate had eaten was closed until 11:00 A.M.
• There was no answer at the University Student Health Center (left a message on the answering machine)

Case Finding
• A call to the emergency room at a local hospital revealed that 23 university students had been seen for acute gastroenteritis in the last 24 hours
• In contrast, only three patients had been seen at the emergency room for similar symptoms from March 5-9, none of whom were associated with the university

Case Finding
• At 10:30 A.M., a student health center physician returned the call and reported that 20 students with vomiting and diarrhea had been seen the previous day (no stool specimens were collected)
• The physician reported that 1-2 students per week typically would have been seen for these symptoms

Outbreak Detection: Is This an Outbreak?
Definition of an outbreak The occurrence of more cases of a disease than expected for a particular place and time
– Expected # of cases: ~5 per week– Actual # of cases: 40+ per day
Outbreak detected?Yes!

Prospective Case Finding
• TDH staff asked local health care providers to report cases of vomiting or diarrhea seen since March 5 at the:– University Student Health Center– Hospital A emergency room– Emergency departments at six other hospitals located
in the general vicinity
• Health care providers were asked to collect stool specimens from any new cases

Case Finding:Descriptive Epidemiology
• Afternoon of March 11, TDH staff visited the emergency room at Hospital A and
reviewed medical records of patients seen for vomiting and/or diarrhea since March 5
• Symptoms among 23 university students seen included:
– Oral temperatures ranged from 98.8/F (37.1/C) to 102.4/F (39.1/C)
– Complete blood counts showed an increase in white blood cells (n=10)

Symptom Profile
90%
68%
67%
66%
49%
85%
0% 20% 40% 60% 80% 100%
vomiting
diarrhea
cramp
fever
headache
muscle ache
Sy
mp
tom
Percent

Case Study
Verify the Diagnosis

Verify the Diagnosis: Microbiology• What broad categories of diseases might be
causing the outbreak?– Enteric viruses– Bacteria– Parasites– Toxins
• Stool specimens had been submitted for routine bacterial pathogens, but no results were available

Verify the Diagnosis: Microbiology• A TDH staff person was designated to help the facilities
identify and report cases
• Bacterial cultures from patients seen in the emergency rooms were performed at the collecting hospital and confirmed at the TDH Laboratory
• Specimens collected by the Student Health Center were cultured at the TDH Laboratory

Verify the Diagnosis: Potential Enteric Agents
Viruses Bacteria Parasites Toxins
Norwalk CampylobacterCyrptospor-idium parvum
Clostridium botulinum
Norwalk-like viruses (caliciviruses)
E. coli CyclosporaStaph. aureus
RotavirusSalmonella spp.
GiardiaMushroom toxins
Hepatitis A ShigellaEntamoeba histolytica
Fish/Shellfish toxins

Verify the Diagnosis: Find Plausible Agents
Evaluate:
• predominant signs and symptoms
• incubation period
• duration of symptoms
• suspected food
• laboratory testing of stool, blood, or vomitus

Verify the Diagnosis: Find Plausible Agents
• Pathogen identification will help identify the
potential incubation period
• Crucial to know the incubation period for
hypothesis generation
• Don’t need to wait for laboratory diagnosis to
proceed

Epidemiological Profiling
Syndrome Incubation
(hours)
Duration
(hours)
Vomiting Fever V / F
Vomiting-toxin
1.5-9.5 6.3-24 50-100 0-28 0-4.3
Diarrhea toxin
10-13 12-24 3.6-20 2.3-10 0.4-1.3
E. coli 48-120 104-185 3.1-37 13-25.3 0.3-1.1
Norovirus 34.5-38.5 33-47 54-70.2 37-63 0.7-1.7
Salmonella-like
18.0-88.5 63-144 8.9-51 31-81 0.2-1.0
Epidemiol Infect. 2001;127:381-7

Epidemiological Profiling
• Case Study chart review results (N=23)
– Vomiting = 90%
– Fever = 67%
– Vomiting / Fever =1.34
– Median duration = 39 hours

Epidemiological Profiling
Kaplan criteria for Norovirus outbreak:
– Incubation period 24 to 48 hrs
– Duration of illness 12 to 60 hrs
– Vomiting >50% of cases
– Modified to include vomiting/fever > 1.0
– Negative for other pathogens

