-
8/13/2019 2001 Respiratory Review
1/46
Review of Respiratory
Physiology
-
8/13/2019 2001 Respiratory Review
2/46
Steady State
Lung O2Uptake rate
= Cell O2Utilization rate
Cell CO2Production rate
= Lung CO2Release rate
-
8/13/2019 2001 Respiratory Review
3/46
Gaseous Environment.
Atmosphere: Nitrogen and Oxygen,
negligible Carbon Dioxide.
Clinical Relevance of Environment Altitude: PO2depends on PB
Suffocation: PO2depends on fractional O2
Oxygen therapy: PO2depends on fractional O2
P F PI I BO O2 247 ( )
-
8/13/2019 2001 Respiratory Review
4/46
Diffusion and Diffusion
Abnormality
-
8/13/2019 2001 Respiratory Review
5/46
Ficks Law for Diffusion for Gases
O2
CO2
T
P1
P2
A
( )V A D
TP P
gas
1 2
-
8/13/2019 2001 Respiratory Review
6/46
Single Breath DLCO
Single inspiration of a dilute CO
mixture
10 second breath-hold
Measure CO uptake using infrared
detector to compare inspiratory and
expiratory concentrations
Normal Value: 25 ml/min/mmHg
-
8/13/2019 2001 Respiratory Review
7/46
Clinical Interpretation of DLCO.
Decreases with loss of surface area.
Decreases with increasing membrane
thickness
Decreases with ventilation/perfusionmismatching
Summary: DLCO better index of overalllung function than
diffusion capabilitiesper se.
-
8/13/2019 2001 Respiratory Review
8/46
Two Factors Affect Gas Transfer
Rate
Diffusion rate of a gas Perfusion Rate (Pulmonary blood
flow)
Gases must be carried away to maintainlocal diffusion gradients
in the lung.
-
8/13/2019 2001 Respiratory Review
9/46
O2Diffusion duringNormoxia
-
8/13/2019 2001 Respiratory Review
10/46
Lung Mechanics in Obstructive
and Restrictive Disease
-
8/13/2019 2001 Respiratory Review
11/46
Measuring vital capacity and its
subcomponents. Use a spirometer.
TLC
RV
VC
TV
FRC
ICIRV
ERV
RV
Can Use
Spiromenter
Cant Use a Spirometer
-
8/13/2019 2001 Respiratory Review
12/46
Measuring Residual Volume
Cant use a Spirometer
Use instead:
Nitrogen Washout
Helium Dilution Method
Plethysmograph
-
8/13/2019 2001 Respiratory Review
13/46
Obstructive Disease
Difficult to get air out of the lungs
Obstruct expiration
Examples:
emphysema
chronic bronchitis
asthma.
-
8/13/2019 2001 Respiratory Review
14/46
Restrictive Disease
Difficult to get air in to the lungs
Restrict inspiration
Examples:
intersitial fibrosis
sarcoidosis
muscular diseases
chestwall deformities.
-
8/13/2019 2001 Respiratory Review
15/46
Lung Capacity and Disease
Summary
Obstructive Disease:
Decreased VC
IncreasedTLC, RV, FRC.
Restrictive Disease:
Decreased VC
DecreasedTLC, RV, FRC.
-
8/13/2019 2001 Respiratory Review
16/46
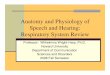
Fig 5: Lung Capacity and
Disease
Normal
RV
ERV
TV
IRV
FRC
VC
Restrictive
RV
ERV
TV
IRV
FRC
VC
Obstructive
RV
ERV
TV
IRV
FRC
VC
125
100
75
50
25
0
%NormalTLC
-
8/13/2019 2001 Respiratory Review
17/46
Forced Vital Capacity
FEV1.0 / FVC Ratio
-
8/13/2019 2001 Respiratory Review
18/46
Small Airways Disease
FEF25-75
-
8/13/2019 2001 Respiratory Review
19/46
Flow -Volume Curves
Peak Flow
-
8/13/2019 2001 Respiratory Review
20/46
Pulmonary Function Summary
Obstructive
Disease
Restrictive
Disease
FEV1.0
Decreased Decreased
FVC Decreased Decreased
FEV1.0/FVC Decreased Unchanged or
IncreasedPeak Flow Decreased Decreased or
Unchanged
RV/TLC Increased Unchanged
-
8/13/2019 2001 Respiratory Review
21/46
CLINICAL USE OF IDEAL
ALVEOLAR GAS VALUES
-
8/13/2019 2001 Respiratory Review
22/46
Ideal Alveolar Gas Equation.
P PP
RP F R
RA IA
A IO OCO
CO O2 2
2
2 21
Clinically Useful Form:
Complete Form:
P PP
RA I
A
O O
CO
2 2
2
-
8/13/2019 2001 Respiratory Review
23/46
USE #1
Compare PAO
2to P
aO
2
Healthy people: PAO2= PaO2
Two Approaches to Comparison
(PAO2 - PaO2) difference
PaO2/ PAO2 ratio
-
8/13/2019 2001 Respiratory Review
24/46
A-a Difference
PAO2- PaO2
Normally 5-20 mmHg
Because of normal anatomical shunt
Ventilation/Perfusion mismatching.