Epidemiological ProfilingDuration Vomiting Vomiting / Fever
Case Study
39 hours
(median)
90% of cases
1.34
Kaplan
Criteria for Norovirus
16 – 20 hours
> 50% of cases
> 1.0

Noroviruses
Today’s Guest Expert:
Penny Padgett, PhD, MPH

NOROVIRUSES
• Norwalk Virus
• Group of related,
SS RNA non-
enveloped viruses
• Cause acute gastro-
enteritis in humans

Physical Properties
• Relatively resistant to environmental challenge: they are able to withstand freezing and temperatures as high as 60 degrees Celsius (steamed shellfish)
• May be present in up to 10 ppm chlorine

NOROVIRUSES
• The estimated total cases of Norovirus infection is 23,000,000 in the U.S. per year.
• Approximately 40% of Norovirus infections are food borne.
• Noroviruses are responsible for 67% of the total food borne infections, 32 % of the hospitalizations and 7% of the deaths.

Clinical Presentation
• Incubation period is usually 24-48 hours
• Acute onset vomiting
• Watery, non-bloody diarrhea with abdominal cramps
• Nausea
• Low-grade fever may occur

Clinical Presentation (Con’t)
• Dehydration is the most common complication, especially among the young and the elderly
• Symptoms usually last between 24 to 60 hours
• Recovery is usually complete and there is no evidence of long term complications
• Asymptomatic infection may occur in as many as 30% of the infected

Treatment and Management
• No specific therapy exists for viral gastroenteritis
• Standard symptomatic therapy consists of replacing fluid losses and correcting electrolyte imbalances through oral and intravenous fluid administration

Virus Transmission
• Noroviruses are transmitted primarily through the fecal-oral route via fecally contaminated food or water or by direct person-to-person spread
• Fomite contamination may also act as a source of infection
• Aerosolization of vomitus may spread the virus but not through the respiratory system

Virus Transmission (Con’t)
• Noroviruses are highly contagious – an inoculum of as few as 10 viral particles may be sufficient
• Shedding usually begins with the onset of symptoms (although there may be some pre-symptom shedding) and may continue for two weeks after recovery

Specimen Collection
Human
Identification can best be made from stool specimens taken within 48-72 hours after the onset of symptoms. Vomitus and serum may also be collected and tested.

Specimen Collection
Environmental
Food and water samples can be collected and tested. Water samples should be filtered to increase the concentration of virus present

Detection of Virus
• Reverse Transcription-Polymerase Chain Reaction (RT-PCR) is considered to be a highly sensitive and accurate method for viral detection
• Direct and Immune electron microscopy
• Detection of a fourfold increase in specific antibodies in acute and convalescent serum samples
• An Enzyme Linked Immunosorbent Assay (ELISA) for detection in stools is under development

Prevention
Prevention is based on:
• The provision of safe food and water
• Correct handling of cold foods
• Frequent hand washing
• Paid sick leave

Cruise Ships

Cruise Ships• Cruise ships represent a closed population
which can be studied as a cohort
• Highly infectious agents can spread very quickly through the population
• Difficult to clean and contain infection during the cruise

Vessel Sanitation Program
• Unannounced, twice yearly inspections
• Inspection takes place in U.S. ports
• Ships are required to maintain a standardized illness report for each cruise

Microbiologic Investigation: Specimen Information
• Each stool specimen should be submitted with:– Patient’s name or identification number– Dates
• Date of collection of specimen• Date of onset of symptoms
– Signs and symptoms • may suggest a particular agent and lead the lab to
perform specific testing

Additional Specimen Information
• If submitting a stool specimen for multiple tests, divide, label, and preserve each sample accordingly
• Indicate on the requisition slip if testing is requested for specific, suspected pathogens

Additional Specimen Information
If you have questions prior to submitting a stool specimen, contact the NC State Laboratory of Public Health at:
– (919) 733-7834
– Web site: http://slph.state.nc.us/

Specimen Collection Recommendations
More information on recommendations for collection of stool specimens for laboratory examination may be found in:
Morbidity and Mortality Weekly Report: Recommendations and Reports 1990; 30 (No. RR-14)

Case Study
Back to the lecture on Verifying the Diagnosis. . .

Verify the Diagnosis: Culture Results
Later in the afternoon of March 11th, culture
results from 17 ill students became available

Verify the Diagnosis: Culture Results
• Results were primarily from the emergency room at Hospital A on March 10
• Results did not identify Salmonella, Shigella, Campylobacter, Vibrio, Listeria, Yersinia, Escherichia coli O157:H7, Bacillus cereus, or Staphylococcus aureus
• Some specimens were positive for fecal leukocytes and fecal occult blood

Microbiology Diagnosis:Interpretation of Results
What do these results mean, and what
questions do they raise?

Microbiology Diagnosis:Interpretation of Results
• Potential reasons for negative results:
– Mishandling of specimen resulting in death of the pathogen (during storage, transport, processing, or culture)
– Specimens collected too late in the illness
– Illness could be due to a bacteria not tested for, or due to a non-bacterial agent

Case Study
Hypothesis Generation

Hypothesis Generation
Day 2 (March 12)…
– 75 persons with vomiting or diarrhea reported
– All were university students who lived on campus
– No cases among faculty or staff, or locals
– Median patient age 19 years (range: 18-22)
– 69% were freshman
– 62% were female

Hypothesis Generation:Line Listing
This line listing has been sorted on the “Age” data field.

Hypothesis Generation:Epidemic Curve
Most dates of illness onset were March 9-12

Hypothesis Generation:Meet with University Officials
– Negotiate cooperation with the university officials
– Inform, update, plan, and coordinate

Hypothesis Generation:Meet with University Officials
Collect information that might provide insights into the source of the outbreak, including:
– Characteristics of the student body– Sources of food/water, dining establishments– Possible contact with animals through classes– Student living arrangements

Hypothesis Generation: Information Collected
• The university is located in a small Texas town with a population of 27,354
• Enrollment of approximately 12,000 students
• 2,386 students live on campus – 36 residential halls on the 200+ acre main
campus– Most enrolled in on-campus meal plan
• About 75% of the students are Texas residents

Hypothesis Generation:Information Collected
• The university uses municipal water and sewage services
• There have been no breaks or work on water or sewage lines in the past year
• There has been no recent road work or digging around campus

Hypothesis Generation:Information Collected
Main cafeteria
– Used by most on campus students
– Serves hot entrees, as well as items from
the grill, deli bar, and a salad bar

Hypothesis Generation:Information Collected
Smaller cafeteria
– Used by students who live off campus
and university staff
– Also serves hot entrees, grilled foods,
and a salad bar, but has no deli bar
– Offers menu selections with a per item
cost
– Accessible to meal plan members

Hypothesis Generation:Information Collected
• Both cafeterias under same management
• Also about half a dozen fast food places on campus

Hypothesis Generation:Information Collected
• Spring break begins on March 13, at which
time all dining services will cease until
March 23
• Many students will leave town during the
break, but about 25% of those living on
campus will remain

Hypothesis Generation:Case Interviews
Hypothesis generating interviews were done with seven of the earliest case-patients reported by the ER and student health center

Hypothesis Generation: Case Interviews
• All 7 cases had onset of illness on March 10
• Four were male and three were female
• All but one was a freshman
• Two students were psychology majors; one each was majoring in English and animal husbandry. Three students were undecided

Hypothesis Generation: Case Interviews
• Except for the psychology majors, none of the other students shared any classes
• Only one student had a roommate with a similar illness
• Lived in five different residential halls

Hypothesis Generation: Case Interviews
• Five students belonged to a sorority or a fraternity
• Three students had attended an all school mixer on March 6, the Friday before the outbreak began

Hypothesis Generation: Case Interviews
• Two students went to an all night science fiction film festival at one of the dorms on March 7
• Students reported attendance at no other special events; most had been studying for midterm exams for most of the weekend

Hypothesis Generation: Case Interviews
Seven day food history:
– All reported eating most of their meals at the
university’s main cafeteria
– All but one student had eaten food from the deli bar
– Two had eaten food from the salad bar
– Three from the grill
– Only one had eaten food from the pizzeria
– No particular food item that was common to all or
most of the students