A-a difference increases with
pulmonary disease. Problem: Normal range changes on
100% O2.
-
8/13/2019 2001 Respiratory Review
25/46
a/A ratio
Normally averages just over 0.8 (Am.Rev. Resp. Dis. 109:
142-145, 1974).
a/A ratio falls with pulmonarydisease.
Lower limit normal:
young (room air) : 0.74 older(room air) : 0.78
Both groups (100% O2): 0.82
-
8/13/2019 2001 Respiratory Review
26/46
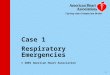
(A-a) Difference vs. a/A Ratio
Normal
Normal
(A-a)PO2Difference(mmHg)
a/A
PO2
ratio
Sick
Sick
-
8/13/2019 2001 Respiratory Review
27/46
Use #2
PAO
2Estimates P
cO
2
Useful for calculation of VenousAdmixture or Shunt
-
8/13/2019 2001 Respiratory Review
28/46
Venous Admixture
'
'
Q
Q
C C
C C
S
T
c a
c v
O O
O O
2 2
2 2
QT CaO2
(QT - Qs ) CcO2
Qs CvO2
PAO2
-
8/13/2019 2001 Respiratory Review
29/46
Diagnosis of True Shunt
Breathing 100% oxygen -
will notabolish hypoxemia due toshunt
REASON: shunted blood never
exposed to the high alveolar PO2.
-
8/13/2019 2001 Respiratory Review
30/46
Blood Gases
-
8/13/2019 2001 Respiratory Review
31/46
Oxygen Blood Gas Quantities
Partial Pressure
Saturation
Content
Carrying Capacity: O2content at
100% saturation.
-
8/13/2019 2001 Respiratory Review
32/46
Significance of Sigmoid Curve
4 Point Curve
Critical PO2
V
-
8/13/2019 2001 Respiratory Review
33/46
Defining Content and Capacity
C Hb SOO
2
2136100%
. [ ] %
-
8/13/2019 2001 Respiratory Review
34/46
Blood
Hemoglobin --> Allows Blood to hold
more oxygen. P50: Reciprical to Hb-O2Affinity
(H+, CO2, Temp, & 2,3-DPG)
Capacity: Anemia, Polycythemia
Hematocrit
Hemoglobin
Hemoglobin variants exist (e.g. Hbf)
-
8/13/2019 2001 Respiratory Review
35/46
Four (+one) Things Change
Oxyhemoglobin Affinity Hydrogen Ion Concentration, [H+]
Carbon Dioxide Partial Pressure, PCO2
Temperature [2,3-DPG]
Special Case: Carbon Monoxide
-
8/13/2019 2001 Respiratory Review
36/46
Three Things That Change O2
Carrying Capacity
Changes in Hb Concentration
Presence of Carbon Monoxide
Formation of Methemoglobin
-
8/13/2019 2001 Respiratory Review
37/46
Minute Ventilation
Flow (vol/time) moved into or out of
the lungs.
Measured by collecting expiredvolume for a fixed time.
Normal value is 7.5 L/min (BTPS).
V V fE T
-
8/13/2019 2001 Respiratory Review
38/46
Partitioning Minute Ventilation.
Alveolar Ventilation: the volume per
min entering gas exchange surfaces.
Dead space Ventilation: the volumeper min that is wasted
( )V V V V V f V f V f A E d T d T d
-
8/13/2019 2001 Respiratory Review
39/46
Alveolar Ventilation Equation.
(Rearranged)
PV (STPD)
863 mmHgACO
CO2
2
( )V BTPSA
-
8/13/2019 2001 Respiratory Review
40/46
Defining Adequate Ventilation
Normal--> PaCO2= 40 mmHg
Hypoventilation --> High PaCO2
Hyperventilation --> Low PaCO2
-
8/13/2019 2001 Respiratory Review
41/46
Respiratory Acid-Base
Henderson-Hasselbach Equation:
Changes in PCO2cause changes in [H+] bymass action. Increased
PCO2 resp. acidosis
Decreased PCO2 resp. alkalosis.
CO H O H CO H H CO 2 2 2 3 3 Carbonic Anhydrase
pHH CO
PCO
6 1
0 03
3
2
. log[ ]
( . )
-
8/13/2019 2001 Respiratory Review
42/46
-
8/13/2019 2001 Respiratory Review
43/46
Hypoxemia Analysis
Step 1
Is PACO2> 40 mmHg
ANDa/A > 0.74 or (A-a) < 20 mmHg
PureHypoventilation
yes
Choose between:
ShuntDiffusion AbnormalityV/Q Mismatching
No
Continue
-
8/13/2019 2001 Respiratory Review
44/46
Hypoxemia Analysis
Step 2
CanHypoxemia be eliminated
by 100% O2
TrueShunt
No
Choose between:
Diffusion AbnormalityV/Q Mismatching
Yes
Continue
-
8/13/2019 2001 Respiratory Review
45/46
Hypoxemia Analysis
Step 3
Is the DLCO
Normal?
Diffusion Normalmust be
V/Q Mismatching
yes
No
Cant choose between:Diffusion AbnormalityV/Q Mismatching
or Combination
-
8/13/2019 2001 Respiratory Review
46/46
Questions?