Hypothesis Generation

Hypothesis Generation
What are your leading hypotheses for the cause of
the outbreak?
Consider:
1. Pathogen
2. Mode of transmission
3. Source of outbreak
4. Time period of interest (incubation)

Hypothesis Generation:1. Pathogen
• Signs and symptoms (vomiting, diarrhea, fever, bloody stools, fecal leucocytes, and fecal occult blood) consistent with acute gastrointestinal infection
• Negative bacterial cultures suggest a viral or parasitic pathogen
• Symptoms more consistent with virus

Hypothesis Generation:1. Pathogen
Epi Curve suggests a point source outbreak and short exposure period
More consistent with a virus than parasite

Hypothesis Generation: 2. Mode of Transmission
• Illness is limited to students living on
campus
• Lack of illness in community, faculty,
suggests city or university water systems
not affected

Hypothesis Generation: 2. Mode of Transmission
• Not spread person-to-person
– Cases did not cluster by dorm or classes
• All 7 students ate at university main
cafeteria and deli bar
– Not used by off-campus students or faculty

Hypothesis Generation: 3. Source
• No common food items identified among 7 students
• Viral agents are commonly transmitted through – Sandwiches– Salads – Raw / undercooked shellfish

Hypothesis Generation: 4. Period of Interest
• Viral gastroenteritis– Incubation ranges <1day to ~7 days
• Majority of onset– March 10 – 12
• Likely exposure period– March 5 – 10– (<1 to 7 days before case onset)

Hypothesis Generation
Leading Hypothesis:
Viral infection spread by a food or beverage served at the university main cafeteria
between March 5 and March 10.

What Next?
• Have you proven your hypothesis?– No!– Information suggests, but does not prove, that
the cause of the outbreak was in the main cafeteria
• Can control measures be taken?– Not yet

What Next?
Next Steps:
1. Environmental investigation
2. Conduct a controlled study

Environmental Investigation
Today’s Guest Expert:
Ron Holdway,
Environmental Health Director, Orange Co. Health Department

ORANGE COUNTY HEALTH DEPARTMENT
DR. ROSEMARY SUMMERS, DIRECTOR
ENVIRONMENTAL HEALTH DIVISION

ORANGE COUNTY HEALTH DEPARTMENT
Presented: April 13th, 2004
THE NOROVIRUS OUTBREAK AT THE UNIVERSITY OF NORTH CAROLINA
January 2004

The UNC Outbreak
• Background
• Questions and Issues
• Environmental Investigation and Control Measures
• Final Analysis / Results

The UNC Outbreak
Background

The UNC OutbreakBackground
• Call from UNC Student Health on January 21st – AM
• A few cases (4-6) presented on 1-20
• Many more (50-60) presented on 1-21
• OCHD Epi Team convened at UNC SHS office

The UNC OutbreakBackground
• Epi Team Work on 1-21– Understanding of situation (easier said than done!)– Met with UNC SHS and EHS representatives – Met with food service representatives– Consulted with State epi representatives– Alert/query to private providers in the community– Outbreak (epidemic) or not? (YES!)– Limited to UNC universe? (Yes)– Case definition

The UNC OutbreakBackground
• Epi Team Work on 1-21 (cont.)
– Possible agents and transmission modes – Questionnaire development & testing– Administer questionnaire (began that night around 8pm after testing)– Implemented general control measures– Interviews with press representatives– Some food samples– At least one vomitus sample

The UNC OutbreakBackground
• Case Definition
– “A UNC student with an acute episode of nausea, vomiting and/or diarrhea with onset on or after 6PM on 1-20-04”

The UNC OutbreakBackground
• Possible Agents
– Based on signs, symptoms and those that occur first or predominate - vomiting was occurring first and appeared to be predominating in this outbreak
– Sudden or gradual increase in cases?

The UNC OutbreakBackground
• Possible Agents (cont.)
– Among those considered for this outbreak:• Bacillus cereus toxin• Staphylococcal aureus toxin• Norovirus• Metal or other elemental poisoning• Fish and shellfish toxins

The UNC Outbreak
Questions and Issues

The UNC OutbreakQuestions and Issues
• Point source or not?
• Contained to UNC?
• Intentional?
• Questionnaire and study
• Snow storm during event

The UNC OutbreakQuestions and Issues
Point Source or Not?
• Time, place, person associations• Epi curve(s) - we reviewed the numbers of cases at least
daily• Surveillance and disease presence in the general
population– ED– Private providers– PHRST Team

The UNC OutbreakQuestions and Issues
Intentional?
• Don’t discount until investigation and analyses are complete– Even then . . . there is the case from The Dalles, Oregon
• Many agents aren’t conducive to intentional releases• Considered but discounted for this outbreak

The UNC OutbreakQuestionnaire and Study
• Case-control study
• Obtain well interviews from sick contacts (room mates, suite mates, etc.)
• Initial software was spreadsheet, but was changed to Epi Info

The UNC OutbreakQuestionnaire and Study
• Food histories (at least 48 hours prior) - on-campus and off
• Contacts
• Other environmental exposures– Vomitus– Dorms– Travel– Swimming pools

The UNC OutbreakQuestionnaire and Study
• Obstacles, Problems and Lessons Learned
– Vast array of foods at UNC dining halls– Study was designed to get controls from contacts of
sick - this approach was flawed– Data from multiple inputs stations could not be
merged by OCHD - problem finally solved by Drew Voetsch

The UNC Outbreak
Environmental Investigation and
Control Measures
(Those used or considered)

The UNC OutbreakEnvironmental Investigation and
Control Measures
• Dorm sweeps• Interviews• SHS waived after hours fees• UNC installed waterless hand sanitizer• stations in the dining halls• Cleaning supplies were made available in
the dorms through the RAs

The UNC OutbreakEnvironmental Investigation and
Control Measures
Communications• Student emails and web postings• Hand wash posters and signs • UNC, State Epi and County officials• Advisories to housekeeping staff• Press

The UNC OutbreakEnvironmental Investigation and
Control Measures– Environmental investigations / interventions
• Water line work on campus in the last two weeks?
• Chemical transportation in the last week?• Increased fomite cleaning• Vomitus control
– Once food and locations was suspected (1-22), close the facility or not?

The UNC OutbreakEnvironmental Investigation and
Control Measures– Sampling through two labs (SLPH and UNC SPH)
• Food (facility keeps samples for one week)• Stool• Vomitus
– Review of food operations and procedures
– Assessment of connection to other concurrent outbreaks in the region

The UNC OutbreakEnvironmental Investigation and
Control Measures
– Once food and location were suspected (1-22), close the facility or not?
• On-going outbreak? (No)
• Extensive problems discovered during operational review? (No)

The UNC Outbreak
Investigation Analysis / Results

The UNC OutbreakAnalysis / Results
• Duration - Jan. 20th thru Feb. 13th
• Total Cases - Suspected and Confirmed - 425 Persons
• Agent was norovirus
• Statistically linked to the salad bar at one dining hall
• Could not link to a specific food item

The UNC OutbreakAnalysis / Results
• Primary outbreak was point-source
• Many secondary cases - person-to-person and environmental exposure

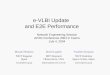
The UNC Outbreak
0
5
10
15
20
25
30
351/
18 M
idni
ght-
6am
1/18
6am
-Noo
n1/
18 N
oon-
6pm
1/18
6pm
-Mid
nigh
t1/
19 M
idni
ght-
6am
1/19
6am
-Noo
n1/
19 N
oon-
6pm
1/19
6pm
-Mid
nigh
t1/
20 M
idni
ght-
6am
1/20
6am
-Noo
n1/
20 N
oon-
6pm
1/20
6pm
-Mid
nigh
t1/
21 M
idni
ght-
6am
1/21
6am
-Noo
n1/
21 N
oon-
6pm
1/21
6pm
-Mid
nigh
t1/
22 M
idni
ght-
6am
1/22
6am
-Noo
n1/
22 N
oon-
6pm
1/22
6pm
-Mid
nigh
t1/
23 M
idni
ght-
6am
1/23
6am
-Noo
n1/
23 N
oon-
6pm
1/23
6pm
-Mid
nigh
t1/
24 M
idni
ght-
6am
1/24
6am
-Noo
n1/
24 N
oon-
6pm
1/24
6pm
-Mid
nigh
t1/
25 M
idni
ght-
6am
1/25
6am
-Noo
n1/
25 N
oon-
6pm
1/25
pm
-Mid
nigh
t1/
26 M
idni
ght-
6am
1/26
6am
-Noo
n1/
26 N
oon-
6pm
1/26
6pm
-Mid
nigh
t
Reported illness onset (6 hour intervals)
An
y re
po
rted
illn
ess
SOURCE: Drew Voetsch, UNC-CH

The UNC Outbreak
PRIMARY AND SECONDARY CASES CONFIRMED AT STUDENT HEALTH SERVICES (BY DAY)
0
10
20
30
40
50
60
70
01/2
0/20
0401
/21/
2004
01/2
2/20
0401
/23/
2004
01/2
4/20
0401
/25/
2004
01/2
6/20
0401
/27/
2004
01/2
8/20
0401
/29/
2004
01/3
0/20
0401
/31/
2004
02/0
1/20
0402
/02/
2004
02/0
3/20
0402
/04/
2004
02/0
5/20
0402
/06/
2004
02/0
7/20
0402
/08/
2004
02/0
9/20
0402
/10/
2004
02/1
1/20
04
DATE
CASES

Case Study
Back to the Texas case study environmental investigation. . .

Environmental Investigation:Conduct Interviews
• TDH environmental sanitarians inspected the main cafeteria and interviewed staff on March 12
• Except for one employee who worked at the deli bar and declined to be interviewed, all dining service personnel were interviewed

Environmental Investigation:Food Handler Interviews
Topics to cover:
1. Food items served during the implicated time period
2. Illness among staff or their family members during the time period
3. Hygienic practices and hand washing facilities
4. Stool specimens from food handlers

Environmental Investigation:Food Handler Interviews
Topics to cover:
5. Watch/reconstruct food preparation/handling practices performed during the time period
6. Which staff were responsible for what during the time period
7. Recipes for food items served, ingredients and their sources

Environmental Investigation: Food Handler Interview Results
• Thirty-one staff members were employed at the cafeteria– 24 (77%) were food handlers
• No food handlers interviewed reported being ill in the last two weeks
• Stool cultures were requested from all cafeteria staff

Environmental Investigation:Food Handling Practices Observed
• In the cafeteria, the deli bar had its own preparation area and refrigerator
– Sandwiches were made to order by a food handler– Newly prepared deli meats, cheeses, and condiments
were added to partially depleted deli bar items from the day before (without discarding leftover food items)
– While the deli was open, sandwich ingredients were not kept refrigerated. The deli bar containers were not routinely cleaned

Environmental Investigation: Sampling
• Samples of leftover food, water, and ice were collected

Environmental Investigation:
Evidence-Based Decision
By dinner on March 12, the City Health
Department closed the deli bar

Environmental Investigation:Points to Consider
• Do you agree with the decision to close the deli bar?– Circumstantial evidence only– Many unsafe practices identified
• What do you think the next step should be?

Today’s Conclusions:
• We detected an outbreak of viral
gastroenteritis
• We developed a leading hypothesis with
the main campus cafeteria as the suspect

Stay Tuned for the
Next Session. . .
Next time we will:
1. Develop a study design to test the leading
hypothesis
2. Determine what evidence we need to act on
the hypothesis

Next Session June 8th
10:00 a.m. - Noon
Topic: “Study Design”

Session I SlidesFollowing this program, please visit one of the web
sites below to access and download a copy of today’s slides:
NCCPHP Training web site:http://www.sph.unc.edu/nccphp/training/index.html
North Carolina Division of Public Health, Office of Public Health Preparedness and Response
http://www.epi.state.nc.us/epi/phpr/

Site Sign-in Sheet http://www.sph.unc.edu/nccphp/
Please mail or fax your site’s sign-in sheet to:
Jennifer HorneyDirector of Training and EducationNC Center for Public Health PreparednessCB #8165, 400 RobersonChapel Hill, NC 27599
FAX: (919) 843 - 5563